")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
A Scoping Review of Anti-Bullying Interventions: Reducing Traumatic Effect of Bullying Among Adolescents
Authors Hikmat R , Yosep I , Hernawaty T, Mardhiyah A
Received 9 October 2023
Accepted for publication 8 January 2024
Published 20 January 2024 Volume 2024:17 Pages 289—304
DOI https://doi.org/10.2147/JMDH.S443841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rohman Hikmat,1 Iyus Yosep,2 Taty Hernawaty,2 Ai Mardhiyah3
1Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Jawa Barat, Indonesia; 2Department of Mental Health, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Jawa Barat, Indonesia; 3Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Jawa Barat, Indonesia
Correspondence: Rohman Hikmat, Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62881023623453, Email [email protected]
Abstract: Bullying is a violent activity that causes significant harm to both victims and perpetrators. Anxiety, despair, low self-esteem, and suicidal ideation are signs of bullying’s traumatic effect. The social environment’s support proved critical in lessening the devastating experience of bullying on adolescents. The purpose of this study is to conduct a scoping Review of Anti-Bullying Interventions with the aim of reporting techniques to reduce traumatic effect of bullying among adolescents. A design scoping review was done in this investigation. The publications were discovered using the PRISMA Extension for Scoping Review method. Three databases were used to find this article: PubMed, CINAHL, and Scopus. The inclusion criteria for this study were that the sample included adolescent victims of bullying, that it was full text, that it was written in English, that it included anti-bullying therapies, that it used randomized control trials or quasi-experimental designs, and that it was published during the last ten years (2014– 2023). The authors found 16 articles were obtained that explored Anti-bullying therapies to minimize symptoms of trauma in adolescent bullies. All of the studies found that the intervention significantly reduced the effects of bullying on victims (p< 0.05). The sample sizes ranged from 31 to 5539 teenage respondents. This study discovered three types of anti-bullying interventions: social support, social skills, and school-based programs. Activities such as education, counseling, and training are used to prevent bullying behavior in schools. Adolescent intervention takes into account the participants’ physical and psychological situations and focuses on completing the stages of adolescent development. Interventions to reduce the impact of trauma on bullying victims need to involve health providers, parents, and adolescents. This aims to form a mutually supportive system in overcoming the problem of bullying.
Keywords: adolescents, anti-bullying intervention, bullying, victims
Introduction
Bullying is defined as any sort of violence or criminality committed purposefully and persistently with the intent of injuring or bringing down someone who is weak.1 Bullying activities undertaken by adolescents against their peers include mocking, spreading, gossiping, giving nicknames, verbally or in writing hurting, isolating, frightening, and even physically attacking.2 Bullying in the youth environment is currently the focus of the community’s attention. Bullying is one of the negative behaviors in which people in positions of authority regularly compel, bully, harass, corner, and hurt weak people.2 Verbal bullying conduct includes insulting, screaming, giving incorrect nicknames, slandering, slandering, and embarrassing others in public. Physical bullying behavior includes hitting weak people, choking, and punching, while mental bullying behavior includes ignoring and isolating, and cyberbullying behavior includes receiving threats or negative messages through social media.3
According to data on bullying cases from the Josephson Institute of Ethics, which conducted a poll of 43,000 adolescents, 47% of 15–18 year olds had experienced bullying, and 50% of adolescents had been taunted, upset, and ridiculed.4 Data from the United Nations Children’s Fund shows that out of 100,000 children in 18 countries, 67% of children have experienced bullying.5 Data from the Program for International Students Assessment (PISA) (2019), bullying in the world occurs most often in Austria, followed by Estonia, Russia and Japan.6 Previous reports show that children aged 13–15 years have been victims of bullying, where the incidence figures were obtained in Africa (47%), Latin America (35%), Europe and Central Asia (32%), and in Indonesia (21%).7 In previous research on 15,600 teenagers, 17% of them reported being victims of bullying and 19% admitted that bullying occurred in their environment.8
There are internal factors and external factors for the occurrence of bullying behavior. Internal factors are personality characteristics, past violence, and the attitude of parents who pamper children so that they do not form a mature personality.9 External factors are the social and cultural environment.10 A previous study identifying factors for the occurrence of bullying include individuals (biology and temperament), family, peer group, and community factors, media schools, and ethnicity.11 Beside of that, factors that can cause bullying include family, peers and school factors.12 Apart from that, bullying occurs due to several causal factors, namely, economic differences, religion, gender, traditions and the habit of seniors to punish their juniors which often occurs.13 There are feelings of revenge or jealousy, there is a desire to dominate the victim with physical strength and sexual attraction.14 These various bullying factors have an impact on victims of bullying behavior.
Efforts to prevent bullying have been carried out through the participation of all parties, both the government, teachers, health workers, parents, peers, the role of a counselor from health workers and the role of the community environment and from within the child himself.15 Empowerment of peers as a medium for conveying information has been widely used in anti-bullying intervention programs, such as implementing psychoeducation programs through peers by making presentations at school or in peer communities by showing dramas, and videos/films followed by discussions.16,17 The same thing is also used in the STAR (Stop Thinking Act Replay) bullying prevention-peer pressure module, namely by using the peer-to-peer discussion method.18,19 Psychoeducation using peer-to-peer methods has been proven effective in intervention programs in cases of bullying.20,21 Various efforts can be made by school counselors to reduce bullying behavior, namely through collaborative efforts.
Community-based program is an intervention strategy carried out jointly by involving a group in the community. The activity begins with the perception or opinion and the same goal in carrying out a prevention and treatment of disease and making changes to individuals, communities and community groups, therefore a group process is carried out in solving a health problem. Previous study have shown that Anti-bullying interventions can be implemented to reduce the incidence of bullying in schools.22 Anti-bullying interventions can be carried out by empowering, peer-support, health education, and forming groups. Previous studies have shown that Anti-bullying interventions are carried out using several methods, namely the school approach, youth approach (forming study groups, social-support or support systems), family approach, skills approach (skill-based community intervention), and group empowerment.15,23
Previous systematic reviews of nursing interventions for reducing bullying incidence show that nursing interventions are beneficial in lowering the negative incidence of bullying but less effective in reducing the negative impact of bullying due to a lack of environmental engagement.24 As a result, the study recommends additional research on social initiatives to mitigate the deleterious effects of bullying on adolescents. Furthermore, prior research indicates that anti-bullying treatments are helpful in avoiding bullying and violence against kids at school.25–27 The report also proposes more research into community-based interventions to lessen the impact of bullying-related trauma. As a result, this is the first scoping assessment of anti-bullying therapies to minimize the impact of bullying trauma in adolescents.
Bullying causes trauma to victims due to the physical and psychological effects. Prolonged trauma results in post-traumatic stress disorder and an increased risk of mortality. Interventions to lessen the impact of bullying are insufficient to be carried out on their own, hence interventions involving many parties such as teachers, parents, youth, and health workers are required to reduce the impact of trauma caused by bullying. The purpose of this study is to conduct a scoping review of Anti-Bullying Interventions with the aim of reporting techniques to reduce traumatic effect of bullying among adolescents.
Materials and Methods
Design
The scoping review that we conducted typically investigates recent topics and challenges globally. Scoping review is a research method that tries to investigate current topics and challenges in the globe.28 Because of its broad conceptualization, this approach can give thorough study results.29 The authors of this study took the following steps: they developed a research topic, determined inclusion and exclusion criteria, selected publications, created extraction tables, analyzed study data and made summaries, and reported the findings of previous studies.30 The PRISMA Extension for Scoping Reviews (PRISMA-ScR) search method was used in this study to discover papers that describe community-based interventions to lessen the detrimental impact of bullying on young victims of bullying. The research question in this study is what the anti-bullying interventions techniques for reducing traumatic effect of bullying among adolescents?
Search Methods
We searched three databases to find relevant articles: CINAHL, PubMed, and Scopus from April 2023 to May 2023. The PCC framework (Populations, Concept, Context) was employed in the search strategy:
Populations: adolescents aged 10–20 years (students, adolescents in community, adolescents)
Concept: anti-bullying interventions (social support, social skills, school-based program)
Context: reduce the traumatic effect (mental health problems such as PTSD, bullying victim questionnaire)
The mayor keywords for search the articles are adolescents OR young adult OR adolescence AND anti-bullying interventions OR bullying interventions AND traumatic disorder OR stress disorder. Search keywords are adjusted to the database used, namely PubMed (Supplementary Table 1), Scopus (Supplementary Table 2), CINAHL (Supplementary Table 3). The authors scanned the database for articles and then filtered them based on the database’s inclusion criteria. The authors then looked for article duplication. The authors then read the title and abstract, followed by the full-text article, to find papers that meet the research objectives. The study’s research questions are: what are the techniques of anti-bullying interventions to decrease the impact of traumatic events on adolescents who are bullied?
Inclusion and Exclusion Criteria
The PRISMA Extension for Systematic Review (PRISM-ScR) search approach was utilized in this study to find community-based intervention methods for minimizing the detrimental impact of bullying on adolescents who have experienced bullying (Figure 1).31 To choose publications for this study, the authors established inclusion and exclusion criteria. The inclusion criteria for this study were that the sample included adolescent victims of bullying aged 10–20, that it was full text, that it was written in English, that it included anti-bullying interventions, that it used randomized control trials or quasi- experimental designs to get adequate articles related to intervention, and that it was published during the last ten years (2013–2022) to get the latest articles about intervention. While the study’s exclusion criteria were articles only provided abstracts, articles were gray literature, and interventions did not focus on reducing the impact of bullying.
 |
Figure 1 PRISMA flow diagram. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.31 |
Data Extraction
In this study, manual tables are utilized to retrieve study results. The manual table was created to assist authors in analyzing and comparing study results. The writer then provides a descriptive description of the study’s findings. The extraction table makes it easy for the authors to compare and categorize the results of each article’s analysis. The authors, year, country, research design, sample, intervention, and study findings are all included in the extraction table.
Quality Appraisal
The authors assessed the article quality to guarantee that the publications reviewed are of high quality. The Joanna Briggs Institute (JBI) instrument was employed by the authors. The Joanna Briggs Institute (JBI) assessment method uses statements from the JBI instrument, which are then scored. The JBI instrument consists of 13 statements for randomized control trial papers and 9 statements for quasi-experimental studies. Each statement contains four evaluation options: yes, no, unclear, and not relevant. A score of “yes” is assigned a value of 1, while scores of “no” and “unclear” are assigned a value of 0. The authors determine that the average rating of the articles utilized in this study is greater than 75%.
Data Analysis
The authors used a descriptive qualitative approach to analyze the data. The authors gathered articles based on inclusion and exclusion criteria, then read and analyzed them. In addition, the authors double-checked the papers retrieved. Data analysis used a thematic analysis approach.32 Data analysis was carried out by two authors independently (IY and SS). When there are differences of opinion, deliberations are held to obtain the results of the discussion. If there was still no agreement, a third author (HSM) was invited to provide his opinion. The research began with comprehensive data collection, gathering literature closely related to the topic of anti-bullying interventions. Once the data was collected, the next stage was to conduct an initial in-depth reading, followed by initial coding. This process was essential in identifying and labeling important segments of the data relating to the research focus. Next, a search for themes that emerged from the data was conducted. A thorough review of the themes was then conducted to ensure that these themes were accurate and representative of the data as a whole. Once the themes were clearly defined and named, drafting the report became the final step. This report not only outlines the main findings, but also integrates these findings with existing literature. The authors presented their findings on anti-bullying interventions for minimizing the detrimental impact of bullying on adolescents who have been bullied. After that the authors classified the types of intervention based on similar methods. The authors classified Anti-bullying interventions based on further research which consist of social support, social skills, and school-based programs.
Results
The total number of articles gathered from the three databases is 397. After eliminating papers based on inclusion criteria, 67 articles were obtained. The authors then deleted articles based on duplicate articles, and we discovered 54 articles. The authors then rejected them based on the outcomes of reading the titles and abstracts, and discovered 29 publications that did not meet the research objectives. The authors then read the full-text publications and deleted them based on exclusion criteria, yielding 16 papers for this study. The authors discovered 16 papers that examined anti-bullying treatments for reducing bullying’s impact on adolescents. To determine the quality of the papers utilized in this study, we employed the JBI Critical Appraisal Tool assessment. For the article criteria utilized in this study, all authors provided a standard score of greater than 75% (Table 1).
 |
Table 1 JBI Critical Appraisal Tool |
The authors discovered 16 papers that examined anti-bullying treatments for reducing bullying’s impact on adolescents. For data extraction, the authors employed handwritten tables. The following table (Table 2) summarizes the findings of the analysis of the 16 papers included in this study:
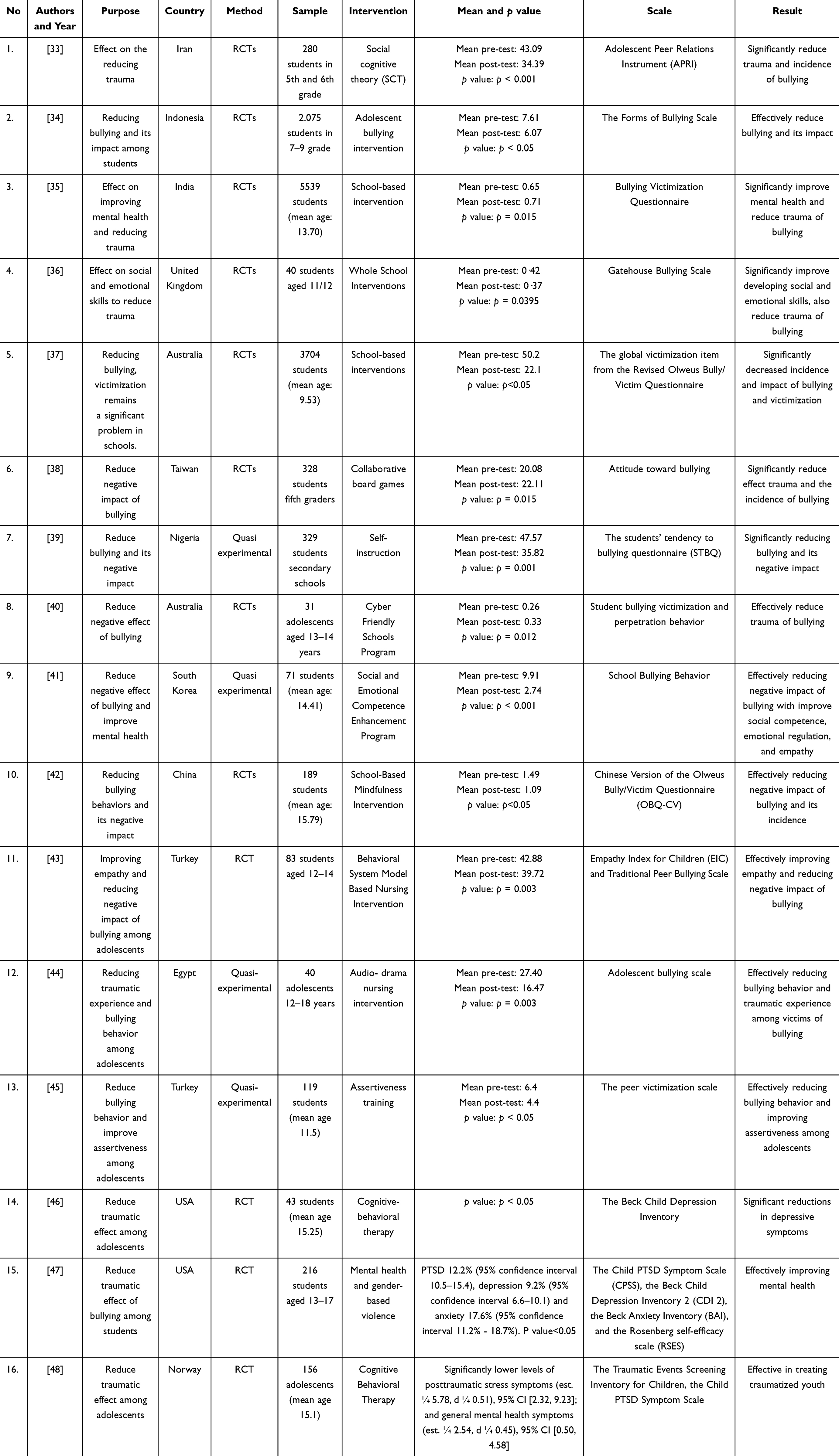 |
Table 2 Extraction Data |
There were 16 publications that talked about community-based interventions for decreasing the negative effects of bullying on adolescents who have been bullied. This study discovered 11 articles from developed countries (1 from the United Kingdom, 2 from Australia, 1 from South Korea, China, 2 from Turkey, and 1 from Egypt, 2 articles from Norway, and 1 article from Norway) and 5 articles from developing countries (1 from Iran, 1 from Indonesia, 1 from India, 1 from Taiwan, and 1 from Nigeria). The sample size ranges from 31 to 5539 respondents. The majority of respondents were from the United Kingdom. We reviewed and analyzed the 16 articles we identified and developed three anti-bullying interventions: social support, social skills, and school-based program.
Anti-bullying interventions are victim-centered interventions that aim to decrease the impacts of bullying-related trauma. Based on the findings of sixteen papers, this intervention is successful in minimizing the effects of bullying trauma on victims (p<0.05). The facilitator’s approach is to provide comfort and protection to the victim so that the victim can actively participate in the process of giving the intervention. The role of the environment that interacts frequently with the victim is critical to the success of the intervention, therefore this intervention includes family, teachers, and friends. The following is an explanation of each anti-bullying intervention method:
Social Support
Social support is a program to reduce the impact of bullying by forming peer tutors. Activities carried out in peer tutoring consist of studying together, sharing between adolescents, and activities to improve psychological health. Activities carried out using the social support method in collaboration with the youth community to increase awareness of bullying. The teachers have a role as a facilitator in the support system activities. Nurses and psychologists have role as leaders to guide support system activities, participants are trained with meditation and relaxation as well as social support.
Whole School Interventions is carried out in collaboration by teachers, health workers, and students.36 Participants took part in discussions about bullying, social and emotional skills, and environmental management to reduce bullying incidents. Students are also facilitated by study groups to support each other during the learning process. This intervention does not significantly reduce the impact of bullying behavior but can create a positive environment in reducing the incidence of bullying.
The Social and Emotional Competence Enhancement Program consists of ten 45-minute sessions that are delivered twice a day for five days in a row. The first and last sessions are face-to-face individual counseling activities, whilst Sessions 2–9 are done in groups utilizing cognitive behavioral techniques.41 Counseling is provided by psychiatric nurses by establishing a therapeutic connection that focuses on participants’ experiences of bullying at school, bullying motives, family dynamics, relationships with peers, unsolved challenges, decision-making patterns, and reflection. To boost participant focus, each session is bundled with pictures, video clips, and games. The outcomes of this intervention show that strengthening empathy, resilience, and problem-solving skills reduces the impact of bullying significantly.
The nursing intervention audio-drama consists of three sessions.44 In the first session, participants were given education about audio-drama about bullying. Then proceed with practice sessions and open questions on the activities carried out. Then the participants continued by watching an audio-drama for 30 minutes. In each activity, participants are invited to discuss to find out how far the participants understand the information provided regarding bullying.
Social Skills
With a youth group approach, social skills are an intervention to build abilities in adolescents in order to lessen the impact of bullying. The activities conducted are beneficial in building resilience and coping abilities in dealing with stressors caused by bullying. This activity involves youth activists in order to enhance youth skills in dealing with bullying. This activity is guided by health specialists, including psychologists and nurses, who help children improve their skills by offering support and counseling services during the training process. A social cognitive theory (SCT)-based intervention is one that aims to improve cognitive abilities in dealing with bullying-related trauma. The intervention lasted 8 sessions (8 weeks).33 Students receive training to help them prevent and mitigate the effects of bullying. Bullying prevention, self-efficacy in controlling bullying, social support, standard norms, expectancies, and establishing positive attitudes are the five key components of this intervention. The SCT-based intervention has been shown to be successful in reducing bullying by raising student awareness.
Another sort of intervention is the Collaborative Board Game, which lasts 8 weeks. Participants play games for one hour per session. The facilitator guides the game by playing an instructional video for the participants to watch.38 Participants engage in games by responding to questions posed by the facilitator. Participants undertake self-reflection guided by the facilitator in each session to determine the increase in bullying knowledge, attitudes, and empathy for each player towards bullying. This game greatly reduces the occurrence of bullying among adolescents.
Based on a Behavioral System Model Nursing intervention was implemented in three stages. The stages are as follows: protection, stimulation, and support.43 Nurses accompany participants while they perform out therapy to reduce the impact of bullying on adolescents. Problem-solving, empathy, and creative drama education are also taught to participants. This study found that treatment can help adolescents cope with bullying.
Self-instruction is a strategy given to students to monitor students’ feelings intensely. The counselor guides students to do peer counseling.39 Self-instruction technique is a cognitive learning strategy, in which each student does his assignments independently and develops strategies to solve problems independently. Activities in the implementation of the intervention are the cognitive modeling stage, open external guidance, individual guidance, and instruction on skills such as empathy and problem solving. Participants took part in 6 sessions of activities. The results of this intervention showed that there was a decrease in the incidence of bullying and its impact after being given the intervention.
Adolescent bullying intervention is an adaptation of the ROOTS method. The intervention was delivered in 12 sessions over the course of 12 weeks. Identity, group trust, and awareness, student impact and reactions to conflict, connecting student-generated changes with behaviors, building student agreements for school violence prevention, and role-playing positive bystander behavior are all components of the intervention.34 Students who have been bullied can seek counseling from psychologists and psychiatric nurses during the intervention. According to the findings of this study, the intervention is helpful in lowering the occurrence and impact of bullying on students.
Adolescent assertiveness training is a treatment that aims to increase assertiveness.45 This course was delivered in eight sessions. Knowledge of (aggressive, assertive, and passive behavior); social rights; notion of restriction; how to say no; body language and communication; and empathy and listening are among the activities. This therapy has been shown to lessen the effects of bullying on students.
Adolescents receive Cognitive Behavioral Therapy for 15 sessions. Psychoeducation, relaxation techniques, affect management, cognitive triangle instruction, working with the trauma story, coping with dysfunctional thoughts, and the parenting component are among the therapies delivered.48 Participants were also offered counselling to help them accept the events of the past. The findings of this intervention revealed that the participants’ mental health improved.
Participants received 12 sessions of cognitive-behavioral treatment. Psychoeducation, relaxation techniques, problem solving, resilience, and self-regulation are among the activities carried out.46 The study’s findings revealed a reduction in the impact of trauma, specifically depression, on participants.
In 12 sessions, participants will learn about mental health and gender-based violence.47 The therapy provided involves empowerment, gender norms, goal-achieving tactics, and self-defense. Psychiatric nurses and psychologists provide in-class counseling to participants. The findings of this intervention suggested that the participants’ mental health problems have decreased.
School-Based Program
School-based programs are activities that collaborate with schools to reduce the impact of bullying and reduce its occurrence. This activity is carried out by health workers and the school to carry out a school-health program. The assessment was carried out on schools that had incidents of bullying and given interventions such as psychoeducation, mindfulness therapy, and improving problem solving for students at school. Teachers become supervisors and companions as long as students carry out school-based program activities. Nurses and psychologists carry out school-health programs as educators and counselors, and facilitate adolescents to form groups as an effort to provide initial psychological support to victims of bullying. The SEHER program with games is a school-based intervention that aims to establish a pleasant environment in order to reduce the incidence and impact of bullying.35 This intervention lasted for ten weeks. The facilitator provides instruction and games to the participants. The education presented focuses on bullying, its effects, how to prevent bullying, and the role of schools in bullying events. The participants were then given the option to speak with one of the teachers about the prevalence of bullying at school. The intervention resulted in a decrease in bullying risk behavior in the school community as well as increased problem-solving skills among adolescents.
School-based interventions use a methodical implementation strategy to enhance school policies and practices, increase students’ social and emotional abilities, and students’ capacities to form positive connections, as well as to prevent and manage bullying and cyberbullying behaviors.37 Boosting empathy and assertiveness, boosting leadership, getting to know the school environment and culture, and building positive relationships between kids, parents, and teachers are all components of executing the intervention. This intervention is carried out by giving pupils with training. According to the study’s findings, there is a decrease in the occurrence and impact of bullying on adolescents.
The School-Based Mindfulness Intervention was delivered in ten sessions over ten weeks.42 The intervention was carried out at school with the participation of students and teachers. This intervention’s content includes an introduction to mindfulness, identifying worry, acting thoughtfully, taking a step back, making friends with difficult things, doing positive things, and practicing empathy. A professionally trained mindfulness instructor provided interventions once a week for 40–45 minutes during the 10-week intervention. Students are also required to carry out the interventions they have been taught on a regular basis and record them in a daily journal. The outcomes of this intervention reveal a reduction in the incidence and harmful impact of bullying on adolescents.
Other efforts include the Cyber Friendly Schools Program, which reviews school policy surrounding bullying situations.40 Students and instructors participate in discussion activities led by health professionals. Following that, participants and instructors were educated on the role of schools in preventing bullying events. The curriculum was delivered in six sessions over the course of eight weeks. Bullying was reduced as a result of the treatments that were implemented.
Discussion
The results of this scoping review showed that Anti-bullying interventions are effective in reducing the impact of trauma on adolescents with bullying experiences. The authors found three community-based program methods, namely social support, social skills, and school-based programs. This community-based program is a collaboration carried out by nurses, teachers, doctors, psychologists, parents, and adolescents to optimize intervention goals. The intervention process pays attention to the physical, psychological, spiritual, and cultural aspects of adolescents so that adolescents feel safe and comfortable during the intervention process.
The sample in this study is adolescents aged 12–18 years. Problems at this stage of adolescent development are dependence on peers, still looking for and trying to hold on to life, and emotional reactions are still unstable and uncontrollable.49 The stages of adolescent development also state that adolescents have unstable emotional conditions and are looking for their identity.50 Adolescent psychology has developed in both emotional and social aspects. These changes make adolescents vulnerable to becoming perpetrators as well as victims of bullying. Previous studies have shown that bullying occurs mostly in adolescents (12–18 years).18,51 Bullying behavior in adolescents is in the form of verbal violence against other students at school. Another study showed that 80% of 10,000 adolescents have bullying experiences.52,53 The bullying behavior most often carried out by adolescents is verbal bullying, namely through words in the form of ridicule, threats and gossip. The peer factor as the cause of bullying also has a significant contribution in this case, because most of the time these adolescents have is to interact with their peers, both at school and in the home environment. In addition, there is a desire to be recognized by other members of their peer group so that they are considered as the holders of full authority over their group.
Bullying can occur in both developed and developing countries. This study found 8 articles from developed countries and 3 from developing countries. The incidence of bullying is not influenced by the conditions of the country’s development. In developing countries, the incidence of bullying is caused by poverty so that adolescents experience difficulties and commit violence in order to meet their biological needs.54 In addition, in developing countries it is also caused by a low level of education. Previous studies have shown that there is a significant relationship between the educational level of adolescents and the incidence of bullying in adolescents.55,56 Whereas in developed countries, the incidence of bullying is caused by difficulties in accepting the differences that arise in adolescents.57 In line with this, previous studies have shown that the incidence of bullying in the USA is caused by adolescents who do not accept differences of opinion between students.58 This shows that bullying can happen anywhere, regardless of the level of progress of the country.
Anti-bullying interventions are carried out with a duration of 8–16 weeks. Interventions to reduce the effects of trauma on victims of bullying require a long time to heal the trauma they experience. The facilitator who guides the course of the intervention needs time to build trust so that the youth feel safe during the intervention. This is in line with previous studies which showed that there was a significant relationship between the duration of the intervention and the trauma recovery process in victims of bullying.12,59 The process of building trust in victims was carried out in the first session, then continued with discussions to deal with the trauma problems they experienced.60 Previous systematic review showed that nursing interventions take 10–18 weeks to reduce the effects of trauma on students who experience bullying.61
Anti-bullying interventions are carried out comprehensively by involving physical, psychological, cultural, and spiritual aspects of adolescents. Every aspect of adolescents must be considered to optimize intervention goals. Previous studies have shown that nursing interventions to reduce the negative effects of bullying are carried out by taking into account the psychological condition of adolescents.62 Nurses also need to pay attention to the development of adolescents to meet the stages of development. Other studies also show that it is important for nurses to pay attention to the stages of adolescent development to improve the psychological health conditions of adolescents.63,64 This shows that the psychological health of adolescents is an important aspect that must be considered in conducting Anti-bullying interventions to reduce the impact of trauma due to bullying.
Social support is an effective social-program-based method by involving youth in the intervention process. Social support utilized discussion groups as well as learning to prevent and reduce the impact of trauma due to bullying. The concept of social support is to utilize peer-support groups between adolescents.65 This is in line with previous study which showed that peer-group significantly reduced the negative impact of bullying on adolescent students.66 At the stage of adolescent development, adolescents need friends their age to find identity and improve emotional and social development in a positive direction. So that this peer-support will make adolescents support each other in the intervention process related to bullying.67 Other studies also show that social support is effective for improving mental health in adolescents who experience bullying.21,35,68 Interventions carried out jointly among adolescents make adolescents support each other to reduce the effects of trauma on victims of bullying. Social support for adolescents is carried out by forming peer counselors and groups of peer tutors who provide information and sharing sessions on bullying. As an effort to increase the output of the intervention, this activity is carried out using a shared learning approach. This shows that interventions carried out jointly among adolescents show significant results in reducing the negative impact of bullying on adolescents.
The community-based program method that can be carried out is Social Skills. This activity was carried out in groups of youth in the community, then youth were empowered to become youth groups who care about bullying. Adolescents are equipped with skills in dealing with stressors due to bullying. This intervention focused on improving youth skills to reduce symptoms of trauma experienced by victims of bullying. Skills trained include communication, problem solving, adaptive coping, and resilience. This skill serves to build a system that is adaptive to bullying incidents experienced by adolescents.26 Previous studies have shown that there is a significant relationship between adaptive coping and resilience in reducing the effects of trauma on victims of bullying.69,70 Resilience and adaptive coping cause adolescents to respond to stressors from unpleasant events to focus on solving problems.61 So that adolescents can survive with the help of health workers as facilitators. Meanwhile, other studies show that effective communication is an important skill that must be possessed by adolescents.71,72 Adolescents are more open to their feelings and conditions through good communication skills.73 So that the intervention process can run smoothly to reduce the symptoms of trauma due to bullying.
Previous study on individual mindfulness therapy show that there is a decrease in bullying behavior in adolescents.74 This therapy is carried out to increase positive behavior and increase empathy and problem solving in adolescents. Adolescents are given individual therapy online. Mindfulness therapy can be done in schools for students to prevent and reduce bullying behavior. This is in accordance with previous studies which show that school-based interventions by practicing meditation can effectively reduce the behavior and impact of bullying.75,76
School-based programs are carried out by focusing on the role of collaboration between health workers, teachers and parents to help adolescents recover from symptoms of trauma due to bullying. Teachers and parents are individuals who spend a long time with adolescents at school and at home. This intervention focuses on activities carried out at school and only on students. Activities also involve teachers as assistants and supervisors in conducting interventions. Students are also trained to build awareness of the school environment to prevent and reduce the impact of bullying.27 Students are also asked to declare anti-bullying so that the school becomes a bullying-free place. Supervision of parents and teachers is important to monitor the condition of adolescents.77 This is in line with previous studies which show that the teacher’s optimal role in supervising and being a facilitator can significantly reduce the negative impact of bullying on adolescents.78,79 Teachers are also a means for youth to express feelings and build a positive environment to reduce bullying in schools. Another study shows that teachers play the role of counselors during school hours to increase the self-confidence of children who experience bullying.80 Parents also have an important role at home, namely being counselors and facilitators in carrying out independent interventions for adolescents who experience bullying. Previous studies have shown that interventions carried out by parents are effective in reducing symptoms of trauma due to bullying in their children.11,81–83 So that school-based programs are effective interventions in reducing the effects of trauma on adolescents who experience bullying.
Anti-bullying interventions are interventions that involve various parties to reduce the impact of bullying on adolescents. This aims to increase the role of each individual optimally so that they can focus on reducing the effects of trauma due to bullying. Awareness that is built collaboratively will be more effective in improving adolescent development. Through Anti-bullying interventions in reducing the impact of bullying, adolescents feel that it is valuable to continue their lives and they are able to improve their physical and psychological health.
This study shows that there are several achievements, namely:
This study can be an illustration in conducting research on systematic-review and meta-analysis to assess the effectiveness of Anti-bullying interventions in reducing the traumatic impact on adolescents as victims of bullying.
This study describes several methods that can be used by the community to reduce the traumatic impact of bullying on adolescents.
Limitation
The limitation in this study is the limited study design, namely randomized control trials and quasi-experiments. This causes the data sources in this study to be limited so that the results of studies based on other design methods cannot be compared. This study is also limited because it only describes the effectiveness of Anti-bullying interventions from the articles reviewed but does not synthesize the level of effectiveness of the Anti-bullying interventions obtained. Besides that, this study is also limited to using three databases in the search for articles so that it does not analyze the results of previous research on Anti-bullying interventions from other databases.
Conclusions
Anti-bullying interventions are carried out in collaboration by various parties, namely health workers, teachers, parents, and adolescents in order to build a system that supports reducing the impact of trauma on adolescents as victims of bullying. Anti-bullying interventions are one of effective for reducing traumatic effects among adolescents as victims of bullying. This study showed that there are three methods of Anti-bullying interventions namely social support, social skills, and school-based programs. The implementation of Anti-bullying interventions pays attention to various aspects of adolescents holistically such as physical, psychological, social and cultural. Participants are given psychoeducation, counseling, and skill improvement in reducing symptoms of trauma experienced due to bullying. The implication of this study is that there is a foundation for health workers in providing interventions to reduce the effects of trauma on adolescents as victims of bullying. Another implication of this research is that it is a reference for the government in making policies in reducing the problem of bullying in adolescents. Recommendations for further research are the need for a systematic review and meta-analysis to determine the effectiveness of Anti-bullying interventions in reducing the impact of trauma on adolescents as victims of bullying.
Acknowledgments
All authors thank Universitas Padjadjaran, Balai Pembiayaan Pendidikan Tinggi (BPPT), and the Education Fund Management Institution or Lembaga Pengelola Dana Pendidikan (LPDP), who has facilitated the database and supported funding for this review.
Funding
There was no external funding in this research.
Disclosure
The authors had no conflicts of interest in this research.
References
1. Nocentini A, Menesini E. KiVa anti-bullying program in Italy: evidence of effectiveness in a randomized control trial. Prev Sci. 2016;17(8):1012–1023. doi:10.1007/s11121-016-0690-z
2. Shamsi NI, Andrades M, Ashraf H. Bullying in school children: how much do teachers know? J Fam Med Prim Care. 2019;8(7):2395–2400. doi:10.4103/jfmpc.jfmpc_370_19
3. Acosta J, Chinman M, Ebener P, Malone PS, Phillips A, Wilks A. Evaluation of a whole-school change intervention: findings from a two-year cluster-randomized trial of the restorative practices intervention. J Youth Adolesc. 2019;48(5):876–890. doi:10.1007/s10964-019-01013-2
4. Mishra DK, Thapa TR, Marahatta SB, Mahotra A. Bullying behavior and psychosocial health - a cross-sectional study among school students of pyuthan municipality. J Nepal Health Res Counc. 2018;16(1):73–78. doi:10.3126/jnhrc.v16i1.19370
5. UNICEF. Peer violence; 2017. Available from: https://www.unicef.org.
6. Patel V, Varma J, Nimbalkar S, Shah S, Phatak A. Prevalence and profile of bullying involvement among students of rural schools of Anand, Gujarat. India Indian J Psychol Med. 2020;42. doi:10.4103/IJPSYM.IJPSYM_172_19
7. Biswas T, Scott JG, Munir K, et al. Global variation in the prevalence of bullying victimisation amongst adolescents: role of peer and parental supports. EClinicalMedicine. 2020;20:100276. doi:10.1016/j.eclinm.2020.100276
8. Gaete J, Valenzuela D, Rojas-Barahona C, Valenzuela E, Araya R, Salmivalli C. The KiVa antibullying program in primary schools in Chile, with and without the digital game component: study protocol for a randomized controlled trial. Trials. 2017;18(1):1–10. doi:10.1186/s13063-017-1810-1
9. Moon H, Lee S. Moderating effects of socio-ecological factors on the relationship between adolescent exposure to media violence and attitudes towards school bullying. J Adv Nurs. 2020;76(11):2921–2932. doi:10.1111/jan.14478
10. Bonell C, Mathiot A, Allen E, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE) trial: update to cluster randomised controlled trial protocol. Trials. 2017;18(1):238. doi:10.1186/s13063-017-1984-6
11. Graham K, Bernards S, Laslett AM, et al. Children, parental alcohol consumption, and intimate partner violence: a multicountry analysis by perpetration versus victimization and sex. J Interpers Violence. 2021;36(11–12):5608–5634. doi:10.1177/0886260518804182
12. van Gils FE, Colpin H, Verschueren K, et al. Teachers’ responses to bullying questionnaire: a validation study in two educational contexts. Front Psychol. 2022;13:830850. doi:10.3389/fpsyg.2022.830850
13. Pozzoli T, Gini G. Behavior during cyberbullying episodes: initial validation of a new self-report scale. Scand J Psychol. 2020;61(1):22–29. doi:10.1111/sjop.12517
14. Morjaria P, Evans J, Gilbert C. Predictors of spectacle wear and reasons for nonwear in students randomized to ready-made or custom-made spectacles: results of secondary objectives from a randomized noninferiority trial. JAMA Ophthalmol. 2019;137(4):408–414. doi:10.1001/jamaophthalmol.2018.6906
15. Ferrer-Cascales R, Albaladejo-Blázquez N, Sánchez-SanSegundo M, Portilla-Tamarit I, Lordan O, Ruiz-Robledillo N. Effectiveness of the TEI program for bullying and cyberbullying reduction and school climate improvement. Int J Environ Res Public Health. 2019;16(4):580. doi:10.3390/ijerph16040580
16. Helfrich EL, Doty JL, Su YW, Yourell JL, Gabrielli J. Parental views on preventing and minimizing negative effects of cyberbullying. Child Youth Serv Rev. 2020;118:105377. doi:10.1016/j.childyouth.2020.105377
17. Yosep I, Pramukti I, Agustina HR, Kurniawan K, Agustina HS, Hikmat R. Triple-P e-Parenting to Improve Awareness of Psychiatric Nurses on Preventing Cyberbullying in Adolescents. Vol. 11. Healthcare; 2023.
18. Schultze-Krumbholz A, Schultze M, Zagorscak P, Wölfer R, Scheithauer H. Feeling cybervictims’ pain-the effect of empathy training on cyberbullying. Aggress Behav. 2016;42(2):147–156. doi:10.1002/ab.21613
19. Khanhkham A, Williams RD, Housman JM, Odum M. Sexual dating violence, school-based violence, and risky behaviors among U.S. high school students. J Community Health. 2020;45. doi:10.1007/s10900-020-00811-1
20. Midgett A, Doumas DM, Sears D, Lunquist A, Hausheer R. A bystander bullying psychoeducation program with middle school students: a preliminary report. Prof Couns. 2015;5. doi:10.15241/am.5.4.486
21. Huang Y, Espelage DL, Polanin JR, Hong JS. A meta-analytic review of school-based anti-bullying programs with a parent component. Int J Bullying Prev. 2019;1(1):32–44. doi:10.1007/s42380-018-0002-1
22. Aboujaoude E, Savage MW, Starcevic V, Salame WO. Cyberbullying: review of an old problem gone viral. J Adolesc Health. 2015;57(1):10–18. doi:10.1016/j.jadohealth.2015.04.011
23. Juárez-Chávez E, Cooney EE, Hidalgo A, Sánchez J, Poteat T. Violence experiences in childhood and adolescence among gay men and transgender women living in perú: a qualitative exploration. J Interpers Violence. 2021;36(9–10):4235–4255. doi:10.1177/0886260518787811
24. Gaffney H, Farrington DP, Espelage DL, Ttofi MM. Are cyberbullying intervention and prevention programs effective? A systematic and meta-analytical review. Aggress Violent Behav. 2019;45:134–153. doi:10.1016/j.avb.2018.07.002
25. Lan M, Law N, Pan Q, et al. Cyberbullying in elementary and middle school students: a systematic review. Comput Educ. 2022;18(5):53–66.
26. Díaz-Caneja CM, Martín-Babarro J, Abregú-Crespo R, et al. Efficacy of a web-enabled, school-based, preventative intervention to reduce bullying and improve mental health in children and adolescents: study protocol for a cluster randomized controlled trial. Front Pediatr. 2021;9:628984. doi:10.3389/fped.2021.628984
27. Yosep I, Hikmat R, Mardhiyah A. School-based nursing interventions for preventing bullying and reducing its incidence on students: a scoping review. Int J Environ Res Public Health. 2023;20(2):1577. doi:10.3390/ijerph20021577
28. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. doi:10.1002/2327-6924.12380
29. Bradbury-Jones C, Aveyard H, Herber OR, Isham L, Taylor J, O’Malley L. Scoping reviews: the PAGER framework for improving the quality of reporting. Int J Soc Res Methodol. 2021;00(00):1–14.
30. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
31. Page MJ. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021. doi:10.1136/bmj.n71
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Salimi N, Karimi-Shahanjarini A, Rezapur-Shahkolai F, Hamzeh B, Roshanaei G, Babamiri M. The effect of an anti-bullying intervention on male students’ bullying-victimization behaviors and social competence: a randomized controlled trial in deprived urban areas. J Res Health Sci. 2019;19(4):1.
34. Bowes L, Aryani F, Ohan F, et al. The development and pilot testing of an adolescent bullying intervention in Indonesia - the ROOTS Indonesia program. Glob Health Action. 2019;12(1):1656905. doi:10.1080/16549716.2019.1656905
35. Singla DR, Shinde S, Patton G, Patel V. The mediating effect of school climate on adolescent mental health: findings from a randomized controlled trial of a school-wide intervention. J Adolesc Health. 2021;69(1):90–99. doi:10.1016/j.jadohealth.2020.09.030
36. Bonell C, Dodd M, Allen E, et al. Broader impacts of an intervention to transform school environments on student behaviour and school functioning: post hoc analyses from the INCLUSIVE cluster randomised controlled trial. BMJ Open. 2020;10(5):e031589. doi:10.1136/bmjopen-2019-031589
37. Rapee RM, Shaw T, Hunt C, Bussey K, Hudson JL, Mihalopoulos C. Combining whole-school and targeted programs for the reduction of bullying victimization: a randomized, effectiveness trial. Aggress Behav. 2020;46. doi:10.1002/ab.21881
38. Nieh HP, Wu WC. Effects of a collaborative board game on bullying intervention: a group-randomized controlled trial. J Sch Health. 2018;88(10):725–733. doi:10.1111/josh.12675
39. Nwokolo CN, Okocha AI. Effect of self-instruction on bullying tendency among secondary school students in Nnewi North local government area of Anambra State. Asian J Educ Soc Stud. 2022;30(4 SE–Original Research Article):):22–30. doi:10.9734/ajess/2022/v30i430730
40. Cross D, Shaw T, Hadwen K, et al. Longitudinal impact of the cyber friendly schools program on adolescents’ cyberbullying behavior. Aggress Behav. 2016;42(2):166–180. doi:10.1002/ab.21609
41. Song YM, Kim S. Effects of a social and emotional competence enhancement program for adolescents who bully: a quasi-experimental design. Int J Environ Res Public Health. 2022;19(12). doi:10.3390/ijerph19127339
42. Liu X, Xiao R, Tang W. The impact of school-based mindfulness intervention on bullying behaviors among teenagers: mediating effect of self-control. J Interpers Violence. 2022;37(21–22):NP20459–81. doi:10.1177/08862605211052047
43. Evgin D, Bayat M. The effect of behavioral system model based nursing intervention on adolescent bullying. Florence Nightingale J Nurs. 2020;28(1):71–82. doi:10.5152/FNJN.2020.18061
44. Salama A, Hassan R, Zayed D. Effect of audio- drama nursing intervention on bullying among adolescent girls with visual impairment. Egypt J Heal Care. 2020;11:1341–1357. doi:10.21608/ejhc.2020.278889
45. Avşar F, Ayaz Alkaya S. The effectiveness of assertiveness training for school-aged children on bullying and assertiveness level. J Pediatr Nurs. 2017;36:186–190. doi:10.1016/j.pedn.2017.06.020
46. Shirk SR, Deprince AP, Crisostomo PS, Labus J. Cognitive behavioral therapy for depressed adolescents exposed to interpersonal trauma: an initial effectiveness trial. Psychotherapy. 2014;51(1):167–179. doi:10.1037/a0034845
47. Friedberg R, Baiocchi M, Rosenman E, Amuyunzu-Nyamongo M, Nyairo G, Sarnquist C. Mental health and gender-based violence: an exploration of depression, PTSD, and anxiety among adolescents in Kenyan informal settlements participating in an empowerment intervention. PLoS One. 2023;18(3):e0281800. doi:10.1371/journal.pone.0281800
48. Jensen TK, Holt T, Ormhaug SM, Egeland K, Granly L, Hoaas LC. A randomized effectiveness study comparing trauma-focused cognitive behavioral therapy with therapy as usual for youth. J Clin Child Adolesc Psychol. 2014;43. doi:10.1080/15374416.2013.822307
49. Smith GM, Ashbridge DM, Davis RH, Steinmetz W. Correlation between reduction of seclusion and restraint and assaults by patients in Pennsylvania’s state hospitals. Psychiatr Serv. 2015;66(3):303–309. doi:10.1176/appi.ps.201400185
50. Wang GF, Jiang L, Wang LH, et al. Examining Childhood maltreatment and school bullying among adolescents: a cross-sectional study from Anhui Province in China. J Interpers Violence. 2019;34(5):980–999. doi:10.1177/0886260516647000
51. Siddiqui SA. Cyberbullying and cyber- victimization: from online suicide groups to “Blue Whale”. In: Menace. Vol. 54. Indian pediatrics. India; 2017:1056.
52. Dema T, Tripathy JP, Thinley S, et al. Suicidal ideation and attempt among school going adolescents in Bhutan - a secondary analysis of a global school-based student health survey in Bhutan 2016. BMC Public Health. 2019;19(1):1605. doi:10.1186/s12889-019-7791-0
53. Midgett A, Doumas DM, Johnston A, Trull R, Miller R. Rethinking bullying interventions for high school students: a qualitative study. J Child Adolesc Couns. 2018;4. doi:10.1080/23727810.2017.1381932
54. Hettiarachchi LV, Kinner SA, Tibble H, Borschmann R. Self-harm among young people detained in the youth justice system in Sri Lanka. Int J Environ Res Public Health. 2018;15(2):209. doi:10.3390/ijerph15020209
55. Rahman MM, Rahman MM, Khan MMA, Hasan M, Choudhury KN. Bullying victimization and adverse health behaviors among school-going adolescents in South Asia: findings from the global school-based student health survey. Depress Anxiety. 2020;37(10):995–1006. doi:10.1002/da.23033
56. Casey EA, Lindhorst T, Storer HL. The situational-cognitive model of adolescent bystander behavior: modeling bystander decision-making in the context of bullying and teen dating violence. Psychol Violence. 2017;7(1):33–44. doi:10.1037/vio0000033
57. Jadambaa A, Thomas HJ, Scott JG, Graves N, Brain D, Pacella R. Prevalence of traditional bullying and cyberbullying among children and adolescents in Australia: a systematic review and meta-analysis. Aust N Z J Psychiatry. 2019;53(9):878–888. doi:10.1177/0004867419846393
58. Shinde S, Weiss HA, Varghese B, et al. Promoting school climate and health outcomes with the SEHER multi-component secondary school intervention in Bihar, India: a cluster-randomised controlled trial. Lancet. 2018;392(10163):2465–2477. doi:10.1016/S0140-6736(18)31615-5
59. van Niejenhuis C, Huitsing G, Veenstra R. Working with parents to counteract bullying: a randomized controlled trial of an intervention to improve parent-school cooperation. Scand J Psychol. 2020;61(1):117–131. doi:10.1111/sjop.12522
60. Winfield AFT, Jirotka M. Ethical governance is essential to building trust in robotics and artificial intelligence systems. Philos Trans R Soc A. 2018;376(2133):20180085. doi:10.1098/rsta.2018.0085
61. Yosep I, Hikmat R, Mardhiyah A, Hazmi H, Hernawaty T. Method of nursing interventions to reduce the incidence of bullying and its impact on students in school: a scoping review. Healthcare. 2022;10(10):1835. doi:10.3390/healthcare10101835
62. Allen BC, Holland P, Reynolds R. The effect of bullying on burnout in nurses: the moderating role of psychological detachment. J Adv Nurs. 2015;71(2):381–390. doi:10.1111/jan.12489
63. Laschinger HKS. Impact of workplace mistreatment on patient safety risk and nurse-assessed patient outcomes. JONA J Nurs Adm. 2014;44(5):1.
64. Griffin M, Clark CM. Revisiting cognitive rehearsal as an intervention against incivility and lateral violence in nursing: 10 years later. J Contin Educ Nurs. 2014;45(12):535–542. doi:10.3928/00220124-20141122-02
65. Yosep I, Hikmat R, Mardhiyah A. Nursing Intervention for preventing cyberbullying and reducing its negative impact on students: a scoping review. J Multidiscip Healthc. 2023;16:261–273. doi:10.2147/JMDH.S400779
66. Rose CA, Espelage DL, Monda-Amaya LE, Shogren KA, Aragon SR. Bullying and middle school students with and without specific learning disabilities: an examination of social-ecological predictors. J Learn Disabil. 2015;48(3):239–254. doi:10.1177/0022219413496279
67. Cowie H. Peer support as an intervention to counteract school bullying: listen to the children. Child Soc. 2011;25(4):287–292. doi:10.1111/j.1099-0860.2011.00375.x
68. Hamm MP, Newton AS, Chisholm A, et al. Prevalence and effect of cyberbullying on children and young people: a scoping review of social media studies. JAMA Pediatr. 2015;169(8):770–777. doi:10.1001/jamapediatrics.2015.0944
69. Hutson E, Kelly S, Militello LK. Systematic review of cyberbullying interventions for youth and parents with implications for evidence-based practice. Worldviews Evidence-Based Nurs. 2018;15(1):72–79. doi:10.1111/wvn.12257
70. Cassidy W, Faucher C, Jackson M. Cyberbullying among youth: a comprehensive review of current international research and its implications and application to policy and practice. Sch Psychol Int. 2013;34(6):575–612. doi:10.1177/0143034313479697
71. Healy KL, Sanders MR. Randomized controlled trial of a family intervention for children bullied by peers. Behav Ther. 2014;45(6):760–777. doi:10.1016/j.beth.2014.06.001
72. Moore B, Woodcock S, Dudley D. Developing wellbeing through a randomised controlled trial of a martial arts based intervention: an alternative to the anti-bullying approach. Int J Environ Res Public Health. 2019;16(1):1–18.
73. Van Hee C, Jacobs G, Emmery C, et al. Automatic detection of cyberbullying in social media text. PLoS One. 2018;13(10):e0203794. doi:10.1371/journal.pone.0203794
74. Botha E, Gwin T, Purpora C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: a systematic review of quantitative evidence protocol. JBI Database Syst Rev Implement Rep. 2015;13(10):21–29. doi:10.11124/jbisrir-2015-2380
75. Messias E, Kindrick K, Castro J. School bullying, cyberbullying, or both: correlates of teen suicidality in the 2011 CDC youth risk behavior survey. Compr Psychiatry. 2014;55(5):1063–1068. doi:10.1016/j.comppsych.2014.02.005
76. Wachs S, Bilz L, Fischer SM, Schubarth W, Wright MF. Students’ willingness to intervene in bullying: direct and indirect associations with classroom cohesion and self-efficacy. Int J Environ Res Public Health. 2018;15(11):2577. doi:10.3390/ijerph15112577
77. Ahtola A, Haataja A, Kärnä A, Poskiparta E, Salmivalli C. Implementation of anti-bullying lessons in primary classrooms: how important is head teacher support? Educ Res. 2013;55(4):376–392. doi:10.1080/00131881.2013.844941
78. Şimşek N, Şahin D, Evli M. Internet addiction, cyberbullying, and victimization relationship in adolescents: a sample from Turkey. J Addict Nurs. 2019;30(3):201–210. doi:10.1097/JAN.0000000000000296
79. Bowllan NM. Implementation and evaluation of a comprehensive, school-wide bullying prevention program in an urban/suburban middle school. J Sch Health. 2011;81(4):167–173. doi:10.1111/j.1746-1561.2010.00576.x
80. Fridh M, Lindström M, Rosvall M. Subjective health complaints in adolescent victims of cyber harassment: moderation through support from parents/friends - a Swedish population-based study. BMC Public Health. 2015;15(1):949. doi:10.1186/s12889-015-2239-7
81. Young R, Tully M, Ramirez M. School administrator perceptions of cyberbullying facilitators and barriers to preventive action: a qualitative study. Heal Educ Behav. 2016;44(3):476–484. doi:10.1177/1090198116673814
82. Lefler NL. The role of sociocultural context in cyberbullying in Israeli society: comparing Arab and Jewish parents’ perceived knowledge of their adolescent children’ s involvement in cyberbullying. Int J Bullying Prev. 2022;2022:0123456789.
83. Yosep I, Hikmat R, Mardhiyah A, Kurniawan K, Amira I. A scoping review of the online interventions by nurses for reducing negative impact of bullying on students. J Multidiscip Healthc. 2023;16:773–783. doi:10.2147/JMDH.S406050
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.