")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Unveiling Patient Trust in Physicians Across China: Insights from a Nationwide Cross-Sectional Study
Authors Mi J, Du X, Aili Y, Li M, Liu Y
Received 25 December 2023
Accepted for publication 23 March 2024
Published 23 April 2024 Volume 2024:17 Pages 1039—1052
DOI https://doi.org/10.2147/RMHP.S456585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jiarun Mi, Xinyu Du, Yilixiati Aili, Mingkun Li, Yuanli Liu
School of Health Policy and Management, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China
Correspondence: Yuanli Liu, School of Health Policy and Management, Chinese Academy of Medical Sciences and Peking Union Medical College, Dongdansantiao, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-13522592907, Email [email protected]
Background: Trust is a major factor affecting patient-physician relationship and healthcare quality. However, there has been a lack of comprehensive study on the extent of and major factors affecting patient trust in healthcare providers of China, the world’s largest developing country. The objective of this study is to elucidate the current status of outpatient trust in physicians in China and its influencing factors, providing empirical evidence to enhance doctor-patient trust and improve doctor-patient relationships.
Methods: Between December 2017 and January 2018, 28,760 patients seeking care at the outpatient departments of 136 tertiary hospitals were interviewed, where they were asked to rate their trust in physicians. We applied a multilevel logistic regression model to explore the association between patients trust and characteristics of hospitals, physicians and patient characteristics. We conducted a series of sensitivity analysis to check the robustness of our findings.
Results: Among 28,760 participants included in this study, 91.54% expressed trust in their physicians, while 7.52% showed moderate trust. Only 0.94% expressly distrusted or strongly distrusted their physicians. Outpatients of hospitals with convenient payment, volunteer guidance and enough seats available in the rest and waiting area showed higher levels of trust. Physicians who had a senior title, showed patience and protection of the patient’s privacy were more likely to be trusted by their patients in the outpatient setting. Compared to their female counterparts, male outpatients showed a higher degree of trust.
Conclusion: While this study highlights an overall high level of Trust in physicians (TIP) among patients in China’s tertiary hospitals, it is found to vary with patient demographic factors as well as provider’s attributes. Hospitals with a more keen sense of protecting patients privacy and better meeting patients’ need for efficient and caring service provision process appeared to yield a higher level of trust.
Keywords: trust in physicians, national survey, outpatients
Introduction
Trust in physicians (TIP) has long been recognized as the core in patient-physician relationships and quality health care,1,2 which is generally defined as the patients’ belief that their physicians will provide medical care, suggestions and treatment in their best interest.3 TIP has been proved to be associated with better adherence to treatment,4 the decrease of patient fear and anxiety,5 less delayed care and fewer miss visits6 and better self-reported health,7 often leading to successful patient care. Due to the inequality of medical knowledge and power in patient-physician relationships,5 patients are often in a vulnerable position in healthcare services, resulting in possible preconceived mistrust in physicians. Therefore, TIP is often difficult to establish. In spite of the strong TIP shown in some early studies,1 there is growing concern that the solid trust is eroding because of the changes in health care systems.8 Compared to high-income countries, the crisis in TIP is more severe in low- and middle-income countries.9 In China, a recent report showed that the proportion of adult patients who did trust their physicians have decreased from 83.4% to 64.2% over a five year period.10
Acknowledging this trend, the literature on TIP and its determinants is expanding. This body of work suggests that the extent of TIP is related to both the supply and demand sides’ characteristics of healthcare. In terms of intrinsic patients characteristics, their age, mental health, sex, race and education and income levels all affect TIP.11–14 Several studies also suggested that patient participation in treatment decisions is an important antecedent variable for building TIP.15,16 For physicians, the technical competence assessed by patients based on qualifications and status (eg, professor or researcher of a medical school and specialist) is of primary importance for TIP.17 Patients are also more likely to trust physicians with whom they spend longer time of consultation18 or have long continuous relationships.19 In addition, quantities of research have shown that physicians’ verbal and non-verbal communication skills such as assurance of treatment, giving more information and showing caring behaviors (eg, displaying empathy and intent listening) are beneficial in establishing TIP.12,20,21 However, studies using nationally representative data about TIP in China are still lacking. Most of the previous studies in China about TIP were based on some specific provinces, cities or even hospitals and their findings were mixed.22,23 With the increasing pressure on the healthcare systems in China, characterizing TIP and its influencing factors in China is helpful to improve the physician-patient relationship and provide higher quality healthcare services. In addition, considering the nearly half of the clinical work undertaken by tertiary hospitals in China,24 how to improve TIP in them should be given more attention by researchers.
Recognizing this, in this study, we used a nationally representative survey data, aiming to investigate the outpatients’ trust in physicians and its influencing factors in tertiary hospitals in China.
Materials and Methods
Study Design
Our study employed a national cross-sectional patient survey design aiming to assess the level of trust in physicians among outpatient patients in China and its influencing factors. The survey was conducted from December 2017 to January 2018 across 136 tertiary hospitals in all 31 provinces of mainland China by the Peking Union Medical College (PUMC) School of Public Health. Briefly, this survey applied a two-stage sampling design to select participants. In the first stage of sampling (hospital level), we selected one general hospital, one traditional Chinese medicine hospital (TCM hospital) and one maternal and child hospital (MC hospital) based on convenience. And we also included 43 National Health and Family Planning Commission (NHFPC)-affiliated hospitals (including 28 general hospitals and 15 specialist hospitals). The second stage of sampling targeted outpatients were conducted in the pharmacy area of each hospital, where they usually complete the process of outpatient consultation and payment and await receiving their drugs. Each participant’s information was collected face-to-face by a well-trained medical student via mobile devices. The validity and reliability of the questionnaire utilized in our study have been previously verified.25 Firstly, all items in the questionnaire were subjected to expert review to ensure their content validity. The construct validity of the questionnaire was assessed using Exploratory Factor Analysis, with all item factor loadings exceeding 0.50, indicating that the construct validity is acceptable. Furthermore, the Cronbach’s alpha coefficients for each dimension exceeded 0.75, demonstrating that our questionnaire possesses good reliability.
Sample Size and Population
In the design of our study, we assumed an 85% satisfaction rate among outpatient services and set the significance level at 0.05. To ensure statistical significance and adequate precision of our results, we employed the following formula to calculate the minimum required sample size for each hospital:

Here, Zα/2 represents the critical value from the normal distribution for α=0.05, equating to 1.96. p is the anticipated proportion of satisfaction, set at 0.85, and E is the permissible error margin we established, at 0.05. Applying this formula, we calculated a minimum sample size of 196 for each hospital. To account for potential non-response and the necessity of data cleansing, we rounded up the sample size to at least 200 per hospital. This sample size ensures that our findings are statistically significant and meaningful. We initially approached a total of 39,379 outpatients and successfully collected 28,822 completed questionnaires, culminating in a response rate of 73%. Before the statistical analyses, we performed data cleaning and removed questionnaires with variable outliers. Finally, we obtained a sample of 28,760 effective questionnaires and the effective rate was 99.78%.
Outcome
The outcome of this study was the extent of TIP, which was measured by a 5-point entry in the questionnaire. Each participant was invited to consider the following statement – “I have full trust in physicians who received me for patient this time” and choose their answer from “strongly disagree”, “disagree”, “moderate”, “agree” and “strongly agree”.
Covariates
The covariates were selected from hospital level, physician level and patient level. The covariates of hospital level included the hospital type (ie, general hospital, traditional Chinese medicine hospital, maternal and child hospital and other specialty hospital), the hospital region (ie, eastern, central and western), the payment convenience, the volunteer guidance and the enough seat availability in the rest and waiting area. The covariates of physician level included the physician’s title, the patience of physicians during consultations and the protection of patient privacy. The covariates of patient level included the patient’s age, sex, education level, occupation, the total cost of this outpatient visit, the patient’s annual household income, household registration and medical insurance. Among them, participants with a senior high school diploma or higher were defined as better educated.
Statistical Analysis
In the descriptive analysis, we calculated the distribution of TIP over each covariate and used chi-square test to compare the differences in the distribution. Covariates with p-values of < 0.1 were considered statistically significant and were included in the further analysis.
Since the participants were nested in 136 hospitals, we then applied the multilevel logistic regression model to explore the association between TIP and the covariates, which allows for the association across participants within hospitals.26 We also calculated the intraclass correlation coefficient (ICC) in our data, which denoted the proportion of which the total variation of TIP could be attributed to the hospital level effect.27 The ICC was 11.2% in our data, further confirming the necessity for the multilevel regression modelling. We defined “strongly disagree”, “disagree” and “moderate” as a negative answer to TIP (0=no) and defined “strongly agree” and “agree” as a positive answer to TIP (1=yes). The association between each covariate and TIP was expressed as an odds ratio (OR) and a 95% confidence interval (CI). In addition, given that the bias in the association estimating caused by defining the response “moderate” as “do not trust physicians”, we excluded these participants for sensitivity analyses. We also added results from the ordinary logistic regression that do not account for multiple levels to test the robustness of our findings. A two-tailed p value of < 0.05 was considered to indicate statistical significance. All statistical analyses were conducted using R software (version 4.2.0).
Results
Descriptive Analysis
The results of the descriptive analysis were shown in Table 1. Of the 28,760 outpatients sampled in 36 tertiary public hospitals, 12,197 (42.4%) were from general hospitals, 6516 (22.7%) were from TCM hospitals, 6254 (21.7%) were from MC hospitals and 3793 (13.2%) were from other specialty hospitals. 12,235 (42.5%) participants were from eastern China, 7258 (25.2%) were from central China and 9267 (32.2%) were from western China. Female participants accounted for 64.6% and 84.6% participants had at least a high school education. As is shown in Table 2, among all participants, 54.24% answered with “strongly agree” to the TIP entry, 37.30% answered with “agree”, 7.52% answered with “moderate” and only 0.94% answered with “disagree” or “strongly disagree”. In Table 3, since the results of chi-square test suggested that the differences in the distributions of all covariates were statistically significant, they were all included in the multilevel regression analysis.
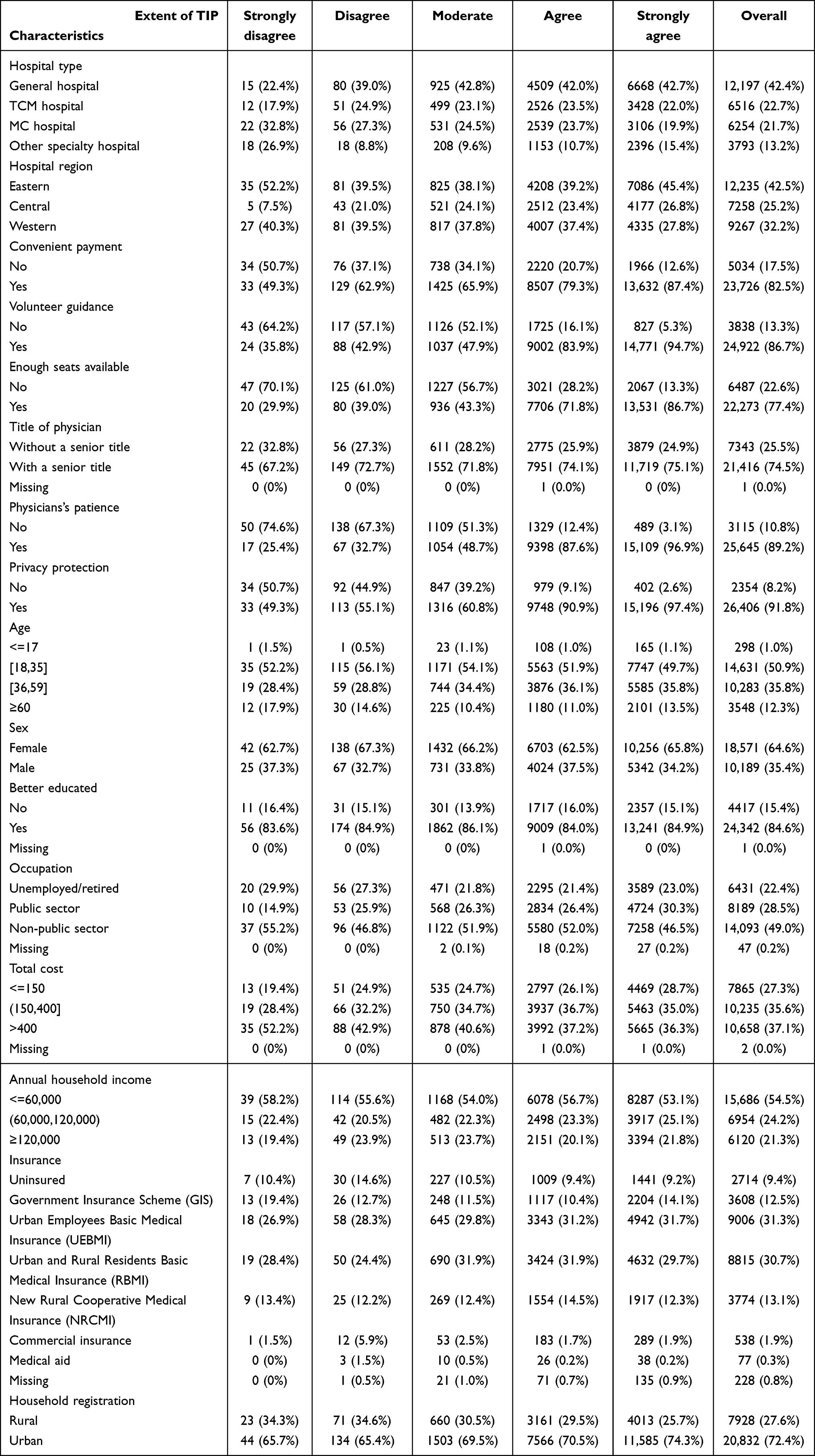 |
Table 1 Sample Characteristics of 28,760 Participants Included in Our Study |
 |
Table 2 Distribution of Responses and Percentages for TIP Outcome |
 |
Table 3 The Results of the Univariate Analysis |
Multilevel Regression Analysis
The results of the multilevel regression analysis were shown in Table 4. In the hospital level, compared to general hospitals, outpatients of other specialty hospitals were more likely to trust their physicians (OR: 1.37, 95% CI: 1.08, 1.73). The effect of hospital regions on TIP was not statistically significant. Outpatients of hospitals with convenient payment (OR: 1.40, 95% CI: 1.25, 1.58), volunteer guidance (OR: 3.2, 95% CI: 2.86, 3.59) and enough seats available in the rest and waiting area (OR: 2.83, 95% CI: 2.55, 3.15) showed higher TIP. In the physician level, physicians who had a senior title (OR: 1.16, 95% CI: 1.06, 1.31), showed patience (OR: 5.71, 95% CI: 5.10, 6.38) and protection of the patient’s privacy (OR: 3.02, 95% CI: 2.67, 3.43) were more likely to be trusted by their outpatients. In the patient level, male outpatients showed higher TIP (OR: 1.16, 95% CI: 1.03, 1.29) compared to female outpatients. Patients with annual household incomes over 120,000¥ (OR: 0.86, 95% CI: 0.75, 0.98) were more likely to distrust their physicians. Compared to uninsured outpatients, patients with New Rural Cooperative Medical Insurance (OR: 1.25, 95% CI: 1.00, 1.55) tend to have greater trust in their physicians. Patients with urban household registration (OR: 1.16, 95% CI: 1.01, 1.33) demonstrate a higher tendency to trust their physicians.
 |
Table 4 Multilevel Regression Analysis About the Association Between TIP and Different Covariates |
Sensitive Analysis
The results of the sensitive analysis were shown in Figures 1 and 2. Although there were some differences ORs compared to the results of the main analysis, the direction of the associations remain unchanged. For instance, as is shown in Figure 1, when removing participants answering with “moderate” to TIP, the OR of the sensitive analysis was larger in participants who experienced the convenient payment (OR: 1.54, 95% CI: 1.16, 2.05) compared to the main analysis (OR: 1.40, 95% CI: 1.25, 1.58), but the direction of the ORs were identical. Similarly, as is shown in Figure 2, even if multiple levels are not considered, the direction of the association based on the ordinary logistic regression is the same as the main result. Therefore, the robustness of our results was confirmed.
 |
Figure 1 Sensitive analysis using multilevel regression model by removing participants answering with “moderate”. |
 |
Figure 2 The results of the association between TIP and covariates based on ordinary logistic regression model without including multiple levels. |
Discussion
In this extensive nationwide cross-sectional study, we meticulously investigated the status and determinants of TIP within tertiary public hospitals in China, focusing on variables at the hospital, physician, and patient levels. Our findings revealed that a notable 91.54% of the respondents exhibited a positive trust in physicians, highlighting a generally favorable TIP status in these healthcare settings. At the hospital level, factors such as payment convenience, the presence of volunteer guidance, and the availability of adequate seating in rest and waiting areas proved pivotal in shaping this trust. The demeanor and professional conduct of physicians were also found to be critical elements. Additionally, patient-level backgrounds, encompassing their sex, medical insurance condition and household registration, also significantly contribute to the formation of trust in their physicians. Despite the straightforward nature of our methodological approach, these findings provide profound insights into the specific dynamics of TIP within China’s tertiary public hospitals, offering crucial guidance for future improvements in medical services and policy formulation.
In an international comparison, our study found that patients’ trust in doctors in tertiary public hospitals in China was 91.54%, a percentage that stands out globally. Compared with related studies in other countries, this percentage is higher in China. For instance, research in Croatia showed a trust level of only 78.3%,28 while another study in Saudi Arabia reported a trust level of 90.4%.29 This discrepancy may stem from differences in the structure of the healthcare system, cultural background, doctor-patient communication styles, and healthcare policies in different countries. The higher level of trust among Chinese patients may reflect the interaction patterns and social trust mechanisms specific to the domestic healthcare system. However, it also raises an important question: does high trust always represent quality healthcare services and patient satisfaction? This finding prompts future research to further explore the complex relationship between trust and healthcare service quality.
At the hospital level, our findings reveal that several key factors, such as ease of payment, the presence of volunteer guides, and the availability of adequate seating in resting and waiting areas, have a significant impact on patient trust in physicians. The importance of these factors has also been demonstrated in previous studies, some of which have shown that the quality of the hospital’s physical environment and services has a significant impact on patient trust.30,31 For example, a semi-structured telephone interview indicated that a welcoming physical environment was associated with higher TIP.31 At the physician level, our data show that a physician’s title level, demonstrated patience, and protection of patient privacy are key factors in gaining patient trust. Consistent with the results of other studies that have found that physicians’ professional skills and interpersonal communication skills are critical to building and maintaining patient trust.32,33 In particular, physicians’ respect for patient privacy have been shown to be key factors influencing patient trust.34 These findings emphasize the dual role of the hospital environment and the individual physician’s skills in improving the quality of healthcare delivery and patient satisfaction. Future research and healthcare policy development needs to focus more on how to enhance patient trust by improving the hospital environment and enhancing physicians’ professional skills, thereby improving the overall quality and effectiveness of healthcare services.
At the patient level, our study reveals the significant role of gender in shaping TIP. Specifically, we found that female patients generally had lower TIP than male patients, which was similar to several studies.35,36 This may be due to the fact that women may face more communication barriers and perceived unequal treatment in healthcare settings, which may lead to lower trust in their healthcare providers. In addition, female patients may have higher concerns about the quality and safety of healthcare services, which may also affect their trust.
Similar to several previous studies,34,37 our study also showed that economic status had a significant impact on patients’ TIP. Specifically, patients with higher annual incomes tended to hold lower levels of trust in their physicians. This may reflect the different expectations of patients from different economic backgrounds regarding the quality and accessibility of healthcare services. Insurance status is also a key factor; for example, patients with the new rural cooperative health insurance showed higher levels of trust compared to uninsured patients, highlighting the importance of health insurance in enhancing patients’ trust in the healthcare system. Taken together, our findings emphasize the need to consider factors such as a patient’s gender, economic status, and insurance coverage when enhancing doctor-patient trust. Understanding and addressing these influencing factors will help improve the quality of healthcare services, promote patient satisfaction, and improve the doctor-patient relationship.
This study has the following limitations. First, given that the research was conducted exclusively in tertiary hospitals in China, the high patient trust level observed might not accurately reflect the broader Chinese healthcare landscape, as these institutions represent the pinnacle of available resources and services. Second, the cross-sectional design of our study limits the ability to trace the evolution of patient trust over time or to establish causal relationships. Third, the study potentially underrepresents the influence of cultural and social factors that are pivotal in shaping patient trust, particularly in a diverse and complex society like China. These limitations suggest caution in generalizing the findings across different healthcare settings within the country.
Conclusions
This study highlights that TIP is generally high among patients in China’s tertiary public hospitals, yet it fluctuates significantly due to patient demographic characteristics and the attributes of healthcare providers. We discovered that TIP is influenced by a multitude of factors across different dimensions—patients, physicians, and medical institutions—reflecting the complex, multifactorial process of trust formation. This understanding underscores the necessity of considering the behavior of healthcare providers, the background characteristics of patients, and the policies and service environment of medical institutions to improve patient trust. Our research provides empirical insights into the elements constituting patient trust within the current Chinese healthcare system and emphasizes the potential of enhancing this trust through specific hospital management and policy adjustments in the context of medical reform. Notably, hospitals that meet patients’ demands for high-quality medical services and offer better patient healthcare experiences appear to achieve higher TIP. Thus, by standardizing diagnostic and treatment processes to protect patient privacy, providing patient-centered medical care, and maintaining open communication channels to improve the patient healthcare experience, medical institutions can effectively enhance trust. Considering the current focus of China’s medical reform on prioritizing patient-centered improvements in the quality and accessibility of healthcare services, our study’s recommendations for concrete measures to elevate patient trust align with the reform’s core objectives.
Ethics Approval and Informed Consent
The study protocol was approved by the Ethics Committee of Peking Union Medical College (SPH201712CHII206). This study was conducted in accordance with the principles of the Declaration of Helsinki, and all participants have signed informed consent forms.
Consent for Publication
Informed consent for publication was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Health and Family Planning Commission, P.R. China. The project was also funded by the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences—A Strategic Study on Healthy China Development and Health System Reform (2021-I2M-1-046).
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Hall MA, Dugan E, Zheng BY, Mishra AK. Trust in physicians and medical institutions: what is it, can it be measured, and does it matter? Milbank Q. 2001;79(4):613. doi:10.1111/1468-0009.00223
2. Lynch TJ, Wolfson DB, Baron RJ. A trust initiative in health care: why and why now? Acad Med. 2019;94(4):463–465. doi:10.1097/ACM.0000000000002599
3. Anderson LA, Dedrick RF. Development of the Trust in Physician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol Rep. 1990;67(3):1091–1100. doi:10.2466/pr0.1990.67.3f.1091
4. Lee YY, Lin JL. The effects of trust in physician on self-efficacy, adherence and diabetes outcomes. Soc Sci Med. 2009;68(6):1060–1068. doi:10.1016/j.socscimed.2008.12.033
5. Hillen MA, de Haes HCJM, Smets EMA. Cancer patients’ trust in their physician-A review. Psycho-Oncol. 2011;20(3):227–241. doi:10.1002/pon.1745
6. Mollborn S, Stepanikova I, Cook KS. Delayed care and unmet needs among health care system users: when does fiduciary trust in a physician matter? Health Serv Res. 2005;40(6):1898–1917. doi:10.1111/j.1475-6773.2005.00457.x
7. Birkhauer J, Gaab J, Kossowsky J, et al. Trust in the health care professional and health outcome: a meta-analysis. PLoS One. 2017;12(2):e0170988. doi:10.1371/journal.pone.0170988
8. Rolfe A, Cash-Gibson L, Car J, Sheikh A, McKinstry B. Interventions for improving patients’ trust in doctors and groups of doctors. Cochrane Database Syst Rev. 2014;3:CD004134. doi:10.1002/14651858.CD004134.pub3
9. Blendon RJ, Benson JM, Hero JO. Public Trust in Physicians — u.S. medicine in international perspective. N Engl J Med. 2014;371(17):1570–1572. doi:10.1056/NEJMp1407373
10. Zhao D, Zhang Z. Changes in public trust in physicians: empirical evidence from China. Front Med. 2019;13(4):504–510. doi:10.1007/s11684-018-0666-4
11. Tanco K, Rhondali W, Park M, Liu D, Bruera E. Predictors of trust in the medical profession among cancer patients receiving palliative care: a preliminary study. J Palliat Med. 2016;19(9):991–994. doi:10.1089/jpm.2016.0089
12. Gopichandran V, Chetlapalli SK. Trust in the physician-patient relationship in developing healthcare settings: a quantitative exploration. Indian J Med Ethics. 2015;12(3):141–148. doi:10.20529/IJME.2015.043
13. Boulware LE, Cooper LA, Ratner LE, LaVeist TA, Powe NR. Race and trust in the health care system. Public Health Rep. 2003;118(4):358–365. doi:10.1016/S0033-3549(04)50262-5
14. Zhao DH, Rao KQ, Zhang ZR. Patient trust in physicians: empirical evidence from Shanghai, China. Chin Med J (Engl). 2016;129(7):814–818. doi:10.4103/0366-6999.178971
15. Yang T, Wu Y. A study on the influence of patient participation on patient trust-based on sample survey in China. Front Psychol. 2018;9:2189. doi:10.3389/fpsyg.2018.02189
16. Tanaka H, Shimaoka M. Trust in physicians and definitive diagnosis time among Japanese patients with specific intractable diseases: a cross-sectional study. INTRACTABLE RARE DIS RES. 2023;12(2):97–103. doi:10.5582/irdr.2023.01017
17. Mechanic D, Meyer S. Concepts of trust among patients with serious illness. Soc Sci Med. 2000;51(5):657–668. doi:10.1016/S0277-9536(00)00014-9
18. Fiscella K, Meldrum S, Franks P, et al. Patient trust: is it related to patient-centered behavior of primary care physicians? Med Care. 2004;42(11):1049–1055. doi:10.1097/00005650-200411000-00003
19. Kao AC, Green DC, Davis NA, Koplan JP, Cleary PD. Patients’ trust in their physicians - Effects of choice, continuity, and payment method. J Gen Intern Med. 1998;13(10):681–686. doi:10.1046/j.1525-1497.1998.00204.x
20. Keating NL, Gandhi TK, Orav EJ, Bates DW, Ayanian JZ. Patient characteristics and experiences associated with trust in specialist physicians. Arch Intern Med. 2004;164(9):1015–1020. doi:10.1001/archinte.164.9.1015
21. Chandra S, Ward P, Mohammadnezhad M. Investigating patient trust in doctors: a cross-sectional survey of out-patient departments in Fiji. Int Q Community Health Educ. 2021;41(4):369–377. doi:10.1177/0272684X20967602
22. Han Y, Lie RK, Li Z, Guo R. Trust in the doctor-patient relationship in Chinese public hospitals: evidence for hope. Patient Prefer Adherence. 2022;16:647–657. doi:10.2147/PPA.S352636
23. Liu PL, Jiang S. Patient-centered communication mediates the relationship between health information acquisition and patient trust in physicians: a five-year comparison in China. Health Commun. 2021;36(2):207–216. doi:10.1080/10410236.2019.1673948
24. Zhang C, Hu L, Ma J, Wu S, Guo J, Liu Y. Factors determining intention to leave among physicians in tertiary hospitals in China: a national cross-sectional study. BMJ Open. 2019;9(3):e023756. doi:10.1136/bmjopen-2018-023756
25. Hu L, Zhou BP, Liu S, Wang Z, Liu Y. Outpatient satisfaction with tertiary hospitals in china: the role of sociodemographic characteristics. Int J Environ Res Public Health. 2019;16(19):3518. doi:10.3390/ijerph16193518
26. Zhou H, Han X, Zhang J, et al. Job satisfaction and associated factors among medical staff in tertiary public hospitals: results from a national cross-sectional survey in China. Int J Environ Res Public Health. 2018;15(7):1528. doi:10.3390/ijerph15071528
27. Bottle A, Faitna P, Aylin PP. Patient-level and hospital-level variation and related time trends in COVID-19 case fatality rates during the first pandemic wave in England: multilevel modelling analysis of routine data. BMJ Qual Saf. 2022;31(3):211–220. doi:10.1136/bmjqs-2021-012990
28. Nikodem K, Ćurković M, Borovečki A. Trust in the healthcare system and physicians in Croatia: a survey of the general population. Int J Environ Res Public Health. 2022;19(2):993. doi:10.3390/ijerph19020993
29. Boubshait LA, AlShamlan NA, AlShammari RZ, et al. Patient trust in primary care physicians: a mixed methods study of persons with diabetes at university- based clinics in the eastern province of Saudi Arabia. Patient Prefer Adherence. 2022;16:3241–3255. doi:10.2147/PPA.S377500
30. Tang X, Lu J, Chen Z, Liu C, Jiang X, Ning M. Influencing factors of patients’ trust in nurses during the COVID-19 pandemic: a mixed-methods study. Disaster Med Public Health Prep. 2022;17:e302. doi:10.1017/dmp.2022.262
31. Greene J, Samuel-Jakubos H. Building patient trust in hospitals: a combination of hospital-related factors and health care clinician behaviors. Jt Comm J Qual Patient Saf. 2021;47(12):768–774. doi:10.1016/j.jcjq.2021.09.003
32. Su F, Wang Y, Wu Q, Wang PJ, Chang X. The influence of stereotypes on trust in doctors from patients’ perspective: the mediating role of communication. Psychol Res Behav Manag. 2022;15:3663–3671. doi:10.2147/PRBM.S389202
33. Gu L, Tian B, Xin Y, Zhang S, Li J, Sun Z. Patient perception of doctor communication skills and patient trust in rural primary health care: the mediating role of health service quality. BMC Prim Care. 2022;23(1):255. doi:10.1186/s12875-022-01826-4
34. Orrange S, Patel A, Mack WJ, Cassetta J. patient satisfaction and trust in telemedicine during the COVID-19 pandemic: retrospective observational study. JMIR Hum Factors. 2021;8(2):e28589. doi:10.2196/28589
35. Irwin K, Edwards K, Tamburello JA. Gender, trust and cooperation in environmental social dilemmas. Soc Sci Res. 2015;50:328–342. doi:10.1016/j.ssresearch.2014.09.002
36. Kim AM, Bae J, Kang S, Kim YY, Lee JS. Patient factors that affect trust in physicians: a cross-sectional study. BMC Fam Pract. 2018;19(1):187. doi:10.1186/s12875-018-0875-6
37. Hutten RJ, Weil CR, King AJ, et al. Multi-institutional analysis of cancer patient exposure, perceptions, and trust in information sources regarding complementary and alternative medicine. JCO Oncol Pract. 2023;19(11):1000–1008. doi:10.1200/OP.23.00179
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.