")
Back to Journals » Patient Preference and Adherence » Volume 18
Treatment Adherence and Related Factors Among Children with Attention-Deficit/Hyperactivity Disorder in Saudi Arabia
Authors Alsubaie MA , Alshehri ZY, Alawadh IA, Abulreesh RY , Altaweel HM, Alateeq DA
Received 27 October 2023
Accepted for publication 26 January 2024
Published 3 February 2024 Volume 2024:18 Pages 337—348
DOI https://doi.org/10.2147/PPA.S443481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Maha Ali Alsubaie,1 Zainah Yahya Alshehri,1 Ibtihaj Abdullah Alawadh,1 Razan Yasser Abulreesh,1 Hussain Mohammed Altaweel,2 Deemah Ateeq Alateeq1
1Internal Medicine Department, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, 16711 Saudi Arabia; 2Psychiatry Department, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Correspondence: Deemah Ateeq Alateeq, Internal Medicine Department, College of Medicine, Princess Nourah Bint Abdulrahman University, P.O. Box 84428, Riyadh, 16711, Saudi Arabia, Email [email protected]
Introduction: Attention-deficit/hyperactivity disorder (ADHD) is a common childhood psychiatric disorder. It frequently persists into adulthood and is a risk factor for other mental disorders and adverse outcomes, mainly if not managed optimally. This study aimed to assess ADHD treatment adherence and explore the underlying causes of non-adherence in ADHD children in Saudi Arabia.
Methods: A cross-sectional study of a convenience sample of 221 participants. The survey included demographic characteristics of the child and parents, the child’s medical history, quality of services evaluation, as well as medication adherence assessment by Medication Adherence Report Scale (MARS), the general beliefs about medicines questionnaire (General-BMQ), in addition to assessing the parents’ beliefs about ADHD and provided/recommended treatment.
Results: The sample was primarily 6 to 8-year-old children (32.81%) and males (78.52%). Most subjects were prescribed extended-release agents (45.7%), and overall, high-quality services were provided to the patients. The adherence rate of ADHD patients to their medication was 89.77%. The mother’s education correlated significantly with patient adherence (p=0.029), and the mother’s age correlated significantly with their beliefs (p=0.021), in addition to the family income (0.033). Children on Methylphenidate Immediate Release had good compliance with the medication (p=0.008). Moreover, Methylphenidate Extended Release has shown continuity results, increasing the adherence rates (p=0.035).
Conclusion: ADHD medication adherence was high and associated with older age, educational status, and type of medication used. Physicians should consider these factors to improve adherence in their patients.
Keywords: attention-deficit/hyperactivity disorder, children, parents, treatment adherence
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common childhood psychiatric disorder. It is characterized by symptoms of persistent inattention and/or impulsivity and hyperactivity, which can significantly impact functioning and behavior in children and adolescents in school and at home.1,2 ADHD frequently persists into adulthood and is a risk factor for other mental disorders and adverse outcomes, mainly if not managed optimally.3,4 The estimated overall prevalence of ADHD worldwide is 7.2%.5 In the Arab Gulf region, the total prevalence of ADHD was estimated at 5.90%.6 Specifically, in 2018, the prevalence of ADHD among primary school students in Saudi Arabia was reported to be 5%.7 Currently, the mainstay therapy of ADHD is the pharmacological options, mainly with stimulants such as amphetamines (AMPHs) and methylphenidates (MPHs).8 Many studies show that using these medications alone or combined with behavioral or cognitive intervention will improve concentration, sustained attention span, and social behavior and decrease excessive motor activity.9 Another study has shown that children with ADHD who are on psychostimulants have better executive function tasks such as working memory, spatial short-term memory, set-shifting, and planning ability.10 Positive outcomes in ADHD patients are directly correlated with treatment adherence, and medication adherence is a process of continuously taking action about the recommended treatment to reach the best quality of life goal.11,12 Despite the proven efficacy of psychostimulant therapy, medication adherence is poor.12
Awareness of the beliefs and factors regarding ADHD medication is essential, as parents of children with ADHD have different beliefs about ADHD that may affect the continuity of their treatment.11,13 There are common factors such as culture and body mass index, age, and gender that have been found to affect adherence to pharmacological treatment.11 Patient characteristics, the duration of medication, symptom improvement, parent beliefs, patients’ type of ADHD, healthcare system, and socioeconomic condition are considered as additional related factors.11,14,15 Parents often express concerns regarding ADHD, such as the belief that their child is too young to receive psychotropic medication and worries about potential misdiagnosis of ADHD; however, the primary factor contributing to ADHD treatment non-adherence is cultural stigma. Parents face societal pressure to conform to perceived norms and expectations, which can result in denial about the legitimacy of ADHD as a medical condition.16 In addition to cultural stigma, controversy and media portrayals are other significant barriers that may prevent individuals with ADHD from receiving an appropriate diagnosis, treatment, and support services, which further contribute to the challenges faced by parents and individuals with ADHD. To address these barriers, parents must have access to reliable information that allows them to make informed decisions and address concerns about medication use for ADHD.17
According to the discontinuity of medication, the prevalence stated by a study depends on a pharmacy database, which is between 13.2% and 64%.12 ADHD medication side effects and medical events should be considered, as one study mentioned 67% less adherence to immediate-release stimulant medications than non-stimulant medicines.11 A study review showed that non-adherence toward ADHD medication is commonly seen in children and adolescents age groups.12 A similar result in research done in the UK documented that 50% of children and adolescents failed treatment adherence.18 Regarding the duration, researchers noted that discontinuation behaviors were primarily associated with children and adolescents with long medication periods.19,20 Another study conducted in Saudi Arabia demonstrated that 36% of participating parents discontinued their child treatment on their own or against the healthcare practitioner’s advice.16
Overall, the non-adherence to medication behavior in ADHD treatment is associated with various factors that are still considered a knowledge gap. This study aims to contribute to the existing literature by assessing treatment adherence levels and exploring the underlying causes of medication non-adherence in children with ADHD, specifically in Saudi Arabia. To the best of our knowledge, this study is one of the first conducted in Saudi Arabia, providing valuable insights into the challenges and factors influencing medication adherence in this population and addressing the quality of services offered to the patients. By filling this research gap, our study will enhance the understanding of treatment adherence in ADHD children in Saudi Arabia and potentially inform the development of targeted interventions and support strategies to improve medication adherence and overall treatment outcomes.
Methods
Study Design and Population
This is a cross-sectional study. The survey was distributed to participants affiliated with Ishraq Association, a non-profit organization in Saudi Arabia that provides comprehensive specialized services for individuals affected by ADHD and works to ensure their rights. The survey was conducted from October 2020 to April 2022. The survey was also distributed to psychiatry clinics and through various social media platforms at different time points within the same timeframe. Data were collected using an anonymous online self-completed questionnaire in Arabic using a convenient non-probability sampling technique.
Primary inclusion criteria for the participants were parents of children and adolescents with confirmed ADHD diagnosis, Arabic speakers, and residents of Saudi Arabia. Exclusion criteria: autism spectrum disorder and intellectual disability patients and those who did not complete all survey sections. The recommended minimum sample size is 235. It was estimated by Raosoft software (Seattle, WA, USA) to be at the 95% confidence level (CI) with a 50% response distribution and margin of error of ±5%. Before commencing the study, ethical clearance was obtained from the Institutional Review Board of Princess Nourah bint Abdulrahman University (PNU), IRB Log number 20–0284. Informed consent was obtained from the parent or legal guardian of the patient. Data were collected and stored anonymously through the Research Electronic Data Capture (ReDCap®) 7.3.6 software hosted by PNU. The study was performed by the ethical principles stated in the Declaration of Helsinki.
Data Collection
Initially, we piloted the survey with 10 participants. However, data from the pilot were excluded from the study analysis. The questionnaire was developed in English and then translated into Arabic. The questionnaire has been reviewed by two experts in general psychiatry and child and adolescent psychiatry. The questionnaire included four main sections. The first part elicited information on demographic children’s characteristics: age, gender, level at school, and the type of school. Demographic parents’ characteristics: age, level of education, marital status, and economic status. The second section comprised medical history: age at diagnosis, who prescribed the medication, the type of medication, and if the patient has another learning disorder. The answers to the second section were all multiple-choice.
The second section was designed to evaluate the quality of services offered to the patients; it contains eleven items. The answer choices are “yes”, “no”, and “I don’t know”. The third section assesses adherence with one of the most well-known, validated, and reliable assessment tools, the Medication Adherence Report Scale (MARS), with Likert-scale answers.21,22 MARS includes ten items with 1 point for the correct answer and zero for the false one. The total score for MARS was 10, with high scores indicating a high level of adherence and low scores indicating a low level of adherence.23,24 The fourth section assessed the parents’ beliefs toward ADHD provided/recommended treatment and medication using 12 general statements considering the parents’ beliefs about ADHD and provided/recommended treatment and the general beliefs about medicines questionnaire (General-BMQ).25 The General-BMQ is a widely recognized instrument used in research to evaluate individuals’ beliefs about medication, and it has been validated and has demonstrated good reliability.24 The 5-point Likert scale was used for the responses to the 12 general statements, which ranged from “strongly disagree =5” to “strongly agree =1”, with a total score of 60. The 5-point Likert scale was also used for the eight items of General-BMQ, which ranged from “strongly disagree =1” to “strongly agree =5” with a total score of 40. High scores indicate a high level of beliefs affecting patient adherence, and low scores indicate low levels of beliefs affecting patient adherence.
Statistical Analysis
Data were analyzed using Statistical Package for Social Studies (SPSS 22; IBM Corp., New York, NY, USA). Continuous variables were expressed as mean ± standard deviation, and categorical variables as percentages. T–tests and one-way ANOVA were used for continuous variables. The Cronbach’s alpha was used to assess the reliability of the questionnaire. A p-value <0.05 was considered statistically significant.
Results
Eight hundred fifty-five participants were enrolled in the study; however, only 221 met the inclusion criteria and completed the survey. Table 1 shows the sociodemographic characteristics of children with ADHD and their parents. Most of the children in this study were 6 to 8 years old (32.81%), and 78.52% were boys. Regarding education, 36.72% of the children were in primary school grades 1–3, and two-thirds were enrolled in regular classes, while a minimum number of the sample were not enrolled in any school (7.81%). Furthermore, more than half of the mothers (55.08%) and most fathers (43.75%) were aged 31 to 40. Additionally, more than half of the mothers (58.98%), as well as half of the fathers (50%), had a college degree, and the majority of the parents live together (85.16%).
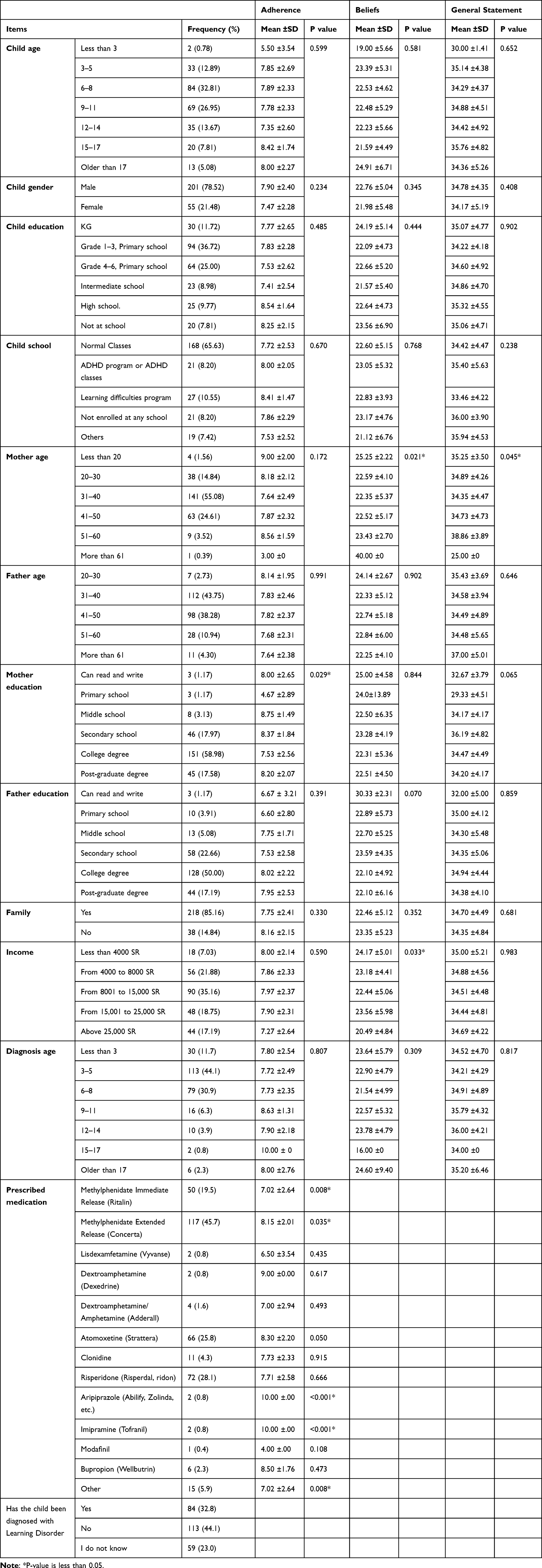 |
Table 1 Socio-Demographic Characteristics, Medical History, Adherence, and Beliefs Toward ADHD Treatment for Children and Their Parents |
A significant percentage of the children were diagnosed between ages 3 and 4 (44.1%), while 30.9% were diagnosed between ages 6 and 8. Regarding the prescribed medication, 45.7% of the children take Methylphenidate Extended-Release (Concerta). Moreover, one-third of the children have been prescribed Risperidone (Risperdal, Ridon), and about half of the children have not been diagnosed with a learning disorder. In contrast, one-third of them were diagnosed with a learning disorder.
Quality of Services Offered to the Patients
Table 2 displays the quality of services offered to the patients. Almost half of the parents reported applying scales to assist the diagnosis filled by them and their teachers (49.2%), while 30.5% have not. And 55.7% of the respondents were educated about the disorder, its prognosis, and the possible comorbidities. Furthermore, most parents were informed about the side effects of the medication (78.0%) and the importance of adhering to a treatment plan (71.8%). Additionally, 58.6% of the respondents learned about the risk of not treating ADHD.
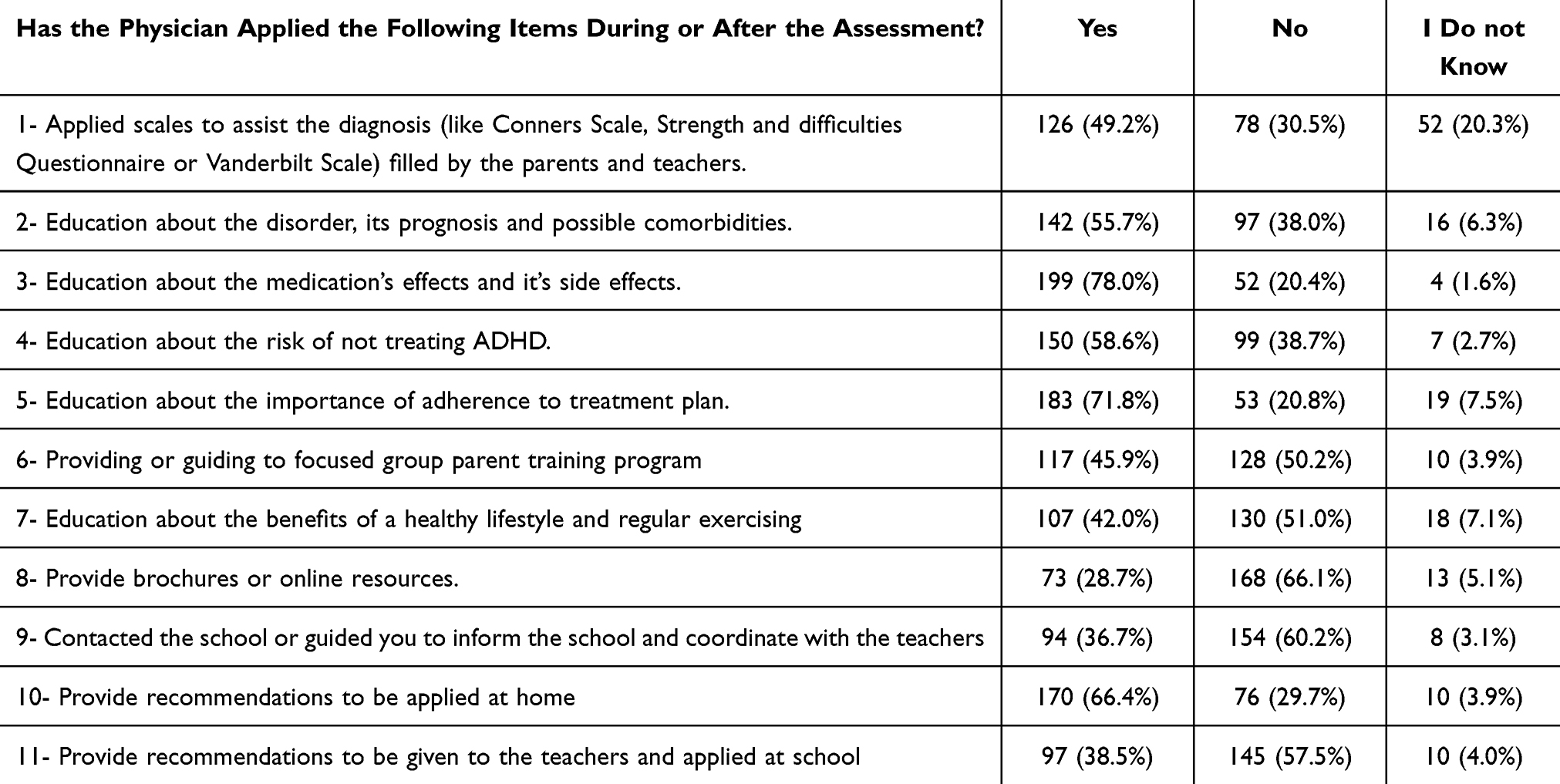 |
Table 2 Quality of Services Offered to the Patients |
On the other hand, it was found that 50.2% of the parents did not receive or were not guided to focused group parent training programs. Additionally, more than half of the parents (51.0%) were not educated about the benefits of a healthy lifestyle and regular exercise, and a significant majority (66.1%) still needed to receive brochures or access to online resources.
About two-thirds of parents should have contacted or guided them to inform the school and coordinate with the teachers (60.2%). Furthermore, this table shows that most parents were given recommendations to be applied at home (66.4%). In comparison, most were not provided recommendations to be given to the teachers and used at school (57.5%).
Adherence
The overall adherence rate of ADHD patients to their medication, as reported by parents using the MARS, was 89.77%, which is high according to a definition from previous research (92–100% of maximal MARS scores).11 The total mean of MARS was 7.81± 2.38 out of 10.
There were no statistically significant differences in socio-demographic characteristics except for the mother’s education level (p=0.029), in which mothers with primary school degrees showed lower adherence than the higher-educated mothers. Moreover, adherence toward ADHD treatment in terms of age and diagnosis was higher among the 15–17 age group (M±SD: 8.42±1.74 and 10, respectively). Elderly mothers aged 61 reported the lowest adherence rates (M: 3). Children with separated parents showed more adherence toward treatment (M±SD: 8.16±2.15).
Furthermore, Table 1 describes the relation between the adherence scores and the type of medication; it shows multiple significant results. Only two patients were using Aripiprazole and Imipramine, and they had the highest adherence rates toward the treatment (p=<0.001). In addition, children on Methylphenidate Immediate Release complied well with the medication (p=0.008). Patients prescribed Methylphenidate Extended Release have shown continuity results, increasing the adherence rates (p=0.035). Moreover, patients on Atomoxetine showed a good adherence value (P=0.050).
Parents’ Beliefs About Provided Treatment and Medications for ADHD
Table 3 displays the parents’ beliefs toward providing treatment to ADHD patients. The total mean score of General-BMQ was 34.65 ± 4.54 out of 60. More than half of the parents (52%) disagreed that their children are young for psychotropic medications, while 21.77% of parents agreed. Along with the benefits of drugs, overcoming the risks is believed by 61.78% of parents. The relationship with the prescribing doctor influences treatment adherence, and it was acknowledged by 79.55% of the parents. Most parents, 89.33%, believed understanding the doctor’s instructions would affect the treatment continuity. More than half of parents agreed that people’s opinions regarding the medication jeopardize their child’s compliance with treatment (54.67%). However, only 13.34% of parents agreed that compliance with medication only because of pressure from other people. The predominance of parents decided that the center’s availability in the region would influence re-prescribing and follow-up appointments (89.34%). Medication side effects are upsetting to 60.26% of the parents.
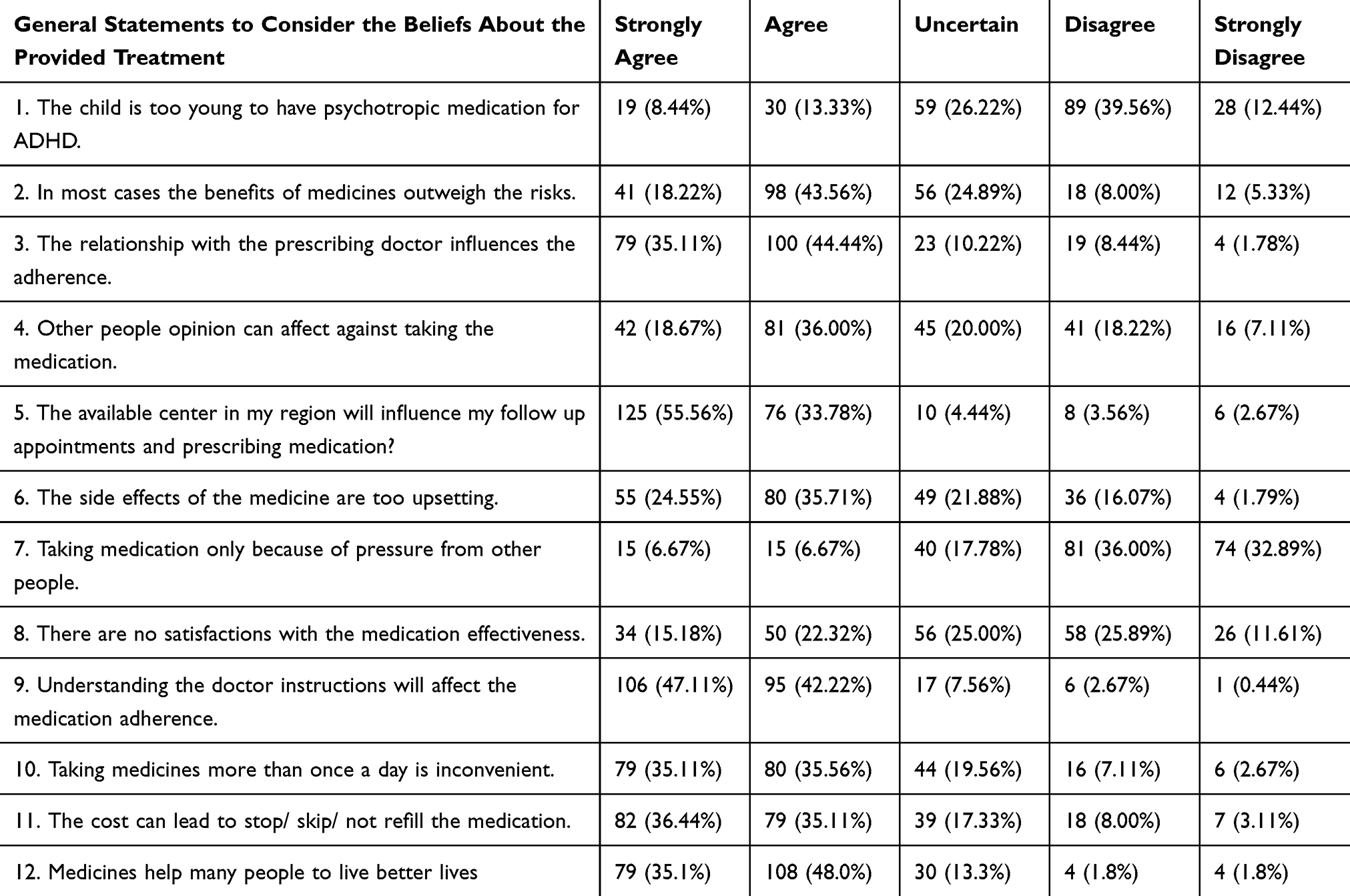 |
Table 3 Parents’ Beliefs About Provided Treatment for ADHD Patients |
Moreover, parents’ satisfaction with the medication’s effectiveness was around 37.5%. Taking medication multiple times daily is inconvenient for 70.67% of the parents. Lastly, the financial cost of medication decreases medication adherence, which was agreed upon by 71.55% of the parents.
Mother age manifested a significant result (p=0.045) towered the general statement of the beliefs about the provided treatment with the highest mean score in the age group 51–60 years (M±SD: 38.86±3.89).
Beliefs about medication, was measured by the General BMQ. Higher scores indicate negative beliefs regarding ADHD treatment. The total mean score of General-BMQ was 22.60 ± 5.13 out of 40. Parents endorse beliefs about ADHD medication based on several statements; more than half of the sample do not agree that their doctors use too many medications (51.1%). However, approximately two-thirds (62.5%) believe doctors trust medicines too much. Additionally, more than half of the participants agreed that doctors would prescribe fewer medicines if they had more time with patients (54.2%). Many indicated that they believe that natural remedies are safer than medicines (24.1%), most medicines are addictive (20%), poisons (10.2%), and do more harm than good (11.2%).
Mother’s age showed significant results in beliefs about medications (p= 0.021) and family income (p= 0.033). The top highly ranked beliefs affecting patient adherence by socio-demographic characteristics for children and their parents are more than 61 for mother age (M= 40), followed by mothers age less than 20 (M=25.25, SD=2.22), and patients older than 17 (M= 24.91, SD= 6.71). The father, education who can read and write, showed a higher mean score (M=30.33, SD= 2.31). Those with separated parents showed a higher mean score in beliefs (M= 23.35, SD= 5.23). Income is a statistically significant variable (p=0.033) that differs between lower and higher income. Lower income has the highest mean score (M= 24.17, SD= 5.01). For diagnosis, for patients older than 17, it has the highest mean score (M= 24.60, SD= 9.40).
Table 4 presents the significant correlation between adherence toward ADHD treatment and General statements of consideration of the beliefs (r = 0.271, p < 0.001). On the other hand, the General-BMQ was inversely and non-significantly related to total score Adherence with (r = −0.066, p =0.324).
 |
Table 4 Correlation Between Total Score of Adherence Toward ADHD Treatment with Total Score of Beliefs Affecting Patient Adherence and Total Score of General Statements to Consider the Beliefs |
Discussion
Nonadherence to medication behavior is associated with many different factors. With this study, we filled the knowledge gap by assessing the impact of services offered, parent beliefs, and the underlying reasons for treatment discontinuation using validated measures.
The results of the present study showed a high level of adherence (89.77%), which, in comparison to other studies, reported the highest adherence rates ranging from 21–71%.9,11,26 One possible hypothesis to interpret this finding is that the conclusions of our study showed that the quality of services provided to the patient was good.
Demographic factors are a predictor of adherence. The current study found that older age tend to have a higher adherence rate toward treatment, in contrast to a similar study that showed that adolescents were significantly less likely to adhere to treatment. This can be explained by how the responsibilities shift from the caregiver to the child.27,28
The effect of a mother’s educational status on the association between adherence to ADHD medication was found to be significant; a higher number of educated mothers play a major role in their children’s adherence to treatment. This result is similar to what was found in a study conducted in Saudi Arabia in 2002.9 This outcome is contrary to that of Parvin Safavi (Iran, 2018), who found that fathers’ education reported higher treatment adherence than mothers’.26 This result may be explained by the fact that mothers in Saudi Arabia play an essential role in their children’s adherence to medication.
The mother’s age showed significant results toward the beliefs (p= 0.021) and a significant result (p=0.045) toward the general statement of the beliefs about the provided treatment. These findings have not been found elsewhere because of the lack of association between the mother’s age and medication adherence.
Families with low income have negative beliefs towards treatment; the result here mirrors those of previous studies, which reported that those who have lower incomes are less likely to use medication consistently.29 These results reflect those of Prabhat Sitholey (2011), who found that one of the reasons for non-adherence is the high cost of medication by 40%.30
Several beliefs were found to influence medication adherence. Our study found that distance from home to hospital may affect the likelihood of obtaining medication by 54%. Sitholey (2011) makes a similar point, stating that it is a significant reason for nonadherence by 40%.30
Medication adherence in the context of ADHD treatment is a complex issue that extends beyond the involvement of parents. The opinions of others can have a significant adverse impact on the individual’s adherence to medication. Stigma emerges as a primary concern affecting medication adherence in the management of ADHD. In our study, approximately 54% of parents expressed concerns and hesitancy in continuing ADHD medication due to the influence of others’ opinions. This highlights the detrimental effect of societal attitudes and perceptions on parents’ decision-making process regarding medication adherence.
Alqahtani (2012) reported similar findings, suggesting that cultural opinions can lead parents to refuse to share their experiences about their child’s ADHD-related problems, hindering their participation in studies. This demonstrates how cultural factors can shape parents’ willingness to engage in research related to their child’s condition.16
Furthermore, Sitholey (2011) also discussed the impact of socio-cultural factors, specifically within the Indian context, on medication adherence. Family members opposing the use of medication can pose challenges to adherence behaviors.30
Most parents believe that the relationship with the prescribing doctor significantly influences adherence, with 79% acknowledging its impact. This belief aligns with another study highlighting the effect of the parent-doctor relationship on treatment adherence and continuity.14 Additionally, mental health providers play a crucial role in promoting best practices and offering psychoeducation to parents and caregivers regarding the safe use and potential side effects of psychiatric medications in children.31
The most known reason for non-compliance to ADHD medications is the side effects of medication.11 Besides that, parents believe that the impact of drugs on their children’s behaviors and attitudes has primarily contributed to increasing the adherence rate, supported by 61.78% of the participants.9
Psychopharmacological medication is the most effective way to control symptoms.32,33 Methylphenidate, amphetamine, and atomoxetine are the most commonly used medications, and psychostimulants remain a viable first-line treatment for ADHD.34
This study found that patients prescribed Methylphenidate Immediate Release had good compliance toward the treatment (p=0.008). Methylphenidate Immediate Release is commonly prescribed. However, it has a short duration of action, resulting in the need for multiple dosing during the day.35 Similar to longer-term reports with various daily doses of short-acting Methylphenidate, the use of an extended-release, once-daily preparation of MPH appears well tolerated over one year.36 In addition, children on Methylphenidate Extended Release have shown continuity results and, thus, increased adherence rates (p=0.035). It was previously found that children will likely continue to respond to Methylphenidate Extended Release.13 Over one year may require a minor dose adjustment.37 Methylphenidate has proven its effectiveness in treatment adherence.13,38 This finding is consistent with that of Efron et al (1997), which shows that Methylphenidate reduces teacher-rated ADHD symptoms.39 It has been concluded that Methylphenidate is the drug of choice.
Moreover, participants on Atomoxetine showed a good adherence value (P=0.050). Previous research has established higher stimulant adherence rates, followed by atomoxetine15 Moreover, it was the first non-stimulant FDA-approved.40
A study in Texas claimed that the highest adherence values were associated with non-stimulants and the lowest with stimulants.15 In contrast to this study, it was shown that the highest adherence values are in patient-prescribed stimulants.
Conclusion
The overall adherence rate of ADHD patients to their medication was high in this study. Significant correlations existed between older age and a high adherence rate toward treatment. In addition, mothers with a higher level of education showed a higher adherence rate. Also, Methylphenidate Immediate Release showed good compliance compared to other medications. Several beliefs were found to influence medication adherence. The physician should consider these factors to improve adherence in their patients.
Acknowledgment
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2024R218), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh A, Yeh CJ, Verma N, Das AK. Overview of attention deficit hyperactivity disorder in young children. Health Psychol Res. 2015;3(2). doi:10.4081/hpr.2015.2115
2. Mirza H, Roberts E, AL-Belushi M, et al. School dropout and associated factors among Omani children with attention-deficit hyperactivity disorder: a cross-sectional study. J Dev Behav Pediatr. 2018;39(2):109–115. doi:10.1097/DBP.0000000000000522
3. Sayal K, Prasad V, Daley D, Ford T, Coghill D. ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry. 2018;5(2):175–186. doi:10.1016/S2215-0366(17)30167-0
4. Mirza H, Al-Huseini S, Al-Jamoodi S, et al. Socio-Demographic and Clinical Profiles of Adult Attention Deficit Hyperactivity Disorder Patients in a University Hospital in Oman. Sultan Qaboos Univ Med J. 2022;22(2):206–211. doi:10.18295/squmj.5.2021.104
5. Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of Attention-Deficit/Hyperactivity Disorder: a Systematic Review and Meta-analysis. Pediatrics. 2015;135(4):e994–e1001. doi:10.1542/PEDS.2014-3482
6. Almojarthe BM. Prevalence of attention deficit hyperactivity disorder in the Arab Gulf countries: systematic review and meta-analysis. Int J Community Med Public Health. 2023;10(2):833–841. doi:10.18203/2394-6040.IJCMPH20230247
7. Alzaben FN, Sehlo MG, Alghamdi WA, et al. Prevalence of attention deficit hyperactivity disorder and comorbid psychiatric and behavioral problems among primary school students in western Saudi Arabia. Saudi Med J. 2018;39(1):52–58. doi:10.15537/smj.2018.1.21288
8. Attention deficit hyperactivity disorder: diagnosis and management NICE guideline; 2018. Available from: www.nice.org.uk/guidance/ng87.
9. Ibrahim ESR. Rates of adherence to pharmacological treatment among children and adolescents with attention deficit hyperactivity disorder. Hum Psychopharmacol Clin Exp. 2002;17(5):225–231. doi:10.1002/HUP.406
10. Kempton S, Vance A, Maruff P, Luk E, Costin J, Pantelis C. Executive function and attention deficit hyperactivity disorder: stimulant medication and better executive function performance in children. Psychol Med. 1999;29(3):527–538. doi:10.1017/S0033291799008338
11. Emilsson M, Gustafsson PA, Öhnström G, Marteinsdottir I. Beliefs regarding medication and side effects influence treatment adherence in adolescents with attention deficit hyperactivity disorder. Eur Child Adolesc Psychiatry. 2017;26(5):559–571. doi:10.1007/s00787-016-0919-1
12. Adler LD, Nierenberg AA. Review of medication adherence in children and adults with ADHD. Postgrad Med. 2010;122(1):184–191. doi:10.3810/PGM.2010.01.2112
13. Sanchez RJ, Crismon ML, Barner JC, Bettinger T, Wilson JP. Assessment of Adherence Measures with Different Stimulants Among Children and Adolescents. Pharmacother J Human Pharmacol Drug Ther. 2005;25(7):909–917. doi:10.1592/PHCO.2005.25.7.909
14. Brinkman WB, Sucharew H, Majcher JH, Epstein JN. Predictors of Medication Continuity in Children With ADHD. Pediatrics. 2018;141(6). doi:10.1542/peds.2017-2580
15. Barner JC, Khoza S, Oladapo A. ADHD medication use, adherence, persistence and cost among Texas Medicaid children. Curr Med Res Opin. 2011;27(SUPPL. 2):13–22. doi:10.1185/03007995.2011.603303
16. Alqahtani MMJ. How do parents view psychological assessment and intervention for their children with ADHD in Saudi Arabia? Asia Pac J Couns Psychother. 2017;8(1):41–52. doi:10.1080/21507686.2016.1260612
17. Ahmed R, Borst JM, Yong CW, Aslani P. Do parents of children with attention-deficit/hyperactivity disorder (ADHD) receive adequate information about the disorder and its treatments? A qualitative investigation. Patient Prefer Adherence. 2014;8:661–670. doi:10.2147/PPA.S60164
18. Ferrin M, Taylor E. Child and caregiver issues in the treatment of attention deficit-hyperactivity disorder: education, adherence and treatment choice. Future Neurol. 2011;6(3):399–413. doi:10.2217/fnl.11.5
19. Charach A, Schachar R, Schachar R. Stimulant Treatment Over Five Years: adherence, Effectiveness, and Adverse Effects. J Am Acad Child Adolesc Psychiatry. 2004;43(5):559–567. doi:10.1097/00004583-200405000-00009
20. Wehmeier PM, Dittmann RW, Banaschewski T. Treatment compliance or medication adherence in children and adolescents on ADHD medication in clinical practice: results from the COMPLY observational study. Atten Defic Hyperact Disord. 2015;7(2):165–174. doi:10.1007/S12402-014-0156-8
21. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (Mars) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/S0920-9964(99)00130-9
22. Chan AHY, Horne R, Hankins M, Chisari C. The Medication Adherence Report Scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/BCP.14193
23. Owie GO, Olotu SO, James BO. Reliability and validity of the Medication Adherence Rating Scale in a cohort of patients with schizophrenia from Nigeria. Trends Psychiatry Psychother. 2018;40(2):85–92. doi:10.1590/2237-6089-2017-0077
24. Alsous M, Alhalaiqa F, Farha RA, Jalil MA, Mcelnay J, Horne R. Reliability and validity of Arabic translation of Medication Adherence Report Scale (Mars) and Beliefs about Medication Questionnaire (BMQ)–specific for use in children and their parents. PLoS One. 2017;12(2):e0171863. doi:10.1371/JOURNAL.PONE.0171863
25. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
26. Safavi P, Saberzadeh M, Tehrani AM. Factors associated with treatment adherence in children with attention deficit hyperactivity disorder. Indian J Psychol Med. 2019;41(3):252–257. doi:10.4103/IJPSYM.IJPSYM_456_18
27. Biederman J, Fried R, DiSalvo M, et al. Evidence of low adherence to stimulant medication among children and youths with ADHD: an electronic health records study. Psychiatric Serv. 2019;70(10):874–880. doi:10.1176/appi.ps.201800515
28. Van Cleave J, Leslie LK. Approaching ADHD as a chronic condition: implications for long-term adherence. J Psychosoc Nurs Ment Health Serv. 2008;46(8):28–37. doi:10.3928/02793695-20080801-07
29. Safavi P, Saberzadeh M, Tehrani AM. Factors Associated with Treatment Adherence in Children with Attention Deficit Hyperactivity Disorder. Indian J Psychol Med. 2019;41(3):252–257. doi:10.4103/IJPSYM.IJPSYM_456_18
30. Sitholey P, Agarwal V, Chamoli S. A preliminary study of factors affecting adherence to medication in clinic children with attention-deficit/hyperactivity disorder. Indian J Psychiatry. 2011;53(1):41–44. doi:10.4103/0019-5545.75561
31. Al-Harthi H, Al-Huseini S, Al-Shukaili M, et al. Parental Attitude Towards the Prescription of Psychotropic Medications for Mental Disorders in Children in a Tertiary Care University Hospital in Oman. Sultan Qaboos Univ Med J. 2023;23(2):190–197. doi:10.18295/squmj.8.2022.049
32. Greenhill LL, Pliszka S, Dulcan MK. Practice Parameter for the Use of Stimulant Medications in the Treatment of Children, Adolescents, and Adults. J Am Acad Child Adolesc Psychiatry. 2002;41(2):26S–49S. doi:10.1097/00004583-200202001-00003
33. Schachter HM, Pham B, King J, Langford S, Moher D. How efficacious and safe is short-acting methylphenidate for the treatment of attention-deficit disorder in children and adolescents? A meta-analysis. CMAJ. 2001;165(11):1475.
34. Brown RT, Amler RW, Freeman WS, et al. Treatment of Attention-Deficit/Hyperactivity Disorder: overview of the Evidence. Pediatrics. 2005;115(6):e749–e757. doi:10.1542/PEDS.2004-2560
35. Swanson J. Compliance with stimulants for attention-deficit/hyperactivity disorder: issues and approaches for improvement. CNS Drugs. 2003;17(2):117–131. doi:10.2165/00023210-200317020-00004
36. Biederman J, Wilens T, Mick E, Spencer T, Faraone SV. Pharmacotherapy of attention-deficit/hyperactivity disorder reduces risk for substance use disorder. Pediatrics. 1999;104(2):e20–e20. doi:10.1542/PEDS.104.2.E20
37. Wilens T, Pelham W, Stein M, et al. ADHD treatment with once-daily OROS methylphenidate: interim 12-month results from a long-term open-label study. J Am Acad Child Adolesc Psychiatry. 2003;42(4):424–433. doi:10.1097/01.CHI.0000046814.95464.7D
38. Steele M. A randomized, controlled effectiveness trial of OROS-methylphenidate compared to usual care with immediate-release methylphenidate in attention deficit-hyperactivity disorder. Can J Clin Pharmacol. 2006;13(4):50–62.
39. Efron D, Jarman F, Barker M. Methylphenidate Versus Dexamphetamine in Children With Attention Deficit Hyperactivity Disorder: a Double-blind, Crossover Trial. Pediatrics. 1997;100(6):e6–e6. doi:10.1542/PEDS.100.6.E6
40. Banaschewski T, Roessner V, Dittmann RW, Santosh PJ, Rothenberger A. Non-stimulant medications in the treatment of ADHD. Eur Child Adolesc Psychiatry. 2004;13(1). doi:10.1007/s00787-004-1010-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.