")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 15
The Impact of Alcohol Consumption and Addiction on Liver Transplantation Programs in the COVID-19 Era
Authors Manikat R, Ahmed A , Kim D
Received 25 July 2023
Accepted for publication 26 September 2023
Published 29 September 2023 Volume 2023:15 Pages 141—149
DOI https://doi.org/10.2147/HMER.S384070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Richie Manikat, Aijaz Ahmed,* Donghee Kim*
Division of Gastroenterology and Hepatology, Department of Medicine, Stanford University School of Medicine, Stanford, CA, USA
*These authors contributed equally to this work
Correspondence: Donghee Kim, Division of Gastroenterology and Hepatology, Stanford University School of Medicine, 300 Pasteur Drive, Stanford, CA, 94304, USA, Tel +1-650-497-9261, Fax +1-650-498-5692, Email [email protected]; [email protected]
Abstract: The coronavirus disease 2019 (COVID-19) pandemic has caused significant shifts in alcohol consumption patterns in the United States, with potential long-term implications for liver transplantation (LT) programs. Alcohol consumption has increased, particularly in women, leading to a rise in alcohol-related liver disease (ALD) and alcohol use disorder. Psychological distress associated with the pandemic may further exacerbate alcohol addiction. ALD is now the most common indication for LT, with higher disease severity and complex clinical presentations, demanding a fundamental transformation in LT programs. Multidisciplinary cooperation among medical specialists, telemedicine, and remote healthcare are essential strategies to address these challenges. However, barriers to telemedicine and costs must be overcome. Curbing alcohol consumption at the societal level and bolstering mental health programs to mitigate healthcare workforce moral injury are recommended to optimize patient care in the post-COVID-19 era. Adequate planning and compassionate management of finite resources will be crucial for the successful continuation of LT programs amidst the concerning trends in alcohol consumption and addiction.
Keywords: alcohol-related liver disease, alcohol use disorder, COVID-19, trend
Introduction
The concerning trends in alcohol consumption and addiction are likely to have powerful shockwaves in the field of liver transplantation (LT), and some of these effects are already beginning to manifest themselves. LT programs are broadly undergoing dynamic changes in the wake of the coronavirus disease 2019 (COVID-19) pandemic. A shifting patient population, increased complexity of diseases, ongoing staffing shortages, and decreasing insurance payouts all contribute to the need for a fundamental transformation in managing these programs. Without adequate planning and forethought, programs may encounter significant difficulties in continuing to operate successfully. Adapting to and flourishing in the post-COVID-19 era will be possible with conscientious organization and dedicated patient care.
Trends in Alcohol Consumption
The COVID-19 pandemic has caused dramatic shifts in the patterns of alcohol consumption in the United States. In the general US population, both the consumption of alcohol and hospitalizations related to alcohol use have steadily increased,1 with impacts that are likely yet to be felt downstream. The sales of spirits, as opposed to beer and wine, were trending up conclusively over the course of the pandemic.2 In April 2020, stores were selling alcohol at rates 26% greater than the same time in 2019, while the amount of alcohol being sold online had increased more than four-fold.3 Rising volumes of alcohol sold, despite ongoing pushes to isolate and socially distance, point to the increasing use of alcohol alone instead of at group gatherings, which by itself may be a risk factor for the eventual development of an alcohol use disorder (AUD).4 The uptrend in alcohol consumption was apparent early in the course of the pandemic. A cross-sectional study was done in the United States which surveyed 993 individuals in February 2020 and then again in April 2020. The number of drinks consumed per day increased by 29%, and 21% higher rates of binge drinking were reported.5 The National Institute on Alcohol Abuse and Alcoholism (NIAAA) has reported that 2019 to 2020 saw the biggest single-year increase in the per capita consumption of alcoholic beverages since 1968.6 This uptrend may foreshadow future effects that are yet to make themselves fully felt. The underlying causes of the uptrend are not clear and are likely multifactorial in etiology. It is not yet clear if economic factors such as ongoing inflation and stagnant wages may be contributing to greater depression after COVID-19 infection,7 and possibly predisposing people to greater alcohol use.
On the other hand, a large European survey study involving 31,964 subjects found that alcohol consumption decreased during the first months of the COVID-19 pandemic in most European countries, except for Ireland and the United Kingdom.8 Decreases in alcohol consumption may be mainly driven by a reduced frequency of heavy episodic drinking events. It suggests a more significant impact of the availability-affordability mechanism than the distress mechanism, at least for Europe.8
A concerning trend is the possibility of increased alcohol use in women during the pandemic. A US study based on 1540 adults found that women reported a 17% increase in the frequency of days in which alcohol was consumed. One in 5 women also had, on average, one additional day of heavy drinking during the pandemic when compared to drinking habits prior to the pandemic.9 These findings are concerning, given the increased adverse effects of alcohol on women’s health due to known gender differences in alcohol pharmacokinetics. Women will develop higher blood alcohol levels drink-for-drink and pound-for-pound because of more total body fat and less total body water, allowing for a higher concentration of alcohol in the body than men. As a result of social stigma, women also commonly have less social support than men, which may lead to an uphill battle during efforts at recovery.10
Trends in Alcohol Addiction and AUD
We summarized essential studies regarding trends in AUD in Table 1. The association between the pandemic and psychological distress is already well-known. Higher rates of depression, anxiety, and post-traumatic stress disorder are commonly seen after major catastrophes like natural disasters and terrorist attacks. After recovery from a respiratory illness like Severe Acute Respiratory Syndrome (SARS), Middle Eastern Respiratory Syndrome (MERS), or COVID-19, the point prevalence rates of certain psychological conditions were 32.2% for post-traumatic stress disorder, 14.9% for depression, and 14.8% for anxiety according to a meta-analysis of 72 studies.11 Due to the high risk for self-medication with alcohol, the risk of AUD is likely elevated. Patients with COVID-19 are also more likely to screen positive for AUD, as a national survey study has reported.12 Hospitalization rates due to somatic consequences associated with alcohol and AUD increased markedly during the COVID-19 pandemic compared to the pre-COVID-19 pandemic in the United States.13 In patients already diagnosed with AUD, relapses are more common. In a Spanish study monitoring patients with AUD, the risk of screening positive for alcohol increased twofold in the 14 weeks after the lockdown started. Posited reasons include the greater amount of psychological distress, the continued availability of alcohol in essential stores, and the decreased social support available during the lockdown.13 About 20% of patients already diagnosed with AUD were found to either increase or decrease their consumption of alcohol. Psychosocial distress may play a role in relapse, and decreases in alcohol intake may be related to the closures of social spaces associated with alcohol, such as bars and pubs.
 |
Table 1 Studies on Trends in Alcohol-Related Liver Disease and Alcohol Use Disorder |
In some countries, lockdowns may precipitate patients with AUD into alternate sources of alcohol, such as home brewing and black-market sales. Isopropyl alcohol, methanol, and alcohol-based sanitizers were also being consumed in more significant quantities leading to increased mortality.19 The risk of acute liver failure would be more significant in these cases and may portend increased volume for larger centers. Though providing medical care for AUD appears daunting, healthcare systems across the globe have made notable efforts. Smaller studies provide potential models for continued care during lockdowns, such as recognizing and supporting psychological care as essential services and allowing for continued patient monitoring through telephone, video, and in-person contact.20 In some health systems, continued contact with an alcohol nurse specialist was associated with a lower risk of relapsing back into alcohol use and even increased the chances for new abstinence.21
Trends in Alcohol-Related Liver Disease
Increased rates of alcohol consumption and addiction are directly leading to higher alcohol-related morbidity. Most patients with AUD have alcohol-associated fatty liver and 10 to 20% of these patients then experience progression to alcohol-related liver disease (ALD).22 The rate of hospitalizations due to ALD had already been increasing before the COVID-19 era,23 although the pandemic appears to have exacerbated the trend. An early hotspot of the pandemic in the United States, studies from New York showed an increase of 62% in interhospital patient transfers for ALD in the post-quarantine period compared to before the start of the pandemic, along with significantly higher rates of hospital admissions related to ALD.14 COVID-19 infection may be associated with poorer outcomes in patients with ALD. A higher risk of infection has been observed in ALD, presumably due to immune dysfunction.24 An inflammatory state already exists at baseline in these patients, so the cytokine storm triggered by the COVID-19 virus may cause outsized deleterious effects leading to worse outcomes.24 Alcohol intake specifically alters cytokine responses in the lung and leads to a higher chance of progression to acute respiratory distress syndrome.24 Even in patients with alcohol-associated fatty liver that has not yet progressed to steatohepatitis, underlying chronic inflammation may provide a milieu that allows COVID-19 to trigger an extreme inflammatory response.25 Hospital admissions for ALD and pancreatitis appear to be rising. A Japanese study reported that the hospitalization rate for these medical conditions was 1.2 times greater during the pandemic when compared to prior periods.15 Hospitalization rates for ALD-related cirrhosis increased significantly (quarterly percentage change: 3.6%, 95% confidence interval [CI]: 2.2%–5.1%), with a notably higher rate during the COVID-19 era.16 Liver transplant centers in the United States also manage higher numbers of referrals for severe ALD with recent unhealthy drinking, defined as drinking within the past six months.17 Concerningly, mortality rates in patients with ALD admitted to hospitals in the United States already appear to be rising. Among hospitalizations with ALD, 60-day mortality increased by 45% between the second quarter of 2020 as compared with the second quarter of 2019.26 Patients with ALD appear to be getting admitted more often, and once admitted, they are also dying more often. The COVID-19 era and COVID-19 infection were independently associated with in-hospital mortality during hospitalization in patients with cirrhosis.16 ALD-related cirrhosis was specifically associated with a 40% higher risk of in-hospital mortality compared with hepatitis C virus-related cirrhosis during the pandemic.16 The long-term effects of increasing alcohol use have not yet been fully realized; however, modeling studies provide the basis for making reasonable predictions. If not adequately addressed, the pandemic may cause an additional 8000 deaths related to ALD, 18,700 more cases of decompensation in patients with cirrhosis, and 1000 additional cases of hepatocellular carcinoma (HCC) over the next 20 years.18 A recent study showed a steady decline in HCC-related mortality with an average quarterly percentage change of −0.4% (95% CI: −0.6% to −0.2%, p < 0.001) before and during the COVID-19 pandemic.27 However, there was a linear increase in the quarterly age-standardized HCC-related mortality from ALD (1.3%, 95% CI: 0.8% to 1.9%) before and during the COVID-19 pandemic.27 These staggering numbers are enough to cause alarm among both the primary centers that will deal with the brunt of the impact and also the tertiary centers receiving referrals for these cases. The studies noted only review the association between ALD and its specific complications like alcohol-related cirrhosis and HCC, not the multisystem impact of AUD, which has yet to be calculated. AUD can impact health on many levels, not only as ALD, but also in cardiovascular diseases and cancer along with respiratory, renal, endocrinologic, and neuropsychiatric disorders.22 LT centers, then, have a vested interest in coordinating with other facilities and with public policymakers to ensure that these complications and their root causes are adequately addressed because, otherwise, volumes are very likely to turn unmanageable. We summarized essential studies regarding ALD in Table 1.
Trends in Alcohol-Related Deaths and Comparison to Other Liver Diseases
Clinical concern was high early in the pandemic regarding the possibility of worse outcomes in patients with chronic liver disease that would be exposed to the COVID-19 virus. In an observational cohort study of 867 patients across 21 centers, the all-cause mortality was 14% among patients with chronic liver disease that had laboratory-confirmed COVID-19, with ALD being a specific risk factor, while NAFLD and hepatitis B were not found to be independent risk factors.28 With a hazard ratio of 2.69, ALD was, in fact, a more significant risk factor than diabetes and hypertension for COVID-19-related mortality. Only decompensated cirrhosis and HCC were more significant liver-specific risk factors than ALD. Data from large international registries confirm that ALD globally increased the risk of death 1.8-fold and is a more significant risk factor for COVID-19-related mortality than viral hepatitis and NAFLD.29 In patients with chronic liver disease and COVID-19, lung injury is the most common cause of death; only 19% of the mortality is due to specific liver-related complications. As cirrhosis is a greater risk factor than ALD, closely monitoring patients with ALD and preventing progression to cirrhosis may directly improve patient outcomes. Mortality for ALD specifically worsened during the pandemic compared to mortality rates in other conditions such as hepatitis B, hepatitis C, and NAFLD. Based on the US national mortality database, quarterly age-standardized all-cause mortality from ALD initially increased at a quarterly rate of 1.1% before the COVID-19 pandemic, followed by a sharp increase during the COVID-19 pandemic at a quarterly rate of 11.2%.30 A significant decrease was seen in all-cause mortality in individuals with hepatitis B and hepatitis C, however, rates for ALD rose rapidly during the COVID-19 pandemic, with NAFLD also trending up.30 Improved screening and appropriate treatment of chronic hepatitis B and the widespread use of direct antiviral agents for treating hepatitis C have definitively decreased the mortality related to viral hepatitis. We summarized essential studies regarding mortality due to ALD and AUD in Table 2. The multifactorial and protean manifestations of both ALD and NAFLD undoubtedly contribute to the difficulties encountered when addressing these conditions before the development of cirrhosis and its multisystem complications. ALD is also commonly associated with complications that can be life-threatening prior to the development of cirrhosis, such as alcoholic hepatitis and pancreatitis.
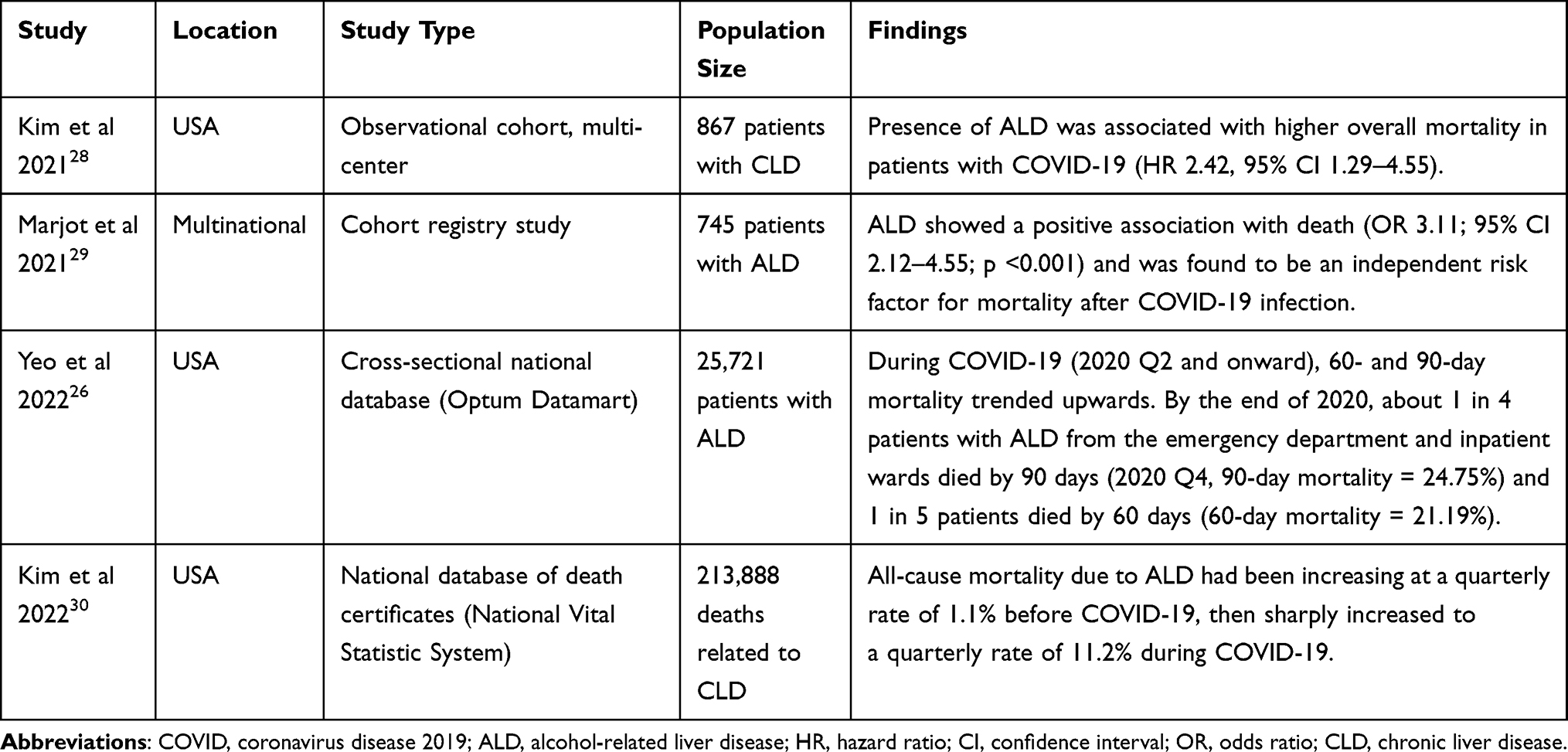 |
Table 2 Studies on Trends in Mortality Due to Alcohol-Related Liver Disease and Alcohol Use Disorder |
Trends in Liver Transplantation (LT) for AUD and ALD
Even before the pandemic, ALD had replaced hepatitis C infection as the most common indication for LT.31 During the COVID pandemic, the rates of listing for LT due to hepatitis C and nonalcoholic steatohepatitis decreased significantly, however, the rise in listing due to ALD resulted in the actual number of patients being listed remaining the same. In fact, more patients are now being listed for ALD than both hepatitis C and nonalcoholic steatohepatitis combined.2 Some changes in the criteria used for patient selection have paralleled the pandemic, such as the gradual disappearance of strict sobriety timeframes in determining eligibility for LT. The Dallas Consensus conference advised comprehensive psychosocial evaluation instead of inflexible abstinence periods during assessments for LT, which, while making the process more challenging, may better address urgency, utility, and equity, the three principles of justice.32 A cohort study compared LT recipients who had less than 6 months of sobriety prior to transplant with recipients who had 6 months or more of sobriety and found no significant differences in patient survival, graft survival, or relapse-free survival.33 Notably, the study period was from October 2012 to November 2020, encompassing the pre-COVID-19 and COVID-19 era. Due to these changes in patient selection, the pool of potential recipients has undoubtedly expanded, likely increasing the number of patients evaluated.
Demographically, the patient population needing LT is changing. Patients are younger, and Model For End-Stage Liver Disease (MELD) scores for patients receiving LT are higher, implying increased disease severity.2 While a younger population may be associated with fewer medical comorbidities, the higher severity of liver disease means that medical management will continue to be challenging. Relapse back into alcohol use after LT is a concern in this patient population and younger age has been associated with a higher risk for relapse. Multiple prior attempts at rehabilitation and the presence of overt hepatic encephalopathy may also predict greater odds of relapsing back into alcohol use.34 Attention to these risk factors during patient selection may be key in determining the optimal allocation of scarce donor organs. Encouragingly, 77% of LT recipients can stay abstinent from alcohol or have less serious “slips” that did not affect long-term five-year survival rates. Close surveillance for relapses, especially in the 12-month period after transplant, has been found to be vital since early relapse is directly linked to significantly worse survival. Patients with early relapse have been found to have 5-year survival rates of 50–60%, compared with 95–100% 5-year survival rates in patients who maintained abstinence or only had minor relapses greater than one year after LT. We summarized essential studies regarding LT trends for AUD and ALD in Table 3.
 |
Table 3 Studies on Trends in Liver Transplantation for Alcohol-Related Liver Disease and Alcohol Use Disorder |
Impact on LT Programs
The rising numbers and more complex clinical presentations of the patients now being listed for LT with a prior history of ALD do not bode well for programs that are not adequately prepared. A proportionate reinforcement of trained clinicians must be recruited to deal with the near-certain increase in patient volume. The unique challenges of this patient population are many, foremost being the significant psychosocial component of the underlying AUD. Multidisciplinary cooperation among psychiatrists, addiction medicine specialists, surgeons, social workers, and hepatologists would be the most effective strategy in ensuring patient motivation and continued abstinence from alcohol. While quarterbacking continued graft function and patient survival, hepatologists will need regular lines of communication with mental health specialists to guard against the threat of recidivism. Close relationships may need to be forged with inpatient alcohol rehabilitation centers and intensive outpatient programs to support patients pre- and post-transplant. In an Italian study, the use of a multidisciplinary team of transplant surgeons, gastroenterologists, clinical toxicologists, psychiatrists, and psychologists resulted in a significantly lower prevalence of mortality in the patients that had been evaluated by this team compared to patients that had not undergone this evaluation. Among the patients with a recurrence of their AUD, the multidisciplinary team was able to diagnose these patients earlier and facilitate more rapid intervention in their care.36 Remote healthcare and telemedicine are already becoming powerful tools in healthcare delivery, and programs must fully utilize these modalities to ensure a high standard of care. Advantages include increasing patient convenience, eliminating transportation costs, and minimizing exposure to respiratory-borne illnesses for these post-transplant patients on immunosuppressive medications. Transplant programs may also be able to bring their services more readily to rural areas that are often underserved by medical care. Physicians may opt for briefer but more frequent check-ins with their patients living a greater distance from large metropolitan areas where transplant centers are often based. A broader reach may facilitate increased volumes, provided centers are able to maintain adequate support in all the relevant domains. Several barriers exist to telemedicine which will need to be addressed before LT programs become reliant on this modality. Patient access is frequently a challenge, especially among people less proficient in the use of technology. A clinical examination, even today, plays a vital role in the assessment of a patient and telemedicine may miss relevant clinical information, such as the auscultation of crackles suggesting fluid overload in a patient with impending decompensation of cirrhosis. The costs associated with telemedicine should also be taken into account. HIPAA-compliant telehealth platforms, along with increased need for private teleconference areas and computers equipped with video cameras, are significant financial burdens which smaller programs especially may find limiting.37
Fortunately, outcomes so far after LT for ALD in the COVID-19 era are encouraging. According to a study reviewing United Network for Organ Sharing (UNOS) data, overall one-year survival in liver transplant recipients is higher for ALD than non-ALD both in the pre-COVID-19 era and during the COVID-19 pandemic, despite higher median MELD at listing during the COVID-19 pandemic.38 LT recipients also do not appear to have an increased risk of mortality if they have COVID-19 infection. As pharmacologic immunosuppression does not increase the risk of death in these patients, the degree of immunosuppression does not need to be routinely reduced. On the other hand, the immune dysfunction associated with cirrhosis pre-liver transplant does increase infection-related morbidity and mortality.39 This information may mean that the post-transplant follow-up may be less complicated, though pre-transplant patients will be of higher acuity and more resource-intensive. These features may help programs strategize workforce deployment, possibly by ensuring high staffing levels on inpatient services while maintaining robust outpatient services.
Conclusion
Rising rates of ALD, including the spectrum from alcohol-related cirrhosis to HCC, combined with increasing challenges in care delivery do not bode well for LT programs in the post-COVID-19 era. However, with adequate preparation, the coming wave of patients needing LT may be able to be stemmed. Increasing alcohol consumption in the general population will need to be curtailed at the societal and policymaking level for the benefit of public health. Harnessing the advantages of telemedicine while widely implementing multidisciplinary care, programs may be able to pivot into a better position to face these issues head-on while being able to help even greater numbers of patients. Addressing the root causes of increased alcohol use, such as bolstering mental health programs for the general population, should be mandatory to mitigate the risk of healthcare workforce moral injury. Through compassionate and deft management of finite resources, programs can set themselves up for success in the phases after COVID-19 and beyond.
Abbreviations
LT, liver transplantation; COVID-19, coronavirus disease 2019; AUD, alcohol use disorder; ALD, alcohol-related liver disease; HCC, hepatocellular carcinoma; NAFLD, nonalcoholic fatty liver disease; MELD, Model for End-Stage Liver Disease.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Aijaz Ahmed and Donghee Kim are co-senior authors for this study. The authors report no conflicts of interest in this work.
References
1. Bittermann T, Mahmud N, Abt P. Trends in liver transplantation for acute alcohol-associated hepatitis during the COVID-19 pandemic in the US. JAMA Netw Open. 2021;4(7):e2118713. doi:10.1001/jamanetworkopen.2021.18713
2. Cholankeril G, Goli K, Rana A, et al. Impact of COVID-19 pandemic on liver transplantation and alcohol-associated liver disease in the USA. Hepatology. 2021;74(6):3316–3329. doi:10.1002/hep.32067
3. Moon AM, Curtis B, Mandrekar P, Singal AK, Verna EC, Fix OK. Alcohol-associated liver disease before and after COVID-19—an overview and call for ongoing investigation. Hepatol Commun. 2021;5(9):1616–1621. doi:10.1002/hep4.1747
4. Creswell KG. Drinking together and drinking alone: a social-contextual framework for examining risk for alcohol use disorder. Curr Dir Psychol Sci. 2021;30:19–25. doi:10.1177/0963721420969406
5. Barbosa C, Cowell AJ, Dowd WN. Alcohol Consumption in Response to the COVID-19 Pandemic in the United States. J Addict Med. 2021;15(4):341–344. doi:10.1097/ADM.0000000000000767
6. Slater M, Alpert H. National institute on alcohol abuse and alcoholism. Surveillance Report #119; 2022. Available from: https://pubs.niaaa.nih.gov/publications/surveillance119/CONS20.htm.
7. Renaud-Charest O, Lui LMW, Eskander S, et al. Onset and frequency of depression in post-COVID-19 syndrome: a systematic review. J Psychiatr Res. 2021;144:129–137. doi:10.1016/j.jpsychires.2021.09.054
8. Kilian C, Rehm J, Allebeck P, et al. Alcohol consumption during the COVID-19 pandemic in Europe: a large-scale cross-sectional study in 21 countries. Addiction. 2021;116(12):3369–3380. doi:10.1111/add.15530
9. Pollard MS, Tucker JS, Green HD. Changes in adult alcohol use and consequences during the COVID-19 Pandemic in the US. JAMA Netw Open. 2020;3(9):e2022942.
10. Holzhauer CG, Cucciare M, Epstein EE. Sex and gender effects in recovery from alcohol use disorder. Alcohol Res Curr Rev. 2020;40(3):03. doi:10.35946/arcr.v40.3.03
11. Rogers JP, Chesney E, Oliver D, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7(7):611–627. doi:10.1016/S2215-0366(20)30203-0
12. Tsai J, Elbogen EB, Huang M, North CS, Pietrzak RH. Psychological distress and alcohol use disorder during the COVID-19 era among middle- and low-income U.S. adults. J Affect Disord. 2021;288:41–49. doi:10.1016/j.jad.2021.03.085
13. Barrio P, Baldaquí N, Andreu M, et al. Abstinence among alcohol use disorder patients during the COVID-19 pandemic: insights from Spain. Alcohol Clin Exp Res. 2021;45(4):802–807. doi:10.1111/acer.14555
14. Rutledge SM, Schiano TD, Florman S, Im GY. COVID-19 aftershocks on alcohol-associated liver disease: an early cross-sectional report from the U.S. Epicenter Hepatol Commun. 2021;5(7):1151–1155. doi:10.1002/hep4.1706
15. Itoshima H, ho SJ, Takada D, Morishita T, Kunisawa S, Imanaka Y. The impact of the COVID-19 epidemic on hospital admissions for alcohol-related liver disease and pancreatitis in Japan. Sci Rep. 2021;11(1):14054. doi:10.1038/s41598-021-92612-2
16. Kim D, Perumpail BJ, Wijarnpreecha K, Manikat R, Cholankeril G, Ahmed A. Trends in aetiology-based hospitalisation for cirrhosis before and during the COVID-19 pandemic in the United States. Aliment Pharmacol Ther. 2023;58(2):218–228. doi:10.1111/apt.17547
17. Chen P-H, Ting P-S, Almazan E, Chander G, Cameron AM, Gurakar A. Inter-hospital escalation-of-care referrals for severe alcohol-related liver disease with recent drinking during the COVID-19 pandemic. Alcohol Alcoholism. 2022;57(2):185–189. doi:10.1093/alcalc/agab047
18. Julien J, Ayer T, Tapper EB, Barbosa C, Dowd WN, Chhatwal J. Effect of increased alcohol consumption during COVID-19 pandemic on alcohol-associated liver disease: a modeling study. Hepatology. 2022;75(6):1480–1490. doi:10.1002/hep.32272
19. Calvey T, Scheibein F, Saad NA, et al. the changing landscape of alcohol use and alcohol use disorder during the COVID-19 pandemic - perspectives of early career professionals in 16 countries. J Addict Med. 2020;14(6):e284. doi:10.1097/ADM.0000000000000735
20. Lear-Claveras A, González-álvarez B, Couso-Viana S, Clavería A, Oliván-Blázquez B. Analysis of clinical parameters, drug consumption and use of health resources in a southern European population with alcohol abuse disorder during COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(3):1358. doi:10.3390/ijerph19031358
21. Kim JU, Majid A, Judge R, et al. Effect of COVID-19 lockdown on alcohol consumption in patients with pre-existing alcohol use disorder. Lancet Gastroenterol Hepatol. 2020;5(10):886–887. doi:10.1016/S2468-1253(20)30251-X
22. Meza V, Arnold J, Díaz LA, et al. Alcohol consumption: medical implications, the liver and beyond. Alcohol Alcohol. 2022;57(3):283–291. doi:10.1093/alcalc/agac013
23. Kim D, Perumpail BJ, Alshuwaykh O, Dennis BB, Cholankeril G, Ahmed A. Changing trends in aetiology-based hospitalizations with end-stage liver disease in the United States from 2016 to 2019. Liver Int. 2022;42(11):2390–2395. doi:10.1111/liv.15381
24. Crews FT, Bechara R, Brown LA, et al. Cytokines and Alcohol. Alcohol Clin Exp Res. 2006;30(4):720–730. doi:10.1111/j.1530-0277.2006.00084.x
25. Marano G, Traversi G, Gaetani E, Pola R, Claro AE, Mazza M. Alcohol use disorder and liver injury related to the COVID-19 pandemic. World J Hepatol. 2022;14(10):1875–1883. doi:10.4254/wjh.v14.i10.1875
26. Yeo YH, Zou B, Cheung R, Nguyen MH. Increased mortality of patients with alcohol-related liver diseases during the COVID-19 pandemic in the United States. J Intern Med. 2022;292(5):837–839. doi:10.1111/joim.13545
27. Kim D, Manikat R, Cholankeril G, Ahmed A. Trends in mortality of liver cancer before and during the COVID-19 pandemic, 2017–2021. Liver Int. 2023;43(9):1865–1870. doi:10.1111/liv.15668
28. Kim D, Adeniji N, Latt N, et al. Predictors of Outcomes of COVID-19 in patients with chronic liver disease: US multi-center study. Clin Gastroenterol Hepatol. 2021;19(7):1469–1479.e19. doi:10.1016/j.cgh.2020.09.027
29. Marjot T, Moon AM, Cook JA, et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: an international registry study. J Hepatol. 2021;74(3):567–577. doi:10.1016/j.jhep.2020.09.024
30. Kim D, Alshuwaykh O, Dennis BB, Cholankeril G, Ahmed A. Trends in etiology-based mortality from chronic liver disease before and during COVID-19 pandemic in the United States. Clin Gastroenterol Hepatol. 2022;20(10):2307–2316.e3. doi:10.1016/j.cgh.2022.05.045
31. Cholankeril G, Ahmed A. Alcoholic liver disease replaces hepatitis C virus infection as the leading indication for liver transplantation in the United States. Clin Gastroenterol Hepatol. 2018;16(8):1356–1358. doi:10.1016/j.cgh.2017.11.045
32. Asrani SK, Trotter J, Lake J, et al. Meeting report: the Dallas consensus conference on liver transplantation for alcohol associated hepatitis. Liver Transpl. 2020;26(1):127–140. doi:10.1002/lt.25681
33. Herrick-Reynolds KM, Punchhi G, Greenberg RS, et al. Evaluation of early vs standard liver transplant for alcohol-associated liver disease. JAMA Surg. 2021;156(11):1026–1034. doi:10.1001/jamasurg.2021.3748
34. Lee BP, Im GY, Rice JP, et al. Patterns of alcohol use after early liver transplantation for alcoholic hepatitis. Clin Gastroenterol Hepatol. 2022;20(2):409–418.e5. doi:10.1016/j.cgh.2020.11.024
35. Lee BP, Dodge JL, Terrault NA. Liver transplant for alcohol-associated liver disease continues to rise 2 years into the COVID-19 pandemic especially among young adults. J Hepatol. 2022;1:1.
36. Magistri P, Marzi L, Guerzoni S, et al. Impact of a multidisciplinary team on alcohol recidivism and survival after liver transplant for alcoholic disease. Transplant Proc. 2019;51(1):187–189. doi:10.1016/j.transproceed.2018.02.212
37. Kichloo A, Albosta M, Dettloff K, et al. Telemedicine, the current COVID-19 pandemic and the future: a narrative review and perspectives moving forward in the USA. Fam Med Community Health. 2020;8(3):e000530. doi:10.1136/fmch-2020-000530
38. Goli K, Lymberopoulos P, Samuel R, et al. Post-transplant outcomes for alcohol-associated liver disease during the COVID-19 pandemic. Liver Transpl. 2023;29(7):777. doi:10.1097/LVT.0000000000000113
39. Marjot T, Webb GJ, Barritt AS, et al. COVID-19 and liver disease: mechanistic and clinical perspectives. Nat Rev Gastroenterol Hepatol. 2021;18(5):348–364. doi:10.1038/s41575-021-00426-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.