")
Back to Journals » Patient Preference and Adherence » Volume 18
The Patients’ Presupposed Distrust to Doctors in China: An Explanatory Sequential Mixed Methods Study
Authors Li Y, Wei Y, Liang X, Dou X
Received 25 October 2023
Accepted for publication 23 January 2024
Published 5 February 2024 Volume 2024:18 Pages 349—359
DOI https://doi.org/10.2147/PPA.S446630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yan Li,1 Yanbin Wei,1 Xueping Liang,1 Xinman Dou1,2
1School of Nursing, Lanzhou University, Lanzhou, People’s Republic of China; 2Second Clinical Medical College, Lanzhou University, Lanzhou, People’s Republic of China
Correspondence: Xinman Dou, Second Clinical Medical College, Lanzhou University, No. 82 Cuiyingmen, Chengguan District, Lanzhou, 730000, People’s Republic of China, Tel +86-13909318916, Email [email protected]
Purpose: The aim of this study was to investigate the current status of patients’ presupposed distrust, and to clarify the causes of high presupposed distrust.
Patients and Methods: An explanatory sequential mixed methods study was conducted using a two-stage design. The first phase was a quantitative cross-sectional survey, a total of 384 patients by convenience sampling completed the survey. Study instruments including demographic and clinical characteristics sheet, patients’ presupposed distrust scale. In the qualitative phase, 16 patients on the basis of their mean score for all PPDS items were higher than 4 were identified as extreme cases participated in one-to-one semi-structured interviews.
Results: The total item mean score for all patients on PPDS was 3.59(3.18, 4.09), which above the median range of the PPDS (item mean score of 3). Personal income level and educational level were significant predictive influencing factors of patients’ presupposed distrust, which could explain 17.347% of the variance. The reasons of high patients’ presupposed distrust were as follows: moral character, health knowledge, patient perceptions, and the social circumstance.
Conclusion: The level of patients’ presupposed distrust was high, which needs to be further decreased. Demographic and clinical variables (personal income level, educational level) are identified to be the major contributing factors. The main causes for the formation of the high patients’ presupposed distrust are patients internal factors and social circumstance.
Keywords: patients, presupposed distrust, root cause analysis, cross-sectional investigation, qualitative research
Introduction
A good doctor–patient trust is the fundamental factor ensuring a normal medical process.1,2 From the perspective of patients, doctor-patient trust can be divided into three stages: presupposition trust before medical treatment, relationship trust in the process of medical treatment, and cognitive trust after medical treatment.3–5 The presupposed trust in doctors is a prerequisite for patients to actively establish a doctor-patient relationship. If the patient does not have presupposed trust in the doctor, it may lead to the breakdown of the doctor-patient relationship.
The patient’s presupposed distrust refers to the patient has presupposed that the medical ethics and technical capabilities of the doctor are not credible before they taking medical treatment.6 It has been hypothesized or demonstrated that patients’ presupposed distrust will lead to corresponding defensive or resistive measures when seeking medical care, including ingratiate with doctors by giving them gifts or bonuses, conceal sensitive information, doubt about the doctor’s diagnosis, not cooperate with examination or treatment, missing a subsequent visit, and dropping out of care.7–9 In addition to the presupposed distrust that patients invest in healthcare professionals having a negative impact on their own quality of care. It is also harm to physicians and the medical system as a whole.10 Therefore, an understanding of the nature of patient’s presupposed distrust, in addition to the reasons for the patient’s presupposed distrust, is exceedingly important for health professionals.
Although the literature on doctor-patient relationship and doctor-patient trust/distrust has been increasing, there are fewer literature focus on the topic of patient’s presupposed distrust. Li et al described behaviors of patient’s presupposed distrust, including (i) not seeing a doctor; (ii) pulling strings and giving red envelopes when seeing a doctor; and (iii) an increase in medical disputes and the occurrence of medical violence.4 Wang et al illustrated patient’s presupposed distrust and doctor-patient trust crisis. They stated that patient’s presupposed distrust of doctors in general plays a dominant role in the doctor-patient trust crisis.11 Xu SQ conducted a survey to explore the relationship between frustration in treatment, patient’s presupposed distrust, and patient aggression.6 Our study aimed to examine patients’ presupposed distrust, using a mixed-methods methodology. The first part was a quantitative study of to investigate the current status and the contributing factors of patient’s presupposed distrust. We then used individual in-depth interviews to clarify the causes of patient’s presupposed distrust.
Materials and Methods
Study Design
This research project was performed as a mixed-methods study, where an explanatory sequential design was adopted.12 In this design, we first conducted a quantitative cross-sectional survey (phase I), followed by qualitative data generated through one-to-one semi-structured interviews in the second phase (phase II).13 The use of a sequential explanatory mixed approach is different compared with previous studies investigating the presupposed distrust among patients. Some studies have conducted reviews, and some have applied quantitative method. The reasons for undertaking a sequential explanatory mixed methods design were: (i) A comprehensive understanding of the problem than conducting a qualitative study or a quantitative study alone;12 (ii)Quantitative data helps the researcher identify the target interview group in the qualitative phase.14
Setting and Sampling
This study was conducted at three large general public hospital in the northwest China province, all of which were Grade-A Tertiary Hospitals. Patients attending these three hospitals were invited to participate. The criteria for inclusion were as follows: (a) being outpatients, emergency, or stable inpatients; (b) a resident of Chinese, and be able to read and understand Chinese; (c) an age of at least 18 years; (d) willing to participate and share experience; and (e) provided informed written consent. Exclusion criteria included patients receiving psychological treatment and medication, and patients admitted to crisis units. For the quantitative study phase, the sample size was estimated using the G*power 3.1.9.7 program.15 Performing multiple linear regression analysis based on a median effect size of 0.15, a statistical power of 95% at a significance level of 0.05, with the number of predictors of 9, the appropriate number of participants was estimated to be 166. Given that 20% of the questionnaires may be invalid, we estimated that a sample size of at least 199 were needed. However, a total of 384 patients by convenience sampling completed the survey. For the qualitative study phase, purposive sampling was used to select participants from a subset of the same quantitative sample based on the Patients’ Presupposed Distrust Scale (PPDS) score. Participants whose mean score for all PPDS items higher than 4 were selected for interviews. Sample size was determined by data saturation,16 that is to say there was no new details provided by other participants in further interviews.
Study Instruments
Demographic and Clinical Characteristics sheet: Demographic and Clinical Characteristics sheet was used to collect information relevant to the participants’ age, gender, place of residence, marital status, education level, personal monthly income (RMB), patient categories, duration of illness, and the payment manner of the medical expenses.
Patients’ Presupposed Distrust Scale (PPDS): Patients’ presupposed distrust were assessed using the PPDS. This scale was developed by Zheng XJ.17 The Cronbach’s alpha of the scale in the study of Zheng XJ was 0.707 and in present study was determined to be 0.800. The PPDS consists of 22 items across eight different dimensions: doctor-patient communication (3 items), patients’ personal experiences (4 items), Medical training (3 items), medical system (2 items), medical ethics of doctors (2 items), doctor’s skills (2 items), patient judgment (3 items), other factors (3 items). All items are scored on a five‐point Likert scale, where 5= strongly high, 4= relatively high,3= middle level,2= relatively low and 1= strongly low.17 The scores of negative items were reversed. Consequently, scale level scores were calculated as the mean score across responses to all PPDS items, and dimensions level scores were calculated as the mean score of responses to all items in each dimension. To help with interpretation, the mean score for all PPDS items were higher than 4 indicating a greater patients’ presupposed distrust.
Semi-structured interview outline: The semi-structured interview outline was formulated based on the results of the quantitative phase and an integrative review of the literature (Table 1).
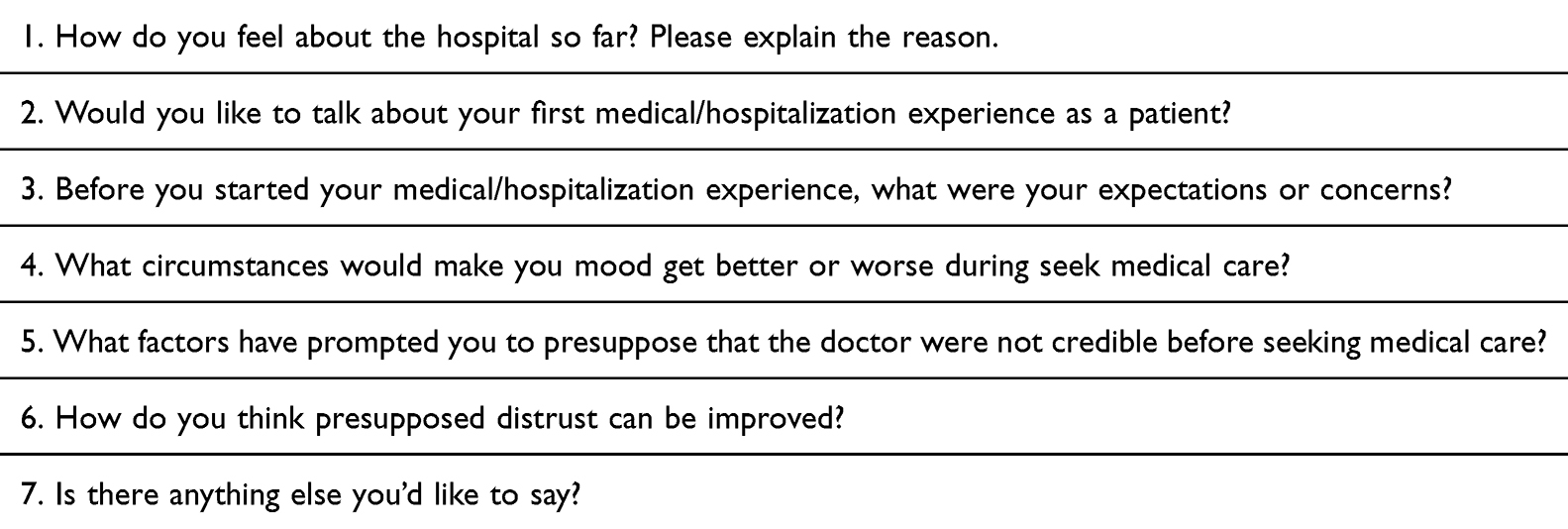 |
Table 1 Semi-Structured Interview Outline |
Data Collection
Collection of data for quantitative phase begun from January 2023 to April 2023. At the research site, we distributed the PPDS, the demographic and clinical characteristics sheet to potential participants via a face-to-face approach. In an attempt to be able to invite selected participants to attend in the qualitative phase, all participants in the quantitative phase were required to provide their cell phone numbers, which was used by the first author to arrange the interview. Qualitative data were collected between May 2023 and June 2023. Individual, in-depth interviews were conducted using the semi-structured interview outline either in web-based video platform WeChat or over the telephone. The average length of interview lasted on 35 min (range: 22–60 min). Each participant was compensated 5 CNY cash upon completion of the quantitative survey and 10 CNY cash upon completion of the qualitative interview.
Data Analysis
In the quantitative phase, data were analyzed using SPSS software (IBM version 22). The statistical significance level was set at p<0.05. Descriptive statistics including frequencies, percentages, median and interquartile range used to evaluate demographic and clinical characteristics data, PPDS scores. We also conducted a series of Mann–Whitney test, Kruskal–Wallis test or Spearman according to characteristics of the sample (demographic and clinical) to compare possible significant differences. Multiple linear regression was used to predict factors that influenced patients’ presupposed distrust.
In the qualitative phase, the semi-structured interview data were analyzed using deductive thematic analysis following the 6-step guidelines by Braun and Clarke.18
Ethical Approval
This study was approved by the Ethics committee of the School of Nursing at Lanzhou University (Letter Number: LZUHLXY20200006), and all procedures of this study performed in accordance with the principles of the Declaration of Helsinki. Furthermore, written informed consent was obtained from each participant, all of them were guaranteed confidentiality and anonymity within any future published work, and each participant in the qualitative study agreed to have their responses analyzed and reported anonymously.
Results
Quantitative Phase results
Participants Demographic and Clinical Characteristics
Across the three Grade-A Tertiary Hospitals, 384 patients complete the survey, of which 14(3.65%) responses were invalid due to missing data. As a result, 370(96.35%) valid data were analyzed. The patients were aged 18–80 years (mean: 35.67, median: 32, SD: 12.84). A total of 70.27% (n = 260) of respondents were outpatients, and a similar proportion (67.03%, n =248) reported married. More details about patients’ demographic and clinical characteristics are shown in Table 2.
 |
Table 2 Demographic and Clinical Characteristics of Patients and Univariate Analysis of PPDS Scores (n=370) |
Patients’ Presupposed Distrust Scores
The total item mean score for all patients on PPDS was 3.59(3.18, 4.09), which above the median range of the PPDS (item mean score of 3). The item mean score for the eight dimensional, in descending order, were Doctor-patient communication, Doctor’s skills, Medical system, Patients’ personal experience, Doctor’s characterization, Other factors, Patients’ judgment, Doctor’s medical ethics (Table 3).
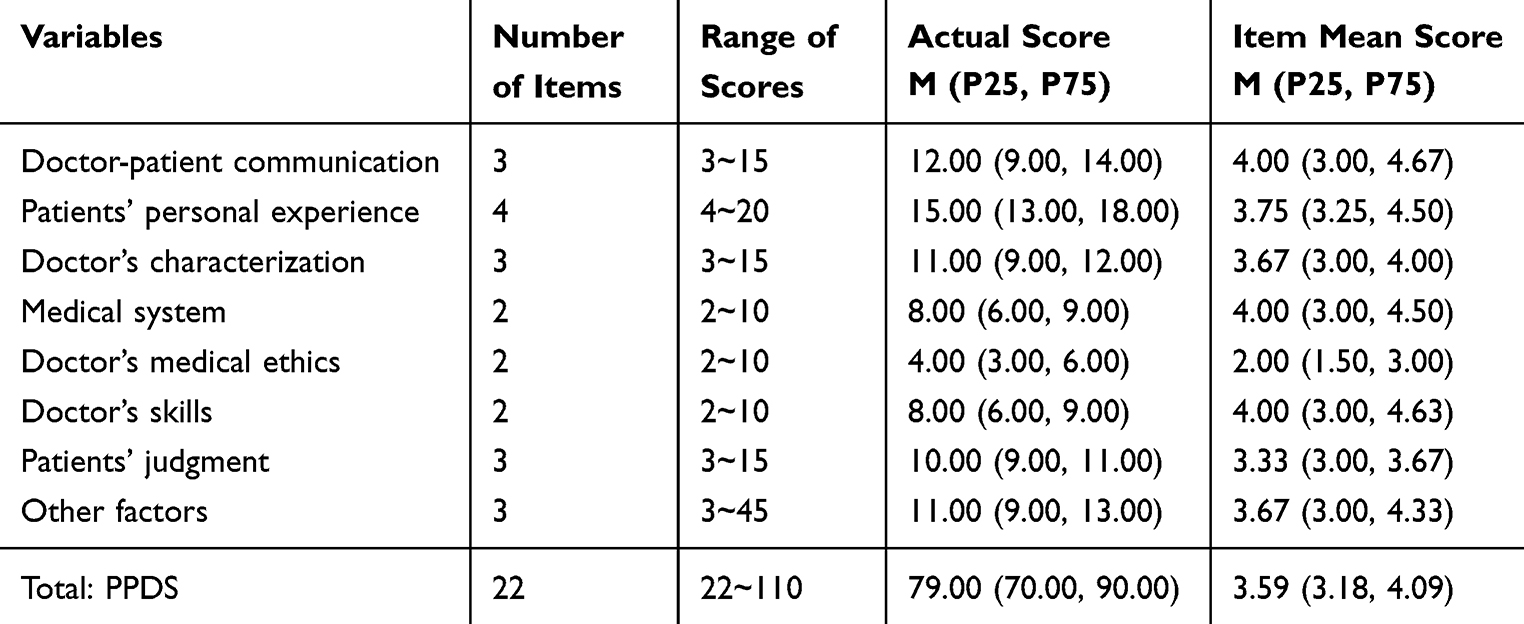 |
Table 3 Presupposed Distrust Scores of Patients (n=370) |
Univariate Analysis
Table 2 reports the univariate analysis of the PPDS scores based on the patient demographic and clinical characteristics. There were statistically significant differences in PPDS item mean scores based on age, educational level and personal monthly income (RMB) (p < 0.05).
Multivariate Linear Stepwise Regression Analysis
Multivariate linear stepwise regression analysis identified that only personal income level and educational level were significant predictive influencing factors of patients’ presupposed distrust (adjusted R2 =0.081, F = 17.347, p <0 0.001) (Table 4).
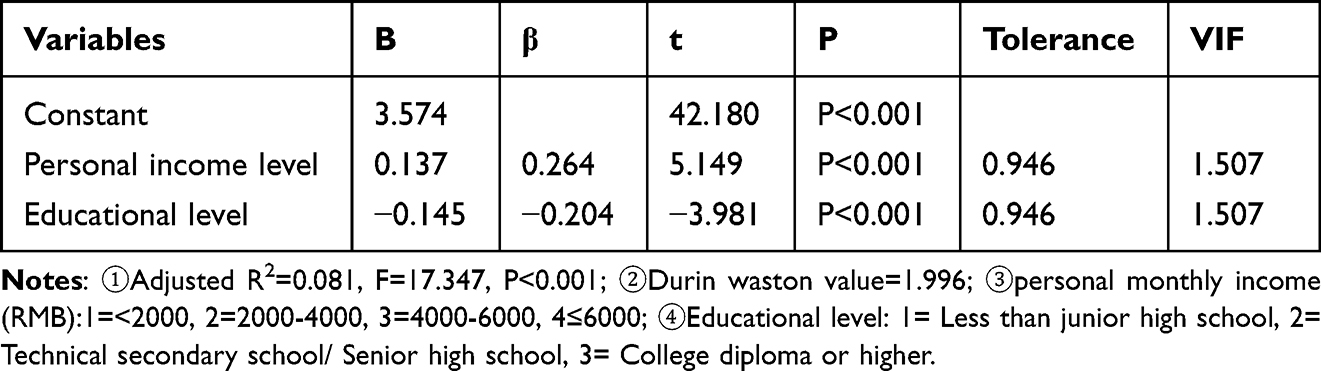 |
Table 4 Multivariate Linear Stepwise Regression Analysis of Factors Influencing Patients’ Presupposed Distrust (n=370) |
Quantitative Phase results
Based on Phase 1 results, 108 patient were selected on the basis of their mean score for all PPDS items were higher than 4. After interviewing 16 patients, it was found that no new information emerged, so a saturated sample size of 16 was reached and patients were coded as N1 to N16 (six women and ten men, ages 18–74 years), recruited from three large general public hospital in the northwest China province. The findings of the qualitative analysis emerged four subthemes and two themes. Below, we present further information on these themes and sub-themes.
Theme 1: Patient Factors
Sub-theme 1.1: Low moral character
Moral qualities are cultivated and formed by individuals over a long period of social practice. Good moral character enables individuals to build positive and healthy relationships and increase trust in each other. Patients attribute the presupposed distrust to doctors while ignoring the impact of their own moral character on presupposed distrust. On the one hand, patients with high moral character are usually more understanding of their doctors and behave relatively gentleness and humility, no matter what situation they are facing. As for patients with relatively low moral character, they usually hold on to a little thing and then suspect or blame the doctor, or even say insulting and hurtful words to the doctor because the doctor does not follow their requirements.
During my visit, there were not many people waiting in front of me, but this doctor was so procrastinate that I waited for a long time before it was my turn, which annoyed me and made me wonder if this doctor was not good at his profession. (N1)
I Think I Paid to Come to the Hospital, so as a Consumer Shouldn’t They Provide Me with Great Service? (N5)
Sub-theme 1.2: Limited health knowledge
Patients with limited health knowledge have a higher level of presuppositional mistrust, and they tend to perceive a knowledge gap between themselves and healthcare professionals, which puts them in a somewhat vulnerable position. As a result, they are more likely to transfer their emotions to healthcare professionals.
They did not explain to me at all why they were doing these tests. I asked them and they dismissed me very perfunctorily, and in the end I still didn’t get it. This made me feel very unsafe. (N5)
I feel like my own health knowledge is limited. I do what they tell me to do, and treatment decisions are completely dependent on them. But I’m actually still a little unsure in my mind. (N7)
My doctor would talk to me about my treatment plan. I feel that what they say is too specialized and I don’t quite understand. But I don’t dare to ask my doctors more questions for fear that they will think I am troublesome. However, I have a lot of doubts about my illness. (N10)
Sub-theme 1.3: Patient perceptions
Sub-theme 1.3.1: perceived lack of professional experience of health care providers
The professionalism of a doctor is one of the most important factors that patients weigh when choosing a doctor. If the patient believes that the doctor’s level of professionalism is low, then the patient will be skeptical of the doctor and thus become wary of him or her in advance.
I don’t think the doctors here are professional at all, at first I didn’t even know how to use the medication and what treatments I had to do. I was completely clueless and it made me skeptical of this doctor. (N1)
When the doctors were on their daily ward rounds, they often brought a large group of people with them and rarely interacted with me the entire time, as if they were going through the motions. I felt like a tool and doubted their ability to take care of me. (N8)
He acted very casually when he examined me and I was worried that he wasn’t as authoritative as I expected him to be. I don’t think he is an expert at all and can’t handle my illness well. (N9)
The doctor was very unskilled in examining me. I thought that this doctor might be inexperienced and was just practicing on me. This made me scared. The point is that I had read the profile of this doctor before registering, but still this result. I feel like I already have a shadow over coming to the hospital. (N6)
Sub-theme 1.3.2: Perceived lack of sincerity and patience of health care providers
Most of the patients expressed the hope that their doctors would maintain a good attitude and patiently provide them with sufficient information during the visit.
The whole time I was at the doctor, it was the student sitting next to the doctor who talked to me. I asked questions and the doctor simply ignored me. The student also tried to get rid of me quickly and started calling the next person while I was still sitting there. I felt so angry and aggravated. I never want to deal with a doctor again. (N9)
I don’t need any extra care. I just want my doctor to talk to me as an equal and not make me feel like I’m being looked down upon. (N14)
During my several visits, the doctor’s face was particularly ugly and his attitude was not kind at all. I felt embarrassed and like a lackey myself. I wouldn’t want to interact with him much and just wanted to get away. (N2)
If the doctor is able to comfort me and make me feel relaxed about the environment, I would be willing to go back to him. (N13)
Will they get annoyed if I always asked this and that? Would I offend them? If they can clearly say that they are very supportive of me asking, then I think I will like them a lot. (N3)
Theme 2: Social Circumstance
Sub-theme 2.1: Popularization of the Internet
The use of the Internet can affect patients’ presupposed distrust. On the one hand, the internet tends to report negative news, which amplifies the impact of adverse doctor-patient events and creates a crisis of presuppositional distrust in doctors; On the other hand, when the health information on the Internet is inconsistent with the information provided by doctors, it will raise patients’ presupposed distrust in doctors.
When I first got sick, I used to learn about the disease first through my cell phone. But when I actually arrived at the hospital, I realized that what the phone said was different from what the doctor said in many ways, and I was confused. (N14)
Before I come to see a doctor, I would go online and search for information about the doctor. If the doctor is little known or has bad reviews, I won’t go to him. (N4)
I’ve read a lot of negative things about hospitals on the internet and it makes me anxious. But I was sick and had to come to the hospital. I was worried that I would be treated the same way. (N3)
Discussion
This paper provides insights into the level of patients’ presupposed distrust and identified the reasons that led to their presupposed distrust. The quantitative findings reveal that participants had a high level of presupposed distrust in doctors. The qualitative findings reveal the main reasons (patients’ low moral character, patients’ limited health knowledge, patients’ perceptions, and social circumstance) for this high level of presupposed distrust as well as the improvements required to reduce patients’ presupposed distrust. These findings provide a deeper understanding about presupposed distrust and the doctor-patient relationship.
Analysis of Patients’ Presupposed Distrust Levels
The results of this study showed that the patients’ presupposed distrust scores were [3.59 (3.18, 4.09)]. The item mean score for the each dimensional, in descending order, were: doctor-patient communication[4.00 (3.00, 4.67)], doctor’s skills[4.00 (3.00, 4.63)], medical system[4.00 (3.00, 4.50)], patients’ personal experience[3.75 (3.25, 4.50)], doctor’s characterization[3.67 (3.00, 4.00)], other factors[3.67 (3.00, 4.33)], patients’ judgment[3.33 (3.00, 3.67)], doctor’s medical ethics[2.00 (1.50, 3.00)].Taking the median of 3 as a criterion, the item mean scores for the scale and the dimensions (except for the dimension of doctor’s medical ethics) were above the median of 3. This indicates that the patients’ presupposed distrust at a high level, which is consistent with the findings of Tucker et al and Nie et al7,8 It means that most patients will a priori put their healthcare professionals in a situation where they cannot be trusted. They even doubt whether healthcare professionals can see and understand diseases, and whether they can treat and cure them.8,19 They are two possible explanations for this. Firstly, most of the relationship between healthcare professionals and patients is that of strangers.20,21 When patients are faced with an unfamiliar healthcare professional, they are often more inclined to choose distrust or half-believe out of self-preservation instincts. Secondly, our medical system is not perfect, and patients lack the general trust of the healthcare professional community.22
Influencing Factors Analysis of Patients’ Presupposed Distrust
This study showed that there were significant differences in PPDS scores between patients with different educational level. The item mean scores for PPDS were higher for patients whose educational level was less than junior high school [3.66 (3.28, 4.25)], in comparison to college diploma or higher patients(3.52 (3.05, 3.89).The reason may be that highly educated patients have their own stable cognition.23 They are able to think independently and acquire more knowledge related to diseases. As a result, they are able to look at the occurrence and development of diseases more rationally and are less likely to misunderstand healthcare professionals. This, to some extent, reduces their preconceived distrust. As for patients with low education level, their health literacy level and expressive skills are generally lower. The ability to accept and understand disease information is weak. Most of them have a stock of medical knowledge that does not support them well in communicating with healthcare professionals about their illnesses.24 And they cannot accept that their health is in a bad state. Therefore, they were prone to hold a distrustful attitude towards healthcare professionals, which leads to higher PPDS scores. This suggests that in clinical work, healthcare professionals should pay more attention to patients with lower education levels. Disease-related lectures can be conducted on a regular basis to provide targeted information support to these patients. In addition, healthcare professionals should try to use easy-to-understand language when explaining disease-related knowledge, so as to help them understand the relevant content of treatment. This will gradually improve their ambiguous understanding of the disease and promote the reversal of patients’ presupposed distrust.
This study found that patients’ presupposed distrust was influenced by their personal monthly income. Patients with a personal monthly income of 4000 RMB [3.82 (3.32, 4.27)] and above had higher PPDS scores compared to lower personal monthly income patients [3.36 (3.00, 3.86)]. The reason for this may be that patients with higher incomes demand higher quantity and quality of health care services. They will be more discerning compared to patients with lower incomes. To put it simply, in the low-income patient group, their demand may just to be able to see a doctor. However, in the high-income patient group, they not only demand to be able to see the doctor and see the doctor well, but also the quality of medical services should be good. Consequently, the PPDS scores increases in high-income patient groups. Based on this, healthcare professionals in China should pay more attention to patients with better financial status so that they can experience the convenience, continuity, and safety of healthcare services in the process of accessing healthcare.25 This will enable them to maximize their health at the appropriate economic cost and reduce their level of preconceived mistrust.
Reasons of Patients’ Presupposed Distrust
The causes of patients’ presupposed distrust include patient factors (moral character, health knowledge, patient perceptions) and the social circumstance.
The higher a patient’s moral character, the greater their ability to respond effectively and self-regulate. They often tend to see things in a positive light. This can buffer the impact of negative clinical events to some extent, thus reducing the level of presupposed distrust. It is suggested that in order to reduce the level of patients’ presupposed distrust, attention should be paid to the molding of their moral character.
Health knowledge was the most important protective factor for presupposed distrust. It is also consistent with the results of quantitative research in which education level is one of influential factor in patients’ presupposed distrust. Therefore, in order to reduce patients’ presupposed distrust, patients’ health knowledge and their ability to acquire health knowledge should be improved.
Patient perception is defined as the subjective evaluation that patients form based on their prior experience and knowledge during their medical visits. Such evaluations are empirical perceptions developed by the patient’s irrational and subjective analysis of his or her medical experience.26 As most patients do not know any medical-related professional knowledge, they are unable to objectively evaluate the standard of their doctors. Then, they can only rely on their own simple perception during the consultation process to judge whether the doctor is trustworthy or not. There are only two areas in which patients can judge whether a doctor is trustworthy or not - treatment results and the experience of the visit. The treatment results are lagging and take a while to be seen. But the experience is immediate, and it determines whether or not the patient has confidence in you and is willing to continue to trust you in the event of an abnormality. The professionalism and attitude of the doctor plays a vital role in shaping the patient experience. In this study, patients’ perceptions were mainly reflected in patients’ perceptions of doctors’ professionalism and attitudes. Most patients described two common scenes to us.
A doctor spoke a lot of specialized term and appeared to be very specialized, but the patient could not understand a word of it. After the visit, the patient was still confused and felt unsafe.
“Doctors were ambiguous or impatient with words”. This suggests that healthcare professionals should not be limited to the practice of medicine alone, but should also include communication, care and empathy with patients. It is important to be able to make patients strongly perceive your professionalism and attitude from your facial expressions and gestures, to perceive that you are conveying care and friendliness, and to gain a sense of security, which in turn creates a sense of trust.
The social environment mainly refers to the role played by the Internet in pushing the envelope. With the rise and popularization of the Internet, it has become an important source of information for individuals to know and understand the current situation of society. Negative news about doctor irresponsibility, misdiagnosis, and violent medical incidents usually gains more attention.27 Individuals, in the course of prolonged contact with negative medical news on the Internet, gradually build up a negative impression of the doctor community based on the world portrayed by the media, which in turn negatively affects patients’ presupposed distrust. It is suggested that, on the one hand, the Internet should not expend negative information and add a lot of emotionally-rendered content in the reporting of medical-related events. This can exacerbate people’s fears and insecurities, leading to less tolerance and even stereotypical prejudice against the doctor community. On the other hand, as a social group, when we are confronted with negative medical information, we have to learn to screen and judge the authenticity and bias of the reports, and to improve our personal media literacy.
Discussing Integrated Findings
Integration is the point in an explanatory sequential mixed method design where the quantitative part interfaces with the qualitative part, and it involves an interaction or conversion between qualitative and quantitative. It reflects the richness of mixed methods study, and leading to a deeper understanding of a phenomenon.14,28 Findings from the quantitative results showed the patients’ presupposed distrust scores were higher in the dimensions of doctor-patient communication and doctor’s skills, followed by subthemes emerged from the qualitative data analysis corresponding to quantitative results. The presentation of this joint points allows the qualitative interviews to complement these key quantitative findings.
Doctor-Patient Communication
The quantitative data suggested that doctor-patient communication was a significant factor in patients’ presupposed distrust. The analysis of the interviews showed that most of the patients wanted their doctors to maintain a good attitude and be patient enough during their visits. Doctor-patient communication mainly refers to the exchange of information and emotional communication between doctors and patients in the process of diagnosis and treatment of disease. It is a basic clinical skill that enables the establishment of a relationship of trust between health care providers and clients. As a result, having good doctor-patient communication was necessary to reduce patients’ presupposed distrust, and incorporating a good attitude and patience in communication was considered an effective way to improve patients’ presupposed distrust.
Doctor’s Skills
Analysis of the quantitative data showed that doctor’s skills were a contributing factor to patients’ presupposed distrust. The qualitative analysis further helped to explain the quantitative findings as it showed that patients showed more presupposed distrust in the group of doctors who behaved casually and went through the motions.
Confirmed by quantitative and qualitative findings, doctor-patient communication and doctor’s skills perceived main way to handle patients’ presupposed distrust.
Implications for Clinical Practice
Firstly, using the identified reasons and factors to improve the current status of patients’ presupposed distrust, and second, continuing this work will allow researchers to develop population-specific interventions, and hopefully improve the level of patients’ presupposed distrust.
Limitation of the Study
This explanatory sequential mixed methods study was conducted in three provincial hospitals in the northwest China province. The sample hospital is located in the urban area of the city. The findings of the study represent the northwest region in China well, but its applicability to other areas of the China may require further research to confirm.
Conclusion
Patients’ presupposed distrust play a critical role in a health doctor-patient relationship. In order to better understand and decrease patients’ presupposed distrust, we need to have a clear view of the reason that cause patients’ presupposed distrust. According to findings from three public hospitals in northwest China province, there remains a higher level of patients’ presupposed distrust. The underlying reasons of the patients’ presupposed distrust include patients’ low moral character, patients’ limited health knowledge, patients’ perceptions, and the social circumstance.
Abbreviations
PPDS, Patients’ Presupposed Distrust Scale; RMB: Renminbi.
Acknowledgments
We express our sincere gratitude to all the patients who volunteered to participate in this study. And special thanks to the three hospitals for their support and help in the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Fundamental Research Funds for the Central Universities of China (No. lzujbky-2019-59, No. lzujbky-2022-51).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harbishettar V, Krishna KR, Srinivasa P, et al. The enigma of doctor-patient relationship. Indian J Psych. 2019;61(Suppl 4):S776. doi:10.4103/psychiatry.IndianJPsychiatry_96_19
2. Kumar B, Paul UK, Pal DK. Perception of doctor–patient relationship in the present time from the viewpoint of doctors: a qualitative study at a tertiary health-care center in Eastern India. Indian J Community Med. 2020;45(1):100.
3. Li DL, Wu YL. The characteristics of trust from the patient-centered perspective. Med Philos. 2012;2:21–23.
4. Li DL, Lu JG. The pie-constructional trust & distrust and their origins from the perspective of patients’ side. Chinese Med Ethics. 2011;024(002):201–203.
5. Gordon HS, Pugach O, Berbaum ML, et al. Examining patients’ trust in physicians and the VA healthcare system in a prospective cohort followed for six-months after an exacerbation of heart failure. Patient Educ Couns. 2014;97(2):173–179. doi:10.1016/j.pec.2014.07.022
6. Xu SQ. Mediation Effect of Presuppose Distrust Between Frustration in Treatment and Patient Aggression[D]. Guangzhou: Southern Medical University; 2017.
7. Tucker JD, Cheng Y, Wong B, et al. Patient–physician mistrust and violence against physicians in Guangdong Province, China: a qualitative study. BMJ open. 2015;5(10):e008221. doi:10.1136/bmjopen-2015-008221
8. Nie JB, Cheng Y, Zou X, et al. The vicious circle of patient–physician mistrust in China: health professionals’ perspectives, institutional conflict of interest, and building trust through medical professionalism. Develop World Bioeth. 2018;18(1):26–36. doi:10.1111/dewb.12170
9. Dang BN, Westbrook RA, Njue SM, et al. Building trust and rapport early in the new doctor-patient relationship: a longitudinal qualitative study. BMC Med Educ. 2017;17(1):1–10. doi:10.1186/s12909-017-0868-5
10. Choy HH, Ismail A. Indicators for medical mistrust in healthcare–a review and standpoint from Southeast Asia. Malays J Med Sci. 2017;24(6):5. doi:10.21315/mjms2017.24.6.2
11. Wang M, Lan YC, Zhao M. Patient’s Presupposed Distrust &Doctor-patient Trust crisis. Med Philos. 2015;36(03):47–50.
12. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Sage publications; 2017.
13. Dossett LA, Kaji AH, Dimick JB. Practical guide to mixed methods. JAMA Surg. 2020;155:254–255. doi:10.1001/jamasurg.2019.4388
14. Creswell JW, Clark VLP. Designing and Conducting Mixed Methods Research. Sage publications; 2017.
15. Faul F, Erdfelder E, Buchner A, et al. Statistical power analyses using G* Power 3.1: tests for correlation and regression analyses. Behavior Research Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
16. Glaser BG, Strauss AL. The Discovery of Grounded Theory. Aldine Publishing Company; 1967.
17. Zheng XJ. Development and Pre Liminary Application of the Patients’ Presupposed Distrust Scale. Southern Medical University (China); 2019.
18. Braun V, Clarke V. (Mis) conceptualising themes, thematic analysis, and other problems with Fugard and Potts’ sample-size tool for thematic analysis. Int J Soc Res Methodol. 2016;19(6):739–743. doi:10.1080/13645579.2016.1195588
19. Mechanic D. Public trust and initiatives for new health care partnerships. Milbank Quart. 1998;76(2):281–302. doi:10.1111/1468-0009.00089
20. Yang KS. Chinese social orientation: an integrative analysis. Chin Soc Mental Health. 1995;1995:19–39.
21. Chen XP, Chen CC. On the intricacies of the Chinese guanxi: a process model of guanxi development. Asia Pacific J Manag. 2004;21:305–324. doi:10.1023/B:APJM.0000036465.19102.d5
22. D TJ, Wong B, Nie JB, et al. Rebuilding patient–physician trust in China. Lancet. 2016;388(10046):755. doi:10.1016/S0140-6736(16)31362-9
23. Lövdén M, Fratiglioni L, M GM, et al. Education and cognitive functioning across the life span. Psychol Sci Public Interest. 2020;21(1):6–41. doi:10.1177/1529100620920576
24. Aelbrecht K, Rimondini M, Bensing J, et al. Quality of doctor–patient communication through the eyes of the patient: variation according to the patient’s educational level. Adv Health Sci Educ. 2015;20:873–884. doi:10.1007/s10459-014-9569-6
25. Shi HM. Study on the Interaction Mechanism of Mutual Influence Between Doctor-Patient Trust and Medical Service Quality Based on Patient’s Perspective. Jiangsu: Jiangsu University; 2021.
26. Lilly B, Tippins MJ, Tippins K, Lilly J. Doctor behaviors that impact patient satisfaction. Patient Exper J. 2023;10(2):103–112. doi:10.35680/2372-0247.1813
27. Han Y, K LR, Li Z, et al. Trust in the doctor–patient relationship in Chinese public hospitals: evidence for hope. Patient Preference Adherence. 2022;Volume 16:647–657. doi:10.2147/PPA.S352636
28. Creswell JW, Fetters MD, Ivankova NV. Designing a mixed methods study in primary care. Anna Family Med. 2004;2(1):7–12. doi:10.1370/afm.104
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.