")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
The Impact of Recent Life Events, Internalizing Symptoms, and Emotion Regulation on the Severity of Non-Suicidal Self-Injury in Adolescents: A Mediation Analysis
Authors Zhou L, Qiao C, Huang J, Lin J, Zhang H, Xie J, Yuan Y , Hu C
Received 14 October 2023
Accepted for publication 22 February 2024
Published 29 February 2024 Volume 2024:20 Pages 415—428
DOI https://doi.org/10.2147/NDT.S444729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Linqi Zhou,1 Changyuan Qiao,1 Jialing Huang,2 Jian Lin,2 Haisheng Zhang,2 Jian Xie,2 Yonggui Yuan,3 Changchun Hu2
1School of the Fourth Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Clinical Psychology, Affiliated Hangzhou First People’s Hospital, Westlake University School of Medicine, Hangzhou, People’s Republic of China; 3Department of Psychosomatics and Psychiatry, Zhong Da Hospital, School of Medicine, Southeast University, Nanjing, People’s Republic of China
Correspondence: Changchun Hu, Department of Clinical Psychology, Affiliated Hangzhou First People’s Hospital, Westlake University School of Medicine, No. 261 Huansha Road, Shangcheng District, Hangzhou, 310002, People’s Republic of China, Tel +86-571-56006902, Email [email protected]
Background: Previous studies have demonstrated a strong association between recent stressful life events and non-suicidal self-injury (NSSI) among adolescents. Internalizing symptoms and difficulty in emotion regulation (DER) may mediate this relationship. This study aimed to investigate the relationship between recent stressful life events and NSSI severity in adolescents and the potential moderating role of internalizing symptoms and DER.
Methods: A total of 224 adolescent inpatients (78.6% female) participated in the study, with an age range of 12– 18 years old. Data on recent stressful life events, internalizing symptoms, DER, and NSSI behaviors were collected using a clinician-rated questionnaire. A structural equation model was used to test the hypothesized model.
Results: The rate of NSSI reporting among adolescents in the past 12 months was 65.18%. Recent stressful life events were found to be directly associated with NSSI severity (β = 0.128, P = 0.023). A chain-mediating effect between recent stressful life events and NSSI was also confirmed (β = 0.034, P = 0.023), with DER and internalizing symptoms playing a chain-mediating role and DER having a significantly indirect association with NSSI through internalizing symptoms.
Conclusion: Recent stressful life events appear to play a role in the etiology of NSSI, particularly punishment and interpersonal relationship events that warrant special attention. DER and internalizing symptoms play a chain-mediating role in the relationship between life events and NSSI. Reducing recent stressful life events, screening for internalizing symptoms, and improving emotion regulation may decrease NSSI behavior among adolescents.
Keywords: non-suicidal self-injury, adolescents, recent stressful life events, internalizing symptoms, difficulty in emotion regulation, structural equation model
Introduction
Non-suicidal self-injury (NSSI) is the deliberate, self-directed damage of body tissue without suicidal intent and for purposes not socially or culturally sanctioned.1 In this study, we primarily focus on direct forms of NSSI, which include but are not limited to behaviors such as cutting, burning, and hitting.2 NSSI is prevalent among adolescents worldwide and is more common in this age group than in others.3 Longitudinal studies have shown that the overall lifetime prevalence of NSSI among adolescents is approximately 19.4–26.7%.4 The typical age of onset for NSSI is 12–14 years old and peaks in mid-adolescence.5 Although NSSI usually does not result in serious medical outcomes, it often occurs repeatedly and increases the risk of fatal outcomes. NSSI has been associated with various psychiatric disorders and a range of internalizing and externalizing disorders.6 It is also one of the strongest predictors of suicidal ideation, suicide attempts, and suicide death.7,8 Due to its high incidence, recurrent behavior, and long-term clinical risk, NSSI among adolescents has received increasing attention as an important public health issue. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has established separate diagnostic criteria for NSSI for the first time9. However, NSSI remains poorly understood and it is difficult for clinicians to accurately predict and prevent these behaviors.10 Given its significance as a public health issue, identifying the factors contributing to NSSI among adolescents is a research priority.
One area that has garnered attention as a possible factor contributing to NSSI is the impact of recent stressful life events. Studies have shown that recent stressful life events are strongly associated with NSSI among adolescents,11–13 and can be conceptualized as a proximal risk factor for NSSI.14,15 Stressful life events refer to negative events encountered by individuals, often resulting from changes in family, work, or academic environments.16 These events can lead to negative psychological and physiological outcomes and serve as psychological social stressors.17 Stress from recent life events may play a unique role in the occurrence of NSSI; individuals with higher levels of life stress are more likely to engage in NSSI behaviors.11,13 This is consistent with the stress-diathesis model,18 which suggests that experiencing a higher proportion of life stress increases the risk of subsequent NSSI. Many previous studies have discussed the role of recent stressful life events in the development of NSSI among adolescents; Adolescents who engage in NSSI experience more recent negative life events than their peers.19 Furthermore, the higher the incidence of stressful life events, the more severe NSSI,20,21 indicating a cumulative effect. Several longitudinal studies have confirmed that stressful life events experienced by adolescents predict the occurrence of NSSI.14,15,22 Other studies have specifically pointed out that interpersonal stress resulting from negative life events is strongly associated with adolescent NSSI.23 However, despite considerable interest in the association between life events and NSSI among adolescents, the specific mechanisms of action have not been thoroughly investigated.
Difficulty in emotion regulation (DER) may serve as an important mediating factor between recent stressful life events and NSSI. DER has been widely reported in individuals experiencing life events.12,24 At the same time, it has been confirmed that there is a correlation between DER and NSSI; Emotional regulation may play a role in the initiation and maintenance of NSSI,25 and certain patterns of emotion regulation may modulate the therapeutic response to NSSI.26 According to Nock’s theoretical model,27 adolescents may experience physiological hyperarousal when confronted with stressful life events. In such situations, NSSI may be used as a stress regulation strategy due to DER.28 Self-injury is often defined as a maladaptive method of emotion regulation; Empirical studies have shown that in the absence of other emotion regulation strategies, the primary reason for individuals to participate in NSSI is to reduce emotional distress triggered by stressful life events.29 Moreover, high-frequency NSSI signifies a greater number of negative life events, poor coping and emotion regulation deficits.30 In addition to being associated with NSSI and life events, DER is also associated with Internalizing symptoms. Emotional dysregulation predicts subsequent internalizing symptoms among adolescents.31 When faced with stressful life events, individuals with difficulty in emotion regulation may be unable to tolerate distressing feelings and are more likely to internalize their distress.32
Internalizing symptoms may serve as another important mediating factor between recent stressful life events and NSSI. Internalizing symptoms refer to the inward transformation of distress, and often include depression, anxiety, physical discomfort, and suicidal ideation among adolescents.33 The most common internalizing symptoms associated with NSSI are depression and anxiety.34 Depression is a significant risk factor for the development of self-injury and may predict future NSSI behavior.35 Hankin et al14 found that depressive symptoms positively predicted self-injury behavior over the next two years, while Guerry et al20 found that depression scores were the only significant predictor of change in the frequency of late NSSI. Anxiety symptoms also increase the risk of NSSI, especially when they co-occur with depressive symptoms.36,37 Additionally, individuals who experience more life events exhibit higher levels of anxiety and depression, which in turn predict NSSI.38–40
Previous research has consistently shown a strong association between recent stressful life events and NSSI among adolescents.11–13 However, the mechanisms through which life events contribute to NSSI remain poorly understood. Given the relevance of DER and internalizing symptoms in the literature,28–31,34–40 we anticipate that these factors may serve as mediators in the relationship between recent stressful life events and NSSI. Therefore, our study aims to explore multiple facets of this relationship. Firstly, we hypothesize that recent stressful life events will have a direct association with NSSI. Secondly, we propose that DER and internalizing symptoms will mediate the relationship between recent stressful life events and NSSI. Finally, we expect a chain mediation effect, where recent stressful life events will be associated with NSSI through a pathway involving both DER and internalizing symptoms. Understanding these pathways would not only contribute to the existing literature but also provide actionable insights for early prevention and intervention strategies targeting adolescents at risk of engaging in NSSI.
This study used structural equation model (SEM) to examine multiple relationships between recent stressful life events, DER, internalizing symptoms, and NSSI. Firstly, we tested the direct association between recent stressful life events and NSSI. Secondly, we tested the mediating effect of DER and internalizing symptoms. Finally, we further tested the chain mediating effect of DER and internalizing symptoms from recent stressful life events to NSSI. At the same time, we estimated each direct or indirect pathway to determine its effect size in explaining the association between recent stressful life events and NSSI.
Materials and Methods
Participants
A total of 245 adolescent inpatients from the Affiliated Hangzhou First People’s Hospital of Westlake University in Hangzhou, China, participated in our study. The recruitment period lasted more than 2 years from August 2019 to November 2021. Twenty-one participants were excluded because they did not complete the questionnaire. Ultimately, 224 participants were included in the current analysis. Utilizing the G-power tool,41 our study determined a minimum required sample size of 207 and accordingly included 224 samples, thereby ensuring robustness for our structural equation modeling. In this study sample, the mean age of the participants was 15.30 years old (SD=1.83, range: 12–18 years old) and the mean years of education were 9.54 years (SD=1.97, range: 6–13 years), of which 176 (78.6%) were female and 48 (21.4%) were male. Approximately 31.2% of the sample had more than one diagnosis, including depressive disorder (72.3%), anxiety disorder (18.8%), and trauma and stressor-related disorder (18.8%).
Procedure
Two experienced clinical psychiatrists conducted the interviews independently. Diagnoses were established based on the DSM-5 criteria. Exclusion criteria were a current or past diagnosis of schizophrenia spectrum disorder, mental retardation, or severe cognitive impairment. After receiving a thorough explanation of the study, both eligible participants and their guardians provided written informed consent. Upon providing informed consent, participants completed a detailed assessment questionnaire to collect demographic information and data on recent stressful life events, DER, and internalizing symptoms. Upon admission, clinical doctors assessed the severity of NSSI behaviors using the Clinician-Rated Severity of Non-Suicidal Self-Injury (CRSNSSI-DSM-5) during structured interviews.
The study was conducted by the Declaration of Helsinki and approved by the ethics committee of Hangzhou First People’s Hospital, affiliated with West Lake University School of Medicine (IRB: 2020-K008–01, January 2020). The parent or legal guardian provided written informed consent to participate in this study, with the assent of the adolescents.
Measurement Tools
Recent Stressful Life Events
Adolescent Self-Rating Life Events Checklist (ASLEC)
For example, one item assessing recent life events asked: “In the past year, have you experienced a significant family conflict?”
The ASLEC developed by Liu et al17 was used to measure recent negative life events in adolescents. The scale consists of 27 items covering 5 dimensions related to life events: interpersonal relationship factor (IRF), learning pressure factor (LPF), punishment factor (PF), loss factor (LF), and health adaptation factor (HAF), and was used to assess the social and psychological stress of adolescents during the last 12 months. For each item, participants first judge whether the event occurs or not. If it had occurred, it was categorized into five levels (1 = no effect, 2 = mild, 3 = moderate, 4 = severe, 5 = extremely severe) based on the psychological feelings at the time of the event. The higher total score on the scale indicates that the life events experienced have a greater impact on the adolescent and a greater overall stress level. The ASLEC has been reported to have good psychometric properties, good validity, and strong pertinence for adolescents. In this study, the Cronbach coefficient alpha was 0.901.
Internalizing Symptoms
Patient Health Questionnaire-9 (PHQ-9)
An example item used to assess the severity of depressive symptoms is: “Feeling down, depressed, or hopeless”.
The PHQ-9 is a simple and efficient self-assessment tool for depression developed by Kroenke K et al42 based on the American Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). The scale consists of 9 items that assess the frequency of 9 depressive symptoms occurring over the past 2 weeks, with scores ranging from 0 (not at all) to 3 (nearly every day). The higher the total score, the more severe the depressive symptoms reflected. The Chinese version of the PHQ-9 has demonstrated good reliability and validity in the assessment of adolescent depression emotions.43 In this study, the Cronbach coefficient alpha was 0.886.
General Anxiety Disorder-7 (GAD-7)
An example item used to assess the severity of anxiety symptoms is: “Feeling nervous, anxious or on edge”.
The GAD-7 is a brief self-rating scale of anxiety symptoms developed by Spitzer RL et al44 based on the diagnostic criteria of the American Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). The scale consists of 7 items that assess the frequency of 7 anxiety symptoms occurring over the past 2 weeks, with items ranging from 0 (not at all) to 3 (nearly every day). Both national and international studies have shown that the GAD-7 has high reliability and validity for screening anxiety.45,46 In this study, the Cronbach coefficient alpha was 0.906.
Difficulty in Emotion Regulation
Difficulties with Emotion Regulation Scale (DERS)
An example item from the DER scale is: “When I’m upset, I lose control over my behaviors”.
The DERS47 is a self-reported measurement tool consisting of 36 items used to assess clinical difficulties with emotion regulation. The scale can be divided into 6 dimensions: non-acceptance of emotional responses, difficulty engaging in goal-directed behaviors, difficulty with impulse control, limited self-perceived access to strategies, lack of emotional awareness, and lack of emotional clarity. All 36 items are scored using a 5-point Likert scale ranging from 1 (rarely) to 5 (almost always), with higher scores indicating greater difficulty in emotion regulation. The Chinese version of the DERS has been widely used. In this study, the Cronbach coefficient alpha was 0.957.
Non-Suicidal Self-Injury
Clinician-Rated Severity of Non-Suicidal Self-Injury (CRSNSSI)
An example item used to assess the severity of NSSI is: “How often have you engaged in self-injury without suicidal intent in the past six months?”
NSSI in the clinical setting was measured by a structured interview designed for this study. The Clinician-Rated Severity of Non-Suicidal Self-Injury measure was developed by the American Psychiatric Association to assess the severity of non-suicidal self-injury behaviors. The scale is divided into 5 levels (0 = none; 1 = subthreshold; 2 = mild; 3 = moderate; 4 = severe) based on the severity of non-suicidal self-injury behaviors experienced by an individual within the past 12 months.48 Higher total scores indicate more severe non-suicidal self-injury behaviors among adolescents.
Statistical Analysis
Firstly, we performed descriptive statistics and correlation analysis of all study variables using SPSS 25.0. Next, we performed a structural equation modeling test of the hypothesized mediation model using Amos 26.0. Emotional awareness and emotional clarity were found to have no significant effect in this model, so they were removed from the mediation analysis. In this model, recent stressful life events (represented by ASLEC score; composed of five dimensions: IRF, LPF, PF, LF and HAF) were used as independent variables, DER (represented by DERS total score) and internalizing symptoms (represented by PHQ-9 and GAD-7 scores) as mediating variables, the NSSI severity as an outcome variable, and gender as a covariate. Finally, we used 5000 iterations of bootstrapping to test the significance of each direct pathway and indirect pathway. The method produced a 95% bias-corrected confidence interval (CI) by resampling 5000 data points. If the 95% CI did not include zero, the effect was considered significant. Previous studies have shown that the model is considered to be a good fit when χ2/df < 5, CFI > 0.90, TLI > 0.90, and RMSEA < 0.08.49
Results
Descriptive Statistics of the Variables
Table 1 presents the demographic characteristics among the 224 participating adolescents, who had a mean age of 15.30 years (Standard Deviation, SD = 1.83). The sample was predominantly female (78.6%), with males making up 21.4%. The participants had an average of 9.54 years of education (SD = 1.97).
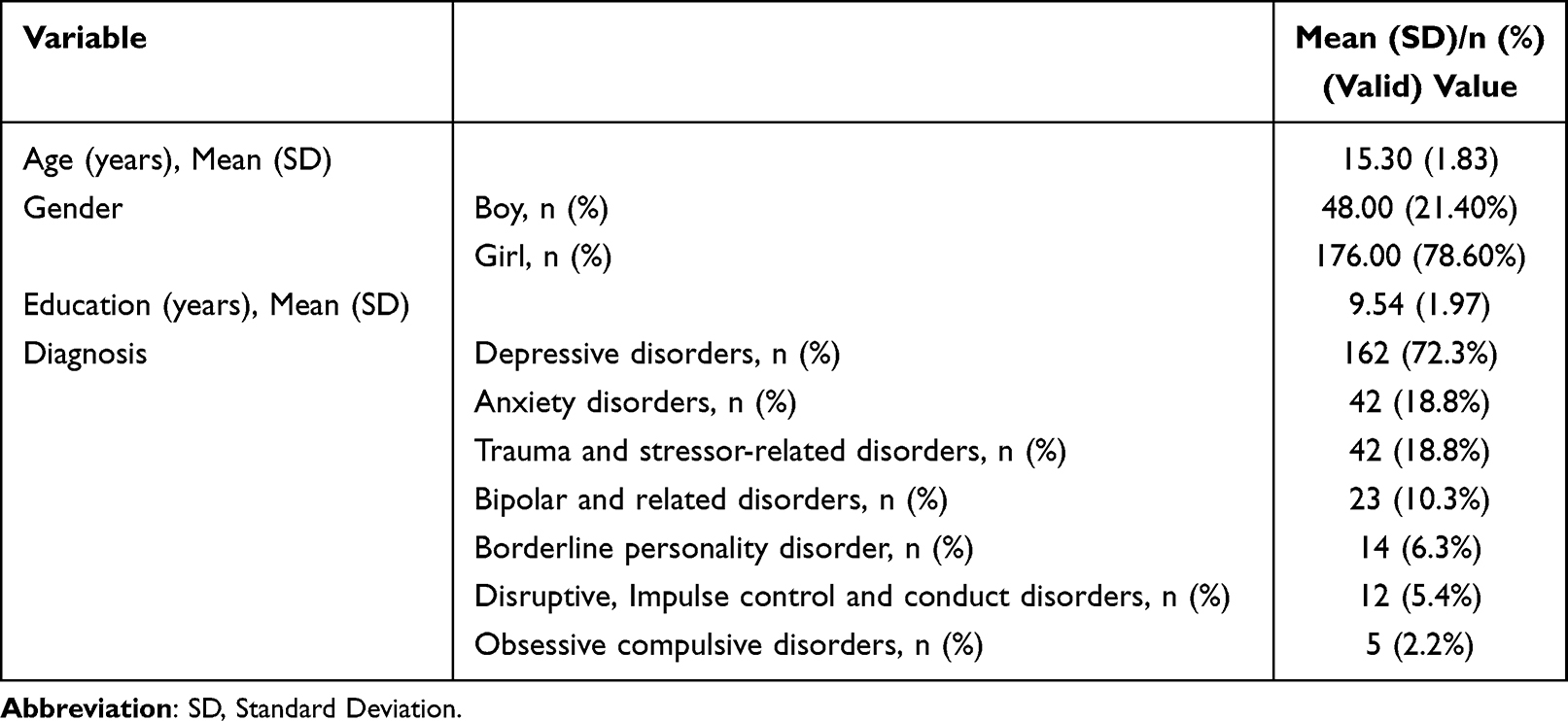 |
Table 1 Demographic Characteristics of Study Participants (n = 224) |
Table 2 presents the descriptive statistics for all study variables of study participants. In the DERS measure, the dimension of emotion regulation with the highest mean score was “Self-Perceived Limited Access to Strategies”. The dimension of “Impulse Control Difficulties” had the second-highest mean score. In the ASLEC measure, the dimension with the highest mean score was “Punishment”, followed by “Health Adaptation”. The mean score (SD) for the PHQ-9 was 18.33 (5.45), and for the GAD-7, it was 13.55 (4.79). Out of the total sample, 174 adolescents (77.67%) reported engaging in NSSI during the past year, and 103 adolescents (46.0%) met the DSM-5 diagnostic criteria for NSSI.
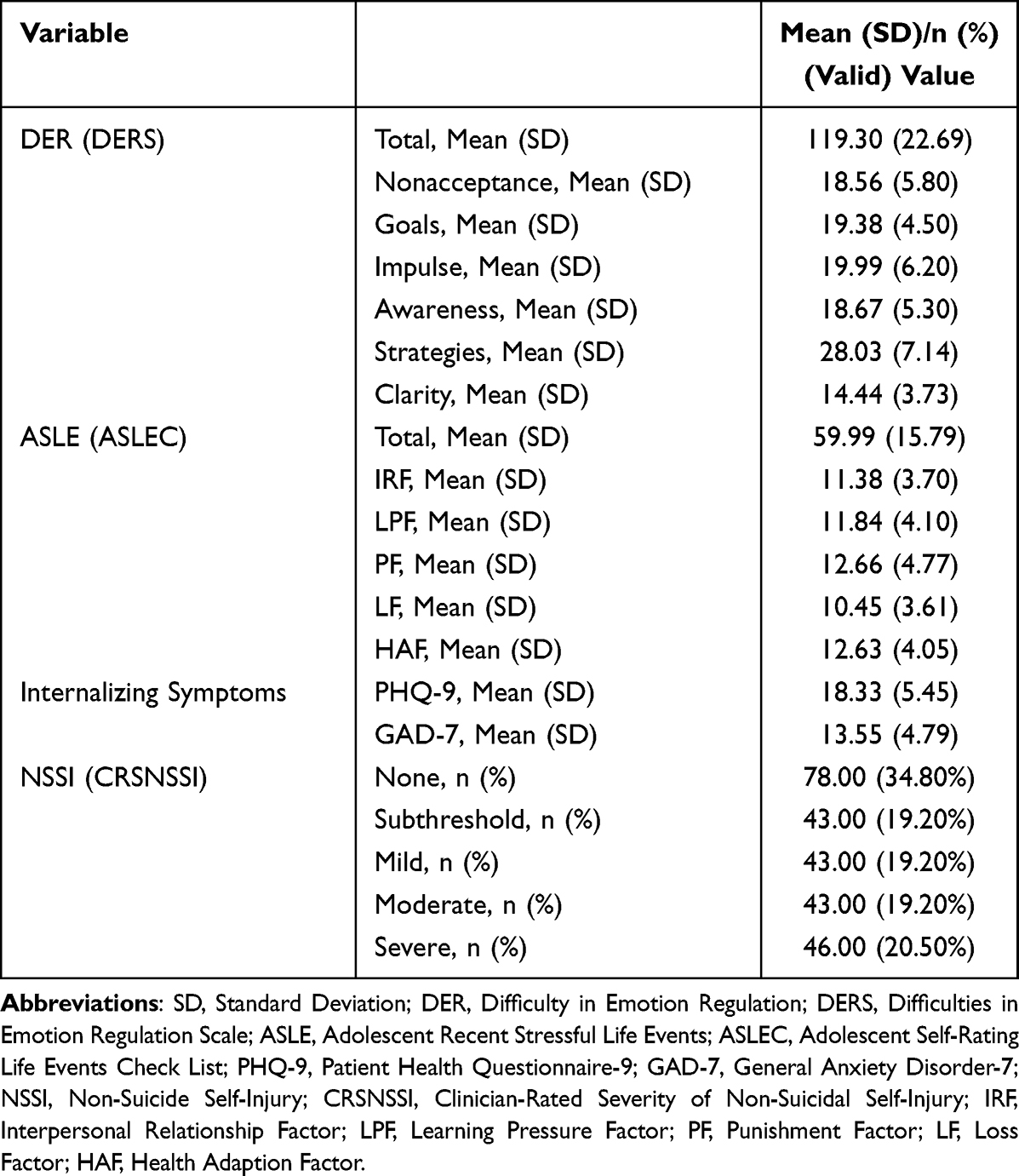 |
Table 2 Descriptive Statistics for All Study Variables of Study Participants (n = 224) |
Correlation Analyses of the Variables
Table 3 displays the correlations among the key variables under investigation. All dimensions of ASLEC (IRF, LPF, PF, LF, and HAF) exhibited significant positive correlations, with coefficients ranging from 0.322 to 0.612 (P < 0.01). Except for “Emotional Awareness”, all other dimensions of DERS were significantly positively correlated, with coefficients ranging between 0.300 and 0.708 (P < 0.01). Severity of NSSI (outcome variable) showed a significant correlation with ASLE severity (independent variable), featuring a correlation coefficient between 0.263 and 0.380 (P < 0.01). The correlation between the hypothesized mediators (internalizing symptoms) and ASLE severity varied from 0.290 to 0.497 (P < 0.01), while the correlation between these mediators and NSSI severity ranged from 0.298 to 0.423. Another hypothesized mediator (DER) also correlated with NSSI severity, with a coefficient ranging from 0.231 to 0.322 (P < 0.01). Additionally, gender (covariate) was found to be correlated with NSSI severity (r = 0.263, P < 0.01).
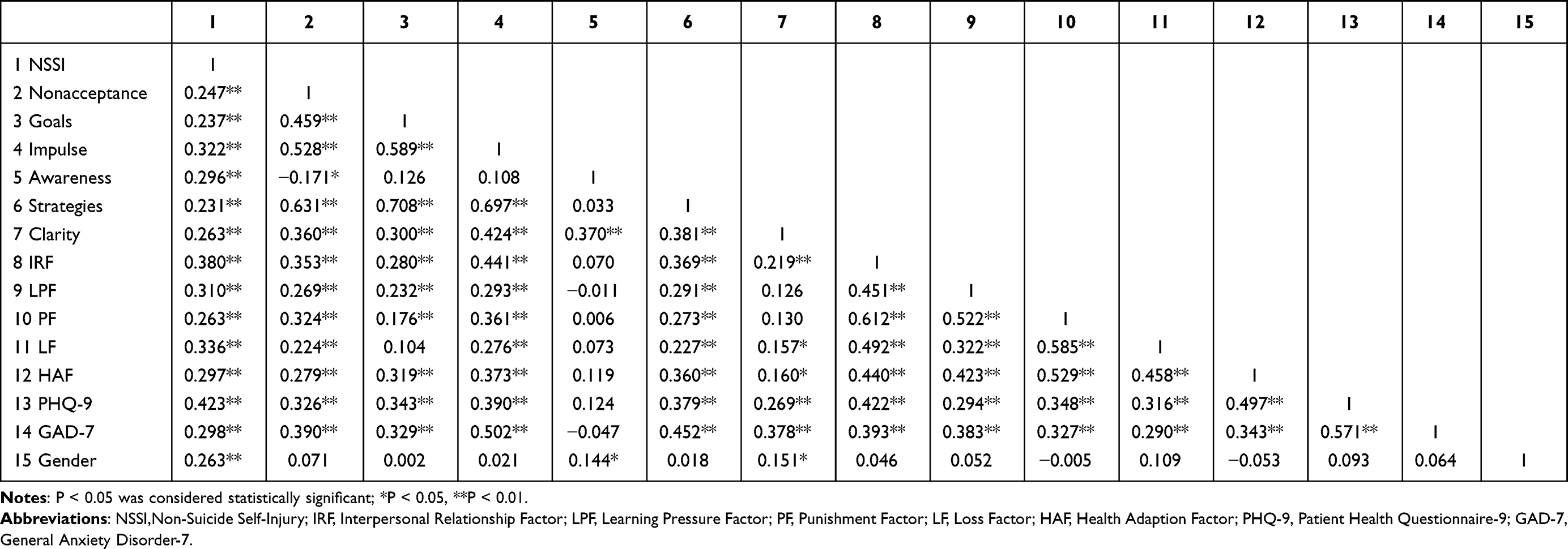 |
Table 3 Correlation Coefficient Matrix Between Study Variables |
Mediation Analysis of the Variables
The proposed chained mediation model encompasses both latent variables (ASLE, DER, and internalizing symptoms) and manifest variables (gender and NSSI), as illustrated in Figure 1. Within DER, four subscales were included: Non-Acceptance of Emotions, Inability to Engage in Goal-Directed Behaviors, Impulse Control Difficulties, and Self-Perceived Limited Access to Strategies. Two additional DER subscales, Emotional Awareness and Emotional Clarity, were excluded from the model due to their non-significant impact (Emotional Awareness, β = 0.079, P = 0.261; Emotional Clarity, β = 0.470, P < 0.01). The proposed model demonstrated an excellent fit based on various indices: χ2 = 122.432, χ2/df = 2.041, P = 0.000, CFI = 0.946, TLI = 0.930, and RMSEA = 0.068. Figure 1 presents the model with significant path coefficients, while Table 4 enumerates the non-standardized total, direct, and indirect effects observed among the variables under study.
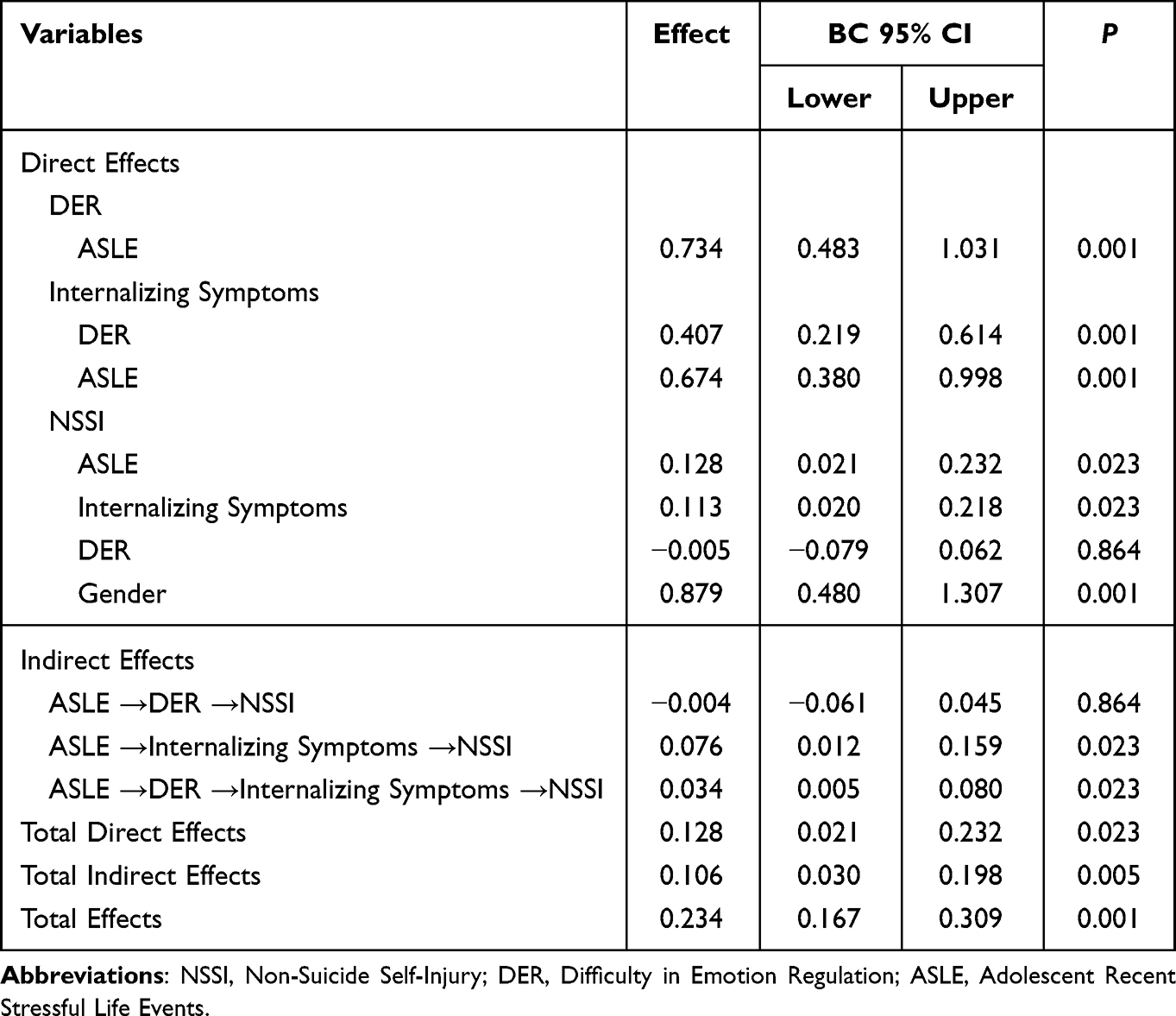 |
Table 4 Non-Standardized Direct and Indirect Effects |
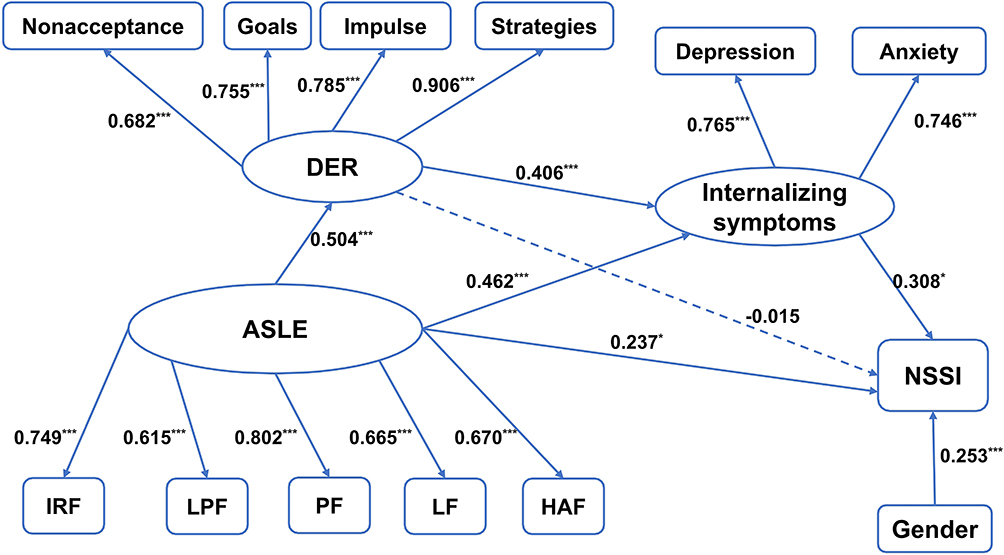 |
Figure 1 Results from path analysis on the hypothesized mediation model Pathways between variables are indicated by standardized beta estimates. Abbreviations: NSSI, Non-Suicide Self-Injury; DER, Difficulty in Emotion Regulation; ASLE, Adolescent Recent Stressful Life Events; IRF, Interpersonal Relationship Factor; LPF, Learning Pressure Factor; PF, Punishment Factor; LF, Loss Factor; HAF, Health Adaption Factor. Note: *P < 0.05, ***P < 0.001. |
ASLE exerted a significant direct effect on the severity of NSSI, as indicated by β = 0.128, P = 0.023. Moreover, ASLE also had an indirect influence on NSSI severity. In terms of the non-standardized indirect effect values, the pathways “ASLE → Internalizing Symptoms → NSSI” and “ASLE → DER → Internalizing Symptoms → NSSI” showed significant increases, with values of 0.076 (P = 0.023) and 0.034 (P = 0.023), respectively. However, the pathway “ASLE → DER → NSSI” did not exhibit a significant indirect effect (β = −0.004, P = 0.864).
Consistent with our hypothesis, we found a mediating role of Internalizing Symptoms in the relationship between ASLE and NSSI. Additionally, a significant chained mediation effect from DER to NSSI through Internalizing Symptoms was identified. The total indirect effect was highly significant (β = 0.106, P = 0.005). The model accounted for 30.3% of the total variance in adolescent NSSI (P < 0.001), with a total mediation effects ratio of 45.3% (P < 0.001).
We made an attempt to construct separate structural equation models for boys and girls. However, due to the limited quantity of boy samples (n=48, P=0.187), we were unable to construct structural equation models for this group. We successfully constructed a structural equation model for the girl sample (n = 176, P = 0.001): Consistent with the results obtained from the total sample, we observed a mediating role of Internalizing Symptoms in the relationship between ASLE and NSSI (β = 0.082, P = 0.021). Furthermore, we identified a significant chained mediation effect from DER to NSSI through Internalizing Symptoms (β = 0.028, P = 0.012). Please note that the sample size of the girls who constructed the structural equation model was below the recommended minimum value of 207 (n=176), and the model fit was deemed poor (RMSEA = 0.081).
Discussion
The primary objective of this research was to elucidate the mechanisms through which recent stressful life events influence NSSI among adolescent psychiatric patients. Utilizing SEM, our findings identified three distinct pathways—two indirect and one direct—through which recent stressful life events may be associated with NSSI. These are: 1) a mediation effect of internalizing symptoms, 2) a co-mediation effect involving both DER and internalizing symptoms, and 3) a direct association of recent stressful life events. Our data showed that adolescents with higher scores on the emotional problems scale were significantly more likely to engage in NSSI behaviors (P < 0.05), which is consistent with previous research suggesting that emotional problems can lead to higher levels of stress and subsequent engagement in NSSI.20,34,35,38–40 Additionally, the chain mediation effect involving DER and internalizing symptoms implies that adolescents struggling with emotion regulation are more prone to internalizing symptoms, subsequently elevating the risk of resorting to NSSI as a temporary coping mechanism.32
This research enriches the existing knowledge on the interplay between life events and NSSI in adolescents. Notably, the prevalence of NSSI in our adolescent sample was over 40%, a figure that markedly surpasses the 4% prevalence rate observed in the general population.50 Such a disparity underscores the gravity of NSSI as a healthcare concern among clinically-diagnosed adolescents. The elevated incidence of NSSI among female participants in our sample aligns with findings from previous studies.5,51 However, it is essential to acknowledge that our sample was limited by the under-representation of male participants, making the model more applicable to girls than to boys. The results of the structural equation model for girls further supported the suitability of the model for this particular gender.
Further analyses of the model indicate a potential gender-specific mechanism in NSSI. Adolescent girls experience significant developmental transformations, such as the onset of menstruation and bodily changes; these milestones often come with heightened emotional experiences and increased sensitivity, coupled with lower psychological resilience; such traits may amplify endocrine or arousal responses to stress, culminating in more intense negative emotional experiences.52 The primary motivation behind self-injury often lies in the alleviation of negative emotions.53 This could partly explain the higher detection rates of NSSI among girls compared to boys. Moreover, females may be more inclined to seek attention and understanding following self-injury behaviors than their male counterparts.54
Our findings establish a direct correlation between life events and the severity of NSSI behaviors in adolescents. Specifically, the impact level of negative life events positively predicts the severity of NSSI. This is in line with previous studies that have also found a strong relationship between stressful life events and NSSI.12,55 However, our results diverge from a handful of studies that did not find a significant direct effect.56 One possible explanation for this discrepancy could be the different demographic backgrounds of the study samples. Experiencing negative life events often leads to negative emotional experiences among adolescents and may indicate that multiple needs are not being met during their personality development; combined with intrinsic factors such as poor stress tolerance and inadequate social problem-solving skills, this may ultimately drive adolescents to use NSSI behavior to cope with psychosocial conflicts.57 Furthermore, among the five types of life events, punishment (β = 0.802, P < 0.001) and interpersonal relationships (β = 0.749, P < 0.001) were found to be most closely associated with adolescent NSSI. Previous studies support the finding that social punishment coupled with high levels of peer exclusion may increase the risk of NSSI among adolescents.58 According to the ASLEC construct, punishments include “failure of expected selection, criticism or discipline, transfer or drop-out, being punished, fight, scolding by parents, accident”, while interpersonal relationships include “being misunderstood, being discriminated against, having disputes with classmates or close friends, public humiliation”. Previous studies addressing the association between interpersonal relationships and NSSI have shown that NSSI behaviors are positively associated with peer isolation, bullying, and alienation.59,60 Thus, it can be seen that poor interpersonal relationships can lead to the occurrence of adolescent NSSI. Interpersonal conflict events may be highly triggering for adolescents vulnerable to NSSI and the use of multiple forms of NSSI may be associated with worse interpersonal relationships.61 NSSI can alleviate the negative emotions brought by poor interpersonal relationships and some adolescents may use NSSI to regulate interpersonal relationships and control others. Punishment is the first time it has been noted to be most closely associated with adolescent NSSI. This result may be related to China’s current one-child policy and traditional Chinese parenting style.62 The entire family revolves around the teenager and encouraging education leads to teenagers developing a self-centered attitude and an inability to accept failure from a young age, thus over-interpreting punishment. This study further demonstrated that different types of life events have different effects on NSSI among Chinese adolescents. Therefore, reducing recent life events will be beneficial for reducing adolescent NSSI behavior. In addition, the prevention and treatment of adolescent NSSI should focus on both avoiding punishment and strengthening interpersonal connections.
We found that in addition to being directly associated with NSSI, life events can also be indirectly associated with NSSI through the mediation of internalizing symptoms and the chain mediating effects of DER and internalizing symptoms. Several previous studies have also identified these variables as significant mediators,31,39 corroborating our findings. Yet, some other studies did not find such mediating effects.63 The differing results could be due to variations in methodologies or sample characteristics. The mediating effect of internalizing symptoms suggests that experiencing life events may lead adolescents to develop internalizing symptoms, such as anxiety and depression, which may further drive them to engage in NSSI as a means of alleviating intolerable emotions. Thus, it seems that internalizing symptoms serve as an important “bridge” between life events and adolescent NSSI behaviors, with alleviating negative emotions being the primary function of NSSI.56 Furthermore, it supports the experiential avoidance model, in which situational events (such as negative life events) trigger negative emotions (such as anxiety and depression) in individuals, leading them to engage in NSSI to reduce or eliminate emotional arousal.64 The chain mediating effect of DER and internalizing symptoms suggests that experiencing high frequency and intensity of negative life events impairs adolescents’ emotion regulation. At the same time, DER causes adolescents to reduce the activation of positive emotions and increase the activation of negative emotions, triggering internalizing symptoms. This means that DER, as a product of negative life events, may further affect adolescents’ emotional experiences when experiencing negative life events, thereby increasing the likelihood and severity of NSSI. These results indicate that preventing NSSI among adolescents requires not only timely management of the direct negative effects of life events, but also interventions for concomitant DER and internalizing symptoms. This includes teaching adolescents how to positively alleviate anxiety and depression. In terms of DER intervention, special attention should be paid to the dimension of “limited access to effective emotion regulation strategies” (β = 0.906, P < 0.001).
Contrary to our expectation, there was no direct link between DER and NSSI in this model; DER influenced adolescent NSSI through the mediating effect of internalizing symptoms. Previous studies have emphasized a strong correlation between DER and NSSI, but the finding that the two were not correlated in this study is surprising.32,65,66 However, given that NSSI is often used as a maladaptive emotion regulation strategy, it is possible that DER is related to NSSI only when internalizing symptoms need to be regulated. Another explanation may be that DER caused by life events may be so temporary or mild that it is not sufficient to be associated with NSSI and therefore need to resort to internalizing symptoms to be associated with NSSI in adolescents.
Our findings also have some clinical significance. Firstly, our research suggests that recent stressful life events play an important direct role in adolescent NSSI, especially in punishment and interpersonal relationship events. Most previous studies investigating the relationship between NSSI and life events have focused on significant childhood trauma rather than recent negative life events. Secondly, recent stressful life events may also indirectly be associated with adolescent NSSI through the mediating effect of DER and internalizing symptoms. Finally, our study validates the internal negative reinforcement and external negative reinforcement functions of the four-function model of NSSI,67 indicating that adolescent participation in NSSI is to alleviate negative emotions and/or break free from negative interpersonal relationships. Therefore, it is of practical significance to evaluate recent stressful life events, DER, and internalizing symptoms among adolescents with NSSI behavior. We should focus on enabling adolescents to establish positive and effective emotion regulation methods. At present, the research on the prevention and treatment of NSSI among adolescents is still in its preliminary stage and more research is needed.
Conclusions and Limitations
Overall, this study explored the underlying mechanism between recent life events and NSSI severity in a sample of Chinese adolescent inpatients. The results suggest that the association between life events and NSSI among adolescents is achieved through three different pathways: the direct association of life events, the mediating effect of internalizing symptoms, and the chain mediating effect of DER and internalizing symptoms. Importantly, our study suggests that recent negative life events, particularly punishment and interpersonal relationship events, play a significant role in adolescent NSSI. In addition, we selected the CRSNSSI(DSM-5) as an evaluation index of self-injury through structured interviews, which can better reflect the severity of NSSI than self-rated self-injury scales. In summary, our findings largely corroborate the existing literature but also introduce nuanced understandings and raise questions that could be addressed in future research. Our study contributes by highlighting the complex interplay of multiple factors in influencing NSSI among adolescents, advocating for a multifaceted approach to understanding and treating this critical issue.
Despite its advantages, some limitations of this study must be acknowledged. Firstly, due to its cross-sectional design, causal relationships between recent stressful life events, DER, internalizing symptoms, and NSSI could not be derived. These causal relationships will need to be validated in future longitudinal studies. Future research should utilize a longitudinal design and consider other possible mediators, such as externalizing symptoms, social support, resilience, as well as other internalized symptoms, including physical discomfort and suicidal ideation. Secondly, the participants were adolescent patients from a hospital in Hangzhou, and male participants were underrepresented. Therefore, the gender imbalance in our sample, which may impact the generalizability of our findings. In addition, the findings should be replicated in a non-clinical sample of adolescents. Thirdly, we used a retrospective self-report questionnaire, which may limit our findings. Participants may report inaccurately due to personal recall bias or misinterpretation of questions. Future studies should use large samples, multicenter, longitudinal designs, and assessment tools other than self-report questionnaires, such as expert opinion or other objective evidence. The limitations of this study remain a major focus for further research.
Abbreviations
NSSI, non-suicidal self-injury; DER, difficulty in emotion regulation; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th edition; SEM, structural equation model; DSM-IV, American Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; CI, confidence interval; SD, Standard Deviation; DERS, Difficulties in Emotion Regulation Scale; ASLEC, Adolescent Self-Rating Life Events Check List; PHQ-9, Patient Health Questionnaire-9; GAD-7, General Anxiety Disorder-7; CRSNSSI, Clinician-Rated Severity of Non-Suicidal Self-Injury; IRF, Interpersonal Relationship Factor; LPF, Learning Pressure Factor; PF, Punishment Factor; LF, Loss Factor; HAF, Health Adaption Factor.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted by the Declaration of Helsinki and approved by the ethics committee of Hangzhou First People’s Hospital, affiliated with West Lake University School of Medicine (IRB: 2020-K008–01, January 2020). The parent or legal guardian provided written informed consent to participate in this study, with the assent of the adolescents.
Funding
This work was funded by National Natural Science Foundation of China (grant number: 81971277; 82271570) and the medical and health research project of Zhejiang province (2023KY920).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. This manuscript has not been published nor is it being considered for publication elsewhere.
References
1. Aghajani M, Veer IM, van Lang ND, et al. Altered white-matter architecture in treatment-naive adolescents with clinical depression. Psychol Med. 2014;44(11):2287–2298. doi:10.1017/S0033291713003000
2. Zetterqvist M. The DSM-5 diagnosis of nonsuicidal self-injury disorder: a review of the empirical literature. Child Adolesc Psychiatr Ment Health. 2015;9:31. doi:10.1186/s13034-015-0062-7
3. Swannell SV, Martin GE, Page A, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life Threat Behav. 2014;44(3):273–303. doi:10.1111/sltb.12070
4. Gillies D, Christou MA, Dixon AC, et al. Prevalence and characteristics of self-harm in adolescents: meta-analyses of community-based studies 1990–2015. J Am Acad Child Adolesc Psychiatry. 2018;57(10):733–741. doi:10.1016/j.jaac.2018.06.018
5. Bresin K, Schoenleber M. Gender differences in the prevalence of nonsuicidal self-injury: a meta-analysis. Clin Psychol Rev. 2015;38:55–64. doi:10.1016/j.cpr.2015.02.009
6. Meszaros G, Horvath LO, Balazs J. Self-injury and externalizing pathology: a systematic literature review. BMC Psychiatry. 2017;17(1):160. doi:10.1186/s12888-017-1326-y
7. Klonsky ED, May AM, Glenn CR. The relationship between nonsuicidal self-injury and attempted suicide: converging evidence from four samples. J Abnorm Psychol. 2013;122(1):231–237. doi:10.1037/a0030278
8. Kiekens G, Hasking P, Boyes M, et al. The associations between non-suicidal self-injury and first onset suicidal thoughts and behaviors. J Affect Disord. 2018;239:171–179. doi:10.1016/j.jad.2018.06.033
9. Wilkinson P, Goodyer I. Non-suicidal self-injury. Eur Child Adolesc Psychiatry. 2011;20(2):103–108. doi:10.1007/s00787-010-0156-y
10. Nock MK. Future directions for the study of suicide and self-injury. J Clin Child Adolesc Psychol. 2012;41(2):255–259. doi:10.1080/15374416.2012.652001
11. Liu RT, Cheek SM, Nestor BA. Non-suicidal self-injury and life stress: a systematic meta-analysis and theoretical elaboration. Clin Psychol Rev. 2016;47:1–14. doi:10.1016/j.cpr.2016.05.005
12. Tang J, Yang W, Ahmed NI, et al. Stressful life events as a predictor for nonsuicidal self-injury in southern Chinese adolescence: a cross-sectional study. Medicine. 2016;95(9):e2637. doi:10.1097/MD.0000000000002637
13. Horváth LO, Győri D, Komáromy D, et al. Nonsuicidal self-injury and suicide: the role of in clinical and non-clinical populations of adolescents. Front Psychiatry. 2020;11:370. doi:10.3389/fpsyt.2020.00370
14. Hankin BL, Abela JR. Nonsuicidal self-injury in adolescence: prospective rates and risk factors in a 2½ year longitudinal study. Psychiatry Res. 2011;186(1):65–70. doi:10.1016/j.psychres.2010.07.056
15. Kaess M, Eppelmann L, Brunner R, et al. Life events predicting the first onset of adolescent direct self-injurious behavior-a prospective multicenter study. J Adolesc Health. 2020;66(2):195–201. doi:10.1016/j.jadohealth.2019.08.018
16. Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1:293–319. doi:10.1146/annurev.clinpsy.1.102803.143938
17. Liu X, Liu L, Yang J, et al. Development and reliability validity testing of the adolescent life events scale. Shand Psychiat Med. 1997;1:15–19.
18. Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr Dir Psychol Sci. 2009;18(2):78–83. doi:10.1111/j.1467-8721.2009.01613.x
19. Xin M, Yang X, Liu K, et al. Impact of negative life events and social support on nonsuicidal self-injury among Chinese middle school students. Am J Mens Health. 2020;14(4):1557988320937124. doi:10.1177/1557988320937124
20. Guerry JD, Prinstein MJ. Longitudinal prediction of adolescent nonsuicidal self-injury: examination of a cognitive vulnerability-stress model. J Clin Child Adolesc Psychol. 2010;39(1):77–89. doi:10.1080/15374410903401195
21. Liu RT, Frazier EA, Cataldo AM, et al. Negative life events and non-suicidal self-injury in an adolescent inpatient sample. Arch Suicide Res. 2014;18(3):251–258. doi:10.1080/13811118.2013.824835
22. Baetens I, Greene D, Van Hove L, et al. Predictors and consequences of non-suicidal self-injury in relation to life, peer, and school factors. J Adolesc. 2021;90:100–108. doi:10.1016/j.adolescence.2021.06.005
23. Miller AB, Linthicum KP, Helms SW, et al. Reciprocal associations between adolescent girls’ chronic interpersonal stress and nonsuicidal self-injury: a multi-wave prospective investigation. J Adolesc Health. 2018;63(6):694–700. doi:10.1016/j.jadohealth.2018.06.033
24. Nock MK, Mendes WB. Physiological arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. J Consult Clin Psychol. 2008;76(1):28–38. doi:10.1037/0022-006X.76.1.28
25. Gratz KL. Targeting emotion dysregulation in the treatment of self-injury. J Clin Psychol. 2007;63(11):1091–1103. doi:10.1002/jclp.20417
26. Slee N, Spinhoven P, Garnefski N, et al. Emotion regulation as mediator of treatment outcome in therapy for deliberate self-harm. Clin Psychol Psychother. 2008;15(4):205–216. doi:10.1002/cpp.577
27. Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–363. doi:10.1146/annurev.clinpsy.121208.131258
28. Gårdvik KS, Torgersen T, Rygg M, et al. Suicidality, function and associated negative life events in an adolescent psychiatric population at 3-year follow-up. BMC Psychiatry. 2021;21(1):109. doi:10.1186/s12888-021-03100-w
29. Voon D, Hasking P, Martin G. The roles of emotion regulation and ruminative thoughts in non-suicidal self-injury. Br J Clin Psychol. 2014;53(1):95–113. doi:10.1111/bjc.12030
30. Tanner A, Hasking P, Martin G. Co-occurring non-suicidal self-injury and firesetting among at-risk adolescents: experiences of negative life events, mental health problems, substance use, and suicidality. Arch Suicide Res. 2016;20(2):233–249. doi:10.1080/13811118.2015.1008162
31. McLaughlin KA, Hatzenbuehler ML, Mennin DS, et al. Emotion dysregulation and adolescent psychopathology: a prospective study. Behav Res Ther. 2011;49(9):544–554. doi:10.1016/j.brat.2011.06.003
32. Ewing L, Hamza CA, Willoughby T. Stressful experiences, emotion dysregulation, and nonsuicidal self-injury among university students. J Youth Adolesc. 2019;48(7):1379–1389. doi:10.1007/s10964-019-01025-y
33. Liu J, Chen X, Lewis G. Childhood internalizing behaviour: analysis and implications. J Psychiatr Ment Health Nurs. 2011;18(10):884–894. doi:10.1111/j.1365-2850.2011.01743.x
34. Kumar G, Pepe D, Steer RA. Adolescent psychiatric inpatients’ self-reported reasons for cutting themselves. J Nerv Ment Dis. 2004;192(12):830–836. doi:10.1097/01.nmd.0000146737.18053.d2
35. Tilton-Weaver L, Marshall SK, Svensson Y. Depressive symptoms and non-suicidal self-injury during adolescence: latent patterns of short-term stability and change. J Adolesc. 2019;75:163–174. doi:10.1016/j.adolescence.2019.07.013
36. Evans E, Hawton K, Rodham K. Factors associated with suicidal phenomena in adolescents: a systematic review of population-based studies. Clin Psychol Rev. 2004;24(8):957–979. doi:10.1016/j.cpr.2004.04.005
37. Foley DL, Goldston DB, Costello EJ, et al. Proximal psychiatric risk factors for suicidality in youth: the Great Smoky Mountains Study. Arch Gen Psychiatry. 2006;63(9):1017–1024. doi:10.1001/archpsyc.63.9.1017
38. You J, Leung F. The role of depressive symptoms, family invalidation and behavioral impulsivity in the occurrence and repetition of non-suicidal self-injury in Chinese adolescents: a 2-year follow-up study. J Adolesc. 2012;35(2):389–395. doi:10.1016/j.adolescence.2011.07.020
39. Jacobson CM, Hill RM, Pettit JW, et al. The association of interpersonal and intrapersonal emotional experiences with non-suicidal self-injury in young adults. Arch Suicide Res. 2015;19(4):401–413. doi:10.1080/13811118.2015.1004492
40. Assari S, Lankarani MM. Association between stressful life events and depression; intersection of race and gender. J Racial Ethn Health Disparities. 2016;3(2):349–356. doi:10.1007/s40615-015-0160-5
41. Faul F, Erdfelder E, Lang AG, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
42. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
43. Leung D, Mak YW, Leung SF, et al. Measurement invariances of the PHQ-9 across gender and age groups in Chinese adolescents. Asia Pac Psychiatry. 2020;12(3):e12381. doi:10.1111/appy.12381
44. Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
45. Löwe B, Decker O, Müller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266–274. doi:10.1097/MLR.0b013e318160d093
46. Wang Y, Chen R, Zhang L. Reliability and validity of Generalized Anxiety Inventory −7 in Chinese general hospital inpatients. J Clin Psychiatry. 2018;28(03):168–171.
47. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopath Behav Assess. 2004;26(1). doi:10.1023/B:JOBA.0000007455.08539.94
48. Association AP. Diagnostic and Statistical Manual of Mental Disorders. Arlington VA: Association AP; 2013.
49. Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res. 1992;21(2):230–258. doi:10.1177/0049124192021002005
50. Klonsky ED, Oltmanns TF, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003;160(8):1501–1508. doi:10.1176/appi.ajp.160.8.1501
51. Yang F, Jiang L, Miao J, et al. The association between non-suicidal self-injury and negative life events in children and adolescents in underdeveloped regions of south-western China. PeerJ. 2022:10:e12665. doi:10.7717/peerj.12665
52. Bangasser DA, Valentino RJ. Sex differences in stress-related psychiatric disorders: neurobiological perspectives. Front Neuroendocrinol. 2014;35(3):303–319. doi:10.1016/j.yfrne.2014.03.008
53. Hepp J, Carpenter RW, Störkel LM, et al. A systematic review of daily life studies on non-suicidal self-injury based on the four-function model. Clin Psychol Rev. 2020;82:101888. doi:10.1016/j.cpr.2020.101888
54. Nam SK, Chu HJ, Lee MK, et al. A meta-analysis of gender differences in attitudes toward seeking professional psychological help. J Am Coll Health. 2010;59(2):110–116. doi:10.1080/07448481.2010.483714
55. Zhang Y, Suo X, Zhang Y, et al. The relationship between negative life events and nonsuicidal self-injury among Chinese adolescents: a moderated-mediation model. Neuropsychiatr Dis Treat. 2022;18:2881–2890. doi:10.2147/NDT.S386179
56. Gu H, Lu Y, Cheng Y. Negative life events and nonsuicidal self-injury in prisoners: the mediating role of hopelessness and moderating role of belief in a just world. J Clin Psychol. 2021;77(1):145–155. doi:10.1002/jclp.23015
57. Mann JJ, Waternaux C, Haas GL, et al. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156(2):181–189. doi:10.1176/ajp.156.2.181
58. Pollak OH, Kwon SJ, Jorgensen NA, et al. Neural reactivity to social punishment predicts future engagement in nonsuicidal self-injury among peer-rejected adolescents. Biol Psychiatry. 2023:40–49. doi:10.1016/j.biopsych.2022.09.030
59. Antila H, Arola R, Hakko H, et al. Bullying involvement in relation to personality disorders: a prospective follow-up of 508 inpatient adolescents. Eur Child Adolesc Psychiatry. 2017;26(7):779–789. doi:10.1007/s00787-017-0946-6
60. Peng Z, Klomek AB, Li L, et al. Associations between Chinese adolescents subjected to traditional and cyber bullying and suicidal ideation, self-harm and suicide attempts. BMC Psychiatry. 2019;19(1):324. doi:10.1186/s12888-019-2319-9
61. Zetterqvist M, Lundh LG, Dahlström O, et al. Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. J Abnorm Child Psychol. 2013;41(5):759–773. doi:10.1007/s10802-013-9712-5
62. Kim SY, Wang Y, Orozco-Lapray D, et al. Does “Tiger Parenting” Exist? Parenting profiles of Chinese Americans and adolescent developmental outcomes. Asian Am J Psychol. 2013;4(1):7–18. doi:10.1037/a0030612
63. Voon D, Hasking P, Martin G. Emotion regulation in first episode adolescent non-suicidal self-injury: what difference does a year make? J Adolesc. 2014;37(7):1077–1087. doi:10.1016/j.adolescence.2014.07.020
64. Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44(3):371–394. doi:10.1016/j.brat.2005.03.005
65. Reinhardt M, Horváth Z, Urbán R, et al. Dissociative tendencies aggregate the impact of negative life events on non-suicidal self-injury among male juvenile delinquents. Arch Suicide Res. 2022;26(1):226–244. doi:10.1080/13811118.2020.1784335
66. Hu C, Huang J, Shang Y, et al. Child maltreatment exposure and adolescent nonsuicidal self-injury: the mediating roles of difficulty in emotion regulation and depressive symptoms. Child Adolesc Psychiatr Ment Health. 2023;17(1):16. doi:10.1186/s13034-023-00557-3
67. Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. J Consult Clin Psychol. 2004;72(5):885–890. doi:10.1037/0022-006X.72.5.885
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.