")
Back to Journals » Clinical Optometry » Volume 16
Wear Experiences with Two Soft Contact Lenses for Astigmatism of Different Modalities
Authors Fogt JS , Satiani N, Bickle KM, Wesley G, Patton K
Received 8 December 2023
Accepted for publication 6 March 2024
Published 26 March 2024 Volume 2024:16 Pages 93—100
DOI https://doi.org/10.2147/OPTO.S452132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Mr Simon Berry
Jennifer Swingle Fogt, Nidhi Satiani, Katherine M Bickle, Gina Wesley, Kimberly Patton
College of Optometry, The Ohio State University, Columbus, OH, USA
Correspondence: Jennifer Swingle Fogt, The Ohio State University College of Optometry, 338 West 10th Avenue, Columbus, OH, 43210-1280, USA, Tel +1 614-292-0882, Email [email protected]
Introduction: Patients expect to have excellent vision and comfort when wearing soft contact lenses. The purpose of this study was to compare the wear experiences of participants with astigmatism when wearing a daily disposable soft toric lens to an established, commonly used reusable toric lens.
Methods: In this crossover study, habitual soft toric lens wearers were fit with a daily replacement soft toric lens (delefilcon A) and a reusable, 1-month replacement soft toric lens (comfilcon A) in a randomized order. After 30 days of wear, Visual analog scale (VAS) surveys were used to assess wear experience, including vision and comfort, for overall wear and end-of-day wear. Scores were compared statistically with mixed-effects linear models. Participants also responded to questions about convenience, ease of use, and satisfaction with both lenses and preference questions based upon comfort, vision, and overall performance.
Results: Fifty-nine participants completed the multi-site crossover study. VAS scores [mean(std dev)] for overall quality of vision for the delefilcon A [80.4(16.4)] and comfilcon A [66.8(27.7)] lenses were statistically significant (P=0.002). The difference in the mean overall comfort scores for the delefilcon A lenses [71.6(26.3)] and comfilcon A lenses [63.2(28.9)] was 8.4, which exceeds the establish criteria for clinical significance, although not statistically significant (P=0.08). Overall satisfaction scores were 68.8(26.9) for the delefilcon A and 59.7(30.3) for the comfilcon A lenses (P=0.08). Both lenses provided mean binocular visual acuities better than 20/20 Snellen equivalent. Over half of the participants preferred the delefilcon A lenses based upon comfort, vision, and overall performance. Convenience, ease of use, and satisfaction all scored higher with delefilcon A lenses.
Conclusion: The results of this study show that wear experience with delefilcon A lenses for astigmatism can meet or exceed that of comfilcon A toric lenses while also providing healthy, daily disposable lens wear.
Keywords: soft contact lenses, astigmatism, toric contact lenses, comfort, experience
Introduction
Astigmatism is a common form of ametropia estimated to be found in over 70% of the population by numerous studies.1–3 While astigmatism is generally corrected fully in a spectacle prescription, low amounts of astigmatism often do not require correction when being fit with soft contact lenses. Studies have shown that failing to correct astigmatism above 0.75 diopters can result in eyestrain and decreased visual acuity.4,5 In order to correct astigmatism with soft lens wear, a toric lens design must be used to provide stable vision correction that matches the orientation of the wearer’s prescription.6 Toric soft lens designs used to stabilize lenses vary among lenses available,6 and eyelid interaction with these designs can make lenses with similar prescriptions perform differently on the eye, requiring eye care practitioners to evaluate lens fit for rotation which may require compensation of the axis portion of the prescription in order to optimize vision. This can vary from one lens design to another, and additional factors that vary between lenses, such as lens materials, diameter, wetting agents, and physical properties, also have been shown to play a role in the fact that soft contact lenses are not interchangeable when prescribed.7
Silicon hydrogel lenses are generally favored in contact lens prescribing for their high oxygen permeability that lessen the risk of ocular hypoxia. Wetting agents or surface modifications have been added to silicone hydrogel lenses with the goal of improving wettability and ultimately comfort. Lens replacement schedules can play a role in lens wear experience. Early studies found less lens deposits8 and improved comfort9 when comparing daily disposable lenses to reusable lenses, and soft contact lenses that are replaced daily have been shown to have fewer ocular health complications, including corneal infiltrative events and corneal punctate staining when compared to reusable lenses.10,11
When fitting soft toric lenses, eye care practitioners often fit lenses that they have successfully fit in the past with the goal of achieving optimized vision and a positive wear experience for their patients. As new lenses become available, it is helpful to evaluate the wear experience of these lenses from many perspectives, including subjective impressions of vision, comfort, and satisfaction of lens wear. In the study presented in this manuscript, the wear experience of participants after 1 month of wear of a widely prescribed silicone hydrogel monthly reusable lens (Biofinity® Toric, comfilcon A, Cooper Vision, Pleasanton, CA, USA) is compared to the wear experience after 1 month of wearing a new soft toric daily disposable lens (Dailies TOTAL1® for Astigmatism, delefilcon A, Alcon, Fort Worth, TX, USA). Comfilcon A is a silicone hydrogel material which consists of long silicone chains to make the lens flexible and has no surface treatment.12 Delefilcon A is a silicone hydrogel material that incorporates a gradient change in chemical composition, modulus, and water content between the lens core and the lens surface.13 Both of the study lenses use a modified prism ballast design to stabilize the lenses on the eyes and both have an overall diameter of 14.5mm. The purpose of the study was to compare the wear experience of patients after wearing both of these lenses.
Methods
This crossover study enrolled participants who were habitual wearers of soft toric contact lenses who did not wear either of the study lenses. This study complies with the Declaration of Helsinki and was approved by the Institutional Review Board at The Ohio State University College of Optometry and registered on ClinicalTrials.gov (#NCT05102383) before the study began. All participants completed the informed consent process before participation.
After completing the informed consent process, participants were examined to assure they met all inclusion and exclusion criteria. Distance LogMAR high contrast visual acuity was assessed initially, and this method was used for all vision testing throughout the study. An evaluation of the ocular surface was completed with biomicroscopy. To meet the eligibility criteria of the study, entering distance visual acuity of 20/25 or better with habitual correction was required, and participants could not have active ocular inflammation or infection, an uncontrolled systemic disorder, a change in medication within the last month, or be currently pregnant or lactating. Following a randomization table, eligible participants were fit with either a daily disposable soft contact lens (Dailies TOTAL1® for Astigmatism Contact Lenses, delefilcon A, Alcon, Fort Worth, TX, USA) or a reusable soft contact lens (Biofinity® Toric, comfilcon A, Cooper Vision, Pleasanton, CA, USA). After lens settling for at least ten minutes, Lens fit and high contrast visual acuity was assessed. A visual analog scale (VAS) survey of initial lens impressions with the lenses was then deployed to the participant’s own smart device using REDCap (Research Electronic Data Capture), a secure, web-based software platform hosted at The Ohio State University that is utilized to capture data for research studies.14,15 Each VAS survey was completed by moving a slider along a line to correspond with their impression of each quality on a scale from 0 to 100. The initial quality of vision VAS was anchored with “POOR Quality” at 0 and “EXCELLENT Quality” at 100. The initial comfort VAS was anchored with “POOR Comfort” at 0 and “EXCELLENT Comfort” at 100. The initial satisfaction VAS was anchored with “NOT Satisfied” at 0 and “EXTREMELY Satisfied” at 100. Participants were then dispensed enough lenses needed to complete 30 days of wear. When wearing the reusable lenses, they were dispensed multipurpose solution (Optifree® Puremoist®, Alcon, Fort Worth, TX, USA) and were reminded how to clean and store the lenses properly.
After 1 month of wear, participants returned for Visit 2 wearing the study lenses they had been assigned. Participants completed VAS surveys to assess subjective responses regarding their overall and end of day wear experience with the study lenses they had worn over the past month, including overall quality of vision, stability of vision, comfort, and satisfaction. The VAS surveys were anchored with “POOR” at 0 and “EXCELLENT” at 100. A VAS survey of dryness with the lenses was completed, with anchors of “NO DRYNESS” at 0 and “MAXIMUM DRYNESS” at 100. The Contact Lens Dry Eye Questionnaire (CLDEQ-8) was also completed. High contrast visual acuity with the study lenses, evaluation of the lens fit and rotation of the lenses, and assessments of ocular health were completed. Participants were then fit with the other study lens and lens fit and visual acuity were assessed. After a successful fit, the participant completed the initial impressions VAS survey for the second study lens, and a 30-day supply of those lenses was dispensed.
Participants returned for Visit 3 after 1 month of wear of the second study lens. The VAS surveys of overall and end-of-day wear experience and the CLDEQ-8 were completed. High contrast visual acuity and lens fit, including lens rotation, were assessed. The participant then responded to questions regarding the convenience, ease of use, and satisfaction with each of the study lenses on a 0–10 scale. They also responded to questions about their study lens preferences based on comfort, vision, and overall performance of the two lenses. A diagram of the study visits can be found in Figure 1.
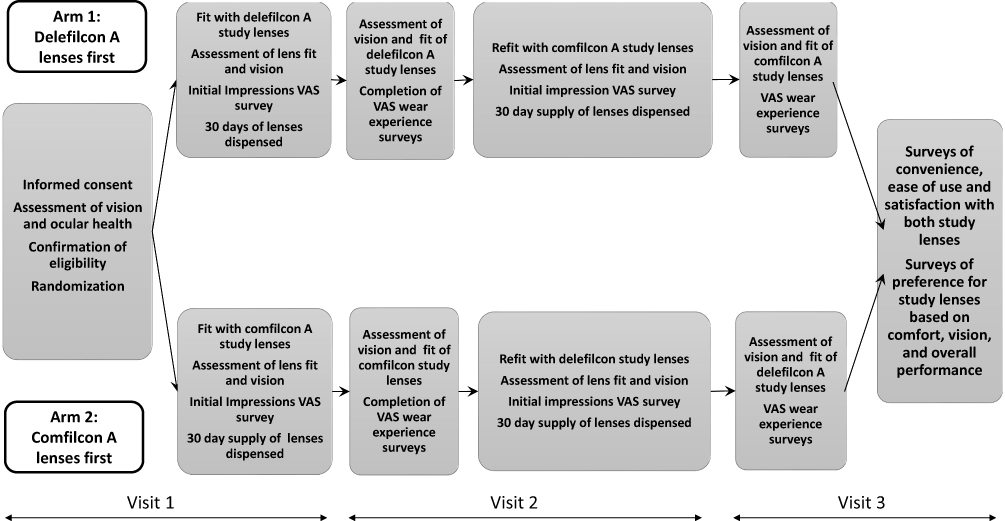 |
Figure 1 Study design. |
The sample size was determined based upon VAS scores of subjective dryness of soft contact from a pilot study, which determined that a sample size of 61 was required for a power of 0.8. All statistical analyses were completed using Minitab® Version 21.3.1 (Minitab LLC, State College, PA). A mixed-effects linear model was used to evaluate differences between the two types of lenses and take into account the randomization order when comparing the initial impression VAS survey questions and the 1-month VAS surveys taken when wearing each lens. Paired t-tests were used to compare visual acuity with each of the study lenses, CLDEQ-8 responses, and the convenience, ease of use, and satisfaction surveys completed at the end of the study. Because there are multiple comparisons made in three of the independent surveys used in this study, Bonferroni correction was used to determine the adjusted alpha values, by dividing the P-value for significance by the number of survey questions in each survey.16 A list of all REDCap surveys used in this study can be found in Table 1.
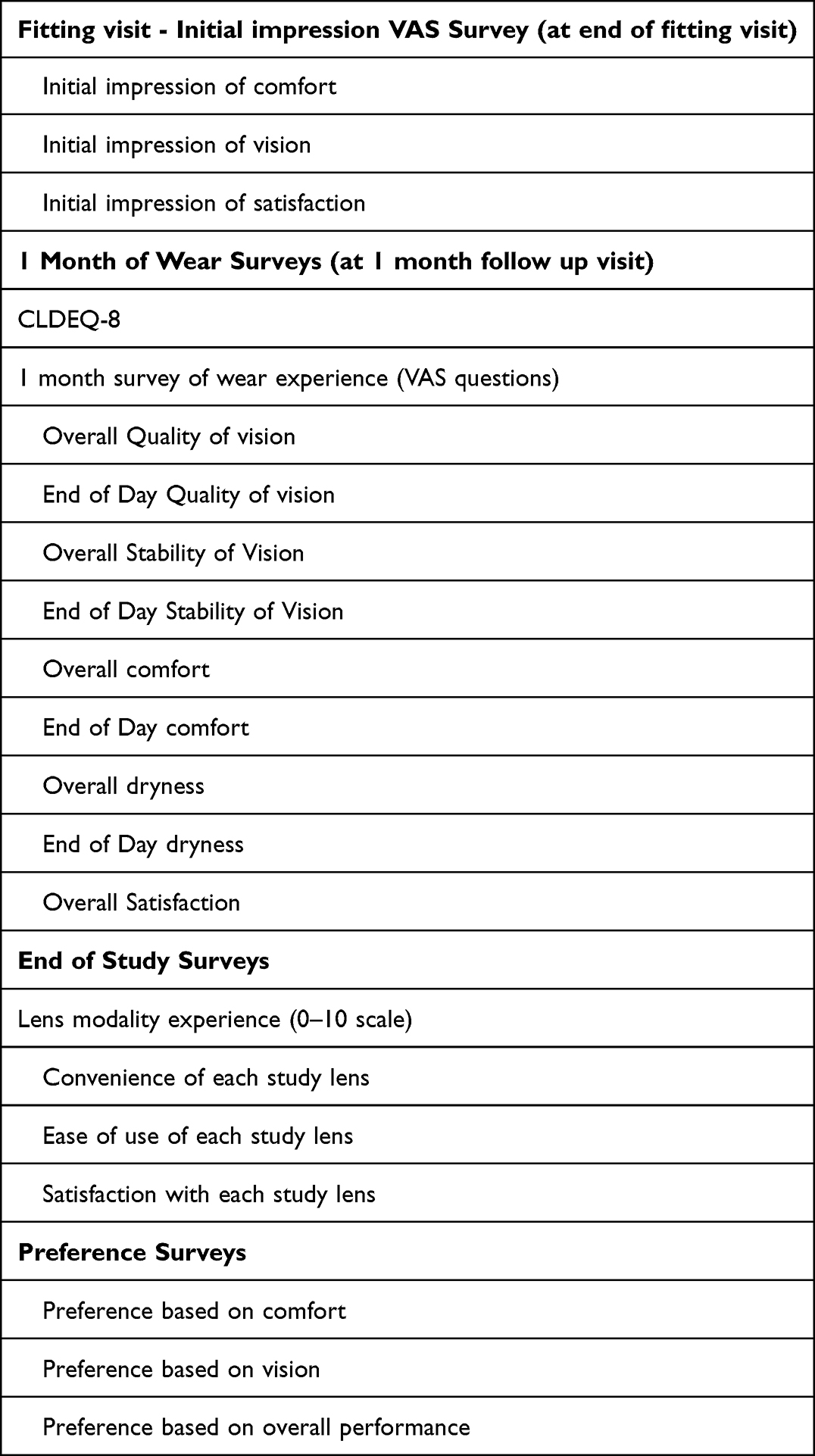 |
Table 1 Surveys Deployed Throughout the Study Using REDCap |
Descriptive statistics of the preference responses are presented.
Results
Sixty-seven subjects completed the informed consent process. Four participants did not meet the inclusion/exclusion criteria and were not eligible to participate. Of the 63 participants enrolled, four exited the study early. Three subjects voluntarily discontinued the study before completing all study visits due to lens discomfort. These subjects were wearing the daily disposable study lenses when they discontinued and did not complete 30 days of wear or completion of surveys. The other early exit was due to an adverse event which occurred while wearing the reusable study lenses.
Fifty-nine participants completed the study. The mean (± standard deviation) age of the participants was 31 (± 10). Thirty-four (58%) were female, 22 (37%) were male, 1 (2%) was transgender male, 1 (2%) was transgender female, and one (2%) identified as nonbinary. A data collection error occurred with one participant when completing the VAS and CLDEQ-8 surveys at 1 month of wear, resulting in 58 usable responses for those questionnaires. Of the eyes fit (188), 63 eyes (53%) wore a −0.75 cylinder lens, 37 (31%) wore a −1.25 cylinder lens, 13 (11%) wore a −1.75 cylinder lens, and 5 (4%) wore a −2.25 cylinder lens. The sphere power in the lenses ranged from plano to −8.00 D. Seventy-nine (67%) eyes had with-The-rule astigmatism (axes within 20 degrees of axis 180), 34 eyes had against-The-rule astigmatism (within 20 degrees of axis 090), and 5 (4%) eyes had oblique astigmatism (all other axes).
Initial Impression Visual Analog Scale Surveys
Initial impressions VAS surveys were completed by participants at the end of the visit in which each of the study lenses were dispensed. Because this survey included three VAS questions, the Bonferroni adjustment (0.05 divided by the number of questions) was used and the P value for significance in this survey became P <0.02. The mean ± standard deviation VAS scores for the initial impression of vision approached significance when comparing the delefilcon A lenses (84.2 ± 16.1) to the comfilcon A lenses (77.3 ± 19.7) with the Bonferroni adjustment for the P value. Results of all the initial impression surveys can be found in Table 2.
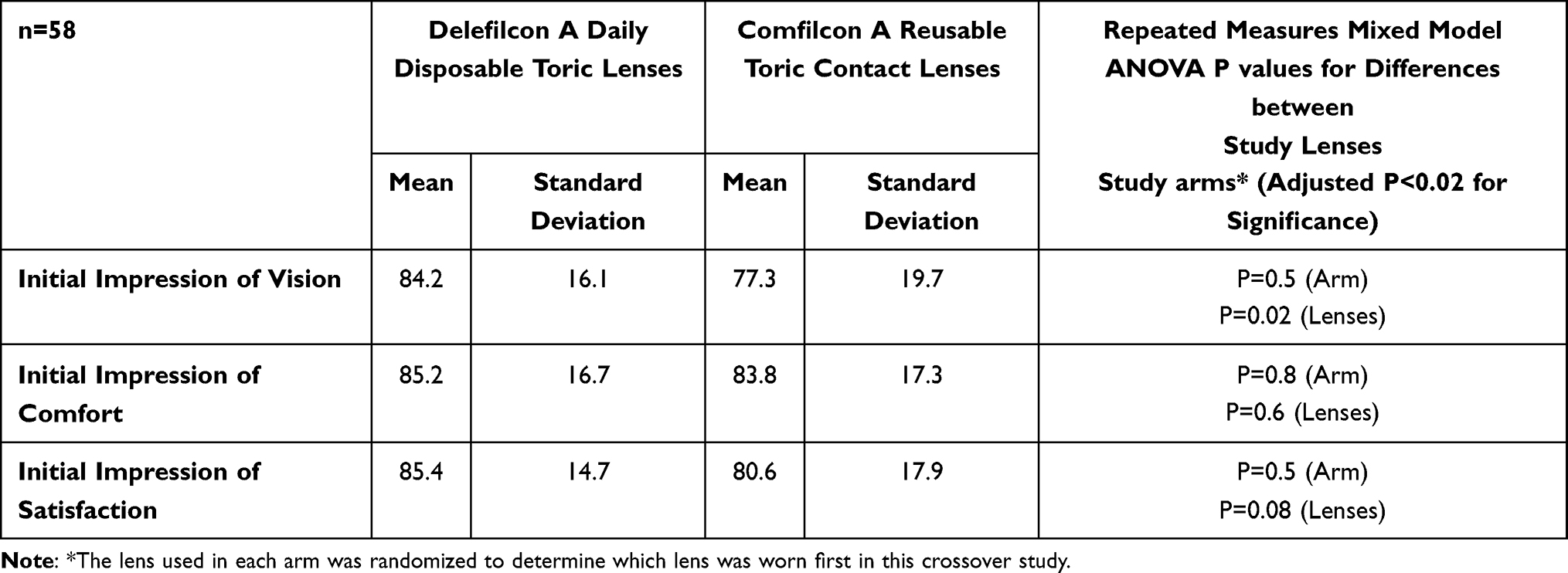 |
Table 2 Mean and Standard Deviations of Initial Impressions Visual Analog Scale Surveys |
Wear Experience Surveys After 1 Month of Lens Wear
After 30 days of lens wear, participants completed VAS surveys of their wear experience with each study lens after 30 days of lens wear. All surveys of vision, comfort, and satisfaction gave numerically higher values for the daily disposable lenses. Bonferroni correction for multiple comparisons was used to account for the nine questions in the survey, resulting in a P value of P=0.006 to show statistical significance. The mean VAS score for overall quality of vision (P=0.002) was statistically significant, with the daily disposable study lenses having significantly higher scores than the reusable study lenses. VAS scores for all surveys presented at the contact lens follow-up visit are presented in Table 3. VAS scores of dryness were not statistically significant for the two study lenses. The mean (stdev) CLDEQ-8 score was 14.3 ± 8.0 for the reusable lenses and 12.6 ± 6.9, but there was not a statistically significant difference (p=0.2).
 |
Table 3 Visual Analog Scale Surveys of Wear Experience After 30 Days of Wear with Study Lenses |
Convenience, Ease of Use, and Satisfaction
At the end of the study, participants completed surveys based upon their experiences with each of the study lenses, ranking convenience, ease of use, and overall satisfaction. The results of these surveys are presented in Table 4. Bonferroni correction for significance was made for these three questions (P=0.02 for significance). All three of these surveys had statistically higher scores for the daily disposable study lenses when compared to the reusable study lenses.
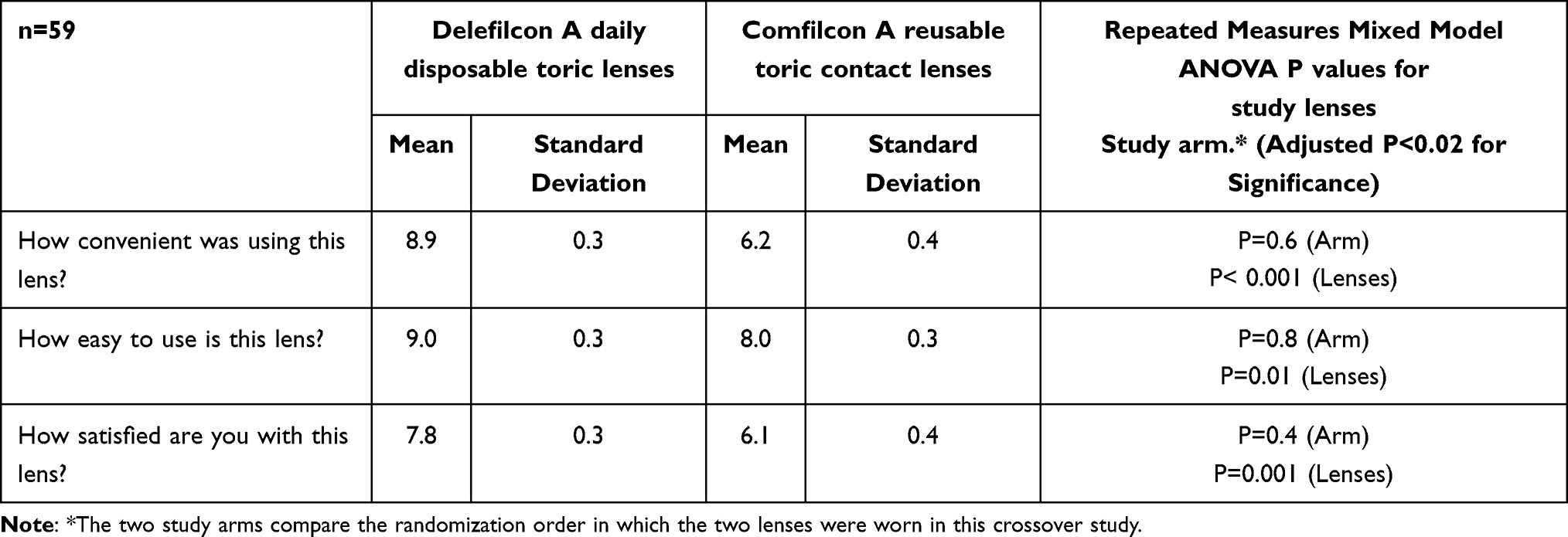 |
Table 4 Convenience, Ease of Use, and Satisfaction Surveys |
Participants were also asked which of the two study lenses they preferred based upon lens comfort, overall vision, and overall performance. Participants could choose either lens or could select “no preference” for each question. The tabulated results of these surveys are reported in Table 5. More than half of the participants selected the delefilcon A daily disposable lens in all three categories.
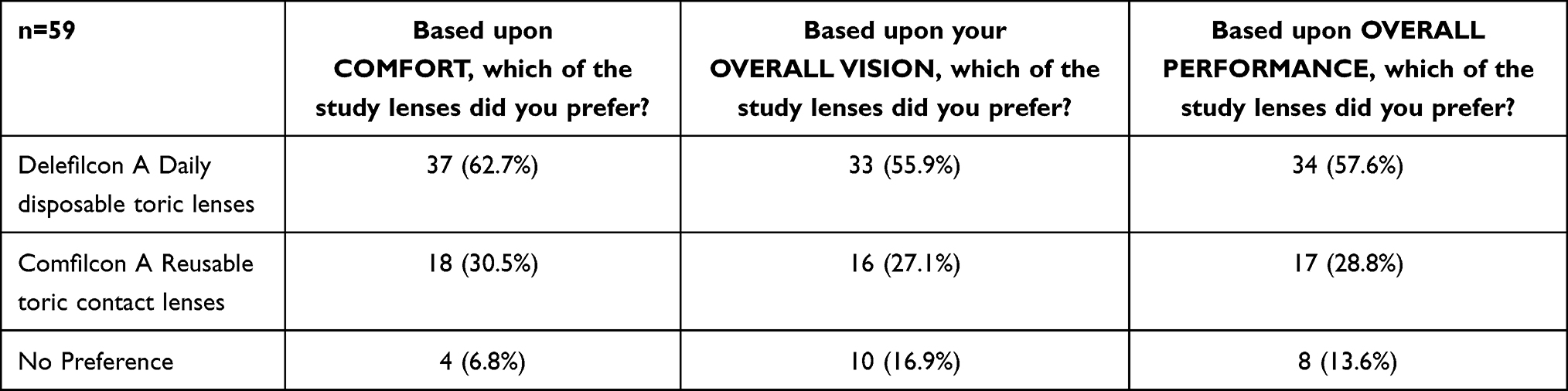 |
Table 5 Number and Percentage of Participants Preferring Each Study Lens |
Lens Rotation
Rotation of lenses was assessed at every visit. Comparison of the rotation assessed during the follow-up visit, in which all participants reported wearing their study lenses, was completed with a paired-t test. There were no statistical differences in the magnitude of rotation when comparing right eyes, left eyes and all eyes. During the follow-up visit, the rotation was less than 10 degrees in 112 eyes wearing the daily disposable study lens and 112 eyes wearing reusable study lens. Rotation was 10 degrees in 6 daily disposable lenses and 3 reusable lenses. None of the daily disposable study lenses had greater than 10 degrees of rotation and 3 of the reusable study lenses had more than 10 degrees of rotation.
Visual Acuity Results
The mean LogMAR visual acuity with both lenses was better than 0.00 LogMAR (20/20 Snellen) in each eye and binocularly for both study lenses. Mean (standard deviation) binocular acuity was −0.14 (0.07) with the delefilcon lenses and −0.12 (0.07) with the comfilcon A lenses (P=0.06). The mean difference in the binocular acuity was the equivalent of 1 letter and is likely not clinically significant.
Discussion
In this study, mean high contrast visual acuity scores were better than 20/20 with both study lenses. It is interesting that subjective scoring of overall quality of vision found statically higher mean scores for the daily disposable lens for astigmatism used in this study. Subjective assessments of vision that rely on patient scoring are typically not used in clinical practice but have been used increasingly in research to explore the patient vision experience that occurs beyond the high contrast acuity charts.17–21 While these assessments are valuable for researching, particularly for patients who may have decreased contrast acuity due to disease or simultaneous vision situations, those patients who wear single vision lenses are not generally asked to rate their vision, and visual acuity measurements are relied on for assessing lens performance. The difference in the subjective scoring of quality of vision in these participants is a reminder that patient impressions of vision include much more than “acuity chart” assessments.
While statistical significance is greatly important in research, clinical significance is valuable to those fitting lenses in clinical practice. A study by Papas in 2011 established a clinical difference in ocular comfort scores using a 1–100 numerical scale.22 A clinically meaningful difference was determined to be 7–8 units.22 The mean overall comfort score with the daily disposable lens used in this study was 8.4 units higher than the mean overall comfort for the reusable lens, which makes this difference clinically significant. While ocular satisfaction scores have not been previously studied for clinical significance threshold purposes, the mean satisfaction score was 9.1 units higher with the daily disposable study lenses compared to the reusable lenses, which is likely clinically relevant in a manner similar to the difference established in comfort scores.
There were some limitations to the study. The two lenses used in this study had different replacement schedules, materials, surface properties, and other bulk properties, which all could contribute to wear experience. Responses to the surveys were based on the wear experiences of the participants and could not differentiate what lens properties contributed to their responses. Although participants were given multipurpose solution and instructed on how to care for the lenses, compliance with solution use was not monitored. The results of this study show that toric delefilcon A lenses perform as well or better than toric comfilcon A lenses for people with astigmatism. Because toric comfilcon A lenses have a long history of success, this reflects highly for both lenses. The high objective and subjective vision scores coupled with the convenience, ease of use and satisfaction scores found in this study suggest that delefilcon A soft contact lenses for astigmatism are an excellent option for eye care practitioners seeking a healthy alternative to reusable lenses.
Data Sharing Statement
Data reported in this manuscript are available within the article. Study-level data including the study protocol are available. To request access to the data, the researcher must sign a data use agreement. All proposals should be directed to Jennifer Swingle Fogt ([email protected]) for up to 36 months following article publication.
Acknowledgments
Funding for this investigator-initiated trial was provided by Alcon, Inc., Fort Worth, TX, USA. The project described was supported in part by Award Number Grant UL1TR002733 from the National Center for Advancing Translational Sciences. The study was designed and conducted by the authors. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
The authors would also like to acknowledge the diligent work of Emma Grant and Spencer Mandel in coordinating this three-site study.
Disclosure
Dr Jennifer Fogt reports grants from Alcon, Inc, Vyluma, Bausch + Lomb, Cooper Vision, Interojo, VizionFocus, Eyenovia; personal fees from Envision Biomedicals, and TearOptix, outside the submitted work. Dr Katherine Bickle reports compensation from Alcon for clinical site, during the conduct of the study; clinical investigator for Johnson and Johnson Vision Care, and CooperVision, outside the submitted work. Dr Gina Wesley reports contract works for Johnson and Johnson, Coopervision, Bausch & Lomb, and Alcon, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Nemeth G, Szalai E, Berta A, Modis L Jr. Astigmatism prevalence and biometric analysis in normal population. Eur J Ophthalmol. 2013;23(6):779–783. doi:10.5301/ejo.5000294
2. Luensmann D, Schaeffer JL, Rumney NJ, Stanberry A, Fonn D. Magnitude of astigmatism - A comparison between eyes. Cont Lens Anterior Eye. 2022;45(5):101510. doi:10.1016/j.clae.2021.101510
3. Joseph S, Krishnan T, Ravindran RD, et al. Prevalence and risk factors for myopia and other refractive errors in an adult population in southern India. Ophthalmic Physiol Opt. 2018;38(3):346–358. doi:10.1111/opo.12447
4. Berntsen DA, Cox SM, Bickle KM, et al. A Randomized Trial to Evaluate the Effect of Toric Versus Spherical Contact Lenses on Vision and Eyestrain. Eye Contact Lens. 2019;45(1):28–33. doi:10.1097/ICL.0000000000000528
5. Richdale K, Berntsen DA, Mack CJ, Merchea MM, Barr JT. Visual acuity with spherical and toric soft contact lenses in low- to moderate-astigmatic eyes. Optom Vis Sci. 2007;84(10):969–975. doi:10.1097/OPX.0b013e318157c6dc
6. Edrington TB. A literature review: the impact of rotational stabilization methods on toric soft contact lens performance. Cont Lens Anterior Eye. 2011;34(3):104–110. doi:10.1016/j.clae.2011.02.001
7. Efron N, Morgan PB, Nichols JJ, et al. All soft contact lenses are not created equal. Cont Lens Anterior Eye. 2022;45(2):101515. doi:10.1016/j.clae.2021.101515
8. Solomon OD, Freeman MI, Boshnick EL, et al. A 3-year prospective study of the clinical performance of daily disposable contact lenses compared with frequent replacement and conventional daily wear contact lenses. Clao j. 1996;22(4):250–257.
9. Nason RJ, Boshnick EL, Cannon WM, et al. Multisite comparison of contact lens modalities. Daily disposable wear vs. conventional daily wear in successful contact lens wearers. J Am Optom Assoc. 1994;65(11):774–780.
10. Ichijima H, Karino S, Sakata H, Cavanagh HD. Improvement of Subjective Symptoms and Eye Complications When Changing From 2-Week Frequent Replacement to Daily Disposable Contact Lenses in a Subscriber Membership System. Eye Contact Lens. 2016;42(3):190–195. doi:10.1097/ICL.0000000000000167
11. Chalmers RL, Keay L, McNally J, Kern J. Multicenter case-control study of the role of lens materials and care products on the development of corneal infiltrates. Optom Vis Sci. 2012;89(3):316–325. doi:10.1097/OPX.0b013e318240c7ff
12. Alves M, Castanheira EMS, Lira M. Interactions between contact lenses and lens care solutions: influence in optical properties. Cont Lens Anterior Eye. 2021;44(5):101414. doi:10.1016/j.clae.2021.01.009
13. Thekveli S, Qiu Y, Kapoor Y, Liang W, Pruitt J. Structure–property relationship of delefilcon a lenses. Contact Lens Anterior Eye. 2012;35:e14. doi:10.1016/j.clae.2012.08.044
14. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
15. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
16. Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. 2014;34(5):502–508. doi:10.1111/opo.12131
17. Jong M, Tilia D, Sha J, Diec J, Thomas V, Bakaraju RC. The Relationship between Visual Acuity, Subjective Vision, and Willingness to Purchase Simultaneous-image Contact Lenses. Optometry Vision Sci. 2019;96(4):283–290. doi:10.1097/OPX.0000000000001359
18. Crabtree HL, Hildreth AJ, O’Connell JE, Phelan PS, Allen D, Gray CS. Measuring visual symptoms in British cataract patients: the cataract symptom scale. Br J Ophthalmol. 1999;83(5):519–523. doi:10.1136/bjo.83.5.519
19. Rutschilling R, Fogt JS. Wear Experience of a Water Surface Daily Disposable Contact Lens in Existing Silicone Hydrogel Planned Replacement Lens Wearers. Clin Optom. 2022;14:27–34. doi:10.2147/OPTO.S353666
20. Fogt JS, Patton K. Long Day Wear Experience with Water Surface Daily Disposable Contact Lenses. Clin Optom. 2022;14:93–99. doi:10.2147/OPTO.S367891
21. Fogt JS, Patton K. Evaluation of Wear Experience with Soft Daily Disposable Lenses for Astigmatism over 16 Hours of Wear. Clin Optom. 2022;14:207–214. doi:10.2147/OPTO.S387740
22. Papas EB, Keay L, Golebiowski B. Estimating a just-noticeable difference for ocular comfort in contact lens wearers. Invest Ophthalmol Vis Sci. 2011;52(7):4390–4394. doi:10.1167/iovs.10-7051
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.