")
Back to Journals » International Journal of Women's Health » Volume 16
Women Health Literacy and Associated Factors on Women and Child Health Care in Ilu Ababor Public Health Facilities, Ethiopia
Authors Jiregna B , Amare M, Dinku M, Nigatu D , Desalegn D
Received 1 November 2023
Accepted for publication 22 January 2024
Published 26 January 2024 Volume 2024:16 Pages 143—152
DOI https://doi.org/10.2147/IJWH.S443198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Bikila Jiregna,1,* Mesganew Amare,2,* Megersa Dinku,3,* Desalegn Nigatu,3,* Defaru Desalegn4,*
1Department of Midwifery, Mattu University, Mattu town, Oromia, Ethiopia; 2Department of Midwifery, Jimma University, Jimma Town, Oromia, Ethiopia; 3Department of Nursing, Mattu University, Mattu town, Oromia, Ethiopia; 4Department of Psychiatry, Mattu University, Mattu town, Oromia, Ethiopia
*These authors contributed equally to this work
Correspondence: Bikila Jiregna, Tel +251917724156, Email [email protected]; [email protected]
Background: Maternal health literacy (MHL) is the ability of mothers to obtain, interpret, appraise, and apply women and child health information that contributes to a reduction in mortality among mothers and children. This is an important concern since a woman’s health during pregnancy may be her first interaction with the healthcare system, and a woman’s comprehension of health information has a direct impact on her unborn child’s growth throughout the process of conception.
Aim: Assess the degree of maternal health literacy and related factors in women’s and children’s health care among mothers whose children have received basic immunizations at the public healthcare facilities in Ilu Abba Boor.
Methods and Materials: A cross-sectional study was carried out in the facility between December 2021 and January 2022. Investigators trained supervisors and data collectors for five days before data collection. Through basic random sampling, 411 mothers whose children had received the minimum set of vaccinations from health facilities in the Ilu Ababor zone of Oromia, Ethiopia, were chosen. Face-to-face interviews were used to gather the data, which were then imported into Epidata 4.1 and exported to SPSS. The factors associated with maternal health literacy in maternal and child healthcare were identified through the application of descriptive statistics, bivariate analysis, and multivariable logistic regression analyses. The findings are displayed in the form of graphs, tables, and figures.
Results: This study had a 100% response rate when 411 participants were invited to participate. The mean maternal health literacy score was 28.5± 10.3. Most of the women (293 [71.3%]) had inadequate health literacy levels while 118 (28.7%) had adequate. The multivariate analysis’s findings indicated that the rate of adequate maternal health literacy was 12.2 times higher among urban women than among rural ones (AOR=12.2 [5.34, 24.48]). Women who gave birth vaginally were 0.24 times less likely to have adequate maternal health literacy than women who had a caesarean section (AOR=0.24 [0.112, 0.503]). Mothers who had four or more prenatal care follow-ups were found to have sufficient maternal health literacy higher than those who had just one (AOR=0.23[0.095, 0.556]), two (AOR=0.26[0.138, 0.307]), and three times (0.14{0.108, 0.167]) antenatal care contacts.
Discussion and Recommendation: This study shows that inadequate maternal health literacy affects the healthcare of mothers and children. Given the significance of health literacy for women’s health, national health authorities ought to develop more educational initiatives aimed at raising health literacy rates and empowering women who are of reproductive age.
Keywords: maternal health literacy, women and child health care
Introduction
The ability of mothers to access, comprehend, evaluate, and apply information about mother and child health is known as maternal health literacy (MHL). MHL helps to reduce the rates of maternal and infant mortality,1,2 which in turn helps to achieve SDGs 3 (good health and well-being: lowering the maternal and child mortality ratio) and 2 (zero hunger: reducing underweight and stunting among young children).3 Maternal health literacy has the potential to influence women’s motivation, comprehension, and utilization of information in ways that support and preserve their own and their children’s health, according to Renkert and Nutbeam. To guarantee healthy maternity and pregnancy outcomes, maternal health literacy and cognitive skills are necessary. According to Kohan et al, these include the capacity to identify risk factors and implement healthier lifestyles and improved nutrition during pregnancy.
Pregnancy may be a woman’s first experience with the healthcare system and her health status, so maternal health literacy is important. Additionally, a mother’s comprehension of health information directly affects her unborn child before conception, during pregnancy, and during the formative years.4 Previous studies conducted in Nigeria have discovered an association between MHL, pregnancy outcomes,5 and the nutritional status of children.6 It was suggested by another Indian study that “initiatives targeting health literacy could improve vaccination coverage”7 that higher MHL was independently correlated with higher childhood immunization rates.
The study conducted in five provinces of Iran revealed that, among the participants, 28.1% had adequate health literacy, 15.3% had borderline health literacy, and 56.6% had deficient health literacy.8 According to a study on pregnant patients sent to Tehran, Iran’s healthcare facilities, 30% and 23.6% of the participants, respectively, had low and borderline health literacy levels.9 44% of women in research on Siberian women who were referred to medical facilities in Russia had inadequate health literacy levels, according to the study’s findings.10
One’s capacity to manage chronic illnesses and take care of oneself is impacted by health literacy. In Ethiopia, research indicates that women with low educational status, little media exposure, and low community women’s literacy had lower rates of early ANC initiation. These findings are related to the implications of women’s literacy in various ways.11 Women with low literacy are more likely than those with high literacy to experience physical violence as norms and positive attitudes, according to another study conducted in Ethiopia.12 A subsequent study revealed that mothers in Ethiopia who were illiterate had a lower likelihood than mothers who were literate of giving their children all four types of vaccinations.13
Maternal health literacy is a significant issue for two reasons: first, a woman’s pregnancy may be her first encounter with the healthcare system; and second, a woman’s health and her comprehension of health information before, during, and during the years of growth and development can have a direct impact on the child. This study’s main goals were to ascertain the maternal health literacy levels regarding mother and child health care in the primary public health facilities under investigation, as well as the factors that impact women’s MHL. Developing understanding of MHL aids in increasing MHL awareness. Policy makers may be able to create more focused interventions in response to the factors pertaining to MHL.
Methods and Materials
Study Area
This study was conducted in the Iluababor zone, which is located in the Oromia regional state of Ethiopia. Mettu is the capital town of the zone and is located 600 km from Addis Ababa in the south-western region of Ethiopia. This zone had a total population of 934,783, of which 453,536 were female and 481,247 male. One referral hospital, one primary hospital, 41 health centers, and 280 health posts were found in this zone. According to the 2020 Zonal Report, 23,392 children were vaccinated. Based on this, the average number of children vaccinated monthly is 1949. The selected thirteen health facilities accounted for 627 children based on the average number of children vaccinated monthly. The study was conducted between December 2021 and January 2022. This study used an institution-based cross-sectional study design.
Population
Every mother whose children fall within the age range where basic vaccinations are administered in the designated health facilities during the study period.
Inclusion Criteria
Every woman whose children are within the age range for which they should receive a basic immunization.
Sample Size and Sampling Procedure
The following assumptions were taken into account while determining the sample size using a single population proportion formula: a 95% confidence interval, a 0.05 margin of error, and a 0.5 proportion of maternal health literacy because no prior research has been done in Ethiopia. Lastly, the total sample size was 411 with a 10% non-response rate.
Thirteen health institutions were chosen at random from this total using the lottery method. Based on the previous year’s report, the average number of women at the thirteen health centers selected had 627 children whose ages were within the range of receiving a basic vaccination within a month. The study participants were selected using a simple random sample method after each health institute was assigned proportionately based on monthly cash flows (Figure 1).
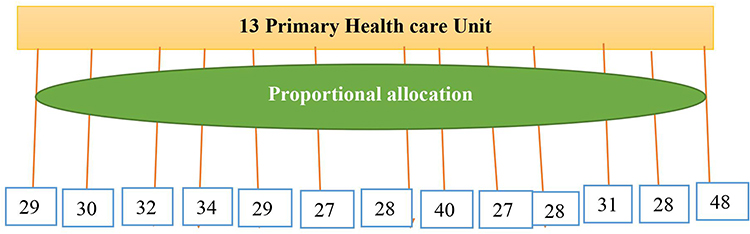 |
Figure 1 The proportional allocation of total participants over the thirteen randomly selected health facilities in Ilu Ababor Zone, Oromia, Ethiopia. |
Variables
Dependent variables
- Level of maternal health literacy
Independent Variables
- Sociodemographic characteristics include age, income, education, ethnicity, religion, and language.
- Obstetric and service-related factors (parity, ANC contact, pregnancy outcomes, children’s nutritional status, child vaccination, exclusive breastfeeding, sources of health-related information, and receiving information)
Operational Definition
Maternal Health Literacy
pertains to a mother’s capacity to obtain, understand, appraise, and apply information regarding maternal and child healthcare throughout her pregnancy, childbirth, and postpartum period. Particular emphasis is placed on important practices such as ANC visits, childbirth, and postpartum care at medical facilities, as well as nutrition and immunization, per WHO guidelines and the National Strategic Action Plan.14,15
Measurement of Health Literacy
A 4-point Likert scale was used to grade each item to determine MHL (4 = extremely difficult, 3 = difficult, 2 = easy, and 1 = very easy). The lowest mean score that could be obtained was 1, and the maximum possible score was 4. Based on their unique index ratings, each person’s mean of all participating items was determined. The formula used to normalize the health literacy indices, which ranged from 0 to 50, was index = (mean-1)*50/3. If 1 was the lowest possible mean value, then the index score’s minimum value was 0, and its highest value was 50. Based on health literacy assessments conducted in Asia and Europe, the cut-off points were classified as “inadequate” (0–33) and “Adequate (33–50)”.16,17
Data Collection Tool and Method
There is no particular tool for MHL, however, it has been measured in other nations,2,18 and the Sørensen health literacy model is commonly used in Europe and Asia.18,19 This study’s research tool will be based on a general literacy tool (scoring the capacity to get, comprehend, appraise, judge, and evaluate, as well as apply and use health information) that was modified for use in mental health care.
Three sections were covered by the research tool used to collect data:
- From earlier research, sociodemographic information on age, religion, ethnicity, language, literacy, education, and income.20,21
- ANC visits, the location of birthing, the number of children, food restrictions/taboos, using hotbeds, smoking, and information received variables were adopted from previous studies and may be associated with factors or behaviors.22
- The National Strategic Action Plan and WHO standards were the basis for the development of the MHL questionnaire, which included 49 topics about mother and child health care during pregnancy, labor, and the postpartum period.14,23 The MHL items were modified to fit the format of a sexual reproductive health literacy tool in Laos,20 as well as a health literacy survey instrument in Asia.17 There were fifteen items about information access in it.
To collect data, thirteen research assistants were hired and given training. For five days, they received training in conducting in-person interviews and accurately completing questionnaires. Thirteen data collectors got experience gathering data in medical facilities outside the scope of the study during the training. To prevent duplicate enrolment, the data collectors chose women who would bring their kids for basic vaccinations and made note on their folder. They also made arrangements based on the mothers’ order of service requests, which included randomly selecting moms beforehand.
Data Analysis
The data was entered into Epidata 4.1 and then exported to SPSS 25.0. For descriptive statistics, the arithmetic mean, standard deviation, numbers, and percentages were employed. Important variables for multivariate logistic regression were chosen using bivariate logistic regression. The dependent variables in multiple logistic regressions were the inadequate and appropriate MHL levels, whereas the independent variables were the sociodemographic and important practices of women. When the p-value was less than 0.05, these factors were put forward into the model to calculate the Adjusted Odds Ratio (AOR), 95% confidence interval, and significance level. Both text and tables are used to present the results.
Data Quality Assurance
The questionnaire was suitably constructed, changed, and adjusted. The study tools were initially designed in English, and then, to assure correctness, translations back and forth between English and the regional languages were performed. These instruments’ validity and reliability were verified.
Before the pilot test, the local supervisor contributed to the last edit. At Bunno Bedelle Hospital in the research area, a pilot test of the local language version was conducted under comparable conditions with 20 women whose children had received basic immunizations. Supervisors and data collectors received training. Every day, the lead investigators and supervisor examined and filled out the questionnaires, and the data collectors received supervision. During the data-collecting process, supervisors and primary investigators conducted monitoring and follow-up. The interviewer took notes during the interview and cross-referenced the information with the responses provided by the mothers in their record books, the child’s immunization record, the ANC visits, and the place of labor (if it was at a medical facility).
Results
This study had 411 women in total, yielding a 100.0% response rate. The following are the outcomes.
Socio-Demographic Characteristics
Out of all the participants, 156 (38.0%) belonged to the 24–28 age group, and 142 (34.5%) to the 29–23 age group, with a mean age of 27.63 ±4.27 years. 166 (40.4%) of the participants were Muslims, while 101 (24.6%) were Orthodox. In terms of women’s educational attainment, 96 (23.4%) had a diploma, 124 (30.2%) had finished grade 8, 61 (14.8%) could read and write, and 37 (9%) could not (Table 1).
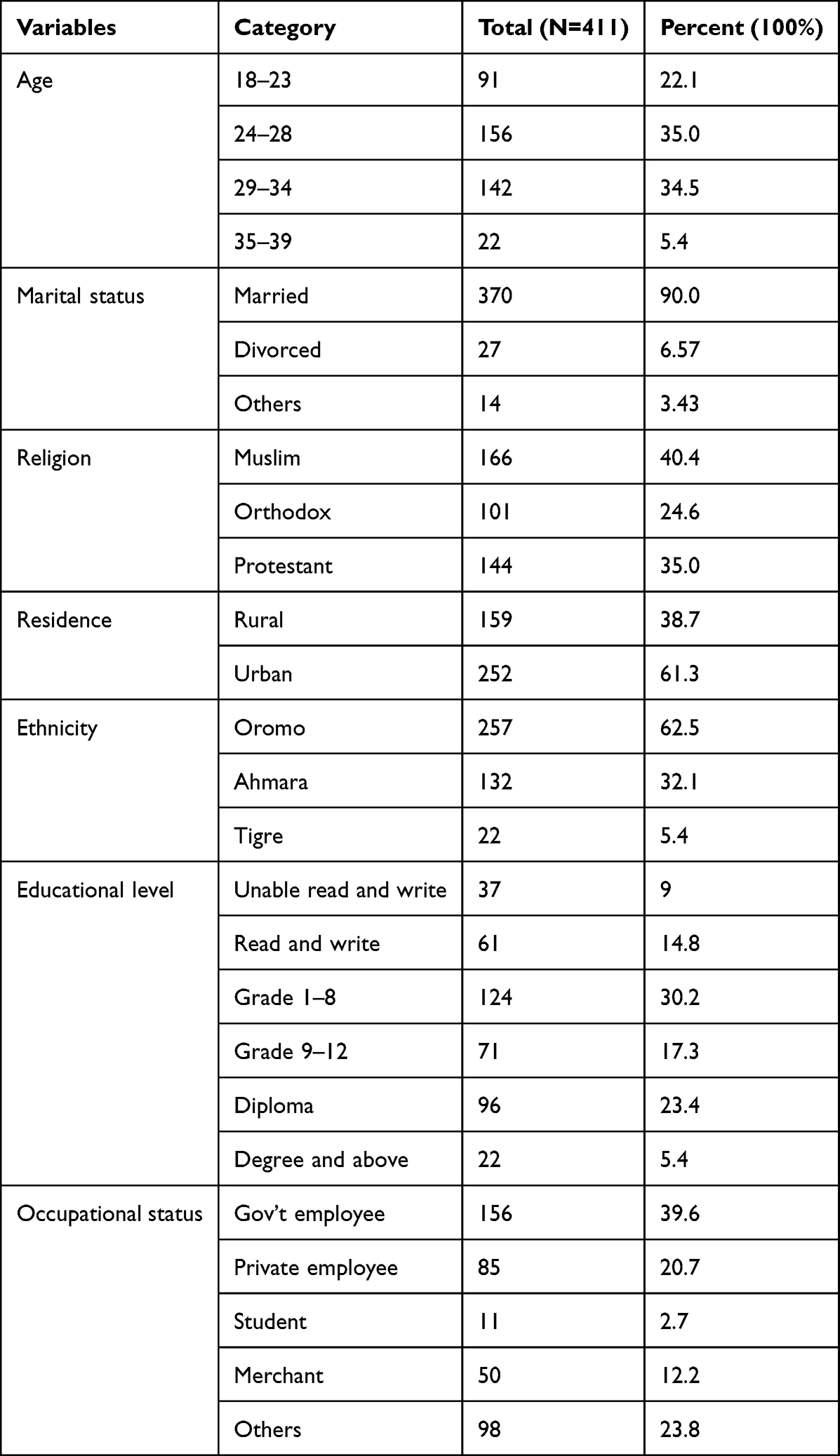 |
Table 1 Socio-Demographic Characteristics of Women at Ilu Abbabor Public Health Facilities, 2022 (N=411) |
Practices of Mothers and Basic Information
Of the total participants more than average, 208 (50.6%) women, had two or three children and 120 (29.2%) had four or more children. 178 (43.3%) women had more than four antenatal care visits during their last childbirth, and 98 (23.8%) had one ANC visit. Most women, 378 (92.0%), gave birth to their last child at a health facility. 359 (87.3%) had given birth vaginally, with 52 (12.7%) giving abdominal delivery. The majority of participants 388 (94.4%) exclusively breastfed their children (Table 2).
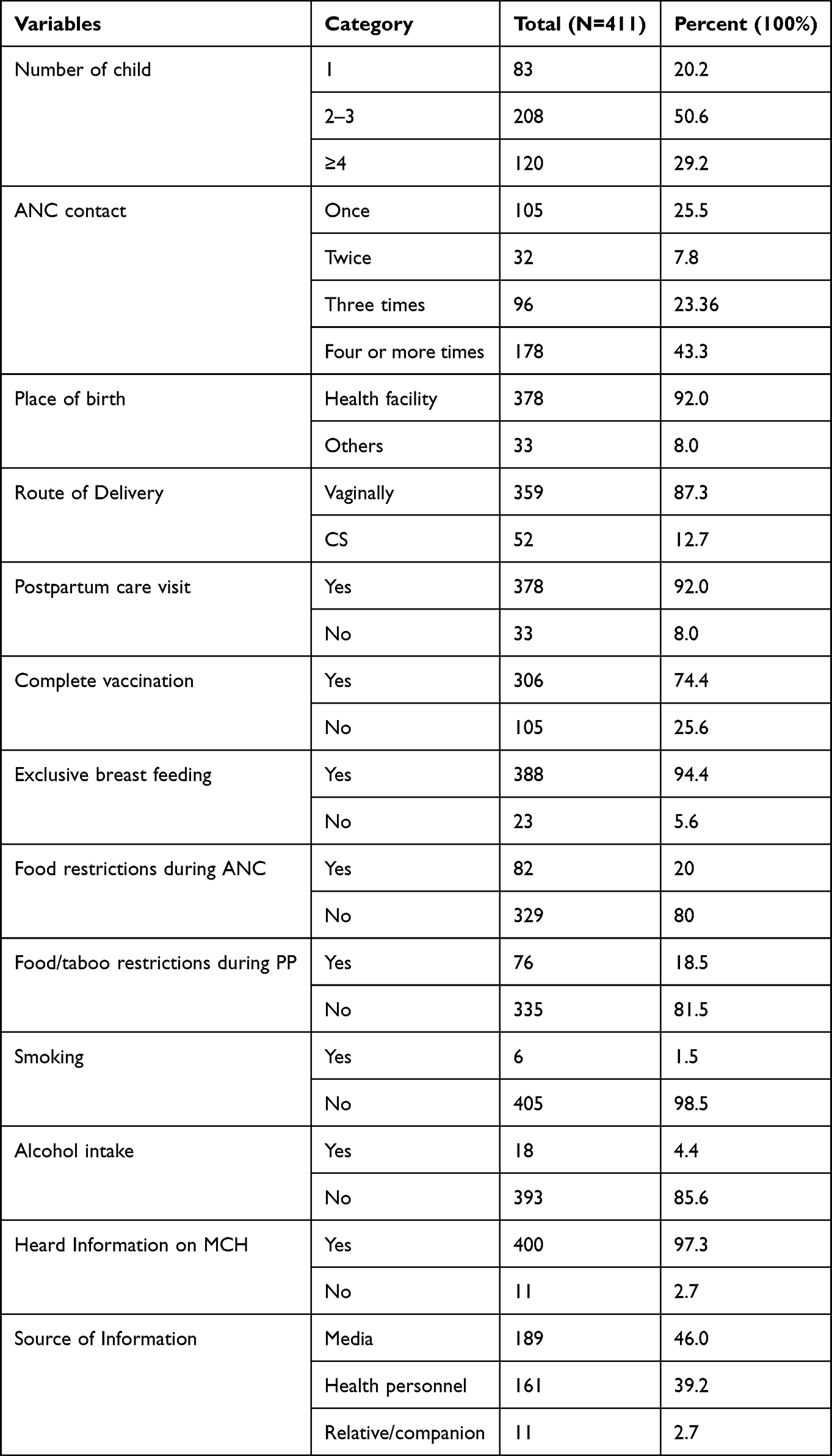 |
Table 2 Practices of Mothers and Basic Information on Maternal and Child Health Care at Ilu Abbabor Public Health Facilities, 2022 (N=411) |
Level of Maternal Health Literacy with Different Dimensions
The mean maternal health literacy score was 28.5±10.3. Most women 293 (71.3%), had inadequate literacy levels and 118 (28.7%) were adequate. 274 (56.0%) women had inadequate access to information on maternal and child health care (Table 3).
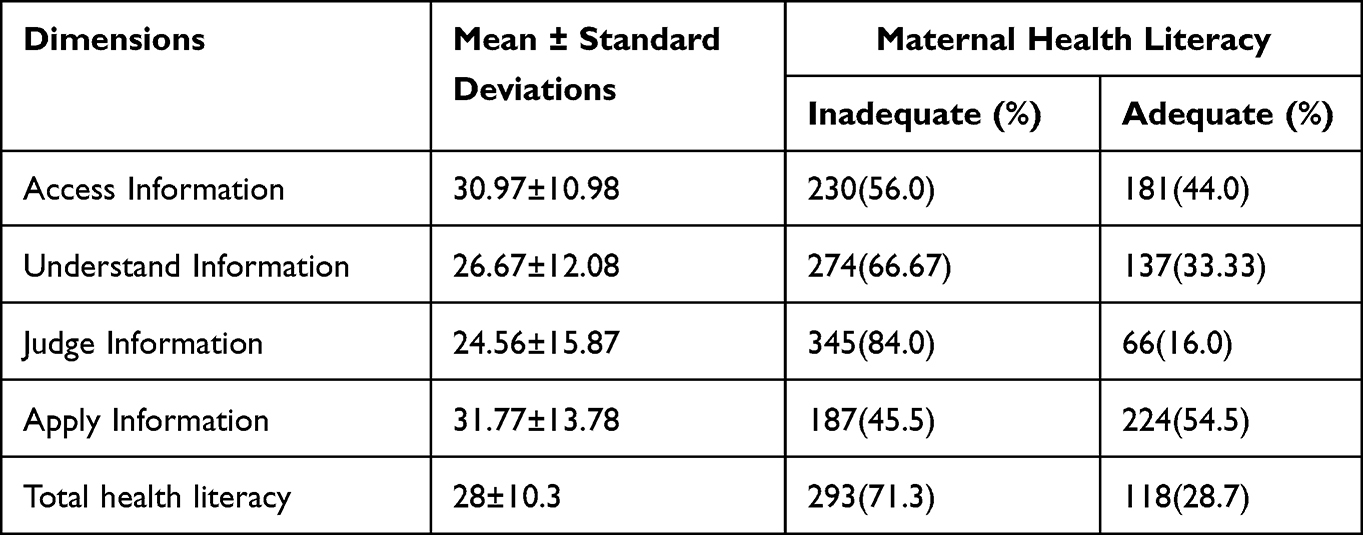 |
Table 3 The Mean Score (Out of 50) and Health Literacy Level in Terms of Health Literacy Dimensions on Mother and Child Health Care Among Women in Ilu Abbabor Public Health Facilities, 2022 (N=411) |
Maternal Health Literacy and Associated Factors
The results of the bivariate analysis showed that maternal health literacy was significantly correlated with sociodemographic variables like age, place of residence, and educational attainment; and practice variables of MCH mothers like the number of children, frequency of follow-up appointments for prenatal care, delivery method and provision of basic child immunization. To account for confounding variables, these significant variables (p-value less than 0.25 in the crude analysis) were added to a multivariate logistic model. In multivariate analysis, variables having a p-value of less than 0.05 were deemed statistically significant, while the remaining variables were disproved.
The results of the multivariate analysis showed that women living in urban areas had a sufficient maternal health literacy rate 12.2 times higher than women living in rural areas (AOR=12.2 [5.34, 24.48]). Compared to women who had a caesarean section, vaginally birthing women were 0.24 times less likely for adequate maternal health literacy (AOR=0.24 [0.112,0.503]). Women who had one antenatal care contact were 0.23 times less likely to have acceptable maternal health literacy than moms who had four or more (AOR=0.23[0.095, 0.556]). Women who complete basic child immunization 0.21 times more likely to for adequate MHL than women with no fully immunized for basic vaccination (AOR=0.21 (0.17, 0.73]) (Table 4).
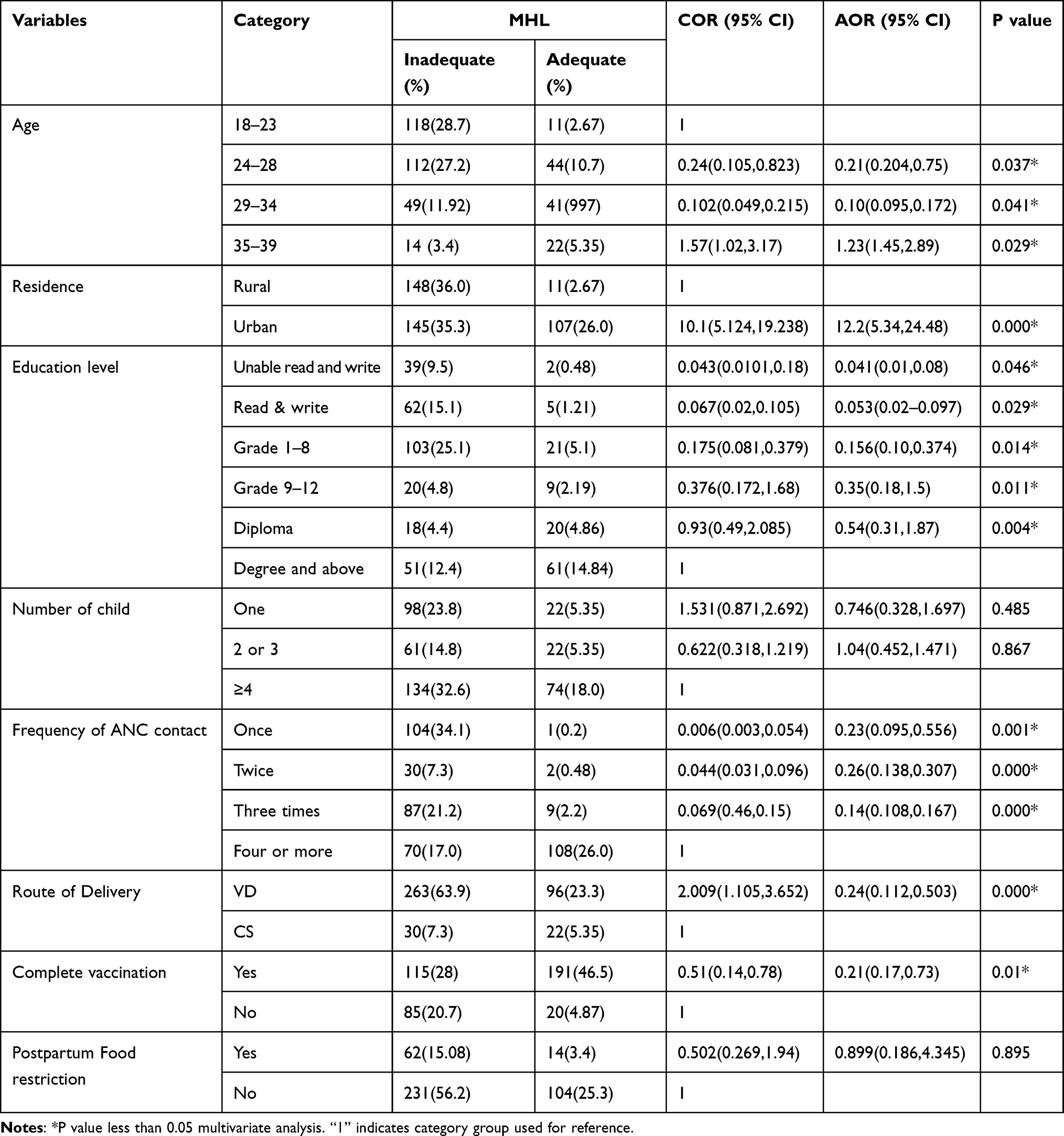 |
Table 4 Bivariate and Multivariate Analysis to Identify Factors Associated with Maternal Health Literacy About Mother and Child Health Care Among Women in Ilu Abbabor Public Health Facilities, 2022 (N=411) |
Discussion
The average maternal health literacy score was 28.5±10.3. Of the women, 293 (71.3%) had low literacy and 118 (28.7%) had adequate literacy. Compared to a study done in Iran, where 98.2% and 61.3% of pregnant women, respectively, had good and adequate MHL levels, the level of maternal health literacy (MHL) in our study is considerably lower.21 This variation may be due to differences in the educational status of the respondents: in the Iranian study, 61% of participants completed high school or higher, whereas in the current study, 54% of participants had no formal education. It may also be due to differences in the study area, as the Iranian study was conducted among women from urban areas, where there is a greater likelihood of acquiring information through media and other sources.21 These figures were greater than those found in Laos, south-eastern Asia, where research found that 80% of expectant mothers had either unsatisfactory or insufficient health.20 According to a study conducted in Vietnam, among other sources of MCH information, family members are crucial for mothers in ethnic minority populations.1 In this survey, however, 46% of women’s information came from the media and 46% from medical professionals.
This research revealed that important predictors of MHL were women’s age, residence, level of education, frequency of ANC visits, method of childbirth, and completion of children’s basic immunizations. The findings showed a direct relationship between maternal health literacy and women’s educational attainment. This shows that compared to women with greater levels of education, illiterate women were less likely to have access to sufficient MHL. These results align with research undertaken in Taiwan24 and Iran.25
Our results also showed a strong correlation between MHL and frequent follow-ups in prenatal care. This outcome is in line with research done in Laos, Southeast Asia.20 This may be the case because women who attended more ANC visits had the chance to speak with medical professionals about issues pertaining to the mother and the newborn, and all of these interventions may have increased MHL.26 In contrast to women who gave birth vaginally, those who underwent abdominal surgery (C-section) were substantially more likely to have appropriate maternal literacy, with regard to this study. The completion of vaccinations was most significantly linked to higher levels of maternal health literacy, while other behaviors—such as smoking, consuming alcohol, and restricting breastfeeding and food taboos during postpartum care—were not correlated with maternal health literacy levels.
This study’s strength is that it’s the first of its kind, so the scientific community may use it as a point of reference. The lack of national and international research to compare the results is one of the study’s limitations. Furthermore, although no research has been done on cause-and-effect reports, this is a cross-sectional study that does not show a cause-and-effect relationship.
Conclusion and Recommendation
This study generally shows that maternal health literacy is low for the purpose of providing healthcare to mothers and children. Health literacy was significantly associated with variables like age, place of residence, educational attainment, frequency of prenatal treatment, mode of delivery, and full series of childhood vaccinations. Nonetheless, there was no correlation found between the level of maternal health literacy and the occupation of women, smoking, alcohol consumption, or exclusive breastfeeding for longer than six months.
More information on maternity and child healthcare, beginning with pre-conception care, should be given by medical experts. Furthermore, there are not many studies, and more is needed especially on health literacy in childbearing age groups, as opposed to married women alone. Local governments ought to concentrate their efforts on setting up adult literacy centers in their individual regions, where women who are ready to have children can get the necessary and pertinent information on being pregnant and giving birth, as well as enhance their reading skills.
Abbreviations
AOR, Adjusted Odds Ratio; ANC, Antenatal Care; CI, Confidence Interval; Km, Kilometer; MCH, Maternal and Child Health; MHL, Maternal Health Literacy; MMR, Maternal Mortality Ratio; OD, Odds Ratio; SDP, Sustainable Development Goal; SPSS, Statistical Packages for Social Science; USA, United States of America; WHO, World Health Organization.
Ethical Consent
The study complies with the ethical principles of the World Medical Association Declaration of Helsinki. Mattu University Institutional Review Board has approved for ethical review and verbal consent process with (reference number: RPG/124/22, date of approval: 23 May, 2022). The data collectors explained the purpose of the study to the participants. The study granted its participants the liberty to withdraw from participation at any point in time and the chance to pose any inquiries they might have about the investigation. All other participant information was kept confidential, including their names.
Acknowledgment
We want to express our sincere gratitude to the Mattu University Research and Technology Transfer Directorate for permitting us to carry out this inquiry. In final remarks, we would like to thank the Ilu Abbabor health bureau for helping us to obtain the data that we needed for this investigation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McKinn S, Linh DT, Foster K, McCaffery K. Distributed health literacy in the maternal health context in Vietnam. Heal Lit Res Pract. 2019;3(1):e31–e42.
2. Smith SA, Carroll LN. Data-driven maternal health literacy promotion and a postscript on its implications. Inform Serv Use. 2017;37:235–252.
3. FDREMoH. The 2017 voluntary national reviews on SDGs of Ethiopia: Government Commitments, National Ownership and Performance Trends. Addis Ababa: National Plan Commission; 2017.
4. Ferguson B. Health literacy and health disparities: the role they play in maternal and child health. Nurs Women’s Health. 2008;12(4):286–298. doi:10.1111/j.1751-486X.2008.00343.x
5. Mojoyinola JK. Influence of maternal health literacy on healthy pregnancy and pregnancy outcomes of Women Attending Public Hospitals in Ibadan, Oyo State, Nigeria. African Res Rev. 2011;5(3):28–39.
6. Mu’awiyyah Babale Sufiyan SS, Bashir AA. Effect of maternal literacy on nutritional status of children under 5 years of age in the Babban-Dodo community Zaria city, Northwest Nigeria. Ann Niger Med. 2013;6(2):61.
7. Johri M, Subramanian SV, Sylvestre M, et al. Child health Association between maternal health literacy and child vaccination in India: a cross-sectional study. J Epidemiol Community Health. 2015;69(9):849–857. doi:10.1136/jech-2014-205436
8. Tehrani Banihashemi SA, Amirkhani MA, Haghdoost AA, et al. Health Literacy and the influencing factors: a study in five provinces of Iran. Strides Dev Med Educ. 2007;4(1):1–9.
9. Ghanbari S, Majlessi F, Ghaffari M, Mahmoodi Majdabadi M. Evaluation of health literacy of pregnant women in urban health centers of Shahid Beheshti Medical University. Daneshvar. 2012;19(97):1–12.
10. Javadzade H, Sharifirad G, Reisi M, Tavassoli ERF. Health literacy among adults of Isfahan, Iran. J Heal Syst Res. 2013;9(5):540–549.
11. Dewau R, Muche A, Fentaw Z, et al. Time to initiation of antenatal care and its predictors among pregnant women in Ethiopia: cox-gamma shared frailty mode. PLoS One. 2021;16(2):e0246349.
12. Deyessa N, Berhane Y, Ellsberg M, Emmelin M, Kullgren G, Högberg U. Violence against women in relation to literacy and area of residence in Ethiopia, Global Health Action. Taylor Fr Gr. 2010;3(1):2070.
13. Lee HY, Oh J, Heo J, et al. Association between maternal literacy and child vaccination in Ethiopia and southeastern India and the moderating role of health workers: a multilevel regression analysis of the Young Lives study. Taylor Fr Gr. 2019;12(1):1581467.
14. World Health Organization. Pregnancy, Childbirth, Postpartum, and Newborn Care: A Guide for Essential Practice.
15. Commitments G, Ownership N. Federal Democratic Republic of Ethiopia The 2017 Voluntary National Reviews on SDGs of Ethiopia: Government Commitments, National Ownership and PerformanceTrends Content; 2017.
16. Ganahl K, Lonska Z S, Pelikan M, Ro FSK. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–1058. doi:10.1093/eurpub/ckv043
17. Duong TV, Aringazina A, Baisunova G. Measuring health literacy in Asia: validation of the HLS-EU-Q47 survey tool in six Asian countries. J Epidemiol. 2017;27(2):80–86. doi:10.1016/j.je.2016.09.005
18. Sørensen K, Van den Broucke S, Fullam J. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Heal. 2012;12(1):80. doi:10.1186/1471-2458-12-80
19. Khorasani EC, Peyman N, Esmaily H. Measuring maternal health literacy in pregnant women referred to the Healthcare Centers of Mashhad, Iran, in 2015. J Midwifery Reprod Health. 2017;6(1):10.
20. Id SP, Essink DR, Wright PE, Jacqueline E, Broerse W, Mayxay M. Maternal health literacy on mother and child health care: a community cluster survey in two southern provinces in Laos. PLoS One. 2021;16(3):1–18.
21. Hakkak HM, Joveini H, Rajabzadeh R, et al. Health literacy level and related factors among pregnant women referring to Bojnord Health Centers in 2017. Int J Pharmaceut Res. 2019;11(1):152–158.
22. Barennes H, Simmala C, Odermatt P. Postpartum traditions and nutrition practices among urban Lao women and their infants in Vientiane, Lao PDR. Eur J Clin Nutr. 2009;63(3):323–333. doi:10.1038/sj.ejcn.1602928
23. FDREMH. National reproductive health strategy 2016–2020; 2016: 13.
24. Lee SY, Tsai TI, Tsai YW, Kuo KN. Health literacy, health status, and healthcare utilization of Taiwanese adults: results from a national survey. BMC Public Heal. 2010;10(1):1–8.
25. Khazaei M, Tehrani H, Vahedian-Shahroodi M, Esmaily H, Taghipour A. Women s Health literacy and its related factors in Mashhad, Iran. J Health Lit. 2021;5(4):9–16.
26. Lori JR, Munro ML, Chuey MR. Use of a facilitated discussion model for antenatal care to improve communication. Int J Nurs Stud. 2016;54:84–94. doi:10.1016/j.ijnurstu.2015.03.018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.