")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Transient Leukoerythroblastic Reaction in a Newborn with Rh-Incompatibility and Hemolysis: Case Report and Literature Review
Authors Arega G , Gashaw H, Muhammed Fedlu N, Ergete W
Received 15 July 2023
Accepted for publication 13 October 2023
Published 18 October 2023 Volume 2023:14 Pages 333—335
DOI https://doi.org/10.2147/PHMT.S430828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Gashaw Arega,1 Henock Gashaw,1 Nuru Muhammed Fedlu,1 Wondwossen Ergete2
1Department of Pediatrics and Child Health, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pathology, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Gashaw Arega, Department of Pediatrics and Child Health, School of Medicine, Addis Ababa University, P.O. Box 9080, Addis Ababa, Ethiopia, Email [email protected]
Abstract: Leukoerythroblastosis is rarely encountered in clinical practice and is characterized by the presence of leukocytosis and erythroid and myeloid blast cells in peripheral blood. The most common causes of leukoerythroblastosis in early childhood are viral infection, juvenile myelomonocytic leukemia, and osteopetrosis. To the best of our knowledge, leukoerythroblastic reactions associated with hemolysis have not been previously reported in newborns. Here, we report a 24-hour-old female term newborn diagnosed with a leukoerythroblastic reaction, severe anemia, and neonatal hyperbilirubinemia secondary to Rh incompatibility based on presentation, laboratory determination, and peripheral morphology. A high index of clinical suspicion is required to avoid life-threatening complications among health professionals in the neonatal care unit.
Keywords: newborn, Rh-incompatibility, hemolysis, leukoerythroblastic reaction
Introduction
The leukoerythroblastic reaction is characterized by the presence of immature erythroid cells and myeloid precursors (metamyelocytes, myelocytes, promyelocytes, myeloblasts, and blasts) in peripheral blood.1 The most common causes of leukoerythroblastosis in early childhood are viral infection, juvenile myelomonocytic leukemia, and osteopetrosis.2
We report an unusual case of leukoerythroblastic reaction with severe anemia and neonatal hyperbilirubinemia secondary to Rh-incompatibility in a 24-hour-old term newborn who was successfully treated with intensive phototherapy and exchange transfusion.
Case Presentation
The patient was a 24-hour-old female newborn born to a para II mother at 37+3 weeks gestational age via cesarean section for an indication of a previous cesarean scar with breech presentation, weighing 2600 g with APGAR scores of 7 and 8 at the first and fifth minutes, respectively. The mother had regular antenatal care follow-up with a B-negative (B−ve) blood group and was found to be sensitized by a positive indirect Coomb test done at five months of gestational age. The pregnancy was uneventful, and no abnormalities were detected during the prenatal follow-up. After the cesarean section, cord blood was sent, and the newborn blood group was O-positive (O+ve). The newborn was referred to the neonatal intensive care unit from the obstetric ward for evaluation by a pediatrician. Neonatal physical examination revealed an active pink newborn with no dysmorphic features. Complete blood count and bilirubin laboratory determination at 8 hours of life showed a white blood count of 185,000/mm3 and bilirubin total of 6.93 mg/dl [Bilirubin total= 6.93 mg/dl and direct bilirubin =0.14 mg/dl]. At 24 hours of life, the complete blood count laboratory determination showed a white blood cell count of 279,000/L with 30% lymphocytes and 65% neutrophils, hemoglobin- 6.5 g/dl, MCV-130 fl, and platelet count of 202,000/L. The newborn developed yellowish discoloration of the body, and repeat bilirubin determination showed a total bilirubin level of 22 mg/dl and a direct bilirubin of 1.4 mg/dl. Peripheral morphology revealed a leukoerythroblastic smear with anisopoikilocytosis, normochromic and some macrocytic red blood cells, adequate platelets, and increased white blood cells with metamyelocytes of 6%, myelocytes of 12%, promyelocytes of 3%, and myeloblasts of 1%). On average, there were 20 normoblasts per high-power field microscope with dyserythropoietic and megaloblastic features [Figure 1, Figure 2]. The results of the direct Coombs test were positive. The newborn was initially subjected to intensive phototherapy, and later, an exchange transfusion was performed as the bilirubin level increased per the Bhutani curve. The newborn was discharged after one week, with follow-up arranged at a high-risk infant clinic. The infant is now six months old and thrives well.
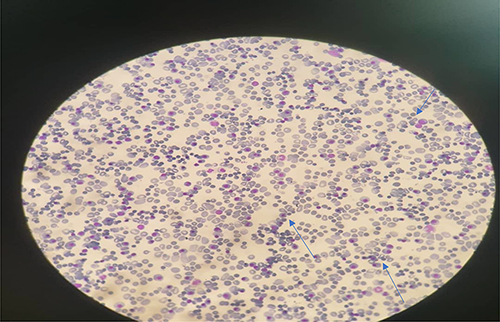 |
Figure 1 Peripheral morphology showed normoblasts and megaloblastic features. |
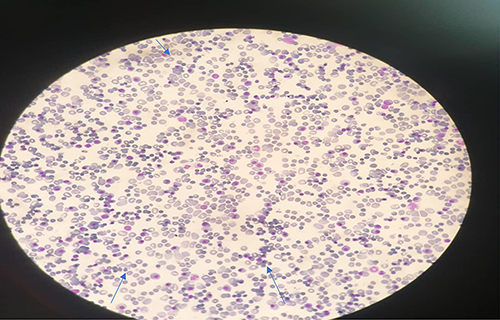 |
Figure 2 Peripheral morphology revealed normoblasts and immature white blood cell. |
Discussion
Leukoerythroblastosis is an uncommon disease in clinical practice and is characterized by the presence of leukocytosis and erythroid and myeloid blast cells in peripheral blood. Leukoerythroblastic reactions in adults are typically observed in disorders associated with bone marrow fibrosis, including myelofibrosis, other myeloproliferative disorders, and cancers with metastatic disease in the bone marrow.1–3 The most common causes of leukoerythroblastosis in early childhood are viral infections (COVID-19 and human parvovirus virus 19), juvenile myelomonocytic leukemia, and osteopetrosis.4–6
The hematological profile in our case was interpreted as severe leukocytosis and neonatal anemia. The blood group mismatch between the mother and newborn (Rh-incompatibly), rising bilirubin level, and positive direct comb test results were suggestive of hemolysis.
A peripheral blood smear suggested a leukoerythroblastic reaction with the presence of severe leukocytosis, erythroblastosis, and myeloblastosis, indicating a leukoerythroblastic smear with the presence of circulating neutrophilic precursors, nucleated red cells, and often teardrop erythrocytes. Leukoerythroblastosis in the newborn was considered to have developed in our case because of bone marrow stress caused by hemolysis secondary to Rh incompatibility. Our patient was managed with intensive phototherapy and exchange transfusion, and the complete blood count and bilirubin level were subsequently normalized.
Conclusion
We have described the case of a term newborn with transient leukoerythroblastic reaction associated with hemolysis secondary to Rh-incompatibility, evidenced by severe anemia, neonatal hyperbilirubinemia, and a positive comb’s test. Leukoerythroblastosis must be considered if a very high leukocyte count with hemolytic features is detected in the neonatal period.
Data Sharing Statement
Data supporting the findings of this case are available upon request from the corresponding author.
Ethical Clearance
Informed consent for publication was obtained from the parents and ethical clearance was obtained from the Department of Pediatrics Research and Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Anand A, Gray ES, Brown T, Clewley JP, Cohen BJ. Human parvovirus infection in pregnancy and hydrops fetalis. N Engl J Med. 1987;316(4):183–186. doi:10.1056/NEJM198701223160403
2. Ozdemir N, Akı H, Hakyemez HT, Çokuğraş FÇ, Apak H. Cokugras ¸ FÇ, Apak H. Parvovirus B19 infection mimicking juvenile myelomonocytic leukemia. Int J Infect Dis. 2010;14(suppl 3):e379–e380. doi:10.1016/j.ijid.2010.04.004
3. Tabares Calvache E, Tabares Calvache AD, Faulhaber GAM. A systematic review of the etiologic association to the leukoerythroblastic reaction. Int J Lab Hematol. 2020;42(5):495–500. doi:10.1111/ijlh.13238.
4. Duran R, Vatansever U, Acunaş B, Orhaner B, Demir M. Transient leukoerythroblastosis in a very low birth weight infant with parvovirus B19 infection. Int J Infect Dis. 2009;13(6):e473–5. doi:10.1016/j.ijid.2009.01.002.
5. Naqvi S, Awasthi NP, Das PK, Husain N. Leukoerythroblastosis - An unusual presentation of COVID-19 infection. Clin Epidemiol Glob Health. 2022;15:101026. doi:10.1016/j.cegh.2022.101026.
6. Mitra A, Dwyre DM, Schivo M, et al. Leukoerythroblastic reaction in a patient with COVID-19 infection. Am J Hematol. 2020;95(8):999–1000. doi:10.1002/ajh.25793.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.