")
Back to Journals » Patient Preference and Adherence » Volume 18
Taking a Newer, Faster, Intranasal Route: A Narrative Review of Transitioning to a Less-Invasive Rescue Treatment for Seizure Clusters
Authors Peters JM, Becker DA, Misra SN, Carrazana E , Rabinowicz AL
Received 1 November 2023
Accepted for publication 23 January 2024
Published 7 February 2024 Volume 2024:18 Pages 383—389
DOI https://doi.org/10.2147/PPA.S447028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jurriaan M Peters,1 Danielle A Becker,2 Sunita N Misra,3 Enrique Carrazana,3,4 Adrian L Rabinowicz3
1Department of Neurology, Harvard Medical School and Boston Children’s Hospital, Boston, MA, USA; 2Department of Neurology, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 3Neurelis, Inc, San Diego, CA, USA; 4Department of Family Medicine and Community Health, John A. Burns School of Medicine, University of Hawaii, Honolulu, HI, USA
Correspondence: Jurriaan M Peters, Division of Epilepsy and Clinical Neurophysiology, Boston Children’s Hospital and Harvard Medical School, 300 Longwood Ave, FE9, Boston, MA, 02115, USA, Tel +1 617-355-7970, Fax +1 617-730-4850, Email [email protected]
Abstract: In the US, 3 rescue treatment options are approved for patients with seizure clusters (ie, acute repetitive seizures), which are intermittent increases of seizure activity. This narrative PubMed review of these 3 treatments examines newer intranasal options that are well suited for adolescent and adult patients who may desire a transition from rectal treatment. Diazepam rectal gel is indicated for patients ≥ 2 years, diazepam nasal spray for those ≥ 6 years, and midazolam nasal spray for those ≥ 12 years. Approvals for diazepam rectal gel and midazolam nasal spray were based on safety and efficacy comparisons with placebo. Approval for diazepam nasal spray was based on results from long-term safety and tolerability studies in addition to its comparable bioavailability to diazepam rectal gel, while also showing less interpatient variability. The safety profiles of diazepam rectal gel and nasal spray are similar, and the medications share safety, warning, and precaution labeling. Thus, patients ≥ 6 years could be introduced to intranasal diazepam, allowing for continuity of familiar treatment while improving access and comfort. Intranasal midazolam also has a well-characterized safety profile. A proxy for effectiveness is the number of seizure clusters that were treated with a single dose, and these differed in separate, noncomparative studies. The safety and effectiveness of diazepam nasal spray have been examined in multiple subpopulations, whereas patient/caregiver experiences with both approved intranasal formulations have been characterized. Users may prefer nasal administration because it is noninvasive and effective, and provides social advantages, comfort, ease of use, and less variability compared with rectal gel. Nasal sprays are portable and convenient for use in the community (school, work, travel), and self-administration was reported in one study, with patients as young as 11 years old self-administering diazepam nasal spray. These newer, intranasal rescue treatments for seizure clusters provide an alternative to the rectal route.
Plain Language Summary: Some people with epilepsy may have seizure clusters, which are often defined as 2 or more seizures in a day that are not part of their normal seizure pattern. Rescue treatments approved in the United States are diazepam rectal gel, diazepam nasal spray, and midazolam nasal spray. These rescue drugs can help stop seizure clusters at home, school, or work. Diazepam rectal gel is for adults and children ages 2 years or older. To give a rectal dose, the caregiver must pull down the patient’s underwear. Spraying nasal treatment into the nose may be less embarrassing. Because some patients may want to switch their treatment, we looked for articles about how to use these treatments and summarized what we found. Diazepam nasal spray is for patients ages 6 years or older and midazolam nasal spray is for patients 12 years or older. Diazepam rectal gel and nasal spray use the same drug, and dosing is based on patient age and weight. Midazolam nasal spray uses a different drug, and everyone uses the same dose. Some drugs may be more likely than others to need a second dose for a seizure. Patients and caregivers (care partners) felt that diazepam nasal spray was easier to use than rectal gel. They were also more comfortable using diazepam nasal spray in public. Patients as young as 11 years have used diazepam nasal spray by themselves. In all, patients may prefer nasal treatment and now have options to change from rectal treatment of seizure clusters.
Keywords: nasal spray, rectal gel, diazepam, midazolam, epilepsy, switch
Introduction
Seizure clusters, also known as acute repetitive seizures, are defined as intermittent increases of seizure activity (≥2 seizures of any type) for a duration of up to 24 hours or longer that occur while on stable regimens of antiseizure drugs.1,2 Approximately 25 years ago, diazepam rectal gel became the first US Food and Drug Administration (FDA)–approved treatment for seizure clusters,3 filling an important unmet medical need for a rapidly effective, long-lasting treatment with a favorable safety profile that was available to nonmedical caregivers in the community.1 It was suggested that this at-home treatment option had the potential to halve the need for visits to the emergency department.4 Importantly, some families reported less disruption of daily activities, work, and school and increased confidence that empowered them to manage epilepsy and make long-term plans and travel.4 However, although diazepam rectal gel is able to provide a large dose volume with high bioavailability (90%), interpatient absorption is inconsistent with possible leakage (ejection of the gel), the route of administration is associated with social concerns,1,5 it may be difficult for caregivers to position patients for treatment (eg, large, fragile, and/or wheelchair-bound patients), and preparation for administration requires multiple steps,6 such as putting on gloves, cleaning the rectal area, and applying rectal lubricant.
Intranasal administration shares many of the same positive attributes as the rectal route while also providing improved ease of use and avoiding first-pass metabolism.1,7,8 The less-invasive, socially acceptable administration may facilitate use by adults and school-aged children at work, school, and social events, as well as empowering caregivers who might not be comfortable with the more complex rectal administration. To date, there are 2 FDA-approved intranasal rescue medications for use in the community to treat seizure clusters: one uses the diazepam molecule and the other uses the midazolam molecule.
Methods
For this practical narrative review of recent literature for the 3 approved rescue therapies, the PubMed database was searched for relevant terms (eg, diazepam rectal gel, midazolam nasal spray, diazepam nasal spray). The resulting papers, which included all primary and secondary Phase 3 results for the approved medications, were assessed by the authors to determine similarities and differences between agents and implications for patients who might prefer to switch to a new treatment.
Results
Diazepam rectal gel is approved for use in patients ≥2 years of age, diazepam nasal spray is approved for use in those ≥6 years, and midazolam nasal spray is approved for those ≥12 years.1,9 Diazepam rectal gel and diazepam nasal spray use similar age- and weight-based dosing strategies, whereas midazolam uses a single dosage irrespective of weight (Table 1).9
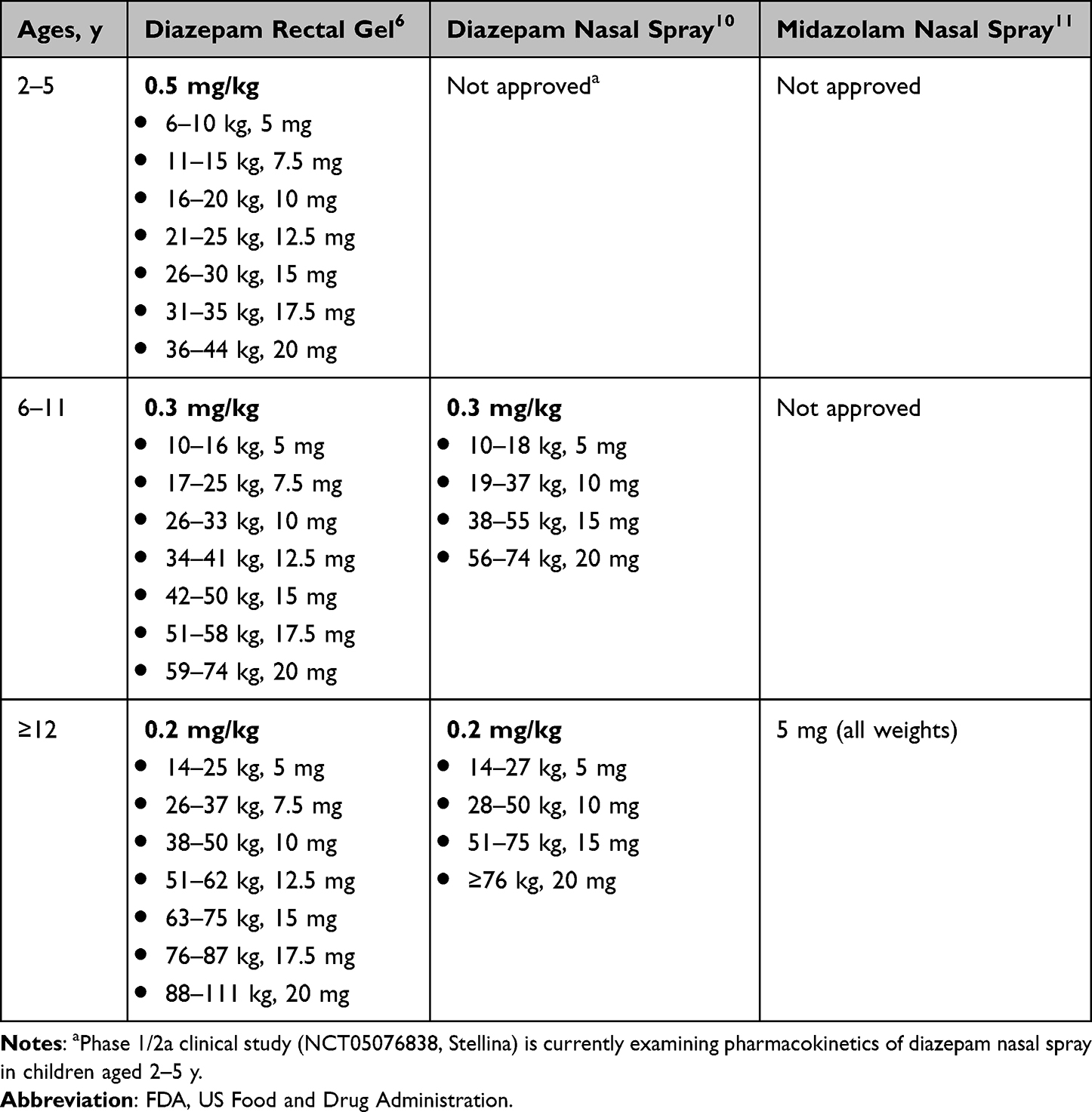 |
Table 1 Recommended Dosages for FDA-Approved Rescue Medications |
Diazepam nasal spray uses the same active ingredient as diazepam rectal gel and incorporates vitamin E to enhance solubility and an excipient to enhance transmucosal absorption.12 The FDA approval of diazepam nasal spray was based on its comparable bioavailability to diazepam rectal gel as a reference drug (97% vs 90%, respectively; bioavailability relative to intravenous administration),1,12 while also showing less interpatient variability.13 Midazolam nasal spray incorporates organic solvents to enhance solubility (absolute bioavailability ~44%),11 and was approved based on safety and efficacy comparisons with placebo14 but was not compared to diazepam rectal gel.
A clinical trial that examined safety and efficacy of midazolam nasal spray consisted of test-dose and comparative phases.14 In the test-dose phase (n=292 [age <18 years, n=18; age 18 to <65 years, n=272; age ≥65 years, n=2]), patients were administered two 5-mg doses of midazolam nasal spray 10 minutes apart to determine safety while under observation. Thirty patients discontinued the trial following the test-dose phase, and 13 discontinued owing to a treatment-related adverse event; 2 patients experienced clinically meaningful respiratory depression. Of the 262 patients who entered the randomized, placebo-controlled comparative phase, 201 received at least 1 double-blind dose of treatment. The proportion of patients who achieved treatment success (seizure termination within 10 minutes of administration and no seizure recurrence from 10 minutes to 6 hours) was significantly greater with midazolam nasal spray than placebo (54% vs 34%, P<0.0109). In the 6 month comparative phase, 28% of patients who received midazolam nasal spray alone reported at least 1 treatment-emergent adverse event (TEAE), 25% experienced a treatment-related TEAE, and 1% reported a serious TEAE (not treatment-related).14 An open-label extension trial was conducted to examine the long-term (median duration 16.8 months) safety and efficacy of midazolam nasal spray in a group of patients from the randomized clinical trial.14,15 In this long-term study (n=161), treatment success occurred in 55% of treated seizure episodes, and 57% of patients reported at least 1 TEAE.15 Treatment-related TEAEs were reported in 35% of patients, 11% reported serious TEAEs, and 2% reported serious treatment-related TEAEs.15
The safety profiles of diazepam rectal gel and diazepam nasal spray are similar4,12 and the medications share safety, warning, and precaution labeling.6,10 In the long-term clinical study of diazepam rectal gel (N=149 [age 2–5 years, n=33; age 6–11 years, n=39; age 12–76 years, n=77]), somnolence occurred in 17% of patients (9% attributed to treatment).4 In the long-term clinical study of diazepam nasal spray, which included patients with history of status epilepticus or who were receiving concomitant daily benzodiazepine treatment for epilepsy (n=163 [age 6–11 years, n=45; age 12–65, n=118]), somnolence occurred in 7% of patients (<2% attributed to treatment); 6% of patients reported nasal discomfort (mostly mild and transient).12 Intranasal midazolam also has a well-known safety profile including a warning about the elevated risk of impaired recall/cognitive impairment for several hours after administration.11 In an open-label extension trial of intranasal midazolam in patients aged ≥12 years without history of status epilepticus or chronic antiseizure benzodiazepine therapy (n=161 [age <18 years, n=8; age 18–64 years, n=153]),14,15 nasal discomfort occurred in 12% of patients and somnolence in 9%.15
The number of seizure clusters that were treated with a single dose—a proxy for effectiveness—differed in 3 separate, noncomparative long-term safety studies.16 In the long-term study of diazepam rectal gel, 77% of seizure clusters were treated with a single dose during the 12-hour observation period,4 whereas in the long-term study of diazepam nasal spray, 87% of seizure clusters were treated with a single dose across 24 hours.12 In the long-term study of midazolam nasal spray, 62% of seizure clusters were treated with a single dose within 6 hours.15 These results suggest that use of second doses of rescue medication or subsequent need for hospitalization are potential factors to consider when analyzing overall healthcare resource use; however formal comparative analyses of rescue medications are lacking.16,17
Outcomes have also been assessed for specific subpopulations and quality-of-life endpoints. In the long-term study of diazepam nasal spray (n=163), the safety and effectiveness in pediatric patients aged 6 to 17 years (n=78; nearly half of total participants);18 those receiving FDA-approved, highly purified cannabidiol (n=23; 22 pediatric)19 or concomitant benzodiazepines (n=125);12,20 and those with seasonal allergies/rhinitis (n=93)12,21 were generally similar to the safety and effectiveness observed in the overall total study population.12 Similarly, average frequency of use per month did not affect safety or effectiveness profiles of diazepam nasal spray,12,22 and there were no observations of a clinically relevant food effect during the clinical development program for this nasal formulation.23 The Quality of Life in Epilepsy Inventory (QOLIE)-31-P was used to evaluate health-related quality of life in the diazepam study.24 Clinically meaningful improvements in key domains of Seizure Worry and Social Functioning were reported, whereas overall QOLIE-31-P scores were maintained over the 12-month study period in these patients with drug-resistant epilepsy. Overall scores, as well as Seizure Worry and Social Functioning subscale scores, were higher in patients who self-administered diazepam nasal spray, suggesting that self-administration may provide a greater sense of seizure control.24
In addition to outcomes of treatment success and standard adverse events, the long-term study of midazolam nasal spray reported adverse events of special interest (AESI) as well as outcomes related to quality of life.8,15 The most common AESIs were in the prespecified categories of route of administration (primarily, nasal discomfort) and potentially abuse-related (primarily, sedation) categories,15 but there were no adverse events indicative of abuse.15 For quality of life, patients and caregivers completed the Short Form-12 Health Survey version 2 (SF-12v2).8 Improvements from baseline to the last visit were noted in several domains (eg, physical functioning, general health) of the SF-12v2. Patients and caregivers also completed the Intranasal Therapy Impact Questionnaire, which assesses patient and caregiver perceptions of how access to midazolam nasal spray affects their level of anxiety and confidence to travel with a portable intranasal treatment. Patient and caregiver anxiety generally decreased over time; and at last study visit, 80% of patients and 82% of caregivers agreed or strongly agreed about their confidence to travel with an intranasal spray they could take with them. Patient experience with midazolam nasal spray was examined with the Treatment Satisfaction Questionnaire for Medication, which consists of effectiveness, side effects, convenience, and global-satisfaction scores. Improvements (satisfaction) from baseline at the final visit were reported for effectiveness, convenience, side effects, and global-satisfaction scores, and general increases in satisfaction were noted in those with repeated use of midazolam nasal spray.8
Recently, a novel analysis was conducted post hoc to explore time between seizure clusters by examining the potential association of change in SEIzure interVAL (SEIVAL) over time with intermittent rescue therapy with diazepam nasal spray.25 In the long-term safety study, mean SEIVAL increased over the 12-month study period. In patients who had ≥1 SEIVAL in each of four 90-day periods (excluding re-treatments for a single seizure cluster), mean SEIVAL increased from 13.9 days at the beginning of the study (first 90-d period) to 26.8 days by the end of the study (last 90-d period), and the pattern of increase in mean SEIVAL was similar regardless of whether patients had a change in drug or dose of concomitant (daily) antiseizure drugs.25 Future studies are needed to fully explore the underlying reasons behind the reduced use, and perhaps requirements for, diazepam nasal spray.
Patients and caregivers may prefer nasal to rectal administration. In the long-term diazepam nasal spray study, patients and caregivers reported improved ease of use compared with rectal gel.7 Administration of the nasal spray requires fewer steps compared with the 14-step process for rectal gel that includes positioning the patient and preparing the applicator.26 Ninety-four percent of caregivers and 78% of patients who self-administered medication rated administration of diazepam nasal spray as extremely easy or very easy, and 84% of patients overall indicated a preference to continue with diazepam nasal spray based on convenience.7 In self-administering patients (reported in patients aged 11–65 y), 67% were extremely, very, or somewhat comfortable with use of diazepam nasal spray in public. Almost two-thirds (64%) of caregivers who had experience with diazepam rectal gel felt that it was not at all easy to use compared with diazepam nasal spray, and 87% were not at all comfortable using diazepam rectal gel in public compared with diazepam nasal spray. Overall, 88% of both patients and caregivers preferred diazepam nasal spray rescue over diazepam rectal gel.7 In a systematic review of administration of midazolam for injection given intranasally and a benzodiazepine given intravenously or rectally for acute seizure control, although all were considered to be effective, midazolam given intranasally decreased the time from hospital arrival to seizure cessation, leading to overall faster cessation time (the midazolam nasal spray formulation was not included in this analysis).27 In a study of pediatric patients (mean age, 10.6 y; range, 3–22 y), caregivers reported that ease of use, comfort, and efficacy were higher with midazolam delivered intranasally compared with rectal diazepam.28 In another study in adults, an early intranasal midazolam spray formulation (pH 4)29 was preferred to diazepam rectal solution by 76% of caregivers and patients.30
Notably, there are no special requirements associated with administration of either of the approved nasal spray formulations, including head position.10,11 The 15- and 20-mg doses of diazepam nasal spray require the use of 2 sprays or devices (one in each nostril) to provide the appropriate age- and weight-based full dose.10 Midazolam nasal spray requires 1 spray (5-mg dose) for the initial dose, sprayed into 1 nostril, irrespective of patient weight.11
Warnings and precautions for both intranasal and rectal formulations are similar6,10,11 owing to class labeling.11 Thus, patients and their caregivers could be introduced to the intranasal options. Diazepam nasal spray is approved for patients aged ≥6 years. Although diazepam spray is not approved for patients <6 years of age, an open-label, phase 1/2a clinical study [NCT05076838, Stellina] is currently underway in children aged 2 to 5 years.31 Because the indication is similar to the rectal gel, initiating diazepam nasal spray requires only prescription of the equivalent dose of diazepam with brief training, which caregivers report to be easy.7 Parents and caregivers may be comfortable transitioning to alternative, easier routes of administration when there is a level of familiarity with the active agent (benzodiazepine). Midazolam nasal spray provides an additional option for administration to patients aged ≥12 years. For patients at risk of respiratory depression, administration under healthcare professional supervision should be considered before initiating at-home treatment.11 The nasal sprays should be used in exactly the same situations for patients with epilepsy in accordance with their approved minimum ages. Intranasal administration may address social concerns and provide convenience for patients aged ≥6 years who would benefit from rescue medications that can easily transition from home to primary education/school settings as well as other activities outside the home. Patients should not operate hazardous machinery or a motor vehicle until the effects of diazepam or midazolam, such as drowsiness, have subsided.6,10,11 For patients initiating midazolam, prescribing information states that midazolam is associated with a high incidence of partial or complete impairment of recall for several hours after an administered dose.11 For pediatric patients, particular care should be taken to ensure safe ambulation.11 The initial dose for midazolam nasal spray is a single spray into 1 nostril (5 mg) and, if the patient has not responded to this dose, then a second 5-mg dose can be sprayed into the other nostril after 10 minutes. For diazepam nasal spray, if a second dose is required (if the patient has not responded to the first dose), then it can be administered after 4 hours. For both nasal sprays, no more than 2 doses should be used to treat a single episode.10,11 These nasal sprays should be used to treat no more than 1 episode every 3 (midazolam nasal spray) or 5 days (diazepam nasal spray), with no more than 5 episodes treated per month for either drug.10,11
Conclusion
The availability of these newer, intranasal rescue treatments for seizure clusters provides an alternative to the older methods of benzodiazepine administration. Because intranasal treatments are of similar efficacy and safety and have been shown to be preferred by many caregivers and patients, physicians should consider the potential benefits of ease of use, social acceptability, reduced disruption to patients’ and caregivers’ daily activities, and empowerment to manage acute seizure clusters.
Acknowledgments
Editorial support was provided by Kirk W. Evanson, PhD, of The Curry Rockefeller Group, LLC (Tarrytown, NY, USA), and was funded by Neurelis, Inc (San Diego, CA, USA).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This manuscript was funded by Neurelis, Inc. (San Diego, CA, USA).
Disclosure
Dr Peters has served as a speaker and consultant for Greenwich Biosciences; Neurelis, Inc.; and Novartis. Dr Becker is a consultant/speaker for Neurelis, Inc.; SK Life Science; UCB; and Jazz Pharmaceuticals; and received research support from SK Life Science. Dr Misra was an employee of Neurelis, Inc., at the time of the development of this manuscript and received stock options from Neurelis, Inc. Dr Rabinowicz is an employee of and has received stock options from Neurelis, Inc. Dr Carrazana is an employee of and received stock and stock options from Neurelis, Inc.
References
1. Cloyd J, Haut S, Carrazana E, Rabinowicz AL. Overcoming the challenges of developing an intranasal diazepam rescue therapy for the treatment of seizure clusters. Epilepsia. 2021;62(4):846–856. doi:10.1111/epi.16847
2. Haut SR, Nabbout R. Recognizing seizure clusters in the community: the path to uniformity and individualization in nomenclature and definition. Epilepsia. 2022;63(suppl):S6–S13. doi:10.1111/epi.17346
3. Cereghino JJ, Mitchell WG, Murphy J, Kriel RL, Rosenfeld WE, Trevathan E. Treating repetitive seizures with a rectal diazepam formulation: a randomized study. The North American diastat study group. Neurology. 1998;51(5):1274–1282. doi:10.1212/WNL.51.5.1274
4. Mitchell WG, Conry JA, Crumrine PK, et al. An open-label study of repeated use of diazepam rectal gel (Diastat) for episodes of acute breakthrough seizures and clusters: safety, efficacy, and tolerance. North American Diastat Group Epilepsia. 1999;40(11):1610–1617.
5. Hua S. Physiological and pharmaceutical considerations for rectal drug formulations. Front Pharmacol. 2019;10:1196.
6. Bausch Health US, LLC. Diastat® C-IV (Diazepam Rectal Gel) [Prescribing Information]. Bridgewater, NJ: Bausch Health US, LLC; 2023.
7. Penovich P, Wheless JW, Hogan RE, et al. Examining the patient and caregiver experience with diazepam nasal spray for seizure clusters: results from an exit survey of a phase 3, open-label, repeat-dose safety study. Epilepsy Behav. 2021;121(Pt A):108013. doi:10.1016/j.yebeh.2021.108013
8. Meng TC, Szaflarski JP, Chen L, et al. Psychosocial outcomes of repeated treatment of seizure clusters with midazolam nasal spray: results of a phase 3, open-label extension trial. Epilepsy Behav. 2023;138:108989. doi:10.1016/j.yebeh.2022.108989
9. Dean P, O’Hara K, Brooks L, Shinnar R, Bougher G, Santilli N. Managing acute seizures: new rescue delivery option and resources to assist school nurses. NASN Sch Nurse. 2021;36(6):346–354. doi:10.1177/1942602X211026333
10. Neurelis, Inc. VALTOCO® (Diazepam Nasal Spray) [Prescribing Information]. San Diego, CA: Neurelis, Inc.; 2023.
11. UCB, Inc. Nayzilam® (Midazolam Nasal Spray) [Prescribing Information]. Smyrna, GA: UCB, Inc.; 2023.
12. Wheless JW, Miller I, Hogan RE, et al. Final results from a phase 3, long-term, open-label, repeat-dose safety study of diazepam nasal spray for seizure clusters in patients with epilepsy. Epilepsia. 2021;62(10):2485–2495. doi:10.1111/epi.17041
13. Hogan RE, Gidal BE, Koplowitz B, Koplowitz LP, Lowenthal RE, Carrazana E. Bioavailability and safety of diazepam intranasal solution compared to oral and rectal diazepam in healthy volunteers. Epilepsia. 2020;61(3):455–464. doi:10.1111/epi.16449
14. Detyniecki K, Van Ess PJ, Sequeira DJ, Wheless JW, Meng TC, Pullman WE. Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters-A randomized, double-blind, placebo-controlled trial. Epilepsia. 2019;60(9):1797–1808. doi:10.1111/epi.15159
15. Wheless JW, Meng TC, Van Ess PJ, Detyniecki K, Sequeira DJ, Pullman WE. Safety and efficacy of midazolam nasal spray in the outpatient treatment of patients with seizure clusters: an open-label extension trial. Epilepsia. 2019;60(9):1809–1819. doi:10.1111/epi.16300
16. Rabinowicz AL, Faught E, Cook DF, Carrazana E. Implications of seizure-cluster treatment on healthcare utilization: use of approved rescue medications. Neuropsychiatr Dis Treat. 2022;18:2431–2441. doi:10.2147/NDT.S376104
17. Faught E. Economic aspects of treating seizure clusters. Epilepsia. 2022;63(suppl 1):S45–54. doi:10.1111/epi.17340
18. Tarquinio D, Dlugos D, Wheless JW, Desai J, Carrazana E, Rabinowicz AL. Safety of diazepam nasal spray in children and adolescents with epilepsy: results from a long-term phase 3 safety study. Pediatr Neurol. 2022;132:50–55. doi:10.1016/j.pediatrneurol.2022.04.011
19. Peters JM, Puri V, Segal E, Misra SN, Rabinowicz AL, Carrazana E. Concomitant cannabidiol does not impact safety and effectiveness of diazepam nasal spray for seizure clusters: post hoc analysis of a phase 3 safety study. Epilepsy Behav. 2023;144:109248. doi:10.1016/j.yebeh.2023.109248
20. Segal EB, Tarquinio D, Miller I, et al. Evaluation of diazepam nasal spray in patients with epilepsy concomitantly using maintenance benzodiazepines: an interim subgroup analysis from a phase 3, long-term, open-label safety study. Epilepsia. 2021;62(6):1442–1450. doi:10.1111/epi.16901
21. Vazquez B, Wheless J, Desai J, Rabinowicz AL, Carrazana E. Lack of observed impact of history or concomitant treatment of seasonal allergies or rhinitis on repeated doses of diazepam nasal spray administered per seizure episode in a day, safety, and tolerability: interim results from a phase 3, open-label, 12-month repeat-dose safety study. Epilepsy Behav. 2021;118:107898. doi:10.1016/j.yebeh.2021.107898
22. Miller I, Wheless JW, Hogan RE, et al. Consistent safety and tolerability of Valtoco® (diazepam nasal spray) in relationship to usage frequency in patients with seizure clusters: interim results from a phase 3, long-term, open-label, repeat-dose safety study. Epilepsia Open. 2021;6(3):504–512. doi:10.1002/epi4.12494
23. Cook DF, Gustin RM, Misra SN, et al. Effectiveness of diazepam nasal spray does not vary across times of day associated with meals and fasting in patients with seizure clusters: post hoc results from a long-term, open-label safety study. Nashville, TN: Presented at: AES; 2022.
24. Cramer JA, Faught E, Davis C, Misra SN, Carrazana E, Rabinowicz AL. Quality-of-life results in adults with epilepsy using diazepam nasal spray for seizure clusters from a long-term, open-label safety study. Epilepsy Behav. 2022;134:108811. doi:10.1016/j.yebeh.2022.108811
25. Misra SN, Sperling MR, Rao VR, et al. Significant improvements in SEIzure interVAL (time between seizure clusters) across time in patients treated with diazepam nasal spray as intermittent rescue therapy for seizure clusters. Epilepsia. 2022;63(10):2684–2693. doi:10.1111/epi.17385
26. O’Hara K, Dewar S, Bougher G, Dean P, Misra SN, Desai J. Overcoming barriers to the management of seizure clusters: ease of use and time to administration of rescue medications. Expert Rev Neurother. 2023;23(5):425–432. doi:10.1080/14737175.2023.2206568
27. Chhabra R, Gupta R, Gupta LK. Intranasal midazolam versus intravenous/rectal benzodiazepines for acute seizure control in children: a systematic review and meta-analysis. Epilepsy Behav. 2021;125:108390. doi:10.1016/j.yebeh.2021.108390
28. Nunley S, Glynn P, Rust S, Vidaurre J, Albert DVF, Patel AD. A hospital-based study on caregiver preferences on acute seizure rescue medications in pediatric patients with epilepsy: intranasal midazolam versus rectal diazepam. Epilepsy Behav. 2019;92:53–56. doi:10.1016/j.yebeh.2018.12.007
29. Knoester PD, Jonker DM, Van Der Hoeven RT, et al. Pharmacokinetics and pharmacodynamics of midazolam administered as a concentrated intranasal spray. A study in healthy volunteers. Br J Clin Pharmacol. 2002;53(5):501–507. doi:10.1046/j.1365-2125.2002.01588.x
30. de Haan GJ, van der Geest P, Doelman G, Bertram E, Edelbroek P. A comparison of midazolam nasal spray and diazepam rectal solution for the residential treatment of seizure exacerbations. Epilepsia. 2010;51(3):478–482. doi:10.1111/j.1528-1167.2009.02333.x
31. ClinicalTrials.gov. Pharmacokinetics study of VALTOCO® in pediatric subjects with epilepsy (NCT05076838). Available from: https://clinicaltrials.gov/ct2/show/NCT05076838.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.