")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Thoracotomy in Children: Review from a Low-Income Country
Authors Gebreselassie HA, Tadesse MM, Woldeselassie HG
Received 24 November 2022
Accepted for publication 9 March 2023
Published 12 March 2023 Volume 2023:14 Pages 99—106
DOI https://doi.org/10.2147/PHMT.S398368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Hana Abebe Gebreselassie,1 Mekdelawit Mesfin Tadesse,2 Hanna Getachew Woldeselassie3
1Department of Surgery, Pediatrics Surgery Unit, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Surgery, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia; 3Department of Surgery, Pediatrics Surgery Unit, Addis Ababa University, College of Health Sciences, Addis Ababa, Ethiopia
Correspondence: Hana Abebe Gebreselassie, Department of Surgery, Pediatrics Surgery Unit, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, Tel +251913766868, Email [email protected]
Background: Thoracotomy is indicated for several congenital and acquired disorders in children. It is among the surgical procedures which require a well-trained and dedicated surgical, anesthesia and critical care team which can be difficult to assemble in a low-income country setup. As the pattern and outcome of thoracotomy in children remained unreported from such setting, this study aims to shed light on this matter.
Methodology: A descriptive cross-sectional review was conducted. Children who have undergone thoracotomy for non-cardiac pathologies were included in the study. Demographic and clinical data were collected by chart review. Frequencies and percentages were used to describe categorical variables while mean, median, standard deviation and interquartile range were calculated for continuous variables.
Results: A total of 68 patients were operated on in the study period, out of which 44 (64.7%) were males. The mean ages of the children at the time of diagnosis and procedure were 4.05 ± 3.9 years and 4.14 ± 4.03 years, respectively. The most common indication for thoracotomy was pulmonary hydatid cyst (17; 25%) followed by congenital lobar emphysema (11; 16.2%). Muscle sparing posterolateral thoracotomy was the most common approach in 66 (97.1%) patients. The analgesic medications that were used in the post-operative period were paracetamol, diclofenac, ibuprofen, tramadol and morphine. Combined analgesics were administered in two-thirds of the patients while a single analgesic was used in the rest of the children. No regional blocks were administered post operatively as pediatric size catheters were not available. The morbidity and mortality rates were found to be 11.8% and 8.8%, respectively.
Conclusion: The most common indication for thoracotomy in this study was pulmonary hydatid cyst. The provision of post-thoracotomy analgesia in our institution is suboptimal as evidenced by no use of regional blocks and poor practice of administering multimodal analgesia. Thoracotomy was associated with fairly high morbidity and mortality.
Keywords: thoracotomy, children, indication, outcome, analgesia
Introduction
Thoracotomy is a surgical procedure which entails opening the chest cavity in order to address pathologies arising from the underlying structures such as the pleura, lung, mediastinum, heart, chest wall and/or the diaphragm. Although the share of thoracotomy among the other surgical procedures in children is not exactly known, based on several hospital-based reports it seems to be uncommon.1–5 Thoracotomy is among the surgical procedures which require a trained and dedicated surgical, anesthesia and critical care team especially in the pediatrics age group. This has resulted in its preferential practice in referral and tertiary care hospitals particularly in low-income countries.
Thoracotomy is indicated for several congenital and acquired disorders in children. Common congenital anomalies requiring thoracotomy include developmental disorders of the lung such as congenital lobar emphysema, congenital pulmonary airway malformation and pulmonary sequestration. Other non-pulmonary congenital anomalies include duplication cysts, esophageal atresia, diaphragmatic hernia and eventration. Acquired disorders include several infectious and non-infectious lesions such as pulmonary hydatid cyst, lung abscess, empyema, foreign body aspiration and bullae.6–8
Several standard surgical approaches can be used to access the thoracic cavity in children. These can be done via traditional open thoracotomy or thoracoscopy.9–12 The thoracoscopic approach is commonly used in high income countries with the advent of minute instruments unlike low- and middle-income countries.13,14 The traditional open thoracotomy approaches include lateral thoracotomy, posterolateral thoracotomy, anterior thoracotomy, median sternotomy and mini thoracotomy.15,16
Thoracic surgery in children can be associated with life-threatening complications such as major bleeding, hypoxia and contralateral pneumothorax. Other complications include atelectasis, post pneumonectomy syndrome, air leak, pulmonary edema, chylothorax, recurrent chest infections and chest deformity. A thorough post-operative monitoring of children after thoracotomy is critical especially in the early post-operative period in order to diagnose and manage these complications in a timely manner.17,18
One of the vital components of patient management after thoracotomy is provision of adequate analgesia as thoracotomy is a painful procedure. For instance, in a cross-sectional study from Italy it was shown that during the immediate post thoracotomy period 37.5% of children had at least one painful episode.19 Post thoracotomy pain can result in a number of deleterious respiratory complications such as atelectasis, pneumonia and hypoxia.18 Hence, optimal analgesia with frequent follow up by means of several clinical parameters and pain scoring should be a routine practice in these patients.
This study has tried to describe the pattern and outcome of non-cardiac thoracic surgeries in pediatric patients in a setup of a tertiary hospital. To our knowledge there are no published data regarding thoracotomies in children from a low-income country and there are only few similar studies done elsewhere. Hence, we believe that this study will provide important baseline information on this subject matter in this region.
Materials and Methods
This study was conducted in Tikur Anbessa Specialized Hospital which is the largest teaching hospital in Ethiopia. This hospital serves as a referral center for patients from the capital city and all over the country. The pediatrics surgery unit within this hospital serves as the major center in Ethiopia for the care of infants and children in need of surgical care.
A descriptive cross-sectional review was conducted. All patients who were admitted to the pediatrics surgical ward in the study period and have undergone thoracotomy for non-cardiac pathologies were included in the study. Cardiac surgeries were not included since the service is not available in our institution.
Ethical clearance was obtained from the IRB of the Department of Surgery of College of Health Sciences, Addis Ababa University. Getting consent from parents/guardians of the enrolled children to review the medical records was not required as there was no personal identifier that was used during data collection and entry. Moreover, a written informed consent to collect individual patient data from the chart for research purposes is always obtained from every patient admitted for surgery as a routine practice in our institution.
The list of the charts of patients who have undergone thoracotomy during the study period was obtained from the log book of the operation room. Socio-demographic and clinical data were collected. Patient data confidentiality was given due attention during data collection, entry and analysis by using assigned codes rather than real patient identifiers.
Frequencies and percentages were used to describe categorical variables while mean, median, standard deviation and interquartile range were calculated for continuous variables. These qualitative analysis methods were used since this is a purely descriptive study.
Result
Socio-Demographic Characteristics
A total of 68 children underwent thoracotomy in the study period out of which 44 (64.7%) were males. The mean age at the time of diagnosis was 4.05±3.9 years with a median of 2.5 years and interquartile range of 6.7 years. The mean age at the time of surgery was 4.14± 4.03 years while the median and the interquartile ranges were 2.6 years and 7.4 years, respectively. Two-thirds of the children were more than 18 months old at the time of initial presentation and diagnosis. The major proportion of the study population, 47 (69.1%), were residents of the capital city (Figure 1).
 |
Figure 1 Age at diagnosis and surgery of children who underwent thoracotomy. |
Clinical Profiles
The most common presenting symptom was cough (42; 61.8%) followed by respiratory distress (31; 48.5%). The mean duration of symptoms was 2.98±6.1 months while the median and the interquartile range were 1 month and 2.5 months, respectively. Among the study population, 6 (8.8%) had associated congenital anomalies: congenital heart disease (n = 2; 2.9%), macrocephaly (n = 1; 1.5%), situs inversus (n = 1; 1.5%), VACTERL association (n = 1; 1.5%) and bladder exstrophy (n = 1; 1.5%) (Table 1).
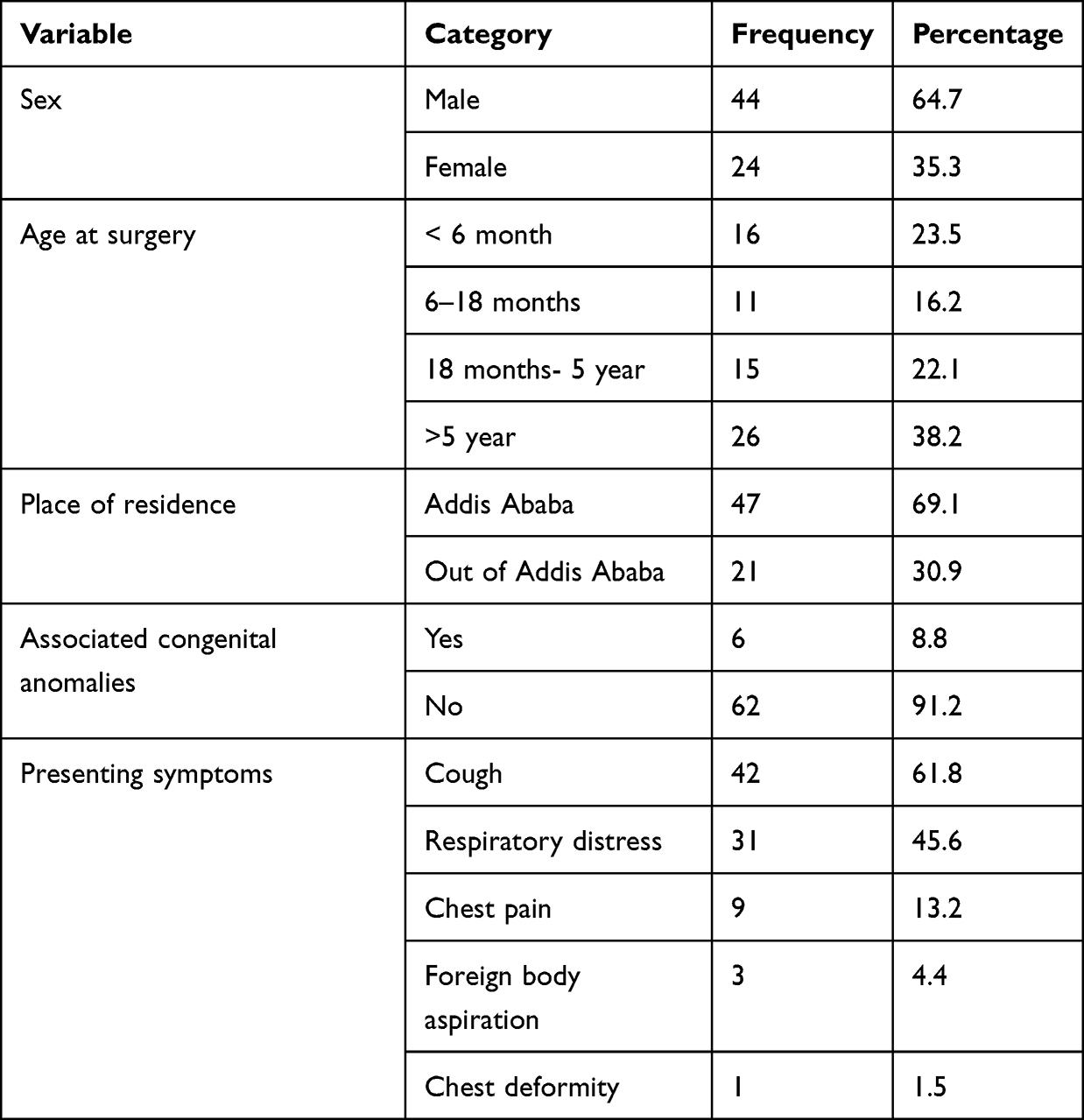 |
Table 1 Socio-Demographic and Clinical Profile of Children Who Have Undergone Thoracotomy |
Regarding the use of imaging modalities, chest radiograph was done in all patients. The other investigations done were chest CT in 49 (72.1%), ultrasound in 6 (8.8%) and chest MRI in 1 (1.4%) patients. Preoperative diagnosis was mostly settled based on imaging findings. The most common indication for thoracotomy was pulmonary hydatid cyst in 17 (25%) children followed by congenital lobar emphysema 11 (16.2%) and empyema 10 (14.8%) (Table 2).
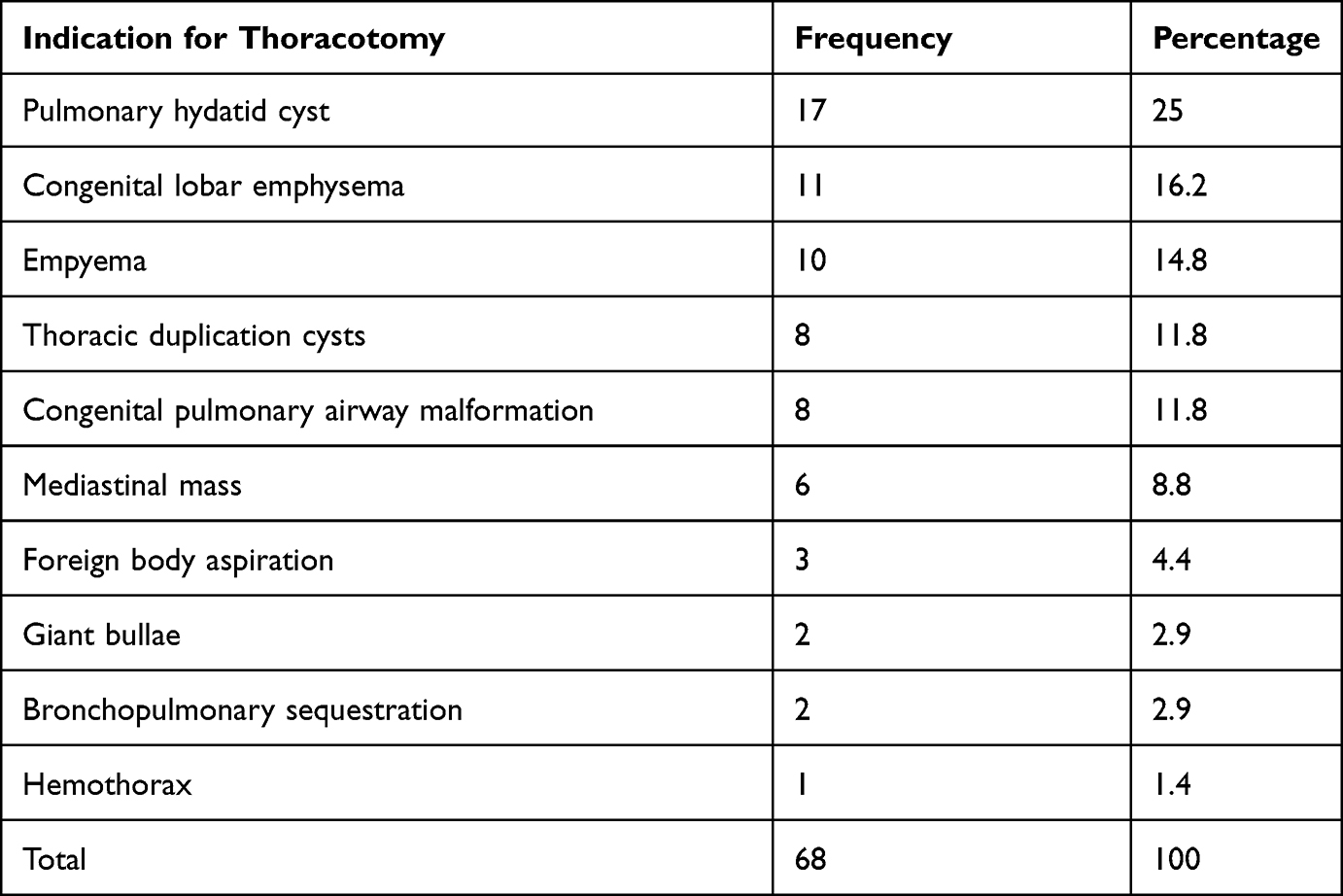 |
Table 2 Indications for Thoracotomy |
Antibiotics were started pre-operatively in 58 (85.3%) of patients. Among the 68 children, 10 (14.7%) with empyema and 1 (1.5%) with hemothorax had chest tubes inserted prior to thoracotomy. Among the operated patients, 4 (5.8%) required direct admission to the pediatric intensive care unit prior to the surgical procedure.
Posterolateral thoracotomy was the most common approach in 66 (97.1%) of patients while right side was mostly used 38 (55.9%). Muscle sparing/splitting approach was used in the great majority of the procedures. In 2 (2.9%) children, the latissimus dorsi muscle was divided after entering the chest cavity due to inadequate exposure of the surgical field. Among patients with pathologies affecting the lung parenchyma, the most affected lung lobes were left upper lobe and the left lower lobe which were affected in 10 (14.7%) patients each followed by right lower lobe (9; 13.2) and right upper lobe (8; 11.8%).
Out of the 68 patients, 67 underwent thoracotomy since one patient died on table upon induction of anesthesia before surgical incision. The most common procedure was lobectomy (17; 25.3%) followed by hydatid cystectomy (14; 20.8%) and decortication (7; 10.4%) (Table 3).
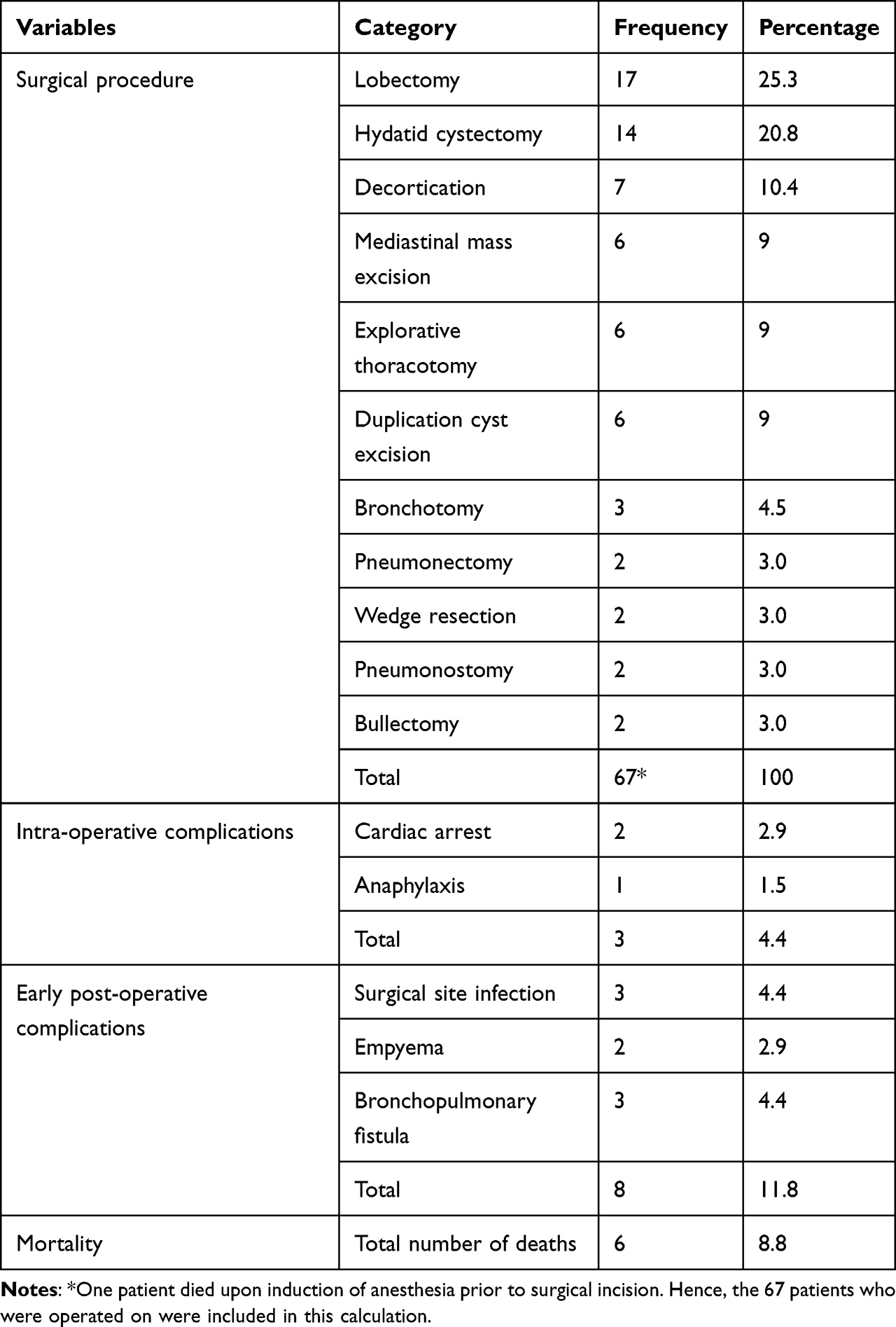 |
Table 3 Surgical Procedures and Post Thoracotomy Complications and Mortality |
The preoperative diagnosis was consistent with the intraoperative finding in 61 (91.0%) of the cases. The mean duration of operation was 1.95±1.1 hours with a median of 1.7 hours and interquartile range of 50 minutes. The mean duration of anesthesia was 2.45±1.14 hours with a median and interquartile range of 2.1 hours and 53.8 minutes respectively. Major intraoperative complications were encountered in 3 (4.4%) patients, anaphylaxis in 1 patient and cardiac arrest in 2 patients, and resulted in death in all 3 patients despite resuscitative efforts. Chest drain or tube was placed in all patients at the completion of the thoracotomy procedure.
The analgesic medications that were used in the post-operative period were paracetamol, diclofenac, ibuprofen, tramadol and morphine. The most common post-operative analgesia used was paracetamol or diclofenac suppository alone in 21 (30.9%) of patients followed by paracetamol or diclofenac suppository in combination with tramadol in 20 (29.4%) of patients. Intravenous tramadol and morphine were used in 6 (8.8%) patients each. No regional blocks were administered post-operatively as pediatric size catheters were not available.
The mean duration of post-operative antibiotics was 12.63±22.9 days with a median of 10 days and interquartile range of 5.5 days. The antibiotics used include ceftriaxone, vancomycin, ceftazidime and meropenem. Albendazole was started on the 7th post thoracotomy day for patients with pulmonary hydatid cyst. Antibiotics and anthelmintic were administered concomitantly in patients operated for pulmonary hydatid cyst if they were still on chest tube on the 7th post-thoracotomy day. Biopsy result was collected in only 19 (27.9%) patients.
Early post-operative complications were seen in 8 (11.8%) patients: 3 (4.4%) developed surgical site infection, 2 (2.9%) patients had empyema while another 3 (4.4%) developed bronchopulmonary fistula. Recurrent chest infection was noticed on further follow-up at the clinic in the post-operative period in 3 (4.4%) patients. The mean hospital stay was 24.9±14.3 days with a median of 21 days and interquartile range of 18.8 days. The overall 30-day mortality in this study was found to be 8.8%. All deaths occurred within the first post-operative month, the latest being on the 27th post thoracotomy day. The mean duration of follow-up at the clinic was 5.6±12.7 months with a median of 3 months and interquartile range of 5.5 months.
Discussion
In comparison with adults, thoracotomy is uncommon surgery in the pediatric age group as the incidence of pathologies requiring this procedure is not high. Moreover, the indications for this procedure in children are different from adults as congenital malformations take the major share in this age group.18,20
Our patients were found to be much younger when compared with similar studies from Germany and Turkey. The male preponderance seen in our study was also reflected in both of these studies with a comparable male to female ratio.18,20
The most common indication for thoracotomy in our study was pulmonary hydatid cyst. This is explained by the fact that Ethiopia is one of the countries with high prevalence of hydatid cyst. The estimated prevalence of this pathology in Ethiopia is reported to be 4.9–49.5% depending on the altitude of residence.21–23 Moreover, the lung is the most common anatomic location for pediatric hydatid cyst infection unlike adults. This is due to the high elasticity and compressibility of the lungs in children.24–26 In one retrospective review of pediatric hydatid cysts from our institution, the lung was found to be the most common site of involvement in 76.5% of the children.27 Pulmonary hydatid cyst was also the most common indication for thoracotomy in a study from Turkey in which it accounted for 35% of the procedures. In a study from Germany, however, oncologic causes contributed for 54.1% of the admissions and were found to be the most common indications for thoracotomy.18,20
Posterolateral thoracotomy, which entails division of the latissimus dorsi, trapezius and serratus anterior muscles, was considered as the standard incision for most pediatric thoracic procedures as it provides good operative exposure for most of the non-cardiac thoracic procedures. Due to concerns such as acute and chronic pain, better shoulder function and chest wall deformity, a muscle splitting/sparing approach was introduced in the 1990s.15,28 Several comparative studies have demonstrated that the later approach is associated with better short- and long-term outcome.29–31 In our study posterolateral incision with a muscle splitting approach was used in the great majority of patients.
Thoracotomy is a painful procedure which can lead to marked impairment of pulmonary function. Several modes of providing analgesia ranging from oral and intravenous medications to regional blocks have been described in children. Among these, the most effective method was found to be provision of epidural analgesia.32–35 Unfortunately, in our institution during the study period post-thoracotomy epidural analgesia was provided for adults but not for children due to lack of pediatric sized epidural catheters. The mainstay of analgesics in our patients were paracetamol, non-steroidal anti-inflammatory drugs and opioids. The most common opioid used was tramadol in combination with either of the other drugs while morphine was used in 6 (8.8%) patients. The practice of using combined analgesics with different mode of action was observed in only two-thirds of patients. These findings suggest that the provision of multimodal analgesia in children who underwent thoracotomy was substandard in our institution.
Children should be followed strictly in the perioperative period for the development of post-thoracotomy complications. Optimal analgesia and aggressive chest physiotherapy are imperative to prevent most of the respiratory complications such as atelectasis and retention of secretions.18 The incidence of surgical site infection and prolonged air leak in our study were comparable between our series and a study from Turkey even if the overall incidence of early post-operative complications was found to be lower in our study.18 The 30-day mortality in our study was comparable to a report from Germany, although they had a major share of thoracotomies done for patients with malignancy.20
To our knowledge, this study is the first of its kind to describe the experience of a tertiary hospital in a low-income country on thoracotomy in pediatrics patients. This review provides important baseline information on this subject matter. Due to the retrospective nature of this study, some important information might have been missed. Hence, a further prospective study with a better data quality is recommended to define this understudied subject better.
Abbreviations
VACTERL, vertebra, anorectal malformation, tracheoesophageal fistula, renal anomalies, limb anomalies; CT, Computed Tomography; MRI, Magnetic Resonance Imaging; IQR, Interquartile range.
Funding
No funding was received for this study.
Disclosure
The authors state that they have no conflict of interest, financial or otherwise to report for this study.
References
1. Akau KS, Danjuma S, Luka AJ, Nuhu Y, Olatunde OO, Godfrey MJ. Pattern and outcome of pediatric surgical admissions in a New Tertiary Hospital in Northwestern Nigeria. J Surg. 2017;5(5):82–85. doi:10.11648/j.js.20170505.13
2. Alagoa PJ, Gbobo I. Pattern of pediatric surgical admissions in a Tertiary Hospital in a Semi – urban Community in the Niger Delta: a three- year review. Int J Trop Dis Health. 2014;4(1):45–51. doi:10.9734/IJTDH/2014/5869
3. Ketema T, Abeya SG, Abdela K, Chaka TE. Pediatric surgical admissions and their outcomes at Adama Hospital Medical College: a facility based cross sectional study. Am J Pediatr. 2017;3(4):23–27. doi:10.11648/j.ajp.20170304.12
4. Abahuje E, Uyisabye I, Ssebuufu R. Epidemiology of pediatric surgery in Rwanda: a one-year review. Rwanda Med J. 2016;73(1):11–16.
5. Somme S, Bronsert M, Morrato E, Ziegler M. Frequency and variety of inpatient pediatric surgical procedures in the United States. Pediatrics. 2013;132(6):1466–1472. doi:10.1542/peds.2013-1243
6. Divya G, Kundal VK, Debnath PR, et al. Musculoskeletal and esthetic complications after neonatal thoracotomy Revisited. J Indian Assoc Pediatr Surg. 2022;27(3):293–306. doi:10.4103/jiaps.JIAPS_19_21
7. Mokdad AA, Gourlay DM, Oldham KT. Congenital malformations of the lung. In: Pediatric Surgery: Diagnosis and Management. Springer International Publishing, Cham; 2023:447–462.
8. Kunisaki SM, Leys CM. Surgical pulmonary and pleural diseases in children lung malformations, empyema, and spontaneous pneumothorax. Adv Pediatr. 2020;67:145–169. doi:10.1016/j.yapd.2020.03.006
9. Casal-Beloy I, Míguez Fortes L, Gómez Tellado MA, González-Rivas D. Thinking uniportal in pediatric thoracic surgery. Pediatr Med. 2019;2:13. doi:10.21037/pm.2019.04.03
10. Bawazir OA. Thoracoscopy in pediatrics: surgical perspectives. Ann Thorac Med. 2019;14(4):239–247. PMID: 31620207; PMCID: PMC6784445. doi:10.4103/atm.ATM_114_19
11. Xie J, Wu Y, Wu C. Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis. Ther Adv Respir Dis. 2020;14. doi:10.1177/1753466620980267
12. Gustaf D, Björn A, Svensso Jan F. Thoracoscopy or thoracotomy for esophageal atresia: a systematic review and meta-analysis. Ann Surg. 2021;274(6):945–953. doi:10.1097/SLA.0000000000004239
13. Petrosyan M, Nadler EP, Zilbert NR, Sidler D. Minimal access surgery in pediatric patients. In: Ameh EA, Bickler SW, Lakhoo K, Nwomeh BC, Poenaru D, editors. Pediatric Surgery. Springer, Cham; 2019. doi:10.1007/978-3-030-41724-6_124
14. Olusoji OO, Ogunleye EO, Olugbemi AJ, Ojo OO, Sanni SB. Early experience with video-assisted thoracoscopic surgery in Nigeria. Ann Afr Surg. 2021;18(4):215–219. doi:10.4314/aas.v18i4.5
15. Bertolaccini L, Pardolesi A. Approaches to the thoracic cavities. Pediatr Med. 2019;2:9. doi:10.21037/pm
16. Chang B, Tucker WD, Burns B. Thoracotomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557600/.
17. Hall MA, Raiten JM. Anesthetic management of post- thoracotomy complications. In: Slinger P, editor. Principles and Practice of Anesthesia for Thoracic Surgery. Springer, Cham; 2019. doi:10.1007/978-3-030-00859-8_53
18. Findik G, Gezer S, Sirmali M, et al. Thoracotomies in children. Pediatr Surg Int. 2008;24:721–725. doi:10.1007/s00383-008-2144-6
19. Marchetti G, Vittori A, Ferrari F, et al. Incidence of acute and chronic post-thoracotomy pain in pediatric patients. Children. 2021;8(8):642. doi:10.3390/children8080642
20. Kanngiesser P, Liewald F, Halter G, Sunder-Plassmann L. Thoracic surgery in children. Eur J Cardio Thorac Surg. 2005;28:50–55. doi:10.1016/j.ejcts.2005.03.010
21. Gessese AT. Review on epidemiology and public health significance of hydatidosis. Vet Med Int. 2020;8. doi:10.1155/2020/8859116
22. Garoma A. Epidemiology of hydatidosis in Ethiopia. J Nurs Healthcare. 2022;7(3):1–6.
23. Shumuye NA, Ohiolei JA, Gebremedhin MB, et al. A systematic review and meta-analysis on prevalence and distribution of Taenia and Echinococcus infections in Ethiopia. Parasites Vectors. 2021;14:447. doi:10.1186/s13071-021-04925-w
24. Chebil N, Sahli S, Fitouri F, et al. Pulmonary hydatidosis in children: a different pattern from adults? Ann Afr Surg. 2022;19(1):23–27. doi:10.4314/aas.v19i1.5
25. Aydin Y, Ulas AB, Ahmed AG, Eroglu A. Pulmonary hydatid cyst in children and adults: diagnosis and management. Eurasian J Med. 2022;54(1):133–144. doi:10.5152/eurasianjmed.2022.22289
26. Delgado AL, Loko EM, Dhaffala A. Lung hydatid cyst in children. J Pharm Pharmacol. 2019;7:32–35.
27. Alemayehu T, Abebe W. Cystic echinococcosis in children: a 5 year retrospective Analysis at Tikur Anbessa specialized teaching Hospital, Addis Ababa, Ethiopia. Ethiop J Pediatr Child Health. 2016;12(1):1–8.
28. Rothenberg SS, Pokorny WJ. Experience with a total muscle-sparing approach for thoracotomies in neonates, infants, and children. J Pediatr Surg. 1992;27(8):1157–1160. doi:10.1016/0022-3468(92)90579-V
29. Safa N, Wei S, Saran N, Guadagno E, Laberge J-M, Emil S. Musculoskeletal deformities after thoracic surgery in children: an observational long-term follow-up study. J Pediatr Surg. 2020;56(1):136–141. doi:10.1016/j.jpedsurg.2020.09.024
30. Gupta R, Mathur P, Bhandari A. Muscle sparing skin crease incision posterolateral thoracotomies in pediatric patients: our experience. J Indian Assoc Pediatr Surg. 2022;27:309–316. doi:10.4103/jiaps.JIAPS_43_21
31. Kaseda K. Minimally invasive open surgery approach with muscle-sparing thoracotomy. J Transl Sci. 2019;5:1.
32. Tomaszek L, Fenikowski D, Komotajtys H, Gawron D. Ropivacaine/fentanyl vs. bupivacaine/fentanyl for pain control in children after thoracic surgery: a randomized study. Pain Manag Nurs. 2019;20(4):390–397. doi:10.1016/j.pmn.2019.02.007
33. Murray-Torres TM, Winch PD, Naguib AN, Tobias JD. Anesthesia for thoracic surgery in infants and children. Saudi J Anaesth. 2021;15:283–299. doi:10.4103/sja.SJA_350_20
34. Tomaszek L, Tomalak W, Gajdosz R, Buchwald J. Intermittent thoracic epidural administration of bupivacaine-morphine versus intravenous infusion of morphine after thoracic surgery in children and adolescents. Anestezjologia i Ratownictwo. 2015;9:260–268.
35. Tomaszek L, Fenikowski D, Gawron D, Komotajtys H. Comparative efficacy of continuous infusion of bupivacaine/fentanyl and ropivacaine/fentanyl for paediatric pain control after the Ravitch procedure and thoracotomy: a prospective randomized study. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2019;163(4):366–373. doi:10.5507/bp.2018.072
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.