")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 17
The Associations Between Abdominal Obesity and Coronary Artery Calcification in Chronic Kidney Disease Population
Received 4 November 2023
Accepted for publication 20 January 2024
Published 1 February 2024 Volume 2024:17 Pages 39—45
DOI https://doi.org/10.2147/IJNRD.S446445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Peng-Tzu Liu,1– 4 Jong-Dar Chen1,4
1Department of Family Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei City, Taiwan; 2Graduate Institute of Chemistry, Fu Jen Catholic University, New Taipei City, Taiwan; 3Graduate Institute of Biomedical and Pharmaceutical Science, Fu Jen Catholic University, New Taipei City, Taiwan; 4School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
Correspondence: Jong-Dar Chen, Center for Occupational and Environmental Medicine, Department of Family Medicine, Shin-Kong Wu Ho-Su Memorial Hospital, 95 Wen Chang Road, Shih Lin, Taipei City, 110, Taiwan, Tel +886-2-28332211, ext. 2626, Fax +886-2-28389468, Email [email protected]
Background: Cardiovascular disease (CVD) is the primary cause of mortality in chronic kidney disease (CKD) patients, with metabolic disorders exacerbating this risk. Compared with body mass index, waist circumference (WC) has been proposed as a more effective indicator of abnormal visceral fat. However, the associations among CKD, abnormal WC, and CVD remain understudied.
Material and Methods: A cross-sectional study in Taiwan (July 2006 to May 2016) involved 10,342 participants undergoing self-paid health checkups at a single medical center. Physical examinations and blood samples were taken to assess metabolic parameters, and renal function was evaluated using the Chronic Kidney Disease Epidemiology Collaboration formula. Coronary artery calcification (CAC) scores were determined through coronary 256-slice multidetector computed tomography angiography, with a CAC score of > 0 Agatston unit (AU) and ≥ 400 AU denoting positive CAC and severe CAC, respectively.
Results: Sex-based comparisons were conducted between individuals with CKD and those without CKD. In the CKD group, both sexes exhibited significantly elevated levels for systolic blood pressure, serum fasting blood glucose (FBG), and hemoglobin A1c (HbA1c) as well as reduced serum high-density lipoprotein cholesterol. Examination of the associations of abnormal WC revealed that for both sexes, individuals with abdominal obesity (AO) were significantly older and had higher systolic/diastolic blood pressure, serum FBG, HbA1c, and lipid profiles compared with those without AO. Multiple logistic regression analysis revealed that CKD patients exhibited a more pronounced association with severe CAC scores compared with AO patients (odds ratios [ORs]: 2.7 and 1.4, respectively). Furthermore, the combined effects of AO and CKD (AO[+]/CKD[+]) resulted in increased risks of positive CAC (OR: 2.4, 95% confidence interval [CI]: 1.6– 3.5) and severe CAC (OR: 4.4, 95% CI: 1.4– 14.2).
Conclusion: Abdominal obesity significantly raised the odds of CAC and was associated to a 4.4-fold increased risk of severe CAC in CKD patients.
Keywords: abdominal obesity, coronary artery calcification, coronary artery calcium score, chronic kidney disease
Introduction
Arteriosclerotic cardiovascular disease (CVD) is a prominent contributor to global mortality and morbidity according to the Global Burden of Disease Study 2019, a multinational collaborative research study conducted from 1990 to 2019.1 Multidetector computed tomography imaging offers exceptional sensitivity and specificity for assessing coronary artery calcification, and this imaging modality also provides a quantitative measurement of the plaque burden on the vessel endothelium as well as the composition of these plaques.2–4 Furthermore, three-dimensional reconstructed images enable the evaluation of vessel lumen stenosis. An elevated coronary artery calcification (CAC) score indicates the elevated presence of fibro-calcified lesions in the coronary arteries, leading to increased vessel wall stiffness.2,3 Accordingly, the CAC score is regarded as a robust predictive marker of the risk of coronary artery disease (CAD).5,6
Among patients with chronic kidney disease (CKD), CAD is the leading cause of both morbidity and mortality.7–9 Shared risk factors such as diabetes and hypertension contribute to the pathogenesis of both CKD and CAD.10–13 Related studies have demonstrated that CKD disrupts renin secretion and promotes the development of insulin resistance, dyslipidemia, and electrolyte imbalance.13–18 Consequently, CAD can manifest in the early stage of CKD,19,20 with the severity of CVD escalating as renal function deteriorates.
Obesity, a well-established risk factor for metabolic disorders, exhibits a significant association with CAD.21,22 Although many studies have employed body mass index (BMI) as an indicator of obesity, it should be noted that the healthy BMI range varies across ethnic populations. Additionally, numerous investigations have revealed that visceral fat exerts a more pronounced influence on CAD than does subcutaneous fat.23–25 Consequently, compared with BMI, waist circumference (WC) has emerged as a superior parameter for assessing abdominal obesity (AO) in relation to CAD risk.
Although both CKD and AO independently increase the incidence of CAD, the combined effects of CKD and AO on CAC remain uncertain. Accordingly, this study elucidated this association and highlighted the importance of WC as a clinical parameter for assessing patients with pre-dialysis CKD.
Materials and Methods
Participants
This study participants were individuals who voluntarily underwent self-paid health checkups at Shin Kong Wu Ho-Su Memorial Hospital in Taiwan between July 2006 and May 2016. During these physical examinations, trained physicians conducted interviews with the participants and collected data regarding their age, body weight, body height, BMI, WC, and blood pressure. The exclusion criteria were a history of renal transplant surgery, currently undergoing hemodialysis or peritoneal dialysis, prior percutaneous coronary intervention with stenting(s), and a history of coronary arterial bypass surgery. A total of 10,342 patients aged ≥18 years (6912 men and 3430 women; mean age 51 ± 10 standard deviation years) were enrolled into this cross-sectional study. The Institutional Review Board of Shin Kong Wu Ho-Su Memorial Hospital approved this study, and written informed consent was obtained from all the participants, each of whom consented to their data being stored as big data in the hospital’s database for retrospective medical research purposes. We conducted our study in compliance with the principles of the Declaration of Helsinki.
Definitions of CKD, Abnormal WC, and Severe CAC and Laboratory Measurements
Renal function was assessed by calculating the estimated glomerular filtration rate (eGFR) by using the Chronic Kidney Disease Epidemiology Collaboration equation.26 This equation was modified based on sex and serum creatinine levels. A patient was considered to have CKD if their eGFR was <60 mL/min/1.73 m2.
Waist circumference was measured according to the relevant World Health Organization guidelines and was defined as the horizontal panel at the midpoint between the lower border of the rib cage and the iliac crest, with measurements taken when the participant exhaled. Abnormal WC, meaning AO, was defined as ≥90 cm (≥35.5 inches) for men and nonpregnant women as per the International Diabetes Federation’s recommendations for South Asian, Chinese, and Japanese populations.27
Coronary artery calcification scores were assessed using coronary 256-slice multidetector computed tomography angiography following the standard protocol. Calcification was defined as an area of hyper-attenuation greater than 130 Hounsfield units within a 1-mm2 area. The scan covered the entire heart in the z-axis direction from the bifurcation of the pulmonary arteries to the apex of the heart during an expiratory pause. Coronary artery calcification scores were calculated using the Agatston method with built-in digital software, and these scores were confirmed by certified cardiac radiologists. The participants with CAC scores of >0 Agatston unit (AU) were considered to have CAC, and those with CAC scores of ≥400 AU were classified as having severe CAC.28
Blood samples were collected after an overnight fast of at least 8 hours. Serum levels of biochemical markers—namely fasting blood glucose (FBG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), hemoglobin A1c (HbA1c), and creatinine—were measured using an automated clinical analyzer (Hitachi 7600; Hitachi Ltd., Tokyo, Japan).
Statistical Analysis
Continuous variables were analyzed using Wilcoxon rank-sum test, and categorical variables were analyzed using the chi-squared test. Frequencies and percentages are used to present categorical variables. Based on their CAC scores, the participants were categorized into three groups (0, >0, and ≥400 AU), and their demographics, cardiovascular risk factors, and renal function–related parameters were assessed by sex. The associations among WC, CKD, and CAC scores were examined through multiple logistic regression. Statistical significance was set at P < 0.05. All statistical analyses were performed using the SAS statistical software package.
Results
The present patient population was divided into four groups based on the presence or absence of CKD in the two sexes (Table 1). Both elderly patients and those with abnormal WC exhibited an elevated prevalence of CKD in both sexes. Male CKD patients demonstrated significantly elevated systolic blood pressure, serum FBG, and HbA1c and reduced serum HDL-C. Female CKD patients had significantly elevated systolic and diastolic blood pressure, serum FBG, HbA1c, TG, LDL-C, and TC and reduced serum HDL-C.
 |
Table 1 Characteristics of Patients of Both Sexes with and without Chronic Kidney Disease |
Table 2 presents the characteristics of male and female participants with or without abnormal WC. Women with AO were significantly relatively old. In both sexes, the participants with AO and had elevated systolic and diastolic blood pressure, serum FBG, HbA1c, TG, LDL-C, and TC along with reduced serum HDL-C and eGFRs, all of which reached statistical significance.
 |
Table 2 Characteristics of Patients of Both Sexes with and without Abdominal Obesity |
Table 3 elucidates the associations of abdominal obesity or chronic kidney disease with CAC. Logistic regression models were adjusted for sex, age, and multiple metabolic parameters. The adjusted odds ratios (ORs) for positive CAC were significantly increased in patients with AO (OR: 1.4) and CKD (OR: 1.4). In addition, CKD patients (OR: 2.7) exhibited significantly higher odds ratio of severe CAC than AO patients (OR: 1.8).
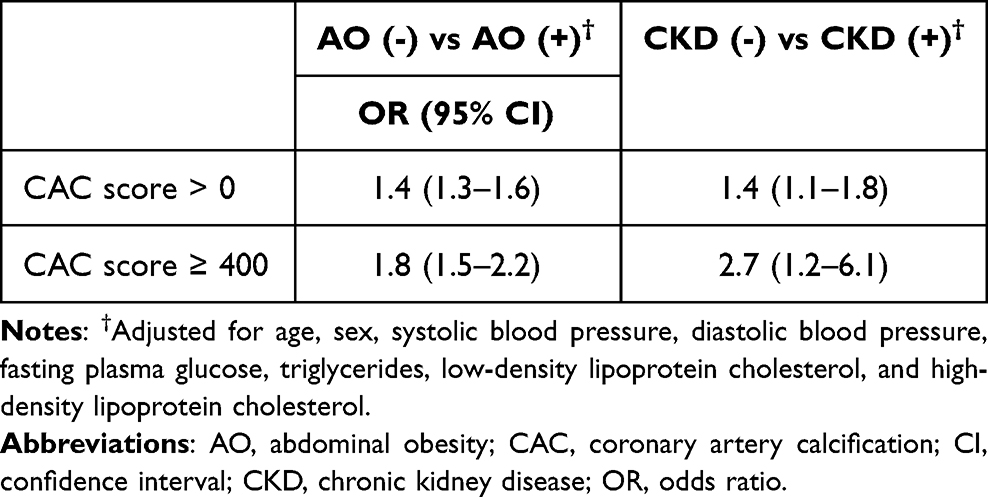 |
Table 3 Odds Ratios (95% Confidence Intervals) of Coronary Artery Calcification in Patients with Abdominal Obesity or Chronic Kidney Disease Compared with Normal Controls |
Table 4 elucidates the associations among AO, CKD, and CAC scores after adjustment for confounding factors. The participants were divided into four subgroups based on the presence or absence of AO or CKD as well as the presence or absence of both conditions. Non-CKD patients with healthy WC (AO[-]/CKD[-]) served as the control subgroup. Non-CKD patients with AO (AO[+]/CKD[-], OR: 1.4) exhibited a significantly increased OR for positive CAC compared with CKD patients with healthy WC (AO[-]/CKD[+], OR: 1.1). However, CKD patients with healthy WC (AO[-]/CKD[+], OR: 2.6) had an increased OR for severe CAC scores compared with non-CKD patients with AO (AO[+]/CKD[-], OR: 1.8). Finally, patients with both CKD and AO (AO[+]/CKD[+]) exhibited significantly elevated OR for severe CAC scores (OR: 4.4).
 |
Table 4 Odds Ratios (95% Confidence Intervals) of Positive Coronary Artery Calcification and Severe Coronary Artery Calcification in Subgroups Calculated Through Multiple Logistic Regression Analyses |
Discussion
In this large population-based study, we observed close associations of CKD and AO with increased risks of both positive CAC and severe CAC. Participants with CKD exhibited adjusted ORs of 1.1 and 2.6 for positive CAC and severe CAC, respectively and the participants with AO had adjusted ORs of 1.4 and 1.8 for positive CAC and severe CAC, respectively. The combined effects of CKD and AO resulted in increased ORs of 2.4 and 4.4 for positive CAC and severe CAC, respectively.
Chronic kidney disease is associated with metabolic dysfunction, including hypertension induced by the renin–angiotensin–aldosterone system, insulin resistance, and dyslipidemia. Furthermore, advanced CKD disrupts the calcium–parathyroid axis, potentially leading to hypercalcemia and hyperphosphatemia. Our findings revealed a significantly elevated prevalence of these metabolic disorders in CKD patients of both sexes compared with individuals without CKD. Moreover, in hyperphosphatemia, vascular smooth muscle cells tend to differentiate into a synthetic phenotype, promoting calcification within the medial wall.14,16,29–31 The binding of osteocalcin to hydroxyapatite further contributes to hydroxyapatite deposition and subsequent calcification.32,33
Previous studies have suggested a relationship between CKD and the CAC severity. For example, Bjergfelt et al reported that the increased maximal carotid plaque thickness was closely associated with CAC severity in 200 patients with CKD stage 3 from the Copenhagen Chronic Kidney Disease Cohort study.34 In the KoreaN Cohort Study for Outcomes in Patients With Chronic Kidney Disease, Yun et al revealed a significant association between high CAC scores and increased risk of adverse kidney outcomes and CKD progression.7 However, notably, the aforementioned two studies categorized CKD populations into three groups on the basis of baseline CAC scores (0, 1–100, and >100 AU) without specifically investigating the association between CKD and severe CAC. In the present study, the participants with CKD exhibited adjusted ORs of 1.1 and 2.6 for positive CAC and severe CAC, respectively.
The prevalence of AO is closely related to that of visceral obesity. In a large cross-sectional study of middle-aged individuals, Lind et al reported that individuals with obesity, even those without metabolic syndrome, had increased severity of coronary artery stenosis.22 Sung et al found an association among obesity, CKD, and CAC;35 however, that study used BMI rather than WC as a measure of obesity and did not specifically explore the associations of obesity and CKD with severe CAC. In our study, WC alone was found to be an effective indicator significantly associated with positive CAC and severe CAC.
A small number of studies have investigated the combined effects of AO and CKD on CAC. Cordeiro et al reported an association between increasing visceral adipose tissue quartiles and increased eGFR and CAC scores in patients with CKD stages 3–5.24 Additionally, in another study, each 1-cm increase in WC was associated with a significant increase in the OR for CAC.5 The present study, which used a large population dataset, revealed a 2.4-fold increased risk of positive CAC and a 4.4-fold increased risk of severe CAC in patients with both CKD and AO.
To the best of our knowledge, this study is the first exploration of the associations among CKD, AO, and CAC in a large population. However, this study has some limitations. First, as a cross-sectional study, it did not establish causal relationships among CKD, AO, and CAC. Second, since the lifestyle questionnaire did not collect precise information regarding alcohol consumption, smoking habits, exercise habits and medical histories, we did not consider these influencing factors in the final analysis. This may have led to an underestimation of their effects.
In conclusion, the present study provides evidence for the combined effects of CKD and AO on CAC. The participants with both CKD and AO exhibited 2.4- and 4.4-fold increased risks of positive CAC and severe CAC, respectively. Accordingly, in clinical practice, increased attention should be paid to reduce AO for individuals with CKD.
Abbreviations
AO, abdominal obesity; AU, Agatston unit; BMI, body mass index; CAC, coronary artery calcification; CAD, coronary artery disease; CI, confidence interval; CKD, chronic kidney disease; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio; TC, total cholesterol; TG, triglyceride; WC, waist circumference.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Shin Kong Wu Ho-Su Memorial Hospital, and written informed consent was obtained from the study patients, who agreed to their data being stored as big data in the hospital database for retrospective medical research purposes.
Consent for Publication
All authors have seen and approved the manuscript being submitted.
Acknowledgment
We thank all the staff members from the health center at Shin Kong Wu Ho-Su Memorial Hospital for their assistance.
Funding
This study was not supported by any funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 Study. J Am Coll Cardiol. 2020;76:2982–3021. doi:10.1016/j.jacc.2020.11.010
2. Criqui MH, Denenberg JO, Ix JH, et al. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA. 2014;311:271–278. doi:10.1001/jama.2013.282535
3. Criqui MH, Knox JB, Denenberg JO, et al. Coronary artery calcium volume and density: potential interactions and overall predictive value: the multi-ethnic study of atherosclerosis. JACC Cardiovasc Imaging. 2017;10:845–854. doi:10.1016/j.jcmg.2017.04.018
4. Al Rifai M, Blaha MJ, Nambi V, et al. Determinants of incident atherosclerotic cardiovascular disease events among those with absent coronary artery calcium: multi-ethnic study of atherosclerosis. Circulation. 2022;145:259–267. doi:10.1161/circulationaha.121.056705
5. Wang MC, Lin CC, Chiang HY, et al. Association between coronary artery calcium and all-cause mortality: a large single-center retrospective cohort study. PLoS One. 2022;17:e0276659. doi:10.1371/journal.pone.0276659
6. Wong ND, Budoff MJ, Ferdinand K, et al. Atherosclerotic cardiovascular disease risk assessment: an American Society for Preventive Cardiology clinical practice statement. Am J Prev Cardiol. 2022;10:100335. doi:10.1016/j.ajpc.2022.100335
7. Yun HR, Joo YS, Kim HW, et al. Coronary artery calcification score and the progression of chronic kidney disease. J Am Soc Nephrol. 2022;33:1590–1601. doi:10.1681/asn.2022010080
8. Xiang X, He J, Zhang W, He Q, Liu Y. Coronary artery calcification in patients with advanced chronic kidney disease. BMC Cardiovasc Disord. 2022;22:453. doi:10.1186/s12872-022-02879-0
9. Bundy JD, Chen J, Yang W, et al. Risk factors for progression of coronary artery calcification in patients with chronic kidney disease: the CRIC study. Atherosclerosis. 2018;271:53–60. doi:10.1016/j.atherosclerosis.2018.02.009
10. Choi IJ, Lim S, Choo EH, et al. Differential impact of chronic kidney disease on coronary calcification and atherosclerosis in asymptomatic individuals with or without diabetes: analysis from a coronary computed tomographic angiography registry. Cardiorenal Med. 2018;8:228–236. doi:10.1159/000489097
11. Hyun YY, Kim H, Oh KH, et al. Arterial stiffness as a risk factor for subclinical coronary artery calcification in predialysis chronic kidney disease: from the KNOW-CKD study. Kidney Blood Press Res. 2019;44:426–434. doi:10.1159/000499648
12. Hyun YY, Kim H, Oh KH, et al. eGFR and coronary artery calcification in chronic kidney disease. Eur J Clin Invest. 2019:e13101. doi:10.1111/eci.13101
13. Kadowaki T, Maegawa H, Watada H, et al. Interconnection between cardiovascular, renal and metabolic disorders: a narrative review with a focus on Japan. Diabetes Obes Metab. 2022;24:2283–2296. doi:10.1111/dom.14829
14. Roy N, Rosas SE. IL-6 is associated with progression of coronary artery calcification and mortality in incident dialysis patients. Am J Nephrol. 2021;52:745–752. doi:10.1159/000518652
15. Shroff GR, Sanchez OA, Miedema MD, et al. Coronary artery calcium progresses rapidly and discriminates incident cardiovascular events in chronic kidney disease regardless of diabetes: the multi-ethnic study of Atherosclerosis (Mesa). Atherosclerosis. 2020;310:75–82. doi:10.1016/j.atherosclerosis.2020.07.026
16. Spoto B, Pisano A, Zoccali C. Insulin resistance in chronic kidney disease: a systematic review. Am J Physiol Renal Physiol. 2016;311:F1087–f1108. doi:10.1152/ajprenal.00340.2016
17. Villa-Bellosta R. Vascular calcification: key roles of phosphate and pyrophosphate. Int J Mol Sci. 2021;22. doi:10.3390/ijms222413536
18. Wu L, Bai YH, Chen T, et al. The relation of calcium-phosphorus metabolism-related indexes with cardiac damages. Eur Rev Med Pharmacol Sci. 2016;20:3244–3248.
19. Roy SK, Cespedes A, Li D, Choi TY, Budoff MJ. Mild and moderate pre-dialysis chronic kidney disease is associated with increased coronary artery calcium. Vasc Health Risk Manag. 2011;7:719–724. doi:10.2147/vhrm.S24536
20. Price AM, Ferro CJ, Hayer MK, Steeds RP, Edwards NC, Townend JN. Premature coronary artery disease and early stage chronic kidney disease. Qjm. 2018;111:683–686. doi:10.1093/qjmed/hcx179
21. Jensen JC, Dardari ZA, Blaha MJ, et al. Association of body mass index with coronary artery calcium and subsequent cardiovascular mortality: the coronary artery calcium consortium. Circ Cardiovasc Imaging. 2020;13:e009495. doi:10.1161/circimaging.119.009495
22. Lind L, Markstad H, Ahlström H, et al. Obesity is associated with coronary artery stenosis independently of metabolic risk factors: the population-based SCAPIS study. Atherosclerosis. 2022;362:1–10. doi:10.1016/j.atherosclerosis.2022.10.007
23. Ryu K, Suliman ME, Qureshi AR, et al. Central obesity as assessed by conicity index and a-body shape index associates with cardiovascular risk factors and mortality in kidney failure patients. Front Nutr. 2023;10:1035343. doi:10.3389/fnut.2023.1035343
24. Cordeiro AC, Qureshi AR, Lindholm B, et al. Visceral fat and coronary artery calcification in patients with chronic kidney disease. Nephrol Dial Transplant. 2013;28(Suppl 4):152–159. doi:10.1093/ndt/gft250
25. Choi SY, Kim D, Oh BH, et al. General and abdominal obesity and abdominal visceral fat accumulation associated with coronary artery calcification in Korean men. Atherosclerosis. 2010;213:273–278. doi:10.1016/j.atherosclerosis.2010.07.052
26. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi:10.7326/0003-4819-150-9-200905050-00006
27. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9(th) edition. Diabet Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
28. Pletcher MJ, Tice JA, Pignone M, Browner WS. Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis. Arch Intern Med. 2004;164:1285–1292. doi:10.1001/archinte.164.12.1285
29. Moser B, Poetsch F, Estepa M, et al. Increased β-adrenergic stimulation augments vascular smooth muscle cell calcification via PKA/CREB signalling. Pflugers Arch. 2021;473:1899–1910. doi:10.1007/s00424-021-02621-3
30. Sarnak MJ, Amann K, Bangalore S, et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol. 2019;74:1823–1838. doi:10.1016/j.jacc.2019.08.1017
31. van Venrooij NA, Pereira RC, Tintut Y, et al. FGF23 protein expression in coronary arteries is associated with impaired kidney function. Nephrol Dial Transplant. 2014;29:1525–1532. doi:10.1093/ndt/gft523
32. Ruiz JL, Hutcheson JD, Aikawa E. Cardiovascular calcification: current controversies and novel concepts. Cardiovasc Pathol. 2015;24:207–212. doi:10.1016/j.carpath.2015.03.002
33. Lee JS, Morrisett JD, Tung CH. Detection of hydroxyapatite in calcified cardiovascular tissues. Atherosclerosis. 2012;224:340–347. doi:10.1016/j.atherosclerosis.2012.07.023
34. Bjergfelt SS, Sørensen IMH, Hjortkjær H, et al. Carotid plaque thickness is increased in chronic kidney disease and associated with carotid and coronary calcification. PLoS One. 2021;16:e0260417. doi:10.1371/journal.pone.0260417
35. Sung KC, Ryu S, Lee JY, et al. Fatty liver, insulin resistance, and obesity: relationships with increase in coronary artery calcium over time. Clin Cardiol. 2016;39:321–328. doi:10.1002/clc.22529
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.