")
Back to Journals » Clinical Optometry » Volume 15
At-Home Trial of Four Different Head-Mounted Displays in Visual Rehabilitation of People with Stargardt Disease
Authors Schmidt DC , Kjølholm CDB, Torner Jordana J , Spange V, Højstrup PD, Larsen BS, Kessel L
Received 11 August 2023
Accepted for publication 28 October 2023
Published 28 November 2023 Volume 2023:15 Pages 271—281
DOI https://doi.org/10.2147/OPTO.S434404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Diana Chabané Schmidt,1 Christine Dahlgren Bohnsack Kjølholm,1 Joaquim Torner Jordana,1 Vibeke Spange,1 Pernille Duelund Højstrup,2 Bo Schack Larsen,2 Line Kessel1,3
1Department of Ophthalmology, Copenhagen University Hospital Rigshospitalet-Glostrup, Glostrup, Denmark; 2Institute for the Blind and Visually Impaired, Hellerup, Denmark; 3Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Diana Chabané Schmidt, Department of Ophthalmology, Copenhagen University Hospital Rigshospitalet-Glostrup, Valdemar Hansens Vej 13, Glostrup, 2600, Denmark, Email [email protected]
Purpose: To examine the potential of different head-mounted displays in the rehabilitation of individuals with visual impairment.
Methods: This prospective explorative study conducted between September 2019 and August 2020 included participants with Stargardt disease with moderate to severe visual impairment and a relatively preserved peripheral visual field. AceSight, eSight 3, IrisVision Live, and Jordy were tested. After instruction and training, participants chose two head-mounted displays for home use for two weeks per device. The Canadian Occupational Performance Measure was used for evaluation.
Results: Twelve participants (aged 16– 53 years) tested all head-mounted displays in the clinic. Distance visual acuity and reading distance improved with all head-mounted displays and eSight and Irisvision improved near visual acuity. Six participants decided not to test the head-mounted display at home due to lack of time or energy, dizziness and discomfort, double vision and peripheral visual field limitation, or aesthetics. After home use, the participants reported improved visual function at a distance with IrisVision, AceSight, and e-Sight, whereas only AceSight improved vision during near tasks. IrisVision and eSight improved reading ability, and none of the devices improved vision during tasks involving computers. Five participants used the devices sparingly, and five avoided public use owing to aesthetics.
Conclusion: We found an improvement in distance visual acuity and increased reading distance for all tested head-mounted displays. Additionally, IrisVision and eSight improved visual function at near and eSight also improved contrast vision at distance. Despite the possibility of improving vision, social stigma and device aesthetics kept the participants from using head-mounted displays in public and limited their use at home.
Plain Language Summary: This study explored the potential of four different head-mounted displays for visual rehabilitation.Visual impairment not only affects daily activities but also limits participation in education, work, and social interactions.Patients with Stargardt disease tested the displays in a clinical setting and at home.We found that the head-mounted displays improved visual function. However, the patients did not wish to use the devices publicly due to social stigma and their aesthetics.The development of smaller and lighter devices that focus on aesthetics could increase usage.
Keywords: head-mounted display, visual aid, visual impairment, electronic glasses, Stargardt disease
Introduction
Blindness and visual impairment affect an estimated 2.2 billion individuals worldwide and can lead to reduced quality of life, limit social interaction, and result in difficulties with education and employment.1,2 In particular, central vision loss affects daily activities, such as reading, cooking, and recognizing faces.3 Individuals with visual impairment commonly use various types of visual aids, including telescopes, microscopes, telemicroscopes, optical or electronic magnifiers, filters, and electronic enhancements on computers.
In the past few decades, commercially available head-mounted displays that utilize a camera to provide visual input to the user have been developed. These devices offer a continuous range of magnification levels, brightness adjustments, contrast enhancements, color inversions, and color adjustments. Previous studies conducted on different head-mounted displays have reported improvements in visual acuity, quality of life, and activities of daily living for individuals with visual impairment.4,5 However, users have also reported experiencing neck pain, dizziness, nausea, and a reluctance to wear the devices due to concerns about stigma and aesthetics.5–7 Studies with independent funding comparing various head-mounted displays are lacking.
Stargardt disease is a rare genetic disease characterized by progressive retinal degeneration, resulting in bilateral central vision loss, photosensitivity, color vision abnormalities, and delayed dark adaptation. Initial vision loss typically occurs in childhood, adolescence, or early adulthood with variable progression rates.8 Patients with Stargardt disease typically have extensive experience with various visual aids and benefit from magnification. In this prospective exploratory study, we aimed to compare the functionality and usability in a real-life setting of four different head-mounted displays (AceSight, eSight, IrisVision, and Jordy) among a group of patients with Stargardt.
Methods
This prospective, exploratory study was conducted between September 2019 and August 2020 at the Department of Ophthalmology, Rigshospitalet-Kennedy Center, and the Institute for Blind and Partially Sighted (IBOS) in Copenhagen, Denmark. Participants were recruited from the Department of Ophthalmology. The inclusion criteria were genetically diagnosed Stargardt disease, age between 16 years and 67 years (the age of retirement), residence in the Capital Region of Denmark, a best-corrected visual acuity of the better-seeing eye between 20/60 and 20/400 feet corresponding to moderate to severe visual impairment, and a peripheral visual field of at least 30 degrees from the edge of the central scotoma. Participants were required to have prior experience using visual aids, including telescopes, microscopes, telemicroscopes, optical magnifiers, or electronic magnifiers, and to benefit from magnification. The study evaluated four different head-mounted displays: AceSight (Zoomax Technology Co., Ltd., MA, USA), eSight 3 (eSight, Corp., CA, USA), IrisVision Live (IrisVision Global Inc., Pleasanton, CA, USA), and Jordy (Enhanced Vision Systems, CA, USA) AceSight featured an 8-megapixel camera and a screen resolution of 1920×1080. The device had a head-mounted weight of 360 g and offered a magnification of up to 15 times. eSight was the most expensive device, with a 21.5-megapixel camera and a 1024×768 OLED screen. It weighed 104 g and offered a magnification of up to 24 times. IrisVision had a 12-megapixel camera and a 2560×1440 OLED screen. It weighed 498 g and had a magnification of up to 12 times. Jordy was the least expensive device with a 0.9-megapixel camera and a screen resolution of 1280×720. It weighed 236 g and had a magnification of up to 30 times (Supplementary Table A1).
This study was reviewed by an independent ethical review board (Scientific Ethics Committee, Journal No. H-19016901), and conformed to the principles and applicable guidelines for the protection of human subjects in biomedical research. The participants provided informed consent and the tenets of the Declaration of Helsinki were followed.
The study had a mixed-method design with the collection of both qualitative and quantitative information and consisted of seven phases including an ophthalmologic examination, visual tests, evaluations of activities of daily living using head-mounted displays, and questionnaires (Figure 1).
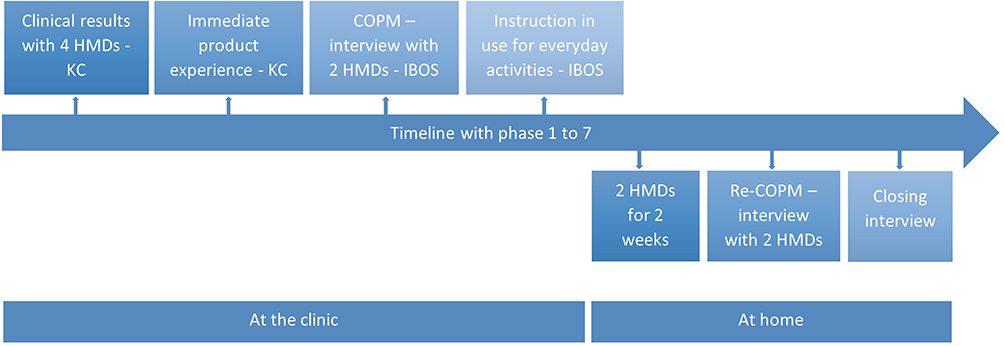 |
Figure 1 Study phases. Abbreviations: HMD, head-mounted display; COPM, Canadian Occupational Performance Measure; IBOS, Institute for the Blind and Partially Sighted. Note: KC, Department of Ophthalmology, Kennedy Center. |
Phase 1
In the first phase, the participants underwent an evaluation of their medical history and a standard eye examination by an ophthalmologist, including kinetic perimetry with Goldmann object size and intensity III-4e (Haag-Streit, Koeniz, Switzerland), static perimetry with Octopus 900 (Haag-Streit International, Koeniz, Switzerland) with the 30–2 pattern and TOP strategy, widefield fundus imaging with Clarus 500 (Carl Zeiss, Dublin, CA, USA), and 3D macular volume scan by optical coherence tomography using Topcon 3D OCT 2000 (Topcon Corporation, Tokyo, Japan).
An optometrist conducted a low-vision examination including measurement of refraction, visual acuity at distance and near, and contrast sensitivity at distance and near. Structured randomization was used to introduce the head-mounted displays in random order and demonstrate their functions. Monocular and binocular distance visual acuity was measured using the ETDRS 4-meter chart (Precision Vision Inc.) with the best subjective optical correction. If the participant could not read more than 19 letters, the chart was moved to 1 m, and a +0.75 spheric correction was added. Additionally, binocular visual acuity was measured using head-mounted displays at a 4-meter distance. Binocular contrast sensitivity with the best subjective correction was measured at 1 m using the Pelli-Robson Contrast Sensitivity Chart (Precision Vision Inc.) under a Luminos daylight lamp model D35600 with 265–380 lux (Daylight Company). Contrast sensitivity was also measured wearing the head-mounted display adjusted to the best subjective contrast and lighting conditions. Near visual acuity for high and low contrast was tested using the Colenbrander Mixed Contrast chart (Precision Vision Inc.), along with the optical correction, lighting, and distance preferred by the participants. When testing visual acuity at near with low contrast using head-mounted displays, the Colenbrander Mixed Contrast chart was placed on an inclined plane.
Phase 2
In the second phase, subjective outcomes were measured, and the participants tested the four head-mounted displays in the clinic and rated viewing at a distance indoors and outdoors, looking near and at a computer, spatial perception, comfort, how easy the head-mounted display was to use, and gave a total score. The assessments, comments, and observations from the instructors were documented, and the participants selected their favorite head-mounted displays in order of priority.
Phase 3
During the third phase, the Canadian Occupational Performance Measure (COPM)9 was used as an interview tool at IBOS to assess participants’ self-evaluation of their ability to perform various activities. The activities selected by the participants could be related to personal care, transportation, housework, education, work life, leisure, or social arrangements. Participants had to choose five activities and score them based on importance, performance, and satisfaction on a scale from 1 (worst) to 10 (best) using their current aids.
Phase 4
In the fourth phase, the first head-mounted display was customized to fit each participant, and they received instructions on the basic functions as well as a brief written guide. To become accustomed to the head-mounted display, the participants had to perform various activities while operating the device: read an expiration date on a product, sort coins into currency units, determine a facial expression, or focus on objects in motion through a window.
Phase 5
During the fifth phase, the participants used two head-mounted displays at home in their everyday lives for two weeks per head-mounted display. They did not have two head-mounted displays at home simultaneously. The head-mounted displays were distributed such that all participants received at least one of the two head-mounted displays that they preferred. They also received a list of the five chosen activities from the COPM to focus on. The IBOS personnel made a service call three days after lending the head-mounted displays to address any technical challenges.
Phase 6
In the sixth phase, the participants returned to IBOS for re-evaluation of the COPM and to provide feedback on the performance and satisfaction of the head-mounted display. The re-evaluation was supplemented with 10 additional questions about the experience of using the head-mounted display. The re-evaluation, feedback, and questions were repeated after trying out the second type of head-mounted display at home.
Phase 7
Finally, in the seventh phase, participants were interviewed using follow-up questions regarding their preferred head-mounted display.
Statistics
All statistical analyses were performed using the statistical software R.10 Descriptive data were summarized in medians, interquartile ranges, and percentages. The distribution of data was assessed using Q-Q plots, and variance was tested using the Fligner-Killeen test. Comparison of medians of non-normally distributed data was performed using the non-parametric Mann–Whitney U-test and adjusting the p-values with the Benjamini-Hochberg procedure with a false discovery rate of 0.05.
Results
Twelve participants (six females) aged 16–53 years (median 30.5 years) completed the first two phases of the project. None of the participants had previous experience with head-mounted displays. Nine participants were employed, two were students, and one was unemployed. Six participants terminated their participation before testing the head-mounted display at home; two participants felt that wearing the head-mounted display did not harmonize with their self-concept, two described a lack of time or energy, one experienced dizziness and discomfort, and one had double vision and limitation of the visual field when using the head-mounted display. Six participants (four females) between the ages of 16 and 51 years (median 41.5) completed all seven phases of the study. Five were employed and one was a student. The participants’ characteristics are shown in Table 1.
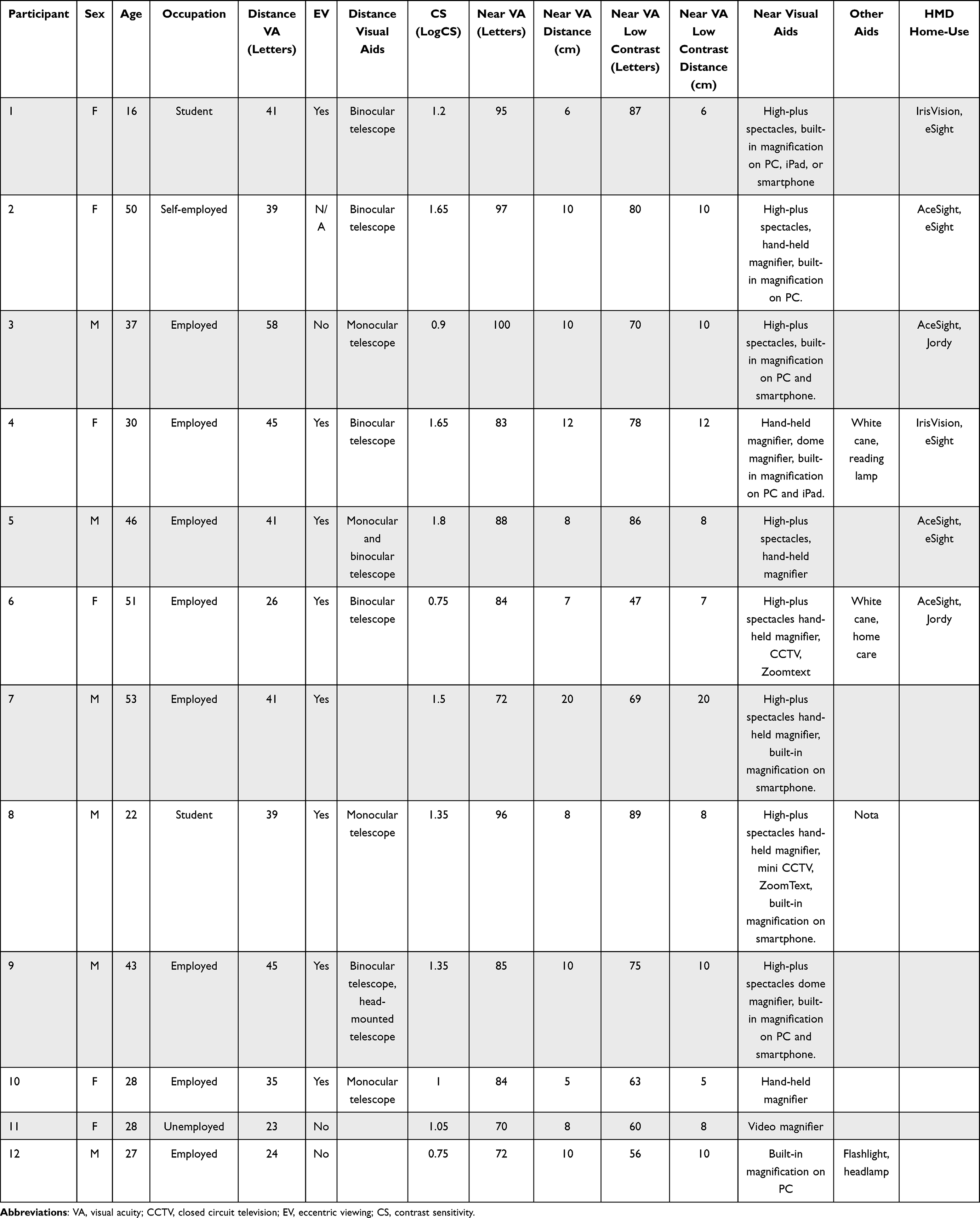 |
Table 1 Patient Characteristics at Baseline. Patients 1–6 Completed the Study, While Patients 7–12 Only Completed Phases 1 and 2 |
Phase 1 and 2
The 12 participants who tested the head-mounted displays in the first two phases had an objective improvement in distance visual acuity with all head-mounted displays. Near visual acuity with high contrast improved with eSight and IrisVision, and all head-mounted displays significantly increased reading distance. Near visual acuity with low contrast was unchanged, but the distance to the chart increased for all head-mounted displays. Distance contrast sensitivity only improved with eSight (Table 2 and Table 3). When the participants assessed the devices, there was a high variability in which device they preferred for which task (Figure 2). Notably, Jordy stood out for being the most user-friendly option, although it was not perceived as helpful during computer work.
 |
Table 2 Clinical Results from Measures with and without the Head-Mounted Displays. Overview with the Initial 12 Participants and the Final Six Participants. Phase 1 |
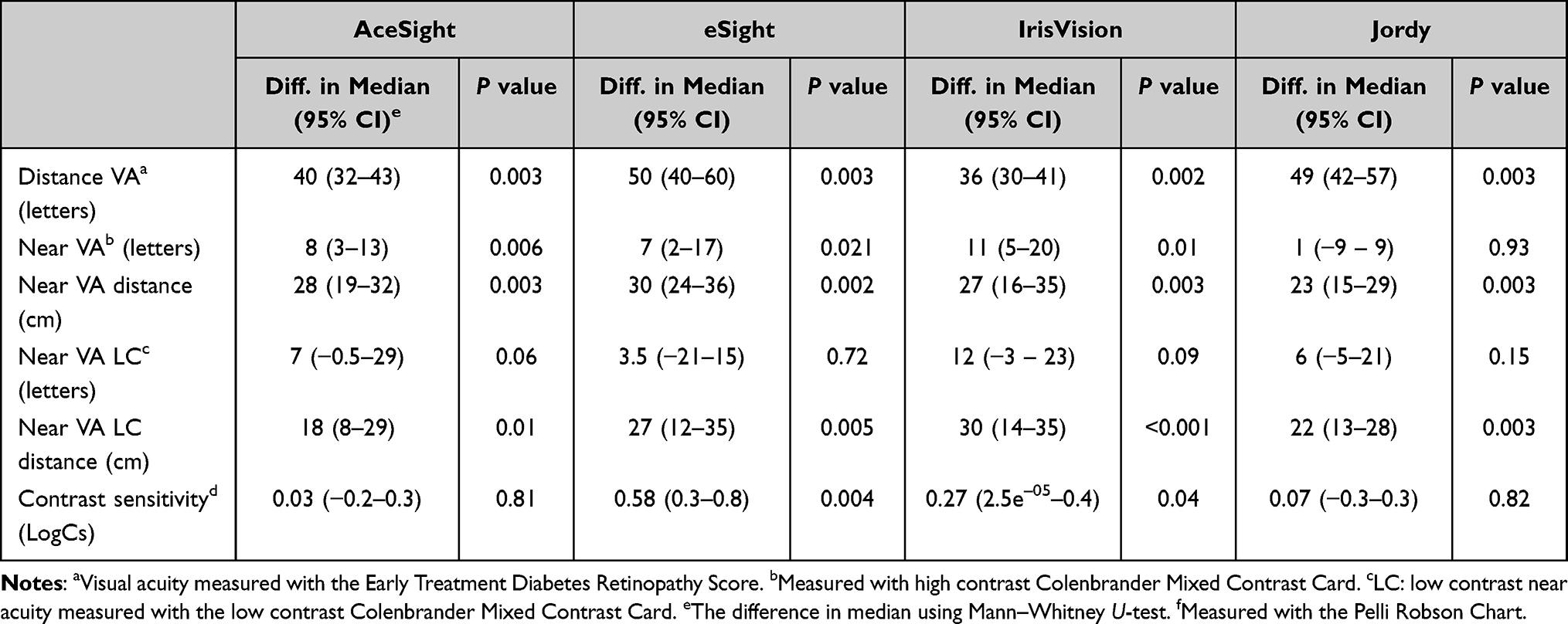 |
Table 3 Comparison of Four Head-Mounted Displays with Baseline Values Using the Mann–Whitney U-Test and Correcting for Multiple Testing. Phase 1 with 12 Participants |
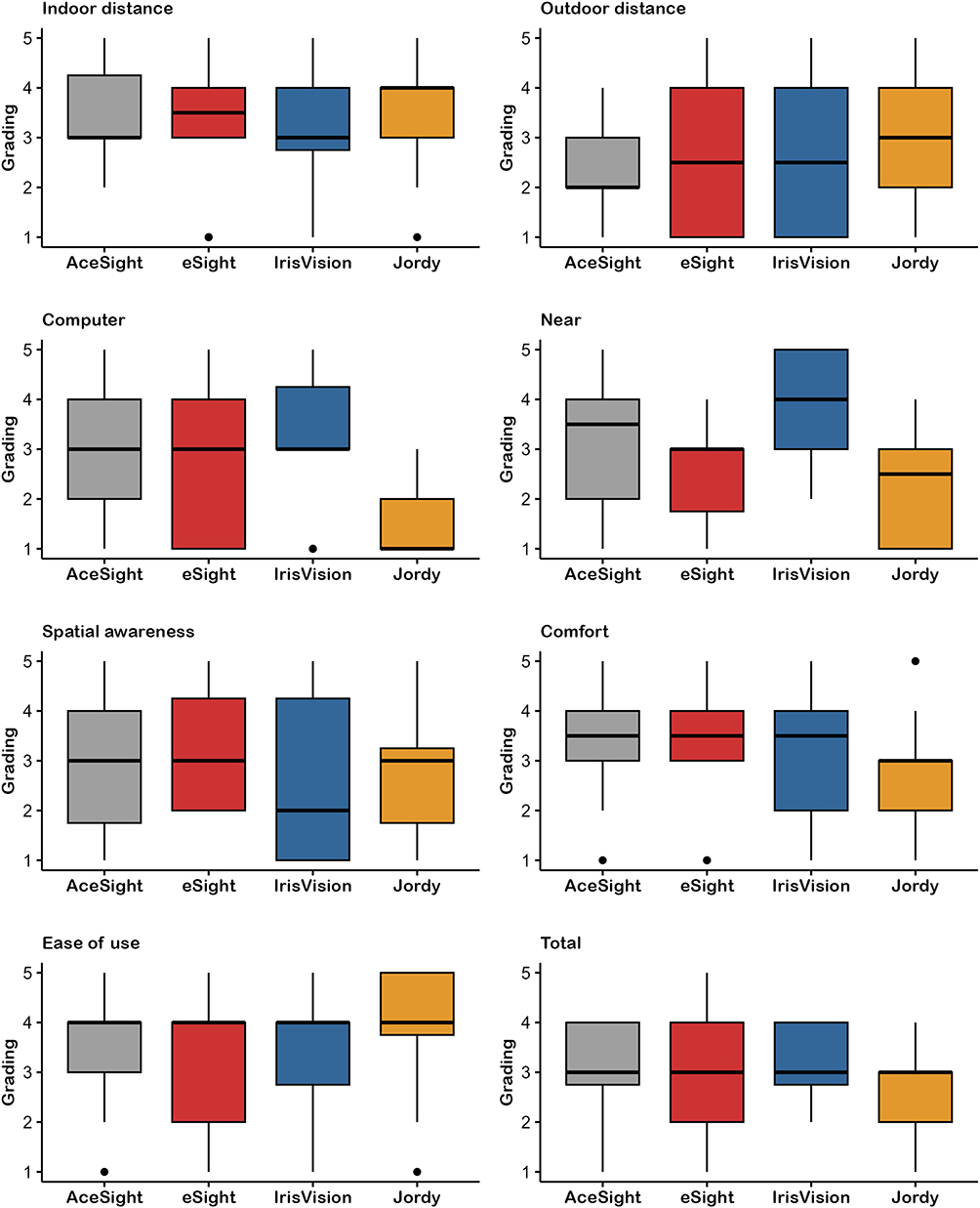 |
Figure 2 Boxplots illustrating the initial subjective evaluation of all four head-mounted displays. Notes: Twelve participants evaluated the devices from 1 to 5, where 5 was the highest score. The functions of the head-mounted displays were tried out in the clinic before home use; AceSight, eSight, Irisvision, and Jordy. Phase 2. |
Phase 3 to 6
Six participants tried two head-mounted displays at home and at work for two weeks each. The results from the COPM interviews showed that AceSight, eSight, and IrisVision improved visual function at a distance, whereas only AceSight improved vision during near tasks (Figure 3, Supplementary Table A2). IrisVision and eSight improved reading, and none of the devices improved vision during computer-related tasks. Reading at a distance was graded higher with AceSight and eSight. Satisfaction with the performance of the preferred tasks was below the baseline in all tasks when using Jordy. Computer-related tasks were rated with lower satisfaction when wearing the devices than when not, except when using IrisVision (Figure 3, Supplementary Table A2).
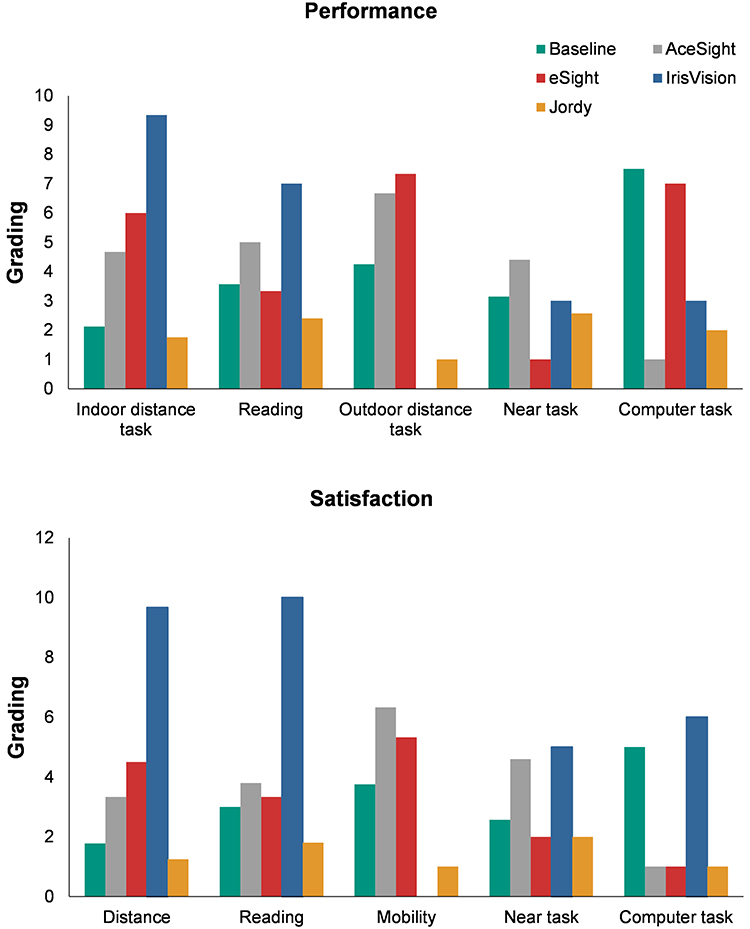 |
Figure 3 Results from the COPM interviews phase 3–6. Notes: Assessment of the performance and satisfaction of tasks wearing the head-mounted displays. Six participants evaluated the devices on a scale from 1 to 10, where 10 was the highest score. The baseline illustrates evaluations without wearing head-mounted displays. Outdoor distance tasks were not assessed for IrisVision. |
Phase 7
In the final evaluation of the head-mounted displays, two participants preferred IrisVision, and two preferred eSight, while AceSight and Jordy were preferred by one participant each. The reason for choosing a particular head-mounted display was that, in most cases, the head-mounted display was described as the most comfortable to wear. To the question: “How much have you used the head-mounted display at home”, five out of six answered “seldom”, and one answered, “most of the time”. Two participants had used the head-mounted display “seldom” at work, while four had not used it at work. When asked if “the appearance of the head-mounted display has kept me from using it in public space”, four out of six answered “completely true”, one answered, “mostly true”, and one answered, “completely wrong”. Half of the participants answered that they would use the head-mounted display if it were granted for private use. Only one participant would use the head-mounted display at work, one was uncertain, and three participants would not use the head-mounted display at work. They reported that head-mounted displays helped them the most when they were looking at a distance or when they had to find their way on a map or read. When asked whether the head-mounted display could replace the current visual aids, three participants agreed, two disagreed, and one was uncertain. Four participants answered that the head-mounted display had lived up to the expectations that they had before the study.
Discussion
In this exploratory study, objective measures showed that all head-mounted displays in the clinical setting significantly improved visual acuity at a distance and that eSight and IrisVision improved high contrast visual acuity at near. All head-mounted displays increased reading distance when reading high and low-contrast letters. Contrast vision at a distance was improved by eSight, and near visual acuity with low contrast was improved by IrisVision. The improvement in distance visual acuity4,11,12 and near visual acuity4 is comparable with previous studies that examined eSight, IrisVision, and Jordy. A study examining eSight found an improvement in contrast vision4 while another study did not find an improvement in contrast vision nor near visual acuity using Jordy.12
Subjective measures showed that participants reported an improvement in distance vision with all head-mounted displays while near vision and reading were improved by IrisVision, AceSight, and eSight after home use. Previous studies testing eSight and IrisVision found subjective improvement in the ability to complete functional tasks and the quality of life.4,13,14 In one study participants reported subjective improvement in visual acuity while in another study participants reported difficulties with functional visual tasks using Jordy.5,11
Most participants in this study did not utilize head-mounted displays at work and expressed hesitation about wearing the devices in public because of their appearance. In a study that tested IrisVision, 26% of participants reported that they might use the device in public, and 30% wished that the device was smaller and lighter.5 A study testing Sightplus, a device with a similar appearance to IrisVision, found that 23% criticized aesthetics and 50% did not want to use the head-mounted display in public.6 Another study found that 8% of participants who already owned an eSight discontinued the use of the device due to embarrassment.4 These findings illustrate the significance of device aesthetics and the social stigma of wearing a head-mounted display, highlighting the need for discreet head-mounted display designs.
In our study, two participants dropped out due to dizziness, discomfort, and double vision when testing the devices at the clinic, but the six participants who took the head-mounted displays home did not report any negative effects. We found an ergonomic benefit of the head-mounted displays as the reading distance at near increased.
Factors influencing the discontinuation of device usage include head-mounted weight, appearance of the device, user discomfort,5,6,13 and handling challenges.5 Among users of eSight the quality of life utilizing the device (PIADS), and the satisfaction with the service received during fitting and follow-up (QUEST), as well as the absence of headaches, were related to continued use.7 Younger age, a longer duration of visual impairment, existing use of electronic devices, and lower baseline contrast sensitivity have also been associated with continued use.6
Previous studies have found a risk of headaches, nausea, tired eyes, and double vision when using HMD and one study found that 13% stopped using the device due to discomfort and 21% due to the weight of the display.4–7 Future smaller and lighter devices could reduce the strain on the neck and reduce headaches and neck pain.
The small number of participants and high dropout rate are limitations of this exploratory study, and future studies with more participants are needed. A strength of the study is the mixed-method design where both qualitative and quantitative information was collected. An additional constraint of the study design is that the participants were required to answer questions directly to the interviewer and might have withheld their true opinions. This could explain why half of the patients expressed that the head-mounted displays could replace their current visual aids and that they would like to have a head-mounted display if granted but only used it sparingly at home. Thus, we found that the clinical results and evaluations did not represent the actual use at home.
Head-mounted displays offer a diverse array of features that have the potential to significantly contribute to the rehabilitation of individuals with visual impairment. However, due to differing user expectations and needs, the preferred device is dependent on the individual. Therefore, it is advisable to consider a home try-out. The development of smaller and lighter devices that focus on aesthetics can result in increased usage.
Conclusion
We found an improvement in distance visual acuity and increasing reading distance for all tested head-mounted displays. Additionally, eSight and IrisVision improved visual function at near and eSight also improved contrast vision at distance. Despite the possibility of improving vision, social stigma and device aesthetics kept the participants from using head-mounted displays in public and limited their use at home.
Acknowledgments
The Danish Eye Research Foundation supported this study. The sponsor had no involvement in any stages of the research.
Disclosure
The authors report no conflicts of interest.
References
1. World Health Organization. World Report on Vision. Vol. 214. World Health Organization; 2019.
2. Renieri G, Pitz S, Pfeiffer N, Beutel ME, Zwerenz R. Changes in quality of life in visually impaired patients after low-vision rehabilitation. Int J Rehabil Res. 2013;36(1):48–55. doi:10.1097/MRR.0B013E328357885B
3. Das K, Gopalakrishnan S, Dalan D, Velu S, Ratra V, Ratra D. Factors influencing the choice of low-vision devices for visual rehabilitation in Stargardt disease. Clin Exp Optom. 2019;102(4):426–433. doi:10.1111/CXO.12867
4. Wittich W, Lorenzini MC, Markowitz SN, et al. The effect of a head-mounted low vision device on visual function. Optom Vis Sci. 2018;95(9):774. doi:10.1097/OPX.0000000000001262
5. Deemer AD, Swenor BK, Fujiwara K, et al. Preliminary evaluation of two digital image processing strategies for head-mounted magnification for low vision patients. Transl Vis Sci Technol. 2019;8(1):23. doi:10.1167/TVST.8.1.23
6. Crossland MD, Starke SD, Imielski P, Wolffsohn JS, Webster AR. Benefit of an electronic head-mounted low vision aid. Ophthalmic Physiol Opt. 2019;39(6):422–431. doi:10.1111/OPO.12646
7. Lorenzini MC, Hämäläinen AM, Wittich W. Factors related to the use of a head-mounted display for individuals with low vision. Disabil Rehabil. 2021;43(17):2472–2486. doi:10.1080/09638288.2019.1704892
8. Kohli P, Kaur K. Stargardt disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
9. Law M, Baptiste S, Mccoll M, Opzoomer A, Polatajko H, Pollock N. The Canadian Occupational Performance Measure: an outcome measure for occupational therapy. Can J Occup Ther. 1990;57(2):82–87. doi:10.1177/000841749005700207
10. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2020. Available from: https://www.r-project.org/.
11. Troyer EJ, Dixon M. Comparison of head borne electronic low vision devices in patients with visual impairment. Invest Ophthalmol Vis Sci. 2018;59(9):634.
12. Culham LE, Chabra A, Rubin GS. Clinical performance of electronic, head-mounted, low-vision devices. Ophthalmic Physiol Opt. 2004;24(4):281–290. doi:10.1111/J.1475-1313.2004.00193.X
13. Lorenzini MC, Wittich W. Head-mounted visual assistive technology-related quality of life changes after telerehabilitation. Optom Vis Sci. 2021;98(6):582–591. doi:10.1097/OPX.0000000000001705
14. Werblin F. Measuring the effectiveness of a portable low vision aid in restoring visual life to low vision users. Invest Ophthalmol Vis Sci. 2020;61(7):933.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.