")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Zanubrutinib (BGB-3111), a Second-Generation Selective Covalent Inhibitor of Bruton’s Tyrosine Kinase and Its Utility in Treating Chronic Lymphocytic Leukemia
Received 14 December 2020
Accepted for publication 17 February 2021
Published 2 March 2021 Volume 2021:15 Pages 919—926
DOI https://doi.org/10.2147/DDDT.S250823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Joanna M Rhodes,1 Anthony R Mato2
1CLL Research and Treatment Center, Northwell Health Cancer Institute, Barbara and Donald Zucker School of Medicine at Northwell/Hofstra, New Hyde Park, NY, USA; 2Chronic Lymphocytic Leukemia Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Correspondence: Joanna M Rhodes
CLL Research and Treatment Center, 410 Lakeville Road Suite 212, New Hyde Park, NY, 11042, USA
Tel +1 516 470-4050
Fax +1 516 470-4250
Email [email protected]
Abstract: The understanding of the B cell receptor (BCR) pathway and its contribution to chronic lymphocytic leukemia (CLL) pathogenesis have led to the development of targeted BCR inhibitors which have transformed the treatment paradigm of CLL. Ibrutinib is a first-in-class oral Bruton’s tyrosine kinase (BTK) inhibitor which has demonstrated improvements in both progression free (PFS) and overall survival (OS) in both the treatment naïve and relapsed/refractory setting as compared to traditional chemoimmunotherapy. Despite its clinical efficacy, many patients discontinue treatment due to adverse events, which are thought to be mediated through off-target kinase inhibition. Zanubrutinib is a second-generation non-covalent BTK inhibitor with higher potency, allowing for inhibition of BTK with fewer off target effects. Early phase clinical trials have demonstrated excellent efficacy and a well-tolerated safety profile. Long-term follow-up is needed, but zanubrutinib holds promise to be an effective therapy for CLL with a manageable side effect profile and will be an exciting addition to our treatment paradigm.
Keywords: chronic lymphocytic leukemia, small lymphocytic lymphoma, BTK inhibitor, zanubrutinib
Introduction
Chronic lymphocytic leukemia (CLL) is a clinically heterogenous disease which predominantly affects older individuals, with a median age of onset of 70 years.1 While the disease course can be indolent, a majority of patients develop symptoms related to their underlying disease and require therapy. Historically, patients were treated with the combination chemoimmunotherapy fludarabine/cyclophosphamide/rituximab (FCR), bendamustine/rituximab (BR) or chlorambucil based regimens.2–5 As our understanding of the role of the B cell receptor (BCR) pathway in CLL pathogenesis evolved, targeted agents were developed to inhibit key components of this pathway. Ibrutinib is a first-in-class Bruton’s tyrosine kinase (BTK) inhibitor that has transformed the management of both treatment-naïve and relapsed/refractory CLL.6 Herein, we focus on the development of the second generation BTK inhibitor zanubrutinib and its use in the treatment of CLL.
Bruton’s Tyrosine Kinase, B Cell Receptor Signaling and CLL
BTK is a TEC family tyrosine kinase expressed in all hematopoietic stem cell lineages except for T cell progenitors.7 BTK plays a pivotal role in the BCR pathway, as activated BTK phosphorylates and activates PLCγ2, releasing intracellular calcium stores leading to upregulation of transcription factors including NFκB.8,9 This initiates integrin activation, chemokine mediated migration, and B cell proliferation.8 BCR signaling is important in the pathogenesis of B cell lymphoma via several mechanisms: constitutive activation of the B cell, chronic activation of BCR, and tonic activation of BCR.10 In CLL this can be through both ligand-dependent antigen-mediated pathways and ligand-independent autonomous pathways.10
Inhibition of BTK is an effective treatment strategy in CLL. Ibrutinib is a first-in-class non-covalent BTK inhibitor which is FDA-approved for treatment of several B cell malignancies,11,12,18 including CLL. Ibrutinib has demonstrated improvements in progression free survival (PFS) for patients with both the treatment-naïve13–15 and relapsed/refractory CLL.6,16 Additionally, ibrutinib is effective in CLL patients with high-risk features, including deletion 17p17 (del17p) and unmutated immunoglobulin heavy chain gene (UM-IGHV).13,16 Despite its robust clinical efficacy, many patients discontinue ibrutinib due to toxicity,19,20 including atrial fibrillation,21,22 ventricular arrhythmias,23 major bleeding,24,25 hypertension,26 and arthralgias/myalgias.27 Inhibition of off-target kinases including TEC, epidermal growth factor receptor (EGFR) and interleukin 2-inducible T cell kinase (ITK) has been implicated as possible etiologies for these side effects.28 Second generation BTK inhibitors have been engineered with more specificity for BTK in an effort to minimize off-target side effects.29,30 Acalabrutinib is a second generation BTK inhibitor and was recently approved for treatment naïve and relapsed/refractory CLL based on data from the ELEVATE-TN31 and ASCEND32 trials which demonstrated improvements in overall response rate (ORR) and PFS compared to chlorambucil-obinutuzumab and either idelalisib or bendamustine-rituximab, respectively.32
Zanubrutinib: Development and Early Phase Data
Zanubrutinib is a highly specific next-generation BTK inhibitor which is FDA-approved for the treatment of relapsed/refractory mantle cell lymphoma (MCL).33 It binds covalently to Cys481 in the adenosine-triphosphate binding pocket of BTK.29 Utilizing a structure–activity relationship (SAR)-driven strategy, several key stoichiometric modifications have allowed for increased specificity for BTK, leading to a decreased rate of inhibition of EGFR, HER2, ITK, JAK3, TEC, BMX and BLK.29 In MCL and diffuse large B cell lymphoma (DLBCL) cell lines, zanubrutinib inhibits BCR aggregation-triggered BTK autophosphorylation, inhibiting downstream PLC2γ signaling and blocking cell proliferation.29 Based on this improved binding to BTK and the decreased inhibition of off-target kinases, zanubrutinib is being studied in the treatment of B cell malignancies.
In the first in human Phase 1 trial, patients with B cell malignancies were treated with continuous single agent zanubrutinib until disease progression or intolerable toxicity in a 3+3 dose-escalation design.34 Oral administration of zanubrutinib lead to maximum serum concentration (Cmax) approximately 2 hours after dosing, and the area under the curve (AUC) increased with increasing doses. The mean Cmax was 346 ng/mL and 658 ng/mL after single dose of 160 mg or 320 mg, and the mean half-life was approximately 4 hours for both 160 mg twice daily dosing and 320 mg daily.34 Median BTK occupancy in the paired nodal samples on day 3 of week 1 was 95% with the 320 g daily dose and was 100% in the 160 mg twice daily dose cohort. Nodal BTK occupancy was >95% in 89% of patients in the 160 mg twice daily cohort compared to 50% in the 320 mg daily dose.34 Given these findings, both 320 mg daily dosing and 160 mg twice daily dosing were further explored in subsequent clinical trials.
Safety and Efficacy of Zanubrutinib Monotherapy in CLL
Three clinical trials have determined the safety and efficacy of zanubrutinib in CLL. In the initial Phase 1 trial, 94 patients with CLL/SLL including 22 treatment-naïve patients were treated with zanubrutinib.34 The median number of prior therapies was 2 (range 1–9). Twenty-three percent had deletion 11q (del11q), 19.1% had del17p or TP53 mutations. Patients received 320 mg daily (n=40) or 160 mg twice daily (n=54). At a median follow-up of 13.7 months, 89 patients (94.7%) remained on study treatment. Two patients discontinued treatment due to progressive disease (PD), 2 for adverse events (AEs) and 1 for unspecified reasons. The most common AEs were contusion (35.1%), upper respiratory tract infection (33%), cough (25.5%) and diarrhea (21.3%). Neutropenia (6.4%), hypertension (2.1%), and pneumonia (2.1%) were the most common serious AEs.34 One patient developed atrial fibrillation and one patient had a major bleeding episode.35 Seventy-eight patients were evaluable for response. Overall response rate (ORR) was 96.2%, with 2 patients achieving a complete response (CR). Responses were similar in patients with high-risk genetic features, including del17p and TP53 mutation (ORR 100%). Median PFS was not reached, and 12-month PFS was 100%.36 This trial determined the recommended Phase 2 dose of 160 mg twice daily and demonstrated a well-tolerated safety profile. ORR was high and was similar in patients with high-risk genetic features.
A phase 2 study of zanubrutinib conducted in China enrolled 91 patients with relapsed/refractory CLL who received 160 mg of zanubrutinib twice daily.36 The median age was 61 years old and patients had received standard chemoimmunotherapy (fludarabine or chlorambucil-based), with a median of 1 prior line of therapy (range 1–9). Forty-five percent of patients had received at least 2 prior lines of therapy. Twenty-four percent had a del17p or TP53 mutated and 56% were UM-IGHV. The ORR was 84.6%, with 3 patients with SLL (3.3%) attaining a CR. For patients with either del17p or TP53 mutation, the ORR was 86.4% and was 82% for UM-IGHV. At a median follow-up of 12.9 months, the estimated 12-month PFS was 87.2%. Four patients died on study, 2 from progressive disease and 2 from cardiopulmonary failure. The most common AEs were neutropenia (69.2%), upper respiratory tract infection (45.1%) and thrombocytopenia (41.8%). Petechiae/purpura/contusion was common (35.2%) as was hematuria (39.5%). There were two patients who experienced ≥ grade 3 bleeding events, one gastrointestinal bleed in the setting of new diagnosis of colon cancer and another a right sided thalamic hemorrhage after fall. Both were assessed as unrelated to zanubrutinib. No patients developed atrial fibrillation and there were no cases of tumor lysis syndrome. As seen in previous trials, zanubrutinib has a consistently high response rate across risk groups. AEs were manageable, with no episodes of atrial fibrillation or major bleeding attributed to zanubrutinib.
The Phase 3 Sequoia trial (NCT03336333) is investigating the use of zanubrutinib in patients with treatment-naïve CLL as compared to bendamustine-rituximab.37 Patients with del17p were treated with zanubrutinib in a non-randomized cohort (Cohort C) which has reported results.38 One hundred and nine patients were enrolled onto the study and ORR was 94.5%. Three patients (2.8%) attained a CR, and one patient (0.9%) had complete response with incomplete count recovery (CRi). There were 9 progression events, with 4 patients having histologic confirmed Richter’s transformation. The median PFS and OS were not reached at median follow-up of 18.2 months. The estimated 18-month PFS rate was 88.6%. Common AEs were upper respiratory tract infection (19.3%), neutropenia (17.4%), diarrhea (16.5%), nausea (14.7%) and rash (13.8%). The most common serious AEs were pneumonia (3.7%) and neutropenia (12.9%). Three patients developed new atrial fibrillation, but no patients needed to discontinue zanubrutinib, and 5.5% of patients had grade 3 or higher bleeding.39 Follow-up for Cohorts A and B has not been reported to date. Cohort D will study zanubrutinib in combination with venetoclax, which will further our understanding of how to best use zanubrutinib in combination.40
Combination Strategies with Zanubrutinib
Despite therapeutic advances, CLL remains incurable with current strategies. Currently, BTK inhibitor monotherapy requires continuous treatment until progression or intolerable side effect. Anti-CD20 monoclonal antibodies and/or venetoclax are currently under study in combination with various BTK inhibitors to determine if these combinations are feasible time-limited treatment options.
Obinutuzumab is a glycoengineered anti-CD20 monoclonal antibody and is FDA-approved for use in combination with ibrutinib, acalabrutinib, chlorambucil and venetoclax as frontline treatment of CLL.31,41–43 To determine the safety and efficacy of zanubrutinib in combination with obinutuzumab, patients with B cell malignancies were treated on a phase 1 trial (NCT02569476) in two parts: in Part 1 patients received zanubrutinib (320 mg daily or 160 mg twice daily) and obinutuzumab to determine the maximum tolerated dose.44 In Part 2, patients were continued on zanubrutinib monotherapy. Twelve patients with CLL were treated on Part 1. The median age was 68, and all patients had relapsed/refractory disease and received a median of 2 lines of prior therapy (range 1–9). Nine patients were treated with 320 mg daily and 3 patients received 160 mg twice daily. In the safety evaluation in Part 1, the most common AEs (all grade) were cough (41.7%), neutropenia (41.7%), upper respiratory tract infection (33.3%), and contusion (25%). The most common serious AEs were neutropenia (16.7%), dyspnea (8.3%), peripheral swelling (8.3%), and QTc prolongation (8.3%). In part 2, a total of 45 patients (20 treatment naïve, 25 relapsed/refractory) received treatment. The most common AEs were upper respiratory tract infection (51%), neutropenia (44%), and contusion (33%). The most common serious AEs were neutropenia (31.3%), pneumonia (8.9%) and thrombocytopenia (6.7%). No patients developed atrial fibrillation or flutter and there was only one major bleeding event (epistaxis). At a median follow-up of 29 months, the ORR was 100% for patients with TN CLL with 6 CRs.44 The ORR was 92% in patients with relapsed/refractory CLL with 7 CRs. At 24 months, the estimated event-free survival rate was 90.4% (95% CI, 76.5% to 96.3%). The median PFS was not reached. The combination of obinutuzumab and zanubrutinib was well tolerated with excellent efficacy, though requires continuous therapy which may limit its use. Further follow-up is necessary to determine long-term efficacy of this combination.
A multi-center Phase I/II trial (NCT03824483) investigated the combination of venetoclax, zanubrutinib, and obinutuzumab (BOVen) to determine the time to response with undetectable minimal residual disease (uMRD).45 Patients received obinutuzumab with zanubrutinib as a debulking strategy, followed by the addition of venetoclax after 2 cycles. Triple combination therapy was continued for 2 cycles after uMRD response in the peripheral blood and bone marrow (10−4 sensitivity by flow cytometry). Thirty-nine patients with treatment-naïve CLL were enrolled. Fifteen percent of patients had a TP53 aberration and 72% were UM-IGHV.45 The most common AEs were neutropenia (49%), thrombocytopenia (46%), infusion reactions (41%), bruising (41%) and diarrhea (41%). There was one fatal bleeding in a patient treated with therapeutic anticoagulation. At a median follow-up of 11 months, 75% of patients were uMRD in the bone marrow and 84% in the peripheral blood.45 The ORR was 100%, with 57% CR rate. The triplet combination demonstrated the ability to attain uMRD states with less than 1 year of treatment with a manageable AE profile. Further follow-up is necessary to determine the duration of responses as well as time to relapse, but these early data are encouraging.
How Does Zanubrutinib Fit into the Treatment Landscape of CLL?
Across early clinical trials, zanubrutinib has excellent response rates which are similar to those seen in trials of ibrutinib in similar patient populations. Neutropenia, upper respiratory tract infections, and pneumonia are some of the most frequent AEs with relatively few serious events reported to date. Relatively few episodes of cardiac arrhythmias have been reported, though the follow-up time period is short. Rates of major hemorrhage are low and are similar compared to ibrutinib. A meta-analysis of 6 clinical trials of patients with B cell NHL treated with zanubrutinib confirmed these findings.46
Several studies have been performed to understand the differences between zanubrutinib compared with ibrutinib. Treatment with ibrutinib, but not zanubrutinib, leads to time and dose-dependent shedding of GP1bα and GPIX from the platelet surface by an ADAM17-dependent mechanism, reduced GP1b-IX complex formation and integrin αIIbβ3 surface expression, and decreased thrombus formation under arterial flow.47 These effects may explain differences in bleeding mechanism between the two drugs, although major bleeding remains a concern with zanubrutinib. In distinction from acalabrutinib, zanubrutinib absorbance is not affected by co-administration with gastric acid-reducing agents, including proton-pump inhibitors.34 Zanubrutinib also does not prolong QTc significantly.48 Zanubrutinib has also been studied in patients with moderate to severe hepatic impairment, and although no formal dosing guidelines exist, there was only a single serious adverse event.35 Additionally, unlike ibrutinib,49 zanubrutinib does not inhibit ITK, which has been shown to decrease NK cell cytotoxicity.50 This may lead to less antagonism of anti-CD20 monoclonal antibodies and provide the rationale for further study of these combinations.
The ongoing Phase 3 ALPINE trial (NCT03734016) and will compare treatment with ibrutinib to zanubrutinib for patients with relapsed/refractory CLL and will provide a head to head comparison of the two drugs.48 Early results from a similar trial in patients with previously treated Waldenstrom’s Macroglobulinemia (ASPEN trial) demonstrated higher rates of CR and very good partial responses (VGPR) in patient’s treated with zanubrutinib (28%) compared to ibrutinib (19%), though these difference were not statistically significant. Importantly, the rates of atrial fibrillation, hemorrhage, and major hemorrhage were lower in patients treated with zanubrutinib, though rates of both neutropenia and febrile neutropenia were higher with zanubrutinib.
Based on the available data, we believe that zanubrutinib will become part of the CLL treatment algorithm as both a monotherapy and in combination in the future if it receives FDA approval. While response rates will likely be similar between zanubrutinib and ibrutinib in CLL, a comparison of the toxicity profiles will help clarify if certain patient subgroups (eg, cardiac comorbidities) may benefit most from treatment with zanubrutinib. There is no robust treatment sequencing data available for zanubrutinib at this time, but it is likely to be active in patients after progression on venetoclax based on data for available for ibrutinib.51,52 As it also binds to Cys481, it is less likely to be effective in patients who progress on ibrutinib as Cys481 mutations are a common resistance mechanism and we would not recommend its use for this patient subgroup.53 Early results from a phase 2 trial treated patients with CLL with zanubrutinib who were intolerant to ibrutinib demonstrated limited recurrence of AEs, signaling another patient population likely to benefit from zanubrutinib, though follow up for efficacy is short.54 Zanubrutinib can be combined with other targeted agents due to its favorable side effect profile (eg, venetoclax and obinutuzumab) in hopes of attaining uMRD and can provide another time-limited treatment option if FDA approved. Ongoing clinical trials will help inform our use of zanubrutinib and results are eagerly awaited (Table 1).
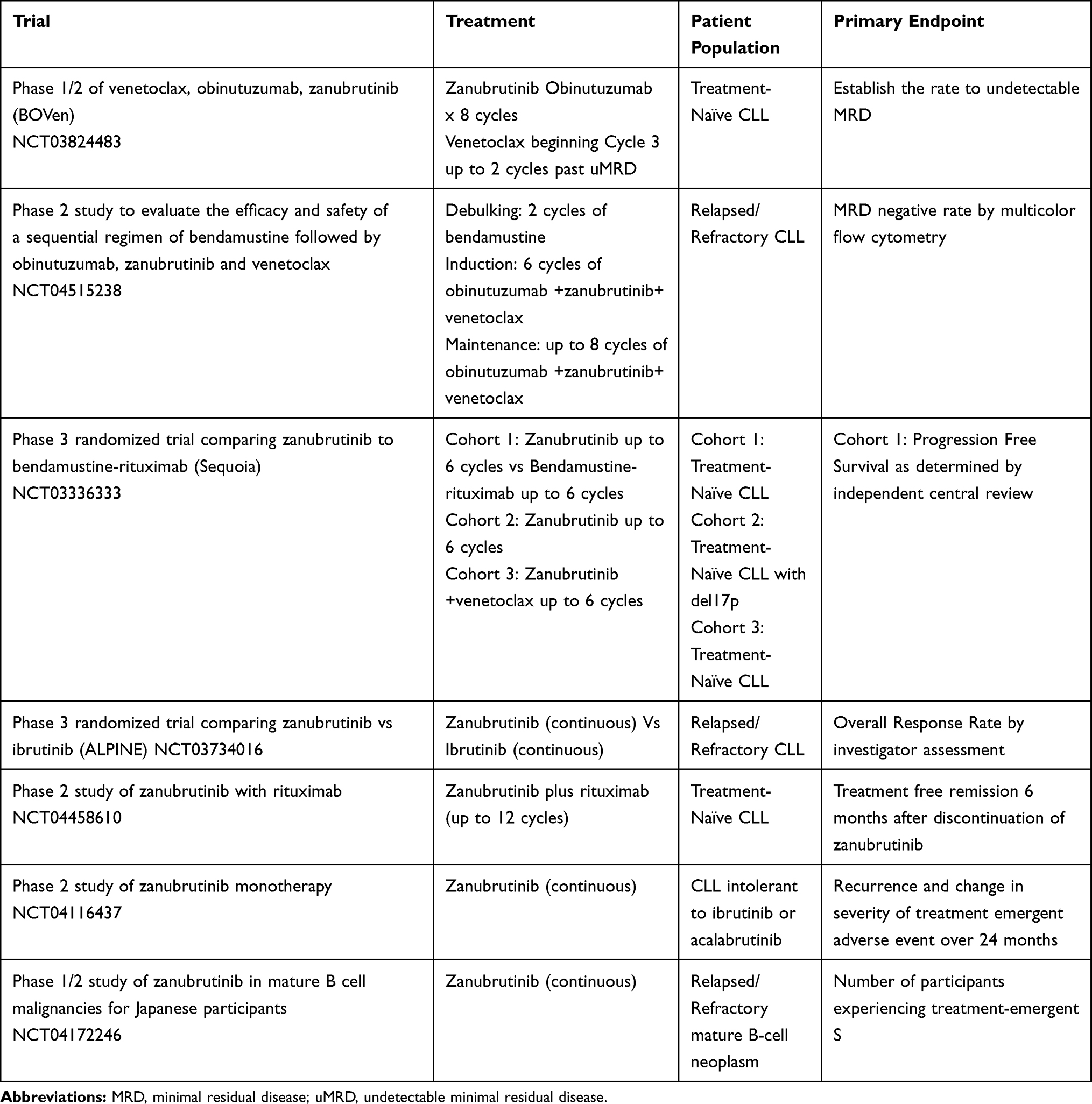 |
Table 1 Ongoing Clinical Trials with Zanubrutinib in CLL |
Conclusions
Zanubrutinib is a second generation BTK inhibitor with an overall favorable safety profile. To date, there have been few episodes of major bleeding or arrhythmia seen in treated patients with CLL. Response rates are comparable to other BTK inhibitors, and zanubrutinib can be safely combined with venetoclax and/or obinutuzumab. These combinations have demonstrated deep responses with many patients attaining uMRD. While further studies and long-term follow-up is necessary to determine if responses are durable, zanubrutinib provides another exciting therapeutic option for patients with CLL.
Disclosure
Dr Joanna M Rhodes reports grants from Conquer Cancer Foundation, during the conduct of the study; personal fees from Pharmacyclics, AstraZeneca, Verastem, and Abbvie/Genentech, outside the submitted work. Dr Anthony R Mato reports grants and/or personal fees from TG Therapeutics, Loxo, Sunesis, Genentech, Abbvie, J and J, Pharmacyclics, DTRM, Octopharma, Aprea, Genmab, Nurix, and Beigene, during the conduct of the study; grants, personal fees from LOXO, TG Therapeutics, AZ, PCYC, J and J, Sunesis, DTRM, Genentech, Nurix, and Genmab, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Hallek M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am J Hematol. 2019;94(11):1266–1287. doi:10.1002/ajh.25595
2. Hallek M, Fischer K, Fingerle-Rowson G, et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet (London, England). 2010;376(9747):1164–1174. doi:10.1016/S0140-6736(10)61381-5
3. Keating MJ, O’Brien S, Albitar M, et al. Early results of a chemoimmunotherapy regimen of fludarabine, cyclophosphamide, and rituximab as initial therapy for chronic lymphocytic leukemia. J Clin Oncol. 2005;23(18):4079–4088. doi:10.1200/JCO.2005.12.051
4. Fischer K, Cramer P, Busch R, et al. Bendamustine combined with rituximab in patients with relapsed and/or refractory chronic lymphocytic leukemia: a multicenter Phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2011;29(26):3559–3566. doi:10.1200/JCO.2010.33.8061
5. Fischer K, Cramer P, Busch R, et al. Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2012;30(26):3209–3216. doi:10.1200/JCO.2011.39.2688
6. Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369(1):32–42. doi:10.1056/NEJMoa1215637
7. Yang W-C, Collette Y, Nunès JA, Olive D. Tec kinases: a family with multiple roles in immunity. Immunity. 2000;12(4):373–382. doi:10.1016/S1074-7613(00)80189-2
8. Arana E, Harwood NE, Batista FD. Regulation of integrin activation through the B-cell receptor. J Cell Sci. 2008;121(14):2279–2286. doi:10.1242/jcs.017905
9. Rhodes J, Mato A, Sharman JP. Monitoring and management of toxicities of novel B cell signaling agents. Curr Oncol Rep. 2018;20(6):49. doi:10.1007/s11912-018-0694-x
10. Burger JA, Chiorazzi N. B cell receptor signaling in chronic lymphocytic leukemia. Trends Immunol. 2013;34(12):592–601. doi:10.1016/j.it.2013.07.002
11. Dimopoulos MA, Tedeschi A, Trotman J, et al. Phase 3 trial of ibrutinib plus rituximab in waldenström’s macroglobulinemia. N Engl J Med. 2018;378(25):2399–2410. doi:10.1056/NEJMoa1802917
12. Noy A, de Vos S, Thieblemont C, et al. Targeting Bruton tyrosine kinase with ibrutinib in relapsed/refractory marginal zone lymphoma. Blood. 2017;129(16):2224–2232. doi:10.1182/blood-2016-10-747345
13. Burger JA, Tedeschi A, Barr PM, et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med. 2015;373(25):2425–2437. doi:10.1056/NEJMoa1509388
14. Shanafelt TD, Wang XV, Kay NE, et al. Ibrutinib–rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med. 2019;381(5):432–443. doi:10.1056/NEJMoa1817073
15. Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N Engl J Med. 2018;379(26):2517–2528. doi:10.1056/NEJMoa1812836
16. Byrd JC, Brown JR, O’Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371(3):213–223. doi:10.1056/NEJMoa1400376
17. O’Brien S, Jones JA, Coutre SE, et al. Ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia with 17p deletion (RESONATE-17): a phase 2, open-label, multicentre study. Lancet Oncol. 2016;17(10):1409–1418. doi:10.1016/S1470-2045(16)30212-1
18. Wang ML, Blum KA, Martin P, et al. Long-term follow-up of MCL patients treated with single-agent ibrutinib: updated safety and efficacy results. Blood. 2015;126(6):739–745. doi:10.1182/blood-2015-03-635326
19. Mato AR, Nabhan C, Thompson MC, et al. Toxicities and outcomes of 616 ibrutinib-treated patients in the United States: a real-world analysis. Haematologica. 2018;103(5):874–879. doi:10.3324/haematol.2017.182907
20. Mato AR, Roeker LE, Allan JN, et al. Outcomes of front-line ibrutinib treated CLL patients excluded from landmark clinical trial. Am J Hematol. 2018;93:1394–1401. doi:10.1002/ajh.25261
21. Brown JR, Moslehi J, O’Brien S, et al. Characterization of atrial fibrillation adverse events reported in ibrutinib randomized controlled registration trials. Haematologica. 2017;102(10):1796–1805. doi:10.3324/haematol.2017.171041
22. Farooqui M, Valdez J, Soto S, Bray A, Tian X, Wiestner A. Atrial fibrillation in CLL/SLL patients on ibrutinib. Blood. 2015;126(23):2933. doi:10.1182/blood.V126.23.2933.2933
23. Guha A, Derbala MH, Zhao Q, et al. Ventricular arrhythmias following ibrutinib initiation for lymphoid malignancies. J Am Coll Cardiol. 2018;72(6):697–698. doi:10.1016/j.jacc.2018.06.002
24. Caron F, Leong DP, Hillis C, Fraser G, Siegal D. Current understanding of bleeding with ibrutinib use: a systematic review and meta-analysis. Blood Adv. 2017;1(12):772–778. doi:10.1182/bloodadvances.2016001883
25. Lipsky AH, Farooqui MZ, Tian X, et al. Incidence and risk factors of bleeding-related adverse events in patients with chronic lymphocytic leukemia treated with ibrutinib. Haematologica. 2015;100(12):1571–1578. doi:10.3324/haematol.2015.126672
26. Caldeira D, Alves D, Costa J, Ferreira JJ, Pinto FJ, Bender R. Ibrutinib increases the risk of hypertension and atrial fibrillation: systematic review and meta-analysis. PLoS One. 2019;14(2):e0211228. doi:10.1371/journal.pone.0211228
27. Rhodes JM, LoRe VA, Mato AR, et al. Ibrutinib-associated arthralgias/myalgias in patients with chronic lymphocytic leukemia: incidence and impact on clinical outcomes. Clin Lymphoma Myeloma Leuk. 2020;20(7):438–444.e431. doi:10.1016/j.clml.2020.02.001
28. Stephens DM, Byrd JC. How I manage ibrutinib intolerance and complications in patients with chronic lymphocytic leukemia. Blood. 2019;133(12):1298–1307. doi:10.1182/blood-2018-11-846808
29. Guo Y, Liu Y, Hu N, et al. Discovery of zanubrutinib (BGB-3111), a novel, potent, and selective covalent inhibitor of bruton’s tyrosine kinase. J Med Chem. 2019;62(17):7923–7940. doi:10.1021/acs.jmedchem.9b00687
30. Harrington BK, Gulrajani M, Covey T, et al. ACP-196 is a second generation inhibitor of Bruton Tyrosine Kinase (BTK) with enhanced target specificity. Blood. 2015;126(23):2908. doi:10.1182/blood.V126.23.2908.2908
31. Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzumab for treatment-naive chronic lymphocytic leukaemia (ELEVATE-TN): a randomised, controlled, phase 3 trial. Lancet. 2020;395(10232):1278–1291. doi:10.1016/S0140-6736(20)30262-2
32. Ghia P, Pluta A, Wach M, et al. ASCEND: phase III, randomized trial of acalabrutinib versus idelalisib plus rituximab or bendamustine plus rituximab in relapsed or refractory chronic lymphocytic leukemia. J Clin Oncol. 2020;38(25):2849–2861. doi:10.1200/JCO.19.03355
33. Song Y, Zhou K, Zou D, et al. Treatment of patients with relapsed or refractory mantle–cell lymphoma with zanubrutinib, a selective inhibitor of bruton’s tyrosine kinase. Clin Cancer Res. 2020;26(16):4216–4224. doi:10.1158/1078-0432.CCR-19-3703
34. Tam CS, Trotman J, Opat S, et al. Phase 1 study of the selective BTK inhibitor zanubrutinib in B-cell malignancies and safety and efficacy evaluation in CLL. Blood. 2019;134(11):851–859. doi:10.1182/blood.2019001160
35. Ou YC, Preston RA, Marbury TC, et al. A phase 1, open-label, single-dose study of the pharmacokinetics of zanubrutinib in subjects with varying degrees of hepatic impairment. Leuk Lymphoma. 2020;1–9.
36. Xu W, Yang S, Zhou K, et al. Treatment of relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma with the BTK inhibitor zanubrutinib: phase 2, single-arm, multicenter study. J Hematol Oncol. 2020;13(1):48. doi:10.1186/s13045-020-00884-4
37. Tam CS, Robak T, Ghia P, et al. Efficacy and safety of zanubrutinib in patients with treatment-naive Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL) with Del(17p): initial results from arm C of the sequoia (BGB-3111-304) trial. Blood. 2019;134(Supplement_1):499. doi:10.1182/blood-2019-125394
38. Tam CS, Robak T, Ghia P, et al. Zanubrutinib monotherapy for patients with treatment naïve chronic lymphocytic leukemia and 17p deletion. Haematologica. 2020. doi:10.3324/haematol.2020.259432
39. Brown JR, Robak T, Ghia P, et al. Efficacy and safety of zanubrutinib in patients with Treatment-Naïve (TN) Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL) with del(17p): follow-up results from arm C of the SEQUOIA (BGB-3111-304) trial. Blood. 2020;136(Supplement 1):11–12. doi:10.1182/blood-2020-134280
40. Tam CS, Flinn IW, Tedeschi A, et al. Zanubrutinib in combination with venetoclax for patients with treatment-naïve chronic lymphocytic leukemia or small lymphocytic lymphoma and del(17p): arm D of the SEQUOIA (BGB-3111-304) trial. Blood. 2020;136(Supplement 1):24–25. doi:10.1182/blood-2020-134179
41. Moreno C, Greil R, Demirkan F, et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in first-line treatment of chronic lymphocytic leukaemia (iLLUMINATE): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(1):43–56. doi:10.1016/S1470-2045(18)30788-5
42. Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med. 2019;380(23):2225–2236. doi:10.1056/NEJMoa1815281
43. Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med. 2014;370(12):1101–1110. doi:10.1056/NEJMoa1313984
44. Tam CS, Quach H, Nicol A, et al. Zanubrutinib (BGB-3111) plus obinutuzumab in patients with chronic lymphocytic leukemia and follicular lymphoma. Blood Adv. 2020;4(19):4802–4811. doi:10.1182/bloodadvances.2020002183
45. Soumerai JD, Mato AR, Carter J, et al. Initial results of a multicenter, investigator initiated study of MRD driven time limited therapy with zanubrutinib, obinutuzumab, and venetoclax. J Clin Oncol. 2020;38(15_suppl):8006. doi:10.1200/JCO.2020.38.15_suppl.8006
46. Tam CS, Opat S, Zhu J, et al. PS1159 pooled analysis of safety data from monotherapy studies of the bruton tyrosine kinase (Btk) inhibitor, zanubrutinib (BGB-3111), in B-cell malignancies. HemaSphere. 2019;3(S1):526. doi:10.1097/01.HS9.0000562920.26603.5b
47. Dobie G, Kuriri FA, Omar MMA, et al. Ibrutinib, but not zanubrutinib, induces platelet receptor shedding of GPIb-IX-V complex and integrin alphaIIbbeta3 in mice and humans. Blood Adv. 2019;3(24):4298–4311. doi:10.1182/bloodadvances.2019000640
48. Hillmen P, Brown JR, Eichhorst BF, et al. ALPINE: zanubrutinib versus ibrutinib in relapsed/refractory chronic lymphocytic leukemia/small lymphocytic lymphoma. Future Oncol. 2020;16(10):517–523. doi:10.2217/fon-2019-0844
49. Kohrt HE, Sagiv-Barfi I, Rafiq S, et al. Ibrutinib antagonizes rituximab-dependent NK cell–mediated cytotoxicity. Blood. 2014;123(12):1957–1960. doi:10.1182/blood-2014-01-547869
50. Flinsenberg TWH, Tromedjo CC, Hu N, et al. Differential effects of BTK inhibitors ibrutinib and zanubrutinib on NK-cell effector function in patients with mantle cell lymphoma. Haematologica. 2020;105(2):e76–e79. doi:10.3324/haematol.2019.220590
51. Jones JA, Mato AR, Wierda WG, et al. Venetoclax for chronic lymphocytic leukaemia progressing after ibrutinib: an interim analysis of a multicentre, open-label, phase 2 trial. Lancet Oncol. 2018;19(1):65–75. doi:10.1016/S1470-2045(17)30909-9
52. Mato AR, Hill BT, Lamanna N, et al. Optimal sequencing of ibrutinib, idelalisib, and venetoclax in chronic lymphocytic leukemia: results from a multi-center study of 683 patients. Ann Oncol. 2017;28:1050–1056. doi:10.1093/annonc/mdx031
53. Woysach JA, Ruppert AS, Guinn D, et al. BTKC481S-mediated resistance to ibrutinib in chronic lymphocytic leukemia. J Clin Oncol. 2017;35(13):1437–1443. doi:10.1200/JCO.2016.70.2282
54. Shadman M, Sharman JP, Levy MY, et al. Phase 2 study of zanubrutinib in patients with relapsed/refractory B-cell malignancies intolerant to ibrutinib/acalabrutinib. Blood. 2020;136(Supplement 1):51–52. doi:10.1182/blood-2020-134621
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.