")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Vascular Endothelial Growth Factor Antagonists: Promising Players in the Treatment of Neovascular Age-Related Macular Degeneration
Authors Hussain RM, Shaukat BA, Ciulla LM, Berrocal AM, Sridhar J
Received 5 May 2021
Accepted for publication 26 May 2021
Published 21 June 2021 Volume 2021:15 Pages 2653—2665
DOI https://doi.org/10.2147/DDDT.S295223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Rehan M Hussain,1 Bilal A Shaukat,1,2 Lauren M Ciulla,3 Audina M Berrocal,4 Jayanth Sridhar4
1Retina Associates Ltd, Elmhurst, IL, USA; 2Department of Ophthalmology, Cook County Hospital, Chicago, IL, USA; 3Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 4Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, 33136,USA
Correspondence: Rehan M Hussain
Retina Associates Ltd, 133 E Brush Hill Road, Suite 300, Elmhurst, IL, 60126, USA
Tel +1 630-288-5540
Fax +1 630-571-5679
Email [email protected]
Abstract: Neovascular age-related macular degeneration (nAMD) treatment has been revolutionized by the introduction of vascular endothelial growth factor antagonists (anti-VEGF), but the need for frequent intravitreal injections poses a heavy burden to patients and physicians. Evolving anti-VEGF therapies include longer duration agents, approaches that target multiple pathways, topical anti-VEGF agents, sustained-release, and genetic therapies. Abicipar pegol, a designed ankyrin repeat protein (DARPin), demonstrated the ability to maintain stable visual acuity with 12-week dosing, but was not approved by the FDA due to higher than usual rates of intraocular inflammation. Conbercept, a recombinant anti-VEGF fusion protein, has been approved in China, and is in Phase 3 trials globally. KSI-301 is an anti-VEGF antibody biopolymer conjugate that allowed 66% of nAMD patients to maintain at least a 6-month treatment-free interval in Phase 1b studies. OPT-302, an inhibitor of VEGF-C/D, will be tested in phase 3 studies that compare anti-VEGF-A monotherapy against combination therapy with OPT-302. Faricimab is a bispecific anti-VEGF/Ang-2 antibody that upregulates the Tie-2 signaling pathway and promotes vascular stability; it is undergoing phase 3 trials with potential for 12- or 16-week dosing. PAN-90806 is a topical anti-VEGF agent that showed the ability to reduce injection frequency by 79% compared to ranibizumab monotherapy in a phase 1/2a trial. Sustained-release anti-VEGF therapies include the ranibizumab Port Delivery System (in phase 3 studies), GB-102 (Phase 2b), OTX-TKI (phase 1), and Durasert (preclinical). Suprachoroidal delivery of the tyrosine kinase inhibitor, axitinib, is in preclinical studies. Genetic therapies in phase 1 studies include RGX-314 and ADVM-022, which introduce a viral vector that modifies the retina’s cellular apparatus to create an anti-VEGF biofactory, potentially serving as a one-time treatment. Further investigation is warranted for drugs and delivery systems that hope to advance visual outcomes and reduce treatment burden of nAMD.
Keywords: ADVM-022, age-related macular degeneration, abicipar pegol, CLS-AX, conbercept, faricimab, GB-102, KSI-301, PAN-90806, OTX-TKI, ranibizumab port delivery system, RGX-314, VEGF
Background
Age-related macular degeneration (AMD) is the most common cause of irreversible blindness in the elderly population of the industrialized world.1 The number of patients globally with AMD is estimated to be 196 million in 2020 and will reach 288 million in 2040.2 AMD is classified into one of two main subtypes: the non-neovascular (dry) and neovascular (wet) forms of the disease. Approximately 90% of all AMD case are characterized as dry AMD, in which accumulation of yellow lipofuscin-rich deposits known as drusen, along with atrophy of the macula, result in gradual vision loss over years.3 Neovascular AMD (nAMD), on the other hand, may result in acute and substantial loss of central vision; the growth of pathologic choroidal neovascularization (CNV) under the macula results in exudation of blood and/or serous fluid into the macula.4,5 The neovascular tissue and associated exudates can progress into submacular fibrosis that causes permanent loss of central vision.
Irregular neovascularization and exudation are caused by increased levels of the pro-angiogenic cytokine, vascular endothelial growth factor-A (VEGF).6 This cytokine was originally called vascular permeability factor because it results in increased exudation from blood vessels.7 Intravitreally administered therapies that neutralize VEGF have substantially reduced the degree of vision loss for patients with nAMD compared to the previous standard of care.8
Existing Treatments
Before the introduction of intravitreal anti-VEGF therapy, treatment options for nAMD included photodynamic therapy with verteporfin, focal laser photocoagulation, intravitreal corticosteroids, and surgical removal of CNV. These treatments have fallen out of favor since they did not significantly improve visual outcomes.9 In 2004, pegaptanib (Macugen, Eyetech) was approved by the United States Food and Drug Administration (US FDA) for the treatment of nAMD, marking the beginning of the anti-VEGF era; more recently it has also fallen out of favor compared to newer and more effective anti-VEGF agents such as ranibizumab, aflibercept, bevacizumab, and brolucizumab (summarized in Table 1). Most recently, in 2019, Brolucizumab (Novartis, Basel, Switzerland) was approved for 12-week dosing intervals in nAMD;10 it has recently come under scrutiny due to reports of occlusive retinal vasculitis associated with its use.11 All of these agents inhibit VEGF-A, which binds VEGF receptor (VEGFR)-2, that mediates angiogenesis and vascular leakage.
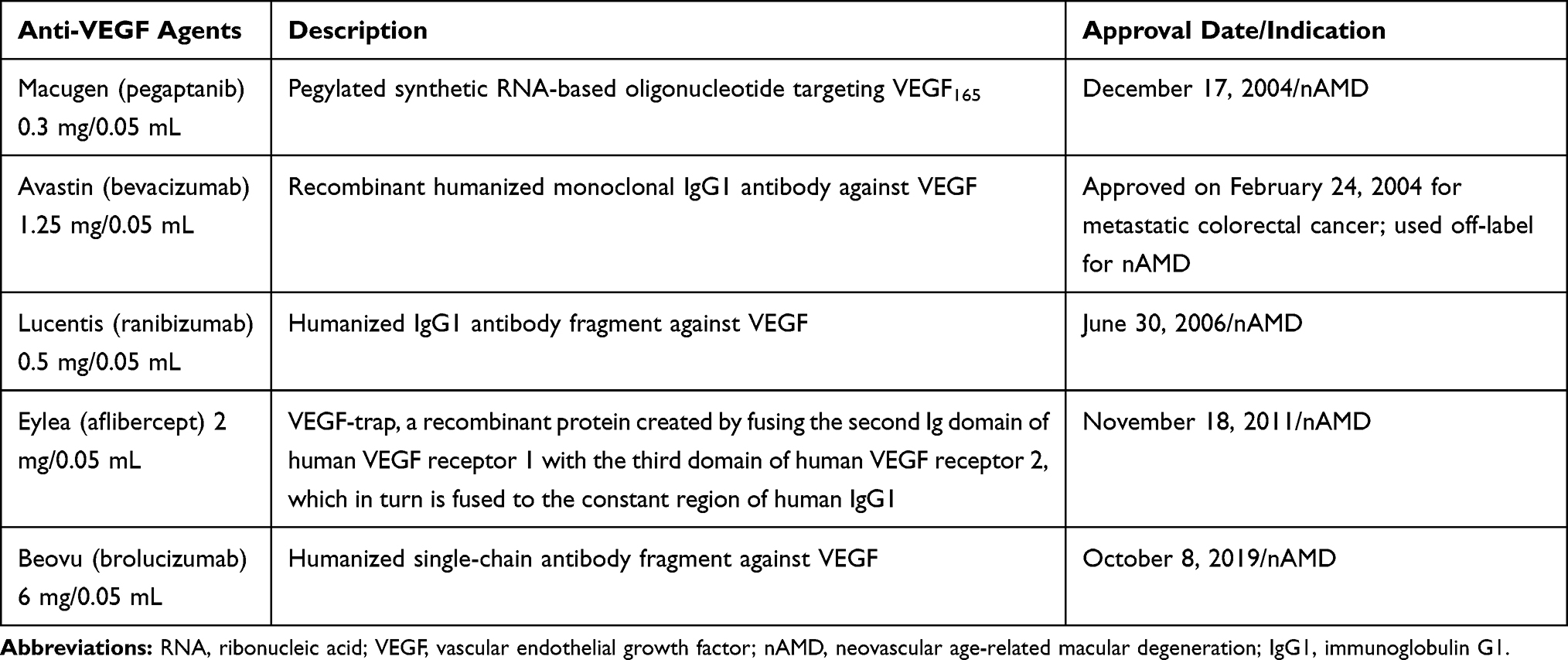 |
Table 1 Summary of Currently Available Intravitreal Anti-VEGF Therapies |
Unmet Needs and Current Research Goals
Despite the substantial progress in nAMD treatments, there are a number of shortcomings to anti-VEGF therapy, including the necessity of repeated injections and inadequate anatomic response in a subset of eyes. Even with monthly repeated injections of anti-VEGF therapy over 12 months, one fifth of patients have declining visual acuity (VA), about half do not achieve 20/40 VA (the requirement for an unrestricted driver’s license in parts of the USA and in most European Union countries), and over 2/3 fail to gain 3 or more lines of ETDRS letters.8,12
Although favorable visual outcomes with treat and extend dosing of aflibercept have been reported,13 many “real world” anti-VEGF injection studies show visual outcomes inferior to those reported in randomized clinical trials (RCTs), likely as a result of non-compliance and under-treatment in the real world.14–29 Many reports have documented a positive correlation between the quantity of anti-VEGF injections over 1 year and better visual outcomes.15–17,21,24,30–32
Compliance with frequent anti-VEGF injection can be limited by factors such as patients’ anxiety toward the needle, financial hardship, scheduling conflicts, and lack of transportation. More durable anti-VEGF formulations may help overcome some of these barriers. Although anti-VEGF drugs improve VA by limiting leakage from CNV, the pathophysiology of nAMD is indeed a complex process requiring attention to many more pathologic mechanisms than just VEGF inhibition. Unfortunately, a large RCT showed that nearly half of anti-VEGF treated eyes developed submacular fibrosis despite 2 years of injections, which limits further visual benefit despite treatment.33 As a result, new therapies and delivery systems are being developed to target other complementary mediators involved in angiogenesis.
In particular, inhibition of VEGF-A has been shown to upregulate other forms of VEGF, which may contribute to limited outcomes. For example, after bevacizumab (anti-VEGF-A) administration in nAMD patients, VEGF-C which also activates the VEGF2 receptor is upregulated.34 This upregulation of other VEGF ligands could contribute to treatment resistance, and a ceiling of efficacy. Tyrosine kinase inhibitors (TKIs), which achieve pan-VEGF receptor inhibition, could address this issue and, consequently, there has been interest in TKIs as investigational agents. TKIs assessed in clinical trials include oral vorolanib, topical sorafenib, regorafenib, and pazopanib, as well as intraocularly-injected sunitinib and axitinib. Although a few investigational anti-platelet-derived growth factor (anti-PDGF) drugs were developed with the objective of combining them with anti-VEGF injections, none have shown advantage over anti-VEGF monotherapy in a phase 3 clinical trial.35,36 The Tie-2 receptor kinase, which enhances vascular stability to minimize leakage, has been another target for investigational therapies.37 Sustained-release drug delivery systems, along with topical and oral anti-VEGF formulations, may also help to reduce injection frequency in the future. Viral vector-based gene therapy can produce continuous anti-VEGF expression after a single treatment.38
Drugs and Delivery Systems in Development
See Table 2 for a summary of investigational anti-VEGF medications and delivery systems.
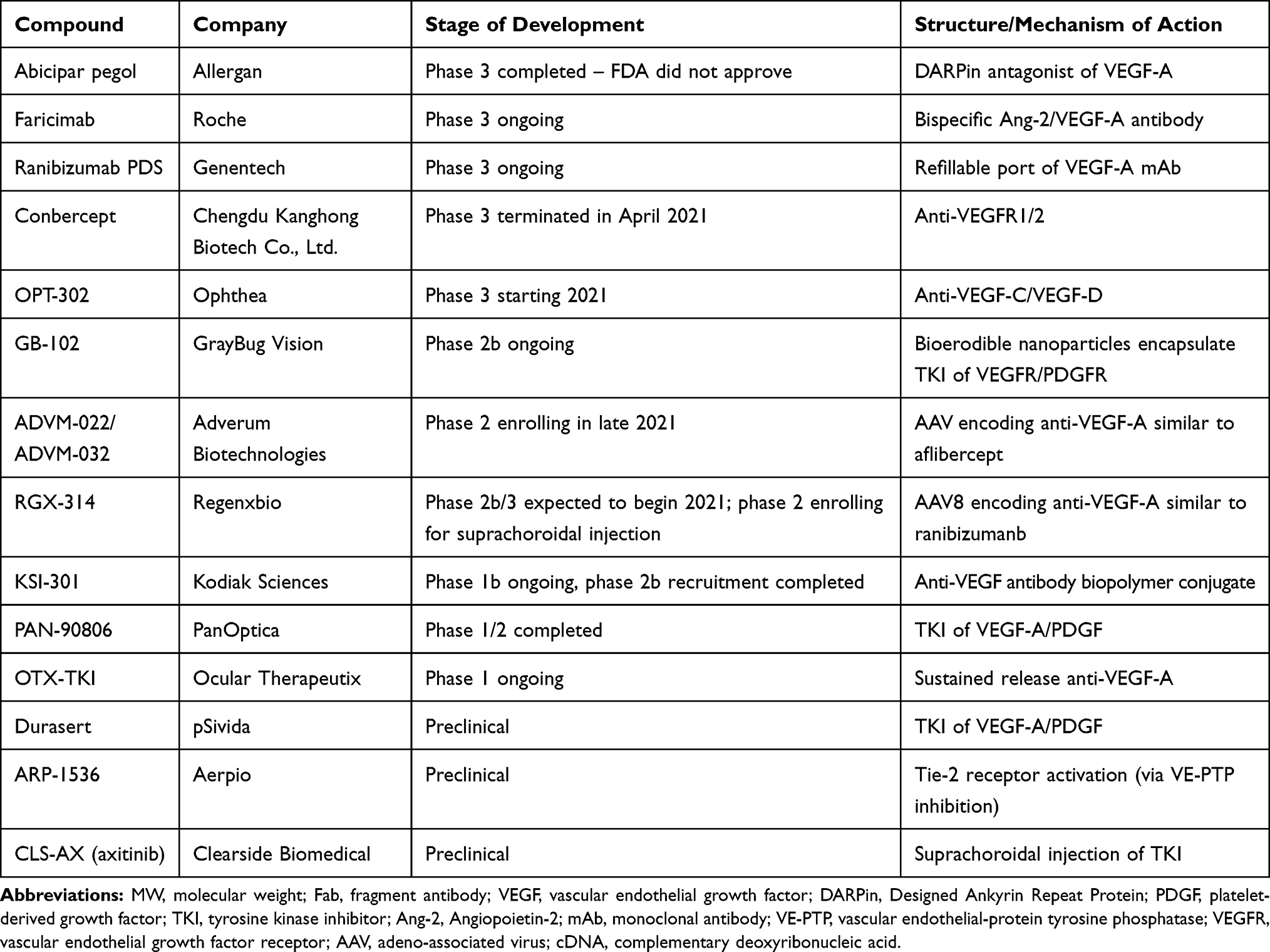 |
Table 2 Summary of Emerging Drugs to Treat Neovascular Age-Related Macular Degeneration (nAMD) |
Abicipar Pegol
Abicipar pegol is a novel anti-VEGF drug based on DARPin® (Designed Ankyrin Repeat Protein) technology. Two phase 3 clinical trials (SEQUOIA and CEDAR) sponsored by Allergan (Dublin, Ireland) and Molecular Partners (Zurich, Switzerland) compared abicipar against ranibizumab.39 Both studies were comprised of three treatment groups: abicipar every 8 weeks, abicipar every 12 weeks, and monthly ranibizumab. The 8-week group was treated with three loading doses and the 12-week abicipar group with two loading doses before switching to their specified treatment interval. The proportion of treated patients with stable vision (<15 ETDRS letters lost) at 1 year was the primary endpoint.
In SEQUOIA, 94.8% and 91.3% of those treated with abicipar every 8 and 12 weeks maintained stable vision. In the group that received monthly ranibizumab, 96% of patients maintained stability. In CEDAR, 91.7% and 91.2% of patients in the abicipar groups maintained stable vision when dosed every 8 and 12 weeks, compared with 95.5% of patients in the monthly ranibizumab group.39
While the durability of abicipar was impressive, the rates of intraocular inflammation were significantly higher in the abicipar groups (15.1–15.7%) compared to the ranibizumab group (0–0.6%). A newer modified version was studied in the smaller MAPLE study. In this open-label study, 123 nAMD patients received three monthly 2 mg abicipar injections followed by 2 mg injections every 8 weeks through week 28. The incidence of intraocular inflammation was 8.9%, mostly mild-to-moderate in severity. The incidence of severe inflammation was 1.6%, with one case of iritis and one case of uveitis. There were no reported cases of endophthalmitis or retinal vasculitis.39 Despite this, in June 2020 the FDA rejected abicipar as a nAMD drug candidate, citing an unfavorable benefit–risk ratio of intraocular inflammation compared to the current treatment options for nAMD. Allergan/AbbVie are to discuss further steps with the FDA.40
OPT-302
OPT-302 (Opthea; Victoria, Australia) inhibits both VEGF-C and VEGF-D, which are thought to serve a supplemental role to VEGF-A in nAMD pathophysiology. As discussed above, broad VEGF inhibition has the potential to address secondary upregulation of other forms of VEGF that follows VEGF-A blockade. The phase 1 trial (NCT02543229) demonstrated that monthly intravitreal injections of combination OPT-302 2 mg and ranibizumab 0.5 mg (to inhibit VEGF-A) had a favorable safety profile. After 12 weeks of follow-up, this regimen showed significant extra visual gains and reduction in CST compared to ranibizumab monotherapy. Of 51 patients enrolled, 25 were treatment-naïve patients, and 26 had been previously treated with intravitreal anti-VEGF-A inhibitors.41
Seven of 13 (54%) patients receiving OPT-302 monotherapy did not need rescue anti-VEGF-A injections and the mean change in BCVA from baseline to week 12 was +5.6 letters. Mean BCVA gains from baseline to week 12 following combination OPT-302 with ranibizumab were +10.8 letters in treatment-naive patients and +4.9 letters in patients with prior anti-VEGF treatment. At week 12, change in mean CST in both groups were −119 μm and −54 μm, respectively; half of treatment-naive patients did not show any detectable CNV at that point. The proportion gaining ≥5, ≥10, or ≥15 ETDRS letters at week 12 was 67%, 44%, and 33%, respectively, in treatment-naïve subjects (baseline mean BCVA of 56.4 letters); for those patients with a history of prior anti-VEGF therapy it was 53%, 16%, and 0% (baseline mean BCVA was higher at 64.5 letters).41
Phase 2b trials compared ranibizumab monotherapy with two doses of combination OPT-302/ranibizumab in 366 treatment-naïve patients. Patients receiving 2 mg OPT-302 combination therapy gained a mean of 14.2 letters by week 24, compared to 10.8 letters in ranibizumab monotherapy group (difference of 3.4 letters, p=0.0107). The 0.5 mg OPT-302 low dose group had a similar outcome to the ranibizumab monotherapy group (+9.4 letters). High dose OPT-302 (2 mg) combination treatment showed improvements across multiple secondary endpoints, including a higher proportion of patients with stable vision (defined as ≤15 letter loss from baseline), and those gaining ≥10 and ≥15 letters of visual acuity.42
Opthea has two upcoming phase 3 trials, ShORe and COAST, which will enroll treatment-naïve patients and assess the efficacy and safety of 2 mg OPT-302 in combination with anti-VEGF-A therapy compared to anti-VEGF-A monotherapy. Patients will be dosed every 4 or 8 weeks (treated with ranibizumab for ShORe and aflibercept for COAST). The primary endpoint of both trials will be the mean change in VA from baseline to week 52, though patients will continue to be dosed until week 96 to evaluate long-term safety. Opthea plans to commence both trials in the first half of 2021.43
Conbercept
Conbercept (Chengdu Kanghong Biotech Co. Ltd.; Chengdu, Sichuan, China) is a recombinant anti-VEGF fusion protein that is composed of portions of VEGFR1 and VEGFR2. The phase 3 PHOENIX trial conducted in China led to its approval there. One treatment arm received conbercept 0.5 mg monthly for 3 months followed by 0.5 mg every 3 months. The delayed treatment group received three monthly sham injections, followed by three monthly conbercept 0.5 mg injections, and finally quarterly conbercept 0.5 mg injections until month 12. The group with the loading doses of conbercept demonstrated an improvement of 9.9 letters, while the delayed treatment arm had 8.8 letter improvement, both of which were statistically significant.44
PANDA-1 (NCT03577899) and PANDA-2 (NCT03630952) are both international phase 3 studies that evaluated safety and efficacy in comparing conbercept 0.5 mg and 1.0 mg to aflibercept. Patients in each of the trials’ three study arms received three monthly loading doses, after which the treatment groups formed were: conbercept 0.5 mg at 8-week intervals, conbercept 1 mg at 12-week intervals, and aflibercept 2 mg at 8-week intervals. The primary outcome was mean change in BCVA at 36 weeks. The PANDA-1 and PANDA-2 trials with a combined enrollment target of 1,140 patients were originally targeted for completion in 2022.45,46 Due to disruptions related to the global pandemic of 2020–2021, in which many patients did not complete adequate follow-up to obtain results with registrational value, the trials were terminated early in April 2021.47
KSI-301
KSI-301 (Kodiak Sciences; Palo Alto, CA) has developed a novel anti-VEGF antibody biopolymer conjugate (ABC platform™) for the treatment of nAMD and other retinal vascular diseases. The ABC platform comprises a humanized IgG1 antibody with inert immune effector function and a biopolymer that is an optically clear high molecular weight phosphorylcholine polymer, which was designed to increase intraocular durability. The phase 1b study for nAMD compares 8-week dosing of aflibercept with 12, 16, and 20-week dosing of KSI-301. Patients were randomized to receive a 2.5 mg/50 µL or 5 mg/100 µL dose with three loading doses at monthly intervals and a mandatory re-treatment at 6 months after the last treatment.48
New KSI-301 data were presented at the Angiogenesis, Exudation, and Degeneration 2021 virtual meeting in February 2021. This data demonstrated promise in 1-year durability, efficacy, and safety in the Phase 1b study. Of nAMD patients, 66% achieved a 6-month or longer treatment-free interval at the 1-year mark and 78% were on a 4-month or longer interval. An average of only 2.0 re-treatments were given in the 10 months after the initial three loading doses. In nAMD patients a 5.7 letter improvement was noted after 1 year.49
There has also been recent completion of recruitment in the USA for Kodiak’s DAZZLE Phase 2b/3 study (NCT04049266) in treatment naive nAMD patients. In this study, after three monthly loading doses patients are randomized to receive KSI-301 on a dosing regimen no more than every 3 months and as infrequently as every 5 months compared to aflibercept every 8 weeks. BCVA at 1 year will mark primary study outcome, with continued following of patients for 2 more years.50
Anti-VEGF-A Plus Tie-2 Receptor Modulator Combination Therapy
The Tie-2 tyrosine kinase receptor, which is expressed on vascular endothelial cells, has also become a target of interest in treating exudative retinal disease. Activation of this receptor reinforces junctional proteins and stabilizes vasculature to limit permeability.51 Angiopoietin-1 (Ang-1) is a ligand that activates the Tie-2 receptor, thus reducing vascular leakage and promoting homeostasis.52 Angiopoietin-2 (Ang-2) is upregulated in pathologic states and is a competitive antagonist to Ang-1; elevated Ang-2 levels promote vascular leakage.53 Several new drugs have been designed to inhibit Ang-2, thus allowing the constitutively secreted Ang-1 to activate the Tie-2 receptor. Another approach targets the enzyme, vascular endothelial protein tyrosine phosphatase (VE-PTP), which inactivates the Tie-2 receptor and more directly affects the phosphorylation and activation of Tie-2.54 Enhancing Tie-2 receptor function in combination with anti-VEGF therapy may provide enhanced efficacy over anti-VEGF monotherapy.
Faricimab
Faricimab (Roche/Genentech; Basel, Switzerland) is a unique bispecific antibody targeting both VEGF-A and Ang-2. The phase 2 AVENUE trial included 273 patients, which compared treatment with ranibizumab 0.5 mg every 4 weeks, faricimab 1.5 mg every 4 weeks, faricimab 6 mg every 4 weeks, faricimab 6 mg every 8 weeks, and faricimab 6 mg/ranibizumab 0.5 mg combination therapy (three ranibizumab injections every 4 weeks, followed by faricimab every 4 weeks) in treatment-naïve nAMD. The primary outcome was mean change in BCVA from baseline at 36 weeks. The 1.5 mg faricimab arm given every 4 weeks demonstrated the best gains of +9.1 letters at 36 weeks. All arms showed significant decreases in central subfield thickness (CST), with the combination therapy arm demonstrating the largest reduction of −185 µm.55
Another phase 2 trial, STAIRWAY, compared faricimab 6 mg given either every 12 or 16 weeks to ranibizumab 0.5 mg every 4 weeks in 76 treatment-naïve nAMD patients. In the two faricimab groups, patients initially received four monthly faricimab injections followed by injections either every 12 or 16 weeks. The ranibizumab group received monthly treatment. At week 24, 65% of all patients treated with faricimab had no protocol-defined activity 12 weeks after their last injection. At 52 weeks, patients in the 12-week group gained a mean of 10.1 letters, those in the 16-week group gained 11.4 letters, and the ranibizumab group gained 9.6 letters.56
Two multi-center Phase 3 trials, LUCERNE (NCT03823300) and TENAYA (NCT03823287), have been launched with 1,280 participants randomized into treatment arms of faricimab every 16 weeks (with the ability to decrease the interval to 12 or 8 weeks) or aflibercept every 8 weeks with the average change of BCVA from baseline to week 48 serving as the primary outcome measure. The expected completion of the Phase 3 trials is Fall 2022. Interim results released in February 2021 revealed that both studies met their primary endpoint, with faricimab demonstrating non-inferior VA gains to aflibercept. In TENAYA and LUCERNE, the mean vision gains from baseline in the faricimab arms were +5.8 and +6.6 letters, respectively, compared to +5.1 and +6.6 letters in the aflibercept arms. Of note, 45.7% (144/315) of patients in TENAYA and 44.9% (142/316) in LUCERNE were able to be treated every 4 months in the first year. An additional 34% (n=107/315) of patients in TENAYA and 32.9% (n=104/316) in LUCERNE were able to be treated every 3 months. Combined, approximately 80% of faricimab-treated patients were able to go 3 months or longer between treatments during the first year. In both studies, faricimab given at intervals of up to 4 months offered reductions in CST similar to aflibercept given every 2 months.57
ARP-1536
ARP-1536 (Aerpio Therapeutics; Blue Ash, OH) is a monoclonal antibody that activates the Tie-2 receptor by inhibiting VE-PTP, which is the most downstream negative regulator of Tie-2. ARP-1536 is administered by intravitreal injection and binds to the extracellular domain of VE-PTP, hindering its function, and thus causing increased activation of the Tie-2 receptor. Pre-clinical studies have established its biologic activity. AKB-9778, Aerpio’s other VE-PTP inhibitor, is administered by subcutaneous injection.37 At the time of this writing, Aerpio has not made any public updates on plans for a phase 1 clinical trial for ARP-1536.
Topical Treatments
There have been several topical therapies developed to inhibit VEGF and PDGF, including pazopanib (a TKI, GlaxoSmithKline; Brentford, UK), squalamine lactate (Ohr Pharmaceutical; New York, NY), regorafenib (Bayer Healthcare; Leverkusen, Germany), and LHA510 (a TKI, Alcon; Fort Worth, TX). None of these drugs were shown to reduce the need for intravitreal anti-VEGF injections, and their clinical development has been discontinued.58
PAN-90806
PAN-90806 (PanOptica; Mount Arlington, NJ), a TKI eyedrop, has been shown to produce anti-VEGF-A biological signaling with topical once daily dosing, according to a phase 1/2 study (NCT02022540). A newer suspension was designed to reduce the incidence of punctate keratopathy as a side-effect, which occurred due to off target inhibition of corneal epithelial growth factor receptor. A new phase 1/2 clinical trial of the updated suspension for patients with nAMD (NCT03479372) has shown significantly improved safety and tolerability compared to the prior (solution) formulation. It demonstrated anti-VEGF biological response at all doses (2 mg/mL, 6 mg/mL, 10 mg/mL) in 51 treatment naïve wet AMD patients as once daily monotherapy for 12 weeks. Twenty-six of 51 (51%) patients completed the study on PAN-90806 eyedrops alone (without rescue ranibizumab injections) through the 1-month post-treatment (week 16) visit; 23 of 26 (88%) non-rescued patients showed clinical improvement or stability based on independent masked review. Those patients requiring rescue treatment at week 4 or earlier had greater CST (444 μm) and baseline BCVA (20/100) compared to those that were never rescued (331 μm, 20/63) or rescued after 4 weeks (365 μm, 20/80). The mean number of rescue ranibizumab injections per patient was 0.84, which represents a reduction of 79.4% compared to monthly ranibizumab treatment.59
Sustained Delivery Treatments
Ranibizumab Port Delivery System
The need for frequent intravitreal injections has spurred several companies to develop sustained-release anti-VEGF-A devices. Genentech (South San Francisco, CA) developed the ranibizumab Port Delivery System (PDS), which is a nonbiodegradable port surgically fixed to the sclera that has a 0.05 mL reservoir that can be refilled in the office.
The phase 2 LADDER trial randomized 179 patients to implantation of the PDS with doses of ranibizumab of either 10 mg/mL, 40 mg/mL, or 100 mg/mL. Among the PDS group with the 100 mg/mL ranibizumab dose, approximately 80% of patients were maintained for 6 months or longer without requiring a medication refill. In the 10 mg/mL and 40 mg/mL groups, 63.5% and 71.3%, respectively, went 6 months or more without a refill. At 9 months, BCVA change from baseline was –3.2, –0.5, +5.0, and +3.9 letters in the PDS 10 mg/mL, PDS 40 mg/mL, PDS 100 mg/mL, and monthly intravitreal ranibizumab 0.5-mg arms, respectively. Initially in the trial, rate of vitreous hemorrhage related to the surgical procedure was as high as 50%. Modifications to the surgical approach were made, including cauterization of the choroid with laser photocoagulation, which then resulted in a reduced postoperative vitreous hemorrhage rate of 4.5%. Other notable complications included endophthalmitis (1.7%), retinal detachment (2.2%), hyphema (4.5%), and cataract (7.3%).60
The Phase 3 ARCHWAY (NCT03677934) trial is currently underway. Primary analysis of results were presented at the American Society of Retina Specialists (ASRS) annual meeting in July 2020, which demonstrated achievement of primary endpoint visual outcomes in PDS patients and reduced treatment burden compared with monthly injections of ranibizumab. Of note, 98% of patients in the PDS cohort did not require a supplemental ranibizumab injection at 6 months. There were no significant differences in safety between the two treatment arms. Expected completion of the ARCHWAY trial is in 2022.61
GB-102
GB-102 (GrayBug Vision; Redwood City, CA) is sunitinib maleate, a TKI with activity against both VEGF-A and PDGF. It is an injectable depot designed for twice per year formulation. The drug is encapsulated within bioerodible polymer nanoparticles that degrade slowly over time. The patented GrayBug formulation is designed to avoid the inflammatory response seen with other nanoparticles, and the nanoparticles remain at the injection site to avoid clouding the visual axis. Phase 1/2a study (ADAGIO) results were announced in January 2019. The study met its primary endpoint of safety and tolerability, with no dose limiting toxicities or serious ocular adverse events. There was a long-lasting pharmacodynamic effect, with 3- and 6-month dosing duration achieved in 88% and 68% of patients, respectively. However, there was microparticle-related anterior chamber migration and mild ocular hypertension, which was self-limited.62
The phase 2b ALTISSIMO study in wet AMD tested a new GB-102 manufacturing process optimized to eliminate particle dispersion. Two doses of GB-102 (1 mg and 2 mg) injected every 6 months were compared against aflibercept injected every 2 months. Following an interim safety analysis, the 2 mg dose arm was discontinued and those patients received the 1 mg dose for their second treatment. The median time to first supportive therapy was 5 months for the GB-102 1 mg group. Forty-eight percent of the patients did not require supportive therapy for at least 6 months, and 62% did not require supportive therapy for at least 4 months more. In all, the GB-102 1 mg dose was well-tolerated by patients. The majority of drug-related adverse events were mild-to-moderate, and medication was detected in the anterior chamber in less than 10% of the 1 mg injections. No vision-threatening inflammation was observed and there were no significant rises in intraocular pressure. CST in the GB-102 1 mg arm was similar to that of the aflibercept control arm, though mean change in BCVA for all 20 completers was approximately 9 ETDRS letters lower compared to aflibercept across all time points. A 6-month extension has been added to the trial, after which full analysis of the trial results will determine future directions.63
OTX-TKI and OTX-AFS
Ocular Therapeutix (Bedford, MA) developed a sustained release formulation of axitinib, a TKI, that is delivered through intravitreal injection. OTX-TKI is a bioresorbable hydrogel that contains TKI particles in an injectable fiber, designed to deliver drug to target tissues for up to 12 months. The hydrogel creates a meshwork that encloses the drug and gradually dissolves, allowing the medication to be released over time. Phase 1 studies of axitinib intravitreal implant (OTX-TKI) are in process; the first patient was dosed in the second quarter of 2018. OTX-AFS is an aflibercept suprachoroidal injection that is being developed in collaboration with Regeneron, which is still in the preclinical phase of investigation.64
CLS-AX
Clearside Biomedical (Alpharetta, GA) is currently sponsoring a Phase 1/2a trial of CLS-AX, a suprachoroidally administered formulation of axitinib. Suprachoroidal delivery can target therapy to affected chorioretinal tissues for potential efficacy benefits, compartmentalizing it away from unaffected vitreous and anterior segment tissues for potential safety benefits, and achieve durability through the use of insoluble suspension formulations.65 This approach was assessed with proof of concept therapy, CLS-TA or Xipere, a proprietary suspension of triamcinolone, for uveitic macular edema, culminating in a successful phase 3 clinical trial; durability was demonstrated in an extension study, with a new drug application planned for 2021.66 In preclinical studies of axitinib, compared to intravitreal administration, suprachoroidal administration resulted in much greater targeted levels of axitinib in retinal and choroidal tissues, with lower levels in the vitreous and anterior segment, which could minimize the risk of off-target effects.65
Durasert
The Durasert™ Bioerodible TKI (EyePoint Pharmaceuticals; Watertown, MA, USA) is a sustained-release implant that delivers vorolanib, a TKI, which was previously assessed in an oral formulation by another sponsor. IND-enabling studies with the Durasert implant are in progress.67
Gene Therapy
The eye has become a target for investigational gene therapy due to the monogenic nature of many inherited retinal diseases (IRD), its accessibility, tight blood–ocular barrier, the ability to non-invasively monitor for functional and anatomic outcomes, as well as its relative immune privileged state. Gene therapy offers potential for long-term continuous expression of anti-VEGF-A protein with a single administration. Viral vectors are conduits for transferring desired genetic material to host cells. Vectors currently used in ocular gene therapy clinical trials include adeno-associated virus (AAV), small single-stranded DNA viruses of the parvovirus family, and lentivirus, RNA viruses of the retrovirus family. After transduction, the target cells transcribe and translate the viral genetic information into therapeutic protein, which then curbs the pathogenesis of the targeted disease process.68 Previous gene therapy candidates such as rAAV.sFLT-1 (Avalanche Biotechnologies, now known as Adverum Biotechnologies; Redwood City, CA), AAV2-sFLT01 (Sanofi Genzyme; Cambridge, MA), and Retinostat (Oxford Biomedica; Oxford, UK) did not advance into later studies but have paved the way for current candidates, ADVM-022 and RGX-314.58
ADVM-022
Adverum Biotechnologies’ gene therapy product, ADVM-022, utilizes an AAV vector (AAV.7m8) that has been optimized for intravitreal injection of vectors carrying anti-VEGF cDNA, leading to the continuous expression of aflibercept. The Phase 1 OPTIC trial (NCT03748784) is a multi-center, open-label, dose-escalation trial that enrolled 30 patients with nAMD who were good responders to prior anti-VEGF therapy. Interim results were presented at the Angiogenesis, Exudation and Degeneration 2021 virtual meeting. There were four cohorts studied. Cohort 1 (n=6) received a high dose of 6×1011 vector genomes (vg)/eye and a 13-day course of oral steroids, cohort 2 (n=6) received a low dose (2x1011 vg/eye) and a 13-day course of oral steroids, cohort 3 (n=9) received a low dose and a 6-week course of topical steroids, and cohort 4 (n=9) received a high dose and a 6-week course of topical steroids.69
ADVM-022 had a favorable safety profile in all groups, with mild inflammation responsive to steroid drops. Patients were eligible for aflibercept rescue injection if they had an increase in CST >75 μm from baseline, loss of ≥10 letters from baseline attributed to intraretinal or subretinal fluid, or the presence of vision threatening hemorrhage due to nAMD. In cohort 1, which had follow-up of median 86 weeks (range=64–92 weeks), a single intravitreal injection of ADVM-022 resulted in no need for supplemental injections in all six patients. Cohort 2 had a median follow-up of 64 weeks (range=64–68 weeks), and 3/6 patients did not need supplemental injections. Cohort 3 had a median follow-up of 48 weeks (range=32–48 weeks), and 7/9 patients did not need supplemental injections. Cohort 4 had a follow-up range of 12–24 weeks, and 8/9 patients did not need supplemental injections. Mean BCVA was maintained and CST was maintained or improved in all groups. The phase 2 Pivotal-a and Pivotal-b trials are planned to initiate trials in late 2021, and will compare ADVM-022 against aflibercept given every 8 weeks in treatment-naïve nAMD patients.70
RGX-314
Regenxbio (Rockville, MD) has developed a novel AAV8 vector, RGX-314, which expresses a soluble anti-VEGF monoclonal antibody fragment, similar to ranibizumab, in transduced retinal cells. The company advocates that their proprietary gene delivery platform (NAV® Technology Platform) may yield higher levels of anti-VEGF expression than earlier generation AAV vectors.71
In the phase 1/2a trial (NCT03066258), RGX-314 was administered via subretinal injection during vitrectomy. Forty-two patients with severe wet AMD requiring frequent anti-vascular endothelial growth factor (anti-VEGF) injections were treated across five dose cohorts, with doses ranging from 3×109 GC/eye to 2.5×1011 GC/eye. New data were reported at the Angiogenesis, Exudation, and Degeneration 2021 conference from Cohort 4 and 5 of RGX-314 Phase I/IIa trial for nAMD and Cohort 3 of its Long-Term Follow-Up study. The data demonstrates potential continued treatment effect out to 3 years. As of January 22, 2021, there was a meaningful reduction in anti-VEGF treatment burden in both Cohorts 4 and 5 as well as stable VA and decreased CST (mean change of −46 µm and −93 µm, respectively). When compared to the mean annualized injection rate during the 12 months prior to RGX-314 administration, patients in Cohort 4 received a mean of 4.4 injections over 1.5 years after RGX-314 administration, and those in Cohort 5 received a mean of 1.7 injections over that time span (a decrease in anti-VEGF treatment burden of 58.3% and 81.2%, respectively). A number of study patients continued into the Long-Term Follow-Up study (NCT03999801) to assess safety up to 5 years after RGX-314 administration, and as of late January 2021 these patients have largely shown no new drug-related ocular adverse events. Over a 3-year period, all six patients from Cohort 3 of the Phase 1/2a trial enrolled in the LTFU study demonstrated a mean BCVA improvement of +12 letters from baseline, and retinal anatomy remained stable at 3 years compared to at 2 years. These patients have also shown a long-term reduction in anti-VEGF treatment burden over the 3-year period, with four out of the six patients receiving no anti-VEGF injections from 9 months to 3 years after RGX-314 administration.72
The long-term data from dose-escalation in Phase 1/2a trials have allowed for further advancement in clinical trials for this potential gene therapy for the treatment of wet AMD. Regenxbio has announced the first of two planned phase 2b/3 trials, ATMOSPHERE (NCT04704921), to evaluate safety and efficacy of RGX-314. The goal is enrollment of approximately 700 patients with nAMD. In one trial the patients will be enrolled across two RGX-314 dose arms versus ranibizumab with primary endpoint being non-inferiority to ranibizumab based on BCVA at 1 year. The second trial, in a similar fashion, will be compared against aflibercept. Both trials are expected to begin dosing patients in 2021. The phase 2 AAVIATE trial (NCT 0454653) is currently enrolling nAMD patients for the evaluation of two dose arms of suprachoroidal injection of RGX-314, which will be compared against monthly ranibizumab injections.73
Discussion
The development of anti-VEGF therapy has significantly changed the landscape for nAMD management. Landmark trials such as the ANCHOR study demonstrated superiority of anti-VEGF injections over photodynamic therapy for preserving and recovering visual acuity.74 The currently available anti-VEGF-A medications in North America include bevacizumab, ranibizumab, aflibercept and brolucizumab. While these medications have drastically improved visual outcomes for nAMD patients globally, there remains a need for new drugs and delivery systems to address the shortcomings of anti-VEGF treatment.
Drugs in the pipeline aim to achieve broad VEGF inhibition, often through TKIs, or to modulate synergistic targets such as Ang-2, PDGF, VEGF-C, and VEGF-D with hopes of outperforming anti-VEGF-A monotherapy. Other drugs utilize sustained release therapy and nanoparticle technology in order to extend the duration of the anti-VEGF effect. Topical anti-VEGF therapies have been developed with hopes to reduce the burden of frequent injections. Gene therapy could serve as a one-time treatment by using the retina’s own cellular apparatus to continuously express anti-VEGF molecules.
The management of nAMD can be burdensome for physicians, patients, families, and the healthcare system. The current paradigm requires an indefinite length of treatment in many cases, and patients need to be counseled that maintaining stable vision (as opposed to achieving visual gains) is still considered a success given the degenerative nature of the disease. In general, real-world outcomes of anti-VEGF treatment do not live up to those obtained in clinical trials due to inadequate numbers of injections to optimize visual gains.28,75 The “treat-and-extend” regimen, in which injections are gradually spaced out further apart until a recurrence of fluid occurs, has gained popularity in attempt to reduce the treatment burden of frequent injections. This regimen appears to perform relatively well in practice based on results of the LUCAS, TREX-AMD, and TREND trials.76–78
Given the unparalleled economic value of bevacizumab compared to other anti-VEGF treatments, it seems likely that it would continue to be a popular first line treatment for most VEGF-mediated diseases globally, with the newly-approved products of the future being utilized more often in refractory cases or in patients in need of longer duration therapy. As biosimilars for aflibercept and ranibizumab become approved and more widely available, they may rival bevacizumab as the most cost-effective first line treatment option.
Anti-VEGF/anti-PDGF combination therapy initially appeared like a promising strategy to address the treatment ceiling of anti-VEGF therapy, however results of the trials of intravitreal rinucumab/aflibercept and pegpleranib/ranibizumab failed to show any advantage over anti-VEGF monotherapy.35,36 Similarly, topical anti-VEGF/anti-PDGF therapies for nAMD so far have been unsuccessful in reducing the need for rescue intravitreal injections, as evidenced by the trials of squalamine lactate, pazopanib, and regorafenib.58,79,80 Based on the early promising results of the phase 1/2 trial, topical PAN90806 could have a possible role for nAMD patients with mild fluid as monotherapy, as an adjuvant to intravitreal anti-VEGF therapy for refractory cases, or as chronic maintenance after loading injections.
In 2019, brolucizumab became the first anti-VEGF drug approved for 12-week dosing. Similarly, abicipar showed promise as a possible 12-week treatment option. However, the issue of increased intraocular inflammation with both of these drugs compared to other anti-VEGF options has hampered their widespread use. In the case of brolucizumab, rare but severe cases of occlusive retinal vasculitis were reported after it became commercially available.11 The Research and Safety in Therapeutics (ReST) committee of the American Society of Retina Specialists (ASRS) has been working with Novartis in tracking the data, which as of June 2020 demonstrate incidence of retinal vasculitis to be 8.65 per 10,000 injections. Data reported at the American Academy of Ophthalmology meeting in November 2020 cited 26 eyes of 25 patients with retinal vasculitis in which vision loss was more severe, with 35% of eyes losing six lines of vision or more without recovery.81 Currently the FDA has not advised against use of brolucizumab, while they work with the ASRS to closely monitor these reports of intraocular inflammation.
Clinical research has continued to broaden the physiological scope of drug development to include medications that upregulate Tie-2 receptor functioning, including nesvacumab, faricimab, and ARP-1536. Of these, nesvacumab did not show sufficiently promising results in Phase 2 trials for further advancement.82 Faricimab is the furthest under development and is differentiated by its unique bispecific antibody design that targets VEGF and Ang-2. In the phase 2 STAIRWAY trial, it showed promising results with visual gains comparable to monthly dosing of ranibizumab with 12- and 16-week dosing of faricimab. Phase 3 trials (LUCERNE and TENAYA) comparing a flexible dosing regimen of faricimab (up to 16-week dosing) against aflibercept every 8 weeks are expected to have results in 2022.
The ranibizumab Port Delivery System is the furthest sustained-release anti-VEGF therapy in development. The phase 3 Archway Study is expected to conclude in 2022; interim results indicate that 98% of patients were able to go 6 months without additional treatment while maintaining visual acuity comparable to the monthly ranibizumab group.61 The need for surgery to implant the refillable port, with higher risk of complications compared to intravitreal injection, may be a deterring factor for some patients. While GB-102 showed an impressive durability and safety profile in its phase 2b trial, it is unclear why patients randomized to GB-102 gained 9 less letters compared to those receiving aflibercept, and this will need to be explored further in a larger scale trial.
Gene therapy with viral vectors could represent the ultimate form of sustained anti-VEGF treatment, as the retina develops its own anti-VEGF biofactory that would diminish the need for subsequent intravitreal injections. While there have been several gene therapy candidates in the past, currently ADVM-022 and RGX-314 are the two that are primed for phase 2 trials in the near future.
In summary, the pathogenesis of nAMD is multifaceted and includes an array of factors that could be targeted in future treatments. Emerging therapies that target alternative pathways, along with novel anti-VEGF therapies that provide extended durability, will provide the retina community with better options for refractory nAMD and reduce the need for monthly injections in many patients.
Disclosure
Dr Audina M. Berrocal reports personal fees, DORC, ALCON, ProQR, AGTC, Novartis, during the conduct of the study. Dr. Rehan Hussain has served on an advisory board for Alimera Sciences. Dr. Jayanth Sridhar is a consultant for Alcon, DORC, Genentech, Regeneron, and Oxurion. The authors report no other conflicts of interest in this work.
References
1. Friedman DS, O’Colmain BJ, Munoz B, et al. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol. 2004;122(4):564–572.
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–116. doi:10.1016/S2214-109X(13)70145-1
3. Ferris FL
4. Gass JD. Pathogenesis of disciform detachment of the neuroepithelium: i. General concepts and classification. Am J Ophthalmol. 1967;63(3,Part 2):
5. Green WR, Enger C. Age-related macular degeneration histopathologic Studies: the 1992 Lorenz E. Zimmerman Lecture. Ophthalmology. 1993;100(10):1519–1535. doi:10.1016/S0161-6420(93)31466-1
6. Leung D, Cachianes G, Kuang W, Goeddel D, Ferrara N. Vascular endothelial growth factor is a secreted angiogenic mitogen. Science. 1989;246(4935):1306–1309. doi:10.1126/science.2479986
7. Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS, Dvorak HF. Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science. 1983;219(4587):983–985. doi:10.1126/science.6823562
8. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
9. Smith AG, Kaiser PK. Emerging treatments for wet age-related macular degeneration. Expert Opin Emerg Drugs. 2014;19(1):157–164. doi:10.1517/14728214.2014.884559
10. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
11. Baumal CR, Spaide RF, Vajzovic L, et al. Retinal vasculitis and intraocular inflammation after intravitreal injection of brolucizumab. Ophthalmology. 2020;127(10):1345–1359. doi:10.1016/j.ophtha.2020.04.017
12. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
13. Barthelmes D, Nguyen V, Daien V, et al. Two year outcomes of “Treat and Extend” intravitreal therapy using aflibercept preferentially for neovascular age-related macular degeneration. Retina. 2018;38(1):20–28.
14. Arevalo JF, Lasave AF, Wu L, et al. Intravitreal bevacizumab for choroidal neovascularization in age-related macular degeneration: 5-year results of the pan-american collaborative retina Study Group. Retina. 2016;36(5):859–867. doi:10.1097/IAE.0000000000000827
15. Cohen SY, Mimoun G, Oubraham H, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the LUMIERE study. Retina. 2013;33(3):474–481. doi:10.1097/IAE.0b013e31827b6324
16. Hjelmqvist L, Lindberg C, Kanulf P, Dahlgren H, Johansson I, Siewert A. One-year outcomes using ranibizumab for neovascular age-related macular degeneration: results of a prospective and retrospective observational multicentre study. J Ophthalmol. 2011;2011:405724. doi:10.1155/2011/405724
17. Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99(2):220–226. doi:10.1136/bjophthalmol-2014-305327
18. Kruger Falk M, Kemp H, Sorensen TL. Four-year treatment results of neovascular age-related macular degeneration with ranibizumab and causes for discontinuation of treatment. Am J Ophthalmol. 2013;155(1):89–95 e83. doi:10.1016/j.ajo.2012.06.031
19. Rakic JM, Leys A, Brie H, et al. Real-world variability in ranibizumab treatment and associated clinical, quality of life, and safety outcomes over 24 months in patients with neovascular age-related macular degeneration: the HELIOS study. Clin Ophthalmol. 2013;7:1849–1858.
20. Rasmussen A, Bloch SB, Fuchs J, et al. A 4-year longitudinal study of 555 patients treated with ranibizumab for neovascular age-related macular degeneration. Ophthalmology. 2013;120(12):2630–2636. doi:10.1016/j.ophtha.2013.05.018
21. Souied EH, Oubraham H, Mimoun G, et al. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: the TWIN Study. Retina. 2015;35(9):1743–1749. doi:10.1097/IAE.0000000000000548
22. Talks JS, Lotery AJ, Ghanchi F, et al. First-year visual acuity outcomes in the united kingdom of providing aflibercept according to the view study protocol for age-related macular degeneration. Ophthalmology. 2015;123(2):337–343. doi:10.1016/j.ophtha.2015.09.039
23. van Asten F, Evers-Birkenkamp KU, van Lith-verhoeven JJ, et al. A prospective, observational, open-label, multicentre study to investigate the daily treatment practice of ranibizumab in patients with neovascular age-related macular degeneration. Acta Ophthalmol. 2015;93(2):126–133. doi:10.1111/aos.12610
24. Writing Committee for the U. K. Age-related macular degeneration E. M. R. Users Group. The neovascular age-related macular degeneration database: multicenter study of 92 976 ranibizumab injections: report 1: visual acuity. Ophthalmology. 2014;121(5):1092–1101. doi:10.1016/j.ophtha.2013.11.031
25. Zarranz-Ventura J, Liew G, Johnston RL, et al. The neovascular age-related macular degeneration database: report 2: incidence, management, and visual outcomes of second treated eyes. Ophthalmology. 2014;121(10):1966–1975. doi:10.1016/j.ophtha.2014.04.026
26. Ross AH, Donachie PH, Sallam A, et al. Which visual acuity measurements define high-quality care for patients with neovascular age-related macular degeneration treated with ranibizumab? Eye (Lond). 2013;27(1):56–64. doi:10.1038/eye.2012.225
27. Rao P, Lum F, Wood K, et al. Real-world vision in age-related macular degeneration patients treated with single anti-VEGF drug type for 1 year in the IRIS Registry. Ophthalmology. 2018;125(4):522–528. doi:10.1016/j.ophtha.2017.10.010
28. Ciulla TA, Hussain RM, Pollack JS, Williams DF. Visual acuity outcomes and anti-vascular endothelial growth factor therapy intensity in neovascular AMD patients: a “Real World” analysis in 49,485 eyes. Ophthalmol Retina. 2020;4(1):19–30. doi:10.1016/j.oret.2019.05.017
29. Mehta H, Tufail A, Daien V, et al. Real-world outcomes in patients with neovascular age-related macular degeneration treated with intravitreal vascular endothelial growth factor inhibitors. Prog Retin Eye Res. 2018;65:127–146. doi:10.1016/j.preteyeres.2017.12.002
30. Dadgostar H, Ventura AA, Chung JY, Sharma S, Kaiser PK. Evaluation of injection frequency and visual acuity outcomes for ranibizumab monotherapy in exudative age-related macular degeneration. Ophthalmology. 2009;116(9):1740–1747. doi:10.1016/j.ophtha.2009.05.033
31. Hussain RM, Hariprasad SM, Ciulla TA. Treatment burden in neovascular amd:visual acuity outcomes are associated with anti-VEGF injection frequency. Ophthalmic Surg Lasers Imaging Retina. 2017;48(10):780–784. doi:10.3928/23258160-20170928-01
32. Kim LN, Mehta H, Barthelmes D, Nguyen V, Gillies MC. Metaanalysis of real-world outcomes of intravitreal ranibizumab for the treatment of neovascular age-related macular degeneration. Retina. 2016;36(8):1418–1431. doi:10.1097/IAE.0000000000001142
33. Daniel E, Toth CA, Grunwald JE, et al. Risk of scar in the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2014;121(3):656–666. doi:10.1016/j.ophtha.2013.10.019
34. Cabral T, Lima LH, Mello LGM, et al. Bevacizumab injection in patients with neovascular age-related macular degeneration increases angiogenic biomarkers. Ophthalmol Retina. 2018;2(1):31–37. doi:10.1016/j.oret.2017.04.004
35. Jaffe GJ, Ciulla TA, Ciardella AP, et al. Dual Antagonism of PDGF and VEGF in neovascular age-related macular degeneration: a phase IIb, multicenter, randomized controlled Trial. Ophthalmology. 2017;124(2):224–234. doi:10.1016/j.ophtha.2016.10.010
36. Dunn EN, Hariprasad SM, Sheth VS. An overview of the fovista and rinucumab trials and the fate of anti-PDGF medications. Ophthalmic Surg Lasers Imaging Retina. 2017;48(2):100–104. doi:10.3928/23258160-20170130-02
37. Hussain RM, Neiweem AE, Kansara V, Harris A, Ciulla TA. Tie-2/Angiopoietin pathway modulation as a therapeutic strategy for retinal disease. Expert Opin Investig Drugs. 2019;28(10):861–869. doi:10.1080/13543784.2019.1667333
38. Al-Khersan H, Hussain RM, Ciulla TA, Dugel PU. Innovative therapies for neovascular age-related macular degeneration. Expert Opin Pharmacother. 2019;20(15):1879–1891. doi:10.1080/14656566.2019.1636031
39. Hussain RM, Weng CY, Wykoff CC, Gandhi RA, Hariprasad SM. Abicipar pegol for neovascular age-related macular degeneration. Expert Opin Biol Ther. 2020;20(9):999–1008. doi:10.1080/14712598.2020.1782379
40. The FDA does not approve allergan’s wet AMD drug candidate Abicipar Pegol [press release]. Eyewire News; 2020.
41. Dugel PU, Boyer DS, Antoszyk AN, et al. Phase 1 Study of OPT-302 inhibition of vascular endothelial growth factors C and D for neovascular age-related macular degeneration. Ophthalmol Retina. 2020;4(3):250–263. doi:10.1016/j.oret.2019.10.008
42. Opthea meets primary endpoint in Phase 2b Study of OPT-302 in Wet AMD [press release]; 2019.
43. Helzner J. Opthea Cleared for 2 Phase 3 Trials in Wet AMD 17(July/August 2020); August 21, 2021. Available from: https://www.retinalphysician.com/issues/2020/july-august-2020/opthea-cleared-for-2-phase-3-trials-in-wet-amd.
44. Liu K, Song Y, Xu G, et al. Conbercept for treatment of neovascular age-related macular degeneration: results of the randomized Phase 3 PHOENIX Study. Am J Ophthalmol. 2019;197:156–167. doi:10.1016/j.ajo.2018.08.026
45. Efficacy and safety trial of conbercept intravitreal injection for neovascular age-related macular degeneration (PANDA-1). Available from: https://clinicaltrials.gov/ct2/show/NCT03577899.
46. Efficacy and Safety Trial of Conbercept Intravitreal Injection for Neovascular Age-related Macular Degeneration (PANDA-2). Available from: https://clinicaltrials.gov/ct2/show/NCT03630952.
47. Rai-Roche S. LoA Update: chengdu Kanghong Pharmaceuticals’ Phase III ophthalmic agent drops 7 points in AMD after trial stop; April 16, 2021. Available from: https://www.clinicaltrialsarena.com/comment/loa-update-chengdu-kanghong-pharmaceuticals-phase-iii-ophthalmic-agent-drops-7-points/.
48. Samanta A, Aziz AA, Jhingan M, Singh SR, Khanani AM, Chhablani J. Emerging therapies in neovascular age-related macular degeneration in 2020. Asia Pac J Ophthalmol (Phila). 2020;9(3):250–259. doi:10.1097/APO.0000000000000291
49. Kodiak announces 1-year durability, efficacy and safety data from ongoing phase 1b Study of KSI-301 in patients with wet AMD, DME and RVO at angiogenesis; 2021. Available from: https://kodiak.com/press-releases/kodiakannounces-1-year-durability-efficacy-and-safety-data-from-ongoing-phase-1b-study-of-ksi-301-in-patients-with-wet-amd-dme-and-rvo-at-angiogenesis-2021/.
50. A Phase IIb/III, prospective, randomized, double-masked, active comparator-controlled, multi-center study to investigate the efficacy and safety of repeated intravitreal administration of KSI-301 in subjects with neovascular (wet) age-related macular degeneration. Available from: https://clinicaltrials.gov/ct2/show/NCT04049266.
51. Davis S, Yancopoulos GD. The angiopoietins: yin and Yang in angiogenesis. Curr Top Microbiol Immunol. 1999;237:173–185. doi:10.1007/978-3-642-59953-8_9
52. Bhattacharya D, Chaudhuri S, Singh MK, Chaudhuri S. T11TS inhibits Angiopoietin-1/Tie-2 signaling, EGFR activation and Raf/MEK/ERK pathway in brain endothelial cells restraining angiogenesis in glioma model. Exp Mol Pathol. 2015;98(3):455–466. doi:10.1016/j.yexmp.2015.03.026
53. Hansen TM, Singh H, Tahir TA, Brindle NP. Effects of angiopoietins-1 and −2 on the receptor tyrosine kinase Tie2 are differentially regulated at the endothelial cell surface. Cell Signal. 2010;22(3):527–532. doi:10.1016/j.cellsig.2009.11.007
54. Fachinger G, Deutsch U, Risau W. Functional interaction of vascular endothelial-protein-tyrosine phosphatase with the Angiopoietin receptor Tie-2. Oncogene. 1999;18(43):5948. doi:10.1038/sj.onc.1202992
55. Helzner J. Faricimab Shows potential for 16-week dosing. Retinal Physician. 2018. Available from: https://www.retinalphysician.com/issues/2018/september-2018/faricimab-shows-potential-for-16-week-dosing. Published 9-1-2018.
56. Khanani AM, Patel SS, Ferrone PJ, et al. Efficacy of every four monthly and quarterly dosing of faricimab vs ranibizumab in neovascular age-related macular degeneration: the STAIRWAY Phase 2 Randomized Clinical Trial. JAMA Ophthalmol. 2020;138(9):964–972. doi:10.1001/jamaophthalmol.2020.2699
57. New phase III data show Roche’s faricimab is the first investigational injectable eye medicine to extend time between treatments up to four months in two leading causes of vision loss, potentially reducing treatment burden for patients;
58. Al-Khersan H, Hussain RM, Ciulla TA, Dugel PU. Innovative therapies for neovascular age-related macular degeneration. Expert Opin Pharmacother. 2019;20(15):1879–1891.
59. Chaney P. PAN-90806: once-daily topical anti-VEGF eye drop for wet AMD and other neovascular eye disease.
60. Campochiaro PA, Marcus DM, Awh CC, et al. The port delivery system with ranibizumab for neovascular age-related macular degeneration: results from the Randomized Phase 2 Ladder Clinical Trial. Ophthalmology. 2019;126(8):1141–1154. doi:10.1016/j.ophtha.2019.03.036
61. Phase 3 data show port delivery system with ranibizumab enabled over 98% of patients to go 6 months between treatments for wet AMD; July 22, 2020. Available from: https://eyewire.news/articles/phase-3-data-show-port-delivery-system-with-ranibizumab-enabled-over-98-of-patients-to-go-6-months-between-treatments-for-wet-amd/.
62. Graybug vision presents top line results of Phase 1/2a ADAGIO Study at Hawaiian Eye & Retina; 2019. Available from: https://graybug.com/graybug-vision-presents-top-line-results-of-phase-1-2a-adagio-study-at-hawaiian-eye-retina-2019/.
63. Delaney-Gesing A. Graybug Vision releases preliminary topline results of Phase 2b ALTISSIMO trial. Ophthalmology Times; March 3, 2021. Available from: https://www.ophthalmologytimes.com/view/graybug-vision-releases-preliminary-topline-results-of-phase-2b-altissimo-trial..
64. Ocular Therapeutix: focused on the Future. Available from: https://www.ocutx.com/research/pipeline/.
65. Wan CR, Muya L, Kansara V, Ciulla TA. Suprachoroidal delivery of small molecules, nanoparticles, gene and cell therapies for ocular diseases. Pharmaceutics. 2021;13(2):288. doi:10.3390/pharmaceutics13020288
66. Yeh S, Khurana RN, Shah M, et al. Efficacy and safety of suprachoroidal CLS-TA for macular edema secondary to noninfectious uveitis: phase 3 Randomized Trial. Ophthalmology. 2020;127(7):948–955. doi:10.1016/j.ophtha.2020.01.006
67. EyePoint pharmaceuticals product pipeline. Available from: https://eyepointpharma.com/pipeline/#4.
68. Moore NA, Bracha P, Hussain RM, Morral N, Ciulla TA. Gene therapy for age-related macular degeneration. Expert Opin Biol Ther. 2017;17(10):1235–1244. doi:10.1080/14712598.2017.1356817
69. Khanani AM Intravitreal gene therapy for exudative AMD and diabetic retinopathy.
70. Advancing novel gene therapies. Available from: https://adverum.com/pipeline/#section-03.
71. Hussain RM, Ciulla TA. Emerging vascular endothelial growth factor antagonists to treat neovascular age-related macular degeneration. Expert Opin Emerg Drugs. 2017;22(3):235–246. doi:10.1080/14728214.2017.1362390
72. Regenxbio announces additional positive interim phase I/IIA and long-term follow-up data of RGX-314 for the treatment of wet AMD; 2021 [February 16, 2021]. Available from: http://ir.regenxbio.com/news-releases/news-release-details/regenxbio-announces-additional-positive-interim-phase-iiia-and.
73. REGENXBIO announces update on RGX-314 and pivotal program for the treatment of wet AMD and new gene therapy program for the treatment of duchenne muscular dystrophy; 2021 [Updated January 5, 2021]. Available from: https://www.prnewswire.com/news-releases/regenxbio-announces-update-on-rgx-314-and-pivotal-program-for-the-treatment-of-wet-amd-and-new-gene-therapy-program-for-the-treatment-of-duchenne-muscular-dystrophy-301201378.html.
74. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
75. Ciulla TA, Bracha P, Pollack J, Williams DF. Real-world outcomes of anti-vascular endothelial growth factor therapy in diabetic macular edema in the United States. Ophthalmol Retina. 2018;2(12):1179–1187. doi:10.1016/j.oret.2018.06.004
76. Berg K, Pedersen TR, Sandvik L, Bragadottir R. Comparison of ranibizumab and bevacizumab for neovascular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology. 2015;122(1):146–152. doi:10.1016/j.ophtha.2014.07.041
77. Wykoff CC, Croft DE, Brown DM, et al. Prospective trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: TREX-AMD 1-year results. Ophthalmology. 2015;122(12):2514–2522. doi:10.1016/j.ophtha.2015.08.009
78. Silva R, Berta A, Larsen M, et al. Treat-and-extend versus monthly regimen in neovascular age-related macular degeneration: results with Ranibizumab from the TREND Study. Ophthalmology. 2018;125(1):57–65. doi:10.1016/j.ophtha.2017.07.014
79. Joussen AM, Wolf S, Kaiser PK, et al. The developing regorafenib eye drops for neovascular age-related macular degeneration (DREAM) study: an open-label Phase II trial. Br J Clin Pharmacol. 2019;85(2):347–355. doi:10.1111/bcp.13794
80. Csaky KG, Dugel PU, Pierce AJ, et al. Clinical evaluation of pazopanib eye drops versus ranibizumab intravitreal injections in subjects with neovascular age-related macular degeneration. Ophthalmology. 2015;122(3):579–588. doi:10.1016/j.ophtha.2014.09.036
81. ReST committee provides update on brolucizumab. Ocular Surgery News; November 15, 2020. Available from: https://www.healio.com/news/ophthalmology/20201115/rest-committee-provides-update-on-brolucizumab.
82. Eylea, nesvacumab combination trials will not continue. Ocular Surgery News; November 27, 2017. Available from: https://www.healio.com/news/ophthalmology/20171127/eylea-nesvacumab-combination-trials-will-not-continue.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.