")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
The Classification and Selection of Adhesive Agents; an Overview for the General Dentist
Authors Arandi NZ
Received 30 June 2023
Accepted for publication 23 August 2023
Published 4 September 2023 Volume 2023:15 Pages 165—180
DOI https://doi.org/10.2147/CCIDE.S425024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Naji Ziad Arandi
Department of Conservative Dentistry, Faculty of Dentistry, Arab American University, Jenin, Palestine
Correspondence: Naji Ziad Arandi, Department of Conservative Dentistry, Faculty of Dentistry, Arab American University, Jenin, Palestine, Tel +972598126111, Email [email protected]
Abstract: Adhesive agents are essential to most restorative procedures used in everyday practice. Depending on the clinical situation, the dentist will choose among a rapidly evolving variety of adhesive agents (bonding agents). Due to the availability of many adhesive agents, appropriate selection can take time and effort. Typically, a practitioner relies more on marketing and experience than in-depth material knowledge. The classification of adhesive agents may need to be clarified and easier to remember due to its lack of relevance to clinical procedures. This paper reviews the published literature retrieved from PubMed, Google Scholar, and Scopus by using specific keywords “adhesive agents”, “classification”, “dentin”, “enamel”, “universal”, “self-etch”, “etch-and-rinse”, and “bonding”. The titles and abstracts were screened, and the relevant literature was retrieved. The list of references from each identified article was examined to find other potentially relevant articles. Adhesive agents can be classified as etch-and-rinse, self-etch, or “multi-mode” according to their approach to interacting with the smear layer, and each approach can be further classified according to the number of clinical steps required during application. This article reviews the classification of current adhesive agents and discusses the properties that make a specific adhesive agent the optimal choice for a particular clinical indication. The review will assist the general dentist in understanding the various types of available adhesive agents and how they function. Overall, the review will facilitate decision-making and allow the selection of appropriate materials.
Keywords: adhesive agents, bonding agents, classification, dentine, enamel, etch-and-rinse, self-etch, universal adhesives
Introduction
Restorative dentistry aims to treat carious or fractured teeth, restoring their structure, function, and aesthetics.1,2 Advancements in dental materials and techniques have changed how dentists approach restorative dentistry.3 Adhesive dentistry led to a paradigm shift in dental practice by allowing dentists to perform minimally invasive procedures, preserve tooth structure, and achieve superior aesthetic outcomes.4,5 Selecting and applying the appropriate adhesive agent from the wide range of adhesives available is crucial to ensuring the success of direct and indirect restorative procedures.2,6
Adhesive agents are commonly categorized from the first to the eighth generation.4,7 The concept of “generation” refers to “when” and in “what order” the manufacturer developed the adhesive.7 Each new generation attempts to simplify the bonding procedure, provide faster application techniques, and offer enhanced chemistry to promote stable and durable bonding.8 The generations overlap, and the classification becomes complex due to the perpetual development of adhesive agents, making generational classification problematic and unclear.9 The other problem with referring to adhesive systems by generation is the misconception that the adhesive system will be better as we go higher in generations.10
A classification of adhesive systems reflecting their approach to interacting with the smear layer rather than “generation” has been proposed.11 Etch-and-rinse (ER) and self-etch (SE) adhesives are the primary categories into which dental adhesives fall. According to the number of application steps during the application, ER adhesive systems are subdivided into “three-step (3-step ER)” and “two-step (2-step SE)” adhesives.12 The SE adhesive systems, in contrast, are further classified into “two-step (2-step SE)” and “one-step (1-step SE)” adhesives.13 The most recent generation of adhesives developed is the universal adhesives. These adhesives provide versatility and reduction in clinical steps. These adhesives are “universal” in two main ways: First, they can be applied to the tooth structures using any application approach (ER, SE, or selective etch) with claims by manufacturers that there is no compromise on bonding effectiveness when either bonding strategy is employed. Second, they can be used on a wide range of substrates; they can be used to bond to dentin and enamel, for the placement of both direct and indirect restorations.14 Figure 1 shows the classification of adhesive agents.
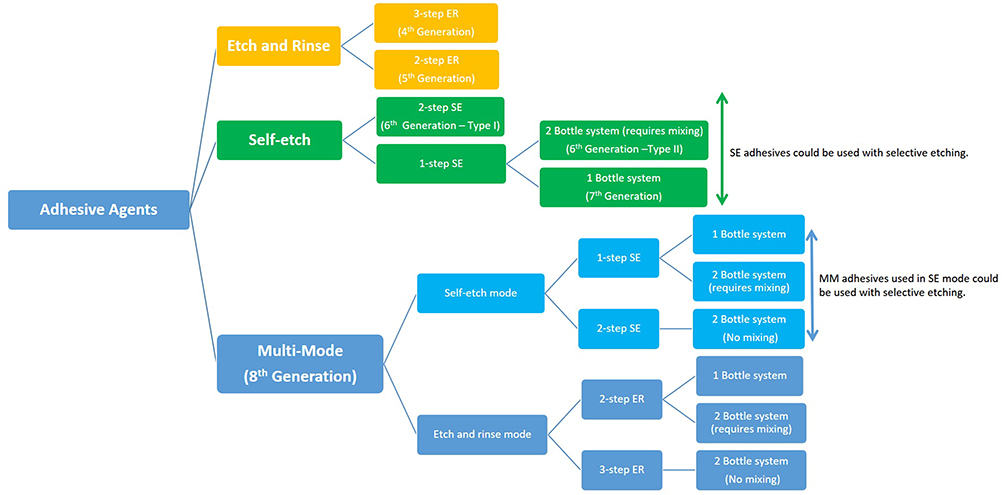 |
Figure 1 The classification of contemporary adhesive agent systems based on the approach to removing the smear layer and the number of application steps. Note: The corresponding generations were included in brackets. |
When it comes to adhesive agents, the dental practitioner has various options, each with its clinical considerations. Choosing an adhesive agent is a critical decision that will affect the procedure’s long-term success. Therefore, knowing the classification of the contemporary adhesive agents will assist the general dental practitioner make decisions. This paper reviews the classification of current adhesive agents and discusses the properties that make a specific adhesive agent the optimal choice for a particular clinical indication.
Materials and Method
A literature search was carried out in Google Scholar, PubMed and Scopus on the classification of adhesive agents. Search terms included the following MeSH terms in various combinations: “adhesive agents”, “etch and rinse”, “self-etch”, “universal”, “bonding”, “enamel”, “dentine”. Related articles that appeared in various search engines were retrieved and evaluated. The reference lists from the identified articles were examined to find other potentially relevant articles. The cross-referencing process went on until no new articles were identified. No limits were imposed on the year of publication, but only full-text articles in English were considered.
Review
Enamel and dentin are two distinct components of a tooth’s structure. Understanding these distinctions helps dental professionals tailor adhesive techniques to ensure reliable and durable bonds in both tooth components.15 Enamel is a homogeneous substrate, by weight percentage, enamel is 96% inorganic matrix and 4% organic material, as well as water, which occupies the free spaces between hydroxyapatite crystals (HA).16 The hydrophobic nature of enamel (due to the low water content) makes it an ideal and predictable substrate for micromechanical adhesion. On the other hand, the structure of the dentin poses some challenges during the adhesive procedure. On a weight basis, dentine is made up of 70% inorganic matrix, 20% organic matrix (mainly type 1 collagen), and 10% water.16 The high protein and water content of dentin makes it a very heterogeneous and dynamic substrate, increasing the difficulty of the bonding procedure. To date, resin-dentin bonds created by infiltration of hydrophilic resin monomers into demineralized dentin are imperfect.17,18 Incomplete permeation of monomer into the full depth of demineralized region may, however, leave, water-filled, exposed collagen fibrils that are unprotected from denaturation challenges19 and cause nanoleakage of water into these regions through a 20–100 nm sized marginal gap, leading to subsequent hydrolytic degradation of these collagen fibrils and the hybrid layer.20 The effect of hydrolytic (water-related) degradation seriously compromises the long-term integrity of the adhesive interface and the durability of the bond strength.20
The Etch-and-Rinse Adhesives
With ER adhesive systems, phosphoric acid is used to etch the enamel and dentin. Phosphoric acid etching raises the enamel’s surface energy and demineralizes the inorganic hydroxyapatite. Etching creates microporosities within which the resin tag extensions of the adhesive agent interlock micromechanically.21 On dentine, the acid removes the smear layer and open dentin tubules increasing dentin permeability and demineralizing the most superficial 1–5 μm of dentin, leaving behind a network of collagen fibers filled with water left from rinsing the acid.22–24
After etching and rinsing, excessive air drying of the dentin should be avoided. Overdrying the etched dentine causes the collapse of the demineralized collagen network and, consequently, the loss of the interfibrillar spaces.8 The loss of interfibrillar spaces makes it hard for the adhesive monomers to diffuse into the etched dentine structure, resulting in poor hybridization and low bond strength.12 The “wet bonding technique” was proposed25 to solve the issues associated with bonding to over-dried dentine. The “wet bonding technique” implies that the etched dentin is kept slightly moist during adhesive procedures to keep the interfibrillar spaces. This helps the diffusion of primer and adhesive monomers into the demineralized dentine and favors the hybridization process.25–27 Overall, determining “how wet dentine should be” makes the dentin bonding technique extremely sensitive. Moreover, achieving ‘moist dentine’ is not straightforward, as the enamel needs to be dried for bonding, and it is challenging to dry enamel alone without drying the dentine.
Solvents are essential components of dental adhesives and critical for optimal bonding to enamel and dentin.28 Solvents dilute the viscous monomers, and are mainly responsible for water displacement from the demineralized dentin, and facilitate their infiltration into the collagen network.25,29 Some adhesives contain acetone, whereas others contain water and/or ethanol.29 Acetone is a water-chaser; acetone-based adhesive agents are highly sensitive to the moisture level of the acid-etched dentin surface. Using acetone-based adhesives on over-dried acid-etched dentin surfaces can lead to poor results as they cannot re-expand the collapsed collagen network.30 Therefore, when an acetone-based ER adhesive is used for dentin bonding, it is necessary to keep the demineralized dentin moist and avoid over-drying the etched dentine (wet-bonding technique).31,32 However, it is challenging to determine dentine’s moisture content when such adhesives are used clinically. Ethanol is currently the solvent most commonly used in adhesive agents. It is used either alone or with water as a co-solvent. These systems are less sensitive to the moisture level, are good at re-expanding the collagen matrix, and yield higher bond strength in dry dentin.30 Normally, applying one coat of the adhesive agent from this category is sufficient to cover the entire surface; additional coats may result in a thick layer of solvent between layers. Therefore, it should be noted that using the same bonding procedure for different adhesive systems with different solvents, volatilities, and water displacement capacities may have unfavorable results.33
Three-Step Etch-and-Rinse Adhesives
The 3-step ER system is applied using a separate etchant, primer, and bonding resin (adhesive resin). The most frequently used etching agent is phosphoric acid, used in gel form. The acid is used in a 30 to 40% concentration with a pH of 0.1 to 0.4. Most etching agents are colored gels (thickened with silica microparticles) to control application and ensure all the gel is rinsed off the tooth surface.4 The primer incorporates one or more hydrophilic monomers with an organic solvent (acetone, ethanol, and/or water). The primer removes the water in the etched dentin and makes it easier for the adhesive resin monomers in the primer to penetrate the acid-etched collagen network.8 Once placed on the tooth surface, primers should not be rinsed off or light-cured; they are only air-dried to evaporate the solvent and decrease the thickness of the adhesive layer before applying the bonding resin.34,35 The bonding resin (adhesive resin) is a hydrophobic solvent-free unfilled resin applied over the primer and then light-cured.36 The hydrophobic bonding resin copolymerizes with and covers the hydrophilic polymerized primer, making it less susceptible to water sorption.8 The solvent-free adhesive resins must be gently air-blown before light curing. This is not for solvent evaporation but rather uniform and even distribution of the adhesive layer.
Two-Step Etch-and-Rinse Adhesives
The 2-step ER system (so-called one-bottle system) was introduced to reduce the number of clinical steps and simplify the procedure. In the 2-step ER adhesive systems, the hydrophilic primer and hydrophobic bonding resin are coupled with solvent(s) in the same bottle (self-priming adhesives).8 This is achieved by incorporating higher concentrations of hydrophilic monomers, such as 2-hydroxyethyl methacrylate (HEMA), to stabilize the mix and facilitate the diffusion of the self-priming adhesive into the demineralized collagen network of the etched dentin. Due to the high concentration of HEMA, the literature reports that 2-step ER systems can be more susceptible to water degradation at the resin–dentin interface than three-step ER systems.3,37
The Self-Etch Adhesives
SE adhesives incorporate acidic functional monomers with a carboxyl or phosphate group that “etches” and “primes” the tooth substrate at the same time. These adhesives leave the smear layer in place. The acidic functional monomers in SE adhesives infiltrate and modify the smear layer and demineralize the underlying tooth substrate.22,38 As a result, the dissolved smear layer and demineralization products are not rinsed away but incorporated in the hybrid layers.
Water, an inorganic and polar solvent, is a fundamental ingredient of SE adhesives. It provides the medium for ionizing the acidic monomers to demineralize dentin.29 Therefore, water is always incorporated alone or with ethanol as a co-solvent in SE adhesives.28 Consequently, SE adhesives are less affected by moisture on the dentinal surface than ER adhesives as ER adhesives are.28 Hence, the technique sensitivity associated with the moisture level of the dentine is no longer a concern for the practitioner.
Although SE adhesives are user-friendly, their inability to etch enamel effectively and phosphoric acid is a crucial shortcoming, as they result in a shallow enamel-etching pattern that may result in marginal discoloration and debonding at the margins.4 To address this issue, selective enamel etching, wherein phosphoric acid in a concentration between 30 and 50% for less than 15 sec is used to etch the enamel before the SE adhesive is applied, has been suggested.39,40 It should be noted that applying the phosphoric acid etchant and the SE system differs from the conventional ER system. Therefore, the practitioner should avoid etching the dentine during the enamel bonding.
The bond strength to the tooth structure may differ depending on the pH level and etching aggressiveness. SE adhesives can be categorized into strong (pH ≤ 1), intermediately strong (pH 1–2), mild (pH ~2), and ultra-mild SE adhesives (pH > 2.5).13 Mild SE adhesives provide excellent dentin bond strengths and poorer enamel bonds. In contrast, more aggressive SE systems provide the opposite—strong SE adhesives induce deep demineralizing effects on both enamel and dentine. For enamel, the acid-etch pattern created by strong SE adhesives resembles the pattern created by phosphoric acid etching. However, it differs from the phosphoric acid etching as the dissolved calcium phosphates are not rinsed away; these embedded calcium phosphates are very unstable and may compromise the integrity of the dentine-adhesive interface. The “ultra-mild” SE adhesives interact superficially with the tooth substrates. They can only expose dentin collagen superficially, producing “a nanohybrid layer” instead of a discrete hybrid layer.41,42
Two-Step Self-Etch Adhesives
In the 2-step SE adhesive systems, a self-etching primer that simultaneously “conditions” and “primes” the dental substrate is applied on enamel and dentin, air-dried, followed by applying and polymerizing a separate hydrophobic bonding resin. The advantage of the two-step SE adhesives is that their efficacy is less dependent on the dentin’s moisture level than the ER adhesives. Generally, 2-step SE adhesives were reported to have better bonding ability than one-step SE adhesives.
One-Step Self-Etch Adhesives
The 1-step SE (all-in-one) adhesives incorporate all the fundamental steps for bonding in one bottle. These adhesives have been made more hydrophilic and acidic than their two-step counterparts to keep these complex chemical mixtures stable. The 1-step SE adhesives are categorized into one- and two-component systems: the first system incorporates all the fundamental bonding components into one bottle. Hence, the dental surfaces’ etching, priming, and bonding are accomplished simultaneously in one step, while the other system is supplied in two bottles; the practitioner must mix the two components before application. Some manufacturers use this approach to keep water separated from the functional monomers until the time of application to avoid monomer degradation inside the bottle that might happen due to the hydrolysis of the ester groups of the resins,43 which limits their shelf life. Examples of 1-step SE adhesive that requires mixing before application include One-up Bond F Plus (Tokuyama Dental Corporation, Tokyo, Japan), Xeno III (Dentsply Caulk, Milford, DE, USA) Adper Prompt L-Pop (3M ESPE, St Paul, MN, USA), All-Bond SE (Bisco Inc, Schaumburg, IL, USA), Brush&Bond (Parkell), Futurabond NR (VOCO, Cuxhaven, Germany).
The omission of the separate application of the hydrophobic bonding resin in the 1-step SE adhesives makes them more prone to hydrolytic degradation and poor clinical performance.4,44–47 The 1-step SE adhesives have been reported to have low immediate and long-term dentin bond strengths,48,49 poor bonding to intact enamel,39 incompatibilities with self-curing resins,50 reduced shelf-life,51 poor clinical outcomes,44,46 among other shortcomings.4,48,52 Also, a meta-analysis of the literature showed that 1-step SE adhesives had weaker bonding ability than 2-step SE adhesives.53
The 1-step SE and 2-step ER adhesives are simplified variants of the 3-step ER and 2-step SE adhesives. Simplified adhesives are user-friendly and have become very popular as dentists tend to select materials that are easier to use.54 Despite their user-friendliness and lower technique sensitivity, the simplification of the adhesive approach has resulted in a lower efficacy and reduced durability.4,37,44 Due to their hydrophilicity and exclusion of hydrophobic bonding resin coating, cured adhesive layers may function as permeable membranes,55 allowing water to pass through the adhesive layer. According to the literature, dental adhesives that include a hydrophobic bonding resin as the final step of the clinical procedure, that is, 3-step ER adhesives and 2-step SE adhesives, are more stable and produce more durable restorations than their simplified counterparts. Some manufacturers offer hydrophobic liners combined with the 1-step SE adhesive (All-Bond SE/All-Bond SE liner, Bisco).
HEMA is a water-soluble monomer frequently incorporated in simplified dental adhesives. It enhances adhesive systems’ wetting properties and the adhesive’s infiltration into the collagen network. Because of its solvent-like properties, it is also added to improve the miscibility and stability of hydrophobic and hydrophilic components. It keeps the ingredients in the solution and prevents phase separation.29 Its high hydrophilicity over time increase water uptake and results in hydrolytic degradation of the adhesive interface.56 Therefore, HEMA-free adhesives were introduced to avoid HEMA’s adverse effects.3 There is no consensus regarding the influence of HEMA the on the clinical performance of composite restorations. The clinical performance of HEMA-free and HEMA-containing adhesive systems has been proven to be comparable in some investigations. However, other studies showed that the adhesive systems (HEMA-free and HEMA-containing) had different clinical results.56
Moreover, the simplified adhesives are incompatible with dual or chemically activated composite resins. When chemical cure and dual-cure resin composites are used with simplified adhesives, residual uncured acidic monomers from the oxygen-inhibited layer of the cured adhesives (not covered with a hydrophobic bonding resin) remain in direct contact with the composite material.50 The acid deactivates the aromatic tertiary amines from the dual or self-cure composite and inhibits their polymerization.50,57–59 This may become more problematic when clinician use composites and adhesives from different manufacturers. Some simplified adhesives are specially formulated for use in combination with their proprietary dual or self-cure composites with separate light curing of the adhesive as a must (eg, Clearfil S3 Bond Plus/ Clearfil DC Core Plus, Kuraray Dental). Other SE bonding systems claim incompatibility with self-cured or dual-cured composites is eliminated by mixing the adhesive with a dual-cure or self-cure activator (eg, AdheSE/ AdheSE DC, Ivoclar Vivadent). Table 1 presents the currently available ER and SE adhesives brands.
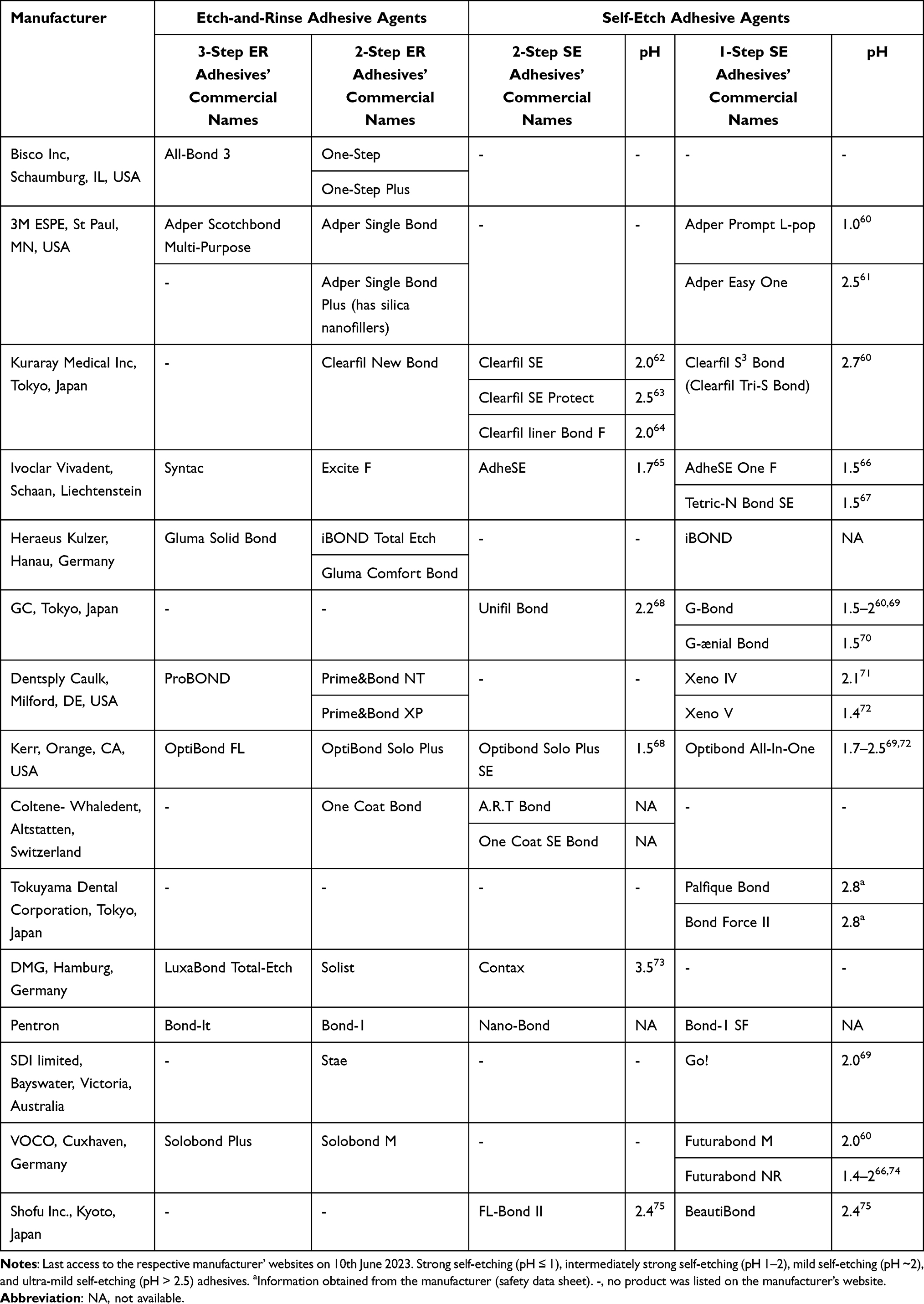 |
Table 1 The Currently Available Etch-and-Rinse and Self-Etch Adhesives Brands |
The Universal (Multi-Mode) Adhesives
Universal or multimode adhesives represent the latest generation of adhesive systems that were recently introduced following the increasing demand for simplified and user-friendly systems. The distinctive property of universal adhesives is that they can be applied with any adhesive strategy (ER, SE, and selective etching), so they have also been labeled “multi-mode”. In addition, some of these universal adhesives have the potential to bond to various other substrates used in direct and indirect procedures, including ceramics, composites, and metal substrates. The pH of the universal adhesives ranges between 1.5–3.2; thus, most of them fall under the ultra-mild (pH >2.5), mild (pH ~ 2), and intermediately strong (pH between 1 and 2) categories.14
Universal adhesives should not be confused with 1-step SE single-bottle or “all-in-one” systems. These adhesives have unique chemical compositions, they contain carboxylate or phosphate monomers. The most common of these monomers is 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP). However, several other functional monomers can be found in universal adhesives (Table 2), such as glycerol phosphate dimethacrylate (GPDM), 4-methacryloxyethyl trimellitic acid (4-MET), 4-methacryloxyethyl trimellitate anhydride (4-META), and dipentaerythritol pentaacrylate phosphate (PENTA).
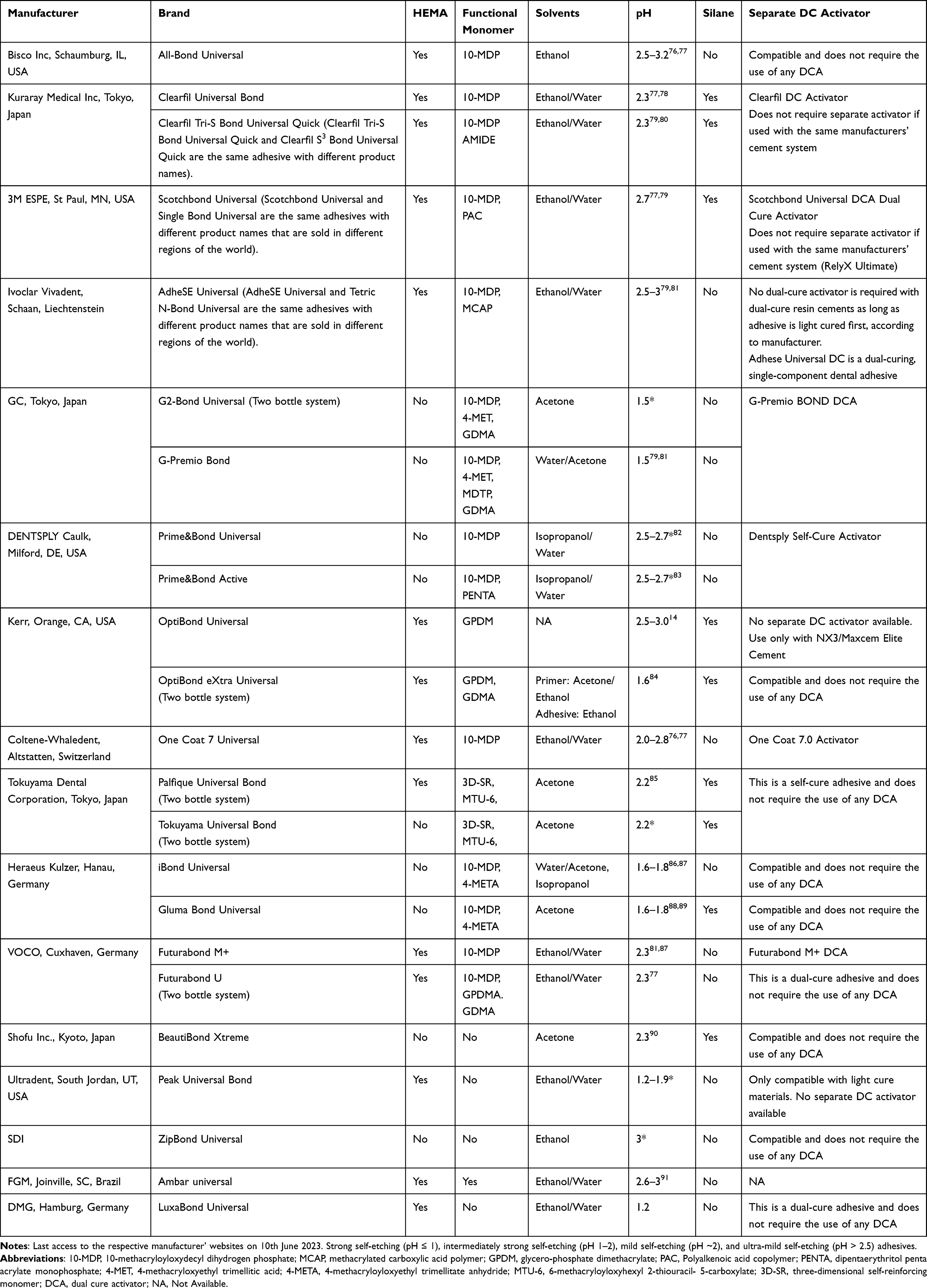 |
Table 2 The Currently Available Universal Adhesives by Brand |
The acidic monomer 10-MDP had been used by one SE adhesive system (Clearfil SE, Kuraray) for years, was added to universal adhesives when the patent expired.92 It has been shown that this 10-MDP monomer forms a stronger and more stable bond to tooth structure than acidic monomers previously used. These universal adhesives provide micromechanical retention and a chemical bond to the tooth tissues. 10-MDP has an affinity for hydroxyapatite and forms a chemical bond with apatite crystallites through ionic bonding.93 The concentration of 10-MDP varies among universal adhesives. It has been shown that the higher the monomer concentration, the better the adhesive’s bond strength.94
Universal adhesives are claimed to facilitate bonding to ceramic restorations. Universal adhesives containing 10-MDP promote bonding to zirconia,95–98 and indirect resin-based composites.99 In contrast, universal adhesives have not been able to replace silane-based primers for glass ceramics like lithium disilicate ceramics.99–102 The manufacturer claims some universal adhesives are compatible with dual-cure and self-cure composite materials.103 Not all universal adhesives are compatible with self-cured or dual-cured resin materials. Acidic universal adhesives can interfere with the polymerization of these materials.103 Some manufacturers provide a dual-cure activator that should be mixed with the universal adhesive if it is to be used with an amine-containing cement or buildup material. Example of this, are Scotchbond Universal Dual Cure Activator (Scotchbond Universal), One Coat 7 Activator, (One Coat 7 Universal) and Clearfil DC Activator (Clearfil Universal Bond Quick). However, some universal adhesives are reported to have a high enough pH that the dual-cure activator is unnecessary (eg, All-Bond Universal).
Silane has been incorporated into universal adhesives to simplify the glass-ceramic bonding procedure (Table 2). Theoretically, clinicians would not need to apply a separate silane solution after the ceramic restoration intaglio has been etched with hydrofluoric acid (HF). However, silanes have been reported to be unstable in acidic conditions containing water, and their premature hydrolysis precludes chemical interaction with glass ceramics.104–106 The literature has challenged the efficacy of using universal adhesives containing silanes with lithium disilicate restorations.101,102,107,108 Therefore, for glass ceramics, a silane coupling agent should be applied separately before applying universal adhesives, even though some of them are silane-containing.22,102,106,108 Some manufacturers provide a primer for bonding to silicate ceramics or metals. An example of this is the Gluma Ceramic Primer is used for adhesive bonding or repair of glass ceramics with Gluma Bond Universal. Likewise, the BeautiBond Universal CR Enhancer which is used as a primer for silicate and lithium silicate glass ceramics with BeautiBond Universal.
Most universal adhesives are one-bottle systems. Nevertheless, there are two-bottle universal adhesive systems. For instance, the G2-Bond Universal is a two-bottle universal adhesive system where the primer and the bonding agent are in separate bottles and applied separately from traditional two-step self-etching adhesives. Likewise, Tokuyama Universal Bond and LuxaBond Universal are two-bottle systems, but their content is intended to be mixed before application. The separation of acidic monomer and ceramic primers can prevent the deterioration of silane coupling agents that could compromise their adhesive properties and shelf time.109
HEMA is the principal hydrophilic monomer in most universal adhesives (Table 2). HEMA can interfere with the interaction between 10-MDP and Ca, potentially impairing the formation of an adequate bond in 10-MDP–containing adhesives. The presence of HEMA110 and both hydrophilic and hydrophobic ingredients in the same bottle may cause water sorption and hydrolysis of the adhesive layer, impairing universal adhesive stability.81 Studies report that universal adhesives are material-dependent4,14,111,112 and that long-term studies are still required to evaluate the stability of resin-dentin interfaces created by contemporary universal adhesives.111,113,114
The clinical performance of universal adhesives largely depends on the adhesive strategy, thus questioning their claimed versatility regarding the application mode in a clinical setting. Several systematic reviews investigated which universal adhesive application mode (SE vs ER) was best for dentin and enamel adhesion. Resin-dentin bonds were similar when using mild adhesives but statistically different (favoring the etch-and-rinse approach) when using ultra-mild adhesives.81,115,116 Additionally, evidence suggests that selective enamel etching with phosphoric acid prior to the application of “universal” adhesives is an advisable strategy for optimizing bonding. Table 2 presents the universal adhesive brands currently available.
Application Protocols
Regardless of the adhesive used, following the manufacturer’s instructions is essential. Each adhesive system will have slightly different protocols and recommended application times that are tailored to the specific composition of that adhesive. Nonetheless, a few key principles apply to all adhesives during the application process are presented in Table 3.
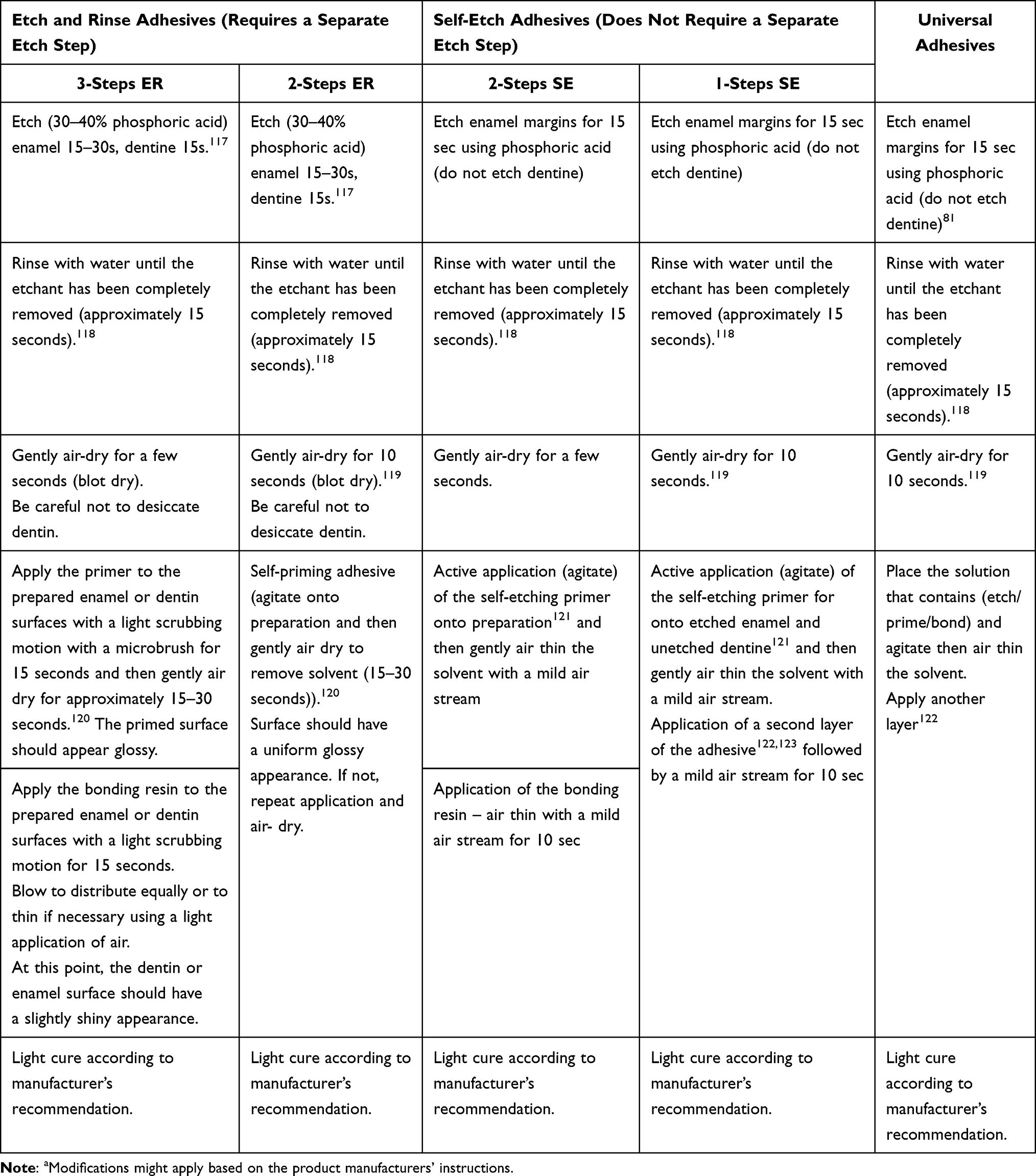 |
Table 3 Protocols of Current Adhesive Systemsa |
Special Variations
Some manufacturers add filler particles to their adhesive agents to improve the mechanical properties of the adhesive layer (eg, Tetric N Bond Total Etch, Ivoclar Vivadent and Gluma 2Bond, Kulzer). Others add Chlorhexidine to their adhesive agents to achieve bond stability by decreasing adhesive bond degradation (eg, Peak Universal Bond, Ultradent and Futurabond U, VOCO). Glutaraldehyde is another ingredient manufacturers add to dental adhesives to prevent post-operative pain and stabilize the collagen fibers in the hybrid layer to improve durability (eg, iBond Total Etch, Heraeus, Kulzer). Manufacturers include antibacterial compounds in the adhesive’s formulation to prevent recurrent caries beneath restorations. Methacryloyloxydodecylpyridinium bromide monomers (MDPB) is an example of an antimicrobial compound used in some adhesives (eg Clearfil Protect Bond, Kuraray). Another example is fluoride (eg, FL-Bond II, Shofu and Futurabond NR, Voco). Some manufacturers add dyes to their adhesives to facilitate the homogeneous mixing of two components and as a visual aid when performing the procedure. The bond becomes colorless after curing (Universal Bond, Tokuyama Dental). In general, the effect of these compounds on the performance of adhesive agents so far remains unclear and should be considered in future investigations.
Conclusion
Adhesive agents have moved towards technique simplification, and the current development of adhesive agents is driven by multitasking. The general dentist should be updated on the continually evolving adhesive agents to facilitate decision-making. The classification of adhesive dental agents typically includes three main categories: ER, SE, and universal adhesives. ER adhesives are available in 3-step and 2-step versions, while SE adhesives are available in 2-step and 1-step versions. The pH of SE adhesives has a significant impact on their bonding effectiveness. According to their pH, SE adhesives have been categorized as strong, moderately strong, mild, and ultra-mild. Universal adhesives offer versatility by enabling the dentist to select the application mode (ER, SE, or selective etch) based on the substrate and clinical situation. ER adhesives generally exhibit excellent bond efficacy. However, they require careful technique and may be sensitive to the level of dentine moisture. SE adhesives offer improved simplicity and reduced technique sensitivity, making them popular choices for clinicians. However, their bond strengths may be slightly lower compared to ER systems. Universal adhesives provide the flexibility of both techniques, combining the benefits of ER and SE adhesives. However, the performance of universal adhesives to dental hard tissues and indirect restorative materials is material-dependent because some adhesives are not indicated for bonding to all types of restorative materials. Understanding each category’s properties and limitations is essential for successful bonding and dental restorations. Continued research and improvement in adhesives will advance the field of adhesive dentistry. Hence, the practitioner must be kept continuously updated.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Cardoso J, Almeida P, Negrao R, et al. Clinical guidelines for posterior restorations based on coverage, adhesion, resistance, esthetics, and subgingival management the CARES concept: part I – partial adhesive restorations. Int J Esthet Dent. 2023;18(3):244–265.
2. O´Connor C, Gavriil D. Predictable bonding of adhesive indirect restorations: factors for success. Br Dent J. 2021;231(5):287–293. doi:10.1038/s41415-021-3336-x
3. Cardoso MV, De Almeida Neves A, Mine A, et al. Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J. 2011;56(1 Suppl):31–44. doi:10.1111/j.1834-7819.2011.01294.x
4. Perdigão J. Current perspectives on dental adhesion: (1) Dentin adhesion – not there yet. Jpn Dent Sci Rev. 2020;56(1):190–207. doi:10.1016/j.jdsr.2020.08.004
5. Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, Eden E. Minimal intervention dentistry for managing dental caries – a review Report of a FDI task group *. Int Dent J. 2012;62(5):223–243. doi:10.1111/idj.12007
6. Zhao Z, Wang Q, Zhao J, Zhao B, Ma Z, Zhang C. Adhesion of Teeth. Front Mater. 2021;7:1–11. doi:10.3389/fmats.2020.615225
7. Sofan E, Sofan A, Palaia G, Tenore G, Romeo U, Migliau G. Classification review of dental adhesive systems: from the IV generation to the universal type. Ann Stomatol. 2017;8(1):1–17. doi:10.11138/ads/2017.8.1.001
8. Sebold M, André CB, Sahadi BO, Breschi L, Giannini M. Chronological history and current advancements of dental adhesive systems development: a narrative review. J Adhes Sci Technol. 2021;35(18):1941–1967. doi:10.1080/01694243.2020.1865611
9. Powers JM, Farah J. Technique sensitivity in bonding to enamel and dentin. Compend Contin Educ Dent. 2010;31:1–8.
10. Kazak M, Donmez N. Development of dentin bonding systems from past to present. Bezmialem Sci. 2019;7(4):322–330. doi:10.14235/bas.galenos.2019.3102
11. Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003;28(3):215–235.
12. Pashley DH, Tay FR, Breschi L, et al. State of the art etch-and-rinse adhesives. Dent Mater. 2011;27(1):1–34. doi:10.1016/j.dental.2010.10.016.State
13. Van Meerbeek B, Yoshihara K, Yoshida Y, Mine A, De Munck J, Van Landuyt KL. State of the art of self-etch adhesives. Dent Mater. 2011;27(1):17–28. doi:10.1016/j.dental.2010.10.023
14. Nagarkar S, Theis-Mahon N, Perdigão J. Universal dental adhesives: current status, laboratory testing, and clinical performance. J Biomed Mater Res Part B Appl Biomater. 2019;107(6):2121–2131. doi:10.1002/jbm.b.34305
15. Liu Y, Tjäderhane L, Breschi L, et al. Limitations in bonding to dentin and experimental strategies to prevent bond degradation. J Dent Res. 2011;90(8):953–968. doi:10.1177/0022034510391799
16. Ortiz-Ruiz AJ, de Dios Teruel-Fernández J, Alcolea-Rubio LA, Hernández-Fernández A, Martínez-Beneyto Y, Gispert-Guirado F. Structural differences in enamel and dentin in human, bovine, porcine, and ovine teeth. Ann Anat. 2018;218:7–17. doi:10.1016/j.aanat.2017.12.012
17. Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R, De Stefano Dorigo E. Dental adhesion review: aging and stability of the bonded interface. Dent Mater. 2008;24(1):90–101. doi:10.1016/j.dental.2007.02.009
18. Vaidyanathan TK, Vaidyanathan J. Recent advances in the theory and mechanism of adhesive resin bonding to dentin: a critical review. J Biomed Mater Res Part B Appl Biomater. 2009;88(2):558–578. doi:10.1002/jbm.b.31253
19. Scotti N, Cavalli G, Gagliani M, Breschi L. New adhesives and bonding techniques. Why and when? Int J Esthet Dent. 2017;12(4):524–535.
20. Hashimoto M, Nagano F, Endo K, Ohno H. A review: biodegradation of resin-dentin bonds. Jpn Dent Sci Rev. 2011;47(1):5–12. doi:10.1016/j.jdsr.2010.02.001
21. Cerci BB, Roman LS, Guariza-Filho O, Camargo ES, Tanaka OM. Dental enamel roughness with different acid etching times: atomic force microscopy study. Eur J Gen Dent. 2012;1(03):187–191. doi:10.4103/2278-9626.105385
22. Perdigão J, Araujo E, Ramos RQ, Gomes G, Pizzolotto L. Adhesive dentistry: current concepts and clinical considerations. J Esthet Restor Dent. 2021;33(1):51–68. doi:10.1111/jerd.12692
23. Carvalho RM, Manso AP, Geraldeli S, Tay FR, Pashley DH. Durability of bonds and clinical success of adhesive restorations. Dent Mater. 2012;28(1):72–86. doi:10.1016/j.dental.2011.09.011
24. Perdigão J, Reis A, Loguercio AD. Dentin adhesion and MMPs: a comprehensive review. J Esthet Restor Dent. 2013;25(4):219–241. doi:10.1111/jerd.12016
25. Kanca J. Improving bond strength through acid etching of dentin and bonding to wet dentin surfaces. J Am Dent Assoc. 1992;123(9):35–43. doi:10.14219/jada.archive.1992.0248
26. Gwinnett A. Moist versus dry dentin: its effect on shear bond strength. Am J Dent. 1992;5(3):127–129.
27. Pereira GDDS, Alexandre L, Paulillo MS, De Goes MF, Dias CTDS. How wet should dentin be? Comparison of methods to remove excess water during moist bonding. J Adhes Dent. 2001;3(3):257–264.
28. Ekambaram M, Yiu CKY, Matinlinna JP. An overview of solvents in resin-dentin bonding. Int J Adhes Adhes. 2015;57:22–33. doi:10.1016/j.ijadhadh.2014.09.007
29. Van Landuyt KL, Snauwaert J, De Munck J, et al. Systematic review of the chemical composition of contemporary dental adhesives. Biomaterials. 2007;28(26):3757–3785. doi:10.1016/j.biomaterials.2007.04.044
30. Pashley DH, Tay FR, Carvalho RM, et al. From dry bonding to water-wet bonding to ethanol-wet bonding. A review of the interactions between dentin matrix and solvated resins using a macromodel of the hybrid layer. Am J Dent. 2007;20(1):7–20.
31. Tay FR, Gwinnett JA, Wei SHY. Micromorphological spectrum from overdrying to overwetting acid-conditioned dentin in water-free, acetone-based, single-bottle primer/adhesives. Dent Mater. 1996;12(4):236–244. doi:10.1016/S0109-5641(96)80029-7
32. Tay FR, Gwinnett JA, Wei SHY. Relation between water content in acetone/alcohol-based primer and interfacial ultrastructure. J Dent. 1998;26(2):147–156. doi:10.1016/S0300-5712(96)00090-5
33. Cavalheiro A, Cruz J, Sousa B, et al. Dentin adhesives application deviations: effects on permeability and nanoleakage. Dent Mater J. 2021;40(5):1160–1168. doi:10.4012/dmj.2020-404
34. Spreafico D, Semeraro S, Mezzanzanica D, et al. The effect of the air-blowing step on the technique sensitivity of four different adhesive systems. J Dent. 2006;34(3):237–244. doi:10.1016/j.jdent.2005.06.004
35. D’Arcangelo C, Vanini L, Prosperi GD, et al. The influence of adhesive thickness on the microtensile bond strength of three adhesive systems. J Adhes Dent. 2009;11(2):109–115. doi:10.3290/j.jad.a15322
36. Loguercio AD, Luque-Martinez I, Muñoz MA, Szesz AL, Cuadros-Sánchez J, Reis A. A comprehensive laboratory screening of three-step etch-and-rinse adhesives. Oper Dent. 2014;39(6):652–662. doi:10.2341/13-236
37. Peumans M, Kanumilli P, De Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Clinical effectiveness of contemporary adhesives: a systematic review of current clinical trials. Dent Mater. 2005;21(9):864–881. doi:10.1016/j.dental.2005.02.003
38. Giannini M, Makishi P, Ayres APA, et al. Self-Etch adhesive systems: a literature review. Braz Dent J. 2015;26(1):3–10. doi:10.1590/0103-6440201302442
39. Sato T, Takagaki T, Hatayama T, Nikaido T, Tagami J. Update on Enamel Bonding Strategies. Front Dent Med. 2021;2:1–10. doi:10.3389/fdmed.2021.666379
40. Szesz A, Parreiras S, Reis A, Loguercio A. Selective enamel etching in cervical lesions for self-etch adhesives: a systematic review and meta-analysis. J Dent. 2016;53:1–11. doi:10.1016/j.jdent.2016.05.009
41. Koshiro K, Sidhu SK, Inoue S, Ikeda T, Sano H. New concept of resin-dentin interfacial adhesion: the nanointeraction zone. J Biomed Mater Res Part B Appl Biomater. 2006;77(2):401–408. doi:10.1002/jbm.b.30450
42. Scholz KJ, Bittner A, Cieplik F, et al. Micromorphology of the adhesive interface of self-adhesive resin cements to enamel and dentin. Materials. 2021;14(3):1–15. doi:10.3390/ma14030492
43. Salz U, Zimmermann J, Zeuner F, Moszner N. Hydrolytic stability of self-etching adhesive systems. J Adhes Dent. 2005;7(2):107–116. doi:10.3290/j.jad.a10282
44. Peumans M, De Munck J, Mine A, Van Meerbeek B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater. 2014;30(10):1089–1103. doi:10.1016/j.dental.2014.07.007
45. Arandi NZ, Thabet M. The clinical effectiveness of adhesive agents in posterior restorations: which adhesive strategy performs better? J Oral Res Rev. 2021;13(1):65–70. doi:10.4103/jorr.jorr_25_20
46. Perdigão J, Dutra-Corrêa M, Anauate-Netto C, et al. Two-year clinical evaluation of self-etching adhesives in posterior restorations. J Adhes Dent. 2009;11(2):149–159. doi:10.3290/j.jad.a15327
47. Reis A, Leite TM, Matte K, et al. Improving clinical retention of one-step self-etching adhesive systems with an additional hydrophobic adhesive layer. J Am Dent Assoc. 2009;140(7):877–885. doi:10.14219/jada.archive.2009.0281
48. Van Landuyt KV, Mine A, de Munck J, et al. Are one-step adhesives easier to use and better performing? Multifactorial assessment of contemporary one-step self-etching adhesives. J Adhes Dent. 2009;11(3):175–190.
49. Sadek FT, Goracci C, Cardoso P, Tay F, Ferarri M. Microtensile bond strength of current dentin adhesives measured immediately and 24 hours after application. J Adhes Dent. 2005;7(4):297–302.
50. Sanares AME, Itthagarun A, King NM, Tay FR, Pashley DH. Adverse surface interactions between one-bottle light-cured adhesives and chemical-cured composites. Dent Mater. 2001;17(6):542–556. doi:10.1016/S0109-5641(01)00016-1
51. Moszner N, Salz U, Zimmermann J. Chemical aspects of self-etching enamel-dentin adhesives: a systematic review. Dent Mater. 2005;21(10):895–910. doi:10.1016/j.dental.2005.05.001
52. Van Landuyt KL, De Munck J, Snauwaert J, et al. Monomer-solvent phase separation in one-step self-etch adhesives. J Dent Res. 2005;84(2):183–188. doi:10.1177/154405910508400214
53. Vanajasan P, Dhakshinamoorthy M, Subba Rao C. Factors affecting the bond strength of self-etch adhesives: a meta-analysis of literature. J Conserv Dent. 2011;14(1):62. doi:10.4103/0972-0707.80746
54. Arandi NZ, Thabet M. Knowledge and Attitudes of Dentists toward Adhesive System Selection: a Cross-sectional Study from Palestine. J Int Soc Prev Community Dent. 2020;10(1):107–115. doi:10.4103/jispcd.JISPCD_385_19
55. Tay FR, Frankenberger R, Krejci I, et al. Single-bottle adhesives behave as permeable membranes after polymerization. I. In vivo evidence. J Dent. 2004;32(8):611–621. doi:10.1016/j.jdent.2004.04.006
56. da Silva TSP, de Castro RF, Magno MB, Maia LC, Silva e Souza MHD. Do HEMA-free adhesive systems have better clinical performance than HEMA-containing systems in noncarious cervical lesions? A systematic review and meta-analysis. J Dent. 2018;74:1–14. doi:10.1016/j.jdent.2018.04.005
57. Tay FR, Suh BI, Pashley DH, Prati C, Chuang S-F, Li F. Factors contributing to the incompatibility between simplified-step adhesives and self-cured or dual-cured composites. Part II. Single-bottle, total-etch adhesive. J Adhes Dent. 2003;5(2):91–105.
58. Suh B, Feng L, Pashley D, Tay F. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual-cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent. 2003;5(4):267–282.
59. Tay F, Pashley D, Yiu C, Sanares AME, Wei SHY. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual-cured composites. Part I. Single-step self-etching adhesive. J Adhes Dent. 2003;5(1):27–40.
60. Ozmen B, Koyuturk AE, Tokay U, Cortcu M, Sari ME. Evaluation of bond strength of self-etching adhesives having different pH on primary and permanent teeth dentin. J Appl Biomater Funct Mater. 2015;13(3):e274–e279. doi:10.5301/jabfm.5000234
61. Zecin-Deren A, Lukomska-Szymanska M, Szczesio-Wlodarczyk A, Piwonski I, Sokolowski J, Lapinska B. The influence of application protocol of simplified and universal adhesives on the dentin bonding performance. Appl Sci. 2020;10(1):1–17. doi:10.3390/app10010124
62. Pinna R, Usai P, Arrica M, Milia E. Effectiveness of two self-etchings bonded clinically in caries affected dentin with homogeneous smear layer. J Nanomater. 2015;2015:1–7. doi:10.1155/2015/489183
63. Khoroushi M, Mansoori M. Marginal sealing durability of two contemporary self-etch adhesives. ISRN Dent. 2012;2012:1–8. doi:10.5402/2012/204813
64. Yavuz HF, Eyüboğlu GB. The effect of blood contamination on shear bond strength of calcium silicate-based pulp capping materials. Cumhur Dent J. 2021;24(4):371–385. doi:10.7126/cumudj.1007704
65. Salvio LA, Di Hipólito V, Martins AL, de Goes MF. Hybridization quality and bond strength of adhesive systems according to interaction with dentin. Eur J Dent. 2013;7(3):315–326. doi:10.4103/1305-7456.115416
66. Nicolas-Silvente AI, Nicolas-Silvente AI, Chiva-Garcia F, Sanchez-Perez A. The effect of dental enamel pre-etching for self-etching adhesives according to their primer pH: an in vitro bond strength, etching pattern and adhesive failure evaluation. J Dent Open Access. 2020;2(1):1–7. doi:10.31487/j.jdoa.2020.01.05
67. Huang YH, Wang YL, Lin PY, Lai YJ, Cheng CW, Chiang YC. Dentists’ performance in dentin-composite resin bonding before and after hands-on course learning. J Formos Med Assoc. 2020;119(1):260–267. doi:10.1016/j.jfma.2019.05.008
68. Di Francescantonio M, de Oliveira MT, Shinohara MS, Ambrosano GMB, Giannini M. Bond strength evaluation of self-etch and total-etch adhesive systems on intact and ground human enamel. Brazilian J Oral Sci. 2007;6(23):1462–1466.
69. Asande Adebayo O, Francis Burrow M, John Tyas M. Bonding of one-step and two-step self-etching primer adhesives to dentin with different tubule orientations. Acta Odontol Scand. 2008;66(3):159–168. doi:10.1080/00016350802123118
70. Amend S, Frankenberger R, Oschmann T, Lucker S, Winter J, Kramer N. Long- term microtensile bond strength of self- etch adhesives and influence of 7- s phosphoric acid etching on adhesion of a 3- step etch- and- rinse adhesive to the dentine of primary teeth. Int J Paediatr Dent. 2021;32(5):649–659. doi:10.1111/ipd.12943
71. Jamadar A, Vanti A, Uppin V, Pujar M, Ghivari S, Vagarali H. Comparative evaluation of shear bond strength of sixth- And seventh-generation bonding agents with varying pH - An in vitro study. J Conserv Dent. 2020;23(2):169–173. doi:10.4103/JCD.JCD_543_19
72. Ulker M, Ulker HE, Karabekiroglu S, Botsali MS, Cetin AR. Effect of alternative modes of application on microleakage of one-step self-etch adhesives. J Dent Sci. 2013;8(4):425–431. doi:10.1016/j.jds.2012.09.017
73. Kim Y-H, Shin D-H. Effect of chlorhexidine application on the bond strength of resin core to axial dentin in endodontic cavity. Restor Dent Endod. 2012;37(4):207. doi:10.5395/rde.2012.37.4.207
74. Poggio C, Beltrami R, Scribante A, Colombo M, Chiesa M. Shear bond strength of one-step self-etch adhesives: pH influence. Dent Res J. 2015;12(3):209–214.
75. Sabatini C. Effect of phosphoric acid etching on the shear bond strength of two self-etch adhesives. J Appl Oral Sci. 2013;21(1):56–62. doi:10.1590/1678-7757201302370
76. Costa DM, Somacal DC, Borges GA, Spohr AM. Bond capability of universal adhesive systems to dentin in self-etch mode after short-term storage and cyclic loading. Open Dent J. 2017;11(1):276–283. doi:10.2174/1874210601711010276
77. Siqueira FSF, Cardenas AM, Ocampo JB, et al. Bonding performance of universal adhesives to eroded dentin. J Adhes Dent. 2018;20(2):121–132. doi:10.3290/j.jad.a40300
78. Malaquias P, Gutiérrez MF, Sutil E, et al. Universal adhesives and dual-cured core buildup composite material: adhesive properties. J Appl Oral Sci. 2020;28:1–15. doi:10.1590/1678-7757-2020-0121
79. Papadogiannis D, Dimitriadi M, Zafiropoulou M, Gaintantzopoulou MD, Eliades G. Universal adhesives: setting characteristics and reactivity with dentin. Materials. 2019;12(10):1720. doi:10.3390/MA12101720
80. Shioya Y, Tichy A, Yonekura K, et al. Sodium p-toluenesulfinate enhances the bonding durability of universal adhesives on deproteinized eroded dentin. Polymers. 2021;13(22):1–11. doi:10.3390/polym13223901
81. Cuevas-Suárez CE, da Rosa WLO, Lund RG, da Silva AF, Piva E. Bonding performance of universal adhesives: an updated systematic review and meta-analysis. J Adhes Dent. 2019;21(1):7–26. doi:10.3290/j.jad.a41975
82. Hardan L, Bourgi R, Cuevas-Suárez CE, et al. The bond strength and antibacterial activity of the universal dentin bonding system: a systematic review and meta-analysis. Microorganisms. 2021;9(6):1230. doi:10.3390/microorganisms9061230
83. Cavalheiro A, Cruz J, Sousa B, et al. Effect of application deviations on dentin sealing of a universal adhesive: permeability and nanoleakage. Eur J Dent. 2023;17(1):242–249. doi:10.1055/s-0042-1745767
84. Takamizawa T, Yokoyama M, Sai K, et al. Effect of adhesive application method on the enamel bond durability of a two-step adhesive system utilizing a universal adhesive-derived primer. Appl Sci. 2021;11(16):1–18. doi:10.3390/app11167675
85. Kamel M, Mehena M, Soliman Z. The impact of application mode of three universal adhesives with different chemical compositions and curing techniques on their micro shear bond strength to dentin. Egypt Dent J. 2022;68(4):3783–3791. doi:10.21608/edj.2022.161374.2249
86. Staxrud F, Valen H. Potential of «universal» bonding agents for composite repair. Biomater Investig Dent. 2022;9(1):41–46. doi:10.1080/26415275.2022.2073234
87. Stape THS, Tulkki O, Salim IA, Jamal KN, Mutluay MM, Tezvergil-Mutluay A. Composite repair: on the fatigue strength of universal adhesives. Dent Mater. 2022;38(2):231–241. doi:10.1016/j.dental.2021.12.003
88. Demirel G, Kaya Demirsoy FF, Irmak Ö. Cytotoxicity evaluation of eluates from universal adhesives by real-time cell analysis. Dent Mater J. 2020;39(5):815–824. doi:10.4012/dmj.2019-221
89. Ugurlu M. Effect of the double application of universal adhesives on the dentine bond strength after radiotherapy. Aust Dent J. 2020;65(3):181–188. doi:10.1111/adj.12744
90. Yuan Y, Intajak P, Islam R, et al. Effect of sodium hypochlorite on bonding performance of universal adhesives to pulp chamber dentin. J Dent Sci. 2023;18(3):1116–1124. doi:10.1016/j.jds.2022.11.007
91. Garcia RN, de Araújo Neto VG, Silva CR, Miguel LCM, Giannini M. Microshear bond strength of universal adhesives to enamel and dentin: an eighteen-month in vitro study. Brazilian Dent Sci. 2021;24(4):1–9. doi:10.4322/BDS.2021.E2791
92. Alex G. Universal adhesives: the next evolution in adhesive dentistry? Compend Contin Educ Dent. 2015;36(1):15–26.
93. Yoshida Y, Nagakane K, Fukuda R, et al. Comparative study on adhesive performance of functional monomers. J Dent Res. 2004;83(6):454–458. doi:10.1177/154405910408300604
94. Yoshihara K, Nagaoka N, Okihara T, et al. Functional monomer impurity affects adhesive performance. Dent Mater. 2015;31(12):1493–1501. doi:10.1016/j.dental.2015.09.019
95. Lima RBW, Silva AF, da Rosa WL, Piva E, Duarte RM, De Souza GM. Bonding efficacy of universal resin adhesives to zirconia substrates: systematic review and meta-analysis. J Adhes Dent. 2023;25(1):51–62. doi:10.3290/J.JAD.B3868649
96. Dos Santos RA, de Lima EA, Mendonça LS, et al. Can universal adhesive systems bond to zirconia? J Esthet Restor Dent. 2019;31(6):589–594. doi:10.1111/jerd.12521
97. Pereira LL, Campos F, Dal Piva AMO, Gondim LD, Souza ROA, Özcan M. Can application of universal primers alone be a substitute for airborne-particle abrasion to improve adhesion of resin cement to zirconia? J Adhes Dent. 2015;17(2). doi:10.3290/J.JAD.A33974
98. Amaral M, Belli R, Cesar PF, Valandro LF, Petschelt A, Lohbauer U. The potential of novel primers and universal adhesives to bond to zirconia. J Dent. 2014;42(1):90–98. doi:10.1016/j.jdent.2013.11.004
99. Makishi P, André CB, Silva JPLE, Bacelar-Sá R, Correr-Sobrinho L, Giannini M. Effect of storage time on bond strength performance of multimode adhesives to indirect resin composite and lithium disilicate glass ceramic. Oper Dent. 2016;41(5):541–551. doi:10.2341/15-187-L
100. Lima RBW, de Muniz IAF, Campos DES, et al. Effect of universal adhesives and self-etch ceramic primers on bond strength to glass ceramics: a systematic review and meta-analysis of in vitro studies. J Prosthet Dent. 2022. doi:10.1016/J.PROSDENT.2022.01.011
101. Kim YR, Kim JH, Son SA, Park JK. Effect of silane-containing universal adhesives on the bonding strength of lithium disilicate. Materials. 2021;14(14):1–11. doi:10.3390/ma14143976
102. Kalavacharla VK, Lawson NC, Ramp LC, Burgess JO. Influence of etching protocol and silane treatment with a universal adhesive on lithium disilicate bond strength. Oper Dent. 2015;40(4):372–378. doi:10.2341/14-116-L
103. Gutiérrez MF, Sutil E, Malaquias P, et al. Effect of self-curing activators and curing protocols on adhesive properties of universal adhesives bonded to dual-cured composites. Dent Mater. 2017;33(7):775–787. doi:10.1016/j.dental.2017.04.005
104. Tichý A, Hosaka K, Tagami J. Universal adhesives - A new direction in the development of adhesive systems. Czech Dent J. 2020;1:4–12.
105. Dimitriadi M, Panagiotopoulou A, Pelecanou M, Yannakopoulou K, Eliades G. Stability and reactivity of γ-ΜPTMS silane in some commercial primer and adhesive formulations. Dent Mater. 2018;34(8):1089–1101. doi:10.1016/j.dental.2018.05.006
106. Yao C, Yu J, Wang Y, Tang C, Huang C. Acidic pH weakens the bonding effectiveness of silane contained in universal adhesives. Dent Mater. 2018;34(5):809–818. doi:10.1016/j.dental.2018.02.004
107. Moro AFV, Ramos AB, Rocha GM, Perez CDR. Effect of prior silane application on the bond strength of a universal adhesive to a lithium disilicate ceramic. J Prosthet Dent. 2017;118(5):666–671. doi:10.1016/j.prosdent.2016.12.021
108. Yoshihara K, Nagaoka N, Sonoda A, et al. Effectiveness and stability of silane coupling agent incorporated in “universal” adhesives. Dent Mater. 2016;32(10):1218–1225. doi:10.1016/j.dental.2016.07.002
109. Iliev G, Hardan L, Kassis C, et al. Shelf life and storage conditions of universal adhesives: a literature review. Polymers. 2021;13(16):2708. doi:10.3390/polym13162708
110. Münchow EA, Zanchi CH, Ogliari FA, Silva MG, de Oliveira IR, Piva E. Replacing HEMA with alternative dimethacrylates in dental adhesive systems: evaluation of polymerization kinetics and physicochemical properties. J Adhes Dent. 2014;16(3):221–228. doi:10.3290/j.jad.a31811
111. Hurtado A, Fuentes V, Cura M, Tamayo A, Ceballos L. Long-Term In Vitro Adhesive Properties of Two Universal Adhesives to Dentin. Materials. 2023;16(9):1–12. doi:10.3390/ma16093458
112. Takamizawa T, Barkmeier WW, Tsujimoto A, et al. Influence of different etching modes on bond strength and fatigue strength to dentin using universal adhesive systems. Dent Mater. 2016;32(2):e9–e21. doi:10.1016/j.dental.2015.11.005
113. Chen C, Niu LN, Xie H, et al. Bonding of universal adhesives to dentine--Old wine in new bottles? J Dent. 2015;43(5):525–536. doi:10.1016/J.JDENT.2015.03.004
114. Salem AA, Nassif MS, El-Korashy DI. Durability of bond strength to dentin using two universal adhesives in different etching modes. Brazilian J Oral Sci. 2021;20:1–15. doi:10.20396/bjos.v20i00.8660445
115. Triani F, Pereira da Silva L, Ferreira Lemos B, Domingues J, Teixeira L, Manarte-Monteiro P. Universal adhesives: evaluation of the relationship between bond strength and application strategies—a systematic review and meta-analyses. Coatings. 2022;12(10):1–16. doi:10.3390/coatings12101501
116. Da Rosa WLDO, Piva E, Da Silva AF. Bond strength of universal adhesives: a systematic review and meta-analysis. J Dent. 2015;43(7):765–776. doi:10.1016/j.jdent.2015.04.003
117. Zhu JJ, Tang ATH, Matinlinna JP, Hägg U. Acid etching of human enamel in clinical applications: a systematic review. J Prosthet Dent. 2014;112(2):122–135. doi:10.1016/j.prosdent.2013.08.024
118. Fallahzadeh F, Atai M, Ghasemi S, Mahdkhah A. Effect of rinsing time and surface contamination on the bond strength of silorane-based and dimethacrylate-based composites to enamel. J Clin Exp Dent. 2018;10(11):e1115. doi:10.4317/jced.55148
119. Carvalho CN, Lanza MDS, Dourado LG, Carvalho EM, Bauer J. Impact of solvent evaporation and curing protocol on degree of conversion of Etch-and-Rinse and multimode adhesives systems. Int J Dent. 2019;2019:1–6. doi:10.1155/2019/5496784
120. Awad MM, Alrahlah A, Matinlinna JP, Hamama HH. Effect of adhesive air-drying time on bond strength to dentin: a systematic review and meta-analysis. Int J Adhes Adhes. 2019;90:154–162. doi:10.1016/j.ijadhadh.2019.02.006
121. Hardan L, Bourgi R, Cuevas-Suárez CE, et al. Effect of different application modalities on the bonding performance of adhesive systems to dentin: a systematic review and meta-analysis. Cells. 2023;12(1):1–22. doi:10.3390/cells12010190
122. Fujiwara S, Takamizawa T, Barkmeier WW, et al. Effect of double-layer application on bond quality of adhesive systems. J Mech Behav Biomed Mater. 2018;77:501–509. doi:10.1016/j.jmbbm.2017.10.008
123. Choi C-K, Son S-A, J-H H, et al. Influence of application methods of one-step self-etching adhesives on microtensile bond strength. J Korean Acad Conserv Dent. 2011;36(3):203. doi:10.5395/jkacd.2011.36.3.203
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.