")
Back to Journals » Patient Preference and Adherence » Volume 18
The Body weight Reducing Effects of Tirzepatide in People with and without Type 2 Diabetes: A Review on Efficacy and Adverse Effects
Authors Jensen TL , Brønden A, Karstoft K, Sonne DP, Christensen MB
Received 3 October 2023
Accepted for publication 17 January 2024
Published 8 February 2024 Volume 2024:18 Pages 373—382
DOI https://doi.org/10.2147/PPA.S419304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Thomas Leth Jensen,1 Andreas Brønden,1 Kristian Karstoft,1,2 David Peick Sonne,1,2 Mikkel Bring Christensen1– 3
1Department of Clinical Pharmacology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, DK-2400, Denmark; 2Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, DK-2200, Denmark; 3Center for Translational Research, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, DK-2400, Denmark
Correspondence: Mikkel Bring Christensen, Email [email protected]
Abstract: Obesity is becoming more frequent and has several negative health impacts. Recent advances in weight management strategies have primarily resided in pharmaceutical treatments, and the glucagon-like peptide-1 (GLP-1) receptor agonists have shown great potential in terms of body weight reduction in addition to improving glycemic control in patients with type 2 diabetes (T2D). Recently, the dual GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptor agonist tirzepatide has been developed. Tirzepatide has shown strong effects on glycated hemoglobin (HbA1C) levels in several clinical trials including participants with T2D (SURPASS program). In addition to its lowering effect on HbA1C, tirzepatide leads to substantial reductions in body weight, and a series of clinical trials (SURMOUNT program) have investigated the effects on body weight as the primary outcome. In these two trial programs, tirzepatide in doses of 5 mg to 15 mg administered subcutaneously once weekly resulted in body weight reduction of up to 15% in participants with T2D and up to 21% in participants without T2D, despite comparable baseline bodyweight. Across the two trial programs, adverse effects were mainly gastrointestinal (nausea, diarrhea, and vomiting) occurring with similar incidences of vomiting and lower incidences of diarrhea and nausea in trial participants with T2D compared to trials participants without T2D. Overall, discontinuation due to adverse events occurred in 3– 7% of participants with no major differences between individuals with and without T2D. The higher weight-reducing efficacy of tirzepatide in trial participants without T2D is currently unexplained and may be partly reflected in dissimilarities in frequencies of gastrointestinal adverse events. The weight reducing effects of tirzepatide hold great promise for weight management in obese patients regardless of the presence of T2D.
Keywords: tirzepatide, weight loss, type 2 diabetes, GLP-1, GIP, dual agonists, safety
Introduction
Obesity, defined by the World Obesity Federation as having a body mass index (BMI) ≥30, is becoming increasingly prevalent with an expected rise from 14% of the global population in 2023 up to 24% of the global population by 2035. Thus, 2 billion people globally are expected to be obese by 2035.1 Obesity has an impact on morbidity and mortality and results inweight-related complications resulting in reduced quality of life for patients, and obesity increases the risk of developing type 2 diabetes (T2D), cardiovascular diseases and certain types of cancer.1,2 According to current trends extrapolating the severe detrimental effects of obesity on health, it has been estimated that overweight and obesity gave rise to a lost income of almost 2 trillion USD on a global scale in 2020, a number expected to rise to over 4 trillion USD in 2035.1
Recent advances in the treatment of obesity include refinement of bariatric surgery, improved efficacy of lifestyle and behavioral interventions, and novel weight-loss medications.2 For many years pharmacological options were limited to compounds with very sparse efficacy (eg, orlistat eliciting <6 kg weight loss after 4 years).3 Recent advancements in weight-loss medications have largely centered around harnessing the physiological effects of the incretin hormones. The incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) amplify insulin secretion in a glucose-dependent manner, and furthermore, GLP-1 has been demonstrated to reduce appetite and food ingestion. This has given rise to the development of GLP-1 receptor agonists that were initially approved for the treatment of T2D, and which have now been approved for the treatment of obesity.4,5 While early GLP-1 receptor agonists showed weight loss in the range of 5% compared with placebo, newer drugs with more continuous activation of the GLP-1 receptor have elicited body weight reductions of up to 15% from baseline.6,7 Currently, the GLP-1 receptor mono-agonists liraglutide and semaglutide have both been approved for the treatment of T2D as well as obesity.8,9
Based on the beneficial potential of GLP-1 receptor agonists, development of dual-agonists (a single molecule with agonistic effect on two different receptors) has included development of drugs with co-agonism at the GLP-1 and/or GIP receptors as well as the glucagon receptor.10 Tirzepatide, a dual-agonist targeting GIP and GLP-1 receptors, had a pronounced effect on body weight reductions in preclinical trials compared to established GLP-1 receptor mono-agonists.5,11 Tirzepatide has shown strong effects on glycated hemoglobin (HbA1C) as a primary outcome in a range of clinical trials (SURPASS program). In addition, several clinical trials have investigated the effects of tirzepatide specifically for the treatment of obesity (SURMOUNT program). Tirzepatide is now approved for treatment of T2D in both the US and in Europe (tradename: Mounjaro®), and in the US for chronic weight management in adults with obesity or overweight and at least one weight-related condition (tradename: Zepbound®).12–14
This review summarizes the effects of the GLP-1 and GIP dual-agonist tirzepatide on weight loss alongside the safety profile of this compound, with a specific focus on differences between patients with and without T2D.
Tirzepatide
Tirzepatide is a dual-agonist molecule that activates both the GLP-1 and the GIP receptor and is administered subcutaneously (s.c.) once weekly.15 Tirzepatide binds to the GLP-1 receptor with a 20% affinity compared with native GLP-1 and activates the receptor (measured by cAMP generation) with a 20-fold lower potency. In comparison, the GLP-1 agonist semaglutide binds to the GLP-1 receptor with a 60% affinity of that of native GLP-1. The affinity and potency of tirzepatide on the GIP receptor is similar to that of native human GIP.16,17 Tirzepatide consists of a single molecule with a linear 39 amino acid peptide backbone with an acyl fat-chain conjugation to enhance albumin binding and prolong half-life.18 The bioavailability of tirzepatide is 81% and the maximum plasma concentration is reached 48 hours (range: 12–96 hours) after administration.12,19,20 The half-life of tirzepatide is 117 hours and it is eliminated by proteolytic cleavage, amide hydrolysis and β-oxidation, while the cytochrome P450 enzymes are not involved in elimination. Neither hepatic nor renal impairment substantially affect the pharmacokinetics of tirzepatide.12,16,17,19–21
Clinical Data
Two clinical trial programs investigating the efficacy and safety of tirzepatide have been performed; one primarily evaluating efficacy on bodyweight (SURMOUNT) and another primarily evaluating the glucose-lowering efficacy (SURPASS). An overview of the SURMOUNT trials is shown in Table 1.22–27 The SURMOUNT-1 trial investigated the weight-reducing effect of tirzepatide in obese participants without T2D (of note 1032 out of 2539 participants had prediabetes defined as having a HbA1C of 5.7–6.4% (39–47 mmol/mol)). The SURMOUNT-2 trial (N = 938) investigated weight loss in participants with T2D and overweight (BMI > 27), and both trials investigated the effect of 10 mg and 15 mg s.c. once weekly doses of tirzepatide, while the SURMOUNT-1 trial also investigated the effect of 5 mg s.c. once weekly.26,27
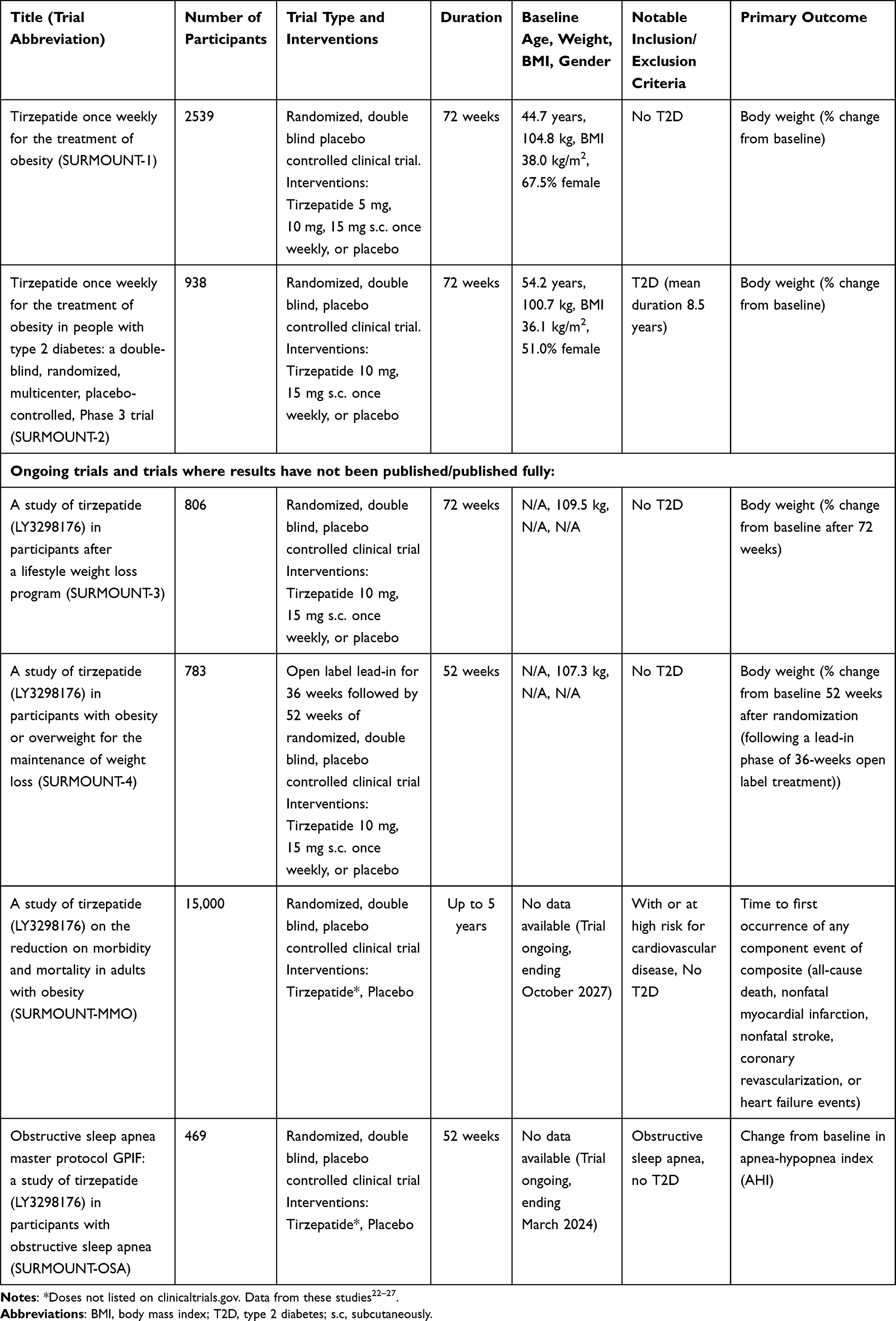 |
Table 1 Overview of Studies in the SURMOUNT Trial Program |
The SURPASS clinical trial program included only participants with T2D and had mean change in HbA1C as the primary endpoint, whereas weight loss was reported as a secondary outcome. In the SURPASS-2 trial tirzepatide was compared to the GLP-1 agonist semaglutide 1 mg s.c. once weekly, and in the SURPASS J-Mono tirzepatide was compared to the GLP-1 agonist dulaglutide 0.75 mg s.c. once weekly. The SURPASS-1 trial examined tirzepatide as monotherapy while the remaining SURPASS trials applied tirzepatide as an add-on to other glucose-lowering therapies comprised by metformin, insulin, SGLT2 inhibitors, sulfonylurea, or a combination of these.28–35
Body Weight
The SURMOUNT-1 trial, investigating doses of 5 mg, 10 mg, and 15 mg s.c. once weekly in individuals with obesity (BMI > 30.0 or BMI > 27 and weight-related complications) but no T2D, reported a reduction in bodyweight of up to 20.9% (treatment policy estimand) after 72 weeks of treatment with maximum dose of tirzepatide (15 mg s.c. once weekly), while placebo elicited a weight loss of 3.1%.27 The SURMOUNT-2 trial investigated doses of 10 mg and 15 mg s.c. once weekly in patients with overweight (BMI > 27) and T2D and reported a weight loss of 14.7% (treatment policy estimand) for the high-dose treatment arm after 72 weeks compared to a weight loss of 3.2% following placebo treatment.26
The SURPASS trials investigated the effect of tirzepatide in participants with T2D and reported weight reductions of 5–14%.28–35 The SURPASS-2 trial compared all doses of tirzepatide to 1 mg s.c. once weekly of semaglutide and reported that the 15 mg dose of tirzepatide on average resulted in an absolute reduction in body weight of 6.6% more than semaglutide.29
Other Outcomes of Interest
Improvements in several metabolic markers have been reported following treatment with tirzepatide. The SURPASS trials reported reductions in HbA1C ranging from 20.4 mmol/mol (5 mg tirzepatide s.c. once weekly dose) to 28.2 mmol/mol (15 mg tirzepatide s.c. once weekly dose) after treatment durations lasting 40–52 weeks.28–35 Trials in Japanese populations reported even greater reductions in HbA1C (reduction of 33.0 mmol/mol in the 15 mg tirzepatide s.c. once weekly dose).34 Furthermore, reductions in systolic blood pressure of 4.7–12.6 mmHg and reductions in diastolic blood pressure of 0.8–5.6 mmHg were reported in the SURPASS trials. Total cholesterol was reduced by 2.2–15.4%, LDL was reduced by 5.3–19.3% (except for the SURMOUNT-2 trial that reported an increase of 2.3–3.2%) and HDL was increased by 0.9–10.8%.26–34 While these changes may be, in part, mediated by body weight reductions, they are nevertheless important improvements in measurable metabolic markers.22,23
Some important sub-group analyses have been performed to investigate other factors affected by treatment with tirzepatide. The SURPASS-1 trial reported a reduction in total body fat mass of 26% [95% confidence interval (CI): 20–31%] for all tirzepatide doses pooled (5 mg, 10 mg and 15 mg tirzepatide s.c. once weekly groups) compared to placebo.28 Magnetic resonance imaging (MRI) was performed for a subgroup in the SURPASS-3 trial to investigate changes in liver fat. In the SURPASS-3 trial, participants had an average T2D duration of 8.4 years, a mean BMI of 33.5 kg/m2, and were treated with metformin alone or in combination with an SGLT2 inhibitor. Participants in the MRI sub-study had a fatty liver index ≥60.30,36 An absolute reduction of 8.1% from a baseline liver fat content of 15.7% was demonstrated for pooled 10 mg and 15 mg s.c. once weekly tirzepatide groups, compared to an absolute reduction in liver fat content of 3.4% in participants treated with insulin degludec.36 Tirzepatide has shown reductions in both body fat mass and lean body mass.37 MRI analysis of body composition in a subset of participants from the SURPASS-3 study revealed a larger decrease in muscle fat infiltration than anticipated. However, it also indicated an overall reduction in fat-free muscle mass (−0.76 liters for the 15 mg s.c. once weekly group).38
Risk of major adverse cardiovascular events (MACE) was analyzed in a meta-analysis for all SURPASS trials and showed no statistically significant differences between pooled tirzepatide groups and control groups (hazard-ratio (HR) 0.80 [95% CI: 0.57–1.11]). The same study provided a meta-analysis of events of cardiovascular death and all-cause mortality in participants treated with tirzepatide and reported HRs of 0.90 [95% CI: 0.5–1.6] and 0.80 [95% CI: 0.51–1.3], respectively.39
Clinical Safety
Tirzepatide has in clinical testing shown to be safe and relatively well tolerated with mild to moderate adverse effects that most frequently were of gastrointestinal nature. In early clinical testing (phase I and Phase II trials) a gradual dose escalation was implemented, which increased tolerability and reduced the frequency of adverse events (AEs).40,41 Thus, in the trial programs tirzepatide was started with a dose of 2.5 mg tirzepatide s.c. once weekly and followed by increases in dose of 2.5 mg every 4 weeks.
AEs in the SURMOUNT-1 trial (participants without T2D) were seen in up to 82% of participants, with 4–7% discontinuing the trial due to AEs (compared with 3% in the placebo group).27 In the SURMOUNT-2 trial (participants with T2D with a mean duration of 8.5 years), up to 78% of participants experienced AEs and 4–7% discontinued due to AEs (compared with 4% in the placebo group).26 Hypoglycemia (<3.0 mmol/L) was seen in up to 2% of participants without T2D (SURMOUNT-1) and up to 4% of participants with T2D, while no cases of severe hypoglycemia was reported in the SURMOUNT-1 or −2 trials.26,27 In patients treated with sulfonylurea at baseline in the SURPAS-4 trial, 9% of participants experienced hypoglycemia, while 19% of participants treated with both sulfonylurea and insulin glargine experienced hypoglycemia.31
Discontinuations due to AEs were primarily due to gastrointestinal events, and AEs were often reported in the dose-escalation phase and then decreased in frequency over time.19,32,34 Frequency of gastrointestinal adverse events in participants with and without T2D, as well as weight loss, is illustrated in Figure 1. The duration of diarrhea, nausea and vomiting was reported in the SURPASS-AP-Combo trial, a trial investigating the effect of tirzepatide in an Asian-Pacific population with T2D, in which the mean duration of these AEs were 3 days, 3–4 days, and 1–2 days, respectively.35 There was a similar frequency of gastrointestinal side-effects compared to semaglutide in the SURPASS-2 trial (1 mg s.c. once weekly).29
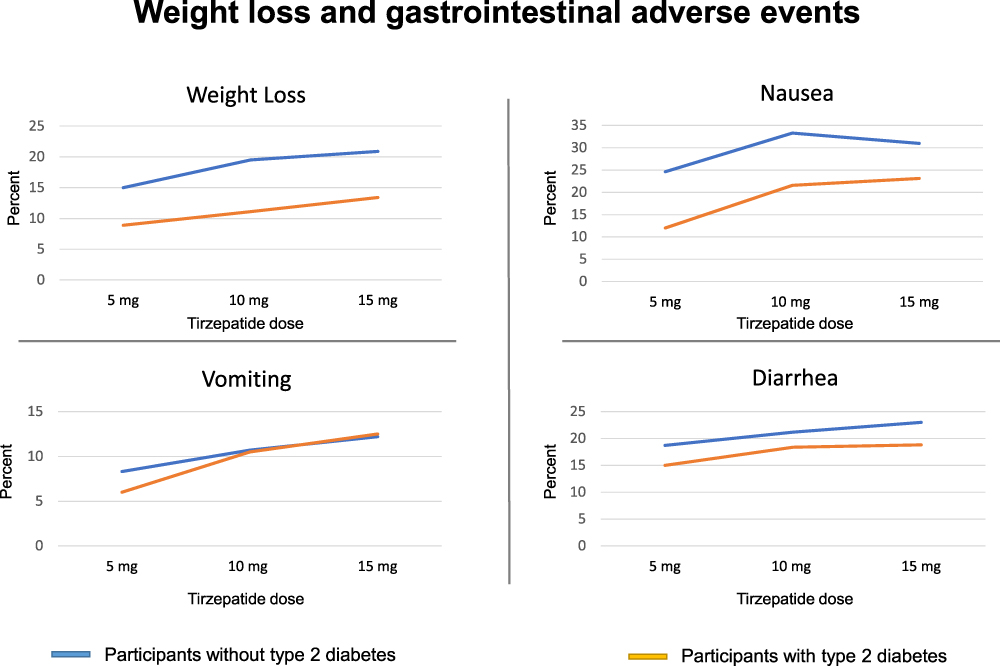 |
Figure 1 Comparisons of weight loss (% change in body weight from baseline) and frequency in percent of gastro-intestinal adverse events reported by participants with type 2 diabetes (Orange lines, pooled data from SURMOUNT-2 and SURPASS-3 trials) and without type 2 diabetes (blue lines, data from the SURMOUNT-1 trial) during 52–72 weeks treatment with tirzepatide 5 mg, 10 mg, or 15 mg s.c. once weekly. |
Serious adverse events (SAEs) for participants treated with tirzepatide were reported with a frequency of 5–7% in participants without T2D (SURMOUNT-1) and 6–9% in participants with T2D (SURMOUNT-2 trial).26,27 The frequency of SAEs in the semaglutide 1 mg once weekly group was 3% compared with 5–7% in the tirzepatide 5–15 mg once weekly groups in the SURPASS-2 trial.29
Antibodies against tirzepatide was analyzed from 7 Phase III trials investigating pharmacokinetics, efficacy, and safety of tirzepatide in participants. In total, 51% of participants developed antidrug antibodies (no difference between 5 mg, 10 mg, or 15 mg once weekly groups) with no observed differences in terms of pharmacokinetics or efficacy in reducing HbA1C for this group compared to participants with no antidrug antibodies. Participants with antidrug antibodies had a higher frequency of injection site reactions, but these were non-serious and transient. Overall, antidrug antibodies were deemed not to have a significant impact on safety.28,30,31,34,42
Discussion
In clinical trials tirzepatide has been demonstrated to elicit substantial weight reduction, with less weight loss in trial participants with T2D compared to participants without T2D. In the SURMOUNT-2 trial, participants with T2D achieved a mean weight loss of up to 14.7% from baseline (11.6% estimated treatment difference relative to placebo) after 72 weeks. On the other hand, in the SURMOUNT-1 trial with a similar dose-escalation and involving slightly younger and more overweight participants without T2D, a mean weight loss of up to 20.9% from baseline (17.8% difference from placebo in change in body weight) was reported after 72 weeks. The mechanisms behind this difference is unknown, but the same trend has been reported for the GLP-1 receptor agonists.43,44 The two SURMOUNT studies provide valuable comparisons since they share a similar duration and involve participant populations that are comparable, with the primary distinction being the presence or absence of T2D among participants. While full data from other SURMOUNT trials have not yet been published, a recent announcement from the manufacturer of tirzepatide (Eli Lilly and Company, Indianapolis, USA) revealed some results from the SURMOUNT-3 and −4 trials. Here, a mean weight reduction of 24.5% (placebo adjusted net weight loss) after 72 weeks of treatment with tirzepatide in obese adults with weight-related comorbidities, but without T2D, was reported for the SURMOUNT-3 trial.45 Furthermore, in the SURMOUNT-4 trial it was reported that overweight or obese participants without T2D, who remained on tirzepatide for a total of 88-weeks had a 26% reduction in bodyweight (not placebo adjusted).45 As such, the difference in efficacy of tirzepatide between individuals with T2D compared with individuals without T2D may prove to be even greater than previously reported. While higher BMI is a predictor for higher absolute weight reduction, it cannot by itself explain these large differences in percentage body weight change from baseline.46 To our knowledge, no clear explanation has been provided for the difference in weight-reducing effects of GLP-1(/GIP) receptor agonists in patients with or without T2D. However, the underlying mechanisms behind this are likely to share similarities to the reduced glucoregulatory effects of both GLP-1 and GIP observed in patients with T2D compared to age- and BMI-matched controls without T2D.47
The GLP-1 receptor mono-agonists constitute relevant efficacy comparisors in terms of weight reduction. While some SURPASS trials compared tirzepatide directly with other GLP-1 receptor mono-agonists (dulaglutide and semaglutide), these comparators were not administered in adequate doses for optimal weight-lowering effects. In the SURPASS-2 trial, semaglutide was administered at a dose of 1 mg once weekly, while doses of up to 2.4 mg once weekly are now approved for weight management therapy. In the SURPASS J-Mono trial, tirzepatide was compared to a weekly dose of 0.75 mg dulaglutide, although doses of up to 4.5 mg once weekly have been approved (and have demonstrated enhanced efficacy).13,29,33,48,49 Semaglutide in doses approved for weight management (2.4 mg semaglutide once weekly) resulted in a weight loss of 6.2% relative to placebo (treatment policy estimand) in individuals with T2D after 68 weeks in the STEP-2 trial.26,50 As such, an indirect comparison of the highest approved doses of semaglutide (2.4 mg once weekly for 68 weeks) with highest dose of tirzepatide (15 mg once weekly for 72 weeks) suggests superior weight reducing effects of tirzepatide in individuals with T2D (ie, 6.2% versus 11.6%). For individuals without T2D, semaglutide 2.4 mg once weekly resulted in a body weight reduction of 12.4% relative to placebo (treatment policy estimand) after 68 weeks (STEP-1 trial) – again lower than the 17.8% relative to placebo reported in the SURMOUNT-1 trial with tirzepatide with only 4 weeks longer treatment duration.6 Thus, the reported weight loss with tirzepatide is superior compared to the weight loss reported with other GLP-1 receptor agonists irrespective of the presence of the T2D diagnosis.
Is the suggested superiority of tirzepatide in terms of weight reduction a result of a better GLP-1 receptor agonism, or is it primarily the addition of the GIP receptor agonism that impacts body weight regulation – or is it perhaps a combination of the two? Tirzepatide activates both the GLP-1 and the GIP receptor, whereas the affinity and potency are different from that of the naturally occurring hormones. Several mechanisms involving GIP receptor agonism are proposed to play a role in weight regulation. One hypothesis describes that GIP receptor activity mitigates the internalization of the GLP-1 receptor thereby enhancing GLP-1 receptor signalling.16 Another hypothesis builds on evidence supporting that GIP receptor agonism in the central nervous system contributes to a reduced food intake and thereby a reduction in body weight. Interestingly, there are studies with contradictory findings regarding the impact of GIP receptor agonism and antagonism on the regulation of body weight.51 GIP and GLP-1 combined are responsible for approximately 60–75% of insulin secretion (the incretin effect). In healthy individuals GIP has been suggested to be the most important contributor of the two hormones, suggesting that GIP may provide important additional effects in terms of body weight reductions perhaps increasingly so in individuals without diabetes or with treatment-induced normalization of body weight and glycaemia.52 Yet another hypothesis builds on the suggested effects of GIP receptor activation to alleviate nausea induced by GLP-1.51 While high doses of semaglutide and tirzepatide have not been directly compared, the weight loss and incidence of gastrointestinal AEs for lower doses of semaglutide 1 mg and tirzepatide 5 mg were very similar when directly compared in the SURPASS-2 trial, implying that any potential impact of GIP on reducing nausea at lower doses is most likely marginal.29 Finally, it must be considered if it is simply a matter of the administered dose, something which an ongoing study evaluating the weight-loss potential of semaglutide 7.2 mg weekly will disclose.53
Safety and tolerance of tirzepatide are important, as are any potential differences in frequency or type of AEs seen in individuals with and without T2D. Comparing the SURMOUNT-1 and −2 trials (similar duration and demographics but participants with and without T2D), nausea was reported by 31% (non-T2D) vs 23% (T2D) of participants during treatment with the highest tirzepatide dose (15 mg). Following the same pattern, diarrhea was reported by 23% (non-T2D) vs 19% (T2D) of participants treated with tirzepatide 15 mg. In contrast, vomiting was reported by a similar proportion of participants in the two groups 12% (non-T2D) vs 13% (T2D) treated with tirzepatide 15 mg. Collectively, AEs in participants without T2D were reported in up to 82% of participants with 4–7% of participants discontinuing due to AEs. For participants with T2D, AEs were reported in up to 77% of with similar number (ie, 4–7%) discontinuing due to AEs. Important SAEs to consider in participants both with and without T2D are the relatively rare events of acute cholecystitis and acute pancreatitis, which did not differ between groups.
Tolerability of tirzepatide was generally improved with a longer dose-escalation period, but the frequency of participants experiencing any adverse effects remained high (77–82% in the SURMOUNT trials), and an even higher frequency of AEs among participants with T2D of up to 95% was reported in an Asian-Pacific population with a lower mean body weight in the SURPASS-AP-combo trial.35 Although the frequency of AEs is high, it is worth noting that AEs were predominantly gastrointestinal in nature and most pronounced during the dose-escalation phase. Additionally, the average duration typically spanned from 2 to 4 days.26,35 Based on the collective trial data most individuals treated with tirzepatide are bound to experience transient, gastrointestinal AEs independent of diabetes status.
Discussions on the beneficial effect of weight loss remains, and an important feature of tirzepatide (or any other weight management drug) is its capacity to lower the occurrence of other diseases, such as cardiovascular outcomes. GLP-1 receptor agonists lower the risk of heart failure hospitalization in patients without prior heart failure; however, no statistically significant reduction has been demonstrated in patients with a history of heart failure.54,55 A recently published study revealed that participants with obesity or overweight who experienced weight reduction (9.4% from baseline) after treatment with 2.4 mg semaglutide for an average of 34 months saw reductions in MACE with a hazard ratio 0.80 [95% CI: 0.72 ─ 0.90] compared to those who received placebo.56 Longer studies of tirzepatide are needed to investigate if similar results are achievable with tirzepatide (as of publication of this article, the longest duration of follow-up in a trial for treatment with tirzepatide has been 72 weeks). Some investigations have tried to examine cardiovascular outcomes, utilizing a post-hoc meta-analysis of SURPASS trials that showed non-significant decreases in HR for MACE. Future studies will investigate if there are significant, positive effects on MACE: SURPASS CVOT (cardiovascular risk assessment, NCT04255433) will finalize in 2024 and SURMOUNT-MMO (reduction in morbidity and mortality in adults with obesity, NCT05556512) will finalize in 2027. These trials will provide important results on the potential benefits of tirzepatide.
Conclusion
Treatment with the dual GIP and GLP-1 receptor agonist tirzepatide elicited substantial weight reduction in individuals both with and without T2D, showing a higher level of efficacy compared to what has been previously documented with GLP-1 receptor mono-agonists. A notable and unexplained discrepancy, akin to what has been observed with other weight-loss medications, continues to exist in the reported weight loss between individuals with T2D compared to the considerably greater weight loss seen in individuals without T2D. Although the occurrence of AEs is relatively common with tirzepatide, these AEs were typically gastrointestinal in nature and self-resolving within a few days. Importantly, the frequency and nature of these AEs did not differ greatly between individuals with or without T2D, apart from a minor difference with participants with T2D reporting lower frequencies of nausea and diarrhea. While future studies are required to validate the effectiveness and safety of tirzepatide in a variety of populations and explore the potential for enhancements in the well-being and survival of treated patients, the reviewed data constitutes a promising prospect for tirzepatide and the future development of weight-loss medications involving agonism at multiple receptors.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Obesity Federation. World Obesity Atlas 2023; 2023. Available from: https://data.worldobesity.org/publications/?cat=19.
2. Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines For Medical Care of Patients with Obesity. Endocr Pract. 2016;22:1–203. doi:10.4158/EP161365.GL
3. Torgerson JS, Hauptman J, Boldrin MN, Sjöström L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161. doi:10.2337/diacare.27.1.155
4. Kim W, Egan JM. The role of incretins in glucose homeostasis and diabetes treatment. Pharmacol Rev. 2008;60(4):470–512. doi:10.1124/pr.108.000604
5. Holst JJ, Gasbjerg LS, Rosenkilde MM. The Role of Incretins on Insulin Function and Glucose Homeostasis. Endocrinology. 2021;162(7):bqab065. doi:10.1210/endocr/bqab065
6. Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183
7. Pi-Sunyer X, Astrup A, Fujioka K, et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N Engl J Med. 2015;373(1):11–22. doi:10.1056/NEJMoa1411892
8. Pedrosa MR, Franco DR, Gieremek HW, et al. GLP-1 Agonist to Treat Obesity and Prevent Cardiovascular Disease: what Have We Achieved so Far? Curr Atheroscler Rep. 2022. doi:10.1007/s11883-022-01062-2
9. Edwards KL, Stapleton M, Weis J, Irons BK. An update in incretin-based therapy: a focus on glucagon-like peptide-1 receptor agonists. Diabetes Technol Ther. 2012;14(10):951–967. doi:10.1089/dia.2012.0098.edw
10. Tschöp MH, Finan B, Clemmensen C, et al. Unimolecular Polypharmacy for Treatment of Diabetes and Obesity. Cell Metab. 2016;24(1):51–62. doi:10.1016/j.cmet.2016.06.021
11. Frias JP, Nauck MA, Van J, et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised, placebo-controlled and active comparator-controlled Phase 2 trial. Lancet. 2018;392(10160):2180–2193. doi:10.1016/S0140-6736(18)32260-8
12. FDA. FDA Product Label - Mounjaro. Mounjaro. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2022/215866Orig1s000lbl.pdf.
13. Wegovy Public Assessment Report. EMA. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/wegovy.
14. Zepbound FDAPL; 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217806s000lbl.pdf.
15. Thomas MK, Nikooienejad A, Bray R, et al. Dual GIP and GLP-1 Receptor Agonist Tirzepatide Improves Beta-cell Function and Insulin Sensitivity in Type 2 Diabetes. J Clin Endocrinol Metab. 2021;106(2):388–396. doi:10.1210/clinem/dgaa863
16. Willard FS, Douros JD, Gabe MBN, et al. Tirzepatide is an imbalanced and biased dual GIP and GLP-1 receptor agonist. JCI Insight. 2020;5(17):e140532. doi:10.1172/jci.insight.140532
17. Coskun T, Sloop KW, Loghin C, et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: from discovery to clinical proof of concept. Mol Metabol. 2018;18:3–14. doi:10.1016/j.molmet.2018.09.009
18. Wang L. Designing a Dual GLP-1R/GIPR Agonist from Tirzepatide: comparing Residues Between Tirzepatide, GLP-1, and GIP. Drug Des Devel Ther. 2022;16:1547–1559. doi:10.2147/DDDT.S358989
19. FDA Clinical Pharmacology Review(s). Center for Drug Evaluation and Research. Application Number: 215866Orig1S000. Tirzepatide. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2022/215866Orig1s000ClinPharmR.pdf.
20. Urva S, Quinlan T, Landry J, Martin J, Loghin C. Effects of Renal Impairment on the Pharmacokinetics of the Dual GIP and GLP-1 Receptor Agonist Tirzepatide. Clin Pharmacokinet. 2021;60(8):1049–1059. doi:10.1007/s40262-021-01012-2
21. Urva S, Quinlan T, Landry J, Ma X, Martin JA, Benson CT. Effects of Hepatic Impairment on the Pharmacokinetics of the Dual GIP and GLP-1 Receptor Agonist Tirzepatide. Clin Pharmacokinet. 2022. doi:10.1007/s40262-022-01140-3
22. SURMOUNT-3 (NCT04657016) information from clinicaltrials.gov. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04657016.
23. SURMOUNT-4 (NCT04660643). Information from clinicaltrials.gov. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04660643.
24. SURMOUNT-MMO (NCT05556512). Information from clinicaltrials.gov. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT05556512.
25. SURMOUNT-OSA (NCT05412004). Information from clinicaltrials.gov. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT05412004.
26. Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2023:S014067362301200X. doi:10.1016/S0140-6736(23)01200-X
27. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022:NEJMoa2206038. doi:10.1056/NEJMoa2206038
28. Rosenstock J, Wysham C, Frías JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143–155. doi:10.1016/S0140-6736(21)01324-6
29. Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
30. Ludvik B, Giorgino F, Jódar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial. Lancet. 2021;398(10300):583–598. doi:10.1016/S0140-6736(21)01443-4
31. Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4): a randomised, open-label, parallel-group, multicentre, phase 3 trial. Lancet. 2021;398(10313):1811–1824. doi:10.1016/S0140-6736(21)02188-7
32. Dahl D, Onishi Y, Norwood P, et al. Effect of Subcutaneous Tirzepatide vs Placebo Added to Titrated Insulin Glargine on Glycemic Control in Patients With Type 2 Diabetes: the SURPASS-5 Randomized Clinical Trial. JAMA. 2022;327(6):534. doi:10.1001/jama.2022.0078
33. Inagaki N, Takeuchi M, Oura T, Imaoka T, Seino Y. Efficacy and safety of tirzepatide monotherapy compared with dulaglutide in Japanese patients with type 2 diabetes (SURPASS J-mono): a double-blind, multicentre, randomised, phase 3 trial. Lancet Diabetes Endocrinol. 2022;10(9):623–633. doi:10.1016/S2213-8587(22)00188-7
34. Kadowaki T, Chin R, Ozeki A, Imaoka T, Ogawa Y. Safety and efficacy of tirzepatide as an add-on to single oral antihyperglycaemic medication in patients with type 2 diabetes in Japan (SURPASS J-combo): a multicentre, randomised, open-label, parallel-group, phase 3 trial. Lancet Diabetes Endocrinol. 2022;10(9):634–644. doi:10.1016/S2213-8587(22)00187-5
35. Gao L, Lee BW, Chawla M, et al. Tirzepatide versus insulin glargine as second-line or third-line therapy in type 2 diabetes in the Asia-Pacific region: the SURPASS-AP-Combo trial. Nat Med. 2023;29(6):1500–1510. doi:10.1038/s41591-023-02344-1
36. Gastaldelli A, Cusi K, Fernández Landó L, Bray R, Brouwers B, Á R. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol. 2022;10(6):393–406. doi:10.1016/S2213-8587(22)00070-5
37. Yabe D, Kawamori D, Seino Y, Oura T, Takeuchi M. Change in pharmacodynamic variables following once-weekly tirzepatide treatment versus dulaglutide in Japanese patients with type 2 diabetes (SURPASS J-mono substudy). Diabetes Obes Metab. 2023;25(2):398–406. doi:10.1111/dom.14882
38. Linge J, Neelan IJ, Dahlqvist Leinhard O, et al. Tirzepatide achieves significant weight loss without adverse effects on muscle composition (SURPASS-3 MRI). In:
39. Sattar N, McGuire DK, Pavo I, et al. Tirzepatide cardiovascular event risk assessment: a pre-specified meta-analysis. Nat Med. 2022;28(3):591–598. doi:10.1038/s41591-022-01707-4
40. Furihata K, Mimura H, Urva S, Oura T, Ohwaki K, Imaoka T. A Phase 1 multiple‐ascending dose study of tirzepatide in Japanese participants with type 2 diabetes. Diabetes Obesity Metab. 2022;24(2):239–246. doi:10.1111/dom.14572
41. Frias JP, Nauck MA, Van J, et al. Efficacy and tolerability of tirzepatide, a dual glucose‐dependent insulinotropic peptide and glucagon‐like peptide‐1 receptor agonist in patients with type 2 diabetes: a 12‐week, randomized, double‐blind, placebo‐controlled study to evaluate different dose‐escalation regimens. Diabetes Obes Metab. 2020;22(6):938–946. doi:10.1111/dom.13979
42. Calderon B, Mullins GR, Hodsdon M, et al. 742-P: antidrug Antibodies Do Not Impact Pharmacokinetics, Efficacy, and Safety of Tirzepatide: analysis of Data from 7 Phase 3 Studies. Diabetes. 2022;71(Supplement_1):742–P. doi:10.2337/db22-742-P
43. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341–1352. doi:10.1016/S0140-6736(11)60205-5
44. Jensterle M, Rizzo M, Haluzík M, Janež A. Efficacy of GLP-1 RA Approved for Weight Management in Patients With or Without Diabetes: a Narrative Review. Adv Ther. 2022;39(6):2452–2467. doi:10.1007/s12325-022-02153-x
45. Lilly Investors. Tirzepatide demonstrated significant and superior weight loss compared to placebo in two pivotal studies. Published July 27th; 2023. Available from: https://investor.lilly.com/news-releases/news-release-details/tirzepatide-demonstrated-significant-and-superior-weight-loss.
46. Kwan A, Maldonado JM, Wang H, Rasouli N, Wilding J. 719-P: tirzepatide Induces Weight Loss in Patients with Type 2 Diabetes Regardless of Baseline BMI: a Post Hoc Analysis of SURPASS-1 through −5 Studies. Diabetes. 2022;71(Supplement_1):719–P. doi:10.2337/db22-719-P
47. Kjems LL, Holst JJ, Vølund A, Madsbad S. The influence of GLP-1 on glucose-stimulated insulin secretion: effects on beta-cell sensitivity in type 2 and nondiabetic subjects. Diabetes. 2003;52(2):380–386. doi:10.2337/diabetes.52.2.380
48. Frias JP, Bonora E, Nevarez Ruiz L, et al. Efficacy and Safety of Dulaglutide 3.0 mg and 4.5 mg Versus Dulaglutide 1.5 mg in Metformin-Treated Patients With Type 2 Diabetes in a Randomized Controlled Trial (AWARD-11). Diabetes Care. 2021;44(3):765–773. doi:10.2337/dc20-1473
49. Frías JP, Auerbach P, Bajaj HS, et al. Efficacy and safety of once-weekly semaglutide 2·0 mg versus 1·0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double-blind, randomised, phase 3B trial. Lancet Diabetes Endocrinol. 2021;9(9):563–574. doi:10.1016/S2213-8587(21)00174-1
50. Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971–984. doi:10.1016/S0140-6736(21)00213-0
51. Samms RJ, Coghlan MP, Sloop KW. How May GIP Enhance the Therapeutic Efficacy of GLP-1? Trends Endocrinol Metab. 2020;31(6):410–421. doi:10.1016/j.tem.2020.02.006
52. Gasbjerg LS, Bergmann NC, Stensen S, et al. Evaluation of the incretin effect in humans using GIP and GLP-1 receptor antagonists. Peptides. 2020;125:170183. doi:10.1016/j.peptides.2019.170183
53. A Research Study to See How Semaglutide Helps People With Excess Weight, Lose Weight (STEP UP), NCT05646706. Sponsor: novo Nordisk.Available from: https://clinicaltrials.gov/study/NCT05646706?tab=table.
54. Huixing L, Di F, Daoquan P. Effect of Glucagon-like Peptide-1 Receptor Agonists on Prognosis of Heart Failure and Cardiac Function: a Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin Ther. 2023;45(1):17–30. doi:10.1016/j.clinthera.2022.12.006
55. Fudim M, White J, Pagidipati NJ, et al. Effect of Once-Weekly Exenatide in Patients With Type 2 Diabetes Mellitus With and Without Heart Failure and Heart Failure-Related Outcomes: insights From the EXSCEL Trial. Circulation. 2019;140(20):1613–1622. doi:10.1161/CIRCULATIONAHA.119.041659
56. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221–2232. doi:10.1056/NEJMoa2307563
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.