")
Back to Journals » Psoriasis: Targets and Therapy » Volume 13
Therapeutic Management of a Case of Severe Psoriasis Coexistent with Bullous Pemphigoid in the Elderly
Authors Di Lernia V , Peccerillo F, Ficarelli E
Received 3 May 2023
Accepted for publication 18 August 2023
Published 22 August 2023 Volume 2023:13 Pages 27—31
DOI https://doi.org/10.2147/PTT.S417427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Vito Di Lernia, Francesca Peccerillo, Elena Ficarelli
Dermatology Unit, Azienda Unità Sanitaria Locale- IRCCS di Reggio Emilia, Reggio Emilia, Italy
Correspondence: Vito Di Lernia, Dermatology Unit, Arcispedale Santa Maria Nuova, Azienda USL-IRCCS di Reggio Emilia, Viale Risorgimento 80, Reggio Emilia, 42123, Italy, Tel +39 522 296873, Email [email protected]
Abstract: A standardised therapeutic approach to coexistent psoriasis and bullous pemphigoid is lacking, although psoriasis is associated with an increased risk of developing bullous pemphigoid. Here, we report an elderly psoriatic patient who developed a refractory bullous pemphigoid and experienced clearance of both diseases following treatment with dymethylfumarate. Due to lymphopenia, this treatment was stopped and the patient was administered risankizumab without relapses. Dymethylfumarate may be able to inhibit the recruitment of neutrophils and monocytes into the skin. Therefore, thanks to pleiotropic effects, dymethylfumarate could be an effective treatment in psoriatic patients who develop bullous pemphigoid.
Keywords: psoriasis, bullous pemphigoid, elderly, treatment, latent tbc
Psoriasis is associated with an increased risk of developing bullous pemphigoid (BP).1,2 Psoriasis usually precedes the diagnosis of BP. Patients with coexisting diseases are younger than patients with BP isolated and show more frequent involvement in the oral cavity. Chronic psoriatic inflammation has been hypothesized to cause pathological changes to the basement membrane zone with consequent early occurrence of antigenicity.3 A relevant association between psoriasis and the rare form of anti-laminin γ1 pemphigoid has also been reported.2
Managing BP in a patient with severe psoriasis may be puzzling due to the possible incompatibility of their standard treatments. Conventional and biologic antipsoriatic treatments may be ineffective in treating BP. In addition, rare cases of BP have been induced by anti-psoriatic treatments, such as TNF-alpha blockers.4 Finally, the use of combined immunosuppressive regimens may be hazardous in elderly patients.
Dimethylfumarate (DMF) is an oral, immunomodulatory drug, which was approved for use in adult patients with moderate-to-severe psoriasis. It is not included in the therapeutic ladder of BP.5 In fact, it is under evaluation by ERA-Net for Research Programmes on Rare Diseases in a prospective, controlled trial in patients with BP as an adjuvant treatment in addition to corticosteroids.
Here, we report an elderly psoriatic patient who developed a refractory BP and experienced clearance of both diseases following treatment with DMF.
An 83-year-old male with an established diagnosis of psoriasis from 20 years before was referred to our clinic with a 3‐month duration of pruritus followed by eruption of pruritic, erythematous and urticarial patches associated with polycyclic lesions on his limbs and trunk. His psoriasis, which had been treated in the past with topical corticosteroids and narrow band ultraviolet B phototherapy, began to quickly worsen in the meantime. Psoriasis Area Severity Index (PASI) was 12. He also had insulin‐dependent diabetes mellitus and hypertension. Current medications included metformin, atenolol and chlorthalidone for many years. The patient was diagnosed with BP with typical histology, positive direct and indirect immunofluorescence findings with Bullous Pemphigoid Disease Area Index (BPDAI) 66. Oral prednisone, 25 mg/day was started. Due to a persistent corticosteroid-induced hyperglycemia, prednisone doses were gradually tapered until a 5 mg/day maintenance dose. While BP improved rapidly with BPDAI 16, psoriasis worsened (Figures 1 and Figure 2). Methotrexate was initiated at 15 mg/week (0.20 mg/kg), but BPDAI increased to 30. Due to ineffectiveness in both diseases, methotrexate was stopped after 12 weeks of therapy. Apremilast was then introduced and discontinued after 3 months due to inefficacy. In order to initiate a biological antipsoriatic therapy, the patient was screened for the presence of tuberculosis, hepatitis B, C and HIV. QuantiFERON-TB Gold resulted positive. The patient refused isoniazid therapy. DMF was then started at a dose of 30 mg/day for 7 days and gradually up-titrated over 8 weeks to a maximum of 150 mg/day. A maintenance dose of prednisone 5 mg on a day was also administered. Within 12 weeks of treatment with DMF 150 mg/day, marked improvement of both psoriasis and BP was observed and pruritus resolved. Complete remission of BP (BPDAI 0) and psoriasis (PASI 0) was finally achieved 6 months from treatment start. Prednisone was then tapered to 5 mg every 2 days without side effects. Over the following months, there was a persistent clinical remission of psoriasis and BP. Due to a progressive lymphopenia with a total lymphocyte count of less than 300/µL, DMF was discontinued after 15 months. The patient experienced relapse of his psoriasis, while clinical remission of BP was observed. Psoriasis was then treated with risankizumab subcutaneously, at a dose of 150 mg at week 0, week 4, and then 12-weekly thereafter, without tuberculosis prophylaxis. At his most recent follow-up visit, 12 months after the initiation of risankizumab therapy, no relapse of both diseases was seen (Figures 3 and Figure 4).
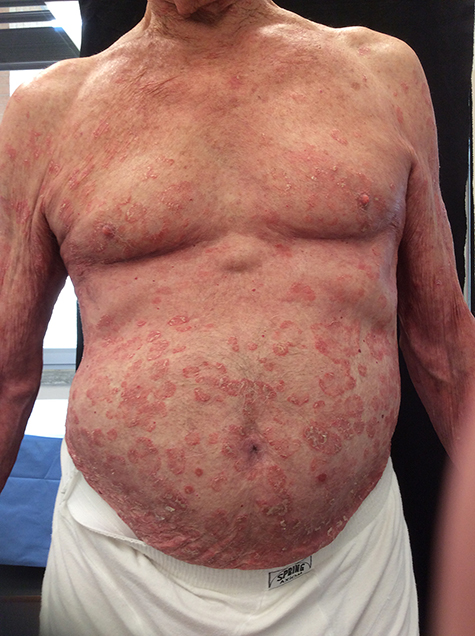 |
Figure 1 Psoriasis worsened (trunk). |
 |
Figure 2 Psoriasis worsened (lower limbs). |
 |
Figure 3 Clinical remission of both psoriatic e PB lesions on the trunk after DMF therapy. |
 |
Figure 4 Clinical remission on lower limbs. |
Autoimmune blistering diseases of the skin may be observed in patients with psoriasis, BP being the most frequently reported. There is no standardised therapeutic approach to coexistent psoriasis and BP. Corticosteroids are the mainstay of treatment for BP. However, their use is limited in diabetic patients due to the risk of acute hyperglycemic complications, particularly in elderly patients. Recently, a successful treatment with dupilumab, a fully human monoclonal antibody targeting the IL-4 and IL-13 signaling pathways, was reported.6 However, cases of dupilumab-induced psoriasis are also described. A potential functional role of the proinflammatory cytokine IL17A has been shown leading to IL17A inhibition as a promising therapeutic strategy.7 Therefore, emerging, novel targeted therapeutic approaches in BP are being awaited with great interest. DMF was able to control both psoriasis and BP in our patient. However, treatment was discontinued due to grade 3 lymphopenia, which is a possible adverse effect of DMF,8 particularly among older patients. Also, Bilgic-Temel et al reported clearance of BP in a patient with multiple sclerosis following treatment with DMF.9 At the cellular level, DMF could act in ABDs through inhibition of neutrophil and monocyte recruitment into the skin.10–12 Considering its pleiotropic effects, DMF could be an effective treatment in psoriatic patients who develop BP. Additional observations are needed to confirm if DMF may be considered a possible therapeutic option in the clinical scenario of BP associated with psoriasis.
Ethics and Consent
Institutional approval was not required to publish the case details. The patient reportedly gave written consent to the Authors for the publication of his clinical history and photographs.
Acknowledgments
Honorariums, grants, or other forms of payment were not given to any of the authors to produce the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hofmann SC, Juratli HA, Eming R. Bullous autoimmune dermatoses. J Dtsch Dermatol Ges. 2018;16:1339–1358.
2. Ohata C, Ishii N, Koga H, et al. Coexistence of autoimmune bullous diseases (AIBDs) and psoriasis: a series of 145 cases. J Am Acad Dermatol. 2015;73:50–55. doi:10.1016/j.jaad.2015.03.016
3. Kridin K, Zelber-Sagi S, Comaneshter D, Cohen AD. Association between pemphigus and psoriasis: a population-based large-scale study. J Am Acad Dermatol. 2017;77:1174–1175. doi:10.1016/j.jaad.2017.07.007
4. Bordignon M, Belloni-Fortina A, Pigozzi B, et al. Bullous pemphigoid during long-term TNF-alpha blocker therapy. Dermatology. 2009;219:357–358. doi:10.1159/000243805
5. Feliciani C, Joly P, Jonkman MF, et al. Management of bullous pemphigoid: the European Dermatology Forum consensus in collaboration with the European Academy of Dermatology and Venereology. Br J Dermatol. 2015;172:867–877. doi:10.1111/bjd.13717
6. Liu JH, Gao Q, Ma WY, Cheng ZL, Luo NN, Hao PS. Successful treatment of psoriasis combined with bullous pemphigoid with dupilumab: a case report. Clin Cosmet Investig Dermatol. 2023;16:1583–1587. doi:10.2147/CCID.S415019
7. Drenovska K, Valeva E, Shahid M, Vassileva S. Case Report: coexistence of bullous pemphigoid and psoriasis: therapeutic challenge and IL17A-targeted parallel treatment strategy. Front Med. 2023;10:1148660. doi:10.3389/fmed.2023.1148660
8. van Hezik DFC, Bovenschen HJ. Association of lymphopenia and eosinophilia with dimethylfumarate treatment efficacy and tolerability in psoriasis: a retrospective study. J Dermatolog Treat. 2020;31(4):378–381. doi:10.1080/09546634.2019.1605135
9. Bilgic-Temel A, Das S, Murrell DF. Successful management of bullous pemphigoid with dimethyl fumarate therapy: a case report. Int J Womens Dermatol. 2019;5:179–180. doi:10.1016/j.ijwd.2019.02.001
10. Wannick M, Assmann JC, Vielhauer JF, et al. The immunometabolomic interface receptor hydroxycarboxylic acid receptor 2 mediates the therapeutic effects of dimethyl fumarate in autoantibody-induced skin inflammation. Front Immunol. 2018;9:1890. doi:10.3389/fimmu.2018.01890
11. Müller S, Behnen M, Bieber K, et al. Dimethylfumarate impairs neutrophil functions. J Invest Dermatol. 2016;136:117–126. doi:10.1038/JID.2015.361
12. Brück J, Dringen R, Amasuno A, et al. A review of the mechanisms of action of dimethylfumarate in the treatment of psoriasis. Exp Dermatol. 2018;27(6):611–624. doi:10.1111/exd.13548
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.