")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Trauma-Informed Care in Psychedelic Therapy Research: A Qualitative Literature Review of Evidence-Based Psychotherapy Interventions in PTSD and Psychedelic Therapy Across Conditions
Authors Modlin NL , Creed M, Sarang M , Maggio C, Rucker JJ , Williamson V
Received 30 July 2023
Accepted for publication 10 November 2023
Published 20 January 2024 Volume 2024:20 Pages 109—135
DOI https://doi.org/10.2147/NDT.S432537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Nadav Liam Modlin,1 Michael Creed,1,2 Maria Sarang,1 Carolina Maggio,1 James J Rucker,1,2 Victoria Williamson3,4
1The Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, SE5 8AF, UK; 2South London and Maudsley NHS Foundation Trust, Maudsley Hospital, Denmark Hill, London, SE5 8AZ, UK; 3King’s Centre for Military Health Research, King’s College London, London, SE5 9RJ, UK; 4Department of Experimental Psychology, Anna Watts Building, University of Oxford, Oxford, OX2 6 GG, UK
Correspondence: Nadav Liam Modlin, The Institute of Psychiatry, Psychology and Neuroscience, King’s College London, 16 De Crespigny Park, London, SE5 8AF, UK, Email [email protected]
Introduction: Post-traumatic stress disorder (PTSD) is associated with significant patient burden. While pharmacotherapies and evidence-based psychotherapy interventions (EBPI) are effective, studies consistently highlight inadequate outcomes and high treatment dropout. Psychedelic therapy (PT) has shown preliminary promise across difficult-to-treat conditions, including MDMA-assisted therapy for PTSD, however trials of classical psychedelics in PTSD are lacking. Understanding patients’ experiences of EBPI could help promote safety in PT.
Aim: To systematically review qualitative research on patients’ subjective experience of EBPI for PTSD, and of PT, and examine areas of overlap and divergence between them.
Methods: Systematic literature searches for studies published between 2010 and 2023 were conducted on OVID, PubMed, Web of Science, and PsycInfo. Included were original studies in English that presented qualitative data of patient experiences of EBPI in PTSD, or PT for any indication. Extracted data from included studies were analysed using thematic synthesis. Syntheses were completed separately for EBPI and PT, before similarities and differences between the therapies were identified.
Results: 40 research articles were included for review: 26 studies on EBPI for PTSD, and 14 studies on PT. EBPI studied were CBT, EMDR, CPT and PE. Psychedelic compounds studied were psilocybin, ibogaine, LSD, MDMA and ketamine, for treatment of substance use disorders, anxiety relating to physical illness, depression, and PTSD. Core themes from patient experiences of EBPI: 1) patient burden in PTSD treatment; 2) readiness; 3) key mechanisms of change; 4) psychological safety and trust. Themes identified in the review of PT: 1) indirect trauma processing; 2) reorganisation of self-narratives via processes of relatedness and identification; 3) key treatment characteristics.
Conclusion: This study suggests overlap between patients’ experience of EBPI and PT in terms of key mechanisms of change, the importance of psychological safety and readiness to engage in treatment. Trauma-informed care paradigms and practices may improve safety and acceptability of PT research.
Keywords: trauma, PTSD, psychotherapy, psychedelic therapy, qualitative, review
Introduction
Trauma exposure is associated with an increased risk for psychopathology1–3 including post-traumatic stress disorder (PTSD), major depressive disorder (MDD) and dissociative disorders. PTSD, characterised by debilitating comorbid symptomatology and psychosocial dysfunction, is associated with significant individual and societal burden.4,5 Pharmacotherapies (eg, paroxetine and sertraline) and evidence-based psychotherapy interventions (EBPI) for PTSD, such as prolonged exposure (PE) or trauma-focused cognitive behavioural therapy (TF-CBT), are considered effective.6–8 Despite EBPIs effectiveness, studies consistently highlight difficulties, including inadequate treatment outcomes9,10 and poor patient retention.11 Psychological treatment of PTSD may be challenging and complex,12 potentially due to the significant symptomatic and psychosocial burden patients endure (eg, perceived negative experiences related to the treatment across different domains, including emotional, relational, physical, systemic, and practical aspects).13 Further, patients who find treatment ineffective and seek additional care are also at increased risk of re-traumatisation due to the need to repeatedly recount their traumatic experiences to providers.14
In response to the unmet clinical need in PTSD15, and difficult-to-treat mental-health conditions16, studies investigating psychedelic forms of therapy have shown promise in so-called “treatment-resistant” patients.17–21 Psychedelic therapy (PT) is an umbrella term for interventions administering serotonergic hallucinogens such as 4-phosphoryloxy-N,N-dimethyltryptamine (psilocybin) and lysergic acid diethylamide (LSD) or entactogens such as 3,4-Methyl enedioxy methamphetamine (MDMA) alongside manualised psychological interventions.22–25 Despite PT’s favourable safety profile in research settings and advances in understanding of its neurobiological, psychological, and behavioural effects,26–29 significant gaps of knowledge remain. Clinically, it is not well understood how PT supports positive outcomes across conditions and compounds.30 Positive results are often associated with patient reports of increased insightfulness,31 emotional breakthrough32 and mystical-type experiences,33 however, experimental studies are needed to establish causality. Importantly, qualitative research has highlighted the significance of the intervention’s non-pharmacological factors,34,35 including interpersonal rapport and music listening to positive outcomes.36,37
In PTSD, MDMA-assisted therapy appears highly efficacious in clinical trials, reducing symptoms and improving quality-of-life in patients with chronic PTSD.20,38 However, completed trials of classical psychedelics in PTSD are lacking, with several early phase studies recruiting as of October 2023. Correspondingly, there is an absence of trauma-focused clinical practice guidelines in PT. Despite considerable advances in treatments for PTSD in recent years,9 there remain significant challenges associated with standard PTSD treatment, including disruptions to the patient’s linguistic capacities and biological stress dysregulation.39 Therefore, considering patients’ experience of EBPI may help personalise care and promote safety outcomes for traumatised participants in PT trials. Further, as the number of psychedelic trials grow40 and with Australia approving the therapeutic use of MDMA and psilocybin in mental-health,41,42 it is vital that regulators, healthcare systems and clinicians have access to a repository of in-depth knowledge of patient experiences to inform operational, clinical, and training protocols that support patient safety. As most PT trial participants must be unsuccessfully treated by first-line interventions, understanding the positive and negative experiences of EBPI patients could help optimise PT protocols.
Qualitative research is well-placed to provide an in-depth understanding of patients’ subjective experience of trauma and treatment.43–45 Therefore, this research aims to review qualitative studies in EBPI for PTSD and PT, examining areas of intersectionality and divergence to promote a multidisciplinary dialogue. A synthesis of the themes in the selected studies will be conducted to provide a broad understanding of patients’ experience of the treatments. Based on the data, areas of clinical interest will be discussed to promote patient outcomes and safety in PT.
Methods
Search Strategy
A systematic literature search was conducted to identify papers studying patients’ qualitative experiences of either EBPI in PTSD, or PT. Given the paucity of existing qualitative literature on PT for PTSD, an expanded second search was conducted to include studies on PT for any clinical indication, including but not limited to depression, substance use disorders, and anxiety associated with life-threatening illness. The search was conducted between January and March 2023. Search terms related to PTSD, psychotherapy, psychedelics, qualitative methods, and patient experience were defined (Table S1) and entered in major research databases (OVID, PubMed, Web of Science, and PsycInfo). Reference lists of included studies on PT and specific relevant journals specialising in psychedelic science and traumatology were manually searched to ensure suitable articles were not missed. Transparent Reporting of Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed.46 The systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO).
Eligibility Criteria
Papers deemed eligible for inclusion were original, peer-reviewed studies presenting qualitative data with an identifiable qualitative research methodology (eg, grounded theory, interpretative phenomenological analysis, etc.), focused on patient experiences of either EBPI in PTSD, or PT for any indication. Papers must have been published between January 2010 and March 2023. This date range was chosen as modern psychedelic research began to emerge after 2010, and such a date range would allow comparison with contemporaneous EBPI literature.
Papers were excluded if they did not present new research (eg, systematic reviews), were not peer-reviewed, not published in English, studied others’ experiences (eg, clinicians, family members) or indications other than PTSD (unless studying psychedelics, where any clinical indication was included as previously outlined). Studies were also excluded if they were not specifically studying the experience of EBPI, or if they were studying internet- or phone-based therapy only. Mixed-methods studies were included if qualitative data of patient experiences was clearly presented. PRISMA diagrams for both literature searches are presented in Figures 1 and 2.
 |
Figure 1 PRISMA flow diagram of evidence-based psychotherapy interventions (EBPI) literature search. |
 |
Figure 2 PRISMA flow diagram for psychedelic therapy (PT) literature search. |
Selected papers were assessed for quality using the Critical Appraisal Skills Programme (CASP) criteria.47 This involves assessing the paper across ten domains, and assigning a score of 0–10, 10 representing a paper of high quality. The overall quality of the included studies was high, with an average rating of 8.2 (range: 5–10) (see Tables 1 and 2).
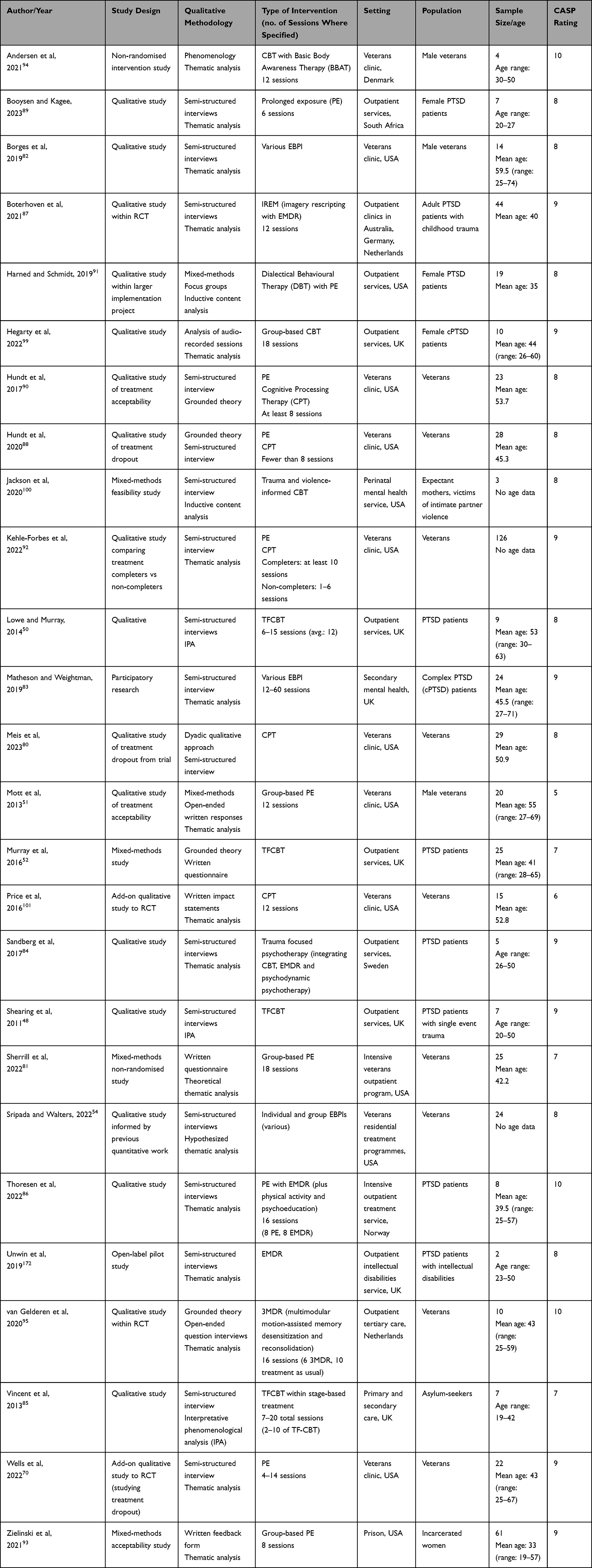 |
Table 1 Overview of EBPI Study Methodologies, Settings, Sample Characteristics and CASP Quality Ratings |
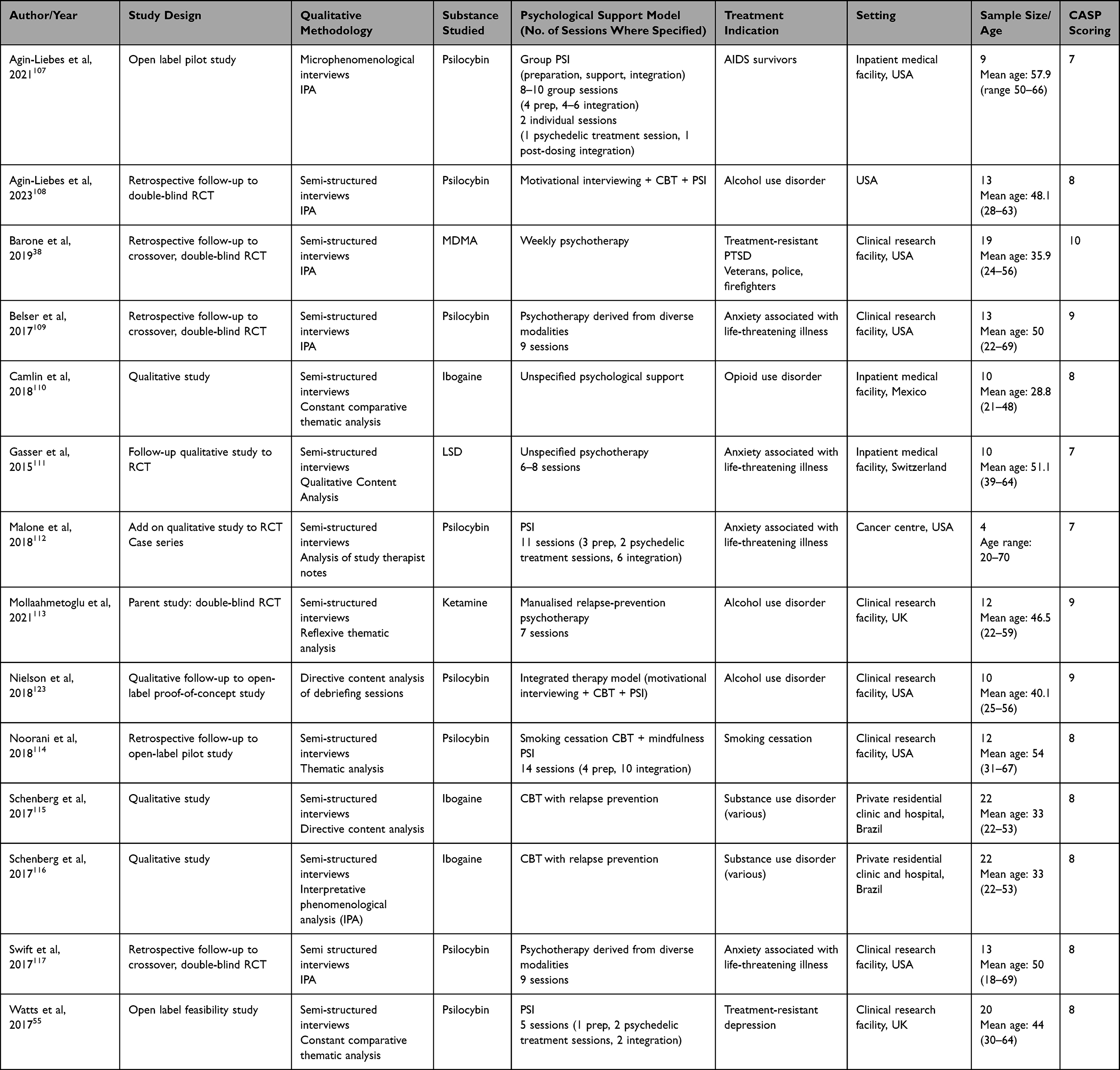 |
Table 2 Overview of PT Study Methodologies, Settings, Sample Sizes and CASP Quality Ratings |
Data Extraction
Data from the included studies were extracted and included: author/year; study design; qualitative methodology; psychological intervention; setting; sample size; demographics; key themes identified; and data relating to patients’ reported experiences. Authors NLM and MC systematically reviewed papers and extracted the data, cross-checking data for concordance.
Data Analysis
Extracted data from the studies was analysed using thematic synthesis.79 Author NLM read and re-read the data before assigning open-coded descriptive themes to the results. Once all themes were assigned, these were then distilled into core themes, with sub-themes to supplement and expand on the core themes. These themes were then reviewed by VW and MC and agreed upon by all authors.
A thematic synthesis was completed separately for the studies of EBPI and studies of PT. After completing these thematic syntheses, similarities and differences between the therapies were identified. Our findings from the EBPI synthesis are presented first, followed by the key themes found across PT studies. Excerpts from included studies are presented to illustrate key findings with additional excerpts in Table S2.
Results
EBPI in PTSD
The initial search returned 1286 papers. After screening and assessing papers for eligibility, the final number included was 26 (see Figure 1 for screening details).
Of the included studies, the majority were conducted in the USA (n=12) and the UK (n=6), with one study each in Denmark, the Netherlands, South Africa, Norway, and Sweden. Psychotherapies studied were TF-CBT (n=6), PE (n=5), eye-movement desensitisation and reprocessing (EMDR, n=3), cognitive processing therapy (CPT, n=2), with a number of studies (n=9) on various or combined therapies. Study designs varied between standalone qualitative studies (n=11), qualitative analyses within clinical trials (n=7), treatment acceptability studies (n=4), and mixed methods (n=3). See Table 1 for further details.
Psychedelic Therapy
128 papers were initially found on PT. After screening and eligibility assessment, 14 papers were included in the review (see Figure 2 for screening details).
Studies were primarily conducted in the USA (n=8), with others in the UK (n=2), Brazil (n=2), Mexico (n=1) and Switzerland (n=1). Psilocybin (n=8) was the substance most studied, with other studies investigating ibogaine (n=3), LSD, MDMA and ketamine (all n=1). Indications for treatment included substance use disorders (n=7), anxiety relating to physical illness (n=5), depression and PTSD (both n=1). See Table 2 for further details.
EBPI in PTSD
Patient Burden in PTSD Treatment
All EBPI studies (n=26) highlighted patient-reported burdens associated with PTSD treatment. For some patients, tolerating these challenges appeared to increase feelings of agency. However, in many cases, this experience caused distress and destabilisation, at times, impacting patient retention.
This synthesis found 4 prominent sub-themes associated with patient-reported burden:
- Real-World Barriers
- Tolerating Treatment Emergent Adverse Events
- Misaligned Treatment Rationale and Expectancy
- Interpersonal difficulties with staff and peers
Real-World Barriers
Related to engaging in treatment, patients across studies reported practical concerns regarding scheduling and travel difficulties and competing practical, financial and/or relational demands.88,91 This was compounded by the psychological burden associated with the treatment (eg, symptom exacerbation) and pre-existing psychosocial stressors. Patients expressed concerns about the potential adverse impact of the treatment on their psychosocial functioning during and after treatment.52,80,81,92 Patients discussed feeling conflicted about complying with the treatment as this often competed with their on-going “real-world” responsibilities.
I felt very overwhelmed, and I felt very lost and very frantic in what I had to do [for therapy]. Especially having the homework to do, but then knowing I could not do it. Because I knew my reaction was going to upset my daughters. So, then trying to find time later at night, but then writing about all of that would disturb my sleep - what little I get. And the disturbed sleep would mean I was up all night. so it just kind of snowballed.80
Some patients reported concerns about the insufficient time allocated for treatment.81–83 These patients expressed their perception that the structure of weekly psychotherapy did not support the full achievement of therapeutic gains.
With weekly sessions, you never truly get over the trauma.81
For some patients, concerns regarding premature endings were also reported.83 This may be due to the short-term nature of the outpatient treatment, the treatment failing to address integral aspects of patients’ difficulties, and/or attachment-related anxieties known to contribute to PTSD psychopathology.49
The therapy has really helped, but I need more because I am just open, you know when you get that blast and you see that mushroom cloud, I am like the mushroom cloud it has not dissipated yet.83
This was contrasted with findings from residential or intensive treatment programs which seemed to mitigate patients’ avoidance of challenging feelings/symptoms, with some patients reporting that this type of care allowed them to get more out of the treatment.
Tolerating Treatment Emergent Adverse Events
All studies reported patients’ experience of intense and difficult to tolerate responses to treatment. Frequently reported internal states associated with exposure to traumatic material included fears about the pain associated with reliving due to the need to openly talk about and/or vividly imagine certain aspects of patients’ index-trauma. Correspondingly, trauma-related “maladaptive defenses”,84 such as experiential avoidance, were reported across most studies.
When you come, you have to really like talk about it and how you’re feeling and that brings it like to the surface and it’s really raw and that’s really hard and sometimes, you know, you don’t feel like doing that ‘cause it’s painful.85
Misaligned Treatment Rationale and Expectancy
Several studies50,80,86,87 highlighted the importance of providing psychoeducation regarding PTSD symptoms, the treatment’s rationale, and its expected effects to positive outcomes.
I really do not understand CPT. Like what it’s supposed to do? I would not really know.80
Studies also reported the significance of managing patient’s pre-treatment expectations and considering the degree of alignment between the treatment’s rationale, procedures, and patient’s needs.80,82,88–90
They [the clinicians] just want to go into the past, but we need or what I need is how to cope with what I have right now, and then everyday civilian life, instead of just regressing and getting to the roots.88
Interpersonal Difficulties with Staff and Peers
Studies highlighted patients’ interpersonal difficulties with clinical staff and, in group-based interventions with their peers, as factors influencing engagement in treatment and outcomes.70,82,91–93 At times these gave rise to patient feelings of disconnection and invalidation.80
I was pissed off that people were trying to desensitize me to something horrible that happened because it almost seems like, ‘Oh you’re overreacting just think about, just be around it enough and you won’t feel that way anymore.91
In group settings, studies reported the impact of negative perceptions of other group members on patient retention and outcomes.
I was overwhelmed with knowing that I would soon have to tell my story. The fear of exposure was almost too much.93
Demonstrating the clinical relevance of strong social support systems outside of the clinic on recovery, patients appeared to use relationships to adhere to the treatment protocol.
Studies70,88,91,92 also discussed how psychosocial stressors such as isolation adversely impacted participants’ experience of the treatment.
I did not really have anyone in-person to talk to. I did not really have a lot of support in terms of like family or friends, or relationships around me that were good.70
Readiness
Studies highlighted the contribution of intrapersonal factors (eg, patient traits, beliefs, and internal resources) to the overall experience of treatment.50–52,81,82,84,85,89–95 Most studies referred to the significant psychological burden PTSD treatment entails (eg, fear of re-traumatisation, worsening of symptoms and functional destabilization). Correspondingly, in this synthesis, we found that intrapersonal factors reportedly influenced patients’ perception of their experience of treatment, and conversely, their willingness to engage in often-challenging therapeutic processes. The umbrella term “readiness” was chosen by authors to reflect various sub-themes identified.96
Patients described processes of coming to terms with the severity of their PTSD symptoms and psychosocial difficulties. This form of tentative acceptance seemed important in overcoming ambivalence about seeking treatment and then, tolerating challenging aspects of the therapeutic process.
Some patients referred to deeply held personal desires and values that encouraged engagement in treatment.
I’m really scared to go into [dialectical behavioral therapy (DBT) prolonged exposure (PE). But. you get your DBT skills first [and] I think that’s what’s going to help me the most. I don’t want to live like this anymore. I deserve to be happy.91
Once in treatment, some patients reported intentional behaviors aimed at making the most out of their treatment, cultivating a willingness to face fears associated with reliving their index-trauma.50–52,81,82,84,85,89–95 In contrast, in the context of possessing a willingness to confront pain, some participants reported feeling incapable of engaging fully in imaginal exposure to traumatic events. This may be due to use of defenses, such as avoidance, and hesitancy about engaging in treatment due to psychosocial instability.53,97
Because I avoided talking about things, I probably didn’t get the full help I could have gotten.82
Key Mechanisms of Change
Reviewed studies suggested a variety of key mechanisms of change associated with positive outcomes. EBPI in PTSD usually entails revisiting traumatic memories to gradually reduce hyper- and hypo-arousal states, characterised by nervous system dysregulation, depersonalisation or dissociation.98 Aspects related to the previous theme (eg, “readiness”) appeared to support patients make use of the treatment process. Mechanisms of change identified in this synthesis include attainment of insight, behavioral activation, corrective emotional experiences, and changes in trauma narratives during and after treatment.
Patients who responded to treatment described attaining insight into their persistent responses to internal states associated with their index-trauma.50–52,81,87–90,95,99–101 Conversely, this may have also supported patients to feel validated and achieve a sense of mastery over their symptoms. Studies discussed the importance of cultivating self-awareness and possessing the capacity to notice “signals”94 surrounding the need for self-regulation.
If I was being triggered. usually it would come out in anger or fear. Before I did not really know why I was doing that and then throughout my therapy I realized it was the fear of their vulnerability.100
In addition to consolidating learning pertaining to individual responses to traumatic stimuli, some treatment responders discussed achieving greater recall of the event, which appeared to play a significant part in the therapeutic process.95
That went a little deeper with every session. And with every trauma, actually. At some point, I could recall things that I had never. That I had never thought about again, that never crossed my mind.95
Beyond attaining insight into emotional and behavioral responses to trauma, some patients described how greater insight facilitated corrective emotional experiences and shifts in their trauma narratives, accompanied by greater compassion towards self.51,87,93,101 Further, referring to the support and encouragement of the therapist, patients detailed how behavioral activation was facilitated by empowering therapists who promoted patients’ sense of agency and autonomy.
[The clinician] left a lot of decisions up to me. I felt like he was taking my experience into consideration and not just his diagnosis [of me]. I felt like he allowed me to take part in what I felt was going to work for me.92
In group-based interventions, fears of exposure and difficult relational dynamics could make it hard to engage in group-based interventions. However, for patients who responded well to the group setting, insights and corrective emotional experiences were facilitated by processes of identification with others, leading to feelings of validation and belonging.51,54
Psychological Safety and Trust
All studies highlighted the importance of psychological safety and trust in patient experience and PTSD treatment outcomes. This core theme distinguishes between psychological safety (PS) and trust. PS in healthcare settings refers to a myriad of systemic and interpersonal attributes leading to a shared belief that the treatment setting is safe to engage in interpersonal risk-taking.102 In the context of mental-health care, PS enhances patient security and feelings of empowerment through promoting an organisational culture imbued with openness and mutual respect.103 Conversely, trust refers to the interpersonal dynamic established between the provider and patient.104 Trust is considered a fundamental component in trauma-informed models of care due to high rates of betrayal and harmful relational power dynamics reported in trauma survivors.105,106
This synthesis identified 3 sub-themes, which taken together, were found to contribute towards and determine the quality of PS and trust perceived by the patient.
These include:
4a. Experience of Therapist
4b. Experience of Group and Wider Psychosocial Setting
4c. Experience of Self
Experience of Therapist
Across all studies, patients reported positive and negative reactions to their therapists which impacted their engagement in treatment. Possessing trust in the therapists’ attunement and competency was associated with patient feelings of safety and validation. This appeared to enhance patients’ ability to engage in the often-challenging treatment processes by supporting openness and affective regulation. On the other hand, some studies70,80,82,92 reported patients felt misunderstood or interpersonally hurt following interactions with their therapists. These occurrences appeared to hinder treatment engagement, highlighting the centrality of interpersonal trust in trauma-focused psychotherapy.
The trust in her [the clinician] and the fact that she understands me and can keep up with me and actually get to know me. This is very, very important.94
Experience of Group and Wider Psychosocial Setting
Patients reported both positive and negative reactions to the impact and clinical utility of group-based interventions. Positive perceptions of the group were characterised by increased feelings of belonging, confidence, and openness. Some patients reported increased anxiety about exposure in a group setting. Hearing the traumatic narratives and experiences of their peers appeared to be challenging in itself.93,99 Others discussed the presence and impact of difficult interpersonal dynamics that emerged in the group.93,99
I found some parts a bit triggering when people recounted their personal experiences. I felt quite frozen and couldn’t speak. I found it harder to concentrate and felt myself go into a darker place when discussing suicide.99
Experience of Self
Patients described a range of positive and negative responses to PTSD treatment that affected their sense of trust and confidence in self.70,85,89,90,95,101 In turn, this seemed, at times, to impact their belief in their ability to endure and benefit from the treatment. Patients described a gradual process characterised by noticing moderate positive changes or differences in their self-narratives, beliefs, and emotional responses.
I noticed changes, I noticed differences. I thought, it is helping. So, let me just come back.89
Correspondingly, patients also described how adverse responses to treatment negatively impacted their perception of self and capacity to utilise the treatment.
I became depressed, withdrawn, I started to have some nightmares again, and I tried it for about a week, and it kept getting worse and worse and I said this is not worth it. I did not feel physically and mentally able to continue because of those reasons.70
Psychedelic Therapy
Although the studies varied in their methodology, patient populations, and psychedelic compounds, there were themes relating to the patient experience of PT in clinical trials that were consistently reported. We present a snapshot of our findings relating to trauma-informed PT below.
Themes identified in this review:
- Indirect Trauma Processing
- Reorganisation of self-narratives via processes of relatedness and identification
- Key Treatment Characteristics
Indirect Trauma Processing
Studies referred to traumatic stress as being a main contributing factor to psychopathology.55,107–117 In most studies, processing traumatic incidents appeared to be an integral part of the narrative surrounding patients’ experience of the therapeutic process. Researchers reported patients confronting adverse childhood events and present-day stressors such as life-threatening diagnoses. Although not the explicit focus of the PT intervention, trauma-related material appeared in the form of visualisations, disturbing conscious and previously repressed memories, somatic trauma responses, and emotional states such as grief and fear. Some patients reported how the treatment supported integrating traumatic incidents into their lives or unburdening themselves from its weight as part of the change process.
Mostly from my childhood, related to my parents quarrelling. I saw a lot of bad things. I saw my father bribing my mother with jewelry, flattering her with leisure activities, with superfluous things. I saw him drinking, falling down where he stored his drinks.115
Reorganisation of Self-Narratives via Processes of Relatedness and Identification
All studies reported themes concerning patients’ perceived changes in self-narratives after PT. Reported changes in self-narratives may be catalysed or accompanied by the previously highlighted mechanisms of change in PT.56,71,118,119 Further, increases in caring emotional responses towards self,57 connectedness towards others,55 experience of positive affect120 and health behavior change121 have been reported.
This synthesis found patients reported changes in self-narratives after describing meaningful PT experiences characterised by processes of relatedness and identification across the following domains:
1a. With psychedelic compound
1b. With condition
1c. With the known biographical self, including body
1d. With significant others
1e. With spiritual or transcendental states
1f. With clinical team
Psychedelic Compound
Patients reported perceiving the compound itself as possessing intentions and wisdom, attributing personifying meaning to the elicited subjective effects, and experiencing a helpful intrapersonal form of communication between self and the compound. Patients discussed how the compound seemingly “gave” or “showed” them something of importance, highlighting areas that required their attention and encouraging engagement with previously avoided challenging experiences.38,55,110,111 Infused with this knowledge or newfound sense of direction, patients reportedly felt reassured and had a perceived sense of empowerment. It is possible that these occurrences may have in turn supported better treatment engagement.
During the session the thoughts were … “Do I travel the right path”? That was my question. Not dealing with death during the session but if I am on the right path. LSD gave me the feeling intensively that I am on the right path. That was nice.111
Condition
Patients reported the presence of a helping relationship between the compound and their condition. Potentially promoting cognitive flexibility,122 patients appeared to have gained a sense of internal space or distance between self and the condition via the interaction between the compound and the condition.55,110,112,116,117,123 Correspondingly, these processes were often accompanied by positive cognitive reconstructions related to the nature of the condition, increased positive affect and reduction in adverse psychological symptoms.
I would say [I have] less anxiety about my body and my sickness coming back, my cancer coming back…I saw this body for what it’s worth, I picked it, it’s mine… I think that acceptance has been liberating.112
Known Biographical Self, Including Body
Patients described how PT appeared to facilitate a reexamination of past as well as present and at times, imagined future oriented, life experiences.38,55,107,112–116 Patients reported perceiving important life experiences during their treatment via imagery, cognitions, emotions, physical sensations, and memories. These biographical remembrances, directly linked with patients’ self-narratives, were reportedly imbued with meaning and affect, which in turn promoted a more open and reflective stance towards their challenging experience and self-representation.
I don’t know if I really learned – it was more like letting back in stuff that I had blocked out?… I don’t think I changed my values, just remembered more of them. Or just remembered to honor them more, or…allow them more.114
Significant Others
Patients described exploring past and present relationships with loved ones and friends.55,107,109,111,113,117,123 Patients described perceiving with more clarity and appropriate affect relational ruptures and experiencing resolution. Some patients reported feeling supported by their loved ones during the psychedelic treatment session, enhancing feelings of connectedness and the significance of others in their own self-narratives.117,123 Notably, some patients reported perceiving the presence of an internal “guide” or a “being” which appeared to have their best interests at heart; at times appearing as a loved one.109,112
I was thinking about relationships I had with other people and thinking I could see them clearly almost as if for the first time. I had fresh insight into things. It was almost as if suddenly the scales dropped from my eyes, I could see things as they really are.55
Transcendental / Spiritual States
Across the included studies, patients reported various transcendental or spiritual states.55,107–117 Patients reported feelings of unity, ego dissolution, profound connection to others, the natural world and the universe. These states, potentially leading to perspective change and feelings of greater contentedness, were often accompanied by a range of intense affects and a visceral sense of knowing. Within these states, some patients reported grappling with existential themes concerning birth and dying. Overall, patients reported dramatically changed perspectives concerning everyday reality, at times accompanied by a greater appreciation towards self, others, and life itself. These experiences were also characterised by an overarching sense of persuasiveness and purposefulness.
I see myself as part of something bigger. I felt myself connected into what had to be the collective mind yesterday, realizing it’s like “Oh, this exists, and we’re all just facets of this. It’s me connected to a wider sense of life or consciousness. And it’s, like, I know that rationally, but it was a time to feel it in a very real sense and experience it as real”.107
Clinical Team
Patients described the significance of therapists’ presence across most studies to positive outcomes. The degree of rapport and interpersonal safety with therapists was associated with feelings of trust towards the often challenging and unfamiliar treatment process. Some, but not all, patients discussed their therapists as an integral component of the treatment, supporting engagement by conveying a sense of confidence in the patient’s capacity to leverage their experience towards improvement.38,55,107–109,113,114 Notably, only one study55 highlighted instances of negative perceptions of therapists and its potential adverse influence on outcomes. These incidents included a brief discussion of a “problematic transference”, in which the patient linked their negative responses towards a therapist with previous experiences of care.
It’s not just the psilocybin sessions [but] it’s that human connection, and the support that comes with that human connection, that ultimately leads to success at the end of the day.114
Key Treatment Characteristics
Ineffability and Awe
Some patients found it difficult to describe or find the “right words” to convey their experience of the psychedelic session.55,107,109–111,113,114,117,123 The richness of the reported experiences and its corresponding therapeutic impact can be inferred by observing treatment responders’ language, often laden with metaphors, symbols, affect and a sense of meaningfulness. When describing their experience, patients appeared to be struck by the multifaceted nature and novelty of PT. Acknowledging the limits of intellectual understanding, most patients in the reviewed studies appeared to be curious about their experience, or positively affected by this sense of awe173 as opposed to being disturbed by it. Of note, the MDMA-AT study112 did not report similar themes. This may be due to the mechanism of action and subjective effects of MDMA, an entactogen, as opposed to classical psychedelics.
It was a feeling beyond an intellectual feeling—it was a feeling to the bottom of my core. that’s one reason that it’s hard to talk about. it’s beyond words.117
Immersive Experiential Immediacy and Intensity
Patients across most studies reported vivid descriptions of intense experiential processes characterised by immersive and dramatic physiological and psychological responses to the compound’s subjective effects and treatment process.38,55,109–116,123 The immediacy effect of the treatment was reported in the context of having direct and unavoidable encounters with the unfolding phenomena observed during their psychedelic treatment session. Of note, the immersive and intense nature of the treatment appeared to empower patients to confront rather than avoid both negative and positive cognitions, emotions, and somatic reactions to the treatment.
I feel like what happened was that in a very short period of intense time I dealt with some really powerful things and put it behind me.109
Arc of Struggle and Distress Towards Resolution
Patients reported being compelled to engage with challenging experiences in the service of promoting healing and change.38,55,107–111,114–117,123 Patients reported a sense of working through burdensome aspects of their experience catalysed by the compound (eg, intense emotional states, somatic reactions, ego-dissolution, and complex imagery) to eventually perceive a sense of resolution. These experiences were characterised by a sense of movement between previously avoided internal states, and a sense of momentum, which appeared to support patients to engage with the unfolding experience. Terms such as “rollercoaster”111 or “turbulence”114 were identified. Acceptance of the struggle and possessing a willingness to engage in experiential excursions into challenging states, appeared supportive in achieving a meaningful perception of resolution.
It was an intense, intense struggle, and that’s where it became medicinal because it allowed that struggle to happen. It didn’t coat it, it wasn’t an antidepressant. it brought it all out.117
Change Beyond Symptom Reduction
Across all studies patients reported responses to treatment that appeared beyond the scope of symptomatic reduction. Patients’ post-treatment made references to possessing a changed perspective regarding self, others, and the world. These shifts were accompanied by a sense of clarity about what matters most (eg, values) and a determination to make meaningful changes aligned with these values. At times philosophical, these changes appeared to be a consequence of and catalyst for increased positive affect post-treatment. Frequently reported values pertained to the importance of meaningful relationships, possessing a more curious stance towards self and others, and a sense of connection to spiritual aspects in everyday life, including the natural world. Of note, patients often reported changes in behavior that appeared to support these shifts, including initiating meditation practices, engaging in new hobbies, and repairing relationships.
I’ve been involved with the local literacy council all the time now … And then the other thing is I’ve become very involved with this environmental group as well … instead of sitting around and just watching television and smoking and doing nothing.114
Difference from Other Treatments
Some studies described patients’ reports of how PT differed from standard treatment.55,110,111,115,117 These accounts were in support of PT over first-line treatments. This is unsurprising given that PT trials are for patients who have not been helped by standard treatments. PT appeared to accelerate therapeutic processes (eg, promoting insights, enhancing access to a wider range of affects, and facilitating a more immediate connection to self during and after treatment). Patients reported confronting, as opposed to avoiding, challenging and yet necessary therapeutic processes. In the context of addressing psychophysical ailments including addiction and cancer-related distress, patients referred to the need for a holistic and integrated approach to care.
In usual psychotherapy it is mainly about talking, about words. In LSD-assisted psychotherapy it is mainly about inner processes, inner change, inner experience, it gets enriched by it.111
Importance of Non-Pharmacological Factors
Studies highlighted patients’ accounts concerning the central importance of the treatment’s non-pharmacological factors.38,55,107,109,111,112,114,116,121,123 Factors often referred to include the impact of therapist presence and interventions, the significance of music and the focus of the non-psychedelic sessions (eg, preparation / integration). Patients made references to the therapeutic utility of the actual physical environment of the psychedelic session, including the lights and sonic ambience inside the treatment room. In a group-based intervention, patients made references to other patients undergoing the treatment. Positive reactions to these factors appeared to enhance feelings of safety and in turn encourage greater immersion in the psychedelic state.
I started not just hearing, but playing the music. My entire body was the musical instrument for every sound which was coming through my head.112
Discussion
This synthesis explores salient themes in patient experience of EBPI in PTSD and PT for mental-health indications in authorised, medically supervised, clinical trials. This study identified a total of 7 key themes from the thematic analysis of the included papers. In EBPI: Patient Burden, Psychological Safety and Trust, Readiness and Key Mechanisms of Change. In PT: Reorganisation of Self-Narratives via Processes of Relatedness and Identification, Indirect Trauma Processing and Key Treatment Characteristics (Figure 3).
 |
Figure 3 Core Themes diagram demonstrating the 7 key themes from Psychedelic Therapy (PT) and Evidence-based Psychotherapy Interventions (EBPI) in PTSD which may contribute to Trauma Informed Care (TIC) in PT. |
Overall, the included studies demonstrated that EBPI in PTSD and PT across indications compel the patient to contend with a range of arduous processes in the service of recovery. In both treatment paradigms, patients highlighted the intense biopsychosocial nature and heavy demands of treatment. Applying insights from this review, below we expand on 5 areas relevant to positive safety outcomes in future PT research and practice.
Traumatic Stress in PT
An integral finding of this study pertains to the overarching presence of trauma-related psychopathology across indications in PT research. This may be due to higher prevalence of trauma exposure in treatment-resistant patient populations.124,125 Correspondingly, researchers have discussed the potential utility of PT to treat PTSD,72 citing psychedelics’ mechanisms of action58,126 and its hypothesised transdiagnostic utility.59,127
Given the prevalence of trauma-related psychopathology across mental-health conditions, the results of this study indicate it is crucial that PT research protocols consider the impact of trauma exposure on patients and the potential value of trauma-informed care (TIC)14,128,129 in mitigating adverse events. Adding to DSM-based conceptualisations of mental ill health,130 TIC considers the unique predispositions patients who have been exposed to traumatic events present with;73 treating the person, rather than the condition, within the context of their psychosocial and cultural lived-experience. Further, comparative research studies investigating the safety and effectiveness of adjunct psychotherapeutic interventions in PT are absent. In this context, some have advocated for CBT to be considered the “default” model in PT,131 while others have highlighted the utility of the common factors theory of psychotherapy,74 psychoanalytic psychology132 and non-specific psychological support.22 It is important that data is gathered to support or refute these hypotheses. However, until an evidence base is developed, implementing trauma-informed approaches, that carefully consider the biopsychosocial effects of psychedelics, may promote positive safety outcomes in PT research by personalising care.
As traumatic experiences may have elements of interpersonal or institutional betrayal, secrecy, or persecution,133,134 TIC highlights interpersonal and intrapersonal dimensions that require careful clinical consideration.135,136 Here we discuss factors relating to psychological safety and trust, which may help inform clinical practice in PT research.
Interpersonal Factors
Adverse interpersonal dynamics, also influenced by patients’ and therapists’ attachment styles contribute to the quality of the therapeutic alliance (TA).137–139 Higher TA scores are associated with greater symptom reduction in PTSD psychotherapy.60 In PT, one study found a correlation between TA and positive outcomes140 while another, larger and multi-centre study, did not find TA to moderate outcomes.141 Nevertheless, given the importance of non-pharmacological factors in PT and healthcare,142 the quality of interpersonal care is considered important to positive outcomes.143
This synthesis suggests that traumatised patients may be acutely sensitive to adverse relational and attachment dynamics that may emerge during and in response to treatment. These may include instances of empathic failures and therapist mis-attunement and power imbalances and ruptures.61,144,145 For example, in this synthesis EBPI patients highlighted the adverse impact of therapists prioritising rigid adherence to the treatment protocol over meaningful interpersonal contact.80,92
Further, excessive shame, past experiences of betrayal, and moral injury might make it difficult for traumatised patients to request support during intense PT sessions, potentially leading to feelings of isolation and withdrawal.75,133 Slipping into traumatic awareness,76 some patients may experience these occurrences as traumatic reenactments, reminiscent of past experiences of neglect and abandonment.146 Taken together, clinicians should be mindful of patients’ experiences of interpersonal trauma, associated impact on personality147 and subsequent capacity to engage in PT, an intervention that may elicit profound regressive states.148
Intrapersonal Factors
Traumatised patients may be burdened by demoralising self-narratives often accompanied by persistent negative affect and negatively biased cognitions.9,149 Failing to achieve progress in treatment may reinforce these self-narratives, potentially leading to increased psychiatric destabilisation and psychosocial dysfunction. Correspondingly, PT trial participants may be more susceptible to these intrapersonal dispositions, perceiving themselves as having failed standard treatments as opposed to have been failed by treatments. Coupled with the high expectations some patients hold towards PT,150 failing to achieve progress may further corroborate these harmful self-narratives, increasing feelings of hopelessness and potentially leading to increased risk. Therefore, viewing these self-narratives as maladaptive but necessary psychological defenses in response to traumatic events may help mitigate patients’ pathologising styles of relating to self, increase curiosity and enhance safety outcomes. Taken together, to promote psychological safety and trust, this theme demonstrates the need to establish clinical and organisational cultures that promote consent, collaboration, agency, transparency, trustworthiness, and cultural humility in EBPI and PT.
Key Mechanisms of Change
This review highlighted a potential thematic overlap between EBPI and PT in the context of psychological mechanisms of change. Broadly, patients discussed how the treatments encouraged behavioral activation, and catalysed novel insights and corrective emotional experiences related to their symptoms and beliefs about self and others. While EBPI patients’ narratives were often focused on the impact of treatment on PTSD symptoms, PT patients reported therapeutic processes that were also linked to obtaining a greater sense of connection to their values, increased meaningfulness, and appreciation of the importance of spirituality. When delivering care in PT trials, it is important that clinicians working primarily in evidence-based approaches possess an appreciation of the clinical utility of value-based,151 meaning reconstructing,152 and psychospiritual processes153,154 on positive outcomes. Further, it has been suggested that PT may modulate psychological defenses,77,155 potentially leading to the immersive, experiential immediacy and intensity of the treatment. Correspondingly, this theme suggests that clinicians should be prepared to support patients through intense therapeutic processes, initiated and completed in a relatively short period of time. Modelling confidence and purposefulness without negating patient safety, clinicians should approach instances of struggle during PT as a potentially valuable component of the treatment process; sensitively conveying trust in the patients’ resources to utilise challenging occurrences during PT. Importantly, clinicians should be prepared to support patients who did not perceive an immediate sense of resolution and treatment non-responders, who may perceive challenging PT experiences as destabilising, potentially reinforcing harmful core beliefs and intensifying negative affect associated with unresolved conflicts.
Re-Organisation of Self-Narratives via Processes of Relatedness and Identification
Along with symptoms such as avoidance and hyperarousal, negative self-narratives may be a consequence of, and a maintaining factor, in trauma-related psychopathology.156,157 Broadly, self-narratives construct identities by organising life experiences into seemingly coherent stories that define the person’s subjective experience of self.158 Correspondingly, harmful self-narratives may include
Negative convictions about the self, low expectations about one’s efficacy and value, and an exaggerated preoccupation with the projected negative judgment of others.65
This study highlighted the potential transformative interaction between patient’s self-narratives and experiences elicited by the psychedelic compound and therapeutic context. Patients reported processes of relatedness and identification with the compound, significant others, and transcendental states. These intrapersonal processes, supported by the treatment’s non-pharmacological factors and potentially facilitated by the patients enhanced neural and cognitive plasticity,66 appeared to help participants re-organise damaging self-narratives. Shifting from “what is wrong with you?”, a self-narrative indicative of cognitive rigidity and blame, to “what happened to you?”; an exploratory and accepting stance towards self.159 This in turn appeared to support therapeutic gains by promoting curiosity towards entrenched negative autobiographies and increase openness to change. However, PT sessions are inherently unpredictable,67 potentially catalysing anxious ego-dissolution and intense negative affect160,161 that may reinforce patient’s harmful self-narratives. Further, positive and negative experiences in PT may increase patients’ suggestibility and vulnerability,68 potentially enhancing patients need and capacity for relatedness and identification. Correspondingly, this may enhance the potential for adverse idealising transferences162 and perceived instances of neglect, requiring thoughtful clinical management. Taken together, on-going therapist training, supervision, and ethical oversight is crucial to mitigate potential risks associated with PT.
Readiness
This research suggested that factors pertaining to patients’ perceived sense of readiness to engage in treatment contribute to positive outcomes. Readiness in this study refers to the patients’ capacity to tolerate intense negative affect, overcome defenses, possess an intentional desire to change and admit that one needs support.78,163 Despite the lack of empirical data, patients’ lack of readiness for treatment may be associated with poorer outcomes, including adverse reactions such as symptomatic deterioration and suicidality.164 Correspondingly, there is a lack of standardised best practices across PT studies, including screening measures evaluating patient’s suitability, rather than medical eligibility, for PT.69,165 Considering the novelty and multifaceted nature of PT, there is an urgent need to provide healthcare systems with validated assessment tools, personalising PT protocols to the patient’s presentation to promote positive and durable outcomes.
Further, this research demonstrated the significance of careful treatment staging and expectancy in outcomes. Treatment staging seeks to optimise outcomes by personalising the type and timing of the intervention to the patients’ current needs, resources, and risk of illness progression.166 As patients may perceive a discrepancy between their needs and abilities or lack a clear understanding concerning the treatment’s rationale, this review highlights the importance of accessible psychoeducation regarding PTs rationale and procedures prior, during and after treatment.
Real-World Barriers
This review demonstrates how patient burden can conflate both logistical factors and the often-demanding treatment procedures. PTSD treatment-specific challenges (eg, exacerbation of existing symptoms) may enhance patients’ sensitivity to so-called “real world” barriers (eg, travel, employment, relationships).167 Correspondingly, real-world difficulties may make it more challenging for patients to utilise interventions that in and of themselves may produce significant distress. Therefore, it is important clinicians pay attention to the patient’s everyday psychosocial circumstances during treatment; failing to situate the patient in the “real-world” or considering the impact of treatment emergent adverse events on psychosocial functioning may lead to poor outcomes. Of note, this finding was prominent in the EBPI group. This is likely due to EBPI being well-established and delivered across healthcare settings and the longer-term structure of treatment, mostly delivered on a weekly basis over the course of weeks/months. Given the immediate and intense effects of PT, if approved and delivered within public healthcare systems, significant consideration to the patient’s real-world responsibilities and realities will be required to promote durable safety and efficacy outcomes.
Implications
Reviewing the results presented in this paper, it is important to consider the implications of these findings. Firstly, our sample contains multiple and different interventions, indications, and cultures. However, we identified several thematic consistencies across the studies. Few of the studies presented conflicting ideas, thus it would be fair to conclude that the identified themes provide a fitting representation of patients’ experiences of EBPI and PT. Correspondingly, the results may support the design of future, trauma-informed, PT research studies exploring the potential safety and effectiveness of first-line psychological therapies as an adjunct to PT. Further, should psychedelic forms of therapy receive regulatory approval, providers will require specialist training to ensure patient safety. The findings of this study may support the development of patient-centred training and supervision programmes by demonstrating a clinical overlap between EBPI and PT and highlighting the similarities and differences of patients’ experience of the treatments.
Limitations
This study has several limitations. Firstly, we were unable to include papers not written in English. As a result, 37 EBPI in PTSD and 2 PT papers were excluded, which may have provided insight into patients’ experiences. An additional limitation is that PT studies generally appeared positively biased, often reporting the experience of treatment responders, and rarely discussing adverse events/responses. As psilocybin and MDMA edge nearer towards regulatory approval and rapid-onset, short-acting psychedelics with limited safety data are developed,168–170 it is vital that future qualitative studies target treatment emergent adverse events in PT to ensure patient safety and inform ethical practice guidelines.
Conclusions
Overall, this synthesis provides important insights into patients’ experience of EBPI in PTSD and PT across conditions. The synthesis provides clinicians unfamiliar with PT with an introductory understanding of the treatment’s opportunities, challenges, and procedures via the analysis of patients’ experiences. Correspondingly, this work provides PT research teams with a broader understanding of PTSD patients’ experience of first-line interventions, including barriers to treatment and the critical impact of traumatic-stress psychopathology on outcomes. Given the potential prevalence of trauma exposure in PT trial participants,171 incorporating transdiagnostic, trauma-informed paradigms of care in PT research protocols may improve safety and acceptability outcomes. Further, this study highlights the need for additional qualitative research in PT, with a particular focus on treatment non-responders. Critical qualitative methods and long-term follow up studies may provide valuable insights into potential interpersonal, intrapersonal, and psychosocial factors impacting outcomes. Lastly, as the field of PT matures, studies investigating the significance of the intervention’s non-pharmacological factors, therapist effects and the suitability of adjunct psychotherapeutic modalities on outcomes are needed. Focusing on patients’ experience, these studies may support a broader, multidisciplinary understanding of PT, identify potential psychological predictors of response, optimise clinical care, and improve treatment outcomes.
Ethical Approval
Ethical approval was not required for this study.
Acknowledgments
Authors thank Ekaterina Malievskaia, Rachel Yehuda, Chantelle Thomas, Scott Aaronson, Jeffrey Guss, Joanne Stubley, Amy Durden, Jan Mars, Mark Burton, and Marc B. Aixalà for sharing their expertise in psychedelic therapy and the treatment of psychological trauma. Special thanks to Tyler McPhee for supporting this work with his extensive knowledge of psychedelic therapy research literature.
Author Contributions
NLM, MC, VW and JR designed the study, in consultation with CM and MS. The first draft of the manuscript was written by NLM. All authors contributed to the execution of the study including search strategy, data extraction, data analysis, writing and critically reviewing the manuscript. NLM, MC and MS contributed to the preparation of the supplementary material. All authors have approved the final manuscript.
Funding
No specific funding was provided towards the review.
Disclosure
All authors declare:
- No shareholdings in pharmaceutical companies
- No shareholdings in companies developing psychedelics
- Dr Rucker, Mr. Nadav Liam Modlin and Ms. Carolina Maggio provide services for the psychoactive trials group at King’s College London. The psychoactive trials group at King’s College London receives grant funding (received and managed by King’s College London) from Compass Pathways, Supporting Wounded Veterans, Multidisciplinary Association for Psychedelic Studies, Beckley PsyTech and National Institute for Health Research.
- Dr Rucker is supported by the UK National Institute for Health Research (NIHR) via Clinician Scientist Fellowship Awards to Dr. Rucker (CS-2017-17-007) and by the NIHR Biomedical Research Centre at South London, Maudsley National Health Service Foundation Trust, and King’s College London. Dr. Rucker has attended trial-related meetings paid for by Compass Pathways, Ltd.; he has consulted for Beckley PsyTech and Clerkenwell Health; and he is employed by Sapphire Medical Clinics, a private medical clinic.
- Nadav Liam Modlin has received consulting fees from Compass Pathways PLC, Small Pharma Ltd and Beckley Psytech Ltd. Carolina Maggio has received consulting fees from Beckley Academy, Entheon Biomedical and Compass Pathways.
References
1. Goldenson J, Kitollari I, Lehman F. The relationship between ACEs, trauma-related psychopathology and resilience in vulnerable youth: implications for screening and treatment. J Child Adol Trauma. 2021;14(1):151–160. doi:10.1007/s40653-020-00308-y
2. Roberts NP, Back SE, Mueser KT, Murray LK. Treatment considerations for PTSD comorbidities. In: Forbes D, Bisson JI, Monson CM, Berliner L, editors. Effective Treatments for PTSD: Practice Guidelines from the International Society for Traumatic Stress Studies. The Guilford Press; 2020:417–450.
3. Solomon SD, Davidson JR. Trauma: prevalence, impairment, service use, and cost. J Clin Psychiatry. 1997;58(9):5–11.
4. Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61:4–14.
5. Watson P. PTSD as a public mental health priority. Curr Psychiatry Rep. 2019;21(7):1–12. doi:10.1007/s11920-019-1032-1
6. Cukor J, Olden M, Lee F, Difede J. Evidence-based treatments for PTSD, new directions, and special challenges. AnN N Y Acad Sci. 2010;1208:82–89. doi:10.1111/j.1749-6632.2010.05793.x
7. Ipser JC, Stein DJ. Evidence-based pharmacotherapy of post-traumatic stress disorder (PTSD). Int J Neuropsychopharmacol. 2012;15(6):825–840. doi:10.1017/S1461145711001209
8. Schnurr PP. Focusing on trauma-focused psychotherapy for posttraumatic stress disorder. Curr Opin Psychol. 2017;14:56–60. doi:10.1016/j.copsyc.2016.11.005
9. Burback L, Brémault-Phillips SNJM, McFarlane A, Vermetten E. Treatment of posttraumatic stress disorder: a state-of-the-art review. Curr Neuropharmacol. 2023;21. doi:10.2174/1570159X21666230428091433
10. Leichsenring F, Steinert C, Rabung S, Ioannidis JPA. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry. 2022;21(1):133–145. doi:10.1002/wps.20941
11. Najavits LM. The problem of dropout from “gold standard PTSD therapies. F1000prime Rep. 2015;7. doi:10.12703/P7-43
12. Black TG. Psychotherapy and outcome research in PTSD: understanding the challenges and complexities in the literature. Can J Counselling Psychothera. 2004;38(4):277–287.
13. Nottingham N, Chadwick C. Conceptualizing a new definition of patient burden. Ann Fam Med. 2022;20(1):2772.
14. Reeves R. A synthesis of the literature on trauma-informed care. Issues Ment Health Nurs. 2015;36(9):698–709. doi:10.3109/01612840.2015.1025319
15. Krystal JH, Davis LL, Neylan TC, et al. It is time to address the crisis in the pharmacotherapy of posttraumatic stress disorder: a consensus statement of the PTSD psychopharmacology working group. Biol Psychiatry. 2017;82(7):e51–e59. doi:10.1016/j.biopsych.2017.03.007
16. Howes OD, Thase ME, Pillinger T. Treatment resistance in psychiatry: state of the art and new directions. Mol Psychiatry. 2022;27(1):58–72. doi:10.1038/s41380-021-01200-3
17. Galvão-Coelho NL, Marx W, Gonzalez M. Classic serotonergic psychedelics for mood and depressive symptoms: a meta-analysis of mood disorder patients and healthy participants. Psychopharmacology. 2021;238(2):341–354. doi:10.1007/s00213-020-05719-1
18. Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression: impact on patient-reported depression severity, anxiety, function, and quality of life. J Affect Disord. 2023;327:120–127. doi:10.1016/j.jad.2023.01.108
19. Ko K, Kopra EI, Cleare AJ, Rucker JJ. Psychedelic therapy for depressive symptoms: a systematic review and meta-analysis. J Affect Disord. 2023;322:194–204. doi:10.1016/j.jad.2022.09.168
20. Mitchell JM, Bogenschutz M, Lilienstein A, et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled Phase 3 study. Nat Med. 2021;27(6):1025–1033. doi:10.1038/s41591-021-01336-3
21. Zeifman RJ, Yu D, Singhal N, Wang G, Nayak SM, Weissman CR. Decreases in suicidality following psychedelic therapy: a meta-analysis of individual patient data across clinical trials. J Clin Psychiatry. 2022;83(2):39235.
22. Goodwin GM, Malievskaia E, Fonzo GA, Nemeroff CB. Must psilocybin always assist psychotherapy? Am J Psychiatry. 2023. doi:10.1176/appi.ajp.20221043
23. Mithoefer MC. Manual for MDMA-assisted psychotherapy in the treatment of posttraumatic stress disorder; 2015.
24. Nutt D. Psychedelic drugs—a new era in psychiatry? Dialogues Clin Neurosci. 2019;21(2):139–147. doi:10.31887/DCNS.2019.21.2/dnutt
25. Schenberg EE. Psychedelic-assisted psychotherapy: a paradigm shift in psychiatric research and development. Front Pharmacol. 2018;9:733. doi:10.3389/fphar.2018.00733
26. Elk M, Yaden DB. Pharmacological, neural, and psychological mechanisms underlying psychedelics: a critical review. Neurosci Biobehav Rev. 2022;140:104793. doi:10.1016/j.neubiorev.2022.104793
27. Breeksema JJ, Kuin BW, Kamphuis J, Brink W, Vermetten E, Schoevers RA. Adverse events in clinical treatments with serotonergic psychedelics and MDMA: a mixed-methods systematic review. J Psychopharmacol. 2022;36(10):1100–1117. doi:10.1177/02698811221116926
28. Banks MI, Zahid Z, Jones NT, Sultan ZW, Wenthur CJ. Catalysts for change: the cellular neurobiology of psychedelics. Mol Biol Cell. 2021;32(12):1135–1144. doi:10.1091/mbc.E20-05-0340
29. Vollenweider FX, Preller KH. Psychedelic drugs: neurobiology and potential for treatment of psychiatric disorders. Nat Rev Neurosci. 2020;21(11):611–624. doi:10.1038/s41583-020-0367-2
30. Nutt D, Spriggs M, Erritzoe D. Psychedelics therapeutics: what we know, what we think, and what we need to research. Neuropharmacology. 2023;223:109257. doi:10.1016/j.neuropharm.2022.109257
31. Davis AK, Barrett FS, So S, Gukasyan N, Swift TC, Griffiths RR. Development of the psychological insight questionnaire among a sample of people who have consumed psilocybin or LSD. J Psychopharmacol. 2021;35(4):437–446. doi:10.1177/0269881120967878
32. Roseman L, Haijen E, Idialu-Ikato K, Kaelen M, Watts R, Carhart-Harris R. Emotional breakthrough and psychedelics: validation of the emotional breakthrough inventory. J Psychopharmacol. 2019;33(9):1076–1087. doi:10.1177/0269881119855974
33. Ko K, Knight G, Rucker JJ, Cleare AJ. Psychedelics, mystical experience, and therapeutic efficacy: a systematic review. Front Psychiatry. 2022;13:917199. doi:10.3389/fpsyt.2022.917199
34. Carhart-Harris RL, Roseman L, Haijen E, et al. Psychedelics and the essential importance of context. J Psychopharmacol. 2018;32(7):725–731. doi:10.1177/0269881118754710
35. Johnson MW, Richards WA, Griffiths RR. Human hallucinogen research: guidelines for safety. J Psychopharmacol. 2008;22(6):603–620. doi:10.1177/0269881108093587
36. Breeksema JJ, Niemeijer AR, Krediet E, Vermetten E, Schoevers RA. Psychedelic treatments for psychiatric disorders: a systematic review and thematic synthesis of patient experiences in qualitative studies. CNS Drugs. 2020;34(9):925–946. doi:10.1007/s40263-020-00748-y
37. Crowe M, Manuel J, Carlyle D, Lacey C. Experiences of psilocybin treatment for clinical conditions: a qualitative meta-synthesis. Int J Mental Health Nurs. 2023;32(1):1–13. doi:10.1111/inm.13110
38. Barone W, Beck J, Mitsunaga-Whitten M, Perl P. Perceived benefits of MDMA-assisted psychotherapy beyond symptom reduction: qualitative follow-up study of a clinical trial for individuals with treatment-resistant PTSD. J Psychoactive Drugs. 2019;51(2):199–208. doi:10.1080/02791072.2019.1580805
39. McFarlane AC, Yehuda R. Clinical treatment of posttraumatic stress disorder: conceptual challenges raised by recent research. Aust N Z J Psychiatry. 2000;34(6):940–953. doi:10.1080/000486700268
40. Borissova A, Rucker J. The development of psilocybin therapy for treatment-resistant depression: an update. BJPsych Bulletin. 2023;1–7. doi:10.1192/bjb.2023.25
41. Eisenstein M. The psychedelic escape from depression. Nature. 2022;609(7929):87–89. doi:10.1038/d41586-022-02872-9
42. Kisely S. The down-scheduling of MDMA and psilocybin(e): too fast and too soon. Aust N Z J Psychiatry. 2023;57(7):933–934. doi:10.1177/00048674231174171
43. Angelo FN, Miller HE, Zoellner LA, Feeny NC. I need to talk about it: a qualitative analysis of trauma-exposed women’s reasons for treatment choice. Behav Ther. 2008;39(1):13–21. doi:10.1016/j.beth.2007.02.002
44. Corbin J, Strauss A. Basics of qualitative research: techniques and procedures for developing grounded theory. Organ Res Methods. 2008;12(3):614–617.
45. Sutton J, Austin Z. Qualitative research: data collection, analysis, and management. Can J Hosp Pharm. 2015;68(3):226–231. doi:10.4212/cjhp.v68i3.1456
46. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;88:n71.
47. Anonymous. 2022. Critical Appraisal Skills Programme.
48. Shearing V, Lee V, Clohessy S. How do clients experience reliving as part of trauma-focused cognitive behavioural therapy for posttraumatic stress disorder. Psychol Psychother. 2011;84(4):458–475. doi:10.1111/j.2044-8341.2010.02012.x
49. Woodhouse S, Ayers S, Field AP. The relationship between adult attachment style and post-traumatic stress symptoms: a meta-analysis. J. Anxiety Disord. 2015;35:103–117. doi:10.1016/j.janxdis.2015.07.002
50. Lowe C, Murray C. Adult service-users’ experiences of trauma-focused cognitive behavioural therapy. J Contemp Psychother. 2014;44:223–231.
51. Mott JM, Sutherland RJ, Williams W, Lanier SH, Ready DJ, Teng EJ. Patient perspectives on the effectiveness and tolerability of group-based exposure therapy for posttraumatic stress disorder: preliminary self-report findings from 20 veterans. Psychol Trauma. 2013;5(5):453. doi:10.1037/a0029386
52. Murray H, Merritt C, Grey N. Clients’ experiences of returning to the trauma site during PTSD treatment: an exploratory study. Behav Cognitive Psychother. 2016;44(4):420–430. doi:10.1017/S1352465815000338
53. Favaretto TC, Both LM, Benetti SPDC, Freitas LHM. Relationship between psychodynamic functioning, defensive mechanisms and trauma in patients with PTSD?. Trends Psychiatry Psychother. 2023. Available from: https://trends.org.br/article/doi/10.47626/2237-6089-2022-0546. Accessed December 28, 2023.
54. Sripada RK, Walters HM. ‘I wish people could come together like we have,’patient and provider perspectives on VA residential PTSD treatment. Psychological Services. 2022;20(4). Available from: https://web.s.ebscohost.com/abstract?direct=true&profile=ehost&scope=site&authtype=crawler&db=pdh&jrnl=15411559&asa=N&AN=2023-03399-001&h=J2tBOgVg9NW7mNoOYNjTFa1rZ%2bv7RX1%2b6r5h637UbRrhb6U6N7Ey%2fVLdiI3%2bk7BoL1uvCuKKsy2VQV8rp38G3Q%3d%3d&crl=c&resultNs=AdminWebAuth&resultLocal=ErrCrlNotAuth&crlhashurl=login.aspx%3fdirect%3dtrue%26profile%3dehost%26scope%3dsite%26authtype%3dcrawler%26db%3dpdh%26jrnl%3d15411559%26asa%3dN%26AN%3d2023-03399-001. Accessed December 28, 2023.
55. Watts R, Day C, Krzanowski J, Nutt D, Carhart-Harris R. Patients’ accounts of increased “connectedness” and “acceptance” after psilocybin for treatment-resistant depression. J Humanistic Psychol. 2017;57(5):520–564. doi:10.1177/0022167817709585
56. Moreton SG, Szalla L, Menzies RE, Arena AF. Embedding existential psychology within psychedelic science: reduced death anxiety as a mediator of the therapeutic effects of psychedelics. Psychopharmacology. 2020;237(1):21–32. doi:10.1007/s00213-019-05391-0
57. Fauvel B, Strika-Bruneau L, Piolino P. Changes in self-rumination and self-compassion mediate the effect of psychedelic experiences on decreases in depression, anxiety, and stress. Psychol Consciousness. 2021;10(1):88–102.
58. Krediet E, Bostoen T, Breeksema J, Schagen A, Passie T, Vermetten E. Reviewing the potential of psychedelics for the treatment of PTSD. Int J Neuropsychopharmacol. 2020;23(6):385–400. doi:10.1093/ijnp/pyaa018
59. Bird CIV, Modlin NL, Rucker JJH. Psilocybin and MDMA for the treatment of trauma-related psychopathology. Int Rev Psychiatry. 2021;33(3):229–249. doi:10.1080/09540261.2021.1919062
60. Howard R, Berry K, Haddock G. Therapeutic alliance in psychological therapy for posttraumatic stress disorder: a systematic review and meta‐analysis. Clin Psychol Psychother. 2022;29(2):373–399. doi:10.1002/cpp.2642
61. Safran JD, Muran JC. The resolution of ruptures in the therapeutic alliance. J Consul Clin Psychol. 1996;64(3):447–458. doi:10.1037/0022-006X.64.3.447
62. Brown LA, Belli GM, Asnaani A. A review of the role of negative cognitions about oneself, others, and the world in the treatment of PTSD. Cogn Ther Res. 2019;43:43143–43173.
63. Crespo M, Fernández-Lansac V. Memory and narrative of traumatic events: a literature review. Psychological Trauma. 2016;8(2):149. doi:10.1037/tra0000041
64. Ranjbar N, Erb M, Mohammad O, Moreno FA. Trauma-Informed Care and Cultural Humility in the Mental Health Care of People from Minoritized Communities. Vol. 18. Focus (American Psychiatric Publishing); 2020.
65. Ginot E. Self-narratives and dysregulated affective states: the neuropsychological links between self-narratives, attachment, affect, and cognition. Psychoanal Psychol. 2012;29(1):59. doi:10.1037/a0023154
66. Zeifman R, Spriggs M, Kettner H, et al. From Relaxed Beliefs Under Psychedelics (REBUS) to Revised Beliefs After Psychedelics (REBAS): preliminary development of the relaxed beliefs questionnaire (reb-q). Sci Rep. 2022. Available from: https://spiral.imperial.ac.uk/handle/10044/1/102760. Accessed December 28, 2023.
67. Modlin NL, Stubley J, Maggio C, Rucker JJ. On redescribing the indescribable: trauma, psychoanalysis and psychedelic therapy. Br J Psychother. 2023;39(3):551–572. doi:10.1111/bjp.12852
68. Villiger D, Trachsel M. With great power comes great vulnerability: an ethical analysis of psychedelics’ therapeutic mechanisms proposed by the REBUS hypothesis. J Med Ethics. 2023;49(12):826–832. doi:10.1136/jme-2022-108816
69. Feduccia A, Agin-Liebes G, Price CM, Grinsell N, Paradise S, Rabin DM. The need for establishing best practices and gold standards in psychedelic medicine. J Affect Disord. 2023;332:47–54. doi:10.1016/j.jad.2023.03.083
70. Wells SY, Morland LA, Hurst S, et al. Veterans’ reasons for dropping out of prolonged exposure therapy across three delivery modalities: a qualitative examination. Psychol Serv. 2023;20(3):483. doi:10.1037/ser0000714
71. Johansen L, Liknaitzky P, Nedeljkovic M. The psychological processes of classic psychedelics in the treatment of depression: a systematic review protocol. Syst Rev. 2022;11:85.
72. Varker T, Watson L, Gibson K, Knight H, O’Donnell M. Hallucinogens as Treatments for PTSD, Anxiety and Depression: A Rapid Evidence Assessment. Report Prepared for the Department of Veterans’ Affairs. Phoenix Australia Centre for Posttraumatic Mental Health; 2017.
73. Sweeney A, Taggart D. Understanding trauma-informed approaches in mental health. J Mental Health. 2018;27(5):383–387. doi:10.1080/09638237.2018.1520973
74. Gukasyan N, Nayak SM. Psychedelics, placebo effects, and set and setting: insights from common factors theory of psychotherapy. Transcult Psychiatry. 2022;59(5):652–664. doi:10.1177/1363461520983684
75. Williamson V, Murphy D, Phelps A, Forbes D, Greenberg N. Moral injury: the effect on mental health and implications for treatment. Lancet Psychiatry. 2021;8(6):453–455. doi:10.1016/S2215-0366(21)00113-9
76. L WD. Information processing bias in post-traumatic stress disorder. Open Neuroimaging J. 2008;2:229–251.
77. Abramson HA. LSD in psychotherapy and alcoholism. Am J Psychother. 1966;20(3):415–438. doi:10.1176/appi.psychotherapy.1966.20.3.415
78. Ogrodniczuk JS, Joyce AS, Piper WE. Development of the readiness for psychotherapy index. J Nerv Ment Dis. 2009;197(6):427–433. doi:10.1097/NMD.0b013e3181a61c56
79. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(8):45. doi:10.1186/1471-2288-8-45
80. Meis LA, Polusny MA, Kehle-Forbes SM, et al. Making sense of poor adherence in PTSD treatment from the perspectives of veterans and their therapists. Psychol Trauma. 2023;15(4):715. doi:10.1037/tra0001199
81. Sherrill AM, Maples-Keller JL, Yasinski CW, Loucks LA, Rothbaum BO, Rauch SA. Perceived benefits and drawbacks of massed prolonged exposure: a qualitative thematic analysis of reactions from treatment completers. Psychol Trauma. 2022;14(5):862. doi:10.1037/tra0000548
82. Borges LM, Bahraini NH, Holliman BD, Gissen MR, Lawson WC, Barnes SM. Veterans’ perspectives on discussing moral injury in the context of evidence‐based psychotherapies for PTSD and other VA treatment. J Clin Psychol. 2020;76(3):377–391. doi:10.1002/jclp.22887
83. Matheson C, Weightman E. A participatory study of patient views on psychotherapy for complex post-traumatic stress disorder, CPTSD. J Ment Health. 2021;30(6):690–697. doi:10.1080/09638237.2020.1803229
84. Sandberg J, Gustafsson S, Holmqvist R. Interpersonally traumatised patients’ view of significant and corrective experiences in the psychotherapeutic relationship. Eur J Psychother Counselling. 2017;19(2):175–199. doi:10.1080/13642537.2017.1313881
85. Vincent F, Jenkins H, Larkin M, Clohessy S. Asylum-seekers’ experiences of trauma-focused cognitive behaviour therapy for post-traumatic stress disorder: a qualitative study. Behav Cognitive Psychother. 2013;41(5):579–593. doi:10.1017/S1352465812000550
86. Thoresen IH, Auren TJB, Langvik EO, Engesæth C, Jensen AG, Klæth JR. Intensive outpatient treatment for post-traumatic stress disorder: a thematic analysis of patient experience. Eur J Psychotraumatol. 2022;13(1):2043639. doi:10.1080/20008198.2022.2043639
87. Boterhoven de Haan KL, Lee CW, Correia H, et al. Patient and therapist perspectives on treatment for adults with PTSD from childhood trauma. J Clin Med. 2021;10(5):954. doi:10.3390/jcm10050954
88. Hundt NE, Ecker AH, Thompson K, et al. “It didn’t fit for me:” A qualitative examination of dropout from prolonged exposure and cognitive processing therapy in veterans. Psychol Serv. 2020;17(4):414. doi:10.1037/ser0000316
89. Booysen DD, Kagee A. Trauma survivors’ perceptions and experiences of prolonged exposure for PTSD at a psychology clinic. South Af J Psychiatry. 2023;29:1869. doi:10.4102/sajpsychiatry.v29i0.1869
90. Hundt NE, Barrera TL, Arney J, Stanley MA. “It’s worth it in the end”: veterans’ experiences in prolonged exposure and cognitive processing therapy. Cogn Behav Pract. 2017;24(1):50–57. doi:10.1016/j.cbpra.2016.02.003
91. Harned MS, Schmidt SC. Perspectives on a stage-based treatment for posttraumatic stress disorder among dialectical behavior therapy consumers in public mental health settings. Community Ment Health J. 2019;55(3):409–419. doi:10.1007/s10597-018-0358-1
92. Kehle-Forbes SM, Ackland PE, Spoont MR, et al. Divergent experiences of US veterans who did and did not complete trauma-focused therapies for PTSD: a national qualitative study of treatment dropout. Behav Res Ther. 2022;154:104123. doi:10.1016/j.brat.2022.104123
93. Zielinski MJ, Karlsson ME, Bridges AJ. “I’m not alone, my story matters”: incarcerated women’s perspectives on the impact and acceptability of group psychotherapy involving imaginal exposure to sexual assault memories. Health Justice. 2021;9:1–14. doi:10.1186/s40352-021-00148-4
94. Andersen MR, Clausen A, Nielsen ABS, Svendsen ALH. Experiences with basic body awareness therapy as an add-on to cognitive behavioural therapy among Danish military veterans with PTSD: an interview study. J Bodywork Bodywork Ther. 2021;27:550–559. doi:10.1016/j.jbmt.2021.03.023
95. van Gelderen MJ, Nijdam MJ, Dubbink GE, Sleijpen M, Vermetten E. Perceived treatment processes and effects of interactive motion-assisted exposure therapy for veterans with treatment-resistant posttraumatic stress disorder: a mixed methods study. Eur J Psychotraumatol. 2020;11(1):1829400. doi:10.1080/20008198.2020.1829400
96. Cook JM, Simiola V, Hamblen JL, Bernardy N, Schnurr PP. The influence of patient readiness on implementation of evidence-based PTSD treatments in Veterans Affairs residential programs. Psychol Trauma. 2017;9(Suppl 1):51–58. doi:10.1037/tra0000162
97. Murray H, Grey N, Warnock-Parkes E, et al. Ten misconceptions about trauma-focused CBT for PTSD. Cognitive Behav Therapist. 2022;15:33. doi:10.1017/S1754470X22000307
98. Cook SC, Schwartz AC, Kaslow NJ. Evidence-based psychotherapy: advantages and challenges. Neurotherapeutics. 2017;14(3):537–545. doi:10.1007/s13311-017-0549-4
99. Hegarty S, Ehntholt K, Williams D, Kennerley H, Billings J, Bloomfield M. Acceptability and mechanisms of change associated with group cognitive behavioural therapy using the recovering from childhood abuse programme among women with CPTSD: a qualitative analysis. Cognitive Behav Therapist. 2022;15:e46. doi:10.1017/S1754470X2200037X
100. Jackson KT, Mantler T, Jackson B, Walsh EJ, Baer J, Parkinson S. Exploring mothers’ experiences of trauma and violence-informed cognitive behavioural therapy following intimate partner violence: a qualitative case analysis. J Psychosomatic Obstet Gynecol. 2020;41(4):308–316. doi:10.1080/0167482X.2019.1707799
101. Price JL, MacDonald HZ, Adair KC, Koerner N, Monson CM. Changing beliefs about trauma: a qualitative study of cognitive processing therapy. Behav Cognitive Psychother. 2016;44(2):156–167. doi:10.1017/S1352465814000526
102. Grailey KE, Murray E, Reader T, Brett SJ. The presence and potential impact of psychological safety in the healthcare setting: an evidence synthesis. BMC Health Serv Res. 2021;21(1):773. doi:10.1186/s12913-021-06740-6
103. Hunt DF, Bailey J, Lennox BR, Crofts M, Vincent C. Enhancing psychological safety in mental health services. Int J Mental Health Syst. 2021;15(1):33. doi:10.1186/s13033-021-00439-1
104. Crits-Christoph P, Rieger A, Gaines A, Gibbons MBC. Trust and respect in the patient-clinician relationship: preliminary development of a new scale. BMC Psychol. 2019;7(1):91. doi:10.1186/s40359-019-0347-3
105. DePrince AP, Brown LS, Cheit RE, et al. Motivated forgetting and misremembering: perspectives from betrayal trauma theory. True False Recovered Memories. 2012;2012:193–242.
106. Smith CP, Freyd JJ. Insult, then injury: interpersonal and institutional betrayal linked to health and dissociation. J Aggression Maltreat Trauma. 2017;26(10):1117–1131. doi:10.1080/10926771.2017.1322654
107. Agin-Liebes G, Ekman E, Anderson B, Malloy M, Haas A, Woolley J. Participant reports of mindfulness, posttraumatic growth, and social connectedness in psilocybin-assisted group therapy: an interpretive phenomenological analysis. J Humanistic Psychol. 2021;58:00221678211022949.
108. Agin-Liebes G, Nielson EM, Zingman M, et al. Reports of self-compassion and affect regulation in psilocybin-assisted therapy for alcohol use disorder: an interpretive phenomenological analysis. Psychol Addict Behav. 2023. doi:10.1037/adb0000935
109. Belser AB, Agin-Liebes G, Swift TC, et al. Patient experiences of psilocybin-assisted psychotherapy: an interpretative phenomenological analysis. J Humanistic Psychol. 2017;57(4):354–388. doi:10.1177/0022167817706884
110. Camlin TJ, Eulert D, Thomas Horvath A, Bucky SF, Barsuglia JP, Polanco M. A phenomenological investigation into the lived experience of ibogaine and its potential to treat opioid use disorders. J Psychedelic Stud. 2018;2(1):24–35. doi:10.1556/2054.2018.004
111. Gasser P, Kirchner K, Passie T. LSD-assisted psychotherapy for anxiety associated with a life-threatening disease: a qualitative study of acute and sustained subjective effects. J Psychopharmacol. 2015;29(1):57–68. doi:10.1177/0269881114555249
112. Malone TC, Mennenga SE, Guss J, et al. Individual experiences in four cancer patients following psilocybin-assisted psychotherapy. Front Pharmacol. 2018;9:256. doi:10.3389/fphar.2018.00256
113. Mollaahmetoglu OM, Keeler J, Ashbullby KJ, Ketzitzidou-Argyri E, Grabski M, Morgan CJ. “This is something that changed my life”: a qualitative study of patients’ experiences in a clinical trial of ketamine treatment for alcohol use disorders. Front Psychiatry. 2021;12:695335. doi:10.3389/fpsyt.2021.695335
114. Noorani T, Garcia-Romeu A, Swift TC, Griffiths RR, Johnson MW. Psychedelic therapy for smoking cessation: qualitative analysis of participant accounts. J Psychopharmacol. 2018;32(7):756–769. doi:10.1177/0269881118780612
115. Schenberg EE, de Castro Comis MA, Alexandre JFM, Chaves BDR, Tófoli LF, da Silveira DX. Treating drug dependence with the aid of ibogaine: a qualitative study. J Psychedelic Stud. 2017;1(1):10–19. doi:10.1556/2054.01.2016.002
116. Schenberg EE, de Castro Comis MA, Alexandre JFM, Tófoli LF, Chaves BDR, da Silveira DX. A phenomenological analysis of the subjective experience elicited by ibogaine in the context of a drug dependence treatment. J Psychedelic Stud. 2017;1(2):74–83. doi:10.1556/2054.01.2017.007
117. Swift TC, Belser AB, Agin-Liebes G, et al. Cancer at the dinner table: experiences of psilocybin-assisted psychotherapy for the treatment of cancer-related distress. J Humanistic Psychol. 2017;57(5):488–519. doi:10.1177/0022167817715966
118. Hayes SC, Law S, Malady M, Zhu Z, Bai X. The centrality of sense of self in psychological flexibility processes: what the neurobiological and psychological correlates of psychedelics suggest. J Contextual Behav Sci. 2020;15:30–38. doi:10.1016/j.jcbs.2019.11.005
119. Yaden DB, Griffiths RR. The subjective effects of psychedelics are necessary for their enduring therapeutic effects. ACS Pharmacol Transl. 2020;4(2):568–572. doi:10.1021/acsptsci.0c00194
120. Jungaberle H, Thal S, Zeuch A, et al. Positive psychology in the investigation of psychedelics and entactogens: a critical review. Neuropharmacology. 2018;142:179–199. doi:10.1016/j.neuropharm.2018.06.034
121. Teixeira PJ, Johnson MW, Timmermann C, et al. Psychedelics and health behaviour change. J Psychopharmacol. 2022;36(1):12–19. doi:10.1177/02698811211008554
122. Dajani DR, Uddin LQ. Demystifying cognitive flexibility: implications for clinical and developmental neuroscience. Trends Neurosci. 2015;38(9):571–578. doi:10.1016/j.tins.2015.07.003
123. Nielson EM, May DG, Forcehimes AA, Bogenschutz MP. The psychedelic debriefing in alcohol dependence treatment: illustrating key change phenomena through qualitative content analysis of clinical sessions. Front Pharmacol. 2018;9:132. doi:10.3389/fphar.2018.00132
124. Kaplan MJ, Klinetob NA. Childhood emotional trauma and chronic posttraumatic stress disorder in adult outpatients with treatment-resistant depression. J Nerv Ment Dis. 2000;188(9):596–601. doi:10.1097/00005053-200009000-00006
125. Williams L, Debattista C, Duchemin AM. Childhood trauma predicts antidepressant response in adults with major depression: data from the randomized international study to predict optimized treatment for depression. Transl Psychiatry. 2016;6(5):799. doi:10.1038/tp.2016.61
126. Elsouri KN, Kalhori S, Colunge D, et al. Psychoactive drugs in the management of post traumatic stress disorder: a promising new horizon. Cureus. 2022;14(5):25235.
127. Kočárová R, Horáček J, Carhart-Harris R. Does psychedelic therapy have a transdiagnostic action and prophylactic potential?. Front Psychiatry. 2021;12:661233. doi:10.3389/fpsyt.2021.661233
128. Butler LD, Critelli FM, Rinfrette ES. Trauma-informed care and mental health. Directions Psychiatry. 2011;31(3):197–212.
129. Anonymous. Substance Abuse and Mental Health Services Administration: Practical Guide for Implementing a Trauma-Informed Approach. SAMHSA Publication; 2023.
130. Kendler K. A history of the DSM-5 scientific review committee. Psychol. Med. 2013;43(9):1793–1800. doi:10.1017/S0033291713001578
131. Yaden DB, Earp D, Graziosi M, Friedman-Wheeler D, Luoma JB, Johnson MW. Psychedelics and psychotherapy: cognitive-behavioral approaches as default. Front Psychol. 2022;13:873279. doi:10.3389/fpsyg.2022.873279
132. Burton J, Ratner A, Cooper T, Guss J. Commentary: psychedelics and psychotherapy: cognitive-behavioral approaches as default. Front Psychol. 2022;13:6261.
133. Freyd JJ. What is a betrayal trauma? What is betrayal trauma theory? 2003. Available from: http://dynamic.uoregon.edu/~jjf/defineBT.html.
134. Smith CP, Freyd JJ. Institutional betrayal. Am. Psychol. 2014;69(6):575. doi:10.1037/a0037564
135. Sweeney A, Filson B, Kennedy A, Collinson L, Gillard S. A paradigm shift: relationships in trauma-informed mental health services. BJPsych Adv. 2018;24(5):319–333. doi:10.1192/bja.2018.29
136. Purkey E, Patel R, Phillips SP. Trauma-informed care: better care for everyone. Can Fam Physician. 2018;64(3):170–172.
137. Diener MJ, Monroe JM. The relationship between adult attachment style and therapeutic alliance in individual psychotherapy: a meta-analytic review. Psychotherapy. 2011;48(3):237. doi:10.1037/a0022425
138. Rubino G, Barker C, Roth T, Fearon P. Therapist empathy and depth of interpretation in response to potential alliance ruptures: the role of therapist and patient attachment styles. Psychother Res. 2000;10(4):408–420. doi:10.1093/ptr/10.4.408
139. Meyer B, Pilkonis PA. Attachment style. Psychotherapy. 2001;38(4):466. doi:10.1037/0033-3204.38.4.466
140. Murphy R, Kettner H, Zeifman R, et al. Therapeutic alliance and rapport modulate responses to psilocybin assisted therapy for depression. Front Pharmacol. 2022;12:788155. doi:10.3389/fphar.2021.788155
141. Anonymous compass ACNP pathway analysis[online]. Available from: https://compasspathways.com/wp-content/uploads/2022/11/COMPASS_ACNP_PathAnalysis.pdf.
142. Kornhaber R, Walsh K, Duff J, Walker K. Enhancing adult therapeutic interpersonal relationships in the acute health care setting: an integrative review. J Multidisciplinary Healthcare. 2016;2016:9537–9546.
143. Thal S, Engel LB, Bright SJ. Presence, trust, and empathy: preferred characteristics of psychedelic carers. J Humanistic Psychol. 2022;002216782210813. doi:10.1177/00221678221081380
144. Coutinho J, Ribeiro E, Hill C, Safran J. Therapists’ and clients’ experiences of alliance ruptures: a qualitative study. Psychother Res. 2011;21(5):525–540. doi:10.1080/10503307.2011.587469
145. Larsson MH, Falkenström F, Andersson G, Holmqvist R. Alliance ruptures and repairs in psychotherapy in primary care. Psychother Res. 2018;28(1):123–136. doi:10.1080/10503307.2016.1174345
146. S LM. A helpful way to conceptualize and understand reenactments. J Psychother Pract Res. 1998;7(3):227–235.
147. Yoo Y, Park H, Park S, Cho MJ, Cho S, Lee JY. Interpersonal trauma moderates the relationship between personality factors and suicidality of individuals with posttraumatic stress disorder. PLoS One. 2018;13(1):0191198. doi:10.1371/journal.pone.0191198
148. Maggio C, Fischer FM, Modlin NL, Rucker J. Psychoanalytic formulations in psychedelic therapy for Treatment Resistant Depression (TRD). J Psychol Psychother. 2023;13:451.
149. Byrne P. Psychiatric stigma. Br J Psychiatry. 2001;178(3):281–284. doi:10.1192/bjp.178.3.281
150. Butler M, Jelen L, Rucker J. Expectancy in placebo-controlled trials of psychedelics: if so, so what?. Psychopharmacology. 2022;239(10):3047–3055. doi:10.1007/s00213-022-06221-6
151. Berkout OV. Working with values: an overview of approaches and considerations in implementation. Behav Anal Pract. 2021;15(1):104–114. doi:10.1007/s40617-021-00589-1
152. Neimeyer R. Meaning reconstruction in the wake of loss: evolution of a research program. Behav Change. 2016;33(2):65–79. doi:10.1017/bec.2016.4
153. Ross S, Agrawal M, Griffiths RR, Grob C, Berger A, Henningfield JE. Psychedelic-assisted psychotherapy to treat psychiatric and existential distress in life-threatening medical illnesses and palliative care. Neuropharmacology. 2022;216:109174. doi:10.1016/j.neuropharm.2022.109174
154. Serfioti D, Murphy D, Greenberg N, Williamson V. Professionals’ perspectives on relevant approaches to psychological care in moral injury: a qualitative study. J Clin Psychol. 2023;79(10):2404–2421. doi:10.1002/jclp.23556
155. Thal SB, Bright SJ, Sharbanee JM, Wenge T, Skeffington PM. Current perspective on the therapeutic preset for substance-assisted psychotherapy. Front Psychol. 2021;12:617224. doi:10.3389/fpsyg.2021.617224
156. He Q, Veldkamp BP, Vries T. Screening for posttraumatic stress disorder using verbal features in self narratives: a text mining approach. Psychiatry Res. 2012;198(3):441–447. doi:10.1016/j.psychres.2012.01.032
157. Jaeger J, Lindblom KM, Parker-Guilbert K, Zoellner LA. Trauma narratives: it’s what you say, not how you say it. Psychological Trauma. 2014;6(5):473–481. doi:10.1037/a0035239
158. Dimaggio G, Salvatore G, Azzara C, Catania D. Rewriting self narratives: the therapeutic process. J Constr Psychol. 2003;16(2):155–181. doi:10.1080/10720530390117920
159. Harris M, Fallot R. Using Trauma Theory to Design Service Systems. New Directions for Mental Health Services. San Francisco, CA: Jossey-Bass; 2001.
160. Bender D, Hellerstein DJ. Assessing the risk–benefit profile of classical psychedelics: a clinical review of second-wave psychedelic research. Psychopharmacology. 2022;239(6):1907–1932. doi:10.1007/s00213-021-06049-6
161. Nour MM, Evans L, Nutt D, Carhart-Harris RL. Ego-dissolution and psychedelics: validation of the ego-dissolution inventory (EDI). Front Hum. 2016;10:269.
162. Hook J, Devereux D. Boundary violations in therapy: the patient’s experience of harm. BJPsych Adv. 2018;24(6):366–373. doi:10.1192/bja.2018.26
163. Krebs P, Norcross JC, Nicholson JM, Prochaska JO. Stages of change and psychotherapy outcomes: a review and meta-analysis. J Clin Psychol. 2018;74(11):1964–1979. doi:10.1002/jclp.22683
164. Linden M, Schermuly-Haupt ML. Definition, assessment and rate of psychotherapy side effects. World Psychiatry. 2014;13(3):306–309. doi:10.1002/wps.20153
165. Modlin NL, Miller TM, Rucker JJ, et al. Optimizing outcomes in psilocybin therapy: considerations in participant evaluation and preparation. J Affect Disord. 2023;326:18–25. doi:10.1016/j.jad.2023.01.077
166. Nijdam MJ, Vermetten E, McFarlane AC. Toward staging differentiation for posttraumatic stress disorder treatment. Acta Psychiatry Scand. 2023;147(1):65–80. doi:10.1111/acps.13520
167. Lewis C, Roberts NP, Gibson S, Bisson JI. Dropout from psychological therapies for post-traumatic stress disorder (PTSD) in adults: systematic review and meta-analysis. Eur J Psychotraumatol. 2020;11(1):1709709. doi:10.1080/20008198.2019.1709709
168. D’Souza DC, Syed SA, Flynn LT, Safi-Aghdam H, Cozzi NV, Ranganathan M. Exploratory study of the dose-related safety, tolerability, and efficacy of dimethyltryptamine (DMT) in healthy volunteers and major depressive disorder. Neuropsychopharmacology. 2022;47(10):1854–1862. doi:10.1038/s41386-022-01344-y
169. Lancelotta RL, Davis AK. Use of benefit enhancement strategies among 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT) users: associations with mystical, challenging, and enduring effects. J Psychoactive Drugs. 2020;52(3):273–281. doi:10.1080/02791072.2020.1737763
170. Heal DJ, Gosden J, Smith SL, Atterwill CK. Experimental strategies to discover and develop the next generation of psychedelics and entactogens as medications. Neuropharmacology. 2022;109375. doi:10.1016/j.neuropharm.2022.109375
171. Hogg B, Gardoki-Souto I, Valiente-Gómez A. Psychological trauma as a transdiagnostic risk factor for mental disorder: an umbrella meta-analysis. Eur Arch Psychiatry Clin Neurosci. 2023;273(2):397–410. doi:10.1007/s00406-022-01495-5
172. Unwin G, Willott S, Hendrickson S, Stenfert Kroese B. Eye movement desensitization and reprocessing for adults with intellectual disabilities: Process issues from an acceptability study. J Appl Res Intellect Disabil. 2019;32(3):635–647.
173. Hendricks PS Awe: a putative mechanism underlying the effects of classic psychedelic-assisted psychotherapy. Int Rev Psychiatry. 2018;30(4):331–342. doi:10.1080/09540261.2018.1474185
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.