")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Trauma-Informed Care: A Missing Link in Addressing Burnout
Authors Elisseou S
Received 19 April 2023
Accepted for publication 4 August 2023
Published 21 August 2023 Volume 2023:15 Pages 169—173
DOI https://doi.org/10.2147/JHL.S389271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Sadie Elisseou1,2
1Department of Medicine, Harvard Medical School, Boston, MA, USA; 2Department of Medicine, Boston University School of Medicine, Boston, MA, USA
Correspondence: Sadie Elisseou, Harvard Medical School, 22 Shattuck St., Boston, MA, 02115, USA, Tel +1 617-752-2689, Fax +1 774-826-3157, Email [email protected]
Abstract: The Covid-19 pandemic and national movements for health equity have highlighted the impact of trauma on public health as well as on health worker well-being. As burnout rates across healthcare climb, we seek creative and effective solutions. Current anti-burnout strategies focus on much needed systems solutions for employee success; however, they often lack a trauma-informed approach. Trauma is highly prevalent in society at large, and health workers are further exposed to trauma in the course of their professional studies and duties. Common symptoms of burnout may actually be manifestations of traumatic stress. Trauma-informed care (TIC) is a strategic framework and growing social movement for providing quality care to survivors of individual, interpersonal, collective, and structural trauma. Importantly, TIC has practical applications to address our healthcare burnout epidemic. In this perspective piece, an expert describes a trauma-informed lens through which to view burnout solutions using SAMHSA’s 4 Rs of a trauma-informed approach: 1) Realize the widespread impact of trauma, 2) Recognize the signs and symptoms in patients and staff, 3) Respond by integrating knowledge about trauma into practice, and actively 4) Resist re-traumatization. Moving forward, key stakeholders must collaborate to build and refurbish efficient systems alongside a trauma-informed organizational model. TIC can transform the healthcare experience for patients and employees alike by fostering community, empowerment, and healing.
Keywords: burnout, trauma, trauma-informed, mental health, healthcare
On May 23, 2022 the US Surgeon General Vivek Murthy, MD released an Advisory naming health worker burnout a national crisis.1 Burnout is an occupational phenomenon afflicting industries globally, and healthcare is among the top professions affected. The COVID-19 pandemic exacerbated what has long been an unresolved problem, with over 60% of health workers now reporting symptoms of burnout.2 Healthcare institutions are struggling to retain staff and maintain daily workplace operations, and rates of mental health concerns among clinical staff are climbing.3
Early pandemic efforts to combat the burnout epidemic targeted health workers’ personal resilience. Administrators offered programming on mindfulness and encouraged clinicians to invest in self-care. Current strategies are revisiting systems barriers to care delivery, such as optimizing EHR efficiency and workflows, and exemplary healthcare networks have built integrated wellness programs. Major organizations are investing in anti-burnout advocacy, including the National Academy of Medicine, Schwartz Center, Gold Foundation, Dr. Lorna Breen Heroes Foundation, and American Medical Association. These are crucial pursuits towards ending the burnout crisis. Yet unlocking the treatment for burnout requires a broadened understanding of the diagnosis.
Common symptoms of burnout—including mental exhaustion, helplessness, and detachment—may actually be manifestations of stress from trauma. The Substance Abuse and Mental Health Services Administration (SAMHSA) defines trauma as resulting from an event(s) or set of circumstances that is experienced as harmful or life-threatening and that has lasting, adverse effects on function and well-being.4 Trauma is highly prevalent in society at large, with nearly 90% of the US population experiencing at least one traumatic event in their lifetime.5
Traditionally, the medical community conceptualized trauma as a physical injury (eg broken bone). We now know that trauma can include community or intimate partner violence, racism, discrimination, war, natural disasters, medical illness, and pandemics. Our next step is to acknowledge trauma as an entity that not only affects our patients–it affects health professions trainees and employees, too. Health workers come into the profession with their own set of challenging lived experiences and have unique exposures to trauma in the course of their training and work. With this in mind, trauma may be the largest, underrecognized contributor to health worker burnout to date.
While the relationship between trauma and burnout is not fully understood, we know that cognitive overload reduces humans’ capacity to cope.6 Prior traumas can increase the likelihood of one perceiving future adversities as traumatic. For example, US Military Veterans with a history of adverse childhood experiences (ACEs) have a significantly higher likelihood of developing combat-related PTSD compared with Veterans without ACEs.7,8 There is a growing understanding among researchers that early adversity can result in trauma and its aftereffects, even in the absence of life-threatening events.9 Considering the cumulative impact of stress on the human brain and body, it is likely that chronic, unmanaged stress at work can worsen the symptoms of unmanaged trauma, and vice versa. Recent surveys of both physicians and nursing students demonstrated a statistically significant relationship between ACEs and burnout.10,11 Further research is needed to more clearly elucidate the statistical and neurobiological relationship between trauma and burnout.
While burnout research and advocacy are booming, there is less attention devoted to trauma-informed care (TIC), a related phenomenon with potential for transformational impact. TIC is an organizational framework and set of actionable guides to support trauma survivors. It emphasizes safety, empowerment, and healing through collaborative relationships. Practicing TIC requires an intentional approach in our interactions with ourselves, with others, and with the systems in which we live and work, to recognize the manifestations of trauma, promote recovery, and foster resilience. In this ripe environment of a burnout epidemic, TIC has expanded to public school systems,12 legal practices,13 medical education,14 and mainstream media.15 Importantly, TIC has practical applications to address our healthcare crisis.
This piece offers a trauma-informed lens through which to view burnout solutions. It follows SAMHSA’s 4 Rs of a trauma-informed approach: 1) Realize the widespread impact of trauma, 2) Recognize the signs and symptoms in patients and staff, 3) Respond by integrating knowledge about trauma into practice, and actively 4) Resist re-traumatization.3 Experts have applied this framework to core healthcare themes including quality patient care,16 health equity,17 and medical education.18 SAMHSA’s 4 pillars can also form the backbone of a wellness strategy that helps healthcare institutions recover from burnout and achieve organizational well-being. While a select number of healthcare institutions have integrated excellent programs such as the Stress First Aid19 or the Sanctuary Model20 for organizational healing, the majority of current anti-burnout strategies are lacking a trauma-informed framework.
Realize the Impact of Trauma
The foundational ACE Study demonstrated that over half of the US population has had at least one traumatic exposure before the age of 18, in the categories of abuse, neglect, or household dysfunction.21 Rates of ACEs among health professionals mirror rates of ACEs in the general population.22,23 In addition to trauma in childhood, both primary and secondary traumatization are occupational hazards of our jobs. In any given shift, we may experience microaggressions, workplace violence, or moral distress. We may also witness pain, suffering, injustice, and death. Healthcare professionals attend to the breadth of the human experience, including its most profound devastations. While each individual health worker’s experience of COVID-19 is distinct, the pandemic served as a mass exposure to trauma and further uncovered the pressing need to invest in healing our workforce.
While the primary drivers of burnout are structural, these individual and interpersonal experiences should not be dismissed. Acknowledging human factors does not mean that we blame or shame health workers. On the contrary, a trauma-informed paradigm shifts from the accusatory question, “What’s wrong with you?” to the more compassionate inquiry, “What happened to you?” Understanding the contributors to work-life stress at all levels can help us build more targeted, multifaceted solutions.
Recognize the Signs and Symptoms of Trauma
Our current methods for measuring burnout lend themselves to blurred lines between burnout symptoms and mental health conditions.24 Repeated or severe exposure to adversity can increase the risk of mental illness, and it can also lead to other health issues, like stroke, cancer, and early death.21 There are well-described, neurochemical mechanisms for these effects.25 In the workplace, trauma can affect our brain, body, and behaviors in a way that contributes to strained relationships with patients and coworkers, impaired concentration, missed work days, and inability to perform.26,27 Ultimately this may translate to the downstream effects we see from health worker burnout: a decline in productivity, reduced employee and patient satisfaction, high turnover, medical errors, and litigation.28,29
Physician suicide is a tragic event with complex contributors, including personal and structural variables. If we describe physician suicide as an outcome of burnout, we miss an opportunity to understand the role of traumatic stress in health worker morbidity and mortality. Trauma can disguise itself in the workplace as burnout, and trauma and burnout can coexist. The brain changes identified in burned-out workers actually align with the changes we find in the brains of persons with PTSD.6,30 Stress occurs along a spectrum, in defined neurobiologic pathways. If you are not inquiring about trauma, you will not know it’s there.
Respond with a Trauma-Informed Approach
A growing body of healthcare research shows promising benefits from TIC. A multi-year TIC implementation by a residential treatment agency demonstrated improved organizational climate, procedures and practices, staff and client satisfaction, and client retention.31 TIC curricula for PCPs result in increased knowledge and screening, as well as improved communication and patient satisfaction.32 TIC implementation can improve workplace and client satisfaction,33 and trauma-informed climate factors may result in reduced burnout.34
Trauma-informed principles resonate with evidence-based drivers of burnout (eg lack of control)29 as well as evidence-based protective factors (eg building community).35 SAMHSA’s 6 principles of TIC synergize with 4 out of the 6 categories of work stress identified by Maslach and Leiter that impact burnout: community, fairness, values, and control.36 There is an abundance of literature describing burnout, secondary traumatic stress, compassion fatigue, vicarious traumatization, and moral injury in clinicians. TIC complements these existing paradigms by including all health workers, both to better understand their suffering as well as to offer much needed solutions.
Table 1 demonstrates a simplified model of the progression of the medical community’s global views of trauma, burnout, and wellness over time. Our workplaces have made tremendous advances to date. Moving forward, healthcare leaders, staff, legislators, and stakeholders must collaborate to build the trauma-informed workplace of our future. SAMHSA has identified 6 key principles of a trauma-informed approach that can be integrated into healthcare systems: 1) Safety, 2) Trustworthiness and Transparency, 3) Peer Support, 4) Collaboration and Mutuality, 5) Empowerment, Voice and Choice, and attending to 6) Cultural, Historical, and Gender Issues. These principles are an optimal road map for healing and recovery, for individuals and communities. Health systems can apply TIC principles as a universal precaution, regardless of whether target groups have known trauma histories.
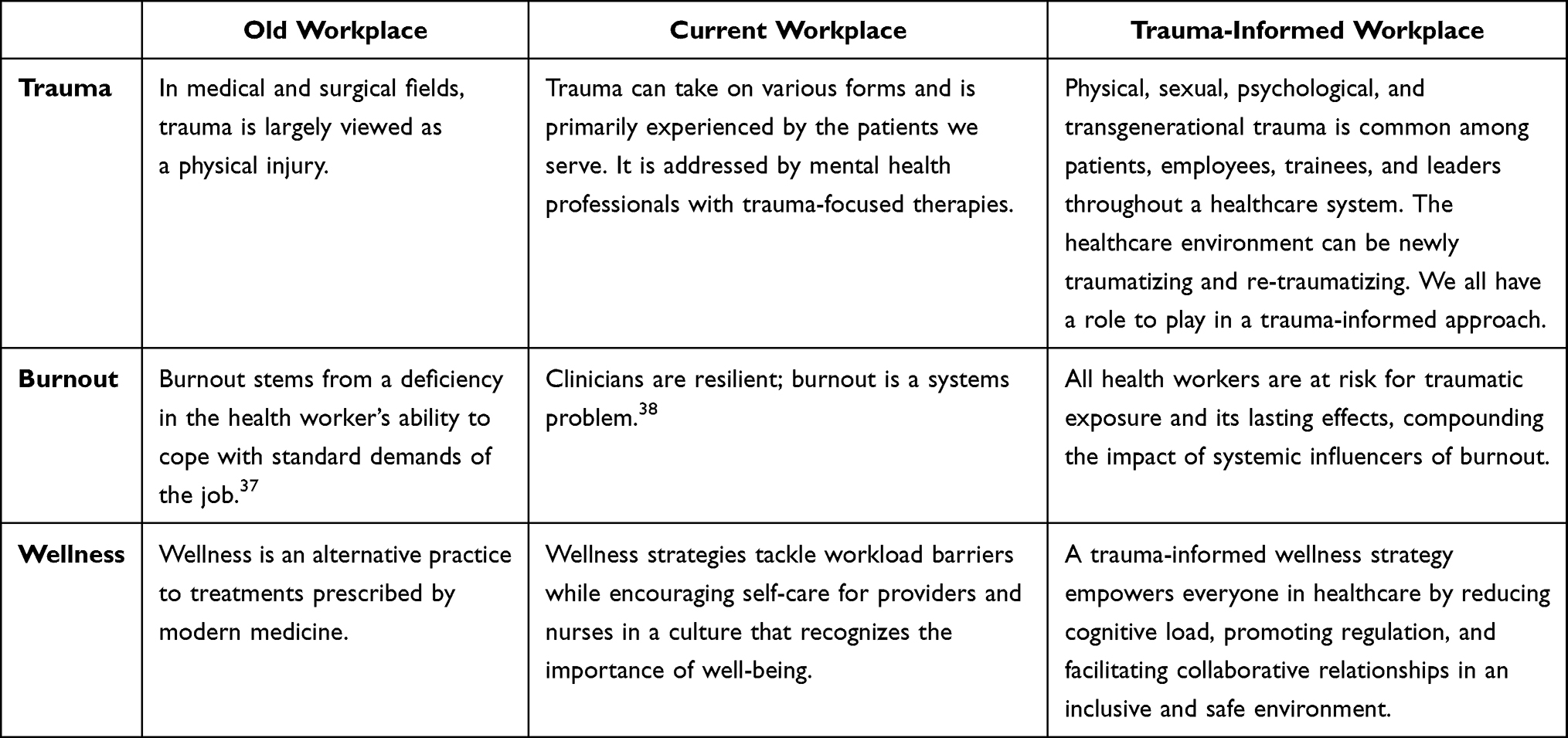 |
Table 1 Defining Views of Trauma, Burnout, and Wellness in the Healthcare Workplace Over Time |
Resist Re-Traumatization
Re-traumatization occurs when stimuli from our current environment activate feelings or reactions that resemble those associated with a prior stressor. For example, the visceral feeling of lack of control as we face a fully-booked, understaffed clinic can mimic feelings of powerlessness from past adversities, leading to a threat response that may affect us unknowingly throughout the day.
Healthcare environments are fraught with the potential for re-traumatization: invasive procedures, hierarchical power dynamics, medical racism, and the constant play between life and death. Health workers who report feeling burned out may, in fact, be grappling with new or reactivated traumatic stress. Applying, integrating, and sustaining interventions that uphold TIC principles may mitigate the risk of re-traumatization at the individual, interpersonal, and institutional levels.
Call to Action
Addressing burnout must be a top priority for healthcare leaders. Once we acknowledge the role of trauma in the burnout crisis, we can invest in trauma-informed solutions. Ultimately, patients’ experience of care is impacted by the way in which we create and sustain a healthy workplace culture. Patients, trainees, and employees alike stand to benefit from empowering processes, safe environments that nurture belonging, and collaborative relationships that foster resilience. Organizational strategies that include a trauma-informed approach to well-being, alongside efficient systems, will boost our chance at lasting success.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Murthy V. Addressing health worker burnout: the U.S. Surgeon General’s advisory on building a thriving health workforce. U.S. Department of Health and Human Services Office of the U.S. Surgeon General. Available from: https://www.hhs.gov/surgeongeneral/priorities/health-worker-burnout/index.html.
2. Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022;97(12):2248–2258. doi:10.1016/j.mayocp.2022.09.002
3. Chen Y, Wang J, Geng Y, et al. Meta-analysis of the prevalence of anxiety and depression among frontline healthcare workers during the COVID-19 pandemic. Front Public Health. 2022;10:984630. doi:10.3389/fpubh.2022.984630
4. Substance Abuse and Mental Health Services Administration (SAMHSA). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. Rockville, MD: HHS Publication No. (SMA) 14-4884; 2014.
5. Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress. 2013;26(5):537–547. doi:10.1002/jts.21848
6. Iskander M. Burnout, cognitive overload, and metacognition in medicine. Med Sci Educ. 2018;29(1):325–328. doi:10.1007/s40670-018-00654-5
7. Cabrera OA, Hoge CW, Bliese PD, Castro CA, Messer SC. Childhood adversity and combat as predictors of depression and post-traumatic stress in deployed troops. Am J Prev Med. 2007;33(2):77–82. doi:10.1016/j.amepre.2007.03.019
8. LeardMann CA, Smith B, Ryan MA. Do adverse childhood experiences increase the risk of postdeployment posttraumatic stress disorder in US marines? BMC Public Health. 2010;10:437. doi:10.1186/1471-2458-10-437
9. Gama CMF, Portugal LCL, Gonçalves RM, et al. The invisible scars of emotional abuse: a common and highly harmful form of childhood maltreatment. BMC Psychiatry. 2021;21(1):156. doi:10.1186/s12888-021-03134-0
10. Yellowlees P, Coate L, Misquitta R, Wetzel AE, Parish MB. The association between adverse childhood experiences and burnout in a regional sample of physicians. Acad Psychiatry. 2021;45(2):159–163. doi:10.1007/s40596-020-01381-z
11. McKee-Lopez G, Robbins L, Provencio-Vasquez E, Olvera H. The relationship of childhood adversity on burnout and depression among BSN students. J Prof Nurs. 2019;35(2):112–119. doi:10.1016/j.profnurs.2018.09.008
12. Thomas M, Crosby S, Vanderhaar J. Trauma-informed practices in schools across two decades: an interdisciplinary review of research. Rev Res Ed. 2019;43(1):422–452. doi:10.3102/0091732X18821123
13. James C. Towards trauma-informed legal practice: a review. Psychiatr Psychol Law. 2020;27(2):275–299. doi:10.1080/13218719.2020.1719377
14. Berman S, Brown T, Mizelle C, et al. Roadmap for trauma-informed medical education: introducing an essential competency set. Acad Med. 2023;98:e005196.
15. Manning K. We need trauma-informed workplaces. Harvard Business Review; 2022. Available from: https://hbr.org/2022/03/we-need-trauma-informed-workplaces.
16. Ravi A, Little V. Providing trauma-informed care. Am Fam Physician. 2017;95(10):655–657.
17. Levy-Carrick NC, Lewis-OʼConnor A, Rittenberg E, Manosalvas K, Stoklosa HM, Silbersweig DA. Promoting health equity through trauma-informed care: critical role for physicians in policy and program development. Fam Community Health. 2019;42(2):104–108. doi:10.1097/FCH.0000000000000214
18. Elisseou S, Adams E, Adler M. A trauma-informed approach to peer physical examination. MedEdPORTAL. 2022;18:11273. doi:10.15766/mep_2374-8265.11273
19. McLean CP, Betsworth D, Bihday C, et al. Helping the helpers: adaptation and evaluation of stress first aid for healthcare workers in the veterans health administration during the COVID-19 Pandemic. Workplace Health Saf. 2023;74:162.
20. Bloom SL, Bennington-Davis M, Farragher B, McCorkle D, Nice-Martini K, Wellbank K. Multiple opportunities for creating sanctuary. Psychiatr Q. 2003;74(2):173–190. doi:10.1023/A:1021359828022
21. Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245–258. doi:10.1016/S0749-3797(98)00017-8
22. Stork BR, Akselberg NJ, Qin Y, et al. Adverse Childhood Experiences (ACEs) and community physicians: what we’ve learned. Perm J. 2020;24(2). doi:10.7812/TPP/19.099
23. Sciolla AF, Wilkes MS, Griffin EJ. Adverse childhood experiences in medical students: implications for wellness. Acad Psychiatry. 2019;43(4):369–374. doi:10.1007/s40596-019-01047-5
24. Wurm W, Vogel K, Holl A, et al. Depression-burnout overlap in physicians. PLoS One. 2016;11(3):e0149913. doi:10.1371/journal.pone.0149913
25. Anda RF, Felitti VJ, Bremner JD, et al. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):174–186. doi:10.1007/s00406-005-0624-4
26. Van der Kolk BA. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. New York: Penguin Books; 2014.
27. Maunder RG, Peladeau N, Savage D, Lancee WJ. The prevalence of childhood adversity among healthcare workers and its relationship to adult life events, distress and impairment. Child Abuse Negl. 2010;34(2):114–123. doi:10.1016/j.chiabu.2009.04.008
28. Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195–205. doi:10.1001/jamainternmed.2016.7674
29. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516–529. doi:10.1111/joim.12752
30. Savic I. Structural changes of the brain in relation to occupational stress. Cereb Cortex. 2015;25(6):1554–1564. doi:10.1093/cercor/bht348
31. Hales T, Green S, Bissonette S, et al. Trauma-Informed Care Outcome Study. Res Soc Work Pract. 2018;29(5):104973151876661.
32. Gundacker C, Barry C, Laurent E, Sieracki R. A scoping review of trauma-informed curricula for primary care providers. Fam Med. 2021;53(10):843–856. doi:10.22454/FamMed.2021.500263
33. Hales TW, Nochajski TH. A structural regression analysis of trauma-informed climate factors, organizational commitment, and burnout among behavioral healthcare providers in a large public hospital. J Community Psychol. 2020;48(3):777–792. doi:10.1002/jcop.22292
34. Hales TW, Green SA, Bissonette S, et al. Trauma-Informed Care Outcome Study. Res Soc Work Pract. 2019;29(5):529–539. doi:10.1177/1049731518766618
35. Swensen S, Shanafelt T. Camaraderie action: cultivating community and commensality. In: Mayo Clinic Strategies to Reduce Burnout. New York: Oxford University Press; 2020:229–238.
36. Leiter MP, Maslach C. Areas of worklife: a structured approach to organizational predictors of job burnout. In: Perrewe PL, Ganster DC, editor. Research in Occupational Stress and Well Being. Vol. 3. Oxford, UK: Elsevier Science, Ltd.; 2004.
37. Panagopoulou E, Montgomery A. From burnout to resilient practice: is it a matter of the individual or the context? Med Educ. 2019;53(2):112–114. doi:10.1111/medu.13784
38. West CP, Dyrbye LN, Sinsky C, et al. Resilience and burnout among physicians and the general US working population. JAMA Netw Open. 2020;3(7):e209385. doi:10.1001/jamanetworkopen.2020.9385
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.