")
Back to Journals » Chronic Wound Care Management and Research » Volume 3
The role of resilience in the recovery of the burn-injured patient: an integrative review
Authors Kornhaber R , Bridgman H, McLean L, Vandervord J
Received 7 February 2016
Accepted for publication 22 March 2016
Published 27 May 2016 Volume 2016:3 Pages 41—50
DOI https://doi.org/10.2147/CWCMR.S94618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
R Kornhaber,1 H Bridgman,2 L McLean,3–6 J Vandervord7
1School of Health Sciences, Faculty of Health, University of Tasmania, Hobart, TAS, 2Centre for Rural Health, School of Health Sciences, Faculty of Health, University of Tasmania, Hobart, TAS, 3Brain and Mind Centre, 4Westmead Psychotherapy Program, Discipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, NSW, 5Sydney West and Greater Southern Psychiatry Training Network, Cumberland Hospital, Western Sydney Local Health District, Sydney, NSW, 6Consultation-Liaison Psychiatry, Royal North Shore Hospital, Sydney, NSW, 7Severe Burns Injury Unit, Royal North Shore Hospital, St Leonards, NSW, Australia
Abstract: Severe burn injuries are catastrophic life events resulting in significant physical and psychological effects. With long periods of hospitalization and rehabilitation, burn survivors encounter many issues, including an altered body image and loss of function and independence that subsequently influence quality of life and the family unit. Consequently, resilience has been identified as a fundamental concept that facilitates the adaptability required to navigate the lengthy and complex recovery process. However, over time, the notion of resilience has shifted from a static, innate trait to a fluid and multidimensional concept. Here, we review the evidence surrounding the role of resilience in the recovery of burn injury. This integrative review was based on a systematic search of five electronic databases. Of the 89 articles identified, ten primary research papers met the inclusion criteria. Three key themes were identified encompassing relational strengths, positive coping, and the resistance to trauma symptoms that are fundamental constructs associated with developing and sustaining resilience that resonate with the broader literature on burn recovery. However, limited evidence is currently available within the burns context. While resilience appears to be a vital component influencing the recovery from burns trauma, it still remains a broad construct within the burns framework. Regular assessment of resilience in burn-injured patients is recommended in clinical practice in addition to longitudinal and intervention studies to best inform patient care.
Keywords: resilience, burn injury, rehabilitation, optimism, tenacity, review
Introduction
Burn injuries are often associated with catastrophic life events that have profound effects both of a physical and psychological nature.1 Enduring long periods of hospitalization and rehabilitation, burn survivors may encounter an altered body image and loss of function and independence that subsequently influences their quality of life.2 Acceptance of an abrupt injury, like a burn, remains challenging for the survivor and their family, with the potential to create a spiral of trauma3 if not mitigated. Subsequently, promoting the benefits of resiliency has the capacity to inform strategies in the development of resilient behaviors among burn survivors.
Resilience pertaining to loss and trauma encompasses the capacity, for those exposed to a trauma event, to maintain relative stability and a level of psychological and physical functioning.4 Therefore, resilience is the capacity to construct a “psychosocial comeback in adversity”.5 The notion of a resilient individual includes the characteristics of a positive outlook, flexibility, adaptive coping skills, and the ability to maintain supportive social networks enabling one to maintain their physical and psychosocial well-being.6 Tools such as the Connor-Davidson Resilience Scale (CD-RISC) are a means to distinguish between those with greater and lesser resilience. The CD-RISC comprises the three dimensions of tenacity, optimism, and self-improvement, demonstrating “that resilience is modifiable and can improve with treatment, with greater improvement corresponding to higher levels of global improvement”.7
It is well reported that the catastrophic nature of a burn injury can lead to long-term rehabilitative needs, requiring both the characteristics of tenacity and endurance. Seminal authors such as Holaday et al8,9 and Williams et al10 who situate resilience within the burns literature have made significant contributions in both the pediatric and adult population. However, the role of resilience has been under reported within the context of burns literature. Furthermore, to the authors’ knowledge, no review has been conducted to investigate the role of resilience within the arena of burn care and rehabilitation. Therefore, this review aimed to understand the role of resilience in those rehabilitating from a burn injury across the life span.
Methods
Review process
Methodologically, this research study employed an integrative review approach. Integrative reviews have been reported within the literature to be a methodologically sound and rigorous process.11 Integrative reviews aim to review, analyze, and synthesize literature situated within a particular area, incorporating both experimental and nonexperimental research. Integrative reviews have the capacity to generate innovative constructs, viewpoints, ideas, and the potential to build knowledge.12,13 This allows for a broader understanding of a phenomenon compared to a systematic review and meta-analysis that remains centered on an exacting synthesis of all research related to one specific question, primarily focused on high-level experimental studies.14 Furthermore, systematic reviews and meta-analyses apply explicit scientific principles that are aimed at reducing bias.15,16 Subsequently, the guiding framework that underpins this review is based on Souza et al’s14 six stages of the integrative review process (Table 1).
 | Table 1 Six stages of integrative review process Notes: Data from Souza et al.14 |
Literature search strategy
A systematic and rigorous search was conducted across five electronic health care databases: PubMed, EMBASE, CINAHL, PsychINFO, and Scopus in December 2015. The databases utilized affirmed a comprehensive and multidisciplinary breadth of research, encompassing literature across the spectrum of health care. Boolean connectors AND, OR, and NOT were used to combine search terms burn*, resilien*, and hardiness. The references of potential papers retrieved were examined to identify any additional papers not captured through the initial search strategy.
Inclusion and exclusion criteria
The search criteria for this integrative review incorporated peer-reviewed primary research published in English that explored the role of resilience in those rehabilitating from a burn injury across the life span continuum. No parameters concerning year of publication were imposed so as to capture the depth and breadth of data. Papers that focused on health care personnel were excluded as they did not focus on the burn survivor. Reviews, conference proceedings, theses, editorials, and secondary sources were also excluded.
Data evaluation
After duplicates were removed, the search strategy identified 89 prospective papers (Figure 1). RK and HB identified 31 potential papers through assessment of title and abstracts. Based on the inclusion/exclusion criteria, all four authors independently reviewed the 31 papers, and any differences were resolved by discussion. Eighteen papers were subsequently eliminated. In addition, upon further in-depth review and analysis, a further three papers were excluded as they did not meet the inclusion criteria, leaving ten papers for inclusion.
 | Figure 1 Decision trail of included studies. |
Data extraction and synthesis
A total of ten papers were systematically summarized and synthesized to identify key themes and relationships. Findings from each study were analyzed and then categorized to form significant themes. Implementing thematic analysis allows for the identification of recurrent relationships across the data to achieve higher order groups.11 Data extracted included author(s), year of publication, country of origin, design, purpose of study, sample and study population, data collection and analysis, and significant findings and outcomes (Table 2). The data from each of the studies were extracted and tabulated by RK and HB. LM checked and assessed the pooled results. In keeping with the integrative review methodology, findings were integrated and synthesized without assessing methodological rigor. This allows the researchers to capture the scope of the presented data.
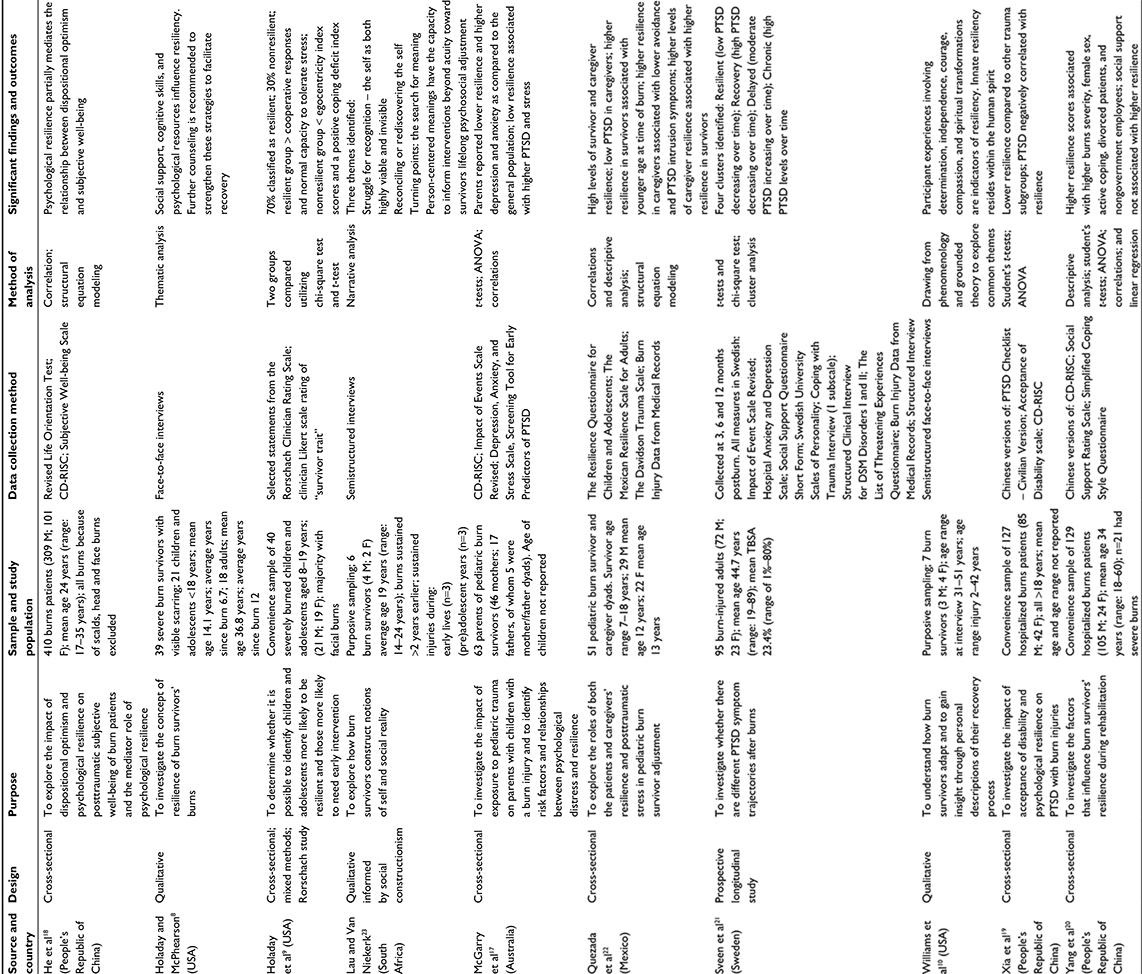 | Table 2 Summary of included studies Abbreviation: ANOVA, analysis of variance; CD-RISC, Connor–Davidson Resilience Scale; F, female; M, male; PTSD, posttraumatic stress disorder; TBSA, total burn surface area; DSM, Diagnostic and Statistical Manual of Mental Disorders. |
Results
Characteristics of included papers
Of the ten included studies, nine comprised 904 burn survivors and one included 63 parents of pediatric burn survivors.17 The studies encompassed populations ranging from pediatric to adolescent and adults. Studies were conducted across six countries, including Australia,17 the People’s Republic China,18–20 Sweden,21 Mexico,22 South Africa,23 and the USA.8–10 Three studies employed qualitative methods using narrative/thematic analysis; one used a mixed methods approach; and six studies used quantitative methods, of which five were cross-sectional and one was a longitudinal in design. The CD-RISC7 was used in four studies17,18–20 to distinguish between those with greater and lesser resilience. Subsequently, the ten included studies were synthesized, and their findings were categorized into three themes: relational strengths, positive coping, and resistance to trauma symptoms. Table 3 depicts a matrix that maps the themes to the source articles.
 | Table 3 Concept matrix mapping themes to source articles |
Relational strengths
The relational strength theme refers to the transformational capacity to restore a positive relationship with the self, post-burns injury and to foster positive social connections with others. Both of these aspects contribute to increased resilience in burn survivors and their caregivers. This theme emerged from seven of the ten included studies.
Lau and Van Niekerk,23 Williams et al,10 and Holaday and McPhearson8 identified themes related to the process of restoring a positive relationship with the self. Lau and Van Niekerk23 described burn survivors struggling to gain recognition of the contrast between the inner self and outer disfigurement in both a personal and social context. For very young survivors, this tension did not arise until confronted with responses from peers (ie, at school),23 whereas for adult survivors, this tension arose immediately.
Survivors experienced a range of emotions in response to their injury.10 For some survivors, their emotional response became self-defining and part of their identity:
Whatever took you through this – it’s yours. If you saw angels […] that’s beautiful. That’s your thing. But anger was mine.10
Acceptance played a large role in personal transformation. Lau and Van Niekerk23 described the process of self-acceptance as occurring with the recognition that despite significant changes in the outer self, the inner self remained more permanent and stable:
When I was little, I wanted the scars to go away, but now I don’t care about them anymore. They’re part of me.8
As well as acknowledging the losses, Williams et al10 described survivors as having the capacity to reframe their adverse experience as important for constructing new personal meaning. Participants described “unexpected gains” such as insight, self-esteem, gratitude, and identity:
I was pretty much dependent you know, (on my looks) […]Maybe (my injury) was the way of telling me, there was more to me.10
Healthy positive self-confidence was significantly associated with higher resilience in pediatric survivors.9 Acceptance of self appeared to impact positively on external social connections and encouraged positive social responses that affirmed the sense of self and promoted further engagement:
I used to ignore them […]. But now when I look down, they [say], “Eh Buhle, don’t look down man, what’s up?” […], I wish I could communicate with this person, and then we talk, we talk, we talk.23
Acceptance of self also fostered compassion and understanding of others’ negative reactions:
I learned that I can’t be responsible for another person’s lack of understanding, so I don’t let it bother me.8
The value of social support was identified across the majority of studies. Sveen et al21 found that survivors in the “resilient” trajectory of recovery (low trauma symptoms and high resilience) and in the “delayed” trajectory (mild trauma symptoms increasing to moderate trauma symptoms) had higher levels of social support as compared with those in the “chronic” trajectory (sustained high trauma symptoms and low resilience). Beyond merely the presence of social support, Holaday et al9 found when comparing resilient versus nonresilient pediatric burn survivors, resilient survivors displayed a higher level of “cooperative movement response”, ie, being socially gregarious and having a higher expectation of relationships to be mutually supportive and harmonious. The resilience of caregivers of pediatric burn survivors was highlighted as important to pediatric burn recovery by Quezeda et al,22 who found an indirect relationship with resilience in female caregivers, predicting symptoms of intrusion via avoidance and subsequently influencing the quality of connection with their child.
Williams et al10 reported that the quality of social relationships was associated with losses and gains, and was a way of adapting and coping with change. Importantly, Holaday and McPhearson8 highlighted that preexisting, long-term community relationships were valuable and positive to adult burn survivors’ well-being. For pediatric survivors, school social support that ameliorated stigma was vital, as well as a long-term relationship with at least one person outside their immediate family that treated them with unconditional positive regard.8 Social interactions were shown as a way of assisting survivors to reframe the meaning or purpose interpreted from their injury experiences.23 Associating with other burn survivors was also helpful for increasing acceptance and normalizing the burn experience.23
The quality of relationships identified by study participants was found to vary from “hurtful and difficult” through to “helpful and uplifting”10 and either empowering or disempowering.18 In contrast to the majority of included papers however, Yang et al20 found no significant correlation with social support and resilience; social support was instead correlated with optimism.
Positive coping
The theme of positive coping encompasses the components of active, nonavoidant coping approaches, optimism, personal choice, and perceived control. Of ten studies, seven identified positive coping strategies as promoting resilience. Avoidant coping was negatively correlated with resilience and associated with personality traits of embitterment and somatic trait anxiety, and substance use.21
Yang et al20 found a positive correlation between high coping scores on the Simplified Coping Style Questionnaire and high resilience scores as measured by the CD-RISC. Positive coping was significantly related to overall resilience and with each of the resilience dimensions of tenacity, strength, and optimism. He et al18 also found that dispositional optimism, defined as the capacity to recover from frustration, directly and significantly increased subjective well-being in adult burn survivors. Furthermore, optimism was mediated by resilience to impact on subjective well-being.18 Similarly, Holaday et al9 found a significant association between healthy positive self-confidence and increased resilience in pediatric burn survivors. Holaday et al9 proposed that a global measure of negative coping was associated with nonresilient children; however, this was not significant potentially because of small sample sizes. Sveen et al21 also reported that a negative coping style was negatively correlated with resilience. In contrast to the optimistic outlook generally associated with resilience, one participant from the Williams et al10 study actively owned his negative affect – “I lived because I had hate”– suggesting that the negative affect style may not be detrimental to burn recovery if used as an active coping style, as opposed to avoidance.
Lau and Van Niekerk23 suggested that the coping styles influence all stages of the process of recovery from burn injury. They proposed that the key to recovery was to create a narrative of meaning that arises from reflexivity with self and others. This could be seen as an active meta-strategy for coping that centers on meaning making for self-transformation. In contrast, one of the participants from Lau and Van Niekerk’s23 study was described as having limited reflexive evaluation, leading to a narrowing view of others – “I have learned that when you are burned people treat you different” – and subsequently a narrowing sense of self. Williams et al10 reported that noticeably the women in their sample perceived the adversity associated with their injury as something that held positive implications:
I know that I am more outspoken and I will stand up for myself if the need arises. I know that it was fortunate and that I survived this tragic event.10
Personal choice and perceived control were uniquely highlighted in Holaday and McPhearson’s8 study as an important component of the development of resilience. They gave examples of survivors feeling empowered to make their own recovery decisions and to take personal control:
We have the right to choose what kind of [anesthetics] we take, and we should be able to say “no” to more surgeries.8
Choice also related to attitudes toward life and acceptance of emotions. One of the participants from Holaday and McPhearson’s8 study expressed:
Sometimes I still choose to feel sorry for myself and have a bad day, and that’s OK.8
Resistance to trauma symptoms
Five of the ten papers highlighted the relationship between trauma symptoms and resilience. Symptoms of trauma in adults were measured by The Davidson Trauma Scale, Impact of Events Scale, and the posttraumatic stress disorder (PTSD) Checklist – Civilian Version (PCL-C). A subscale of the Rorschach Clinician Rating Scale was used to assess capacity to tolerate stress in children. The relationship between low trauma symptoms and high resilience was consistent across all studies despite different measures of trauma employed.
Holaday et al9 found that resilient children displayed higher tolerance to stress as compared to nonresilient children; however, the authors acknowledged the limited power of their study. Acknowledging the critical role of caregivers in supporting pediatric burn survivors, two studies17,22 assessed caregiver trauma and resilience. Parents of pediatric burn survivors were shown to experience significantly greater levels of PTSD symptoms, particularly intrusion and avoidance, as compared to the general population.17 Past trauma predicted more severe symptoms, in particular hyperarousal, intrusion, and stress. Resilience was negatively correlated with symptoms of PTSD and all three symptom clusters (intrusion, avoidance, and hyperarousal), and no difference between the sexes was found.17 Quezeda et al,22 however, found that resilience levels only in female caregivers of pediatric burn survivors predicted symptoms of trauma avoidance and intrusion that subsequently impacted on pediatric resilience.
Xia et al19 assessed trauma symptoms with the PCL-C associated with burn injury and found that the three resilience domains from the CD-RISC, tenacity, self-improvement, and optimism, negatively correlated with the total score on the PCL-C. Sveen et al21 explored PTSD trajectories at 3, 6, and 12 months after burn injuries in adults using the Impact of Events Scale. Four discrete clusters of response were identified. The “Resilient” cluster had low trauma symptoms pre and post, the “Recovery” cluster started with high trauma symptoms that reduced to low symptoms at 12 months, the “Delayed” cluster started with mild trauma symptoms and had moderate trauma symptoms at 12 months, and the “Chronic” cluster maintained high trauma symptoms consistently. Early predictive identification of recovery trajectories offers a key opportunity for early intervention, promoting resiliency.
Discussion
This integrative review sought to investigate the role of resilience within the arena of burn injury and recovery. Three main themes emerged associated with the role of resilience: relational strengths, positive coping, and resistance to trauma symptoms. These themes suggest that resilience plays a vital role in the recovery of burns trauma across the life span. Here, we have focused on the more explicit use of the term resilience and its measurement. However, wider aspects of the three themes identified are documented in the burn injury recovery literature: the importance of positive social and emotional supports from family, peers, and community or a religious or spiritual source;1,24–27 a positive versus avoidant coping style,27,28 including active attention to both the physical and emotional aspects of coping, often with the concomitant challenge of accepting the realities of injury and recovery;26 and the robustness to resist ongoing breakdown of sense of self secondary to trauma or to engage in a restorative or transformative process of integration posttrauma that can result in posttraumatic growth.24,25,29,30
This literature sits within the broader notions of human response to trauma via adaptation, coping, and meaning-making versus traumatic breakdown31–35 and contemporary attempts to explore and acknowledge the developmental and relational origins and pathways to protective coping style and capacity.30,36 The overall picture is of the importance of personal and social context of recovery and the need to optimize the psychosocial strengths and supports for burn injury survivors and their surrounding systems of care.1,25,37 Although resilience can be hard to define in a circumscribed way, it is reassuring that in Bonanno et al’s38 study of the aftermath of the September 11, 2001, attacks on New York, resilience to PTSD was high, with results remaining robust even when broader versus narrower definitions of resilience were applied. However, those who were physically injured or actually present in the towers had higher levels of PTSD and less resilience. The notion that the intimacy of the insult as relevant is important and is mirrored in the burns literature around the importance of meaning ascribed to loss of identity or function and seen in the qualitative literature reviewed here.23 Therefore, the survivor then has a more arduous task to resist traumatic breakdown or achieve posttraumatic recovery and/or growth. Holaday et al’s9 association of past trauma with less resilience has some support in the burns literature30 and is an important issue as many survivors have histories of chronic complex trauma. However, the past navigation of trauma can also provide the templates for positive adjustment and resilience: a fruit of prior posttraumatic growth.24 The outcomes of the review reiterate the importance of assessing burn survivors and pediatric caregivers for pre existing trauma and vulnerabilities to target appropriate early intervention and support strategies promoting recovery.
Implications for research and practice
This review has highlighted important areas within the burns arena worthy of further investigation related to facial burns, validated assessment tools, and long-term resilience trajectories in recovery. Previous research has suggested that disfigurement associated with the burn injury, in particular facial burns, has a significant impact on sense of identity and quality of life.30,39 The current studies reviewed, however, did not find a strong association between type, size and location of burn, and the role of resilience. Given the significant visibility and distress associated with facial burns, investigation of the role of resilience, specifically in relation to facial disfigurement, is warranted.
The use of validated assessment tools to measure resilience is in its infancy within the burns arena. Of the five studies that used a validated tool to measure resiliency, four used the CD-RISC. In a recent review of resilience measures, the CD-RISC was rated as one of the top 3 of 15 resilience scales for psychometric ratings.40 However, despite significant increasing interest from a policy and procedures standpoint, there is no current gold standard measure of resilience available.40 Furthermore, only one study was of a longitudinal design spanning a 12-month period.21 Given the evolving nature of resilience and the long-term context of burn recovery and rehabilitation, it is imperative that future research uses a longitudinal methodology to capture the breadth and depth of patient experiences as they transition through their recovery. Although there is evidence that resilience is malleable,7 there remains a dearth of intervention strategies directed to developing resilience within the burns context. The burgeoning evidence by Sveen et al,21 suggestive of four clusters of predictable recovery patterns, posits hopeful opportunities for early intervention to cultivate resilience in burn survivors and their caregivers. Given the vital role that resilience plays in recovery from burns, it is recommended that resilience be regularly assessed during the recovery period to help inform psychosocial intervention, treatment planning, and improve patient care.
Limitations and strength of evidence
This integrative review identified a small number of studies that met the inclusion criteria. Only one study was of a longitudinal design. However, these studies focused on a broad range of samples from acute through to long-term burn survivor recovery, with representation across the life span. Studies were based across six countries that encompassed both developed and developing nations, therefore giving a global perspective. The included studies explored a range of demographic and psychosocial variables associated with resilience and offered a breadth and depth of data using quantitative, qualitative, and mixed methods designs.
The incongruence of the methodological design was mitigated by the use of the integrative review method. A meta-analysis was not viable because of the differing scales used to measure resilience and trauma symptoms. Although the search strategy was comprehensive and targeted five key health care-focused databases, it is possible some papers may have been missed. To ensure rigor, the four authors independently reviewed all papers for inclusion in the review.
Conclusion
Resilience is a vital component of the recovery from burn injuries and has been shown to facilitate transformational recovery over time. This integrative review identified three key themes encompassing relational strengths, positive coping, and the resistance to trauma symptoms. These are fundamental constructs associated with developing and sustaining resilience that resonate with the broader literature on burn recovery. Despite the limited evidence available, resilience is a significant component of adjustment to and recovery from burns trauma. In clinical practice, regular assessment of resilience will help to inform psychosocial interventions to better support patients during their recovery from their burn injury. To further understand how resilience may be nurtured and developed, particularly for those with preexisting vulnerabilities and trauma experiences, future research should focus on robust longitudinal studies, using validated measures, and assess the impact of interventions specifically designed to address low resilience in burn survivors and their caregivers.
Disclosure
The authors report no conflicts of interest in this work.
References
Kornhaber R, Wilson A, Abu-Qamar MZ, McLean L. Adult burn survivors’ personal experiences of rehabilitation: an integrative review. Burns. 2014;40(1):17–29. | ||
Kornhaber R, Wilson A, Abu-Qamar MZ, McLean L. Coming to terms with it all: adult burn survivors’ ‘lived experience’ of acknowledgement and acceptance during rehabilitation. Burns. 2014;40(4):589–597. | ||
Kornhaber R. Roads to Recovery: Adult Burn Survivors’ ‘Lived Experience’ of Rehabilitation. Adelaide, Australia: School of Nursing, University of Adelaide; 2013. | ||
Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. 2004;59(1):20–28. | ||
Kadner K. Resilience. Responding to adversity. J Psychosoc Nurs Ment Health Serv. 1989;27(7):20–25. | ||
Iacoviello BA, Charney DS. Psychosocial facets of resilience: implications for preventing posttrauma psychopathology, treating trauma survivors, and enhancing community resilience. Eur J Psychotraumatol. 2014;5:23970. | ||
Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. | ||
Holaday M, McPhearson RW. Resilience and severe burns. J Counseling Dev. 1997;75(5):346–356. | ||
Holaday M, Terrell D. Resiliency characteristics and Rorschach variables in children and adolescents with severe burns. J Burn Care Rehabil. 1994;15(5):455–460. | ||
Williams NR, Davey M, Klock-Powell K. Rising from the ashes: stories of recovery, adaptation and resiliency in burn survivors. Soc Work Health Care. 2003;36(4):53–77. | ||
Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546–553. | ||
Russell CL. An overview of the integrative research review. Prog Transplant. 2005;15(1):8–13. | ||
Soares CB, Hoga LA, Peduzzi M, Sangaleti C, Yonekura T, Silva DR. [Integrative review: concepts and methods used in nursing]. Rev Esc Enferm USP. 2014;48(2):335–345. | ||
Souza MT, Silva MD, Carvalho Rd. Integrative review: what is it? How to do it? Einstein (São Paulo). 2010;8(1):102–106. | ||
Mulrow CD. Rationale for systematic reviews. BMJ. 1994;309(6954):597–599. | ||
Oxman A, Guyatt G. Guidelines for reading literature reviews. Can Med Assoc J. 1988;138(8):697–703. | ||
McGarry S, Girdler S, McDonald A, Valentine J, Wood F, Elliott C. Paediatric medical trauma: the impact on parents of burn survivors. Burns. 2013;39(6):1114–1121 | ||
He F, Cao R, Feng Z, Guan H, Peng J. The impacts of dispositional optimism and psychological resilience on the subjective well-being of burn patients: a structural equation modelling analysis. PLoS One. 2013;8(12):e82939. | ||
Xia ZY, Kong Y, Yin TT, Shi SH, Huang R, Cheng YH. The impact of acceptance of disability and psychological resilience on post-traumatic stress disorders in burn patients. Int J Nurs Sci. 2014;1(4):371–375. | ||
Yang Z, Wang JQ, Zhang BZ, Zeng Y, Ma HP. Factors influencing resilience in patients with burns during rehabilitation period. Int J Nurs Sci. 2014;1(1):97–101. | ||
Sveen J, Ekselius L, Gerdin B, Willebrand M. A prospective longitudinal study of posttraumatic stress disorder symptom trajectories after burn injury. J Trauma. 2011;71(6):1808–1815. | ||
Quezada L, Gonzalez MT, Mecott GA. Explanatory model of resilience in pediatric burn survivors. J Burn Care Res. Epub May 28, 2015. | ||
Lau U, van Niekerk A. Restorying the self: an exploration of young burn survivors’ narratives of resilience. Qual Health Res. 2011;21(9):1165–1181. | ||
McLean L, Proctor M, Rogers V, Shaw J, Kwiet J, Streimer J. Secure attachment to God and a secure/comfortable attachment organization may both promote healthy recovery from severe burns injury. In: Hochheimer JL, Fernandez-Goldborough J, editors. Spirituality: Conversations for the 21st Century. Oxford, UK: Inter-Disciplinary Press; 2013:147–170. | ||
Kornhaber R, Wilson A, Abu-Qamar M, McLean L, Vandervord J. Inpatient peer support for adult burn survivors – a valuable resource: a phenomenological analysis of the Australian experience. Burns. 2015;41(1):110–117. | ||
Kornhaber R, Wilson A, Abu-Qamar MZ, McLean L. Coming to terms with it all: adult burn survivors’ ‘lived experience’ of acknowledgement and acceptance during rehabilitation. Burns. 2014;40(4):589–597. | ||
Lawrence JW, Fauerbach JA. Personality, coping, chronic stress, social support and PTSD symptoms among adult burn survivors: a path analysis. J Burn Care Res. 2003;24(1):63–72. | ||
Kildal M, Willebrand M, Andersson G, Gerdin B, Ekselius L. Coping strategies, injury characteristics and long-term outcome after burn injury. Injury. 2005;36(4):511–518. | ||
McLean L. Leaving the old house in story and song: an attachment and relational perspective on personal and communal crises and post-traumatic growth. In: Bray P, McLean L, editors. At the Crossroads of Crisis and Opportunity: Interdisciplinary Conversations. Oxford, UK: Inter-Disciplinary Press; 2015. | ||
McLean LM, Rogers V, Kornhaber R, et al. The patient-body relationship and the “lived experience” of a facial burn injury: a phenomenological inquiry of early psychosocial adjustment. J Multidiscip Healthc. 2015;8:377–387. | ||
Vaillant GE. Adaptation to life. Cambridge, MA: Harvard University Press; 1977. | ||
Janoff-Bulman R. Shattered Assumptions. New York, NY: The Free Press; 2010. | ||
Tedeschi RG, Calhoun LG. Posttraumatic growth: conceptual foundations and empirical evidence. Psychol Inq. 2004;15(1):1–18. | ||
Neimeyer RA. Complicated grief and the reconstruction of meaning: conceptual and empirical contributions to a cognitive-constructivist model. Clin Psychol Sci Pract. 2006;13(2):141–145. | ||
Frankl VE, Lasch I, Kushner HS, Winslade WJ. Man’s Search for Meaning. Boston, MA: Beacon Press; 2006. | ||
Maunder RG, Hunter JJ. Attachment and psychosomatic medicine: developmental contributions to stress and disease. Psychosom Med. 2001;63(4):556–567. | ||
Badger K, Royse D. Adult burn survivors’ views of peer support: a qualitative study. Soc Work Health Care. 2010;49(4):299–313. | ||
Bonanno G, Galea S, Bucciarelli A, Vlahov D. Psychological resilience after disaster: New York City in the aftermath of the September 11th terrorist attack. Psychol Sci. 2006;17(3):181–186. | ||
Gullick JG, Taggart SB, Johnston RA, Ko N. The trauma bubble: patient and family experience of serious burn injury. J Burn Care Res. 2014;35(6):e413–e427. | ||
Windle G, Bennett KM, Noyes J. A methodological review of resilience measurement scales. Health Qual Life Outcomes. 2011;9(1):8. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.