")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
The Association Between Skeletal Facial Types and Third Molars Impaction in a Saudi Arabian Subpopulation: A CBCT Study
Authors Bin Rubaia'an MA , Neyaz A, Talic F , Alkhamis A, Alghabban A, Assari A
Received 25 May 2023
Accepted for publication 4 August 2023
Published 15 August 2023 Volume 2023:15 Pages 143—156
DOI https://doi.org/10.2147/CCIDE.S419325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Muslat A Bin Rubaia’an,1 Aymen Neyaz,1 Faisal Talic,1 Ali Alkhamis,1 Abdulmalek Alghabban,1 Ahmad Assari2
1College of Dentistry, Riyadh Elm University, Riyadh, Kingdom of Saudi Arabia; 2Oral and Maxillofacial Surgery and Diagnostic Sciences Department, Riyadh Elm University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Muslat A Bin Rubaia’an, Tel +966 557020222, Email [email protected]
Purpose: To assess the state of mandibular and maxillary third molars in relation to different facial types in a Saudi population using cone-beam computed tomography (CBCT) records.
Patients and Methods: A retrospective study was performed on CBCTs. Statistical analysis determined the relationship between impacted maxillary and mandibular third molars and different skeletal facial types. The degree of third molar impaction was evaluated.
Results: A total of 198 CBCTs from subjects were evaluated, with a mean age of 34.2 years. Archer II classification was found to be significantly associated with all skeletal profiles. The incidence of mesioangular impactions in lower third molar showed a notable increase in the brachyfacial group, which was statistically significant.
Conclusion: In conclusion, this study demonstrates that different facial types are associated with the angulation of third molar impactions.
Keywords: impacted, wisdom tooth, brachyfacial, dolichofacial, mesiofacial, retrospective
Introduction
Impaction, also known as the failure of teeth to erupt, can occur due to obstruction in the tooth erupting pathway or improper tooth positioning.1,2 Third molars typically erupt between the ages of 18 and 24.1 The frequency of their impaction varies significantly, ranging from 16.7% to 73.82%.3 Impaction is more commonly observed in women and tends to occur more frequently in the mandible than in the maxilla.4 Impacted third molars can lead to various pathological conditions, including cysts, neoplasms, and conditions such as pericoronitis, root resorption, and dental caries. Additionally, they have been associated with mandibular incisor crowding.5
Various classifications are employed to categorize impacted third molars. The Pell and Gregory classification system and Winter’s classification are among the most widely used methods for assessing mandibular third molar impactions.6 According to the Pell and Gregory classification system, third molars are categorized into three classes based on their contact with the ascending mandibular ramus and the available space distal to the second molar. Additionally, this classification considers three levels of third molar depth in the bone relative to the occlusal plane.4 On the other hand, Winter’s classification is based on the angle formed by the longitudinal axes of the second and third molars.4 In contrast, Archer’s classification focuses on the anatomical position of the maxillary third molar in relation to the adjacent second molar, considering the relative depth of the impacted maxillary third molar.7,8
Insufficient space between the distal surface of the second molar and the anterior border of the ramus, the degree of remodeling and width of the ramus, the rate of third molar development, the inclined position of the posterior dentition, the size of the dentition in relation to the jaws, and systemic factors are all etiological factors that contribute to molar impaction.1,2,4,9 Furthermore, facial growth in various spatial dimensions can influence the impaction of permanent teeth.
Third molar impaction is significantly associated with insufficient retromolar space.4,9 In a study conducted among the Saudi population, Hassan reported that a mean length of 21.28 for the retromolar space was linked to mandibular third molar impaction.9 Furthermore, the jaw size is correlated with the incidence of mandibular third molar impaction.4 Jaw size also influences the direction of mandibular growth rotation, ultimately determining the facial type. Smaller craniums and jaw sizes can result in the evolutionary loss of space, leading to crowding of the third molars within the jaws.10
Cephalometric analysis is the primary diagnostic approach for evaluating skeletal tissues. Various researchers have made significant contributions to the development of diverse cephalometric film analyses, which have been named after them.11 According to Rickett’s classification, facial types can be categorized as brachyfacial, dolichofacial, and mesiofacial.12 Brachyfacial individuals have a reduced facial vertical dimension and a wider face, while dolichofacial individuals have longer and narrower faces. The mesiofacial type is characterized by well-balanced facial proportions.13 When assessing the sagittal maxillary and mandibular relationship, the ANB angle is one of the most widely accepted and used cephalometric parameters.14 McNamara’s analysis is also widely recognized and offers certain advantages over other analyses, such as the linear evaluation of maxillary and mandibular lengths.15,16
Both lateral cephalometric and cone-beam computed tomography (CBCT) analyses are commonly used methods for craniofacial assessment in orthodontic and surgical patients.17 However, lateral cephalograms present challenges in terms of image interpretation and landmark detection due to the superimposition of anatomical structures. Given the substantial source-to-object distance, it is important to note that structures closer to the radiation source experience greater magnification than those closer to the detector. Variations in projection geometry and observational variability in landmark detection are known to introduce significant inaccuracies, which further complicate cephalometric research.18
Three-dimensional computed tomography (CBCT) is advantageous as it avoids the issue of anatomic superimposition and other challenges encountered in lateral cephalograms.17,19 CBCT has demonstrated high reliability rates for landmark identification, with an error rate of less than 1.5%.19 Moreover, specific software allows for generating 2D lateral cephalometric images from CBCT records, offering a convenient and reliable method for orthodontic analysis.18
The association between third molar impaction and specific dental and skeletal characteristics remains a topic of debate, with variability observed among different populations.9,20 While several studies on third molar impaction can be found in the literature,3,4,10,21 there is a limited number of studies utilizing CBCT imaging to investigate the relationship between the types of third molar impaction and facial types in the Saudi population. Therefore, this study aimed to assess the condition of third molars in relation to different facial types within a subpopulation of Saudi Arabia using CBCT records.
Methodology
Study Design and Sampling Criteria
This retrospective study utilized existing 198 CBCT records from September 2019 to September 2021 of patients who visited the Department of Radiology at Riyadh Elm University Hospital. The CBCT data was obtained using the Sirona Galileos system from Germany, operating at 85 kV, 5–7 mA, and 14s. The study focused on pretreatment CBCT records of 198 third molars with fully developed roots, which were either fully erupted or impacted. These patients had no history of maxillofacial trauma, previous orthodontic treatment, missing or extracted permanent teeth, dysplasia, dentofacial deformities, endocrine disorders in the maxillofacial region, or nonsyndromic conditions. Additionally, complete patient records were available, along with CBCT images that were free of artifacts and provided a clear view of the full dentition.
Assessment of Images
The analysis used GALILEOS Viewer software (Sirona, Bensheim, Germany), version 1.6. Axial, coronal, and sagittal sections and panorex view were utilized for detailed analysis. The CBCT-derived lateral cephalograms were exported to the Webceph platform (Assemble Circle, Gyeonggi-do, Korea) for digitalized tracing. The SN-GoGn angle was measured, representing the angle between the Sella-Nasion line and the Gonion-Gnathion line. This angle assessed skeletal facial types based on the Rickett classification: Brachyfacial (<27°), mesiofacial (27–37°), and dolichofacial (>37°). The mandibular effective length was measured as the distance from Condylion (Co) to Gnathion (Gn), while the maxillary effective length was measured as the distance from Condylion (Co) to point A. These measurements are shown in (Figure 1).
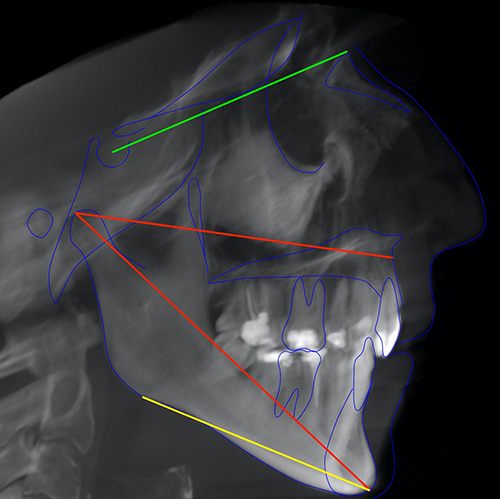 |
Figure 1 A CBCT-derived lateral cephalogram showing SN-GoGn angle (red), and effective length of maxilla (green), and effective length of mandible (yellow). |
The sagittal facial profile was categorized into three skeletal classes: Class 1 (4° ≥ ANB ≥ 0°), Class 2 (ANB > 4°), and Class 3 (ANB < 0°), following Steiner’s ANB angle analysis (Figure 2). The points used to determine the angle are as follows: A - the innermost curvature from the anterior nasal spine to the prosthion, N - the nasion, which is the junction of the frontal and nasal bones, B - the innermost curvature from the chin to the alveolar junction.
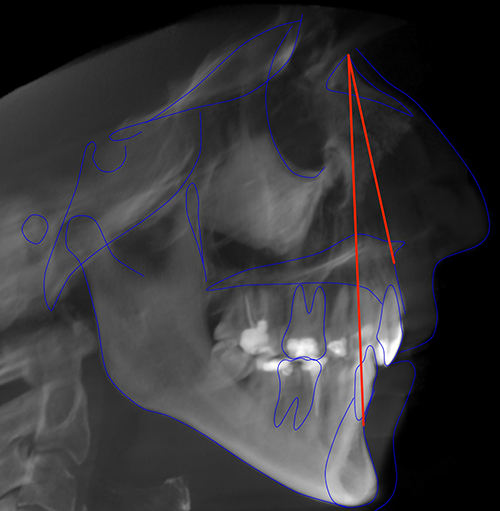 |
Figure 2 A CBCT-derived lateral cephalogram showing ANB angle. |
Similarly, the mandibular third molar impaction was classified according to Pell & Gregory’s classification system based on the position of the distal surface of the third molar crown concerning the anterior border of the ascending ramus. Class I referred to the crown as anterior to the anterior border. Class II indicated that the anterior border covered half of the crown, and Class III denoted the anterior border fully covering the crown. Additionally, their classification considered the relationship between the third molar’s cementoenamel junction (CEJ) and the bone level. Level A indicated that the tooth was not completely covered by bone, level B indicated partial coverage if any portion of the CEJ was below the level of the surrounding bone, and level C represented complete coverage by bone. Both classifications are shown in (Figure 3).
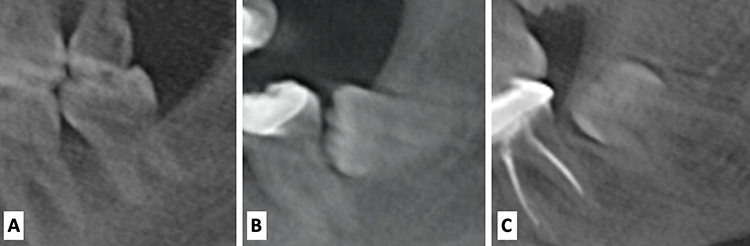 |
Figure 3 Pell & Gregory’s classification of ramus relation and impaction depth of lower third molars, (A) Class 1, Level A, (B) Class 2 Level B, (C) Class 3 Level C. |
Winter’s classification was utilized to determine the angle between the longitudinal axis of the second and third molars. The impaction angles were categorized as follows: vertical (10°–10°), mesioangular (11°–79°), horizontal (80°–100°), and distoangular (−11°–-79°) (Figure 4).
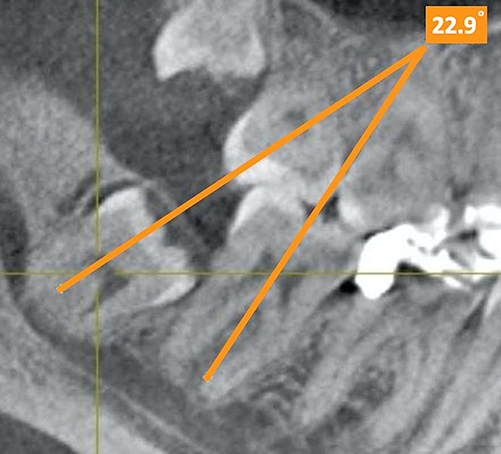 |
Figure 4 Winter’s classification, showing a mesioangular impaction. |
To assess the horizontal position of the lower third molar, the study evaluated the median of the third molar’s crown contour in relation to the molar line.22 The molar line extended horizontally from the median of the lower first premolar to the median of the second molar. The position of the third molar crown was classified into three categories: median position (distance between the crown’s median and the molar line <0.5 mm), buccal position (median of the crown located buccal to the molar line with a distance >0.5 mm), and lingual position (median of the crown located lingual to the molar line with a distance >0.5 mm) (Figure 5).
 |
Figure 5 Lower third molar horizontal position, showing a lingually positioned third molar. |
Additionally, the Archer classification was employed to categorize maxillary third molar impactions based on the position of the maxillary third molar’s long axis relative to the long axis of the maxillary second molar. Type A indicated that the maxillary third molar was located at or below the occlusal plane, Type B represented the positioning between the occlusal plane and the cervical line, Type C denoted the location between the cervical line of the second molar and the middle third of its root, Type D indicated the maxillary third molar being at or above the apical third of the second molar root, and Type E indicated the maxillary third molar being positioned above the apical third of the second molar root (Figure 6). The angulation of the maxillary third molar in relation to the long axis of the second molar was also classified as mesioangular, distoangular, vertical, buccoangular, or horizontal (Figure 7).
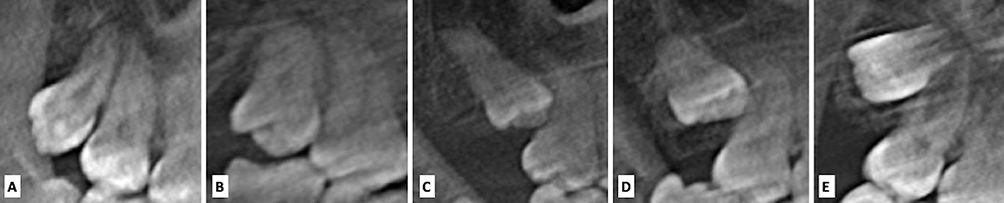 |
Figure 6 Archer l classification of upper third molars, (A) Type A, (B) Type B, (C) Type C, (D) Type D, (E) Type E. |
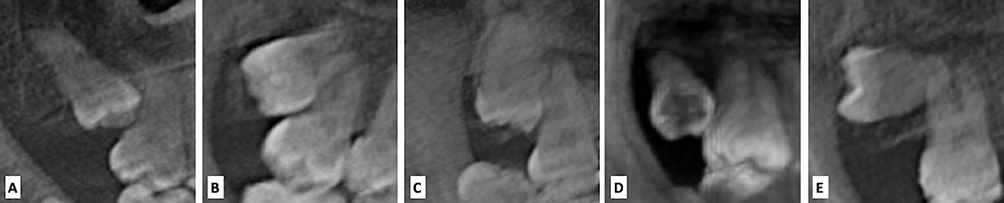 |
Figure 7 Archer ll classification of upper third molars, (A) mesioangular, (B) distoangular, (C) vertical, (D) buccoangular, (E) horizontal. |
The impacted status of the third molar was determined based on the presence of fully developed roots and the absence of functional occlusion. Two independent examiners conducted all measurements, and their findings were consistently reviewed by a third expert surgeon. The results were carefully documented using a data collection sheet.
Ethical Approval
The study was conducted in accordance with the 2013 Declaration of Helsinki, and all participants provided written informed consent for the anonymous use of their data for research purposes. The study was approved by the institutional review board and the local ethical committee of Riyadh Elm University, Riyadh, Saudi Arabia, under the institutional review board (IRB) number: (FUGRP/2020/193/277/264).
Statistical Analysis
Data analysis was conducted using IBM SPSS software version 19.0 (IBM, Armonk, NY, USA). Descriptive statistics, including means and frequencies, were calculated for all variables. The Chi-square test was utilized to examine the association between categorical variables. To compare continuous data among more than two groups, a one-way analysis of variance (ANOVA) test was employed. A p-value of ≤ 0.05 was considered statistically significant for all tests. Inter-examiner reliability assessment was performed on ten cases to evaluate the level of agreement among the investigators.
Results
The result of the Cohen’s kappa test, which assessed the degree of agreement among investigators, was 0.777, indicating substantial agreement for conducting the study. A total of 198 CBCT records were evaluated (Table 1). Among the participants, 54.5% were female.
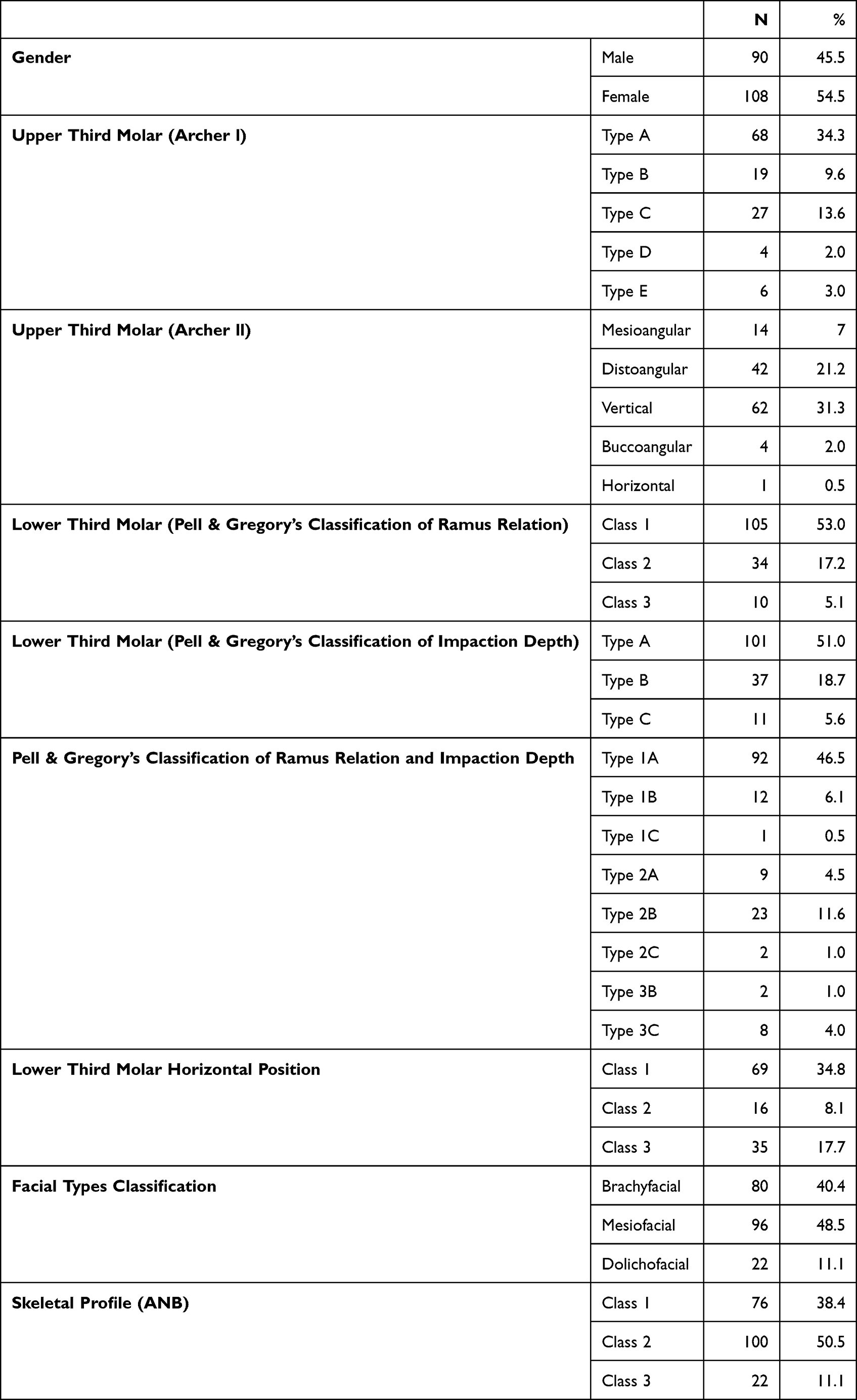 |
Table 1 Descriptive Characteristics of Study Participants |
No statistically significant differences were found between the right or left side third mandibular molars (p = 0.09) or maxillary third molars (p = 0.88). The most common type of impaction in the upper third molar was Type A, according to Archer I classification, and vertical type, according to Archer II classification. In the lower third molar impactions, 46.5% were classified as Class 1 and Type A based on Pell & Gregory’s classification system.
Regarding facial types, 48.5% of the participants were classified as mesiofacial and 40.4% were classified as brachyfacial. We also examined the association between facial type classification and all study variables, but no statistically significant associations were found (p>0.05) (Table 2).
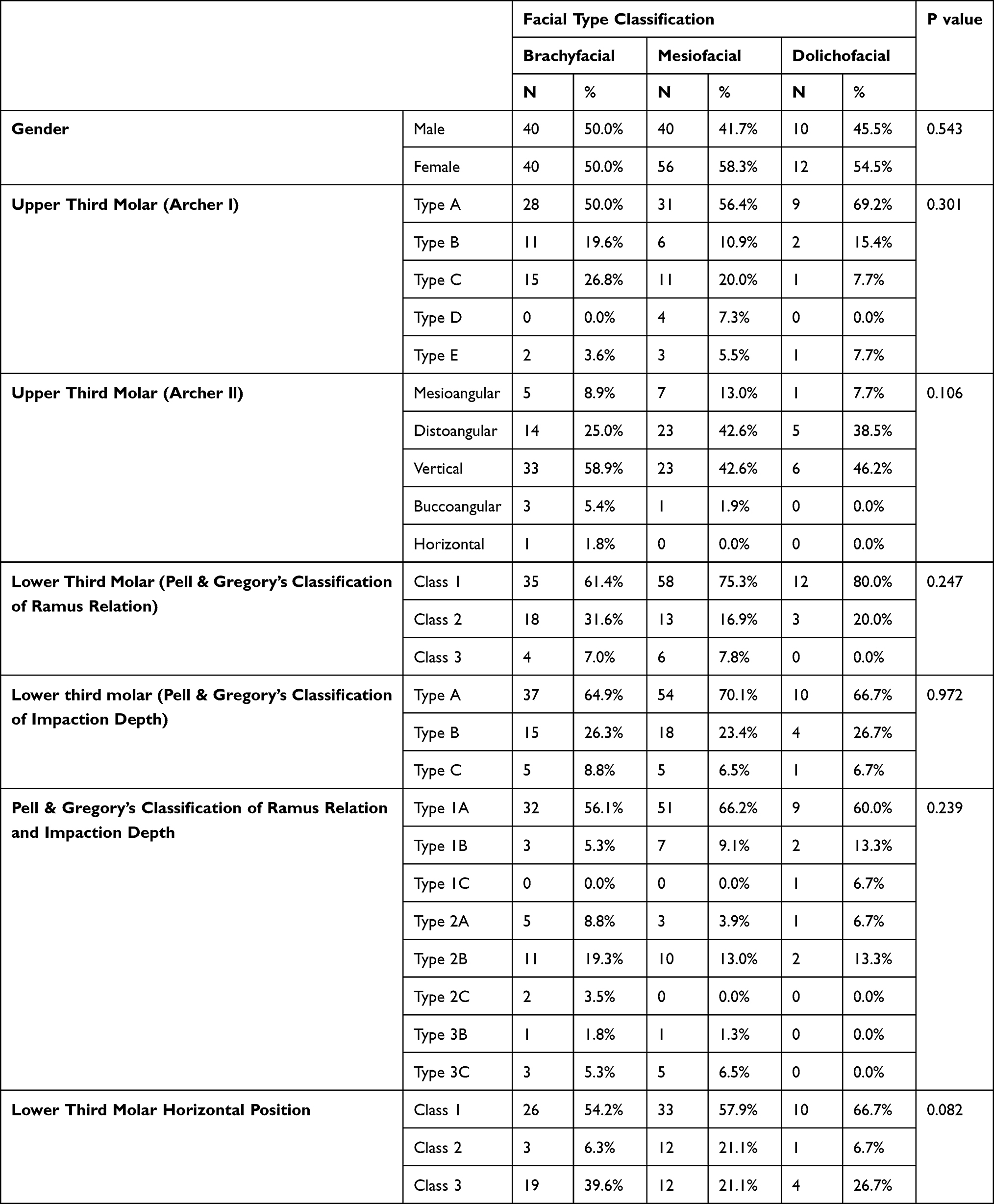 |
Table 2 Association Between Facial Types and Study Variables (Categorical) |
Furthermore, the association between facial types and study variables, specifically continuous data, was evaluated. A statistically significant association was observed between age and facial type. The highest mean age was found in the brachyfacial group (36.8 years), followed by the dolichofacial group (35.8 years) (Table 3).
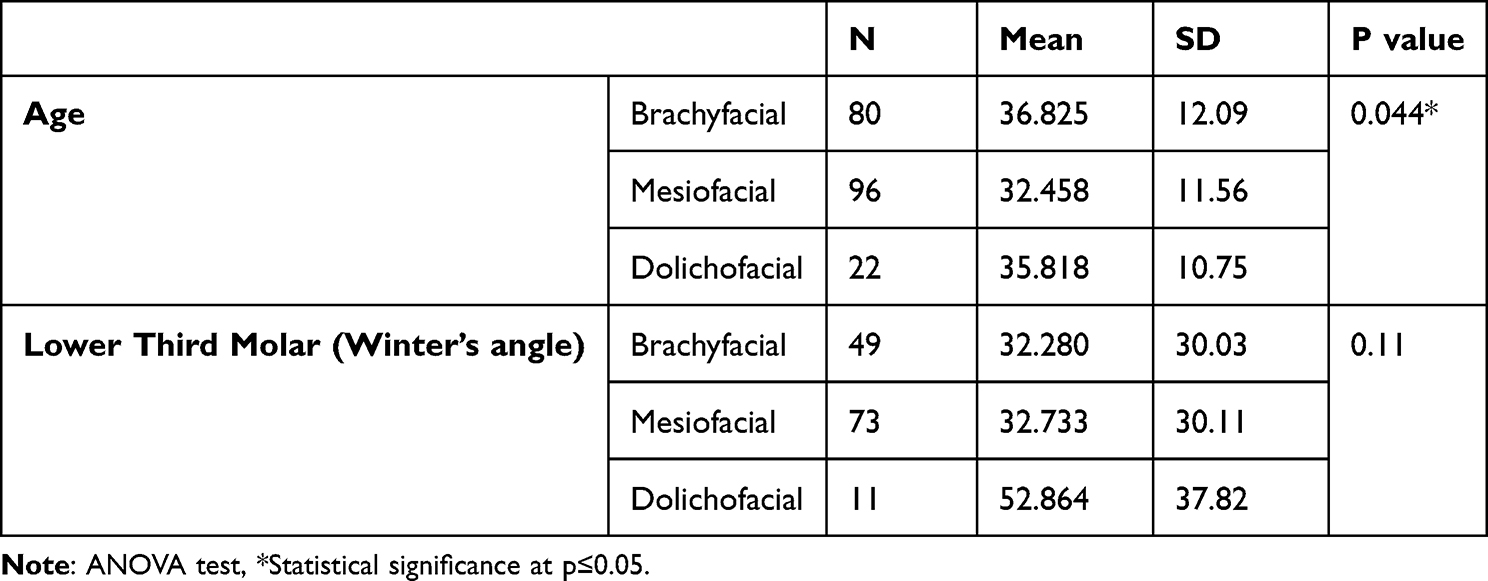 |
Table 3 Association Between Facial Type and Study Variables (Continuous) |
The association between skeletal profile ANB and the remaining variables was examined (Table 4). Among them, only the upper third molar classes (Archer II) showed a statistically significant association with skeletal profile (p = 0.013). The vertical type of lower third molar impaction was most commonly observed in Class I and Class II skeletal profiles. However, the frequencies of vertical and disto-angular impacted lower third molars were nearly equal in the Class II skeletal profile.
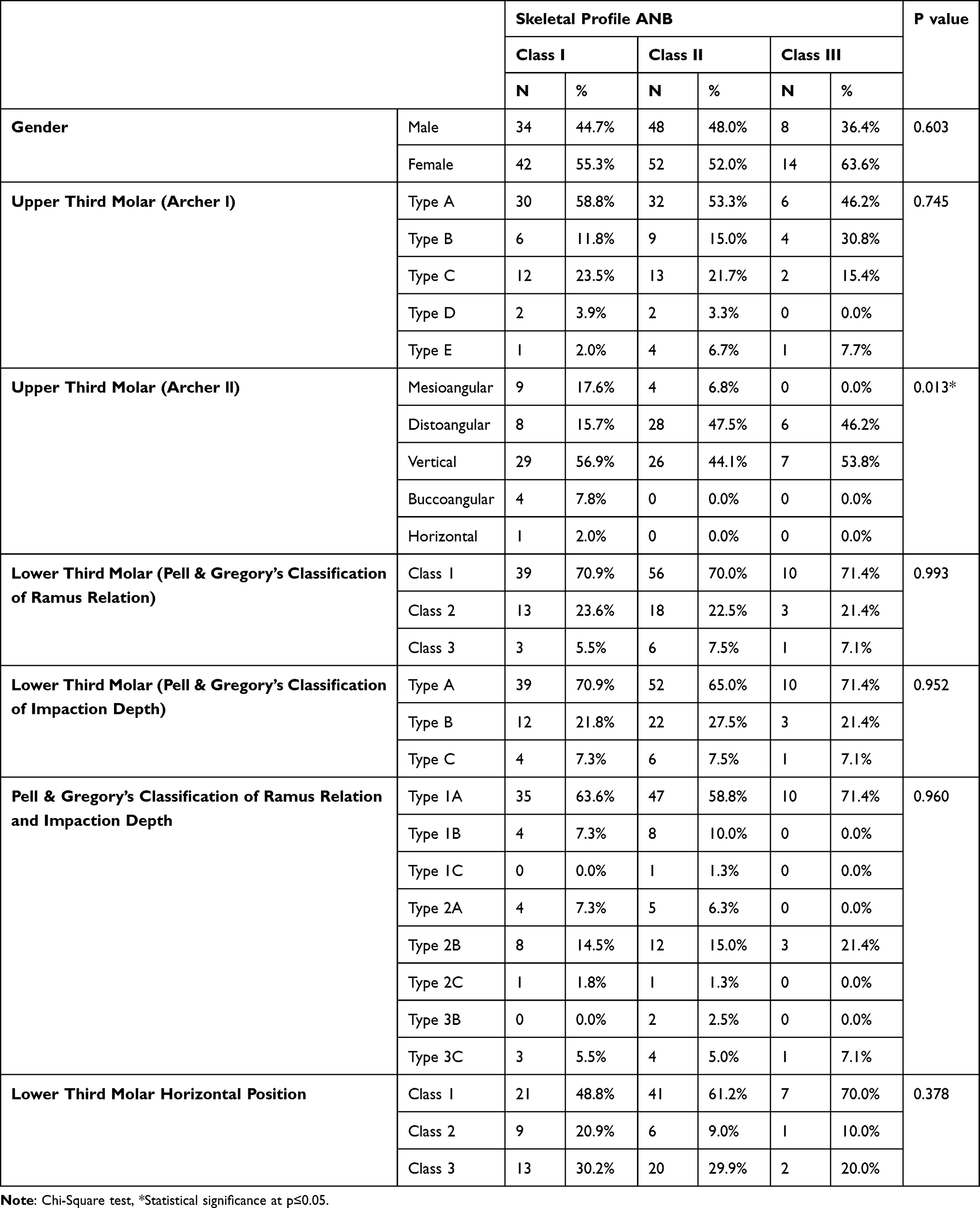 |
Table 4 Association Between Skeletal Profile and Study Variables (Categorical) |
Regarding the association between skeletal profile and study variables (continuous data), no statistically significant associations were found between skeletal shape and the study variables (p = 0.53, p = 0.24, p = 0.19) (Table 5).
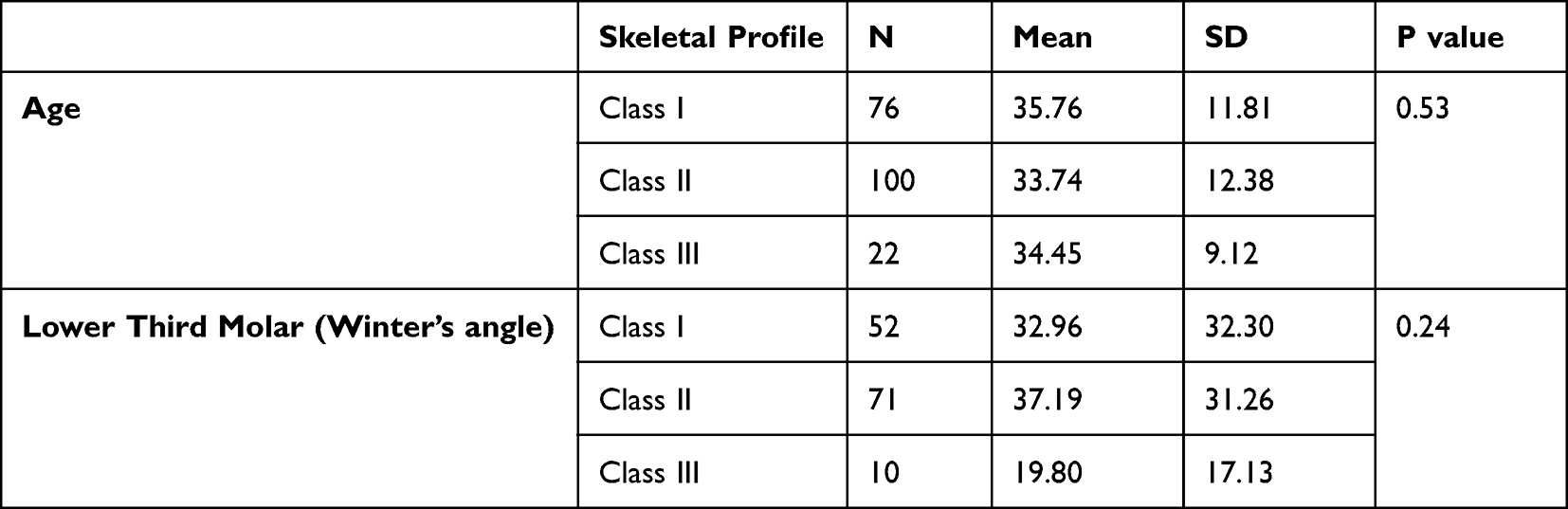 |
Table 5 Association Between Skeletal Profile and Study Variables (Continuous) |
Furthermore, the upper third molar variables did not exhibit any statistically significant association with the effective length of the maxilla (p = 0.269 and p = 0.275) (Table 6). Similarly, the lower third molar variables did not demonstrate any statistically significant association with the effective length of the mandible (p = 0.902 and p = 0.655) (Table 7).
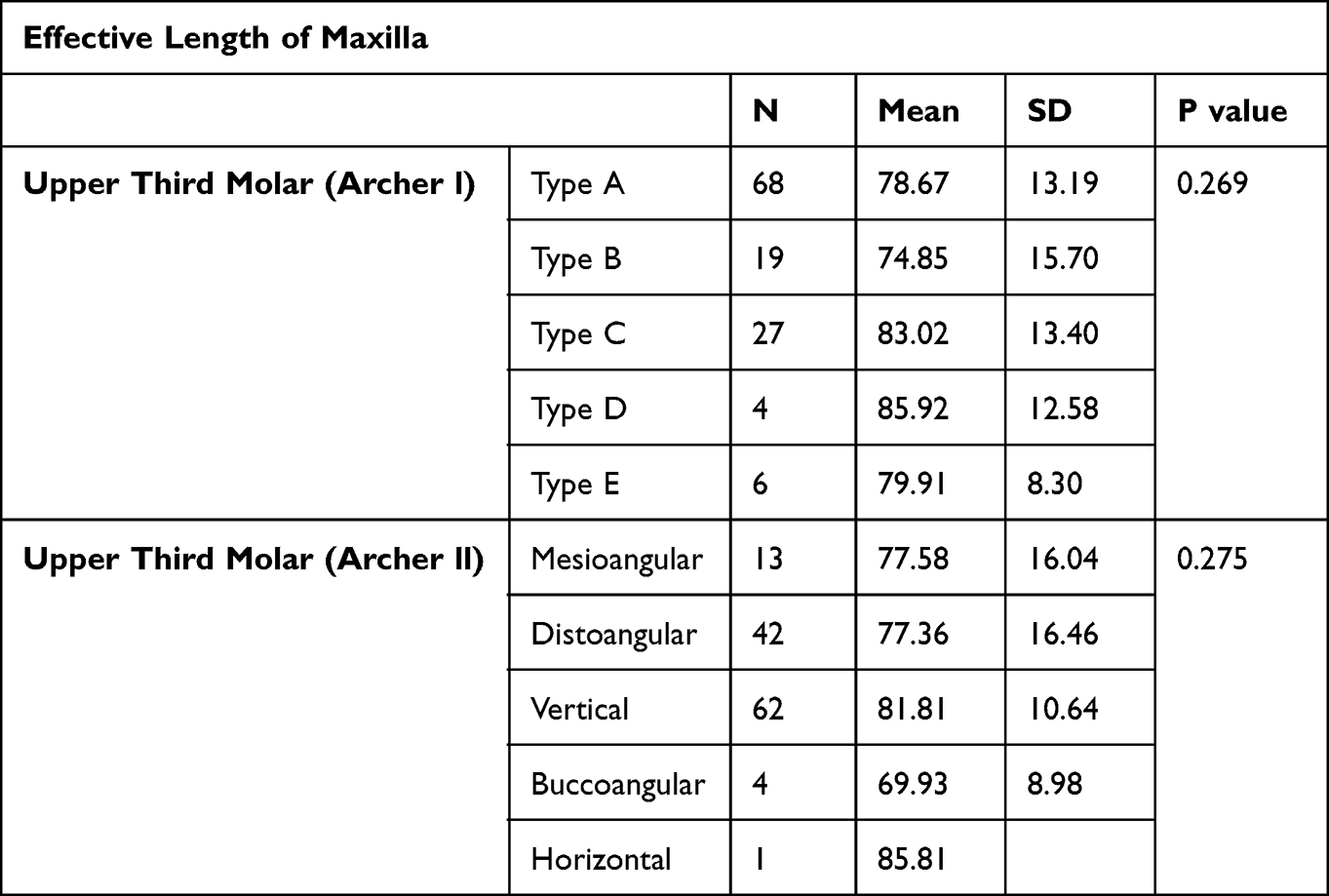 |
Table 6 Association Between Effective Length of Maxilla with Upper Third Molar Variables |
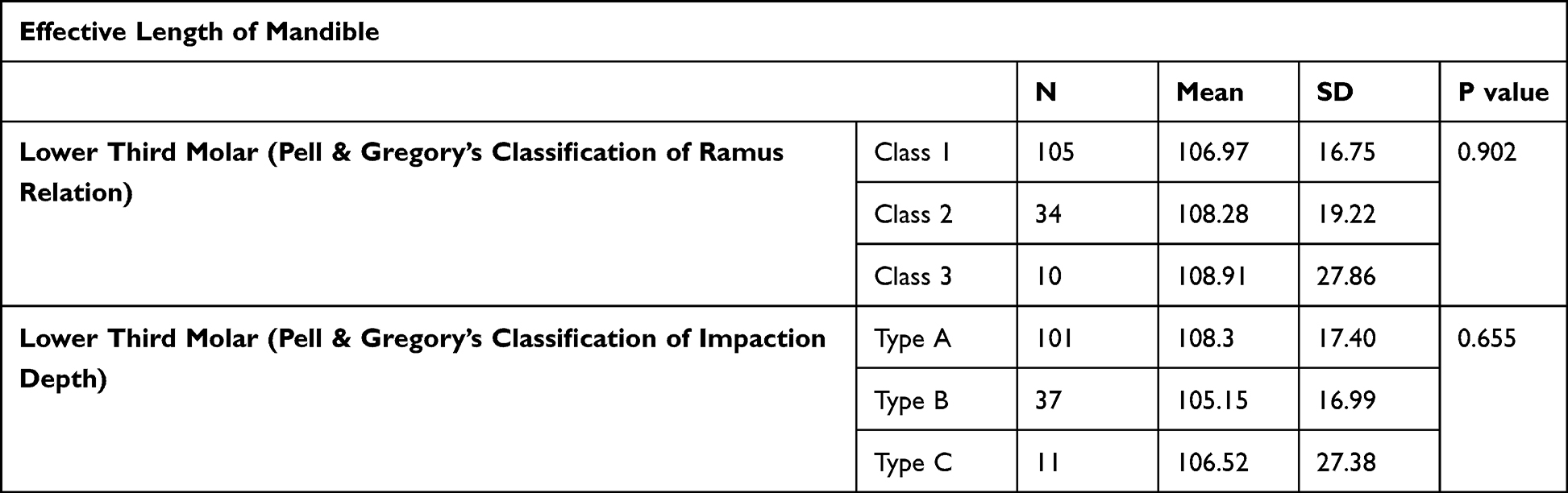 |
Table 7 Association Between Effective Length of Mandible with Lower Third Molar Variables |
The Pearson correlation test was employed to analyze the relationship between the continuous variables (Table 8).
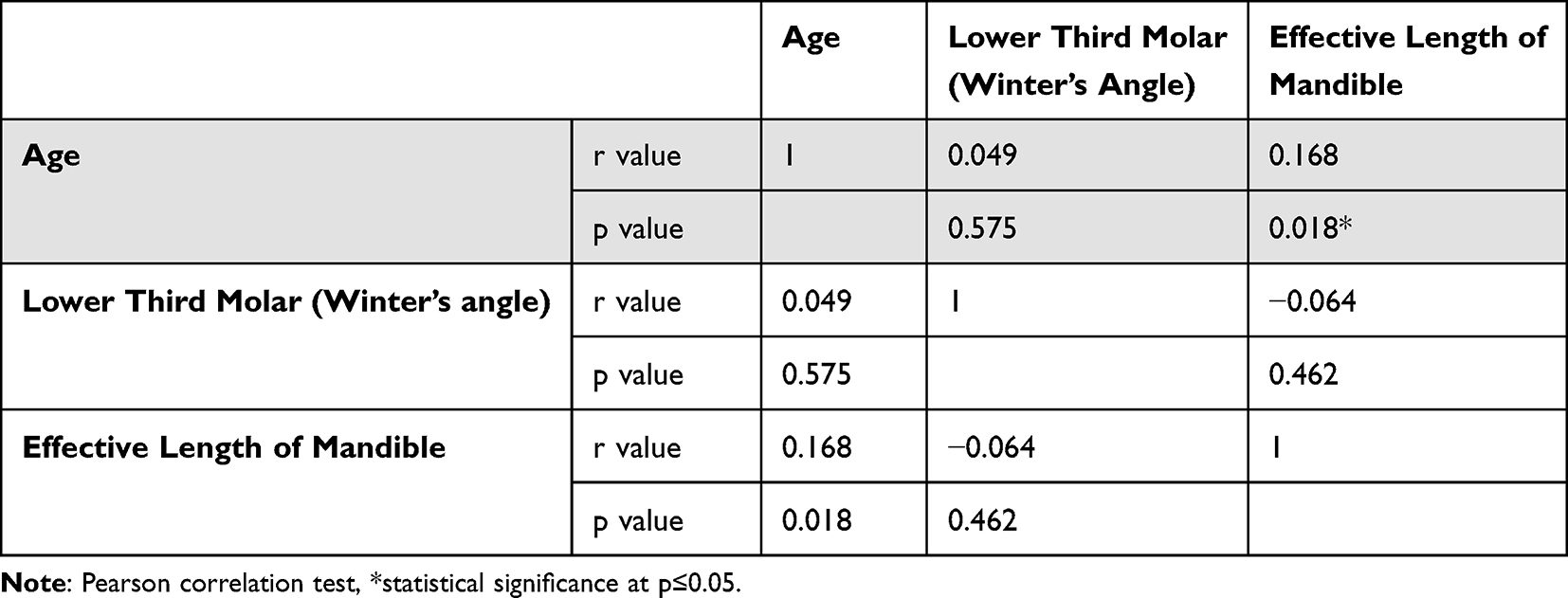 |
Table 8 Correlation Between the Continuous Variables |
Discussion
“Wisdom teeth” or third molars, are the teeth most frequently affected by impaction and should only be extracted if specific criteria are met.1–4,9,23 Prophylactic extraction of impacted third molars has improved patients’ quality of life.24 Furthermore, there is a significant association between increased age and immediate and chronic complications following extraction.25 To avoid this persistent morbidity, prophylactic extraction is suggested to be performed before reaching the age of 25.25 Among other factors, skeletal facial types are associated with impaction,9 making them a useful tool for predicting impaction.
The main objective of this study was to assess the state of third molars in relation to different facial types in a cohort of the Saudi subpopulation using CBCT records. To our knowledge, no population-based studies in Saudi Arabia have evaluated the association between third molar impaction and facial types using CBCT. Since the introduction of CBCT, conventional radiographic errors such as magnification, image distortion, and superimposition have been overcome.19 CBCT allows for 3D analysis and enables the generation of 2D lateral cephalogram images without magnification, which has been found to be more reliable.18
From the literature, it is evident that the inability of the mandibular third molar to erupt is primarily due to insufficient space within the alveolar arch located between the distal aspect of the second molar and the ascending mandibular ramus.1,4 Mandibular growth and development are correlated with the availability of sufficient space for the correct placement of the mandibular third molar.4 Several skeletal factors have been shown to reduce the space required for the third molar, including limited mandibular length (measured from the gonion to the condylar head), vertical orientation of condylar development, and backward-oriented eruption of the dentition.20
The impaction of the third molar can be alleviated by extracting the second molar and premolar as part of orthodontic intervention.20 Various factors contribute to this phenomenon, including the magnitude, quantity, and orientation of mandibular growth, the remodeling and length of the ramus, the pace of third molar maturation, the inclination of posterior dentition, and the proportion of dentition in relation to the jaws.1,4,9 Impaction has also been associated with genetic factors and eating habits.4 Furthermore, Hassan suggests that the disparities in results among previous studies could be attributed to variations in samples and methods.9
Third molar impaction is a common problem that affects a significant portion of the global population. In the present investigation, the incidence of mandibular third molar impaction was found to be 64.5%, while the incidence of maxillary third molar impaction was 65.4%. These incidences reported in the present study exceed the previously reported incidences by Alfadil et al (58.5% and 41.5%) and Hassan (53.1% and 31.8%).21,26 These differences could be attributed to variations in sample size. Additionally, no correlation was found between impaction rate and gender, which is consistent with previous studies.21,26 However, other studies have discovered that females are more likely than males to have a third molar impaction.4,8 The higher frequency reported in females is due to the difference in growth rates between males and females.4 Males’ jaws continue to grow during the eruption of the third molars, while females’ jaws stop growing when the third molars are just beginning to erupt, creating more space for the third molars to erupt. The mean age of the studied sample was 34.2 years, which is consistent with previous studies conducted on the Saudi population by Idris et al (30.8 years) and Alfadil et al (30.67 years).4,21 However, it slightly differs from other studies conducted on different populations by Ahmad et al (28.87 years) and Khouri et al (26.25 years).8,27 The considerable variation in age can be attributed to differences in ethnicity and racial backgrounds.4,27
The present investigation aimed to determine the potential correlation between skeletal facial development patterns and third molar impaction. In terms of facial type, vertical type (Archer II) impactions were found to be common in brachycephalic faces, while Type A (Archer I) impactions were prevalent in dolichocephalic faces. Only the upper third molar Classes (Archer II) showed a statistically significant association with the skeletal profile (p = 0.0013). Our study also revealed that impaction of the upper third molar was mostly classified as Type A (34.3%) and Vertical type (31.3%) according to the Archer I and Archer II classifications, respectively.
Regarding mandibular impaction, the assessment based on the Pell and Gregory classification revealed that Level A impaction was the most common, which is consistent with previous studies.8,28 However, this conflicts with other studies that have reported Level B as the predominant level among the Saudi population,26 or Level C.21 These differences could be attributed to variations in sample selection criteria. Furthermore, the determination of the horizontal position of the lower third molar was found to be not correlated with facial types (p = 0.082), or ANB angle (p = 0.378). To our knowledge, this study is the first to examine these correlations.
Additionally, over 77% of mandibular third molar impactions were of the mesioangular type, which is consistent with the findings of other studies where mesioangular impaction was predominant.4,21 The Chi-square test revealed a notable increase in the incidence of mesioangular impactions in the brachyfacial group, which was statistically significant (p = 0.003). According to our findings, the prevalence of mandibular third molar impaction was higher in individuals with a dolichofacial type than those with a brachyfacial type; however, the results were not statistically significant. This can be attributed to the vertical orientation of the condyle, a characteristic commonly observed in individuals with a dolichofacial type. The results of the present study are consistent with those of Hasan et al, who observed a reduced occurrence of third molar impaction in individuals with a brachyfacial growth pattern compared to those with a dolichofacial type.1 This phenomenon can be explained by the brachyfacial growth pattern, which exhibits a higher growth potential and facilitates greater remodeling resorption of the anterior border of the ramus. Hasan et al also found that short mandibles are more susceptible to third molar impaction.1 The presence of a lengthy, upwardly inclined ramus and a comparatively shorter mandibular length are indicative of mandibular third molar impaction. The study revealed that individuals with a dolichofacial growth pattern had a relatively shorter mandibular length, supporting the hypothesis that they are more susceptible to experiencing third molar impaction.1,29
What was unexpectedly interesting was the lack of significant difference in the incidence of impactions observed among the Brachyfacial, mesiofacial, and dolichofacial subjects (p = 0.812). Specifically, a t-test analysis yielded a statistically insignificant result when comparing dolichofacial and Brachyfacial groups (p = 0.147). However, it is important to exercise caution when drawing statistical conclusions due to the small sample size.
The research findings suggest that individuals with a brachyfacial type have a lower incidence of mandibular third molar impaction than those with a dolichofacial type. However, the results were statistically insignificant due to the limited sample size (n= 198). It is important to note that the present study utilized a non-randomized sample obtained from a single hospital within a specific city in Saudi Arabia. Future investigations should aim to assess the impact of third molars in a randomized sample that accurately represents the broader population of Saudi Arabia. Moreover, further prospective studies are needed to enhance our understanding of third molar impaction, as these teeth have the potential to change their position and continue erupting from their current location. These studies would allow for monitoring potential changes in the inclination of third molars and further validate the use of skeletal facial types as a predictive tool of third molar impaction.
Conclusion
The findings from a sample of the Saudi subpopulation revealed a significant prevalence of third molar impaction, with no observed correlation between impaction and sex or age. The most common angulation for impaction was vertical in the maxilla and mesioangular in the mandible. Type A upper third molar impaction was commonly observed in individuals with a dolichocephalic face. The Archer II classification of upper third molar showed a statistically significant association with skeletal profile. There was an association between facial type and the angulation of lower third molar impactions. The growth potential of the mandible in brachyfacial types may provide sufficient space for third molar eruption. Alternatively, the growth direction of the mandible may be more anterior, resulting in a horizontal occlusal plane and increased resorption of the anterior border of the ramus. Further research is warranted to better understand the relationship between third molar impaction and facial types.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Disclosure
The authors report no potential conflicts of interest for this work.
References
1. Hasan KM, Sobhana CR, Rawat SK, Singh D, Mongia P, Fakhruddin A. Third molar impaction in different facial types and mandibular length: a cross-sectional study. Natl J Maxillofac Surg. 2021;12(1):83. doi:10.4103/njms.NJMS_111_20
2. Yilmaz S, Adisen MZ, Misirlioglu M, Yorubulut S. Assessment of third molar impaction pattern and associated clinical symptoms in a Central Anatolian Turkish population. Med Princ Pract. 2016;25(2):169–175. doi:10.1159/000442416
3. Kaomongkolgit R, Tantanapornkul W. Pattern of impacted third molars in Thai population: retrospective radiographic survey. J Int Dent Med Res. 2017;10(1):30.
4. Idris AM, Al-Mashraqi AA, Abidi NH, et al. Third molar impaction in the Jazan Region: evaluation of the prevalence and clinical presentation. Saudi Dent J. 2021;33(4):194–200. doi:10.1016/j.sdentj.2020.02.004
5. Husain S, Rengalakshmi S. Correlation between mandibular third molar and mandibular incisor crowding: a retrospective CBCT-based study. J Dent Res Dent Clin Dent Prospects. 2021;15(4):247. doi:10.34172/joddd.2021.040
6. Jaroń A, Trybek G. The pattern of mandibular third molar impaction and assessment of surgery difficulty: a Retrospective study of radiographs in east Baltic population. Int J Environ Res Public Health. 2021;18(11):6016. doi:10.3390/ijerph18116016
7. Archer WH. Oral and Maxillofacial Surgery. WB Saunders; 1975.
8. Ahmad P, V’Vian T, Chaudhary FA, et al. Pattern of third molar impactions in north-eastern peninsular Malaysia: a 10-year retrospective study. Niger J Clin Pract. 2021;24(7):1028. doi:10.4103/njcp.njcp_499_20
9. Hassan AH. Mandibular cephalometric characteristics of a Saudi sample of patients having impacted third molars. Saudi Dent J. 2011;23(2):73–80. doi:10.1016/j.sdentj.2010.11.001
10. Kindler S, Ittermann T, Bülow R, et al. Does craniofacial morphology affect third molars impaction? Results from a population-based study in northeastern Germany. PLoS One. 2019;14(11):e0225444. doi:10.1371/journal.pone.0225444
11. Ocak Y, Cicek O, Ozkalayci N, Erener H. Investigation of the relationship between sagittal skeletal nasal profile morphology and malocclusions: a lateral cephalometric film study. Diagnostics. 2023;13(3):463. doi:10.3390/diagnostics13030463
12. Ricketts R. The influence of orthodontics treatments on facial growth and development. Angle Orthod. 1960;30:179–199. doi:10.1043/0003-3219(1960)030<0179:AROTRP>2.0.CO;2
13. Batwa W. The influence of the smile on the perceived facial type esthetics. Biomed Res Int. 2018;2018:1–7. doi:10.1155/2018/3562916
14. Jena AK, Nayyer N, Sharan J, Behera BK, Marya A. Geometrical approaches for the accurate identification of normal vertical positions of sella and nasion points in cephalograms. Int J Dent. 2022;2022:1–7. doi:10.1155/2022/2705416
15. Storniolo-Souza JM, Seminario MP, Pinzan-Vercelino CRM, Pinzan A, Janson G. McNamara analysis cephalometric parameters in White-Brazilians, Japanese and Japanese-Brazilians with normal occlusion. Dental Press J Orthod. 2021;26. doi:10.1590/2177-6709.26.1.e2119133.oar
16. Sami Q, Ali B, Farooqui WA. Effects of Alt-RAMEC protocol with facemask therapy in cleft lip palate patients in a sample of Pakistani population. BMC Oral Health. 2023;23(1):401. doi:10.1186/s12903-023-03093-w
17. Abdelkarim A. Cone-beam computed tomography in orthodontics. Dent J. 2019;7(3):89. doi:10.3390/dj7030089
18. Li C, Teixeira H, Tanna N, et al. The reliability of two-and three-dimensional cephalometric measurements: a CBCT study. Diagnostics. 2021;11(12):2292. doi:10.3390/diagnostics11122292
19. Zamora N, Llamas JM, Cibrián R, Gandia JL, Paredes V. A study on the reproducibility of cephalometric landmarks when undertaking a three-dimensional (3D) cephalometric analysis. Med Oral Patol Oral Cir Bucal. 2012;17(4):e678. doi:10.4317/medoral.17721
20. Tassoker M, Kok H, Sener S. Is there a possible association between skeletal face types and third molar impaction? A retrospective radiographic study. Med Princ Pract. 2019;28(1):70–74. doi:10.1159/000495005
21. Alfadil L, Almajed E. Prevalence of impacted third molars and the reason for extraction in Saudi Arabia. Saudi Dent J. 2020;32(5):262–268. doi:10.1016/j.sdentj.2020.01.002
22. Chen Y, Zheng J, Li D, et al. Three-dimensional position of mandibular third molars and its association with distal caries in mandibular second molars: a cone beam computed tomographic study. Clin Oral Investig. 2020;24:3265–3273. doi:10.1007/s00784-020-03203-w
23. Bashir S, Rasool G, Afzal F, Hassan N. Incidence of mandibular 3rd molar impactions in different facial types of orthodontic patients seen at Khyber college of dentistry. Pakistan Oral Dent J. 2016;36(2):1.
24. Hounsome J, Pilkington G, Mahon J, et al. Prophylactic removal of impacted mandibular third molars: a systematic review and economic evaluation. Health Technol Assess. 2020;24(30):1.
25. Vranckx M, Fieuws S, Jacobs R, Politis C. Prophylactic vs. symptomatic third molar removal: effects on patient postoperative morbidity. J Evid Based Dent Pract. 2021;21(3):101582. doi:10.1016/j.jebdp.2021.101582
26. Hassan AH. Pattern of third molar impaction in a Saudi population. Clin Cosmet Investig Dent. 2010;2010:109–113.
27. Khouri C, Aoun G, Khouri C, Saade M, Salameh Z, Berberi A. Evaluation of third molar impaction distribution and patterns in a sample of Lebanese population. J Maxillofac Oral Surg. 2022;2022:1–9.
28. Hashemipour MA, Tahmasbi-Arashlow M, Fahimi-Hanzaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a Southeast Iran population. Med Oral Patol Oral Cir Bucal. 2013;18(1):e140. doi:10.4317/medoral.18028
29. Ricketts RM. Studies leading to the practice of abortion of lower third molars. Dent Clin North Am. 1979;23(3):393–412. doi:10.1016/S0011-8532(22)01207-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.