")
Back to Journals » Psoriasis: Targets and Therapy » Volume 12
The Effect of Lifestyle Changes on Disease Severity and Quality of Life in Patients with Plaque Psoriasis: A Narrative Review
Authors van Acht MR, van den Reek JMPA , de Jong EMGJ , Seyger MMB
Received 3 February 2022
Accepted for publication 31 March 2022
Published 9 April 2022 Volume 2022:12 Pages 35—51
DOI https://doi.org/10.2147/PTT.S294189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Uwe Wollina
Maartje R van Acht, Juul MPA van den Reek, Elke MGJ de Jong, Marieke MB Seyger
Department of Dermatology, Radboud University Medical Center (Radboudumc), Nijmegen, the Netherlands
Correspondence: Maartje R van Acht, Department of Dermatology, Radboud University Medical Center (Radboudumc), Mailbox 9101 6500 HB, Nijmegen, the Netherlands, Tel +31 24 36 10265, Fax +31 24 36 35122, Email [email protected]
Objective: To evaluate the effect of lifestyle changes on the severity of psoriasis and the quality of life in patients with psoriasis.
Methods: For this narrative review, PubMed, Embase and ClinicalTrials.gov were searched for lifestyle intervention studies with an intervention duration of at least 12 weeks.
Results: Thirty-four intervention studies were included. Most studies performed interventions in the diet of patients with psoriasis (n=9), or added supplements to the diet (n=18). Three studies comprised relaxation techniques and four studies combined relaxation or stress-reducing techniques with an educational program or exercise. No interventional studies were carried out regarding smoking, alcohol and sleep. Especially dietary and relaxation interventions showed promising results with respect to psoriasis severity and dermatology-related QoL, respectively. Regarding dietary supplements, the three largest studies investigating fish oil or vitamin D did not show significant effects.
Conclusion: There is some evidence that dietary and relaxation interventions could be promising with respect to psoriasis severity and dermatology-related QoL, respectively. Furthermore, our review identified important gaps in psoriasis lifestyle research regarding study design and reporting of outcomes.
Keywords: psoriasis, lifestyle, health, severity, diet, exercise
Introduction
Psoriasis is a chronic inflammatory skin disease with a prevalence of 2–4% in western countries, of which plaque psoriasis is present in 80% of the patients.1,2 Psoriasis is associated with multiple comorbidities, such as obesity, type 2 diabetes mellitus and cardiovascular disease.3,4 These comorbidities can be influenced by lifestyle, such as an unhealthy diet or physical inactivity.3–6 Psoriasis is significantly associated with current smoking7 and an association is suggested between smoking more cigarettes and more severe psoriasis.8 Alcohol consumption is higher in patients with psoriasis compared to the general population.9,10 In studies, patients with psoriasis performed less vigorous physical activity compared to patients without psoriasis.11 A negative correlation was found between the Psoriasis Area and Severity Index (PASI) and physical activity in women,12 whilst another study did not find a correlation between PASI and physical exercise.13 Stress might be associated with a more severe psoriasis14; however, other studies did not find a correlation between PASI and stress severity.13,15 In patients with psoriasis, decreased quality of sleep occurred significantly more frequently compared to subjects without psoriasis.16,17 The correlation between sleep quality and the PASI was investigated in several studies and showed contradictory results.16–18 Especially in diabetes and cardiovascular diseases, lifestyle interventions have been proven to limit disease severity.19–21 In psoriasis, the influence of lifestyle on disease severity is getting more attention in literature and on social media. In 2019, a Cochrane systematic review showed that a low-caloric diet may positively impact the severity of psoriasis and the quality of life (QoL) of patients with psoriasis.22
In the current review, the influence of lifestyle changes on the severity of psoriasis and the QoL of patients with psoriasis will be described. This review provides an update of the available literature and, in addition to the lifestyle Cochrane review of Ko et al, other interventional study designs, apart from Randomized Controlled Trials (RCTs) will be reviewed. In addition to Ko et al, interventional studies on dietary supplements and relaxation will be discussed. The following six lifestyle domains will be investigated: diet, relaxation, exercise, smoking, alcohol and sleep.
Methods
Search Strategy
In this narrative review, PubMed, Embase and ClinicalTrials.gov were searched from inception to August 19, 2021. The search term psoriasis was combined with terms for all six lifestyle domains (diet, relaxation, exercise, smoking, alcohol and sleep) and terms related to lifestyle such as “nutrition”, “health promotion” and ‘weight loss’. A detailed description of the performed literature search is depicted in Supplement 1 Table S1. Duplicates were removed before screening the articles on title and abstract. Hereafter, studies were reviewed based on full text. Additional studies were found through citing and screened on full text as well.
In- and Exclusion Criteria
English or Dutch studies investigating the effect of a lifestyle intervention in any of the six lifestyle domains in patients with psoriasis vulgaris were included. A quantifiable disease severity outcome measure (eg, PASI, Body Surface Area (BSA), % total clearance) or QoL measure (eg, Dermatology Life Quality Index (DLQI)) had to be present. Only studies with an intervention duration of at least 12 weeks were included, which is the duration of short-term clinical trials in psoriasis and is in line with the review of Ko et al.22,23 Pilot studies, non-blinded studies and RCTs were reviewed. Studies investigating patients with psoriatic arthritis as main diagnosis and case reports were excluded.
Results
In total, 34 studies were included in this review. A flow diagram depicting the selection process of the articles included in this review is shown in Figure 1. After title and abstract screening, 142 studies were included, of which 108 studies were excluded based on full text for the following reasons: intervention duration less than 12 weeks, no quantifiable severity or QoL outcome measure, another type of psoriasis than plaque psoriasis/psoriasis vulgaris, and patients with psoriatic arthritis as main diagnosis. Two studies were excluded since the intervention was only for patients with psoriasis using lithium24 or having antibodies to gliadin.25 The 34 included studies are shown in evidence Table 1. Evidence on the effects of changes in the lifestyle domains smoking, alcohol and sleep on the severity of psoriasis or QoL in patients with psoriasis was not found.
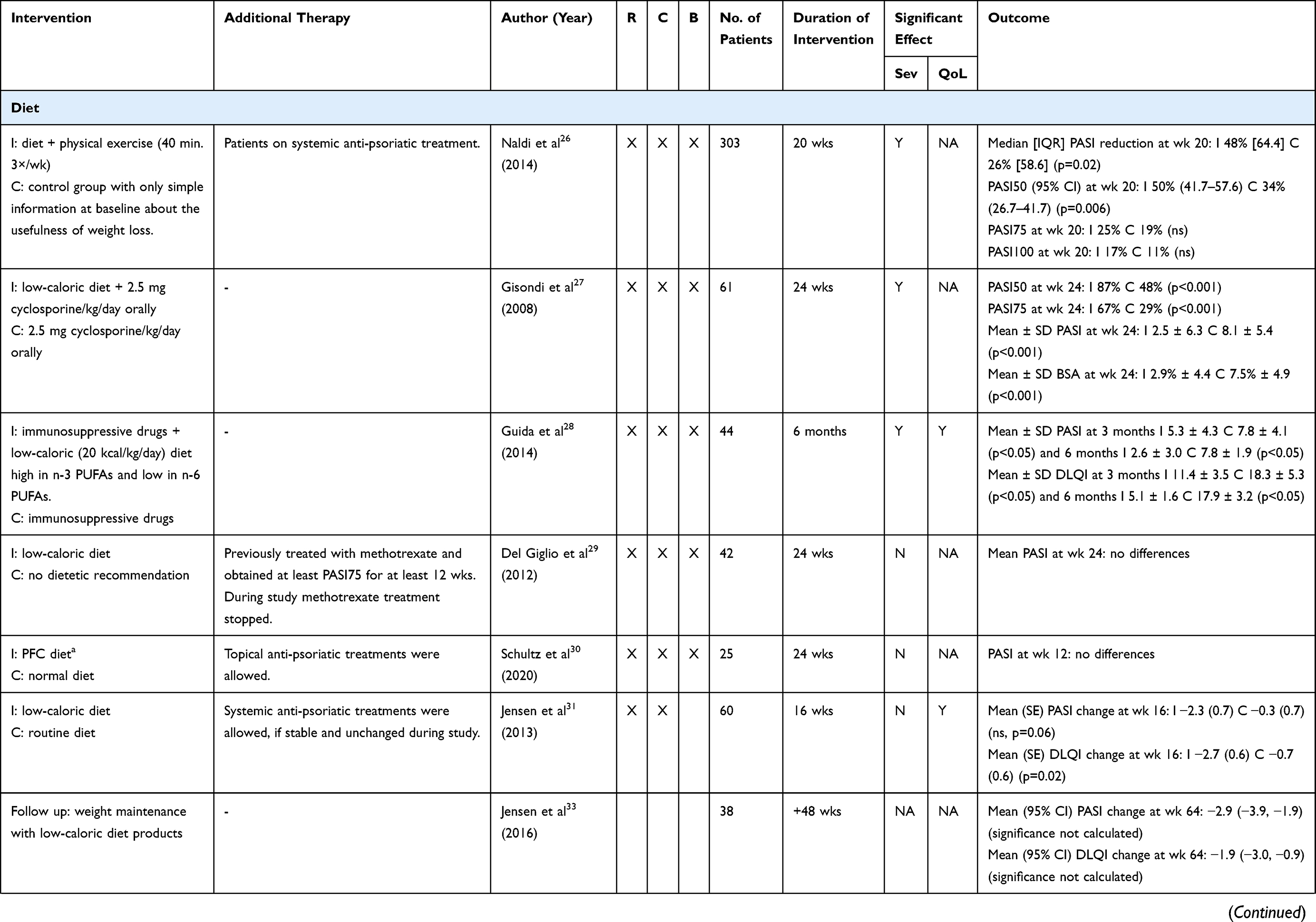 |  | 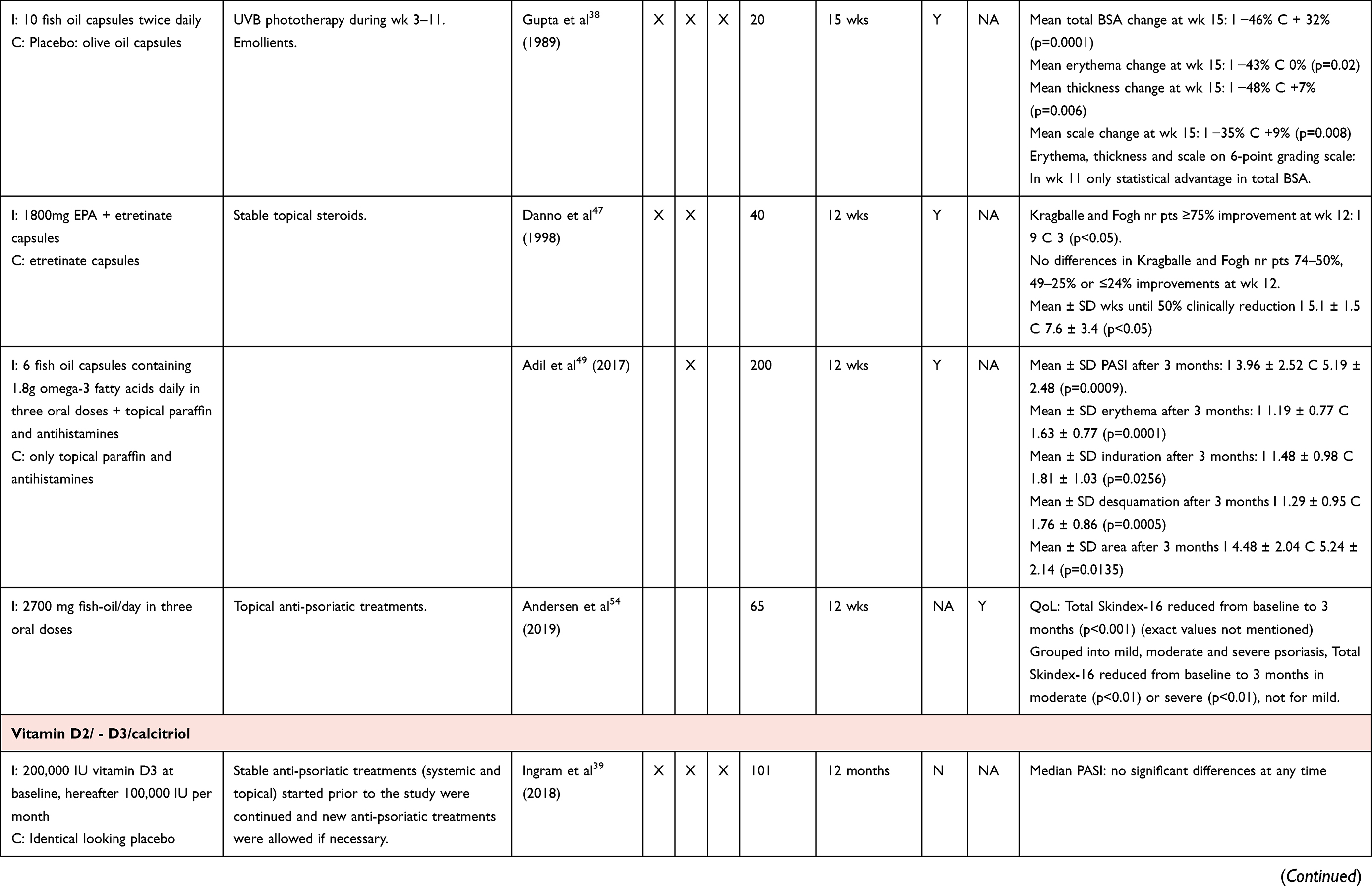 |  | 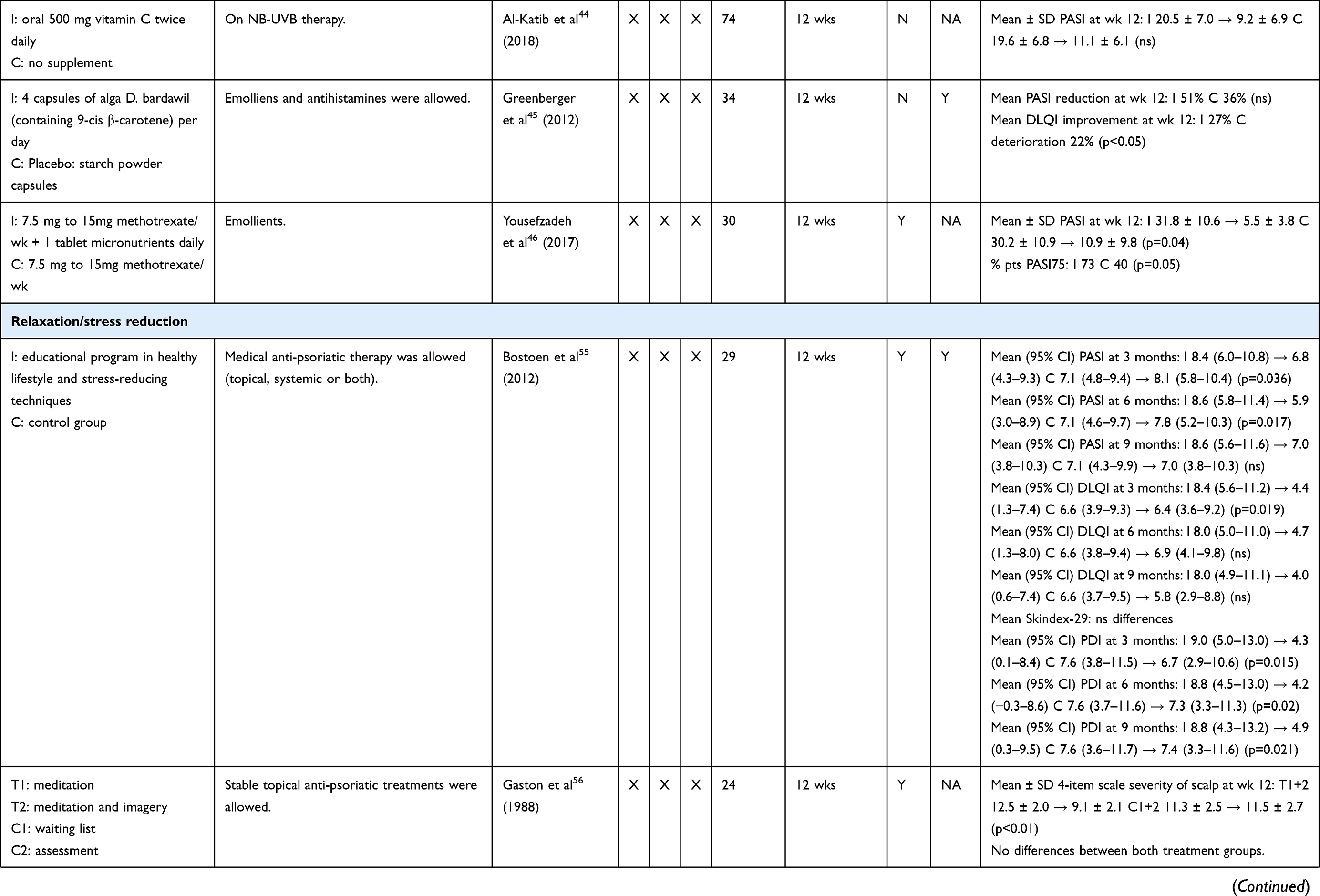 | 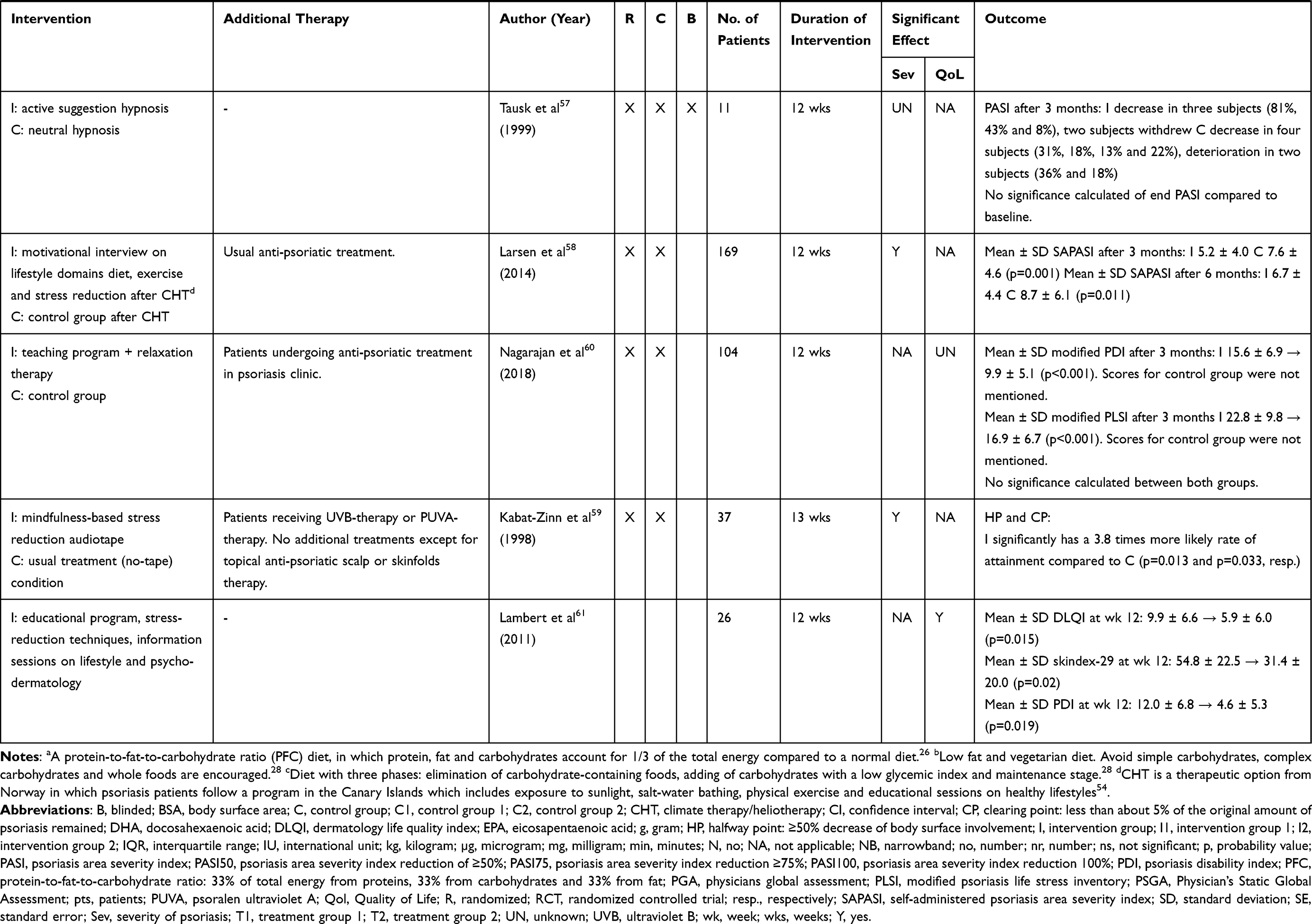 |
Table 1 Evidence Table of Included Intervention Studies |
 |
Figure 1 Article flow diagram. |
The Effect of Diet on Psoriasis Severity
The influence of dietary changes on psoriasis severity and QoL will be reviewed in this paragraph. These dietary changes include a low-caloric diet combined with exercise, low-caloric diets alone, Ornish diet, South Beach diet and protein-to-fat-to-carbohydrate ratio (PFC) diet. The studies in which supplements (eg, fish oil, vitamin D) were added to a diet will be discussed in the section ‘dietary supplements’.
Seven RCTs,26–32 one extension study33 of a previous RCT31 and one non-controlled study34 investigated the effect of dietary changes on the severity of psoriasis.
The largest RCT (blinded), in which 303 obese patients with psoriasis on systemic treatments participated, investigated the effect of a low-caloric diet combined with physical exercise on PASI improvement.26 At baseline, 43% of all patients used a systemic conventional treatment and 58% used a systemic biologic treatment. Weight-adjusted therapies were modified when relevant. After 20 weeks, median PASI reduced by 48% in the low-caloric + physical exercise group compared to 26% in the control group (p=0.02). Moreover, significantly more subjects in the low-caloric diet + exercise group achieved PASI50 compared to controls (50% vs 34%, resp. p=0.006). The percentages of subjects achieving PASI75 or PASI100 did not differ between groups.
The effect of a low-caloric diet on the severity of psoriasis was investigated in another blinded RCT (n=61), which investigated the effect of a low-caloric diet in combination with low-dose cyclosporine compared to low-dose cyclosporine only.27 Cyclosporine doses were adjusted according to weight during the trial. Subjects in the intervention group were also instructed to avoid alcohol and were encouraged to perform moderate physical exercise. After 24 weeks, significantly more patients taking the low-caloric diet compared to the control group reached PASI50 (87% vs 48%, resp. p<0.001) and PASI75 (67% vs 29%, resp. p<0.001) and had lower mean PASI (2.5 vs 8.1, resp. p<0.001) and mean BSA scores (2.9% vs 7.5%, resp. p<0.001). Data regarding alcohol use or amount of exercise were not mentioned. Another blinded RCT investigated a low-caloric diet in 22 patients on systemic conventional and biologic drugs, compared to the use of these drugs alone (n=22).28 Mean PASI scores were significantly lower in the intervention group compared to control group after 3 months (5.3 vs 7.8, resp. p<0.05) and 6 months (2.6 vs 7.8, resp. p<0.05). In a very small non-controlled study comprising 10 patients, the effect of a low-caloric diet on psoriasis severity was shown with a significant decrease in mean PASI after 12 weeks (from 5.72 to 3.2, p<0.05) and 24 weeks (from 5.72 to 3.8, p<0.05).34 Concomitant use of systemic and topical treatments was allowed, though the authors did not specify systemic medication used. The other two RCTs investigating a low-caloric diet on psoriasis severity did not show significant beneficial effects when compared to no dietary intervention, although the difference in mean PASI change between the low-caloric diet group and control group was almost significant in favor of the low-caloric diet (−2.3 vs −0.3, resp. p=0.06) in the Jensen study (n=60, non-blinded).29,31 Del Giglio (blinded RCT) investigated whether a low-caloric diet (n=22) was able to maintain disease remission after methotrexate (MTX) treatment compared to no dietary intervention (n=20).29 Mean PASI at the end of the study was not significantly different between the low-caloric group and the control group, but a trend in favor of the low-caloric group was seen.
The effects of the Ornish diet (n=10), South Beach diet (n=10) and no dietary intervention (n=10) on mean PASI scores were compared within one non-blinded RCT in which all three groups were treated with NB-UVB phototherapy.32 After 12 weeks, the mean improvement in PASI scores was 78%, 72% and 71% for the Ornish diet, South Beach diet and non-dietary group, respectively. PASI75 rates were 83%, 56% and 38%, respectively (p=0.30 between the Ornish and South Beach diet). Statistics between the dietary group versus non-dietary group were not described. A protein-to-fat-to-carbohydrate ratio (PFC) diet (n=25) was described in a short communication article. The study was set up as a blinded RCT.30 Four patients completed the study, the authors stated that the PASI was identical in both groups at week 12 and 24.
In the study of Naldi et al, exercise was part of the intervention.26 In the study of Gisondi, only patients in the dietary intervention group were encouraged to perform physical exercise.27 The other studies investigating dietary interventions did not provide information on physical exercise.
The Effect of Diet on Quality of Life
The influence of dietary interventions on the QoL of patients with psoriasis was investigated in three studies, of which two were randomized and controlled. All three studies investigated the effect of a low-caloric diet on DLQI score in patients with psoriasis and all found significant improvements at the end of the study. In one blinded RCT, large differences in mean DLQI score were found between the low-caloric diet group (n=22) and the control group (n=22) after 3 months (11.4 vs 18.3, resp. p<0.05) and 6 months (5.1 vs 17.9, resp. p<0.05) respectively.28 A smaller but significant difference in mean DLQI change was also found in favor of the low-caloric diet group (n=30) compared to the control group (n=30) in a non-blinded RCT (−2.7 vs −0.7, resp. p=0.02) of Jensen et al.31 A non-controlled study comprising 10 patients showed an improvement in DLQI score after 12 weeks (63%) and 24 weeks (40%) compared to baseline.34 As stated above in the section on psoriasis severity, the authors did not specify systemic medication used.
The Effect of Dietary Supplements on Psoriasis Severity
Seventeen studies investigated the effect of dietary supplements on the severity of psoriasis, of which 12 were blinded RCTs,35–46 and two studies were non-blinded RCTs47,48 The other studies had a different design: one non-randomized controlled non-blinded study,49 and two non-controlled studies.50,51
Six studies (five RCTs35–38,47 and one non-randomized controlled non-blinded study49 investigated the effect of supplementation of fish oil or eicosapentaenoic acid (EPA; an omega-3 fatty acid present in fish oil49) on psoriasis severity.35–38,47,49 The largest RCT (n=145, blinded) showed no significant differences in mean PASI between the group with a daily intake of six fish oil capsules during 16 weeks and the placebo group taking corn oil capsules.35 The daily intake of 10 capsules of herring roe oil in another blinded RCT (64 patients; 26 weeks) resulted in a mean delta PASI of −1.8, versus a mean delta PASI of −0.6 in the placebo group (p=0.045) after 26 weeks.36 A smaller blinded RCT (n=32) did not find statistical differences in total BSA change at week 12 between patients taking 10 fish oil capsules daily versus a placebo. However, a very subtle, but statistically significant difference in erythema score was found between the groups, in favor of the fish oil group compared to the control group (erythema −1.1 vs - 0.2, resp. p<0.5).37 The effect of 10 fish oil capsules twice daily for 15 weeks on severity of psoriasis was also investigated in an even smaller blinded RCT (n=20).38 Here, concomitant phototherapy with UVB was given during week 3–11 to both the intervention group and the placebo group using olive oil. After 15 weeks, statistical significant differences in changes from baseline in total BSA, erythema, thickness and scaling between both groups were found, in favor of the fish oil group (fish oil group −46%, −43%, −48%, −35% resp.; placebo group +32%, 0%, +7%, +9% resp.; all p-values <0.02). Eicosapentaenoic acid (EPA) supplements were investigated in a non-blinded RCT where 40 subjects received either EPA capsules with etretinate or etretinate only during 12 weeks.47 The number of patients with a decrease in total Kragballe and Fogh score52 (a lower score corresponded to less severe psoriasis) of ≥75% was significantly higher in the EPA group compared to the control group (9 vs 3, resp. p<0.05). A large (n= 200) non-randomized controlled non-blinded study found a statistically significant lower mean PASI after 3 months in patients using fish oil capsules (3.96) compared to no supplements (5.19; p<0.0009).49 The difference in mean PASI was 1.2 between the groups. Both groups were allowed to use topical paraffin. Baseline disease severity scores were not significantly different between both groups, correction for possible confounders was not performed.
Vitamin D2/-D3 or calcitriol, the active metabolite of cholecalciferol,53 were supplemented in three blinded RCTs,39–41 one non-blinded RCT48 and one non-controlled pilot study.50 In the largest two RCTs (blinded), in which the effect of vitamin D3 supplementation on psoriasis severity was compared to placebo in 166 patients, no significant differences in PASI were found after 12 months.39,40 In both studies, anti-psoriatic treatments were allowed if necessary and were accounted for in analyses. A smaller blinded RCT (n=45) described a small statistically significant difference in mean delta PASI between the vitamin D group (delta PASI −1.43) and the placebo group (delta PASI 0.33; p=0.03) after 3 months, but this was no longer significant after 6 months (delta PASI −2.15 vs −0.71, resp.).41 Another RCT (n=40; non-blinded) investigated calcitriol supplementation in addition to acitretin treatment with acitretin treatment alone on the severity of psoriasis.48 A significantly higher mean PASI improvement was found in the combination group compared to acitretin alone (delta PASI −18 vs −13.6, resp; p<0.05) after 90 days.
Two studies (one blinded RCT and a non-controlled study) investigated the effect of oral curcuma on the severity of psoriasis.42,51 The blinded RCT (n=63) showed a significantly larger median PASI reduction in the curcumin group (PASI from 5.6 (baseline) to 1.3 (wk 12) to 1.4 (wk 16)) compared to the control group (PASI from 4.7 (baseline) to 2.4 (wk 12) to 2.5 (wk 16); p<0.05).42 The non-controlled study (n=12) was terminated due to very low response rates.51
The effect of daily probiotic supplementation on psoriasis severity was investigated in one recent blinded RCT with 90 participants.43 After 12 weeks, in which both groups were also treated with topical betamethasone and calcipotriol, the percentage of patients achieving PASI75 was significantly higher in the probiotic group compared to the control group (67% vs 42%, resp. p.0317). However, the percentage of patients reaching PASI<6 (91% vs 77%) or clear PGA after 12 weeks (49% vs 30%) did not significantly differ between intervention and control group, respectively.
A blinded RCT (n=74) investigated 12 weeks of vitamin C supplementation compared to no supplementation, given to patients on NB-UVB therapy.44 After 12 weeks, mean PASI score did not significantly differ between the vitamin C group and control group, who was also treated with NB-UVB. (from 20.5 to 9.2 and from 19.6 to 11.1 resp.).
The effects of four capsules of Alga Dunaliella bardawil (Alga D bardawil) daily on the severity of psoriasis was investigated in one blinded RCT, compared to the control group, who received a placebo (n=34).45 Alga D bardawil consists of high levels of 9-cis β-carotene, which is a precursor of 9-cis retinoid acid.45 All subjects were allowed to use emollients. After 12 weeks of supplementation, no significant differences in mean PASI improvement (%) were found between the intervention group and the control group (51% vs 36%, resp.).
The effect of daily supplementation of a tablet micronutrients on psoriasis severity was investigated in a blinded RCT with 30 patients who were also treated with MTX.46 After 12 weeks, the group on combination of micronutrients and MTX had a significantly larger improvement in mean PASI score compared to the group on MTX alone (from 31.8 to 5.5 vs from 30.2 to 10.9, resp., p=0.04). Doses of MTX in both groups ranged from 7.5 to 15 mg per week and were similar between both groups at baseline (p>0.05).
The Effect of Dietary Supplements on Quality of Life
Five studies investigated the effect of dietary supplements on QoL.36,40,45,51,54 Herring roe oil was not found to influence beneficially QoL in a blinded RCT with 64 participants.36 A non-controlled study investigated the supplementation of 2700 mg fish oil per day during 12 weeks to a diet of 65 patients and showed a significant improvement in total Skindex-16 compared to baseline (p<0.0001).54 Patients were allowed to use topical treatments as well. However, a control group was lacking and the exact improvements of the Skindex-16 score were not mentioned. Twelve months of vitamin D3 supplementation showed no significant beneficial effects on QoL compared to controls in a blinded RCT (n=65).40 A non-controlled study investigating effects of curcuminoid C3 complex on Skindex-29 compared to controls (n=12) was terminated due to very low response rates.51 Alga D bardawil supplementation positively influenced Qol compared to the control group (blinded RCT, n=34), with a decrease of 27% in mean DLQI score in the intervention group, compared to an increase in DLQI of 22% in the control group at 12 weeks (p<0.05).45 Patients in this study were only allowed to use emollients.
The Effect of Relaxation/Stress Reduction on Psoriasis Severity
Five RCTs investigated the effect of relaxation and/or stress reduction on psoriasis severity, of which three were blinded55–57 and two unblinded.58,59 The largest blinded RCT (n=29) investigated the combination of an educational program, stress-reducing techniques, information on lifestyle factors and psycho-dermatology.55 A significant difference in reduction in mean PASI in the educational group compared to the control group was found after three (from 8.4 to 6.8 vs from 7.1 to 8.1, resp. p=0.036) and 6 months (from 8.6 to 5.9 vs from 7.1 to 7.8, resp. p=0.017), which was no longer found after 9 months (from 8.6 to 7.0 vs from 7.1 to 7.0, resp.). The influence of meditation (group 1) and meditation + imagery (group 2) on severity of scalp psoriasis was investigated in a small blinded RCT (n=24), compared to control groups.56 After 12 weeks, mean scalp severity score (measured with a 4-item scale defined by the authors) was significantly lower in both treatment groups compared to the control groups (9.1 vs 11.5, resp. p<0.01). In this study, subjects with mainly scalp psoriasis were included, and the influence of the intervention on plaques outside the scalp was not investigated. The influence of hypnosis on psoriasis severity was investigated in a blinded RCT (n=11) in which two types of hypnosis (active suggestion hypnosis and neutral hypnosis) were compared with each other.57 Three subjects in the active suggestion hypnosis group had an improvement in PASI score, two subjects withdrew from the study. Four subjects in de neutral hypnosis group had an improvement in PASI, in two subjects PASI deteriorated. For the percentages change in PASI, see Table 1. Unfortunately, no significance was calculated when comparing end PASI to baseline. The effects of motivational interviewing (lifestyle domains diet, physical activity and stress management) after climate therapy/heliotherapy (CHT) compared to no motivational interviewing after CHT on psoriasis severity was investigated in a 12-week non-blinded RCT comprising 169 patients.58 Smoking cessation, alcohol and weight reduction could be discussed during the motivational interviews as well. The mean self-administered PASI (SAPASI) after CHT, but before randomization for motivational interviews or no motivational interviews, was 1.8 ± 2.5 in the intervention group and 1.9 ± 3.2 in de control group (ns). After 12 weeks, the mean SAPASI was significantly less increased in the group who underwent motivational interviews compared to controls (SAPASI at wk 12: 5.2 vs 7.6, resp. p=0.001) and remained significantly different up to 6 months (6.7 vs 8.7 for intervention and controls, resp. p=0.011). Both patients in the intervention group as well as in the control group received their usual psoriasis treatment. Authors did not mention the treatments used by the subjects. Kabat-Zinn (non-blinded RCT; n=37) investigated the effects of a mindfulness-based stress reduction audiotape given to the intervention group compared to a control group, during UVB or PUVA phototherapy.59 Patients receiving mindfulness tapes were significantly more likely (3.8 times) to attain a halfway point (HP) (≥50% decrease in body surface involved) or clearing point (CP) (less than about 5% of the original amount of psoriasis remained) compared to the groups without the intervention (p=0.013 and p=0.033, resp.) after an average of 13 weeks.
The Effect of Relaxation/Stress Reduction on Quality of Life
Three studies investigated the effect of relaxation/stress reduction on the QoL of patients with psoriasis.55,60,61 A 12-week blinded RCT (n=29) investigated the combination of an educational program, stress-reducing techniques, information on lifestyle factors and psycho-dermatology on DLQI, Psoriasis Disability Index (PDI) and Skindex-29.55 A significant difference in reduction of mean DLQI was found in favor of the educational program group compared to controls after 3 months (from 8.4 to 4.4 vs from 6.6 to 6.4, resp. p=0.019), but not after 6 and 9 months. In the intervention group the mean PDI was significantly reduced compared to controls after three (from 9.0 to 4.3 vs from 7.6 to 6.7, resp. p=0.015), 6 (from 8.8 to 4.2 vs from 7.6 to 7.3, resp. p=0.02) and 9 months (from 8.8 to 4.9 vs from 7.6 to 7.4, resp. p=0.021). A large non-blinded RCT (n=104) investigated an educational program together with muscle relaxation techniques, compared to controls.60 The intervention group as well as the control group received treatment in a psoriasis clinic. After 3 months, both mean PDI and Psoriasis Life Stress Inventory (PLSI) decreased significantly in the intervention group compared to baseline (from 15.6 to 9.9, p<0.001 and from 22.8 to 16.9, p<0.001, resp.). PDI and PLSI scores of the control group after 3 months were not mentioned in the article, outcomes were not compared between both groups. A non-controlled study (n=26) investigated an educational program, stress-reducing techniques, information on lifestyle factors and psycho-dermatology.61 After 12 weeks, mean DLQI, mean Skindex-29 and mean PDI were significantly decreased compared to baseline (from 9.9 to 5.9, p=0.015; from 54.8 to 31.4, p=0.02 and from 12.0 to 4.6, p=0.019, resp.).
Discussion
In this review, the effects of lifestyle interventions in the domains diet, relaxation, exercise, smoking, alcohol and sleep on the severity of psoriasis and on the QoL of patients with psoriasis was studied. Thirty-four intervention studies were included. Most studies performed interventions in the diet of patients with psoriasis (n=9), or added supplements to the diet (n=18). Three studies comprised relaxation techniques and four studies combined relaxation or stress-reducing techniques with an educational program or exercise. Evidence on the effects of changes in the lifestyle domains smoking, alcohol and sleep on the severity of psoriasis or QoL in patients with psoriasis was not found.
Nine studies investigated the effects of dietary changes on the severity of psoriasis,26–34 of which seven were RCTs.26–32 Most dietary changes investigated comprised low-caloric diets. Three RCTs comprising 408 patients in total found beneficial effects of dietary interventions on the severity of psoriasis.26–28 These additional effects of the dietary intervention on psoriasis severity were statistically significant. In order to interpret the clinical relevance of the differences found, the Minimal Clinically Important Difference (MCID; Δ PASI = 3.2)62 as described by Mattei et al, based on data of 13 RCTs, can be used. Based on this MCID, the differences found after 6 months in the studies of Gisondi and Guida seemed to be clinically relevant.27,28 However, it remains unclear whether the diet itself influences psoriasis severity or the weight loss following the diet, since BMI/body weight were significantly more reduced in the dietary groups compared to the control groups at end of studies26–28 and there was a statistically significant correlation between PASI improvement and body weight/BMI.26,27 In the study of Gisondi et al, only patients in the dietary intervention group were encouraged to perform physical exercise.27 Since some data suggest that physical exercise combined with dietary interventions may lead to more weight loss compared to dietary interventions alone,63 physical exercise might be a confounder when assessing the effect of diet on psoriasis severity.27 The other four RCTs (157 participants in total), did not find significant differences in psoriasis severity between the dietary intervention groups and the control groups.29–32 Thus, there is some evidence that dietary interventions, with or without physical exercise, might improve psoriasis severity of obese patients, which is in line with the findings of the Cochrane review of Ko et al.22 However, since all studies were executed in overweight or obese patients, the effect in non-obese patients remains unclear. Conducting dietary research in general can have its challenges. Confounding is often present in dietary intervention research64 and low adherence to the diet may occur.65
In addition to the Cochrane review, we described 17 studies investigating the effect of dietary supplements on the severity of psoriasis,35–51 of which 12 were blinded RCTs35–46 and two non-blinded RCTs.47,48 This high number of (blinded) RCTs reflects the interest of research groups in investigating the effect of dietary supplements on psoriasis severity. The most frequently investigated dietary supplements were fish oil/EPA (n=6), vitamin D2/-D3/calcitriol (n=5) and curcuma (n=2). Six studies investigated the effect of fish oil or EPA supplementation on psoriasis severity in 501 participants.35–38,47,49 Interest in fish oil regarding psoriasis arises from the anti-inflammatory effects of EPA and DHA, which fish oil contains.66 The largest RCT (n=145) comparing fish oil capsules with corn oil did not find any differences in PASI after 16 weeks.35 Other studies found significant differences in PASI36,49 or erythema score37 in favor of fish oil groups compared to control groups, although the small differences in outcome measures used, raise questions about clinical relevance. Moreover, the used outcome measure (Kragballe and Fogh score) in the study of Danno et al was difficult to interpret.47 The body of evidence on the efficacy of fish oil on severity of psoriasis is quite large. However, the effect sizes found in the included studies were rather small. This raises the question whether fish oil supplementation really is of added value for psoriasis patients. Five studies investigated the effect of supplementation of vitamin D2/ -D3 or calcitriol on psoriasis severity in 260 patients,39–41,48,50 of which the two largest RCTs (n= 166) found no differences in PASI scores after 12 months.39,40 Six studies investigated the effect of other dietary supplements (curcumin, probiotics, vitamin C, alga D bardawil, micronutrients) on psoriasis severity.42–46,51 Significant differences were found in favor of curcumin, probiotics and micronutrients.42,43,46 Clinical relevance of the differences found with curcumin can be debated, since the difference in PASI reduction between both groups was relatively small.42 Micronutrients showed larger differences in PASI reduction between both groups, exceeding the aforementioned MCID of 3.2.46 In summary, most of the smaller studies on dietary supplements showed significant improvements regarding psoriasis severity, but effect sizes were mainly small. However, the three largest studies investigating fish oil or vitamin D did not show significant effects.35,39,40 Moreover, follow-up durations were, except for the studies in the vitamin D section, relatively short.
Five RCTs investigated relaxation/stress reduction on the severity of psoriasis.55–59 Four of these, comprising 259 patients in total, showed a significant improvement in the intervention group compared to controls regarding PASI,55 scalp severity,56 SAPASI58 and HP/CP.59 However, some differences found were lower than the MCID of 3.255 or difficult to interpret due to less common outcome measures used.56,59 Summarizing, most of the evidence showed significant results in favor of the relaxation/stress reduction; however, some effect sizes were small and uncommon outcome measures were used.
Eleven out of 34 studies described the effect of lifestyle interventions on dermatological QoL. The QoL of patients with psoriasis using a low-caloric diet was only investigated in three studies, of which two RCTs. All three studies showed improvement of the QoL.28,31,34 Basra published the MCID for DLQI for inflammatory diseases and recommended a value of 4 as a clinical meaningful difference in QoL.67 From this perspective, only the results of Guida et al can be interpreted as clinically relevant.28
Five studies investigated the effect of dietary supplements on the QoL of patients with psoriasis.36,40,45,51,54 Total Skindex-16 significantly reduced in a non-controlled study (n=65) investigating fish oil.54 However, given the non-controlled study design and the fact that exact data were not published, it is difficult to interpret the relevance for clinical practice. The same accounts for the percentage improvement of DLQI in the RCT investigating alga D. bardawil (n=34).45 More research is necessary in order to interpret the effect of dietary supplements on QoL of patients with psoriasis.
Three studies investigated relaxation/stress reduction on the QoL in patients with psoriasis with 159 subjects in total.55,60,61 A blinded RCT (n=29) and a non-controlled study (n=26) investigated the combination of an educational program, stress-reducing techniques, information on lifestyle factors and psycho-dermatology and showed significant improvements in DLQI, PDI and Skindex-29 in favor of the intervention group.55,61 Thus, evidence in relaxation/stress reduction on the QoL of patients with psoriasis is scarce, but relaxation/stress reduction may have a positive impact. With respect to QoL, we like to underline the fact that only dermatological QoL has been investigated in the studies mentioned above. As lifestyle interventions will probably affect more aspects of QoL, a more generic QoL outcome measure would be of additional value.68
This narrative review shows an updated and extended body of evidence regarding diet, dietary supplements and stress/relaxation on severity or dermatological QoL of patient with psoriasis. Dietary interventions, whether or not combined with physical exercise, show the largest potential in terms of amount of evidence and effect sizes, especially on psoriasis severity. The studies found were heterogenous in terms of population, concomitant treatments and outcome measures. Some studies investigated only specific populations (eg, obese patients). If concomitant (systemic) treatments were allowed, exact use and adherence were not always registered. Since (systemic) treatments can improve psoriasis disease severity drastically, a difference in the usage of (systemic) treatments between the intervention and control group might influence the results and should therefore be taken into account when interpreting the results of those studies. Moreover, especially in older studies unconventional outcome measures were used. The most detected limitations were insufficient power of studies, short duration of follow-up, incomplete reporting of values and statistical analyses. These limitations might have influenced the outcomes of the studies. To study the efficacy of lifestyle interventions in patients with psoriasis, sound RCTs are important.
Conclusions
In recent years, attention increased for healthy lifestyle and its positive impact on severity of psoriasis and QoL of patients. In this review, it was demonstrated that especially dietary and relaxation interventions showed some promising results regarding psoriasis severity and dermatology-related QoL, respectively. However, our review identifies important gaps in lifestyle research regarding study design and the reporting of outcomes. Suggestions for future studies on lifestyle interventions in patients with psoriasis would include well-powered RCTs also assessing generic aspects of QoL.
Disclosure
MR van Acht carried out clinical trials for Janssen. All funding was not personal but went to the independent research fund of the department of dermatology of Radboud university medical center Nijmegen, the Netherlands. JMPA van den Reek carried out clinical trials for AbbVie, Celgene, and Janssen and has received speaking fees/attended advisory boards from AbbVie, Janssen, BMS, Almirall, LEO Pharma, Novartis, UCB, and Eli Lilly and reimbursement for attending a symposium from Janssen, Pfizer, Celgene, and AbbVie. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud university medical center Nijmegen, the Netherlands. EMGJ de Jong has received research grants for the independent research fund of the Department of Dermatology of the Radboud University Medical Centre Nijmegen, the Netherlands, from AbbVie, BMS, Novartis, Janssen, Leo Pharma, and UCB. Has acted as consultant and/or paid speaker for and/or participated in research sponsored by companies that manufacture drugs used for the treatment of psoriasis including AbbVie, Janssen, Galapagos, Sanofi, Novartis, Lily, Celgene, Leo Pharma, UCB, and Almirall. All funding is not personal but goes to the independent research fund of the department of dermatology of Radboud university medical center Nijmegen, the Netherlands. MMB Seyger received grants from/was involved in clinical trials from Abbvie, Amgen, Celgene, Eli Lilly, Janssen, Leo Pharma, and Pfizer. She served as a consultant for Abbvie, Eli Lilly, Janssen, Leo Pharma, Novartis, UCB, and Pfizer; fees were paid directly to the institution. The authors report no other conflicts of interest in this work.
References
1. Parisi R, Symmons DP, Griffiths CE, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339
2. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
3. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
4. Oliveira Mde F, Rocha Bde O, Duarte GV. Psoriasis: classical and emerging comorbidities. An Bras Dermatol. 2015;90(1):9–20. doi:10.1590/abd1806-4841.20153038
5. Chareonrungrueangchai K, Wongkawinwoot K, Anothaisintawee T, Reutrakul S. Dietary factors and risks of cardiovascular diseases: an umbrella review. Nutrients. 2020;12(4):1088. doi:10.3390/nu12041088
6. Paulweber B, Valensi P, Lindström J, et al. A European evidence-based guideline for the prevention of type 2 diabetes. Horm Metab Res. 2010;42(Suppl 1):S3–36. doi:10.1055/s-0029-1240928
7. Armstrong AW, Harskamp CT, Dhillon JS, Armstrong EJ. Psoriasis and smoking: a systematic review and meta-analysis. Br J Dermatol. 2014;170(2):304–314. doi:10.1111/bjd.12670
8. Richer V, Roubille C, Fleming P, et al. Psoriasis and smoking: a systematic literature review and meta-analysis with qualitative analysis of effect of smoking on psoriasis severity. J Cutan Med Surg. 2016;20(3):221–227. doi:10.1177/1203475415616073
9. Brenaut E, Horreau C, Pouplard C, et al. Alcohol consumption and psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2013;27(Suppl 3):30–35. doi:10.1111/jdv.12164
10. Gerdes S, Zahl VA, Weichenthal M, Mrowietz U. Smoking and alcohol intake in severely affected patients with psoriasis in Germany. Dermatology. 2010;220(1):38–43. doi:10.1159/000265557
11. Zheng Q, Sun XY, Miao X, et al. Association between physical activity and risk of prevalent psoriasis: a MOOSE-compliant meta-analysis. Medicine. 2018;97(27):e11394. doi:10.1097/MD.0000000000011394
12. Auker L, Cordingley L, Pye SR, Griffiths CEM, Young HS. What are the barriers to physical activity in patients with chronic plaque psoriasis? Br J Dermatol. 2020;183(6):1094–1102. doi:10.1111/bjd.18979
13. Nowowiejska J, Baran A, Grabowska P, Lewoc M, Kaminski TW, Flisiak I. Assessment of life quality, stress and physical activity among patients with psoriasis. Dermatol Ther. 2022;12(2):395–406. doi:10.1007/s13555-021-00662-1
14. Stewart TJ, Tong W, Whitfeld MJ. The associations between psychological stress and psoriasis: a systematic review. Int J Dermatol. 2018;57(11):1275–1282. doi:10.1111/ijd.13956
15. Rousset L, Halioua B. Stress and psoriasis. Int J Dermatol. 2018;57(10):1165–1172. doi:10.1111/ijd.14032
16. Nowowiejska J, Baran A, Lewoc M, Grabowska P, Kaminski TW, Flisiak I. The assessment of risk and predictors of sleep disorders in patients with psoriasis-a questionnaire-based cross-sectional analysis. J Clin Med. 2021;10:644. doi:10.3390/jcm10040664
17. Melikoglu M. Sleep quality and its association with disease severity in psoriasis. Eurasian J Med. 2017;49(2):124–127. doi:10.5152/eurasianjmed.2017.17132
18. Luca M, Musumeci ML, D’Agata E, Micali G. Depression and sleep quality in psoriatic patients: impact of psoriasis severity. Int J Psychiatry Clin Pract. 2020;24(1):102–104. doi:10.1080/13651501.2019.1659372
19. García-Molina L, Lewis-Mikhael AM, Riquelme-Gallego B, Cano-Ibáñez N, Oliveras-López MJ, Bueno-Cavanillas A. Improving type 2 diabetes mellitus glycaemic control through lifestyle modification implementing diet intervention: a systematic review and meta-analysis. Eur J Nutr. 2020;59(4):1313–1328. doi:10.1007/s00394-019-02147-6
20. Doughty KN, Del Pilar NX, Audette A, Katz DL. Lifestyle medicine and the management of cardiovascular disease. Curr Cardiol Rep. 2017;19(11):116. doi:10.1007/s11886-017-0925-z
21. Colpani V, Baena CP, Jaspers L, et al. Lifestyle factors, cardiovascular disease and all-cause mortality in middle-aged and elderly women: a systematic review and meta-analysis. Eur J Epidemiol. 2018;33(9):831–845. doi:10.1007/s10654-018-0374-z
22. Ko SH, Chi CC, Yeh ML, Wang SH, Tsai YS, Hsu MY. Lifestyle changes for treating psoriasis. Cochrane Database Syst Rev. 2019;7(7):Cd011972. doi:10.1002/14651858.CD011972.pub2
23. Ryan C, Korman NJ, Gelfand JM, et al. Research gaps in psoriasis: opportunities for future studies. J Am Acad Dermatol. 2014;70(1):146–167. doi:10.1016/j.jaad.2013.08.042
24. Allan SJ, Kavanagh GM, Herd RM, Savin JA. The effect of inositol supplements on the psoriasis of patients taking lithium: a randomized, placebo-controlled trial. Br J Dermatol. 2004;150(5):966–969. doi:10.1111/j.1365-2133.2004.05822.x
25. Michaëlsson G, Gerdén B, Hagforsen E, et al. Psoriasis patients with antibodies to gliadin can be improved by a gluten-free diet. Br J Dermatol. 2000;142(1):44–51. doi:10.1046/j.1365-2133.2000.03240.x
26. Naldi L, Conti A, Cazzaniga S, et al. Diet and physical exercise in psoriasis: a randomized controlled trial. Br J Dermatol. 2014;170(3):634–642. doi:10.1111/bjd.12735
27. Gisondi P, Del Giglio M, Di Francesco V, Zamboni M, Girolomoni G. Weight loss improves the response of obese patients with moderate-to-severe chronic plaque psoriasis to low-dose cyclosporine therapy: a randomized, controlled, investigator-blinded clinical trial. Am J Clin Nutr. 2008;88(5):1242–1247. doi:10.3945/ajcn.2008.26427
28. Guida B, Napoleone A, Trio R, et al. Energy-restricted, n-3 polyunsaturated fatty acids-rich diet improves the clinical response to immuno-modulating drugs in obese patients with plaque-type psoriasis: a randomized control clinical trial. Clin Nutr. 2014;33(3):399–405. doi:10.1016/j.clnu.2013.09.010
29. Del Giglio M, Gisondi P, Tessari G, Girolomoni G. Weight reduction alone may not be sufficient to maintain disease remission in obese patients with psoriasis: a randomized, investigator-blinded study. Dermatology. 2012;224(1):31–37. doi:10.1159/000335566
30. Schultz A, Jensen P, Zibert JR, et al. Recruitment and retention in a randomized control trial of increased dietary protein-to-carbohydrate ratios in patients with psoriasis. Acta Derm Venereol. 2020;100(1):adv00021. doi:10.2340/00015555-3380
31. Jensen P, Zachariae C, Christensen R, et al. Effect of weight loss on the severity of psoriasis: a randomized clinical study. JAMA Dermatol. 2013;149(7):795–801. doi:10.1001/jamadermatol.2013.722
32. Kimball AB, Alavian C, Alora-Palli M, Bagel J. Weight loss in obese patients with psoriasis can be successfully achieved during a course of phototherapy. J Eur Acad Dermatol Venereol. 2012;26(12):1582–1584. doi:10.1111/j.1468-3083.2011.04361.x
33. Jensen P, Christensen R, Zachariae C, et al. Long-term effects of weight reduction on the severity of psoriasis in a cohort derived from a randomized trial: a prospective observational follow-up study. Am J Clin Nutr. 2016;104(2):259–265. doi:10.3945/ajcn.115.125849
34. Roongpisuthipong W, Pongpudpunth M, Roongpisuthipong C, Rajatanavin N. The effect of weight loss in obese patients with chronic stable plaque-type psoriasis. Dermatol Res Pract. 2013;2013:795932. doi:10.1155/2013/795932
35. Søyland E, Funk J, Rajka G, et al. Effect of dietary supplementation with very-long-chain n-3 fatty acids in patients with psoriasis. N Engl J Med. 1993;328(25):1812–1816. doi:10.1056/NEJM199306243282504
36. Tveit KS, Brokstad KA, Berge RK, et al. A randomized, double-blind, placebo-controlled clinical study to investigate the efficacy of herring roe oil for treatment of psoriasis. Acta Derm Venereol. 2020;100(10):adv00154. doi:10.2340/00015555-3507
37. Bittiner SB, Tucker WF, Cartwright I, Bleehen SS. A double-blind, randomised, placebo-controlled trial of fish oil in psoriasis. Lancet. 1988;1(8582):378–380. doi:10.1016/S0140-6736(88)91181-6
38. Gupta AK, Ellis CN, Tellner DC, Anderson TF, Voorhees JJ. Double-blind, placebo-controlled study to evaluate the efficacy of fish oil and low-dose UVB in the treatment of psoriasis. Br J Dermatol. 1989;120(6):801–807. doi:10.1111/j.1365-2133.1989.tb01378.x
39. Ingram MA, Jones MB, Stonehouse W, et al. Oral vitamin D(3) supplementation for chronic plaque psoriasis: a randomized, double-blind, placebo-controlled trial. J Dermatolog Treat. 2018;29(7):648–657. doi:10.1080/09546634.2018.1444728
40. Jarrett P, Camargo CA
41. Disphanurat W, Viarasilpa W, Chakkavittumrong P, Pongcharoen P. The clinical effect of oral vitamin d2 supplementation on psoriasis: a double-blind, randomized, placebo-controlled study. Dermatol Res Pract. 2019;2019:1–9. doi:10.1155/2019/5237642
42. Antiga E, Bonciolini V, Volpi W, Del Bianco E, Caproni M. Oral curcumin (meriva) is effective as an adjuvant treatment and is able to reduce IL-22 serum levels in patients with psoriasis vulgaris. Biomed Res Int. 2015;2015:283634. doi:10.1155/2015/283634
43. Navarro-López V, Martínez-Andrés A, Ramírez-Boscá A, et al. Efficacy and safety of oral administration of a mixture of probiotic strains in patients with psoriasis: a randomized controlled clinical trial. Acta Derm Venereol. 2019;99(12):1078–1084. doi:10.2340/00015555-3305
44. Al-Katib SR, AL-Wakeel HA, AL-Rawaf RF. Role of vitamin c as antioxidant in psoriasis patients treated with nb-UVB phototherapy. Indian J Public Health Res Dev. 2018;9(10):375–380. doi:10.5958/0976-5506.2018.01372.4
45. Greenberger S, Harats D, Salameh F, et al. 9-cis-rich β-carotene powder of the alga dunaliella reduces the severity of chronic plaque psoriasis: a randomized, double-blind, placebo-controlled clinical trial. J Am Coll Nutr. 2012;31(5):320–326. doi:10.1080/07315724.2012.10720430
46. Yousefzadeh H, Jabbari Azad F, Banihashemi M, Rastin M, Mahmoudi M. Evaluation of psoriasis severity and inflammatory responses under concomitant treatment with methotrexate plus micronutrients for psoriasis vulgaris: a randomized double blind trial. Acta Dermatovenerol Alp Panon Adriat. 2017;26(1):3–9. doi:10.15570/actaapa.2017.2
47. Danno K, Sugie N. Combination therapy with low-dose etretinate and eicosapentaenoic acid for psoriasis vulgaris. J Dermatol. 1998;25(11):703–705. doi:10.1111/j.1346-8138.1998.tb02487.x
48. Ezquerra GM, Regaña MS, Millet PU. Combination of acitretin and oral calcitriol for treatment of plaque-type psoriasis. Acta Derm Venereol. 2007;87(5):449–450. doi:10.2340/00015555-0290
49. Adil M, Singh PK, Maheshwari K. Clinical evaluation of omega-3 fatty acids in psoriasis. Przegl Dermatol. 2017;104(3):314–323.
50. Finamor DC, Sinigaglia-Coimbra R, Neves LC, et al. A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis. Dermatoendocrinol. 2013;5(1):222–234. doi:10.4161/derm.24808
51. Kurd SK, Smith N, VanVoorhees A, et al. Oral curcumin in the treatment of moderate to severe psoriasis vulgaris: a prospective clinical trial. J Am Acad Dermatol. 2008;58(4):625–631. doi:10.1016/j.jaad.2007.12.035
52. Kragballe K, Fogh K. A low-fat diet supplemented with dietary fish oil (Max-EPA) results in improvement of psoriasis and in formation of leukotriene B5. Acta Derm Venereol. 1989;69(1):23–28.
53. Vieth R. Vitamin D supplementation: cholecalciferol, calcifediol, and calcitriol. Eur J Clin Nutr. 2020;74(11):1493–1497. doi:10.1038/s41430-020-0697-1
54. Andersen AD, Almegaard A, Schultz AN, Zibert JR. Effect of omega-3 supplementation on quality of life in patients with psoriasis: a digital survey-based study. Acta Derm Venereol. 2019;99(10):907–908. doi:10.2340/00015555-3215
55. Bostoen J, Bracke S, De Keyser S, Lambert J. An educational programme for patients with psoriasis and atopic dermatitis: a prospective randomized controlled trial. Br J Dermatol. 2012;167(5):1025–1031. doi:10.1111/j.1365-2133.2012.11113.x
56. Gaston L, Crombez J-C, Joly J, Hodgins S, Dumont M. Efficacy of imagery and meditation techniques in treating psoriasis. Imagin Cogn Pers. 1988;8(1):25–38. doi:10.2190/PQKE-CMAM-T4MT-QVBL
57. Tausk F, Whitmore SE. A pilot study of hypnosis in the treatment of patients with psoriasis. Psychother Psychosom. 1999;68(4):221–225. doi:10.1159/000012336
58. Larsen MH, Krogstad AL, Aas E, Moum T, Wahl AK. A telephone-based motivational interviewing intervention has positive effects on psoriasis severity and self-management: a randomized controlled trial. Br J Dermatol. 2014;171(6):1458–1469. doi:10.1111/bjd.13363
59. Kabat-Zinn J, Wheeler E, Light T, et al. Influence of a mindfulness meditation-based stress reduction intervention on rates of skin clearing in patients with moderate to severe psoriasis undergoing phototherapy (UVB) and photochemotherapy (PUVA). Psychosom Med. 1998;60(5):625–632. doi:10.1097/00006842-199809000-00020
60. Nagarajan P, Thappa DM. Effect of an educational and psychological intervention on knowledge and quality of life among patients with psoriasis. Indian Dermatol Online J. 2018;9(1):27–32. doi:10.4103/idoj.IDOJ_111_17
61. Lambert J, Bostoen J, Geusens B, et al. A novel multidisciplinary educational programme for patients with chronic skin diseases: Ghent pilot project and first results. Arch Dermatol Res. 2011;303(1):57–63. doi:10.1007/s00403-010-1082-z
62. Mattei PL, Corey KC, Kimball AB. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): the correlation between disease severity and psychological burden in patients treated with biological therapies. J Eur Acad Dermatol Venereol. 2014;28(3):333–337. doi:10.1111/jdv.12106
63. Swift DL, McGee JE, Earnest CP, Carlisle E, Nygard M, Johannsen NM. The effects of exercise and physical activity on weight loss and maintenance. Prog Cardiovasc Dis. 2018;61(2):206–213. doi:10.1016/j.pcad.2018.07.014
64. Weaver CM, Miller JW. Challenges in conducting clinical nutrition research. Nutr Rev. 2017;75(7):491–499. doi:10.1093/nutrit/nux026
65. Mirmiran P, Bahadoran Z, Gaeini Z. Common limitations and challenges of dietary clinical trials for translation into clinical practices. Int J Endocrinol Metab. 2021;19(3):e108170. doi:10.5812/ijem.108170
66. Yang SJ, Chi CC. Effects of fish oil supplement on psoriasis: a meta-analysis of randomized controlled trials. BMC Complement Altern Med. 2019;19(1):354. doi:10.1186/s12906-019-2777-0
67. Basra MK, Salek MS, Camilleri L, Sturkey R, Finlay AY. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology. 2015;230(1):27–33. doi:10.1159/000365390
68. Daundasekara SS, Arlinghaus KR, Johnston CA. Quality of life: the primary goal of lifestyle intervention. Am J Lifestyle Med. 2020;14(3):267–270. doi:10.1177/1559827620907309
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.