")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
Utility of SpeedCourt System: A Novel Study of 100 Professional Footballers at FIFA Medical Centre of Excellence Dubai UAE
Authors Ghrairi M, Dalal S , Esteban-García E , Chomier P , Valle X, Pruna R
Received 11 September 2023
Accepted for publication 17 October 2023
Published 31 October 2023 Volume 2023:14 Pages 79—87
DOI https://doi.org/10.2147/OAJSM.S434554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Mourad Ghrairi,1,2 Shaival Dalal,3 Esther Esteban-García,4 Philippe Chomier,5 Xavier Valle,2 Ricard Pruna2
1Department of Sports Medicine, FIFA Medical Centre of Excellence, Dubai, United Arab Emirates; 2Department of Sports Medicine, FIFA Medical Centre of Excellence FC Barcelona, Barcelona, Spain; 3Department of Orthopedics and Sports Medicine, Arthro One Sports Injuries and Rehabilitation Centre, Ahmedabad, Gujarat, India; 4Department of Physiotherapy, FIFA Medical Centre of Excellence, Dubai, United Arab Emirates; 5Department of Rehabilitation, FIFA Medical Centre of Excellence, Dubai, United Arab Emirates
Correspondence: Shaival Dalal, Arthro One Orthopaedic Centre, 4th Floor, NIRAMYA, Near Rajpath Club, Bodakdev, Ahmedabad, 380054, India, Tel +91-9904915211, Email [email protected]
Purpose: The SpeedCourt system has been confirmed as an effective and dependable tool for evaluating multi-directional change-of-direction (COD) maneuvers. It has also been employed in the rehabilitation process following Anterior Cruciate Ligament (ACL) injuries and for multi-directional training purposes. This study investigated by means of the SpeedCourt system determines 1) whether there is any difference in COD parameters and countermovement jumps (CMJ) between United Arab Emirates (UAE) and non-UAE professional footballers 2) whether there is any difference between the two lower limbs during change-of-direction manoeuvres.
Methodology: This analysis included 100 professional football players from UAE or Non-UAE football clubs who were tested at FIFA Medical Centre of Excellence. With the help of Speedcourt system, 6-s tapping, countermovement jump (CMJ) and chase 15-s tests were performed. Comparison was done between UAE and non-UAE footballers and also between the dominant and non-dominant sides.
Results: Out of the 100 players, 83 players were right foot dominant. Apart from the countermovement jump test, there was no significant difference in results between UAE and non-UAE football players. Average time to turn for dominant and non-dominant sides did not show any significant difference, for either group.
Conclusion: There is no difference in 6-s tapping, Chase 15-s tests or limb asymmetry amongst UAE and Non-UAE footballers. However, the non-UAE footballers showed significantly better performance in Countermovement Jump Test. The data provide baseline values for forthcoming sports medicine research, which can be taken into account when creating injury prevention or return-to-sport protocols, particularly with regard to change of direction parameters and countermovement jump.
Keywords: Speedcourt, rehabilitation, prevention, countermovement
Introduction
Team sports such as football are linked to a heightened risk of significant knee injuries that occur without direct contact with another player.1 These sports are particularly susceptible to high-risk movements during matches, notably side-cuts and multi-directional manoeuvers.2 One of these movements, the stop phase, bears the highest risk of Anterior Cruciate Ligament (ACL) injury of all side-cutting phases.3 As a result, there is a demand for clinical tools aimed at recognizing potential risk factors and pinpointing athletes who are at an elevated risk of experiencing a severe knee injury, thus preventing a potential knee injury. Unexpected disturbance rehabilitation program with response below 200 milliseconds (ms) has been shown to be advantageous in terms of injury prevention and rehabilitation.4 The SpeedCourt system (Globalspeed GmbH, Hemsbach, Germany) has been confirmed as a valuable and dependable tool for evaluating multi-directional change-of-direction maneuvers.5 It has also found application in the rehabilitation process following ACL injuries and in multi-directional sprint training.6 When athletes repeatedly perform precise and rapid movements characteristic of their sport over extended periods, their bodies undergo specific adaptations to handle these demands, which often result in asymmetrical load distribution. For example, in football, the dominant shooting leg bears a significant portion of the load during gameplay. Such asymmetry or limb dominance has been described with conflicting evidence as a major risk factor for sustaining knee injury.2,7
The Countermovement Jump (CMJ) has proven to be a valuable tool for monitoring the effects of various training programs (strength, endurance, speed, and plyometric) and assessing mechanical and neuromuscular fatigue in both individual and team sports.8 Researchers have found that CMJ performance serves as an objective indicator of athlete fatigue and overcompensation, and it has also been linked to a higher risk of lower extremity muscle injuries.9 Moreover, studies have identified a connection between the decrease in CMJ mechanical variables, such as jump height, and metabolic markers like lactate or ammonium levels during sprinting.10 This suggests that monitoring CMJ height loss can provide valuable insights into muscle fatigue, metabolic stress, and athlete workload, ultimately contributing to injury prevention.10
This study utilized the SpeedCourt system to examine and assess 1) whether there is any difference in Change of Direction (COD) parameters and Countermovement jump distance between UAE and non-UAE professional footballers 2) whether there is any difference between the two lower extremities during change-of-direction manoeuvres. This study is the first comprehensive overview of baseline values within a standardized testing environment for professional football players.
Materials and Methods
This analysis included 100 professional football players (Table 1) from UAE or Non-UAE football clubs who were tested at FIFA Medical Centre of Excellence. Anthropometric and medical information, encompassing factors such as age, height, body weight, and limb dominance, were evaluated using a standardized questionnaire.
 |
Table 1 Patient Demographics |
SpeedCourt System
The SpeedCourt system comprises a 5.0×5.0 m platform equipped with 12 contact sensor plates arranged symmetrically (Figure 1). Each of these sensor plates responds to a minimum force of 150 N, enabling precise detection of contact times in milliseconds. The eight peripheral plates measure 34.5 by 34.5 cm and the four central plates 30.0 by 30.0 cm.
 |
Figure 1 Speedcourt System consisting of a platform (5.0 × 5.0 m) with 12 contact sensor plates positioned in symmetrical order. |
The sensor plate distribution is highlighted on a large screen hung on the wall for perfect visualization, therefore indicating the running direction path to the player by a lighting system.
Test Protocol (Table 2)
All players underwent identical test protocol, and they were already acquainted with the Speedcourt system prior to the tests. Additionally, the players participated in a standardized warm-up regimen, which involved light running and a series of progressive sprints. All the tests were conducted using running shoes and comfortable sports clothes.
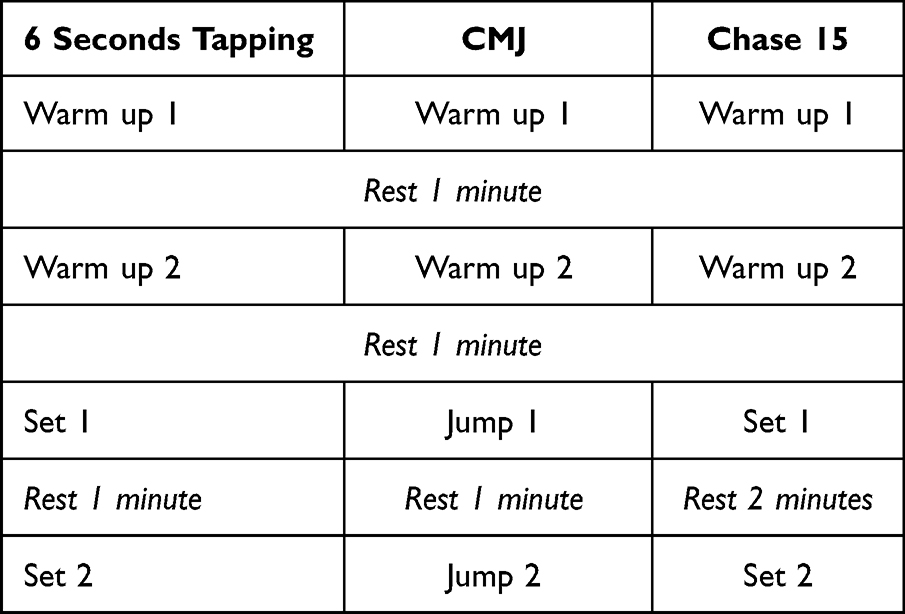 |
Table 2 Speedcourt Testing Protocol |
The following parameters were analysed (Table 3):
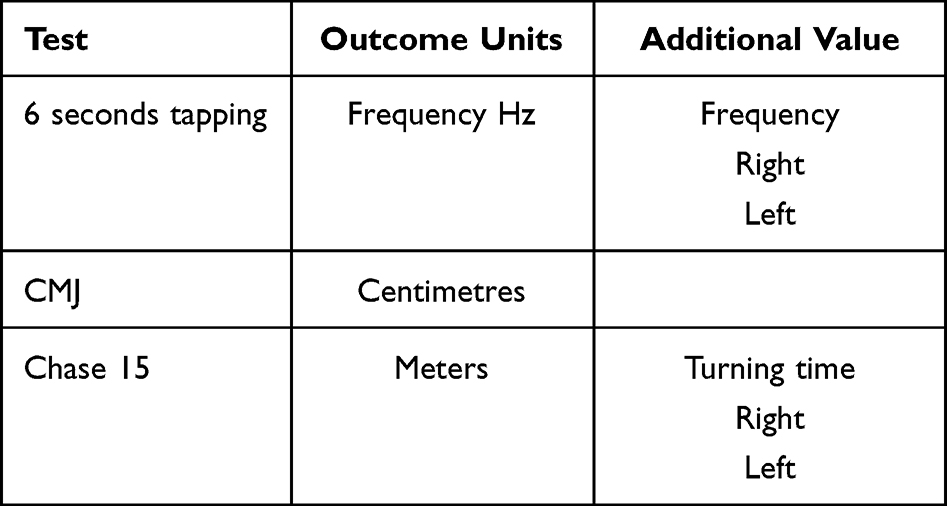 |
Table 3 Speedcourt Outcome Parameters |
Two trials will be performed before the two official tests and the highest frequency will be recorded.
 |
Figure 2 Player performing Chase 15 second test. Informed consent has been taken for the photo from the player. |
Players will perform a trial test at medium speed to understand the test and to ensure perfect performance. Then, the test will be performed for two sets at full speed with a free recovery of 2 min in between the tests.
The best score will be chosen for the records: the longest distance covered and the right and left turning time.
Ethics Consideration
As this is a non-interventional, retrospective study performed on healthy athletes, ethical approval was not needed. This was confirmed by the Ethical Committee-Health and Medical Services Group (HMS), Dubai (Reference number – HMS 20656). Informed consent was taken from all participants, and all guidelines were followed as outlined in the Declaration of Helsinki.
Statistical Analyses
Continuous data were presented in the form of mean values along with their respective standard deviations (SD), while categorical data were represented as frequency counts and percentages. To identify any statistically significant distinctions both between and within groups, a t-test was performed. The significance threshold was established at p < 0.05. All statistical analyses were conducted using IBM SPSS Statistics version 24.0.
Results
Out of the 100 players, eighty-three (83%) players were right leg dominant. The anthropometric data is as shown in Table 1.
6 Second Tapping Test
The average frequency (Hertz (Hz)) in UAE players was 10.4 ± 1.46 Hz, whereas that in non-UAE players was 10.9 ± 1.01 Hz. There was no statistical difference between the two groups (p value 0.16). Figure 3 shows the comparison values with 95% confidence intervals.
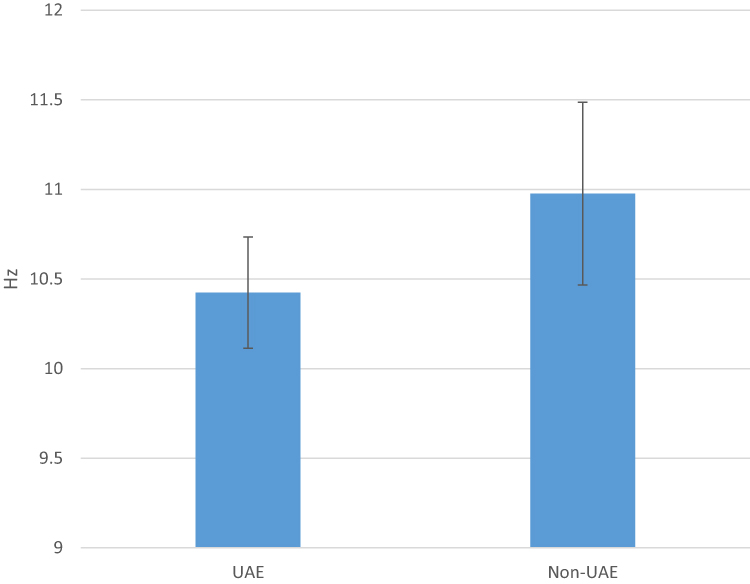 |
Figure 3 Comparison of 6 second tapping test between UAE and non-UAE players. |
Countermovement Jump Test
On comparing the Countermovement Jump distance, the mean distance in UAE players (48.8 cm ± 4.9) was significantly less compared to the mean distance in Non-UAE players (52 cm ± 5.2) (p value-0.02). Figure 4 shows the comparison values with 95% confidence intervals.
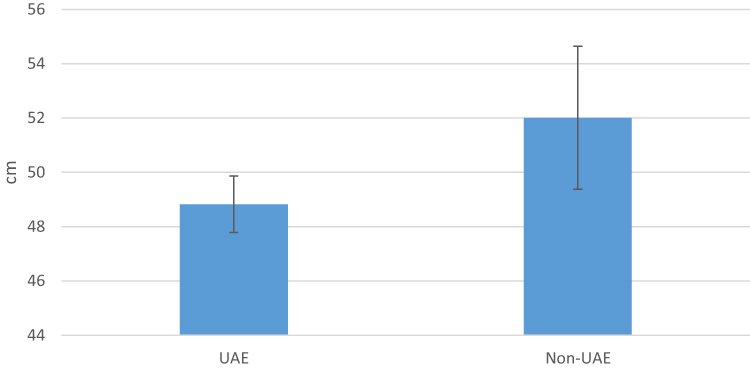 |
Figure 4 Comparison of Countermovement Jump test between UAE and non-UAE players. |
Chase 15 Second Test
Mean distance covered in Chase 15-s test for UAE players was 21.5 m ± 2.9, whereas that covered by Non-UAE players was 21.2 ± 3.4 m. There is no statistical significance between the two groups (p value 0.69). Figure 5 shows the comparison values with 95% confidence intervals.
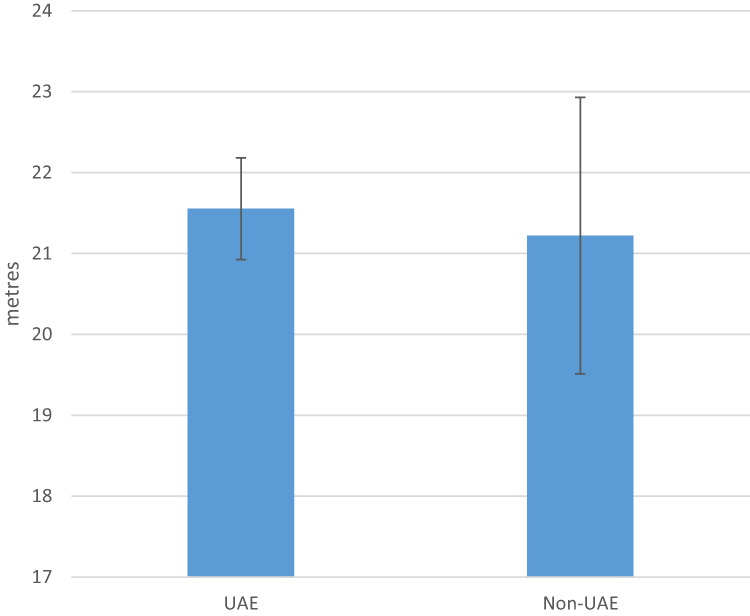 |
Figure 5 Comparison of 15 second between UAE and non-UAE players. |
Change of Direction Parameters
Average time taken to turn on dominant and non-dominant sides for UAE and non-UAE players is as shown in Table 4. There is no significant difference between dominant and non-dominant sides in either group.
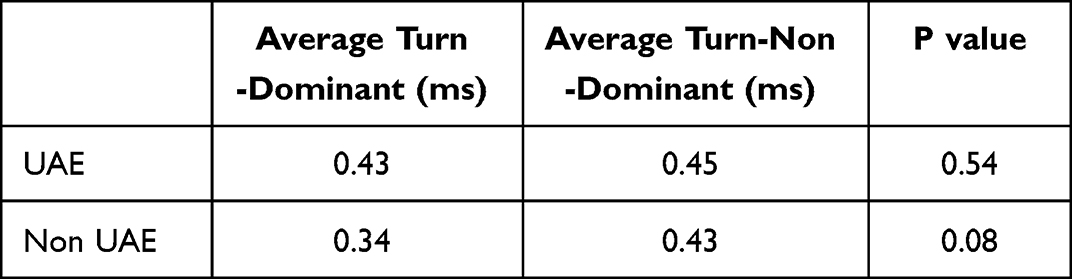 |
Table 4 Comparison of Average Time Taken to Turn on Dominant and Non-Dominant Side Between UAE and Non-UAE Players |
Discussion
The most important finding of the study was the fact that there is no difference between the 6-s tapping test and Chase 15-s parameters analysed for UAE and non-UAE players, but there is a difference in the Countermovement Jump Distance, with Non-UAE players showing better results compared to UAE players. Furthermore, there is no discernible distinction between the dominant and non-dominant extremities in terms of the time required to pivot in either of the groups. The data can be valuable in comparing the baseline values in a similar cohort of non-injured athletes.
Change-of-direction movements are associated with an increased risk of knee injury, such as ACL tear, and hence this particular aspect should be a primary focus in the decision-making criteria for progression, return-to-sports and return-to-competition after injury.2,11 However, there are no specific recommendations for athletes from different regions amongst sporting populations. Although surgical and rehabilitation techniques have made significant progress in the restoration of knee function, the efforts of sports physicians, physiotherapists, and sport therapists in facilitating the recovery of injured athletes’ normal motor and sensory function have not consistently yielded successful outcomes.12–15 Reports indicate that 20% to 50% of individuals who undergo anterior cruciate ligament (ACL) reconstruction surgery do not return to their pre-surgery level of sports participation. Furthermore, among those who do return to their preinjury sports, a range of 10% to 70% experience reduced performance or significant functional limitations.12–15 The Unexpected-Disturbance rehabilitation Program involving response below 200 ms has shown to significantly improve outcomes including 20-m sprint, 1-repetition-maximum single-leg press, standing long jump, single leg sway and perceived confidence, and is thus an important aspect of return-to-sport decision-making.4 The outcomes of our study, using the Speedcourt system which utilises similar COD parameters, can offer objective insights into the decision-making process regarding when and under what circumstances athletes, especially professional football players, can safely resume sporting activities following injuries like ACL tears or ACL reconstructions. Pre-injury baseline values for each individual player can be used to compare the performance of the same program, of the same player after an injury or surgery. This will serve as an adjunct to making return-to-sport decision along with clinical and other rehabilitation parameters.
Conducting pre-competition screening for healthy athletes can help identify individuals at risk of injury, allowing physicians to implement specialized neuromuscular injury prevention programs. Using this cohort of UAE and non-UAE players, this study aims to establish reliable baseline values for different regions and age groups, benefiting all players.
CMJ (Countermovement Jump) has been recognized as a straightforward, efficient, and widely embraced assessment tool for assessment after ACL injury or reconstruction and for monitoring performance.16,17 Moreover, when considering the impact of sport-specific training methods, CMJ performance has been employed to gauge the outcomes of endurance, strength, plyometric and speed training.8,10,18 Common methods to estimate jump height are based on flight time or vertical reaction force.19 As per the study done by Attia et al, there was a high correlation between the two methods, however the vertical reaction force remained the gold standard method.19 The advantage of the Speedcourt system is that there are 12 sensor plates allowing us to record the CMJ and COD performance with the highest accuracy. In our study, CMJ performance of non-UAE players was significantly better than that of UAE players. Further research and larger numbers will be needed to conclude whether this statistically significant difference extrapolates to any difference in performance and injuries or not.
Unlike numerous clinical tools designed for evaluating athletes in static exercises, the SpeedCourt system offers the capability to assess players during unpredictable, sports-specific change-of-direction movements. This system, which has undergone evaluation for appraising multi-directional change-of-direction maneuvers, is employed by numerous elite sports clubs in Europe.5,20 Notably, this study demonstrated the utility of the recently developed and scientifically examined SpeedCourt system as an effective instrument for the standardized assessment of team sports athletes. This system, in combination with other tests such as isometric hip abductor and adductor strength, eccentric knee flexor strength, CMJ kinetics and single-leg hop kinetics can be used to assess objectively for pre-season assessment and return to play after injury.21,22
The notion of inter-limb asymmetry pertains to how one limb performs in comparison to the other. Our findings align with prior research, underscoring that there is no discernible distinction between the dominant and non-dominant legs.23
This study has several limitations. In addition to the small sample size (n=100), not all age groups have been analysed using this system. The range of the age of the players was from 19 to 40. Moreover, all the players were professional players, and so the data cannot be directly compared to a recreational player or a sedentary person undergoing the test. Comparisons and correlations with clinical tools such as single-leg hop or jump have not been made and remain a subject of further study. The strength of this study is the standardised test setting and sample of athletes belonging to UAE and other regions, which can be used as baseline values for future comparisons. The SpeedCourt system allows reliable, valid and reproducible data, which strengthens the quality of the study. Additional research is necessary to validate the study’s findings. The potential clinical significance of the Speedcourt system can be extrapolated to two main areas:
Conclusion
There is no difference in 6-s tapping, Chase 15-s test or limb asymmetry amongst UAE and non-UAE footballers. However, the non-UAE footballers showed a significantly better performance in Countermovement Jump Test. The data provide baseline values for forthcoming sports medicine research, which can be taken into account when creating injury prevention or return-to-sport protocols, particularly with regard to changes in direction parameters and countermovement jumps.
Abbreviations
COD, change-of-direction; CMJ, Countermovement jump; UAE, United Arab Emirates; ACL, Anterior Cruciate Ligament.
Disclosure
The authors report no conflict of interest in this work.
References
1. Krutsch W, Zeman F, Zellner J, Pfeifer C, Nerlich M, Angele P. Increase in ACL and PCL injuries after implementation of a new professional football league. Knee Surg Sports Traumatol Arthrosc. 2016;24(7):2271–2279. doi:10.1007/s00167-014-3357-y
2. Alentorn-Geli E, Myer GD, Silvers HJ, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanism of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc. 2009;17(7):705–729. doi:10.1007/s00167-009-0813-1
3. Xie D, Urabe Y, Ochiai J, Kobayashi E, Maeda N. Sidestep cutting maneuvers in female basketball players: stop phase poses greater risk for anterior cruciate ligament injury. The Knee. 2013;20(2):85–89. doi:10.1016/j.knee.2012.07.003
4. Teichmann J, Suwarganda EK, Lendewig C, et al. Unexpected-disturbance program for rehabilitation of high-performance athletes. J Sport Rehabil. 2016;25(2):126–132. doi:10.1123/jsr.2014-0280
5. Bartels T, Proeger S, Brehme K, et al. The SpeedCourt system in rehabilitation after reconstruction surgery of the anterior cruciate ligament (ACL). Arch Orthop Trauma Surg. 2016;136(7):957–966. doi:10.1007/s00402-016-2462-4
6. Düking P, Born DP, Sperlich B. The SpeedCourt: reliability, usefulness, and validity of a new method to determine change-of-direction speed. Int J Sports Physiol Perform. 2016;11(1):130–134. PMID: 26061971. doi:10.1123/ijspp.2015-0174
7. Gokeler A, Welling W, Benjaminse A, Lemmink K, Seil R, Zaffagnini S. A critical analysis of limb symmetry indices of hop tests in athletes after anterior cruciate ligament reconstruction: a case control study. Orthop Traumatol Surg Res. 2017;103(6):947–951. PMID: 28428033. doi:10.1016/j.otsr.2017.02.015
8. Claudino JG, Cronin J, Mezêncio B, et al. The countermovement jump to monitor neuromuscular status: a meta-analysis. Sci. Med. Sport. 2017;20(4):397–402. doi:10.1016/j.jsams.2016.08.011
9. Small K, McNaughton L, Greig M, Lovell R. Effect of timing of eccentric hamstring strengthening exercises during soccer training: implications for muscle fatigability. J Strength Cond Res. 2009;23(4):1077–1083. doi:10.1519/JSC.0b013e318194df5c
10. Jiménez-Reyes P, Pareja-Blanco F, Cuadrado-Peñafiel V, Ortega-Becerra M, Párraga J, González-Badillo JJ. Jump height loss as an indicator of fatigue during sprint training. J Sports Sci. 2019;37(9):1029–1037. doi:10.1080/02640414.2018.1539445
11. Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804–808. doi:10.1136/bjsports-2016-096031
12. Gobbi A, Francisco R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigation. Knee Surg Sports Traumatol Arthrosc. 2006;14(10):1021–1028. doi:10.1007/s00167-006-0050-9
13. Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2005;13(5):393–397. doi:10.1007/s00167-004-0591-8
14. Lee DY, Karim SA, Chang HC. Return to sports after anterior cruciate ligament reconstruction—a review of patients with minimum 5-year follow-up. Ann Acad Med Singapore. 2008;37(4):273–278. doi:10.47102/annals-acadmedsg.V37N4p273
15. Waldén M, Hagglund M, Magnusson H, Ekstrand J. Anterior cruciate ligament injury in elite football: a prospective three-cohort study. Knee Surg Sports Traumatol Arthrosc. 2011;19(1):11–19. doi:10.1007/s00167-010-1170-9
16. O’Malley E, Richter C, King E, et al. Countermovement jump and isokinetic dynamometry as measures of rehabilitation status after anterior cruciate ligament reconstruction. J Athl Train. 2018;53(7):687–695. doi:10.4085/1062-6050-480-16
17. Taylor K, Chapman DW, Cronin J, et al. Fatigue monitoring in high performance sport: a survey of current trends. J Aus Strength Cond. 2012;20:12–23.
18. Smith DJ. A framework for understanding the training process leading to elite performance. Sports Med. 2003;33(15):1103–1126. doi:10.2165/00007256-200333150-00003
19. Attia A, Dhahbi W, Chaouachi A, Padulo J, Wong DP, Chamari K. Measurement errors when estimating the vertical jump height with flight time using photocell devices: the example of Optojump. Biol Sport. 2017;34(1):63–70. doi:10.5114/biolsport.2017.63735
20. Dos’Santos T, Thomas C, Jones PA, Comfort P. Mechanical determinants of faster change of direction speed performance in male athletes. J Strength Cond Res. 2017;31(3):696–705. doi:10.1519/JSC.0000000000001535
21. Ghrairi M, Chomier P, Khelifa M, et al. ISOKINETIC STRENGTH AND RATIO OF PROFESSIONAL FOOTBALL PLAYERS IN UAE. Br J Sports Med. 2013;47(10):e3. doi:10.1136/bjsports-2013-092558.24
22. Collings TJ, Diamond LE, Barrett RS, et al. Strength and biomechanical risk factors for noncontact ACL injury in elite female footballers: a prospective study. Med Sci Sports Exerc. 2022;54(8):1242–1251. PMID: 35320148. doi:10.1249/MSS.0000000000002908
23. Greska EK, Cortes N, Ringleb SI, Onate JA, van Lunen BL. Biomechanical differences related to leg dominance were not found during a cutting task. Scand J Med Sci Sports. 2017;27(11):1328–1336. doi:10.1111/sms.12776
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.