")
Back to Journals » International Journal of Women's Health » Volume 16
The High Sensitivity of the Multi-Cancer Detection Test ONCOVERYX-F Offers a Promising Platform for Ovarian Cancer Screening
Authors Nagarkar R, Gopichand M, Pal SK , Gupta A, Saquib NM, Sagar G, Rao KV , Siddiqui Z , Longkumer I
Received 11 October 2023
Accepted for publication 28 December 2023
Published 3 January 2024 Volume 2024:16 Pages 1—7
DOI https://doi.org/10.2147/IJWH.S444258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Rajnish Nagarkar,1 Mamillapalli Gopichand,2 Suparna Kanti Pal,3 Ankur Gupta,4,5 Najmuddin Mohd Saquib,4,5 Ganga Sagar,4 Kanury VS Rao,4,5 Zaved Siddiqui,4,5 Imliwati Longkumer6
1Surgical Oncology, HCG Manavta Cancer Centre, Nashik, Maharashtra, India; 2Surgical Oncology, HealthCare Global Enterprises Limited, Vijayawada, India; 3Radiotherapy, Indoriv Clinical, Kolkata, India; 4Research and Development Section, PredOmix Technologies Private Limited, Gurugram, India; 5Research and Development Section, PredOmix Health Sciences Private Limited, Singapore; 6Biochemistry, North East Cancer Hospital and Research Institute, Guwahati, Assam, India
Correspondence: Imliwati Longkumer; Zaved Siddiqui, Email [email protected]; [email protected]
Abstract: We evaluated the potential relevance of our multi-cancer detection test, OncoVeryx-F, for ovarian cancer screening. For this, we compared its accuracy with that of CA125-based screening. We demonstrate here that, in contrast to CA125-based detection, OncoVeryx-F detected ovarian cancer with very high sensitivity and specificity. Importantly here, Stage I cancers too could be detected with an accuracy of > 98%. Furthermore, again unlike CA 125, the detection accuracy of OncoVeryx-F remained comparable in both Caucasian and South Asian/Indian women. Thus, the robustness and accuracy of OncoVeryx-F, particularly for early-stage detection, underscores its potential utility for ovarian cancer screening.
Keywords: CA 125, Oncoveryx-F, OvC, NoC, LC-MS/MS
Introduction
Although the 5-year survival rate for Stage I and II OvC is close to 90%, the overall 5-year survival rate currently averages to only about 45%. This is because most OvC cases are only diagnosed in the late stage when the survival rate drops to just about 20–40%.1–4 Consequently, early detection – especially in the pre-symptomatic stages where prognosis is more favorable – is critical for women with OvC. Presently, the serum tumor marker cancer antigen 125 (CA125) is widely used for OvC screening in symptomatic women presenting to primary care.5 Its limited accuracy, however, has so far precluded its more general use in population-based screening for OvC.5–7 Clinical interpretation based on CA125 levels is also complicated by the fact that these levels naturally fluctuate in a variety of conditions. In addition to tumor subtype and tumor burden,8–10 benign conditions such as age, BMI, ethnicity, and menopausal status also cause variability in baseline CA125 levels.11–14 Further, about 20% of women with OvC do not express any circulating CA125, which then limits the maximal achievable sensitivity to 80%.15–17
We had previously developed a non-invasive, serum-based, method for simultaneous detection of the four female-specific cancers of the breast, endometrium, cervix, and ovary.18 We named this method as OncoVeryx-F, which integrates untargeted serum metabolomics with AI-powered analytics to detect metabolite signatures that are specific to cancer.18 This method could detect all four cancers with an overall sensitivity of 98% and specificity of 98.3%.18 Especially pertinent here was that this detection accuracy was also maintained for Stage-0 and Stage-I cancers,18,19 thus highlighting the relevance of OncoVeryx-F for early-stage detection of the four female-specific cancers, including OvC. Given this potential, and its implications for OvC screening, we wanted to evaluate how the performance of OncoVeryx-F compared with that of CA125, the currently employed serum biomarker for OvC screening. Our results demonstrate that, as compared to CA125 which yielded relatively poor sensitivity and specificity, OncoVeryx-F provided a highly accurate method for early-stage OvC detection. Importantly, OncoVeryx-F was equally effective in both Caucasian and South Asian/Indian women, underscoring its potential as a new platform for early-stage OvC screening.
Methods
Details of the Serum Samples Employed
Of the 370 OvC serum samples and 731 normal control (NoC) samples used for this study, 186 OvC samples and 298 NoC samples were purchased from two commercial biobanks: Dx Biosamples (San Diego, CA) and Reprocell USA Inc. (Beltsville, MD). These samples had all been obtained from Caucasian donors. The remaining samples (184 OvC samples and 433 NoC samples) were obtained through an investigator-initiated retrospective observational study (CTRI/2023/03/050316). Samples were collected from volunteers across north-eastern and central India, after obtaining written informed consent from them. For the OvC group, samples were taken only from histopathologically confirmed adults (between 20 and 90 yrs), prior to either surgery or chemotherapy. Individuals with either high-grade dysplasia, autoimmune diseases, or CKD were excluded from the study.
Determination of CA 125 Levels in Patient Sera
CA 125 levels were determined by Chemiluminescence Immunoassay (CLIA) detection using the ARCHITECT CA 125 II system (Abbot).
Profiling of the Serum Metabolome and Data Analysis for Identification of OvC-Positive Samples (OncoVeryx-F)
Extraction of metabolites from serum and subsequent untargeted metabolome profiling by liquid chromatography with tandem mass spectrometry was done as previously described.18 The resulting data was analyzed using our previously developed AI model to distinguish OvC samples from normal controls.18 This model generates y-scores for each sample where a y-score of >0 denotes a cancer-positive status while a y-score of <0 indicates the absence of cancer. Sensitivity, Specificity, and Accuracy were calculated from the below formulae:
Accuracy: (TP+TN)/(TP+TN+FP+FN)
Sensitivity: TP/(TP+FN)
Specificity: TN/(TN+FP).
Results
Samples Employed in the Present Study
Table 1 describes the serum sample set used in this study, along with their distribution across the various age groups. Supplementary Table 1 provides a more detailed description of each OvC sample including the stage of cancer, ethnicity, age, and BMI of the donor. In addition, the serum CA 125 levels determined, as well as the y-scores obtained from the OncoVeryx-F test are also included. Supplementary Table 2 lists the NoC samples along with the age and ethnicity of the donor, along with the CA 125 levels and y-scores as determined by OncoVeryx-F. The overall participant flow through the study is depicted in the STARD 2015 flowchart shown in Figure 1.
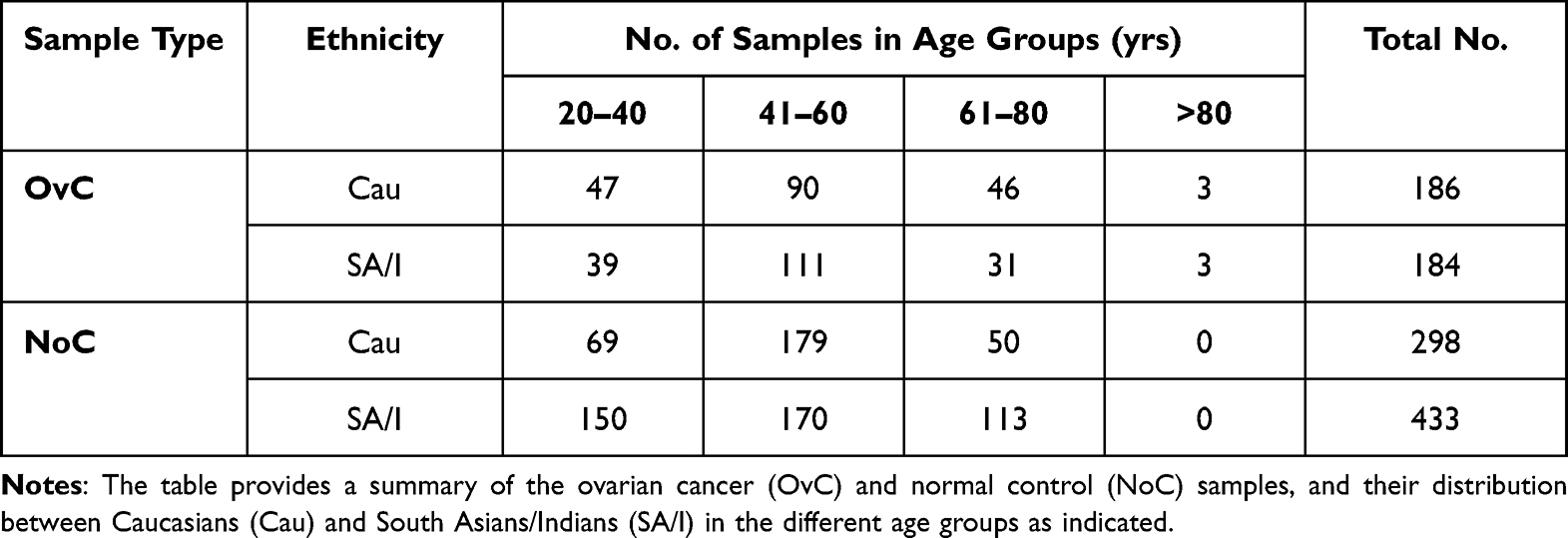 |
Table 1 The Sample Set Employed for the Study |
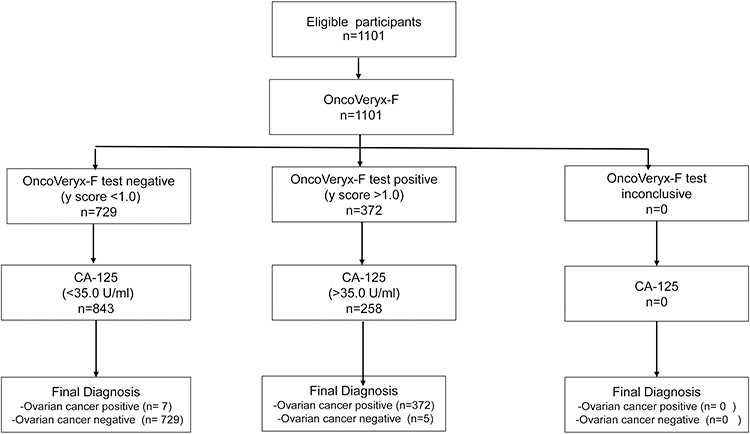 |
Figure 1 STARD diagram to report flow of participants through the study. |
A Comparison of OvC Detection Accuracy Between OncoVeryx-F and That Based on CA 125 Levels
Figure 2A shows the confusion matrix that was generated after analysis of the metabolome data of OvC and NoC samples by the OncoVeryx-F protocol.18,19 As is evident, of the 370 OvC samples tested, 5 were falsely identified as OvC-negative whereas 7 of the 731 NoC samples were misidentified as false positives. The sensitivity was calculated to be 98.6% and the specificity was 99.0%.
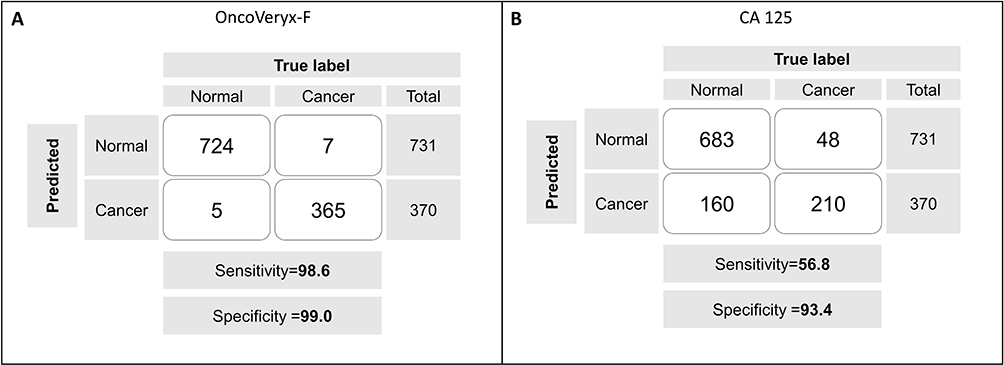 |
Figure 2 A comparison of the efficacies of OncoVeryx-F and CA 125-based testing for OvC detection. (A) Shows the confusion matrix generated from the y-scores estimated by OncoVeryx-F for the individual OvC and NoC samples. The sensitivity obtained was 98.6% (96.41, 100) at 95% CI, at a specificity of 99.03% (97.08, 100) at 95% CI, and the accuracy was 98.85% (97.32, 100) at 95% CI. (B) Shows the corresponding matrix obtained when OvC versus NoC discrimination was derived on the basis of the CA 125 cut-off level of 35 U/mL. The sensitivity and specificity obtained in each case is also given here. |
Figure 2B depicts the confusion matrix obtained when serum CA 125 levels, at the cut-off value of >35 U/mL,5,20,21 were used to discriminate between OvC and NoC samples. While 48 of the 731 NoC samples were mis-designated as OvC-positive, as many as 160 of the 370 OvC samples were also missed by this criterion. This resulted in a sensitivity and specificity of 56.8% and 93.4%, respectively. Thus, Figure 2 demonstrates that the detection accuracy of OncoVeryx-F for OvC is far superior to that of the currently used CA 125-based diagnosis.6,7
Efficacy of OncoVeryx-F is Comparable Between Caucasian and South Asian/Indian Women
Of the multitude of benign conditions that influence serum CA 125 levels, race is one such independent predictor.14 For example, African and Asian women were found to have lower levels of CA 125 when compared to Caucasian women.14 Since our present sample set was comprised of donors from two ethnic groups – Caucasian and South Asian/Indian – we thought it pertinent to assess how OncoVeryx-F performed in these two groups, in comparison to CA 125.
A comparison of the distribution of CA 125 levels in the OvC and NoC sample sets revealed that the spread across higher CA 125 concentrations was significantly greater in the Caucasian as opposed to the Indian OvC group (Figure 3). The mean CA 125 concentration obtained for the Caucasian OvC group (332 U/mL) was over 2-fold higher than that for the Indian OvC sample set (161.5 U/mL, Figure 3). Importantly, as many as 127 out of the 184 Indian OvC samples had CA 125 levels of <35 U/mL. In contrast, the proportion of OvC samples with CA 125 levels below the cut-off value in the Caucasian group was only 33 out of 186 samples. With respect to the NoC samples, however, the mean CA 125 concentration for Indian women was marginally higher than that for the Caucasian group (22.9 U/mL versus 15.8 U/mL) (Figure 3). These results suggest that, in comparison with their Caucasian counterparts, a significantly higher proportion of Indian women with OvC have CA 125 levels that are lower than the cut-off value for OvC diagnosis.
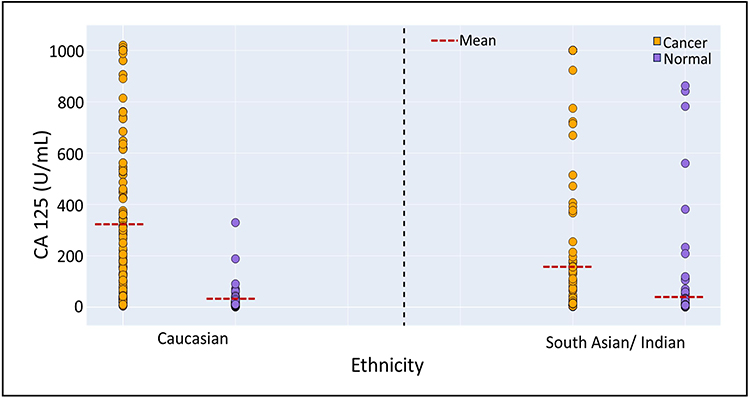 |
Figure 3 Ethnicity-dependence of the performance of CA 125 and OncoVeryx-F for OvC detection. Shows the distribution of CA 125 concentrations in samples from the OvC and NoC groups in both Caucasian and South Asian/Indian women. |
The sensitivity and specificity of the CA 125-based analysis, calculated from Figure 3, is summarized in Table 2. As expected, the results varied markedly between the two ethnic groups. For samples from Caucasian women, the sensitivity and specificity obtained was 83.7% and 92.8%, respectively. The sensitivity, however, dropped to only 32.8% for South Asian/Indian women although the specificity remained relatively unchanged (Table 2). These latter results are consistent with the previous findings that CA 125-based detection performs poorly in Indian OvC patients and that this test is of dubious value, contributing only to patient anxiety and clinical uncertainty.22 Importantly, in contrast to the results with CA 125, the performance of OncoVeryx-F remained relatively constant across both ethnic groups yielding a sensitivity and specificity of >98% in both cases. The specificity obtained in South Asian/Indian women (99.5%) was, however, marginally higher than that obtained in Caucasian women (98.3%, Figure 3). Thus, while the results in Figure 3 underscore a vulnerability of CA 125 as a screening tool for OvC, they also highlight the marked resilience of the OncoVeryx-F test in terms of maintaining its high accuracy across at least the two ethnic groups tested.
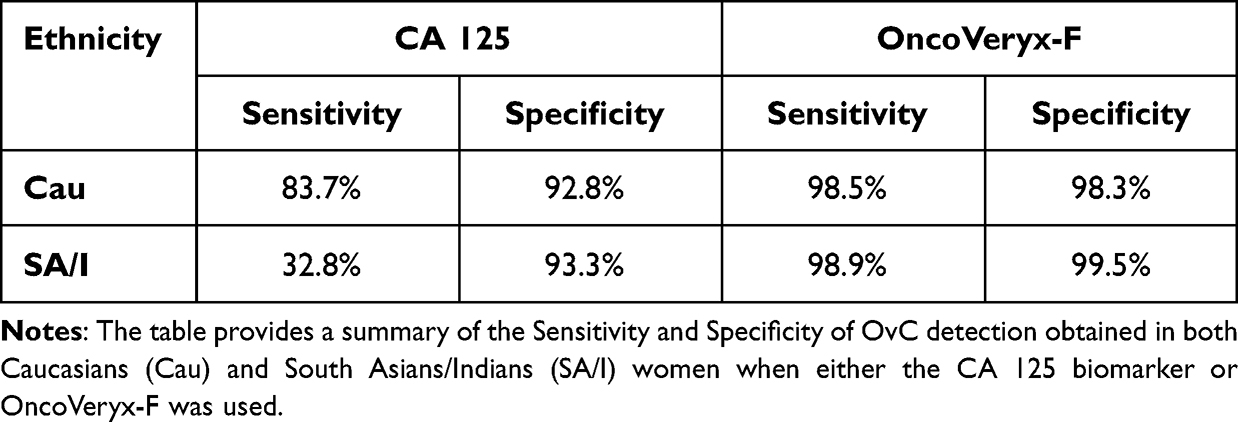 |
Table 2 Ethnicity-Dependant OvC-Detection Accuracy of CA 125 and OncoVeryx-F Test |
OncoVeryx-F Detects Stage I OvC with High Accuracy
Given the importance of early-stage OvC detection, we were interested in specifically evaluating how OncoVeryx-F performed in the detection of Stage I OvC. We were able to assess this with some degree of confidence because, of the 370 OvC samples employed in this study, 208 were obtained from women in Stage I of the disease (Supplementary Table 1). Of these, the majority (185) were from Caucasian women whereas the remaining 23 samples were from Indian donors. We performed a comparative analysis of the sensitivity and specificity of OncoVeryx-F with that of CA 125-based testing, when discriminating between OvC and NoC. In this exercise, all 731 NoC samples were taken for the estimation of specificity. The results obtained are shown in terms of the confusion matrices generated in Figure 4. Panel A of this figure shows the results obtained with OncoVeryx-F where the sensitivity and specificity were calculated to be 98.6% and 99.1%, respectively. In contrast, CA 125-based discrimination yielded a sensitivity of 77.4% and a specificity of 93.4% (Figure 4B). Thus, OncoVeryx-F offers a far more accurate method for early-stage OvC detection when compared to the CA 125-based test.
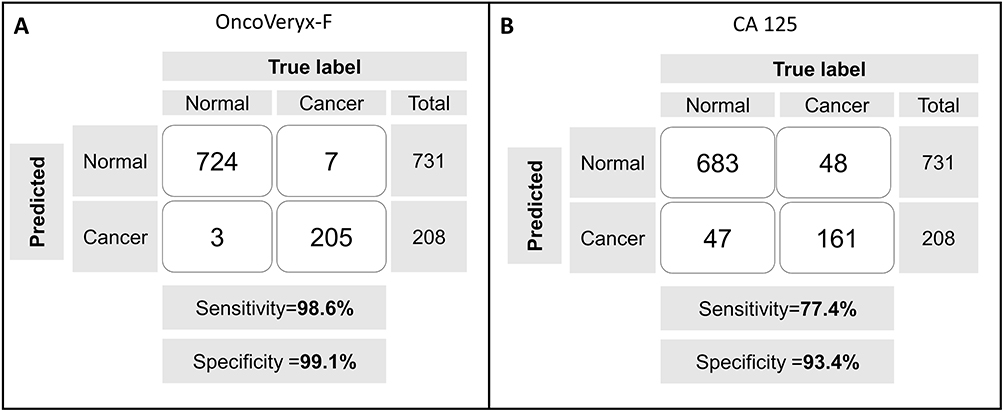 |
Figure 4 Comparative efficacy of Stage I OvC detection by OncoVeryx-F and CA 125. Shown here are the confusion matrices obtained for detection of Stage I OvC samples using either OncoVeryx-F (A) or CA 125 (B) as the test system. |
Discussion
Because about 70% of women with OvC are diagnosed only at the advanced stage, this cancer has emerged as the fifth-leading cause of cancer deaths in women between the ages of 35 to 74.1,23,24 While this underscores the need for early-stage OvC detection, CA125 is the only tumor marker currently recommended for clinical use in the diagnosis and management of OvC.5–8 However, its poor detection sensitivity and specificity precludes the use of CA 125 as a screening test.25 Alternate methods for accurate early-stage detection are, therefore, warranted to reduce the OvC morbidity and mortality.
We demonstrate here that OncoVeryx-F was relatively unhindered by at least some of the handicaps associated with CA 125-based screening and can, therefore, potentially provide a far superior option for early-stage OvC screening. In this context, our observation that the accuracy of OncoVeryx-F remained relatively invariant regardless of whether the test population was Caucasian or South Asian/Indian women is a particularly significant finding. This was in contrast CA 125-based testing where the OvC detection sensitivity was profoundly dependent on ethnicity of the test population. Although a broader range of ethnicities remain to be tested, these initial results suggest that OncoVeryx-F could serve as a more amenable screening test, at least in comparison with CA 125.
While the superior OvC detection accuracy of OncoVeryx-F relative to CA 125-based testing is one of the key findings of our current report, a particularly noteworthy aspect here is that the high sensitivity of >98% and specificity of >99% was also retained for samples from Stage I of the cancer. Here again the test samples were comprised of sera from both Caucasian and South Asian/Indian donors. Thus, our present results highlight the promise of further developing OncoVeryx-F as a possible screening test for OvC.
Conclusion
Because of its poor accuracy, CA 125-based screening cannot be employed to achieve the goal of reducing OvC mortality. This was highlighted in a recent report from the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS), which showed that despite the 47.2% increase in detection at Stage I obtained with CA 125 screening, there was no significant reduction in OvC deaths.26 It was inferred that a much higher accuracy of early-stage OvC was needed to achieve a large enough shift from late- to early-stage detection that can reduce OvC-related deaths.26 Here, given that OncoVeryx-F can detect Stage I OvC with an accuracy of >98%, it will be of interest to explore whether this test can serve as a high-fidelity screening test that can contribute to reducing OvC mortality.
Data Sharing Statement
Individual deidentified participant data will be available for six months from date of publication of the corresponding author.
Details of Ethics Approval
The study was approved by the Institutional Ethics Committee at North East Cancer Hospital and Research Institute (reference number IEC/04/06/2022) and Health Point Ethics Committee at Health Point Hospital (reference number HP/EC/APVL/22-23/011 dt. 19/may/2022), in accordance with the Declaration of Helsinki.
Author Contributions
All Authors made significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspect of the work.
Disclosure
AG, GS, ZS, NMS and KVSR are fulltime employees of PredOmix Technologies Private Limited. KVSR is a cofounder and owns stock in both PredOmix Technologies Private Limited and PredOmix Health Sciences Pte. Ltd. AG, ZS, and NMS own stock in PredOmix Health Sciences Pte. Ltd. SP is one of the Principal Investigators in studies sponsored by Predomix Technologies. The work described in this report is included in an Indian Provisional Patent Application filing. Application No. 202311002270. The authors report no other conflicts of interest in this work.
References
1. Hennesy BT, Coleman RL, Markman M. Ovarian Cancer. Lancet. 2009;374:1371–1382.
2. Zeppernick F, Meinhold-Heerlein I, Meinhold-Heerlien AI. The new FIGO staging system for ovarian, fallopian tube, and primary peritoneal cancer. Arch Gynecol Obs. 2014;290:839–842. doi:10.1007/s00404-014-3364-8
3. Schiavone MB, Herzog TJ, Lewin SN, et al. Natural history and outcome of mucinous carcinoma of the ovary. Am J Obstet Gynecol. 2011;205:
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021. doi:10.3322/caac.21660
5. Charkhchi P, Cybulski C, Gronwald J, et al. CA125 and ovarian cancer: a comprehensive review. Cancers. 2020;12(12):3730. doi:10.3390/cancers12123730
6. Clarke-Pearson DL. Clinical practice. Screening for ovarian cancer. N Engl J Med. 2009;361:170–177. doi:10.1056/NEJMcp0901926
7. Jacobs I, Prys Davies A, Bridges J, et al. Prevalence screening for ovarian cancer in postmenopausal women by CA 125 measurement and ultrasonography. Br J Med. 1993;306(6884):1030–1034. doi:10.1136/bmj.306.6884.1030
8. Bast RC, Klug TL, John ES, et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Eng J Med. 1983;309(15):883–887. doi:10.1056/NEJM198310133091503
9. Kobel M, Kalloger SE, Boyd N, et al. Ovarian carcinoma subtypes are different diseases: implications for biomarker studies. PLoS Med. 2008;5:1749–1760.
10. Zanaboni F, Vergadoro F, Presti M, et al. Tumor antigen CA125 as a marker of ovarian epithelial carcinoma. Gynecol Oncol. 1987;28:61–67.
11. Skates SJ, Mai P, Horick NK, et al. Large prospective study of ovarian cancer screening in high-risk women: CA125 cut-point defined by menopausal status. Cancer Prev Res. 2011;4:1401–1408. doi:10.1158/1940-6207.CAPR-10-0402
12. Urban N, Thorpe J, Karlan BY, et al. Interpretation of single and serial measures of HE4 and CA125 in asymptomatic women at high risk for ovarian cancer. Cancer Epidemiol. 2012;21:2087–2094.
13. Erbagci AB, Yilmaz N, Kutlar I. Menstrual cycle dependent variability for serum tumor markers CEA, AFP, CA 19-9, CA125 and CA 15-3 in healthy women. Dis Markers. 1999;15:259–267. doi:10.1155/1999/960934
14. Pauler DK, Menon U, Mcintosh M, et al. Factors influencing serum CA125II levels in healthy postmenopausal women. Cancer Epidemiol Biomark Prev. 2001;10:489–493.
15. Sopik V, Rosen B, Giannakeas V, Narod SA. Why have ovarian cancer mortality rates declined? Part III. Prospects for the future. Gynecol Oncol. 2015;138:757–761. doi:10.1016/j.ygyno.2015.06.019
16. Rosen DG, Wang L, Atkinson JN, et al. Potential markers that complement expression of CA125 in epithelial ovarian cancer. Gynecol Oncol. 2005;99:267–277.
17. Akinwunmi BO, Babuc A, Vitonis AF, et al. Chronic medical conditions and CA125 levels among women without ovarian cancer. Cancer Epidemiol Biomark Prev. 2018;27:1483–1490. doi:10.1158/1055-9965.EPI-18-0203
18. Gupta A, Sagar G, Siddiqui Z, et al. A non-invasive method for concurrent detection of early-stage women specific cancers. Sci Rep. 2022;12:2301. doi:10.1038/s41598-022-06274-9
19. Ramamoorthy S, Sundaramoorthy S, Gupta A, et al. Beta-validation of a non-invasive method for simultaneous detection of early-stage female-specific cancers. Biol Med. 2023;15:1. doi:10.35248/0974-8369.23.15.610
20. Felder M, Kapur A, Gonzalez-Bosquet J, et al. MUC16 (CA125): tumor biomarker to cancer therapy, a work in progress. Mol Cancer. 2014;13:1
21. Funston G, Hamilton W, Abel G, et al. The diagnostic performance of CA125 for the detection of ovarian and non-ovarian cancer in primary care: a population-based cohort study. PLoS Med. 2020;17(10):e1003295. doi:10.1371/journal.pmed.1003295
22. Gupta R, Mahajan S, Kaur S, et al. Demographic profile, staging and CA-125 levels in a patient with pelvic lesions of probable ovarian origin at presentation in a tertiary care hospital. Int J Adv Med. 2021;8:662–666. doi:10.18203/2349-3933.ijam20211472
23. Khazael Z, Namayandeh SM, Beiranvand R, et al. Worldwide incidence and mortality of ovarian cancer and Human Development Index (HDI): GLOBOCAN sources and methods. J Prev Med Hyg. 2021;62:E174–E184.
24. Scholler N, Urban N. CA125 in ovarian cancer. Biomarker Med. 2007;1:513–523. doi:10.2217/17520363.1.4.513
25. Hellström I, Raycraft J, Hayden-Ledbetter M, et al. The HE4 (WFDC2) protein is a biomarker for ovarian carcinoma. Cancer Res. 2003;63:3695–3700.
26. Menon U, Gentry-Maharaj A, Burnell M, et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): a randomised controlled trial. Lancet. 2021;397(10290):2182–2193. doi:10.1016/S0140-6736(21)00731-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.