")
Back to Journals » Patient Preference and Adherence » Volume 18
The Impact of Patient Adherence to Dual Antiplatelet Medication Following Percutaneous Coronary Intervention on the Occurrence of Adverse Cardiovascular Events
Authors Mansurova JA , Orekhov A , Zhunuspekova AS , Kassymova AA , Karazhanova LK
Received 19 November 2023
Accepted for publication 3 February 2024
Published 17 February 2024 Volume 2024:18 Pages 425—434
DOI https://doi.org/10.2147/PPA.S450317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
J A Mansurova, Andrey Orekhov, A S Zhunuspekova, A A Kassymova, L K Karazhanova
Department of Therapy, Non-Commercial Joint-Stock Company “Semey Medical University”, Semey, The Republic of Kazakhstan
Correspondence: Andrey Orekhov, Department of Therapy, Non-Commercial Joint-Stock Company “Semey Medical University”, Molodogvardeyskaya 34-1 Street, Semey, F18E9T9, The Republic of Kazakhstan, Tel +87774141476, Email [email protected]
Background: The objective of this study is to examine the impact of medication adherence on the timing of non-cardiovascular serious events (NCDS) onset in patients with acute coronary syndrome (ACS) after percutaneous coronary intervention (PCI).
Methods: This prospective study was conducted at a single center and involved 220 ACS patients who underwent sequential PCI with stenting. The Morisky Green Levine Medication Adherence Scale was employed to assess adherence to dual antiplatelet therapy (DAPT) and its impact on NCDS occurrence. Early in their hospitalization, all patients received education at the Coronary Heart Disease School. The survival rates of patients in both the main group and a control group (n=355) were subsequently evaluated.
Results: The study findings indicated an inverse relationship between stent thrombosis development (Rho=− 0.334; p=0.001) and the timing of recurrent myocardial ischemia. There was also an inverse correlation between patient adherence and stent thrombosis development (Rho=− 0.275; p=0.009). Non-adherent individuals had a 16.8 times higher likelihood of experiencing stent thrombosis compared to compliant patients (p< 0.001). Following participation in the CHD School program, treatment adherence increased from 56.5% to 88.2%. Education for ACS patients post-stenting was significantly associated with all-cause mortality within the first 6 months (p=0.040).
Conclusion: Secondary preventive measures, including education, impact the success of endovascular interventions in both the early hospital phase and the long term. Patient education can serve as a supplementary intervention to enhance DAPT adherence, thus diminishing the risk of recurrent cardiovascular events and mortality post endovascular intervention.
Keywords: acute coronary syndrome, percutaneous coronary intervention, adherence, education, dual antiplatelet therapy
Introduction
Coronary heart disease (CHD) remains the leading cause of premature mortality among individuals in good physical condition, resulting in over 7 million fatal cases annually.1 Among the various manifestations of CHD, acute coronary syndrome (ACS) stands out as particularly severe, carrying a significant risk of adverse cardiovascular outcomes. The widespread adoption of early invasive treatment strategies for ACS has notably enhanced patient outcomes,2 but ongoing monitoring of such patients has unveiled novel challenges, including recurrent episodes of ischemia, thrombosis, and stent restenosis. Inadequate adherence to long-term treatment regimens following coronary interventions stands as a primary factor contributing to the suboptimal efficacy of therapies.3 This deficiency leads to heightened occurrences of recurrent cardiovascular complications and elevated mortality rates, consequently escalating healthcare expenditures. Statistical data indicate that merely 40–75% of patients sustain secondary prevention practices post-intervention.4
Enhancing patient compliance can be achieved through approaches such as training initiatives5 and the emergence of remote monitoring systems for patients.6 However, the comprehensive benefits of educating ACS patients have not undergone exhaustive exploration. Nonetheless, current guidelines underscore the importance of comprehensive rehabilitation,7 including educational components,8 for individuals with cardiovascular disorders. Thus, the objective of this study was to analyze the influence of treatment adherence on the temporal emergence of adverse cardiovascular complications in ACS patients who have undergone percutaneous coronary interventions (PCI). Additionally, the study aimed to assess the contribution of patient education to secondary prevention efforts targeting ischemic events.
Methods
Study Design, Participants, and Setting
This prospective investigation encompassed a cohort of 220 patients diagnosed with acute coronary syndrome (ACS) who were admitted to the cardiology department of the University Hospital “SMU” in the Republic of Kazakhstan. The study spanned from January 2018 to September 2019 and focused on patients who had undergone coronary artery angiography (CAG) followed by stenting of the infarct-related artery. Within this patient group, a subset of 89 individuals (40.5%) experienced recurrent myocardial ischemia after previous percutaneous coronary intervention (PCI) and subsequently underwent repeated coronary intervention. The study examined the causal factors and temporal occurrence of these recurrent cardiac events using CAG data. To assess treatment adherence within this subgroup of patients and its impact on the timing and causes of recurrent ischemic events, the Morisky Green Levine Medication Adherence Scale was employed.9 A comparative analysis was performed on the survival outcomes of two groups: the study group, consisting of patients who underwent secondary prevention training at the School of Coronary Heart Disease, and the control group (n=355), age and gender-matched, who did not participate in the School’s program. The primary endpoint of this study phase was all-cause mortality.
Inclusion and Exclusion Criteria
Inclusion criteria encompassed confirmed cases of ACS, both with and without ST segment elevation, as per CAG assessment, and the presence of coronary artery lesions necessitating myocardial revascularization followed by double antiplatelet therapy (DAPT). Exclusion criteria encompassed patients with end-stage renal insufficiency initially receiving programmed hemodialysis, intolerance to antiplatelet agents, and those who declined participation.
Ethical Considerations and Informed Consent
This study adhered to the principles outlined in the Helsinki Declaration. The study design received approval from the Ethics Committee of the Non-Commercial Joint-Stock Company “Semey Medical University” (Protocol No. 9, dated September 13, 2017). All participants provided written informed consent to participate in the study.
Patient Information and Education
To enhance treatment adherence during hospitalization, a foundation of trust was established with patients. Educational sessions were conducted based on the curriculum of the School of Coronary Heart Disease, encompassing information on coronary heart disease pathogenesis, risk factors, lifestyle modifications, secondary prevention medications, and the duration of DAPT.
Statistical Analysis
Statistical analysis was conducted utilizing the SPSS program (version 20.0). The Kolmogorov–Smirnov test was utilized to assess the conformity of variable distribution to a normal distribution. Descriptive statistics included means and standard deviations (M+SD) for normally distributed quantitative variables, and medians and interquartile ranges (Me(IQR)) for variables not conforming to normal distribution. Dichotomous variables were expressed as fractions (absolute number of patients (%)). The comparison of quantitative variables involved Student’s t-test and Mann–Whitney U-test for independent samples, while Pearson’s chi-squared test, continuity correction, and Fisher’s exact test were employed for nominal variable associations. Kaplan-Meier analysis and Cox regression were employed to analyze the relationship between patient adherence to treatment, the timing of recurrent ischemic events after primary PCI, patient awareness, and survival probabilities at specified time points. Significance was deemed at p<0.05.
Results
The study cohort encompassed a total of 220 patients, with an average age of 61.3± 11 years, ranging from 32 to 87 years. The comprehensive clinical profiles of patients, stratified by gender, are depicted in Table 1. Within this participant group, a notable subset of 89 individuals (40.5%) possessed a history of percutaneous coronary intervention (PCI). This subgroup exhibited an average age of 62.5±10.4 years, comprising 62 males (69.7%) and 27 females (30.3%). The male and female subsets displayed average ages of 60.6±10.0 and 66.9±10.2 years, respectively (p=0.009).
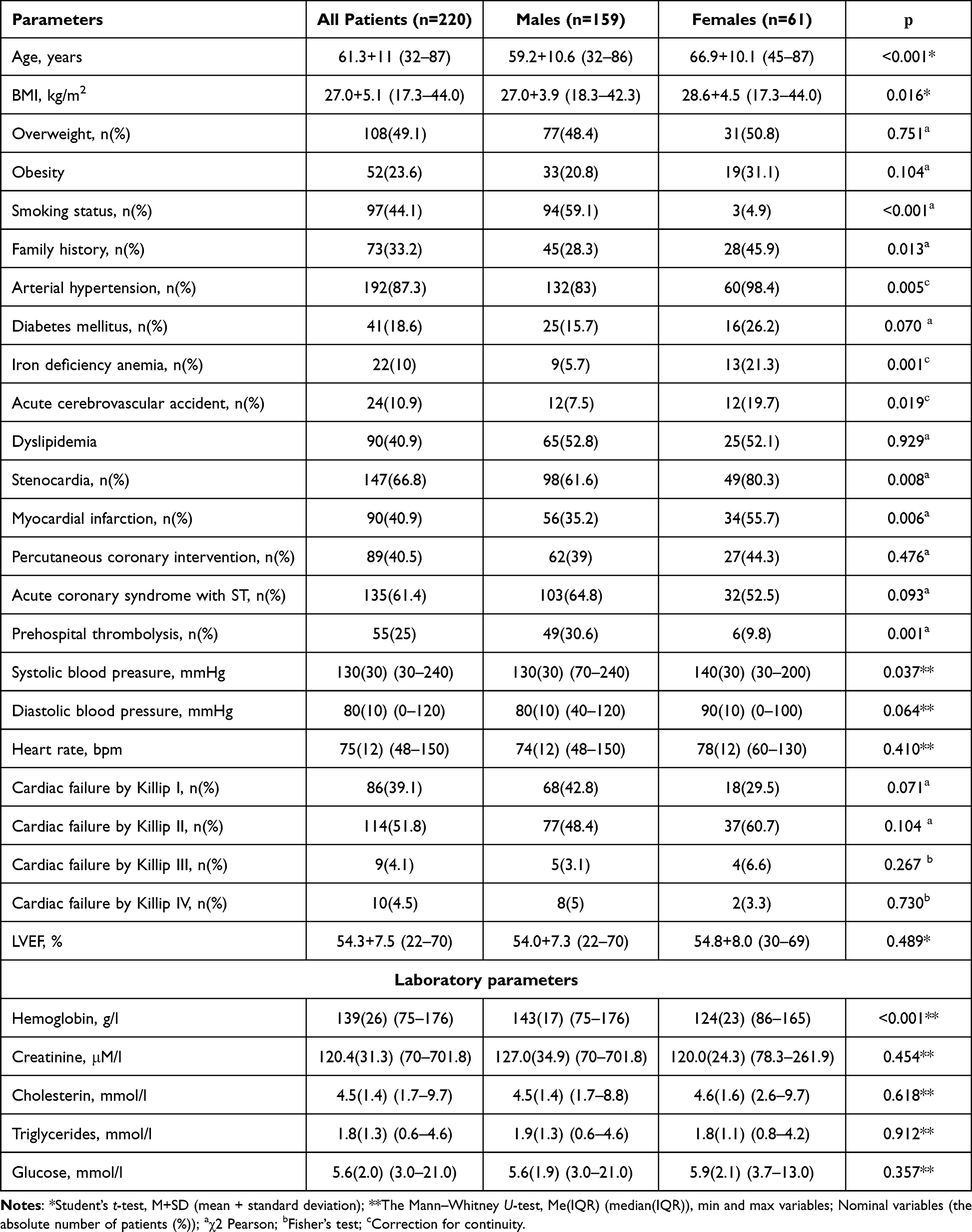 |
Table 1 General Clinical Characteristics of Patients Categorized by Gender |
A meticulous analysis of angiograms illuminated the preponderant lesion localization within the anterior descending artery, manifesting in 57.3% (51 cases) of instances. Conversely, pathology involving the right and circumflex coronary arteries was observed in 28 cases (31.5%) and 10 patients (11.2%), respectively. Scrutinizing the scope of coronary artery involvement revealed a prevailing dual-vascular affliction in 48.3% of cases. The less frequent occurrences encompassed single-vessel (34.8%, n=31) and three-vessel (16.9%, n=15) lesions.
The spectrum of angiographic presentations of recurrent myocardial ischemia encompassed distinct categories: atherosclerosis progression culminating in substantial stenosis (48.3%, n=42), stent thrombosis (27%, n=24), incomplete revascularization during primary intervention (11.2%, n=10), and stent restenosis (10.1%, n=9). Additionally, a subset of cases (4.5%, n=4) exhibited a recurrence without detectable obstructive changes.
Analysis of Treatment Adherence
A cohort of 89 patients, marked by recurrent coronary artery disease subsequent to repeated PCI, was subjected to scrutiny through the Morisky Green Levine Medication Adherence Scale. The findings unveiled a nuanced spectrum of adherence levels: 22 individuals (24.7%) demonstrated full treatment commitment, while 28 (31.5%), 20 (22.5%), 13 (14.6%), and 6 (6.7%) patients were classified as having insufficient, low, very low, and negligible adherence, respectively. Intriguingly, a gender-dependent analysis showcased a relatively heightened level of treatment adherence among women in comparison to men, with mean scores of 2.9±1.3 and 2.4±1.1, respectively (p=0.025).
Correlation Between Recurrent Coronary Events, Timing, and Patient Adherence
Stratification of patients who had undergone repeated PCI based on the temporal emergence of recurrent ischemic events yielded six distinct groups: occurrences within 10 days, between 10 days and 1 month, 1 to 3 months, 3 to 6 months, 6 months to 1 year, and beyond 1 year. Subsequent analysis of repeated coronary angiography data discerned the etiological landscape of recurrent ischemic events. Within the initial post-PCI month, “early” stent thrombosis predominated as the causative agent of recurrent endovascular interventions (72.2%). This pattern transitioned in the ensuing months, wherein progressive atherosclerosis took ascendancy. Notably, the identification of “very late” stent thrombosis, observed a year post-endovascular intervention, comprised 25% of all stent thrombosis cases. An inversely proportional correlation emerged between stent thrombosis (Rho=−0.334; p=0.001) and the timing of recurrent ischemic events, alongside a direct correlation with atherosclerosis progression (Rho=0.401; p<0.001).
An inverse relationship was documented between patient adherence and stent thrombosis development (Rho=−0.275; p=0.009), signifying that reduced adherence escalated the incidence of stent thrombosis. Levels of treatment adherence within the comparative groups are delineated in Table 2.
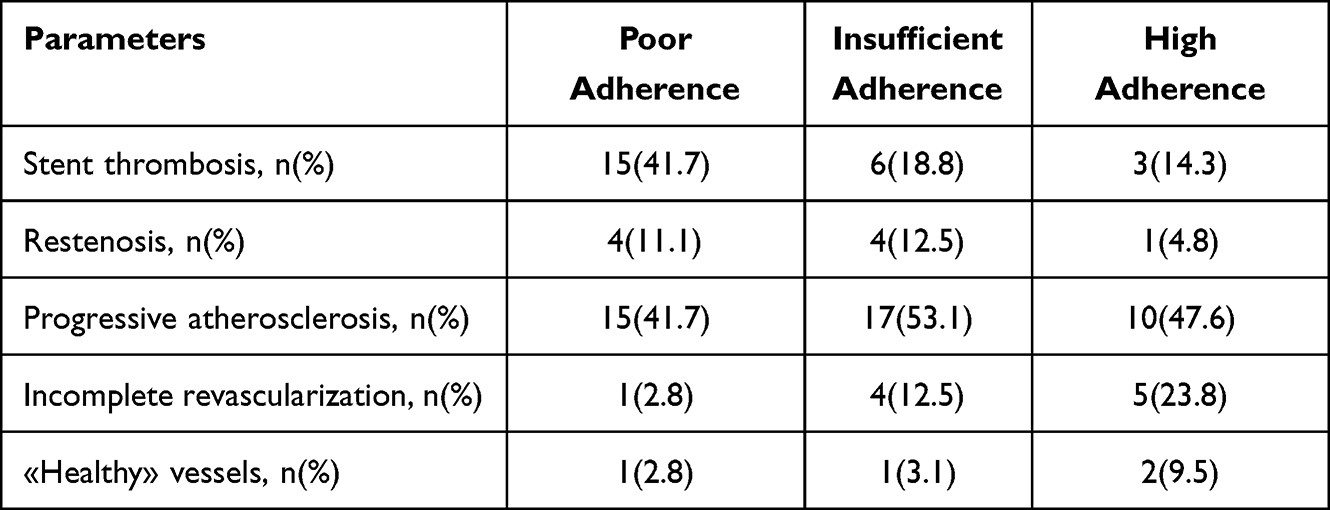 |
Table 2 Reasons for Returning to the IHD Clinic, Depending on the Degree of Treatment Adherence |
The temporal trajectory for the emergence of recurrent ischemic events manifested an average duration of 479±666 days, inclusive of a minimum of 3 days and a maximum of 2920 days. The Kaplan-Meier methodology was harnessed to scrutinize patient survival prior to event occurrence (Figure 1).
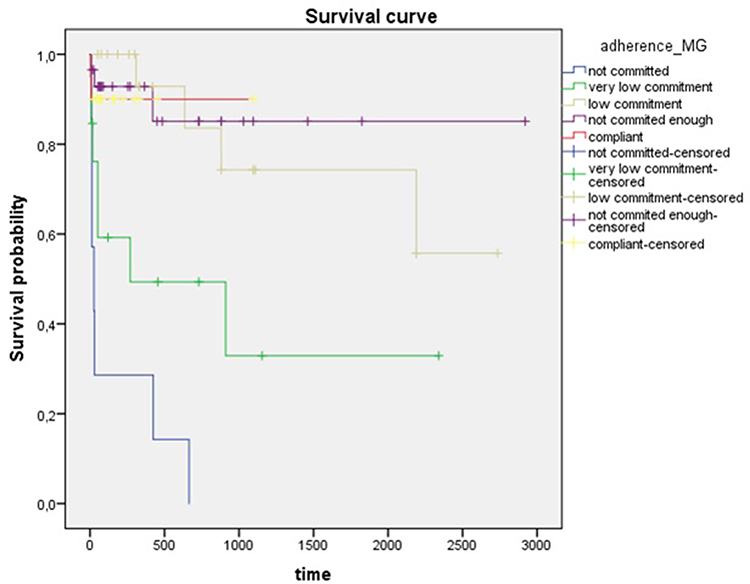 |
Figure 1 Survival function of patients before stent thrombosis. The figure presents cumulative survival/probability curves elucidating the dynamics of stent thrombosis over the follow-up period, contingent upon varying levels of patient adherence to treatment. Notably, reduced compliance is associated with an accelerated development of the thrombotic event. |
Subsequent Cox regression analysis revealed a hazard ratio of 16.8 (95% CI 3.471 to 81.055; p<0.001) for lack of adherence to treatment, indicating a 16.8-fold acceleration in stent thrombosis development. While the correlation between progressive atherosclerosis-related recurrent events and treatment adherence did not reach significance (p=0.092), the survival curve (Figure 2) spotlighted “early” stent thrombosis instances in compliant patients in the initial days post-primary PCI. Of the 13 cases of stent thrombosis occurring in the first month, 7 (53.8%) transpired during the early hospital phase, wherein all patients adhered to treatment. This underscores the significance of patient adherence in the secondary prevention of ischemic complications, while early hospital-acquired stent thrombosis suggests the potential for antiplatelet therapy resistance.
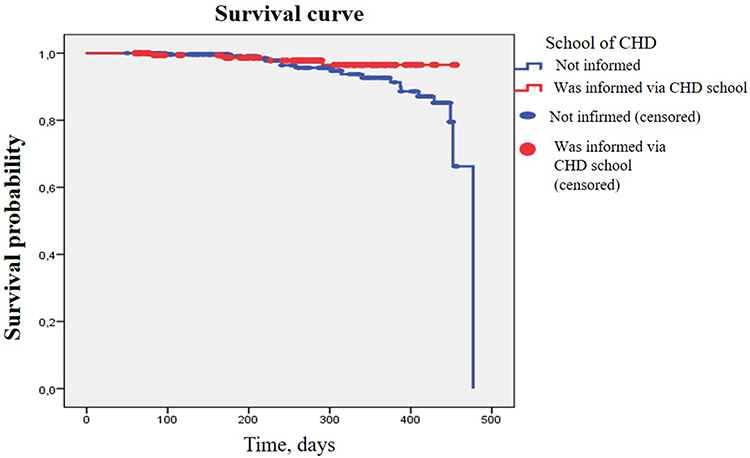 |
Figure 2 Survival curves depicting the outcomes of patients informed and uninformed within the context of the CHD program are presented for the follow-up period extending up to 6 months. Patients uninformed through the CHD School program exhibit a threefold higher probability of experiencing a fatal outcome from all causes within the initial 6-month period (p=0.040). |
Impact of Patient Education on Enhanced Adherence to DAPT
Among the initial cohort of 220 patients, 17 were excluded due to mortality, concurrent oncological pathology, and severe heart failure. The control group encompassed 355 patients hospitalized during the stipulated timeframe, all having undergone PCI with stenting. The efficacy of ACS patient education following PCI was gauged through the incidence of adverse cardiovascular events (nonfatal heart attacks, strokes, and cardiovascular-related mortality). Comparative analysis substantiated the parity of both patient groups (Table 3).
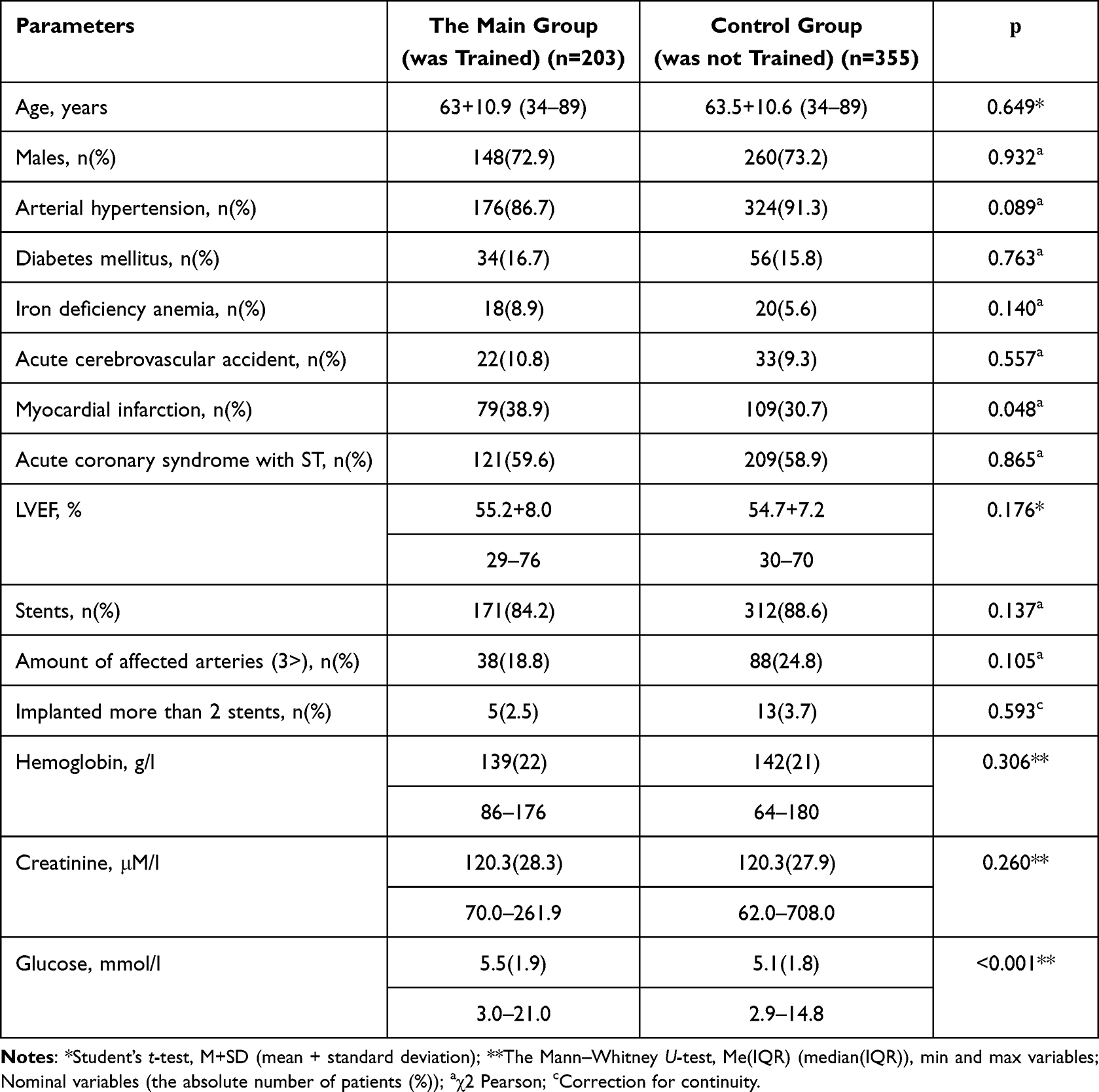 |
Table 3 Comparative Characteristics of Patients Who Have Passed and Failed Training |
Among them, 62 patients (11.1%) succumbed to all-cause mortality within the year-long follow-up period. Notably, survival rates of patients trained within the CHD School program exhibited a statistically significant elevation compared to the untrained cohort after 6 months (97.7% vs 93.5%; p=0.040). The Kaplan-Meier survival curves delineated patient outcomes in terms of all-cause mortality over a 6-month span (Figure 2).
The study group exhibited a larger number of patients who lived after one year compared to the control group (91.1% vs 87.6%). However, this difference did not reach statistical significance (p=0.202). Figure 3 depicts the survival curves of patients who had training (represented by the red curve) and those who did not get training (represented by the blue curve) as part of the CHD School program. These curves illustrate the outcomes observed throughout the follow-up period of one year.
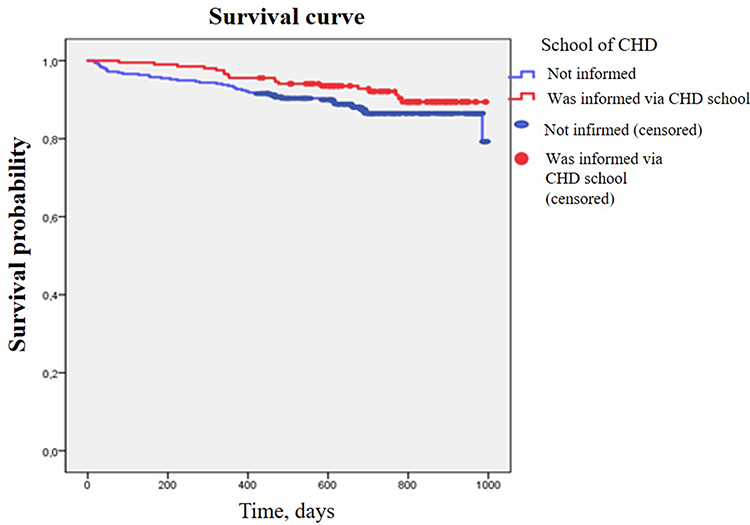 |
Figure 3 Survival curves delineating the outcomes of patients, stratified by their level of information exposure (informed and uniformed) within the CHD School program, are presented for the follow-up period. Surviving patients informed through the CHD School program exhibit a proportionately higher rate compared to their uninformed counterparts over the one-year follow-up period (p=0.202). |
Furthermore, the odds ratio for patients educated through the CHD School program in comparison to uninformed counterparts after 6 months was calculated as [OR 3.012, 95% CI 1.002 to 9.052; p=0.050]. This observation elucidates a threefold elevated risk of all-cause mortality within the initial 6-month interval for ACS patients after PCI and stenting who did not undergo education through the CHD School program. A statistically significant yet weak correlation between patient education and mortality probability was discerned (Rho=0.097; p=0.040), which diminished over time and ceased to be statistically significant after 6 months (p=0.113).
Discussion
Adherence to treatment entails the meticulous observance of prescribed medications, dietary adjustments, and lifestyle modifications. Among the cardinal imperatives in post-acute coronary syndrome (ACS) care is secondary prevention, which stands as the bulwark against the recurrence of cardiovascular events. Notably, dual antiplatelet therapy (DAAT) constitutes a pivotal facet of this paradigm. Currently endorsed guidelines advocate for the incorporation of aspirin and a P2Y12 receptor inhibitor,2 with more potent agents like prasugrel and ticagrelor preferred in Europe,10 while clopidogrel retains prominence in the USA.11
The crux of the matter is that suboptimal adherence to DAPT holds paramount significance, particularly in averting stent thrombosis during the precarious initial 30-day window post-percutaneous coronary intervention (PCI). Prior investigations revealed that merely 54.3% of patients exhibited steadfast commitment to clopidogrel treatment within a year post-myocardial infarction (MI). Importantly, those displaying nonadherence were four times more likely to undergo recurrent acute coronary events (11.0% vs 2.8%, p=0.044).12 In a parallel study by O. Kourti,13 adherence to antiplatelet therapy was assessed, yielding no discernible association with the chosen P2Y12 inhibitor. In our study, clopidogrel was the secondary component of DAPT for all patients. However, our data underscore a noticeable decline in antiplatelet therapy adherence post-30 days, reaching 49.3% as determined through survey responses.14
Patient education, alongside physical rehabilitation and psychological support, constitutes a pivotal vector of secondary prevention. Although a comprehensive review failed to establish substantial mortality reductions attributable to educational interventions, a multitude of studies have substantiated their efficacy in diminishing nonfatal recurrent ischemic events.15 Experts advocate that such educational initiatives can notably complement the comprehensive care of post-ACS patients, especially within the inaugural year post-event.
In our inquiry, we probed the event-free survival trajectory predicated on participation in the School of Coronary Heart Disease’s secondary prevention program at 6 and 12 months. The study group (n=203) encompassed educated patients, while the control group (n=355) comprised those not exposed to the program. During the follow-up, all-cause mortality accounted for 11.1% of patients. The proportion of patients surviving at the 12-month mark exhibited a favorable trend in the study group compared to the control (91.1% vs 87.6%), though statistical significance was not attained (p=0.202). Contrastingly, at the 6-month juncture, survival rates among informed patients from the CHD School program significantly surpassed the uninformed group (97.7% vs 93.5%; p=0.040). Notably, a correlation (p=0.040) persisted between mortality probability and patient awareness, maintaining significance within the first 6 months post-intervention. Our findings are concordant with prior investigations.16
A notable trial, TEXTMEDS, assessed the impact of medication-related text messages on treatment adherence in the year following ACS. Although modest effects on adherence were discerned 12 months post-ACS (relative risk 0.93, 95% CI 0.84–1.03; p=0.15), discernible enhancements in risk factor control were noted.6 Worth noting is the structured nature of this study, which delivered four weekly messages over six months. Conversely, our study entailed comprehensive training within a university clinic’s School of Coronary Heart Disease, involving eight direct patient-physician interactions.
Our findings establish the temporal confines of educational programs’ therapeutic efficacy, particularly in elevating adherence to DAPT. It is evident that trained patients manifest a more pronounced reduction in the risk of non-fatal secondary coronary events during the initial six months post-ACS. However, this impact evens out beyond the six-month threshold. Consequently, periodic reiterations of educational interventions potentially offer an optimal strategy for fostering treatment adherence in post-ACS patients.
In summary, our investigation reinforces the notion that diminished patient awareness and adherence correlate with the accelerated onset of recurrent coronary events—a consensus consistent with prevailing literature.17
Conclusion
In essence, patients evincing subpar adherence in the early stages of post-ACS care are vulnerable to heightened stent thrombosis risk. A personalized treatment approach encompassing early education through programs like the School of Coronary Heart Disease emerges as a pivotal determinant of both early and long-term success in endovascular intervention. Such initiatives serve as formidable adjuncts in the secondary prevention of recurrent coronary events, elevating treatment adherence and consequently reducing the incidence of repeated cardiovascular complications and post-endovascular intervention mortality.
Funding
The study was funded via a local grant provided by the “SMU” NCJSC (No. 379 dated 12.09.2022).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Vedanthan R, Seligman B, Fuster V. Global perspective on acute coronary syndrome: a burden on the young and poor. Circ Res. 2014;114(12):1959–1975. doi:10.1161/CIRCRESAHA.114.302782
2. Collet JP, Thiele H, Barbatoet E. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
3. Dexter PR, Miller DK, Clark DO. Preparing for an Aging Population and Improving Chronic Disease Management. AMIA Annu Symp Proc. 2010;2010:162–166.
4. Cheng K, Ingram N, Keenan J, et al. Evidence of poor adherence to secondary prevention after acute coronary syndromes: possible remedies through the application of new technologies. Open Heart. 2015;2(1):e000166. doi:10.1136/openhrt-2014-000166
5. Anderson L, Brown JP, Clark AM. Patient education in the management of coronary heart disease. Cochrane Database Syst Rev. 2017;6(6):CD008895. doi:10.1002/14651858.CD008895.pub3
6. Chow CK, Klimis H, Thiagalingamet A, et al. Text Messages to Improve Medication Adherence and Secondary Prevention after Acute Coronary Syndrome: the TEXTMEDS Randomized Clinical Trial. Circulation. 2022;145(19):1443–1455. doi:10.1161/CIRCULATIONAHA.121.056161
7. Balady GJ, Williams MA, Ades PA, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2007;115(20):2675–2682. doi:10.1161/CIRCULATIONAHA.106.180945
8. Kabboul NN, Tomlinson G, Francis TA, et al. Comparative effectiveness of the core components of cardiac rehabilitation on mortality and morbidity: a systematic review and network meta-analysis. J Clin Med. 2018;7(12):514. doi:10.3390/jcm7120514
9. Morisky DE, Green LW, Morisky LD. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
10. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
11. Rodriguez F, Harrington RA. Management of Antithrombotic Therapy after Acute Coronary Syndromes. N Engl J Med. 2021;384(5):452–460. doi:10.1056/NEJMra1607714
12. Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med. 2006;166(17):1842–1847. doi:10.1001/archinte.166.17.1842
13. Kourti O, Konstantas O, Farmakis IT, et al. Potent P2Y12 inhibitors versus clopidogrel to predict adherence to antiplatelet therapy after an acute coronary syndrome: insights from IDEAL-LDL. Rev Cardiovasc Med. 2022;23(3):81. doi:10.31083/j.rcm2303081
14. Batista Santos V, Silva LL, Guizilini S, et al. Adherence to antiplatelet and statin therapy by patients with acute coronary syndrome following discharge. Enferm Clin. 2022:32(2);115–122. doi:10.1016/j.enfcli.2020.02.020
15. Anderson L, Brown JPR, Clark AM. Patient education in the management of coronary heart disease (Review). Cochrane Database Syst Rev. 2017;6. doi:10.1002/14651858.CD008895.pub3
16. Cohen A, Assyag P, Boyer-Chatenet L, et al. An education program for risk factor management after an acute coronary syndrome a randomized clinical trial. JAMA Intern Med. 2014;174(1):40–48. doi:10.1001/jamainternmed.2013.11342
17. Chinwong S, Doungsong K, Channaina P, Phrommintikul A, Chinwong D. Association between medication adherence and cardiovascular outcomes among acute coronary syndrome patients. Res Social Adm Pharm. 2021;17(9):1631–1635. doi:10.1016/j.sapharm.2021.01.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.