")
Back to Journals » Journal of Inflammation Research » Volume 14
The Inverted-U Relationship Between Dietary Inflammatory Potential and Hearing Loss Among Adults Aged 20 Years and Over in the United States: A Cross-Sectional Study
Authors Fu Y , Chen W, Guo L , Liu Y
Received 4 September 2021
Accepted for publication 20 November 2021
Published 8 December 2021 Volume 2021:14 Pages 6671—6683
DOI https://doi.org/10.2147/JIR.S337737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yanpeng Fu,1 Wenyu Chen,2 Liqing Guo,1 Yuehui Liu1
1Department of Otorhinolaryngology Head and Neck Surgery, Second Affiliated Hospital of Nanchang University, Nanchang, People’s Republic of China; 2Nursing Department, Second Affiliated Hospital of Nanchang University, Nanchang, People’s Republic of China
Correspondence: Yuehui Liu
Department of Otorhinolaryngology Head and Neck Surgery, Second Affiliated Hospital of Nanchang University, No. 1 Minde Road, Nanchang, People’s Republic of China
Email [email protected]
Purpose: The purpose of this study was to examine the relationship between dietary inflammatory index and objective hearing loss (HL).
Materials and Methods: A cross‐sectional analysis of a nationally representative sample of participants was performed based on data in National Health and Nutrition Examination Survey (NHANES) (2009– 2016). HL was defined as pure tone averages > 25 dB at 500, 1000, and 2000 Hz (low frequency); 3000, 4000, 6000, and 8000 Hz (high frequency) in either ear. The energy‐adjusted dietary inflammatory index (E‐DII) score was calculated for each participant based on two 24‐h dietary recalls to assess diet‐associated inflammation. Multivariable logistic regression was used to examine the linear relationship between HL and E‐DII score or E-DII quartiles. Restricted cubic spline was applied to identify any non‐linear associations of the E‐DII score with hearing loss. Subgroup analyses were performed by age and gender to explore the moderating roles of these factors. Akaike’s Information Criterion (AIC) values were used to select the better-fitted model among linear and non-linear models.
Results: An inverted-U shaped relationship with low-frequency hearing loss (LFHL) was identified for the E‐DII score (P-nonlinear =0.023) after adjustment for potential confounders. But significant linear or nonlinear association between E-DII score and high-frequency hearing loss (HFHL) was not found.
Conclusion: E-DII score had inverted-U relationship with LFHL. Both pro-inflammatory diet and anti-inflammatory diet seemed to be associated with a decreased risk of LFHL compared to diet that was neither pro-inflammatory diet nor anti-inflammatory diet.
Keywords: dietary inflammatory index, inflammation, NHANES, hearing loss
Introduction
Hearing loss has been a critical concern for global public health. According to the World Health Organization (WHO), more than 466 million people across the world acquire varying degrees of hearing loss, and that number is estimated to double by 2050, over 900 million people will suffer from a disabling hearing loss.1 Hearing loss not only affects the physical and psychological health of the afflicted individuals, but also imposes a significant social and economic burden on families and society, unaddressed hearing loss incurs an annual global societal cost of $750 billion.2 Estimations of the global occupational limitations occurring due to hearing loss are $105 billion annually.2
The causes of hearing loss are myriad and result from a number of intrinsic and extrinsic factors, such as age, genetic predispositions,3 noise exposure, poor nutrition4 and current ototoxic drugs used. Animal experiments have indicated the association between immune function and hearing loss.5 Observational studies have shown an association between plasma inflammatory markers and hearing loss.6,7 Diet plays a key role in regulating an individual’s inflammatory status,8 randomized controlled trials indicated that Mediterranean diet is associated with low CRP concentrations.9,10 A meta-analysis revealed that healthy dietary patterns lead to reduced CRP.11 Results from the Nurses’ Health Study II also suggested that dietary patterns characterized by high intake of fruit, vegetables, legumes, whole grains, nuts, poultry, and fish, with moderate alcohol intake display a lower risk of hearing loss.12 Retrospective data from southern Italy showed that consumed more dairy, olives and vegetable oil, spirits and less fruits was associated with a higher risk of hearing loss.13 Recently, a cross-sectional study from the Korea National Health and Nutrition Examination Survey suggested that dietary antioxidants or anti-inflammatory food may help reduce the risk of hearing loss.14 In order to assess an individual’s dietary inflammatory potential, the dietary inflammatory index (DII) has been developed, which is a literature-based dietary score calculated from the inflammatory scores of 45 food parameters.15 To data, DII has been reported to be associated with an increased risk of a variety of inflammatory diseases and conditions, including diabetes mellitus,16 metabolic syndrome,17 cardiovascular disease,18 and chronic kidney disease.19 Andreeva et al found that a higher DII score is related with increasing risk of subjective hearing loss in old males based on a 12-year follow-up cohort from 3435 French adults.20 No study has yet reported the association between DII and objective hearing loss. This study aimed to examine the relationship between dietary inflammatory index (DII) and Low and High frequency of hearing loss in a cohort representative of the general population of adults aged 20 years old in the United States, so as to explore the effects of dietary inflammatory potential on auditory conduction.
Materials and Methods
Study Population
The National Health and Nutrition Examination Survey (NHANES) is an ongoing, cross-sectional, nationally representative series of surveys conducted by the National Center for Health Statistics (NCHS). All NHANES protocols are reviewed and approved by the NCHS Research Ethics Review Board. A stratified, multistage probability sampling design is applied to select a nationally representative sample of the resident civilian noninstitutionalized US population. In the current study, data on sociodemographic, lifestyle factors, audiometry and dietary information were analyzed for adults ≥20 years old during the 4 cycles of NHANES from 2009 to 2016, we also excluded individuals with extreme total energy intakes outside the range of 500–5000 Kcal/day.21
Audiometric Measurements and Definition of Hearing Loss
All audiometric exam sections were administered by trained examiners on participants in a sound- isolating booths in the mobile examination center (MEC). Participants using hearing aids who were not able to remove them for testing and participants who had sufficient ear pain at the time of the exam and could not tolerate headphones were excluded from the audiometry component. Hearing threshold testing was conducted on both ears of participants at seven frequencies (500, 1000, 2000, 3000, 4000, 6000, and 8000 Hz). Audiometric testing was conducted according to a modified Hughson Westlake procedure using the automated testing mode of Interacoustics Model AD226 audiometer and middle ear testing was conducted by Interacoustics Titan (middle ear analyzer). A Welch Allyn otoscope (model 25020) was used for otoscopic examination of the ears.
The low-frequency (LF) hearing threshold was defined as the average of pure-tone hearing levels at 0.5, 1, and 2 kHz, and the high-frequency (HF) hearing threshold as the average of pure-tone hearing levels at 3, 4, 6, and 8 kHz. Sensorineural hearing loss (SNHL) was inferred when either ear meet the condition of pure-tone hearing threshold >25 dB,22 normal otoscopic examination findings, normal tympanogram findings (the compliance of tympanogram range from 0.3 to 1.75, the middle ear pressure > −100 daPa).
Dietary Assessment
Two 24-hour dietary recall interviews were conducted by trained interviewers to obtain dietary information using methods developed using USDA’s dietary data collection instrument, the Automated Multiple Pass Method (AMPM) (http://www.ars.usda.gov/nea/bhnrc/fsrg). The first dietary recall was conducted in MEC and the second dietary recall was collected 3–10 days later by telephone. The mean values of nutrient intakes for day one and day two of the 24 h dietary recalls were used to calculate E-DII. NHANES applies a total of 27 food components to calculate the DII score: carbohydrate; protein; total fat; dietary fiber; cholesterol; saturated, monounsaturated, and polyunsaturated fatty acids; omega‐3 and omega‐6 polyunsaturated fatty acids; vitamins A, B1, B2, B3 (niacin), B6, B9 (folic acid), B12, C, D, and E; alcohol; beta‐carotene; caffeine; iron; magnesium; zinc; and selenium. A z‐score for each food parameter was computed by subtracting the world standard means and then dividing it by its standard deviation. Thereafter, each food parameter’s z‐score was converted to a centred percentile score and multiplied by the literature‐derived inflammatory effect score.15 All of the specific food parameters’ dietary inflammatory index scores were then summed to create each participant’s overall score. E-DII scores derived from 25 to 30 food parameters usually range from −5.5 to +5.5.23 To control the total energy intake effect, the dietary inflammatory index was calculated per 1000 kcal of food consumed (E‐DII).23 Higher positive E‐DII scores represented more pro-inflammatory diets, whereas more negative values represented more anti-inflammatory diets.
Covariates
Demographic characteristics included gender, age, race/ethnicity (non-Hispanic black, non-Hispanic white or other), education level (Less than high school, High school graduate or GED, some college or AA, College graduate or more); Health-related covariates included smoking status (never smoker, former smoker, current smoker), energy intake and BMI; Self-reported chronic diseases included diabetes, hypertension, stroke and congestive heart failure (CHF); Noise exposures were also based on self-report, work-related noise exposure was defined by a “yes” or “no” answer to the question “Ever had job exposure to loud noise?” Firearm exposure was determined by a “yes” or “no” answer to the question “Ever used firearms?” Recreational noise exposure was determined by a “yes” or “no” answer to the question “Ever had non-job exposure to loud noise?”; Use of ototoxic drug was determined by a “yes” or “no” answer to the question “In the past 30 days, have you used or taken medication for which a prescription is needed?”, ototoxic drugs included antineoplastic drug, aminoglycosides, non-steroidal anti-inflammatory drug, diuretics,24 taking any of these drugs above is considered to have used ototoxic drug.
Statistical Analysis
The 2009/2010, 2011/2012, 2013/2014, 2015/2016 cycles were combined. According to tutorials of NHANES, 8-years sampling weights were calculated by using quarter of the 2-years sampling weight (WTMEC2YR).
We computed survey-weighted least square means and 95% confidence intervals (95% CIs) for E-DII after adjusting for age, gender, race/ethnicity, education, smoking status, BMI, diabetes, hypertension, stroke and CHF. We compared the baseline characteristics of DII quartiles using the weighted chi-square test for categorical variables. Weighted multivariable logistic regression was used to examine the relations between HL and continuous E‐DII or quartile E‐DII after adjusting for different covariates. Restricted cubic splines with three knots within the range of E‐DII were used to examine the potential non‐linear relationships, non-linearity was assessed using the Wald test. The smaller Akaike’s Information Criterion (AIC) value25 was used to select the better-fitted model.
The interaction effects of age, gender, noise exposure and ototoxic drugs were examined comparing models excluding and including the interaction terms. Stratified analyses were conducted to explore the effect modification by age groups (age≥40 and age <40) and gender. In the sensitivity analysis, we reanalyzed the data without accounting for the sampling weights to test the linear and non-linear relationship between continuous E-DII and HL by multivariable logistic regression and restricted cubic splines regression.
All statistical tests were two-sided with P<0.05 considered significant and were conducted using R Project for Statistical Computing (version 4.0.4), weighted logistic regression models were fitted using the “survey” package in R, restricted cubic splines were fitted using the “rms” package in R (Supplementary Material 9).
Results
Characteristics
The participant screening process is shown in Figure 1. Table 1 shows survey-weighted participant characteristics of the US adults more than 20 years old in low-frequency model (LF model) and high-frequency model (HF model). The majority of participants were Non-Hispanic White (68.2% in LF model and 69.0% in HF model). There were slightly more female participants (54.8% in LF model and 53.8% in HF model). 11.8% and 42.3% had low-frequency and high-frequency HL. The intakes of single nutrients in LF and HF models are shown in Table S1. The E-DII score ranged from −5.54 to 4.89: the first quartile (E-DII range from −5.54 to −0.51), the second quartile (E-DII range from −0.51 to 0.75), the third quartile (E-DII range from 0.75 to 1.81) and the fourth quartile (E-DII range from 1.81 to 4.89). Characteristics of participants in LF model and HF model by E-DII quartiles are shown in Tables S2 and S3, compared with those in the first quartile of E‐DII score, participants in the fourth quartile were more likely to be male and less educated. Survey-weighted least square means of E-DII were higher in participants with LFHL (Table S4).
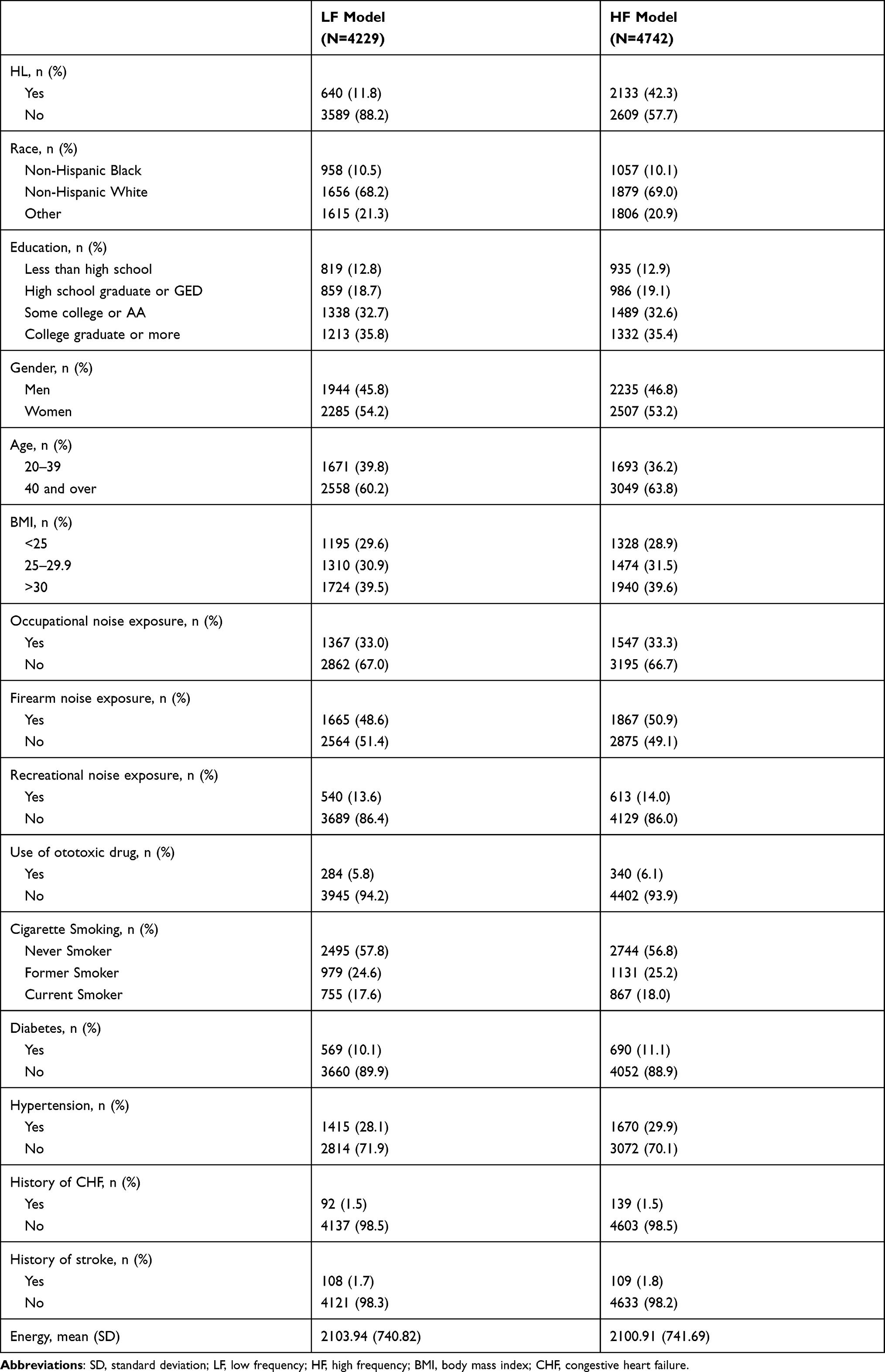 |
Table 1 Characteristics of Study Population in LF Model and HF Model |
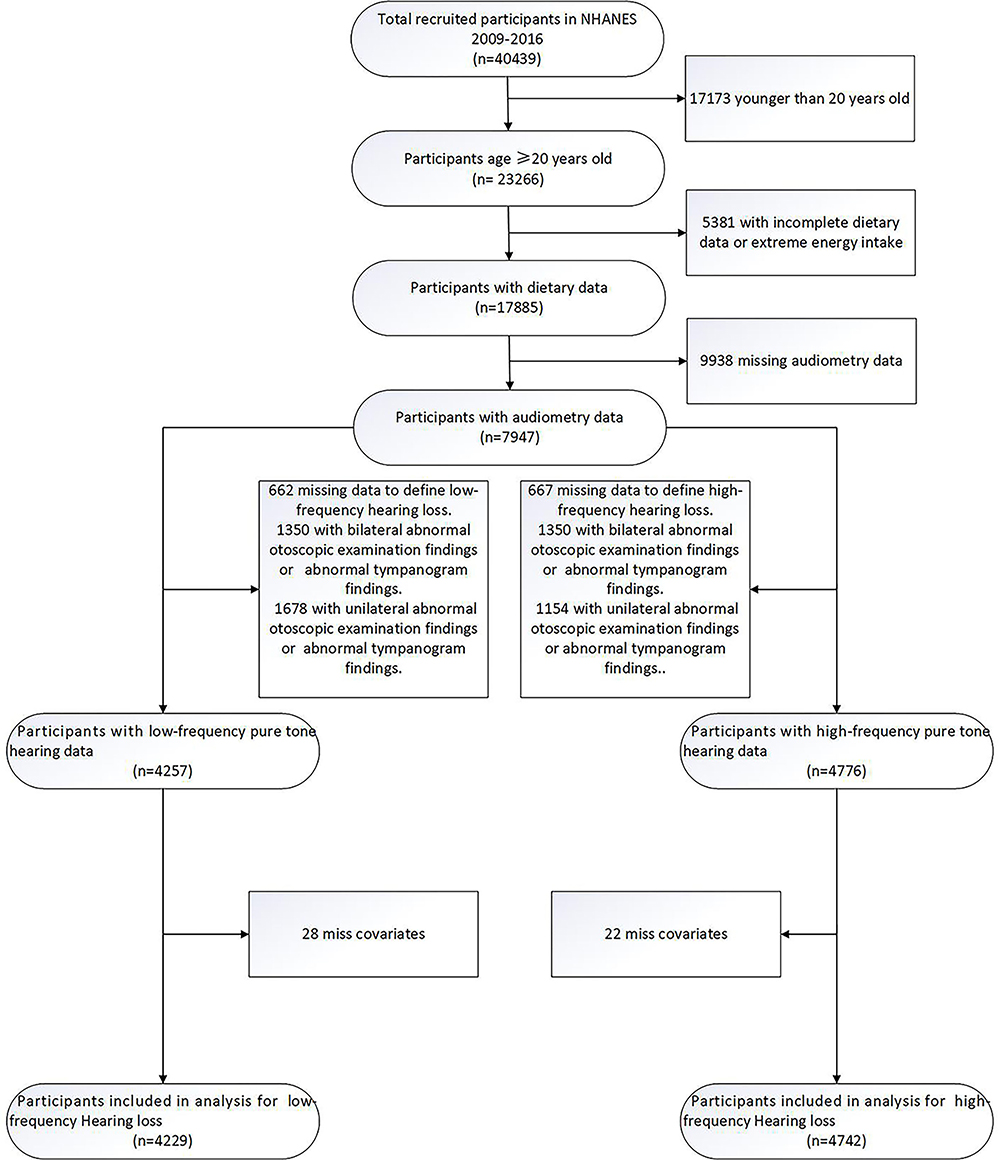 |
Figure 1 Flow diagram of analytic samples from NHANES 2009–2016. |
Association Between E-DII and Hearing Loss
Four thousand two hundred and twenty-nine participants were included in LF model. There were no significant associations between E-DII and low-frequency hearing loss (LFHL) was found in unadjusted logistic regression model and multivariable logistic regression models after adjusting for different covariates (Tables 2 and S5). In the restricted cubic spline regressions (Figure 2A–D), we found significant inverted-U associations between E-DII score and LFHL after adjusting for different covariates (Figure 2C and D), the risk of LFHL was increased before the E‐DII score was around 0.7 then decreased afterward. Then we considered the E-DII score as a categorical variable with quartiles, individuals in the lowest E-DII quartile were considered as anti-inflammatory diet, individuals in the second E-DII quartile were considered as neutral dietary pattern, participants in the third and highest E-DII quartiles were considered as weak pro-inflammatory diet and pro-inflammatory diet. To explore the inverted-U association between E-DII score and LFHL, individuals in the second E-DII quartile were set as reference. We found that, compared with individuals in the second E-DII quartile, those in the lowest E-DII quartile and the third E-DII quartile had lower clinical LFHL risk in multivariable logistic regression models after adjusting for different covariates (Figure 3B–D), those in the highest E-DII quartiles also appeared to have lower clinical LFHL risk although there is statistical significance only in unadjusted logistic regression (Figure 3A). The AIC values and Pseudo-R2 of different models are displayed in Table 3, the restricted cubic spline regression models and logistic regression models of E-DII quartiles had a smaller AIC value than the logistic regression models of continuous E-DII.
 |
Table 2 β Values of E-DII Score in Logistic Regression Models After Adjusting for Different Covariates |
 |
Table 3 AIC Values and Pseudo R2 in Different Models |
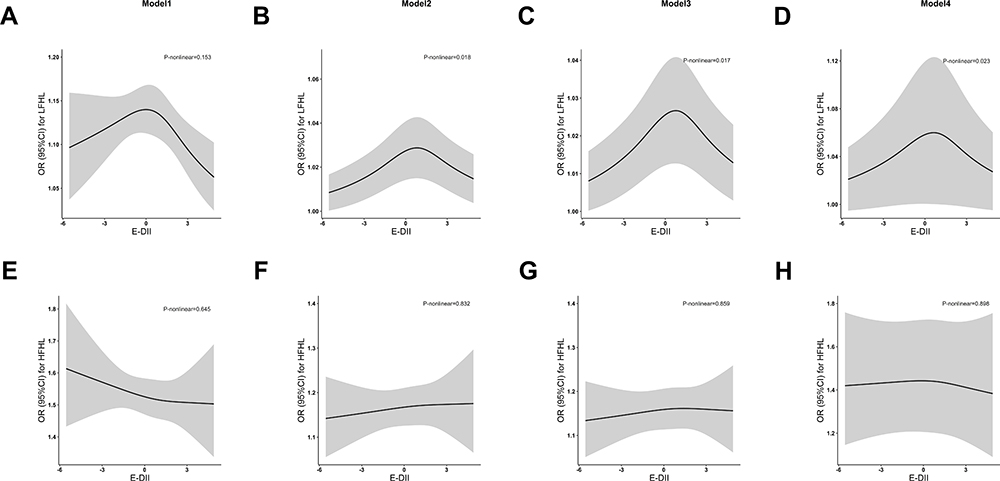 |
Figure 2 Restricted cubic spline regressions of E‐DII and the risk of HL after adjusting for different covariates: (A–D) Restricted cubic spline regression of E‐DII and the risk of LFHL in model 1, model 2, model 3, and model 4; (E–H) Restricted cubic spline regression of E‐DII and the risk of HFHL in model 1, model 2, model 3, and model 4. Model 1, unadjusted model; Model 2 adjusted for gender, age, race/ethnicity, education level and BMI; Model 3 adjusted for model 2 plus noise exposure and ototoxic drugs; Model 4 adjusted for model 3 plus hypertension, stroke, congestive heart failure, smoking status, energy intake. The black line and gray area represent the estimated OR values and their corresponding 95% Cis. P-nonlinear values are from the Wald test and adjusted by false discovery rate (FDR). |
 |
Figure 3 Forest plot of the associations between the quartiles of E‐DII and risk of HL after adjusting for different covariates: Association was deemed significant if the 95% CI does not include one; OR values were based on logistic regression models. (A) Model 1, unadjusted model; (B) Model 2, adjusted for gender, age, race/ethnicity, education level and BMI; (C) Model 3, adjusted for model 2 plus noise exposure and ototoxic drugs; (D) Model 4, adjusted for model 3 plus hypertension, stroke, congestive heart failure, smoking status, energy intake. |
Four thousand seven hundred and forty-two participants were included in HF model. Neither continuous E-DII score nor E-DII quartiles were found to be associated with high-frequency hearing loss (HFHL) in different logistic regression models and restricted cubic spline regressions (Table 2, Figures 2E–H and 3A–D).
Subgroup Analyses
There was no interaction found between E-DII and age, gender, noise exposure and ototoxic drugs in this study, but previous studies have shown that age and gender could modify the relationship between DII and hearing loss.20 When stratified by age and gender in LF model, there were no significant associations between E-DII and low-frequency hearing loss (LFHL) was found in all subgroups in multivariable logistic regression models after adjusting for all covariates (Table S6). Then we considered the E-DII score as a categorical variable with quartiles (Figure 4A–D), compared with individuals in the second E-DII quartile, those in the lowest E-DII and the third quartile had more significant lower clinical LFHL risk among middle-aged/elderly (age≥40) group and male group (Figure 4B and C), suggesting the inverted-U associations between E-DII score and LFHL could be modified by gender and age, although the interaction terms were not significant. We also performed restricted cubic spline regressions in different subgroups and the results revealed inverted-U associations between E-DII score and LFHL except for youth subgroup (age<40) (Figure S1A–D), although the association was significant only in middle-aged/elderly group (p=0.028). Moreover, we compared linear and nonlinear models, we found that nonlinear models have smaller AIC values than linear models except the young subgroup (Table S7).
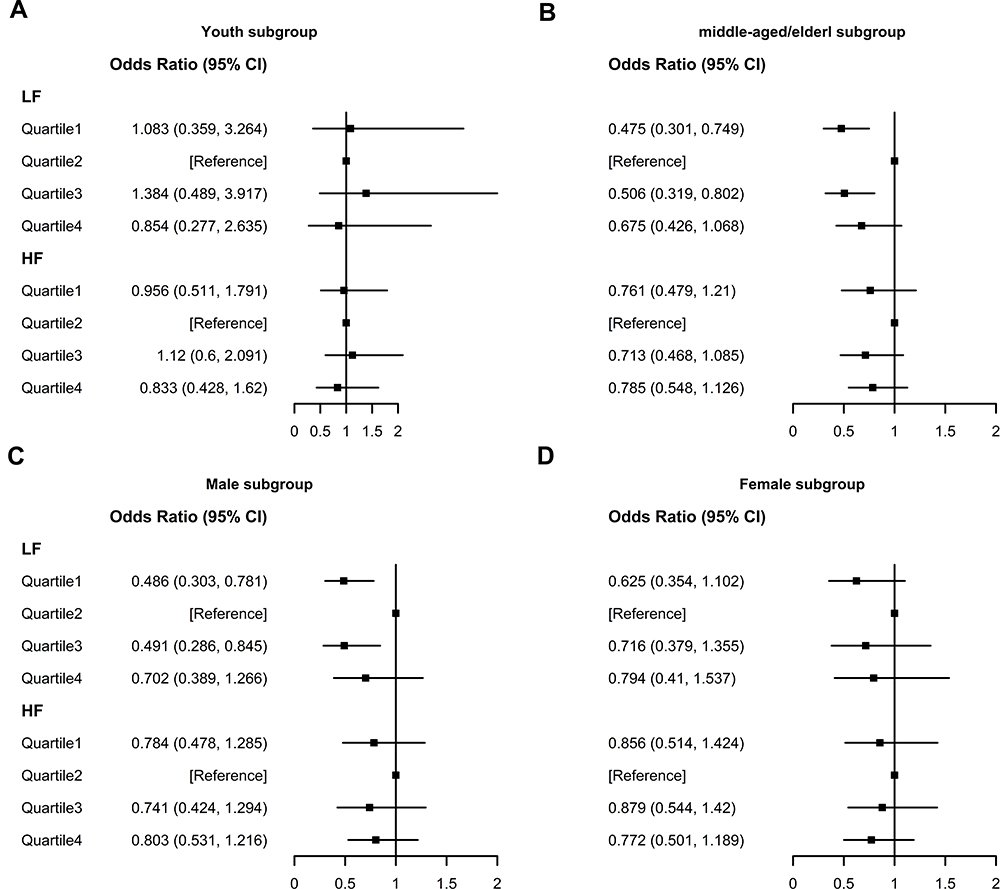 |
Figure 4 Forest plots of the associations between the quartiles of E‐DII and risk of HL in different subgroups: (A) Youth subgroup (age<40) subgroup; (B) middle-aged/elderly (age≥40) subgroup; (C) Male subgroup; (D) Female, subgroup. Association was deemed significant if the 95% CI does not include one. OR values were based on logistic regression models adjusted for age, gender, race/ethnicity, education, smoking status, energy intake, BMI, diabetes, hypertension, stroke, CHF, work-related noise exposure, firearm exposure, recreational noise exposure, use of ototoxic drug. |
There was no significant association observed between quartile or continuous E‐DII and HFHL in all subgroups (Figures 4A–D and S1E–H, Table S6). Unsignificant Inverted-U associations between E-DII score and HFHL were observed in the female group, but nonlinear models have greater AIC values than linear models in all subgroups (Table S7).
Sensitivity Analyses
We reanalyzed the data without accounting for the sampling weights by performing restricted cubic splines regression and multivariable logistic regression. Significant inverted-U associations between E-DII score and LFHL were also observed in unweighted data (p=0.015, Figure 5A). Moreover, the nonlinear model showed a better fit than the linear model (Table S7).
 |
Figure 5 Restricted cubic spline regression in unweighted data: (A) LF model; (B) HF model. The black line and gray area represent the estimated OR values and their corresponding 95% CIs; P-nonlinear values are from the Wald test and adjusted by false discovery rate (FDR). All models were adjusted for age, gender, race/ethnicity, education, smoking status, energy intake, BMI, diabetes, hypertension, stroke, CHF, work-related noise exposure, firearm exposure, recreational noise exposure, use of ototoxic drug. |
Significant linear or nonlinear association between E-DII score and HFHL was not found in unweighted data (Figure 5B, Table S6).
Discussion
To the best of our knowledge, this study is the first to investigate the association between the dietary inflammatory potential and objective HL. We utilized two 24-hour dietary recall interviews to estimate long-run average nutrient intakes and calculated E-DII score. We found that the E-DII score had a significant inverted-U relationship with the risk of LFHL. To verify the inverted-U association between the E-DII score and the risk of LFHL, subgroup analyses and sensitivity analyses were performed and showed that the fit of the nonlinear models were better than the linear models. We also explored the associations between the risk of LFHL and E‐DII quartiles and found that both pro-inflammatory diet and anti-inflammatory diet seemed to be associated with a decreased risk of LFHL compared to a diet that was neither pro-inflammatory diet nor anti-inflammatory diet especially in male and middle-age/elderly group (Figure 4B and C). However, there was no obvious association between E-DII score and HFHL found in this study.
Previous studies have associated HL with polyunsaturated fats,26–28 triglycerides29 and vitamins.30–34 Compared to single nutrient analysis, dietary patterns account for the combined effect of various foods and may have a stronger association with disease risk than for individual components.35,36 Prior studies have examined the relationship between dietary patterns and HL,13,37,38 however, these dietary patterns were not designed to explore the inflammatory potential of diets. Moreover, the results of previous studies for the relationship between inflammatory food consumption and hearing loss are inconsistent. Sardone et al found that consumption of pro-inflammatory foods with a high-sugar content was positively related with hearing loss, anti-inflammatory foods were not associated with hearing loss in a cohort of Southern Italy.39 Recently, Andreeva et al20 conducted a retrospective longitudinal study based on the French cohort to describe the relationship between inflammatory potential of the diet and subjective hearing loss, they found that less diet-related inflammation was associated with a lower risk of HL in male subgroup, but it is unexpected that DII and subjective HL were inversely associated in female subgroup. Although, they conjectured that there was a nonlinear association between the inflammatory potential of the diet and subjective hearing loss, they did not further explore the nonlinear association. Interestingly, Huang et al38 also found that higher adherence to a Mediterranean-style diet, which is considered as an anti-inflammatory diet, was positively associated with low-frequency hearing loss among middle–older aged male adults in the USA. These results may imply inflammation plays a dual role in the risk of hearing loss. In this study, the inflammatory potential of the overall diet was estimated by the E-DII score which improved prediction in comparison to unadjusted DII score,23 after adjusting for covariates, we observed the inverted-U association between E-DII score and LFHL, which did not be modified by subgroup analyses and sensitivity analyses obviously. But there was no significant linear or nonlinear relationship between E-DII score and HFHL after adjusting for covariates. According to traveling wave theory, Basal regions of the cochlea perceive high frequency sound wave and apical regions of the cochlea perceive low frequency sound wave, our results may suggest that the inflammatory potential of diets have a greater effect on apical regions of the cochlea, which merit further exploration in the future.
Chronic inflammation might alter brain neurotropism and further affect the function of the auditory cortex and the hippocampus, which may promote hearing loss and cognitive decline.40 A recent study has associated age-related hearing Loss with cognitive frailty, which may imply that systemic inflammation was the common mechanisms of age-related hearing loss and cognitive frailty.41 Experimental studies of inner ear inflammation have revealed the production of TNF-α, IL-1β, and IL-6 in the cochlea and synergic leukocyte infiltration.42 Disrupted vascular integrity in the stria vascularis and disturbed endolymph ion homeostasis are hypothesized to be associated with hearing loss induced by inflammatory factors.43 Animal model investigations have shown that blockage of the cytokine IL-6 pathway could improve hearing after noise exposure.44 Aspirin, a weak anti-inflammatory agent, has been shown to be protective against aminoglycoside-induced or cisplatin-induced hearing loss through anti-inflammatory mechanisms.45 However, there is conflicting evidence about aspirin’s effect on hearing, research also reported that long-term use of aspirin was associated with an increase in hearing loss.46,47 Rapid increases in our understanding that nutrition influences inflammatory and immune responses have led to the development of DII24 This analysis extends evidence about the association of inflammatory potential of the diet with hearing impairment.
Our study has several strengths. First, hearing loss has been measured using objectively measured audiometry assessments in our study, which was considered as a gold standard.48 Second, nutrient intakes were assessed using two 24-h dietary recalls, which could estimate long-run average nutrient intakes.
Several limitations of this analysis should be considered. First, subjective measure error and diet-associated recall bias are inevitable in a questionnaire study. Second, the E‐DII score was calculated based on 27 of 45 food parameters, which may affect the findings in this study. However, the previous study has shown that there was no change in the predictive ability of the E‐DII food parameters available in NHANES data to evaluate inflammation compared with the full list.49 Thirdly, individuals with monogenic non-syndromic mutations were not identified in this study, which may exert a mediation effect or interaction effect in the relationship between the E-DII and hearing loss. Furthermore, a large proportion of NHANES participants have been excluded from the analyses, which led to the population included in this study may not be nationally representative. Finally, it is impossible to deduce causal relationships between E-DII and HL due to the cross-sectional nature of our analyses. The possibility of reverse causality cannot be dismissed, such as hearing loss can lead to symptoms of depression and social isolation, which may have an effect on diet.
Conclusion
In summary, E-DII score had inverted-U relationship with LFHL, the risk of LFHL approach highest when the E-DII score was around 0.7. This inverted-U relationship may suggest that inflammation has a dual effect on the risk of LFHL, both anti-inflammation and pro-inflammation associated with lower risk of LFHL, which could partly explain the inconsistent results of previous studies and require further research. Moreover, the association between E-DII score and HFHL was not found, which may imply that the inflammatory potential of diets had a greater effect on apical regions of the cochlea than basal regions of the cochlea. The exact reaction mechanism of the relationship between inflammatory potential of diets and HL requires further analysis.
Ethical Statement
The study was approved by the Second Affiliated Hospital of Nanchang University Medical Research Ethics Committee (No. Review [2021] No. (006)) (Supplementary Material 10).
Author Contributions
Contributions: (I) Conception and design: All authors; (II) Administrative support: Yuehui Liu; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: Yanpeng Fu; (V) Data analyses and interpretation: Yanpeng Fu. (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Chadha S, Cieza A. World Health Organization and its initiative for ear and hearing care. Otolaryngol Clin North Am. 2018;51(3):535–542. doi:10.1016/j.otc.2018.01.002
2. Chadha S, Lopez L, Agarwal P, et al. Global Costs of Unaddressed Hearing Loss and Costs-Effectiveness of Interventions. A WHO Report. WHO Offset Publication; 2017.
3. Hoffmann TJ, Keats BJ, Yoshikawa N, et al. A large genome-wide association study of age-related hearing impairment using electronic health records. PLoS Genet. 2016;12(10):e1006371. doi:10.1371/journal.pgen.1006371
4. Spankovich C, Le Prell CG. Healthy diets, healthy hearing: national health and nutrition examination survey, 1999–2002. Int J Audiol. 2013;52(6):369–376. doi:10.3109/14992027.2013.780133
5. Shi X. Pathophysiology of the cochlear intrastrial fluid-blood barrier (review). Hear Res. 2016;338:52–63. doi:10.1016/j.heares.2016.01.010
6. Gupta S, Curhan SG, Curhan GC. Biomarkers of systemic inflammation and risk of incident hearing loss. Ear Hear. 2019;40(4):981–989. doi:10.1097/AUD.0000000000000678
7. Nash SD, Cruickshanks KJ, Zhan W, et al. Long-term assessment of systemic inflammation and the cumulative incidence of age-related hearing impairment in the epidemiology of hearing loss study. J Gerontol a Biol Sci Med Sci. 2014;69(2):207–214. doi:10.1093/gerona/glt075
8. Galland L. Diet and inflammation. Nutr Clin Pract. 2010;25(6):634–640. doi:10.1177/0884533610385703
9. Esposito K, Marfella R, Ciotola M, et al. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA. 2004;292(12):1440–1446. doi:10.1001/jama.292.12.1440
10. Chrysohoou C, Panagiotakos DB, Pitsavos C, et al. Adherence to the Mediterranean diet attenuates inflammation and coagulation process in healthy adults: the ATTICA Study. J Am Coll Cardiol. 2004;44(1):152–158.
11. Neale EP, Batterham MJ, Tapsell LC. Consumption of a healthy dietary pattern results in significant reductions in C-reactive protein levels in adults: a meta-analysis. Nutr Res. 2016;36(5):391–401. doi:10.1016/j.nutres.2016.02.009
12. Curhan SG, Wang M, Eavey RD, et al. Adherence to healthful dietary patterns is associated with lower risk of hearing loss in women. J Nutr. 2018;148(6):944–951. doi:10.1093/jn/nxy058
13. Lampignano L, Quaranta N, Bortone I, et al. Dietary habits and nutrient intakes are associated to age-related central auditory processing disorder in a cohort from Southern Italy. Front Aging Neurosci. 2021;13:629017. doi:10.3389/fnagi.2021.629017
14. Choi JE, Ahn J, Moon IJ. Associations between Age-related hearing loss and dietary assessment using data from Korean National Health andNutrition Examination Survey. Nutrients. 2021;13(4):1230. doi:10.3390/nu13041230
15. Shivappa N, Steck SE, Hurley TG, et al. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
16. Laouali N, Mancini FR, Hajji-Louati M, et al. Dietary inflammatory index and type 2 diabetes risk in a prospective cohort of 70,991 women followed for 20 years: the mediating role of BMI. Diabetologia. 2019;62(12):2222–2232. doi:10.1007/s00125-019-04972-0
17. Kim H-Y, Lee J, Kim J. Association between dietary inflammatory index and metabolic syndrome in the General Korean population. Nutrients. 2018;10(5):648.
18. Khan I, Kwon M, Shivappa N, et al. Positive association of dietary inflammatory index with incidence of cardiovascular disease: findings from a Korean population-based prospective study. Nutrients. 2020;12(2):588. doi:10.3390/nu12020588
19. Mazidi M, Shivappa N, Wirth MD, et al. Greater Dietary Inflammatory Index score is associated with higher likelihood of chronic kidney disease. Br J Nutr. 2018;120(2):204–209. doi:10.1017/S0007114518001071
20. Andreeva VA, Péneau S, Julia C, et al. The inflammatory potential of the diet is prospectively associated with subjective hearing loss. Eur J Nutr. 2021;60(7):3669–3678. doi:10.1007/s00394-021-02531-1
21. Shin D, Hur J, Cho E-H, et al. Pre-pregnancy body mass index is associated with dietary inflammatory index and C-reactive protein concentrations during pregnancy. Nutrients. 2017;9(4):351. doi:10.3390/nu9040351
22. World Health Organization. WHO | Deafness and hearing loss. World Health Organization. 2013.
23. Hébert JR, Shivappa N, Wirth MD, et al. Perspective: the dietary inflammatory index (DII)-lessons learned, improvements made, and future directions. Adv Nutr. 2019;10(2):185–195. doi:10.1093/advances/nmy071
24. Lanvers-Kaminsky C, Zehnhoff-Dinnesen AA, Parfitt R, et al. Drug-induced ototoxicity: mechanisms, Pharmacogenetics, and protective strategies. Clin Pharmacol Ther. 2017;101(4):491–500. doi:10.1002/cpt.603
25. Akaike H, Petrov BN, Czaki F Information theory and an extension of the maximum likelihood principle.
26. Gopinath B, Flood VM, Rochtchina E, et al. Consumption of omega-3 fatty acids and fish and risk of age-related hearing loss. Am J Clin Nutr. 2010;92(2):416–421. doi:10.3945/ajcn.2010.29370
27. Dullemeijer C, Verhoef P, Brouwer IA, et al. Plasma very long-chain n-3 polyunsaturated fatty acids and age-related hearing loss in older adults. J Nutr Health Aging. 2010;14(5):347–351. doi:10.1007/s12603-010-0078-x
28. Curhan SG, Eavey RD, Wang M, et al. Fish and fatty acid consumption and the risk of hearing loss in women. Am J Clin Nutr. 2014;100(5):1371–1377. doi:10.3945/ajcn.114.091819
29. Gopinath B, Flood VM, Teber E, et al. Dietary intake of cholesterol is positively associated and use of cholesterol-lowering medication is negatively associated with prevalent age-related hearing loss. J Nutr. 2011;141(7):1355–1361. doi:10.3945/jn.111.138610
30. Durga J, Verhoef P, Anteunis LJC, et al. Effects of folic acid supplementation on hearing in older adults: a randomized, controlled trial. Ann Intern Med. 2007;146(1):1–9. doi:10.7326/0003-4819-146-1-200701020-00003
31. Gopinath B, Flood VM, Rochtchina E, et al. Serum homocysteine and folate concentrations are associated with prevalent age-related hearing loss. J Nutr. 2010;140(8):1469–1474. doi:10.3945/jn.110.122010
32. Choi Y-H, Miller JM, Tucker KL, et al. Antioxidant vitamins and magnesium and the risk of hearing loss in the US general population. Am J Clin Nutr. 2014;99(1):148–155. doi:10.3945/ajcn.113.068437
33. Curhan SG, Stankovic KM, Eavey RD, et al. Carotenoids, vitamin A, vitamin C, vitamin E, and folate and risk of self-reported hearing loss in women. Am J Clin Nutr. 2015;102(5):1167–1175. doi:10.3945/ajcn.115.109314
34. Szeto B, Valentini C, Lalwani AK. Low vitamin D status is associated with hearing loss in the elderly: a cross-sectional study. Am J Clin Nutr. 2021;113(2):456–466. doi:10.1093/ajcn/nqaa310
35. Gao X, Chen H, Fung TT, et al. Prospective study of dietary pattern and risk of Parkinson disease. Am J Clin Nutr. 2007;86(5):1486–1494. doi:10.1093/ajcn/86.5.1486
36. Dawes P, Cruickshanks KJ, Marsden A, et al. Relationship between diet, tinnitus, and hearing difficulties. Ear Hear. 2020;41(2):289–299. doi:10.1097/AUD.0000000000000765
37. Suzuki K, Kaneko M, Murai K. Influence of serum lipids on auditory function. Laryngoscope. 2000;110(10 Pt 1):1736–1738. doi:10.1097/00005537-200010000-00033
38. Huang Q, Jin Y, Reed NS, et al. Diet quality and hearing loss among middle-older aged adults in the USA: findings from National Health and Nutrition Examination Survey. Public Health Nutr. 2020;23(5):812–820. doi:10.1017/S1368980019002970
39. Sardone R, Lampignano L, Guerra V, et al. Relationship between inflammatory food consumption and age-related hearing loss in a prospective observational cohort: results from the Salus in Apulia Study. Nutrients. 2020;12(2):426. doi:10.3390/nu12020426
40. Calsolaro V, Edison P. Neuroinflammation in Alzheimer’s disease: current evidence and future directions. Alzheimers Dement. 2016;12:719–732. doi:10.1016/j.jalz.2016.02.010
41. Sardone R, Castellana F, Bortone I, et al. Association between central and peripheral age-related hearing loss and different frailty phenotypes in an older population in Southern Italy. JAMA Otolaryngol Head Neck Surg. 2021;147:561–571. doi:10.1001/jamaoto.2020.5334
42. Hashimoto S, Billings P, Harris JP, et al. Innate immunity contributes to cochlear adaptive immune responses. Audiol Neurootol. 2005;10(1):35–43. doi:10.1159/000082306
43. Zhang J, Chen S, Hou Z, et al. Lipopolysaccharide-induced middle ear inflammation disrupts the cochlear intra-strial fluid-blood barrier through down-regulation of tight junction proteins. PLoS One. 2015;10(3):e0122572. doi:10.1371/journal.pone.0122572
44. Wakabayashi K, Fujioka M, Kanzaki S, et al. Blockade of interleukin-6 signaling suppressed cochlear inflammatory response and improved hearing impairment in noise-damaged mice cochlea. Neurosci Res. 2010;66(4):345–352. doi:10.1016/j.neures.2009.12.008
45. Sha S-H, Qiu J-H, Schacht J. Aspirin to prevent gentamicin-induced hearing loss. N Engl J Med. 2006;354(17):1856–1857. doi:10.1056/NEJMc053428
46. Curhan SG, Eavey R, Shargorodsky J, et al. Analgesic use and the risk of hearing loss in men. Am J Med. 2010;123(3):231–237. doi:10.1016/j.amjmed.2009.08.006
47. Zolot J. Long-term NSAIDs and acetaminophen linked to hearing loss in women. Am J Nurs. 2017;117(4):16. doi:10.1097/01.NAJ.0000527472.38965.1f
48. Kiely KM, Gopinath B, Mitchell P, et al. Evaluating a dichotomized measure of self-reported hearing loss against gold standard audiometry: prevalence estimates and age bias in a pooled national data set. J Aging Health. 2012;24(3):439–458. doi:10.1177/0898264311425088
49. Shivappa N, Wirth MD, Hurley TG, et al. Association between the dietary inflammatory index (DII) and telomere length and C-reactive protein from the National Health and Nutrition Examination Survey-1999–2002. Mol Nutr Food Res. 2017;61(4):1600630. doi:10.1002/mnfr.201600630
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.