")
Back to Journals » Journal of Pain Research » Volume 17
Acupuncture in Multiple Myeloma Peripheral Neuropathy: A Systematic Review
Authors Lyu C , Xiao H, Yin X, Li Z, Han C, Xu R
Received 16 November 2023
Accepted for publication 4 April 2024
Published 24 April 2024 Volume 2024:17 Pages 1571—1581
DOI https://doi.org/10.2147/JPR.S448634
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Chunyi Lyu,1 Hongyan Xiao,1 Xuewei Yin,2 Zonghong Li,1 Chen Han,1 Ruirong Xu3,4
1First Clinical Medical College, Shandong University of Traditional Chinese Medicine, Jinan, 250014, People’s Republic of China; 2Affiliated Eye Hospital of Shandong University of Traditional Chinese Medicine, Jinan, 250002, People’s Republic of China; 3Key Laboratory of Integrated Traditional Chinese and Western Medicine for Hematology, Health Commission of Shandong Province; Institute of Hematology, Shandong University of Traditional Chinese Medicine, Jinan, 250014, People’s Republic of China; 4Department of Hematology, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, 250014, People’s Republic of China
Correspondence: Ruirong Xu, Email [email protected]
Background: Peripheral neuropathy (PN) is a prevalent complication of multiple myeloma (MM), due to the disease itself or its treatment. Despite extensive research, the optimal treatment for multiple myeloma peripheral neuropathy (MMPN) remains unclear. Clinical practice has shown the potential efficacy of acupuncture in managing MMPN. This study aimed to conduct a comprehensive analysis of the literature to assess the effectiveness and safety of acupuncture as a treatment for MMPN.
Methods: The PubMed, Web of Science, MEDLINE, Cochrane Library, and Embase databases were comprehensively searched from inception to November 1, 2023 to identify relevant studies pertaining to the use of acupuncture to treat MMPN.
Results: A total of five studies, encompassing 97 patients diagnosed with drug-related PN, were ultimately included in this analysis. The literature lacks any reports pertaining to the utilization of acupuncture for disease-related PN. ST36, LI4, SP6, and EX-LE-10 were found to be the most frequently chosen acupoints. Following acupuncture treatment, there was a consistent reduction in scores on the Visual Analogue Scale (VAS), Neuropathic Pain Scale (NPS), Brief Pain Inventory-Short Form (BPI-SF), and Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (FACT/GOG-Ntx) among MMPN patients. The results of Nerve Conduction Velocity (NCV) tests yielded conflicting results. No severe adverse effects were reported.
Conclusion: The use of acupuncture for disease-related PN has not been studied to date. Acupuncture is safe for drug-related PN and is helpful for relieving pain. But uncertainty exists regarding the efficacy of this approach because there is substantial heterogeneity with respect to acupuncture treatment regimens, and more high-quality studies on this topic are warranted.
Keywords: multiple myeloma peripheral neuropathy, acupuncture, pain, systematic review
Introduction
Multiple myeloma (MM) is a neoplastic disorder characterized by the proliferation of plasma cells within the bone marrow.1 Peripheral neuropathy (PN) is a common complication of MM that mainly manifests as sensory neuropathies and motor neuropathies in severe cases.2 Multiple myeloma peripheral neuropathy (MMPN) can be divided into disease-related PN and drug-related PN. In disease-related PN, sensory modalities may be affected, resulting in axonal sensorimotor neuropathy with a length-dependent pattern of axonal regrowth.3 Drug-related PN is mainly caused by first-line drugs such as the proteasome inhibitor bortezomib and the immunomodulator thalidomide, which is one of the major challenges in the current drug management of MM.4 Clinical evaluations suggest that up to 20% of patients with MM develop PN at diagnosis, and up to 75% of patients may develop therapeutic PN during treatment.5 Among drug-related PNs, the incidence of bortezomib-induced peripheral neuropathy (BIPN) can reach 40%, and the incidence of thalidomide-induced peripheral neuropathy (TIPN) varies greatly, ranging from 25% to 75%.6
MMPN has a significant impact on patients’ physical and mental health and quality of life. The occurrence and severity of drug-related PN are strongly related to the drug dose.7 Severe drug-related PN can only control the development of neurotoxicity by adjusting the dose, changing the route of administration, interrupting drugs or prolonging the interval between chemotherapy, which also reduces the therapeutic effect of the primary disease. Available treatment options for the prevention and treatment of MMPN are limited. Generally, vitamin B drugs are administered to nourish nerves, and painkillers are used to relieve pain, but the effect is not satisfactory. Therefore, an effective treatment method is urgently needed to control the occurrence and development of MMPN. A large amount of medical evidence indicates that acupuncture plays a potential role in relieving cancer pain, and the analgesic effect of acupuncture is one of its most widely accepted effects.8 Additionally, available studies have suggested that acupuncture is effective in the treatment of diabetic PN and paclitaxel- and oxaliplatin- induced PN,9,10 suggesting that acupuncture is a useful alternative to relieve symptoms of PN. Previous investigations have shown the synergistic impact of acupuncture and bortezomib on prolonging the survival of mice with MM.11 Acupuncture has been regarded to have strong potential as an adjunctive therapy for treating MMPN.12 Several studies have explored the potential clinical implications of using acupuncture to treat MMPN, but no systematic review has examined this topic. The objective of this study was to perform a comprehensive analysis of clinical studies evaluating the efficacy and safety of acupuncture in patients with MMPN and to offer a systematic perspective for clinical practice.
Materials and Methods
Registration and Protocol
This systematic review was conducted in accordance with the PRISMA 2020 checklist,13 (Supplementary Table 1), which has been registered on the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY202370046).
Search Sources and Data Extraction
This systematic review investigated the use of acupuncture as a therapeutic approach for the management of MMPN. The PubMed, Web of Science, MEDLINE, Embase, and Cochrane Library databases were searched using the following terms: (multiple myeloma OR MM) AND (peripheral neuropathy OR PN) AND acupuncture. The databases were searched from their respective inception to November 11, 2023. Only English studies with human participants were included. The inclusion criterion for this study was patients diagnosed with MMPN who had received acupuncture treatment. The exclusion criteria were as follows: animal studies, incomplete or inaccessible data, and data obtained from nonprimary sources. In cases where multiple publications were available for the same study, preference was given to the article containing the most comprehensive information. The personal information includes both general and disease-related information. The outcome indicators included the result of the Visual Analogue Scale (VAS), the Neuropathic Pain Scale (NPS), the Brief Pain Inventory-Short Form (BPI-SF), the Nerve Conduction Velocity (NCV), the Functional Assessment of Cancer Therapy - General (FACT-G), the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (FACT/GOG-Ntx), proinflammatory and neurotrophic biomarkers, and adverse reaction. Two investigators (C.L. and H.X.) independently retrieved the literatures and extracted the data.
Quality Assessment
The quality assessment of the case reports, single-arm clinical trials, and randomized controlled trials was conducted utilizing the JBI critical appraisal tool for case report14 the MINORS tool15 and the modified Jadad scale,16 respectively. The literature quality assessment was independently completed by two researchers (C.L. and C.H.) by referring to the relevant literature.
Data Analysis
Due to the heterogeneity of the data, it was unfeasible to amalgamate them for the purpose of conducting a meta-analysis. Descriptive approaches were employed to analyze the aggregated data. To explore the regularity of acupoint combinations, frequency analysis and association rule analysis were conducted using SPSS Statistics (version 26.0) and SPSS Modeler (version 15.0), respectively. The Apriori algorithm for association rule mining was adopted to analyze the confidence and support of acupoint combinations. The minimum acceptable confidence and support values were considered for the purpose of pruning the rules. Specifically, a minimum confidence of 100% and a minimum support of 20% were considered. The higher the confidence degree and support values are, the greater the degree of credibility. The acupoint combination network was visualized using Cytoscape (version 3.9.1).
 |
Table 1 The Basic Characteristics of the Included Studies |
Results
Search results and Study Characteristics
A total of 64 studies were initially screened from 5 databases, and 34 studies remained after removing duplicates. The literature was then screened by first reading the title and abstract, and 20 irrelevant studies were excluded. The full texts of the remaining literatures were then searched, and a total of 7 studies went into full-text assessment, of which 1 was excluded because of a lack of complete data,22 and 1 were excluded because they contained duplicate data.23 The literature screening process is shown in Figure 1. Ultimately, five studies with a total of 97 patients were included17-21 (Table 1). There were two single-arm clinical trials,18,19 one randomized controlled trial,17 and two case reports.20,21 In three studies, patients received acupuncture after the discontinuation of bortezomib,17–19 and in one case report, patients received bortezomib during acupuncture treatment.20 All patients in the included studies were diagnosed with drug-related PN, and none of the studies reported the use of acupuncture for disease-related PN. Among the five studies, three studies included 95 patients who were diagnosed with drug-related PN of grade ≥ ;17–19 two of these studies used the CTCAE diagnostic criteria (version 3.0),17,18 and one study used the NCI-CTC diagnostic criteria (version 4.0).19 Two studies mentioned only that patients were in a state of BIPN according to neurological exams and electro neurophysiological tests.20,21 To evaluate the efficacy of acupuncture, the VAS was used in two studies,17,21 the NPS was used in two studies,19,20 the BPI-SF was used in one study,18 the NCV test was used in three studies,17–19 the FACT-G was used in one study,18 the FACT/GOG-Ntx was used in three studies,17–19 and proinflammatory and neurotrophic biomarkers were assessed in one study.19 Four studies reported whether there were adverse reactions.17,19–21
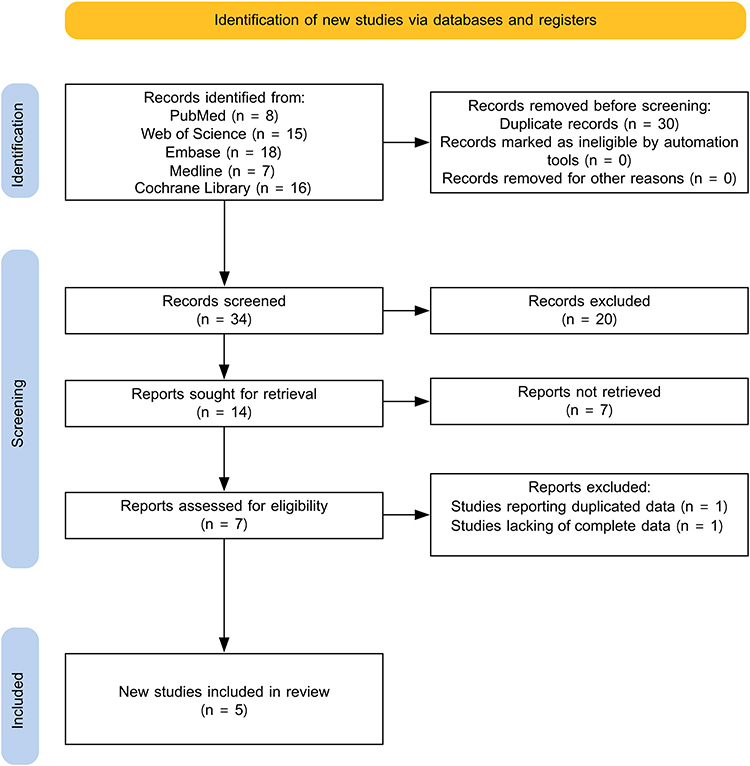 |
Figure 1 Flow chart of literature screening. |
 |
Figure 2 The distribution pattern of selected acupoint. (a) Types of selected acupuncture. (b) Frequency of selected acupoints. (c) The combination rules of selected acupoints. |
Two case reports20,21 were evaluated as having high methodological quality in accordance with the JBI critical appraisal tool for case report (Supplementary Table 2). The MINORS tool was used to assess the quality of two single-arm clinical trials;18,19 these trials were found to be of medium quality (Supplementary Table 3). The quality of randomized controlled trials17 was evaluated using the modified Jadad scale these trials were found to be of low-quality (Supplementary Table 4).
Summary of Intervention
The details of the acupuncture treatment methods used are summarized in Table 2. In two single-arm clinical trials18,19 and two case reports,20,21 patients received synergistic symptomatic treatment involving acupuncture. In a randomized controlled trial,17 patients in the treatment group received acupuncture combined with methylcobalamin, and patients in the control group received only methylcobalamin. Four studies used body acupuncture,17,18,20,21 and only one study used a combination of auricular acupuncture plus body acupuncture19 (Figure 2a). Among the studies that used body acupuncture, one used electroacupuncture,18 and the other used manual acupuncture.
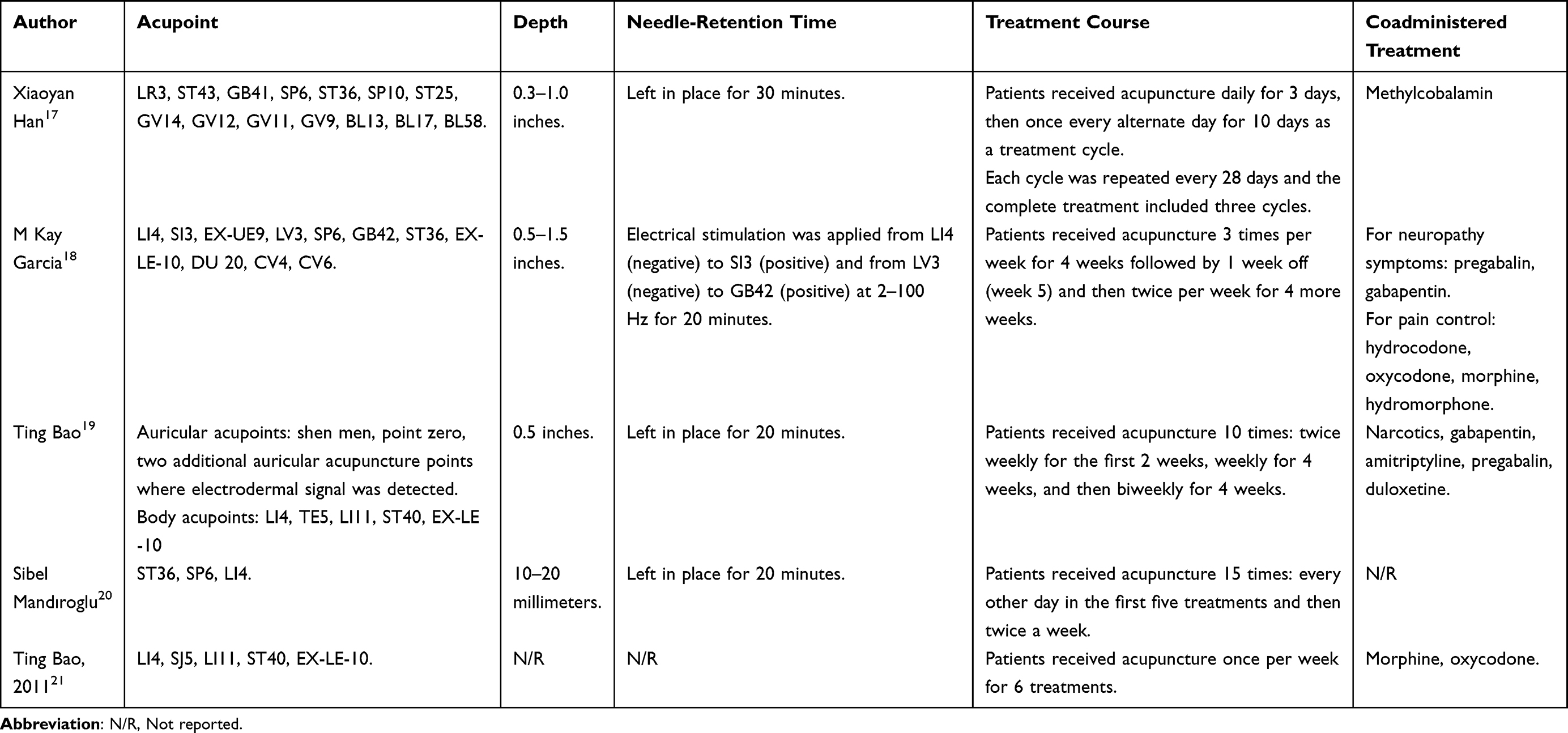 |
Table 2 The Details of the Intervention Protocol |
The acupoints utilized in auricular acupuncture included shen men, point zero, and two supplementary acupoints where the electrodermal signal was observed.19 ST36, LI4, SP6 and EX-LE-10 were the most-frequently used acupoints for body acupuncture (Figure 2b). According to the results of association rule mining, the SP6-ST36 combination (support value: 60%, confidence value: 100%), LI4- EX-LE-10 combination (support value: 40%, confidence value: 100%), and SP6-ST36-LI4 combination (support value: 40%, confidence value: 100%) were the core acupoint combinations (Figure 2c and Supplementary Table 5).
In studies using body acupuncture, the needle was positioned after de qi. Needle retention for 30 minutes was reported in one study,17 and that for 20 minutes was reported in three studies.18–20 Four studies reported the depth of needling: 0.3–1.0 inches,17 0.5–1.5 inches,18 0.5 inches,19 and 10–20 mm.20
Efficacy and Safety Assessment
The safety and efficacy of acupuncture for improving pain, neurological function, quality of life, and biomarkers levels in patients with MMPN are summarized in Table 3.
 |
Table 3 Summary of the Efficacy and Safety Assessments |
Improvements in Pain
Pain improvement was assessed using the VAS, NPS, and BPI-SF. The VAS is a commonly used measure for evaluating variations in pain intensity in the area of cancer pain assessment.24 The NPS is a multifaceted instrument that employs a self-reported visual analogue to delineate levels of pain intensity and its corresponding attributes.25 The BPI-SF is a self-administered survey utilized to evaluate the magnitude of pain and its influence on patients’ daily activities.26 Higher NPS, VAS and BPI-SF scores indicate worse pain symptoms.
Two studies reported VAS scores. Ting Bao reported that the VAS score of patients decreased from 8/10 to 2/10 after acupuncture treatment.21 Xiaoyan Han reported that the VAS score significantly decreased in the acupuncture combined with methylcobalamin group compared to that in methylcobalamin group.17 Two studies reported the results of the NPS. In a case reported by Sibel Mandıroglu, the NPS decreased from 4/10 to 0/10 after acupuncture treatment.20 Similarly, Ting Bao reported a decrease in the NPS after acupuncture treatment.19 According to a single-arm clinical trial conducted by M Kay Garcia, the BPI-SF indicated notable improvements in pain severity at all measured time points.18
Neurological Function
Neurological function was measured using the NCV test, which included assessments of motor nerve conduction velocity (MCV) and sensory nerve conduction velocity (SCV). These tests were performed using an electromyography machine.
Three studies reported the result of NCV tests. Only one study reported the MCV and SCV (except for the median nerve SCV) were improved in the acupuncture combined with methylcobalamin group compared with the methylcobalamin group.17 M Kay Garcia reported that no significant changes were detected in NCV tests,18 and Ting Bao reported that NCV test results did not change between baseline and the end of the study.19
Quality of Life
The assessment of the quality of life of MMPN patients was conducted utilizing the FACT/GOG-Ntx and FACT-G. The FACT/GOG-Ntx subscale, comprises an 11-item neurotoxicity module that supplements the primary quality of life measurement of the FACT-G questionnaire,27 commonly employed to evaluate chemotherapy-induced peripheral neuropathy (CIPN) in individuals with cancer.28
The FACT/GOG-Ntx score was reported in three studies. Xiaoyan Han reported that the FACT/GOG-Ntx score decreased significantly in the acupuncture combined with methylcobalamin group compared to the methylcobalamin group.17 M Kay Garcia demonstrated that the FACT/GOG-Ntx score decreased significantly between baseline and all subsequent time points.18 Ting Bao reported that the average FACT/GOG-Ntx score decreased and remained at a low level at the endpoint of treatment, and a decrease in the FACT/GOG-Ntx score was noted for ambulation, manual dexterity, and auditory capabilities, and there was no decrease in overall functionality (joint pain or muscular cramps and weakness).19
In a study conducted by M Kay Garcia, the FACT-G score was measured.18 The findings indicated that acupuncture had a noteworthy temporal effect on the physical well-being scale score, with a notable decrease at the treatment period and during the follow-up. However, no notable improvements were observed in the domains of social/family well-being, emotional well-being, or functional well-being.
The Expression Levels of Biomarkers
One study19 reported changes in biomarkers after acupuncture. The biomarkers included eight proinflammatory cytokines, interleukin-6 (IL-6), IL-8, IL-10, IL-17a, macrophage inflammatory protein-1α (MIP-1α), tumor necrosis factor-α (TNF-α), vascular endothelial growth factor (VEGF), and insulin-like growth factor-1 (IGF-1), and four neurotrophic factors: nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3), and β-endorphin (β-EP). There were no statistically significant alterations in any of the 12 biomarkers.
Safety Assessment
Four studies reported adverse effects, and no adverse events occurred.17,19–21
Discussion
Proteasome inhibitors and the immunostimulatory greatly improve progression-free and overall survival for MM patients, but TIPN and BIPN have a significant impact on the quality of life of patients, often necessitating the reduction, postponement, or premature discontinuation of effective treatment, which is widely recognized as a major challenge in the management of drug side effects in MM.29 The American College of Chest Physicians (ACCP) evidence-based clinical practice guide points out that acupuncture as a complementary therapy and adjuvant therapy can effectively control cancer pain and PN.30 In clinical practice, acupuncture is often used for the empiric treatment of MMPN. The aim of the present study was to systematically evaluate the efficacy and safety of acupuncture in the treatment of MMPN by reviewing the literature. Three studies reported 95 patients who were diagnosed with grade ≥2 PN,17–19 and two patients were only diagnosed with BIPN in two case reports.20,21 Patients in three studies received acupuncture treatment after the discontinuation of bortezomib,17–19 and in one case report, they received acupuncture treatment during bortezomib treatment,20 which precluded the reversibility of the effect of acupuncture after the discontinuation of BIPN.
Body acupuncture is the most commonly used technique and was reported in all five included studies. Among the studies that used body acupuncture, one used electroacupuncture.18 Needle retention for 30 minutes was reported in one study,17 and 20 minutes was reported in three studies.18–20 Based on the findings of three studies employing body acupuncture, the placement of needles subsequent to the attainment of de qi, characterized by sensations of numbness, tingling, or warmth at the site of needle insertion, is pivotal for the efficacy of acupuncture. Furthermore, de qi is reported to serve as the fundamental mechanism underlying the sustained analgesic outcomes associated with acupuncture.31 ST36, LI4, SP6 and EX-LE-10 were the most frequently used, and the SP6-ST36 combination, LI4-EX-LE-10 combination, and SP6-ST36-LI4 combination were the core acupoint combinations for MMPN patients. In previous studies, ST36 and SP6 were the most widely used acupoints for diabetic neuropathy,32 and LI4 acupressure was effective at decreasing pain and duration of labour.33 Acupuncture at ST36 has shown clinical benefits in relieving inflammation through mechanisms such as vagus nerve activation, macrophage polarization, and regulation of the MAPK signaling pathway, TLR4/NF-κB signaling, and the cholinergic anti-inflammatory pathway.34 One study used auricular acupuncture in combination with body acupuncture. The auricular acupuncture acupoints used were shen men, point zero, and 2 additional auricular acupuncture points where the electrodermal signal was detected. According to evidence-based medicine, auricular therapy has been demonstrated to be both efficacious and safe in managing cancer-related pain.35 Furthermore, the combination of auricular therapy and drug therapy has shown superior effectiveness compared to the use of analgesic drugs alone in terms of both alleviating pain and minimizing adverse reactions.36 Auricular point acupressure has the potential to serve as a cost-effective and efficacious complementary modality for individuals seeking to self-manage chemotherapy-induced neuropathy.37
According to the results of the included studies, acupuncture provides appropriate pain relief. A consistent decrease in pain intensity was observed according to the result of VAS, NPS, and BPI-SF results, indicating a significant advantage of acupuncture for MMPN patients experiencing pain. The analgesic efficacy of acupuncture has been demonstrated in animal-based research, whereby the activation of nerves that innervate muscles induces the secretion of neurotransmitters, including endorphin and enkephalin, and these neurotransmitters play a crucial role in modulating the pathways of the spinal cord, midbrain, and hypothalamo-hypophyseal system.38 These alterations elicit the activation of descending pain pathways and exert a regulatory influence on the limbic system.39 Additionally, the impact of acupuncture on CIPN can be elucidated through the release of opioid peptides and the mitigation of proinflammatory cytokines, and the anti-inflammatory effect of acupuncture is reported to be a key mechanism.40 However, in a study by Tingbao,19 there were no significant changes in any of the proinflammatory cytokines or neurotrophic factors at any time point after acupuncture.
The NCV test evaluates the degree of neural function, and discordant results existed among the included studies. The NCV test results did not significantly change between the baseline assessment and the end of the study in two studies,18,19 and one study reported that the MCV and SCV results improved.17 The FACT/GOG-Ntx and FACT-G reflect changes in CIPN patients’ quality of life. Three studies reported that the FACT/GOG-Ntx score was decreased after acupuncture.17–19 According to results reported by Tingbo,19 enhancements in ambulation, manual dexterity, and auditory capabilities were observed. However, there was no observed improvement in joint pain, muscle cramps, or weakness. M Kay Garcia reported that the FACT-G score improved only on the physical well-being scale.18 These findings indicated that acupuncture has the potential to relieve pain, restore neurological function, and improve quality of life, but more studies with a larger number of patients are needed to confirm these findings.
Heterogeneity in acupuncture therapy protocols, limitations of study design, differences in settings, and varying proficiencies of the acupuncturists have had an impact on the outcome. Although acupuncture is a relatively safe and empirically used treatment modality, there is a lack of high-quality evidence for the effectiveness of acupuncture with advanced methodology, which limits its popularization in clinical applications. PN was observed as a common clinical manifestation associated with MM or as a complication resulting from oncological treatment. All current research focuses on the BIPN, and the efficacy and safety of acupuncture for treating disease-related PN should be assessed in future studies.
Conclusion
The above findings indicate that acupuncture has the potential to ameliorate pain and improve quality of life for MMPN patients, but there is a lack of consistent evidence on the efficacy of acupuncture in improving neural function. More randomized controlled trials are needed to validate the efficacy and safety of acupuncture in MMPN. Additionally, the extant studies involved only auricular or body acupuncture, and there is still in the homogeneity for the retention time, depth of the needle, and the treatment course. Effective cases and complete details of treatment should be encouraged to establish comprehensive acupuncture modalities and optimize standard treatment regimens for the treatment of MMPN.
Data Sharing Statement
The detailed information is available from the corresponding author on reasonable request.
Funding
This study was supported by the Natural Science Foundation of Shandong Province (grant number: ZR2020KH023).
Disclosure
The authors have no conflict of interest to disclose.
References
1. Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and Management of Multiple Myeloma: a Review. JAMA. 2022;327(5):464–477. doi:10.1001/jama.2022.0003
2. Dong M, Zhang J, Han X, He J, Zheng G, Cai Z. Baseline peripheral neuropathy was associated with age and a prognostic factor in newly diagnosed multiple myeloma patients. Sci Rep. 2022;12(1):10061. doi:10.1038/s41598-022-13935-2
3. Vallat JM, Vital C. The spectrum of peripheral neuropathy in myeloma. Neurology. 1981;31(10):1372–1373. doi:10.1212/wnl.31.10.1372-a
4. Alkhawajah NM, Dunnigan SK, Bril V. Comparison of monoclonal gammopathy of undetermined significance-associated neuropathy and chronic inflammatory demyelinating polyneuropathy patients. J Neurol. 2014;261(8):1485–1491. doi:10.1007/s00415-014-7357-0
5. Richardson PG, Delforge M, Beksac M, et al. Management of treatment-emergent peripheral neuropathy in multiple myeloma. Leukemia. 2012;26(4):595–608. doi:10.1038/leu.2011.346
6. Morawska M, Grzasko N, Kostyra M, Wojciechowicz J, Hus M. Therapy-related peripheral neuropathy in multiple myeloma patients. Hematol Oncol. 2015;33(4):113–119. doi:10.1002/hon.2149
7. Petrucci MT, Giraldo P, Corradini P, et al. A prospective, international Phase 2 study of bortezomib retreatment in patients with relapsed multiple myeloma. Br J Haematol. 2013;160(5):649–659. doi:10.1111/bjh.12198
8. Chen WH, Hsieh CL, Huang CP, et al. Acid-sensing ion channel 3 mediates peripheral anti-hyperalgesia effects of acupuncture in mice inflammatory pain. J Biomed Sci. 2011;18(1):82. doi:10.1186/1423-0127-18-82
9. Tong Y, Guo H, Han B. Fifteen-day acupuncture treatment relieves diabetic peripheral neuropathy. J Acupunct Meridian Stud. 2010;3(2):95–103. doi:10.1016/S2005-2901(10)60018-0
10. Lu W, Giobbie-Hurder A, Freedman RA, et al. Acupuncture for Chemotherapy-Induced Peripheral Neuropathy in Breast Cancer Survivors: a Randomized Controlled Pilot Trial. Oncologist. 2020;25(4):310–318. doi:10.1634/theoncologist.2019-0489
11. Ke M, Qian J, Hao F, et al. Acupuncture Synergized with Bortezomib Improves Survival of Multiple Myeloma Mice via Decreasing Metabolic Ornithine. Front Oncol. 2021;11:779562. doi:10.3389/fonc.2021.779562
12. Zhou Y, Garcia MK, Chang DZ, et al. Multiple myeloma, painful neuropathy, acupuncture? Am J Clin Oncol. 2009;32(3):319–325. doi:10.1097/COC.0b013e318173a520
13. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
14. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: Systematic reviews of etiology and risk. Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis: JBI; 2020. doi:10.46658/jbimes-20-08
15. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–716. doi:10.1046/j.1445-2197.2003.02748.x
16. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12. doi:10.1016/0197-2456(95)00134-4
17. Han X, Wang L, Shi H, et al. Acupuncture combined with methylcobalamin for the treatment of chemotherapy-induced peripheral neuropathy in patients with multiple myeloma. BMC Cancer. 2017;17(1):40. doi:10.1186/s12885-016-3037-z
18. Garcia MK, Cohen L, Guo Y, et al. Electroacupuncture for thalidomide/bortezomib-induced peripheral neuropathy in multiple myeloma: a feasibility study. J Hematol Oncol. 2014;7:41. doi:10.1186/1756-8722-7-41
19. Bao T, Goloubeva O, Pelser C, et al. A pilot study of acupuncture in treating bortezomib-induced peripheral neuropathy in patients with multiple myeloma. Integr Cancer Ther. 2014;13(5):396–404. doi:10.1177/1534735414534729
20. Mandıroğlu S, Cevik C, Aylı M. Acupuncture for neuropathic pain due to bortezomib in a patient with multiple myeloma. Acupunct Med. 2014;32(2):194–196. doi:10.1136/acupmed-2013-010491
21. Bao T, Zhang R, Badros A, Lao L. Acupuncture treatment for bortezomib-induced peripheral neuropathy: a case report. Pain Res Treat. 2011;2011:920807. doi:10.1155/2011/920807
22. Bao T, Lao L, Medeiros M, Zhang R, Dorsey SG, Badros A. Improvement of Painful Bortezomib-Induced Peripheral Neuropathy Following Acupuncture Treatment in a Case Series of Multiple Myeloma Patients. Med Acupunct. 2012;24(3):181–187. doi:10.1089/acu.2011.0868
23. Zhi WI, Ingram E, Li SQ, Chen P, Piulson L, Bao T. Acupuncture for Bortezomib-Induced Peripheral Neuropathy: not Just for Pain. Integr Cancer Ther. 2018;17(4):1079–1086. doi:10.1177/1534735418788667
24. Jensen MP. The validity and reliability of pain measures in adults with cancer. J Pain. 2003;4(1):2–21. doi:10.1054/jpai.2003.1
25. Galer BS, Jensen MP. Development and preliminary validation of a pain measure specific to neuropathic pain: the Neuropathic Pain Scale. Neurology. 1997;48(2):332–338. doi:10.1212/wnl.48.2.332
26. Im DD, Jambaulikar GD, Kikut A, Gale J, Weiner SG. Brief Pain Inventory-Short Form: a New Method for Assessing Pain in the Emergency Department. Pain Med. 2020;21(12):3263–3269. doi:10.1093/pm/pnaa269
27. Calhoun EA, Welshman EE, Chang CH, et al. Psychometric evaluation of the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (Fact/GOG-Ntx) questionnaire for patients receiving systemic chemotherapy. Int J Gynecol Cancer. 2003;13(6):741–748. doi:10.1111/j.1525-1438.2003.13603.x
28. Cheng HL, Lopez V, Lam SC, et al. Psychometric testing of the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (FACT/GOG-Ntx) subscale in a longitudinal study of cancer patients treated with chemotherapy. Health Qual Life Outcomes. 2020;18(1):246. doi:10.1186/s12955-020-01493-y
29. Delforge M, Bladé J, Dimopoulos MA, et al. Treatment-related peripheral neuropathy in multiple myeloma: the challenge continues. Lancet Oncol. 2010;11(11):1086–1095. doi:10.1016/S1470-2045(10)70068-1
30. Mosher CE, Hanna N, Jalal SI, et al. Support service use and interest in support services among lung cancer patients. Lung Cancer. 2013;82(1):162–167. doi:10.1016/j.lungcan.2013.06.020
31. Wu N, Huang J, Yang X, et al. The long-term effect of acupuncture for patients with knee osteoarthritis: study protocol for a randomized controlled trial. Medicine (Baltimore). 2020;99(42):e22599. doi:10.1097/MD.0000000000022599
32. Cho E, Kim W. Effect of Acupuncture on Diabetic Neuropathy: a Narrative Review. Int J Mol Sci. 2021;22(16):8575. doi:10.3390/ijms22168575
33. Hamidzadeh A, Shahpourian F, Orak RJ, Montazeri AS, Khosravi A. Effects of LI4 acupressure on labor pain in the first stage of labor. J Midwifery Womens Health. 2012;57(2):133–138. doi:10.1111/j.1542-2011.2011.00138.x
34. Oh JE, Kim SN. Anti-Inflammatory Effects of Acupuncture at ST36 Point: a Literature Review in Animal Studies. Front Immunol. 2022;12:813748. doi:10.3389/fimmu.2021.813748
35. Mao JJ, Liou KT, Baser RE, et al. Effectiveness of Electroacupuncture or Auricular Acupuncture vs Usual Care for Chronic Musculoskeletal Pain Among Cancer Survivors: the PEACE Randomized Clinical Trial. JAMA Oncol. 2021;7(5):720–727. doi:10.1001/jamaoncol.2021.0310
36. Yang Y, Wen J, Hong J. The Effects of Auricular Therapy for Cancer Pain: a Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2020;2020:1618767. doi:10.1155/2020/1618767
37. Yeh CH, Lukkahatai N, Campbell C, et al. Preliminary Effectiveness of Auricular Point Acupressure on Chemotherapy-Induced Neuropathy: part 1 Self-Reported Outcomes. Pain Manag Nurs. 2019;20(6):614–622. doi:10.1016/j.pmn.2019.04.005
38. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/s0166-2236(02)00006-1
39. Hui KK, Marina O, Liu J, Rosen BR, Kwong KK. Acupuncture, the limbic system, and the anticorrelated networks of the brain. Auton Neurosci. 2010;157(1–2):81–90. doi:10.1016/j.autneu.2010.03.022
40. Zhang B, Shi H, Cao S, et al. Revealing the magic of acupuncture based on biological mechanisms: a literature review. Biosci Trends. 2022;16(1):73–90. doi:10.5582/bst.2022.01039
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.