")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Systemic Drugs for Hepatocellular Carcinoma: What Do Recent Clinical Trials Reveal About Sequencing and the Emerging Complexities of Clinical Decisions?
Authors Himmelsbach V, Koch C, Trojan J , Finkelmeier F
Received 12 October 2023
Accepted for publication 7 February 2024
Published 19 February 2024 Volume 2024:11 Pages 363—372
DOI https://doi.org/10.2147/JHC.S443218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Vera Himmelsbach, Christine Koch, Jörg Trojan, Fabian Finkelmeier
Department of Gastroenterology, Hepatology and Endocrinology, University Hospital Frankfurt, Frankfurt, Germany
Correspondence: Jörg Trojan, Medizinische Klinik 1, Klinikum der Johann Wolfgang Goethe-Universität, Theodor-Stern-Kai 7, Frankfurt, 60590, Germany, Tel +49 069 6301 7860, Fax +49 69 6301 6448, Email [email protected]
Abstract: Liver cancer was the fourth leading cause of cancer death in 2015 with increasing incidence between 1990 and 2015. Orthotopic liver transplantation, surgical resection and ablation comprise the only curative therapy options. However, due to the late manifestation of clinical symptoms, many patients present with intermediate or advanced disease, resulting in no curative treatment option being available. Whereas intermediate-stage hepatocellular carcinoma (HCC) is usually still addressable by transarterial chemoembolization (TACE), advanced-stage HCC is amenable only to pharmacological treatments. Conventional cytotoxic agents failed demonstrating relevant effect on survival also because their use was severely limited by the mostly underlying insufficient liver function. For a decade, tyrosine kinase inhibitor (TKI) sorafenib was the only systemic therapy that proved to have a clinically relevant effect in the treatment of advanced HCC. In recent years, the number of substances for systemic treatment of advanced HCC has increased enormously. In addition to tyrosine kinase inhibitors, immune checkpoint inhibitors (ICI) and antiangiogenic drugs are increasingly being applied. The combination of anti-programmed death ligand 1 (PD-L1) antibody atezolizumab and anti-vascular endothelial growth factor (VEGF) antibody bevacizumab has become the new standard of care for advanced HCC due to its remarkable response rates. This requires more and more complex clinical decisions regarding tumor therapy. This review aims at summarizing recent developments in systemic therapy, considering data on first- and second-line treatment, use in the neoadjuvant and adjuvant setting and combination with locoregional procedures.
Keywords: hepatocellular carcinoma, systemic therapy, checkpoint inhibitors, neoadjuvant treatment, adjuvant treatment
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and develops in 80–90% due to liver cirrhosis.1 Therefore, in addition to tumor stage, the presence and extent of the liver cirrhosis, as well as the underlying disease of the cirrhosis, are major factors in evaluating the various therapeutic options. As the prognosis is significantly influenced by liver function and any underlying disease, the BCLC classification (Barcelona Clinic Liver Classification) for HCC2 also includes liver function and ECOG status (Eastern Cooperative Oncology Group) in addition to tumor extent. In early stages (BCLC 0 and A), resection, as well as local ablative procedures are also available as curative therapy options. HCC recurrence after resection or ablation occurs in 70–80%.3 In order to evaluate their effectiveness on recurrence free survival (RFS), neoadjuvant and adjuvant therapies were performed in the context of clinical trials.3–5
In the intermediate stage (BCLC B), when no curative therapy options are available, transarterial chemoembolization (TACE) or radioembolization (TARE) can be performed if liver function is preserved.6,7
Resection, transcutaneous ablation, and transarterial procedures can also be applied for bridging and downstaging to liver transplantation.8,9
For HCC patients with distant metastases or intrahepatic tumor manifestation that is not resectable and cannot be controlled by locoregional procedures, the antiproliferative and antiangiogenic tyrosine kinase inhibitor (TKI) sorafenib has been approved since November 2007.10 Since its approval, the multityrosine kinase inhibitor sorafenib was the only option in systemic treatment of HCC available for a decade. In the past five years, there have been fundamental changes in terms of systemic therapy options for advanced HCC.
With the TKI lenvatinib showing non-inferiority to sorafenib a second option for systemic therapy was established in 2018.11 In 2020, the combination of the immune checkpoint inhibitor (ICI) atezolizumab (anti-PD-L1 antibody) and the antiangiogenic bevacizumab (anti-VEGF antibody) proved superiority in the IMBRAVE-150 trial to sorafenib and is since then considered the standard of care in systemic first-line treatment of HCC.12,13 Limiting factors in the application of atezolizumab and bevacizumab are liver function and the individual patient’s risk of variceal bleeding.12–14
There have also been advances in second-line therapy in recent years: The TKI regorafenib is very similar to sorafenib in terms of molecular structure and mechanism of action. In the Phase 3 RESORCE study, a significantly prolonged median overall survival (mOS 10.6 months with regorafenib vs 7.8 months with placebo) was achieved in patients with tumor progression under sorafenib but good tolerability of the agent.15 Cabozantinib is a multityrosine kinase with approval in second- and third-line treatment of HCC. Cabozantinib showed a median overall survival (mOS) comparable to regorafenib in phase 3 study CELESTIAL.16 Especially in case of discontinuation of sorafenib therapy due to toxicity, second-line therapy with cabozantinib is recommended in preference to regorafenib therapy.15,16 In addition, the anti-VEGF 2 receptor antibody ramucirumab can be used in the second-line for patients with alpha-fetoprotein (AFP) ≥ 400 ng/mL.17
In this review, we will consider the current trials of new therapeutic options and discuss their implications for treatment sequencing in HCC.
Emerging Agents for Systemic HCC Treatment
Immune Checkpoint Inhibitors
In first-line setting, the combination of atezolizumab and bevacizumab (A+B) and two TKI lenvatinib and sorafenib were available so far.10,11,13 In October 2022, the Food and Drug Administration (FDA) approved the combination of the anti-programmed cell death ligand 1 (PD-L1) antibody durvalumab with a single “priming” dose of the anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) antibody tremelimumab (STRIDE regimen) for first-line treatment of HCC due to the convincing results in phase 3 trial.18 With regard to median overall survival durvalumab and tremelimumab (D+T) showed superiority to sorafenib (16.43 months (95% confidence interval [CI] 14.16–19.58) versus 13.77 months (95% CI 12.25–16.13; hazard ratio [HR] 0.78; p = 0.0035)). The secondary objective, the non-inferiority of durvalumab to sorafenib (16.56 months (95% CI 14.06–19.12) versus 13.77 months (95% CI 12.25–16.13; HR 0.86; p = 0.0674)) was reached as well (Table 1). D+T showed more frequent and severe immune-mediated reactions than durvalumab alone. Both D+T and durvalumab monotherapy were not associated with relevant liver toxicity. Under therapy with D+T or durvalumab no esophageal or gastrointestinal bleeding events were observed.
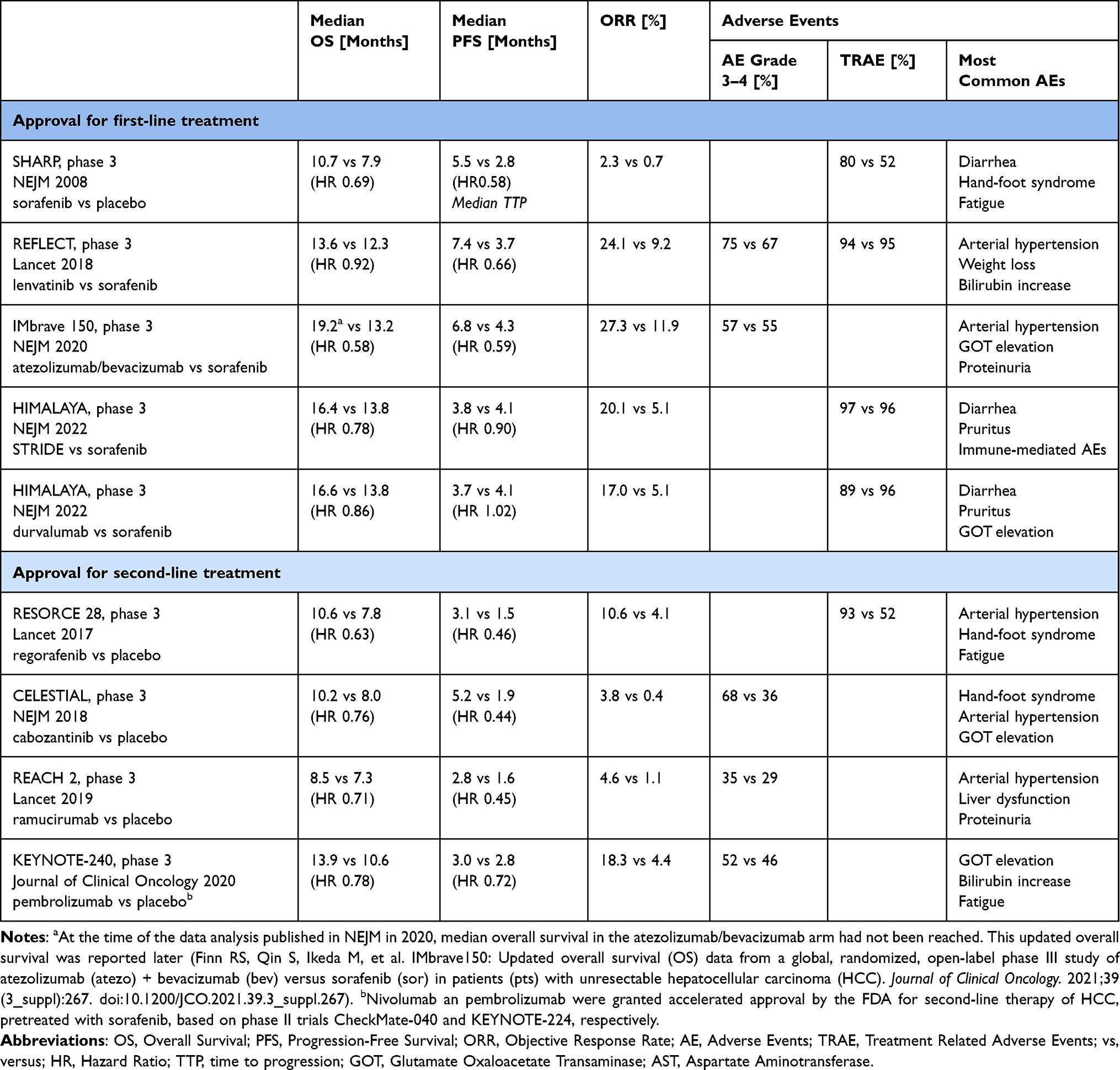 |
Table 1 Results of Published Phase 3 Trials of Approved Systemic Therapy for Advanced Hepatocellular Carcinoma |
D+T remained only slightly behind A+B (19.2 months (95% CI 17.0–23.7) vs 13.4 months (95% CI 11.4–16.9) under sorafenib (HR 0.66; 95% CI 0.52–0.85; p < 0.001)) and provides a good alternative, especially for patients with contraindications to antiangiogenic bevacizumab due to a high risk of bleeding events or high risk of hepatic decompensation12,14 (Figure 1).
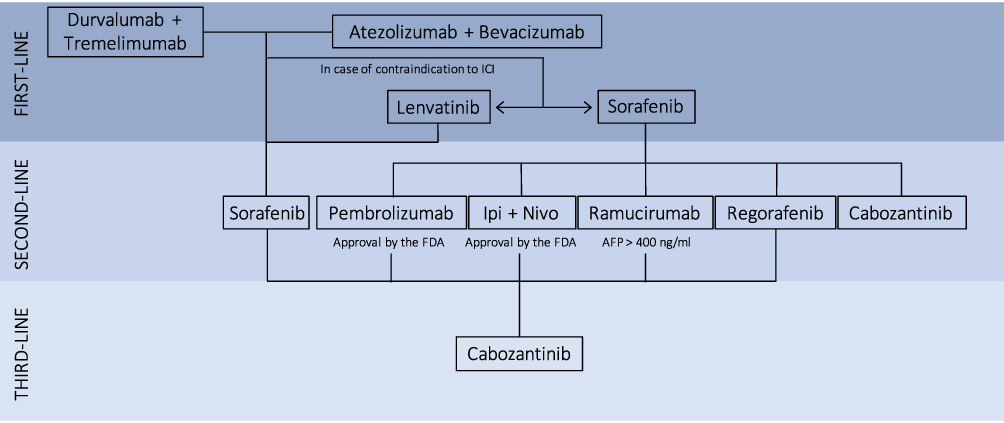 |
Figure 1 Algorithm for systemic therapy of hepatocellular carcinoma. Abbreviations: ICI, immune checkpoint inhibitor; Ipi + Nivo, ipilimumab plus nivolumab; AFP, Alpha fetoprotein; FDA, Food and Drug Administration. |
As another immune checkpoint inhibitor (ICI), anti-PD-1 antibody pembrolizumab obtained accelerated approval from the FDA in November 2018 based on results from the global Phase 2 KEYNOTE-224 study conducted in second-line patients following therapy with sorafenib.19,20 In the global phase 3 KEYNOTE-240 study, a similar favorable benefit-risk profile was observed for pembrolizumab in combination with best supportive care (BSC) compared to placebo plus BSC. However, the KEYNOTE-240 trial failed to meet the statistical significance criteria for overall survival (OS) or progression-free survival (PFS).21
The KEYNOTE-394 trial was conducted to determine whether pembrolizumab plus BSC would improve efficacy compared with placebo plus BSC in Asian patients with advanced HCC previously treated with sorafenib- or oxaliplatin-based chemotherapy.22
In terms of median OS (14.6 versus 13.0 months (HR 0.79; 95% CI 0.63–0.99; p = 0.0180)), median PFS (2.6 versus 2.3 months (HR 0.74; 95% CI 0.60–0.92; p = 0.0032)), and ORR (12.7% (95% CI 9.1–17.0) versus 1.3% (95% CI 0.2–4.6; p < 0.0001)), pembrolizumab was superior to BSC. Safety profile was consistent with previously observed results.
Nivolumab, PD-1 inhibitor as well, and the combination of nivolumab and the anti-CTLA-1 antibody ipilimumab were granted accelerated approval for the treatment of HCC pre-treated with sorafenib in 2017 due to durable responses observed in CheckMate-040.23 However, in CheckMate-459 nivolumab alone in a first-line setting failed to improve mOS compared to sorafenib (16.4 months (95% CI 13.9–18.4) vs 14.7 months (95% CI 11.9–17.2; HR 0.85; p = 0.075)),24 despite having a similar mOS to D+T. Consequently, the approval of nivolumab in second-line treatment was withdrawn. The data on nivolumab plus ipilimumab versus sorafenib or lenvatinib in first-line from CheckMate-9DW are still pending (NCT04039607).
The anti-PD1 antibody tislelizumab met its primary endpoint and demonstrated non-inferiority to sorafenib in first-line treatment with regard to mOS (15.9 months vs 14.1 months; HR: 0.85 (95.003% CI: 0.712–1.019)). Median PFS (mPFS) with tislelizumab was 2.2 months and 3.6 months with sorafenib (HR 1.1 (95% CI: 0.92–1.33)).25,26
Combination of Immune Checkpoint Inhibitors with Tyrosine Kinase Inhibitors
The combination of the PD1 antibody camrelizumab and the selective VEGFR-2 inhibitor rivoceranib (apatinib) demonstrated superiority over sorafenib in a phase 3 study with a prolonged mOS (22.1 months (95% CI 19.1–27.2) vs 15.2 (95% CI 13.0–18.5; HR 0.62)) and mPFS (5.6 months (95% CI 5.5–6.3) vs 3.7 (95% CI 2.8–3.7; HR 0.52)). However, serious treatment-related adverse events occurred more often under camrelizumab and rivoceranib compared to sorafenib (n=66 (24%) vs n=16 (6%)).27 A strict weighing of benefits and risks will be required before any approval is granted.
In COSMIC-312, a randomized phase 3 study, the combination of cabozantinib and atezolizumab showed a significantly prolonged median progression-free survival (mPFS) compared to sorafenib (6.8 months (99% CI 5.6–8.3) versus 4.2 months (99% CI 2.8–7.0; HR 0.63; p = 0.0012)).28 However, mOS did not significantly differ between the treatment groups in the interim analysis (15.4 months (96% CI 13.7–17.7) versus 15.5 months (12.1 – not estimable; HR 0.90; p = 0.44)). Further studies must be awaited to see if individual subgroups might benefit from therapy with cabozantinib and atezolizumab.
In addition, an evaluation of the response and safety of atezolizumab plus lenvatinib or sorafenib after progression under atezolizumab and bevacizumab in the first-line setting is currently being performed within the scope of IMbrave-251 (NCT04770896).
The LEAP-002 trial (NCT03713593) aimed at assessing efficacy and safety of lenvatinib plus pembrolizumab versus lenvatinib monotherapy in first-line setting. Primary endpoints mOS and mPFS were not met. However, a remarkably mOS was reached for both lenvatinib plus pembrolizumab and lenvatinib monotherapy (21.2 months (95% CI 19.0–23.6) vs 19.0 months (95% CI 17.2–21.7); HR 0.840; p = 0.0227).29
Resumption of Immune Checkpoint Inhibitors
Currently, data from prospective studies of consecutive ICI treatment in ICI-pretreated patients with HCC are lacking.30–32 An international retrospective multicenter trial assessed the efficacy and safety of ICI resumption. Patients showed similar objective response rates (ORR) while receiving therapy with the first and second ICI regimen (22% vs 26%), which were comparable to those published in phase 3 trials.12,13,18,33 Even in patients who manifested immune-related adverse events under the first ICI-based regimen, there was adequate safety under the second ICI regimen.33 This finding is consistent with current recommendations that ICI can be rechallenged after a convalescence period, depending on severity, with or without immunosuppressive treatment.34,35
Systemic Therapy in Combination with Locoregional Procedures
Transarterial Chemoembolization Plus Sorafenib
The TACTICS trial compared TACE plus sorafenib versus TACE alone.36 Tumor progression was defined as tumor growth into a stage that is not addressable by TACE anymore. Criteria for this were intrahepatic tumor progression >25% from baseline according to Response Evaluation Criteria in Cancer of the Liver (RECICL),37 transient CHILD-Pugh C situation after previous TACE, macrovascular invasion, or extrahepatic progression. New-onset intrahepatic lesions were not considered tumor progression as long as they continue to be treatable by TACE. In this study, the primary endpoint was met with a prolonged PFS in the TACE plus sorafenib group of 25.2 months versus 13.5 months in the TACE group. Analysis of overall survival showed no significant difference between the two groups with 36.2 months in the TACE plus sorafenib arm versus 30.8 months with TACE alone (HR 0.861; 95% CI 0.607–1.223; p = 0.40).38
In the SPACE trial, 307 patients received TACE with doxorubicin-eluting beads (DEB-TACE), and concomitant systemic treatment with sorafenib or placebo.39 The primary endpoint of the study with time to progression (TTP) showed no relevant difference between the two groups TACE plus placebo vs TACE plus sorafenib (166 days vs 169 days). As a secondary endpoint, in overall survival (OS) no statistical distinction was observed either.
Comparable results were reported for the TACE2 trial (n=313 randomized 1:1 in TACE plus sorafenib group and TACE plus placebo group), that did not provide evidence of improved outcome in TACE plus sorafenib group.
In SORAMIC trial, patients with BCLC B who were unable to receive TACE, were treated in the palliative cohort with SIRT plus sorafenib or sorafenib alone.40 Median OS in the SIRT plus sorafenib arm (12.1 months) did not differ significantly from mOS in the sorafenib arm (11.4 months; hazard ratio [HR] 1.01; 95% CI 0.81–1.25; p = 0.9529). Subgroup analyses of patients treated by protocol suggest potential benefits in patients with nonalcoholic cirrhosis or without cirrhosis, or in patients aged 65 years or younger. In the local ablation cohort of SORAMIC trial the benefit of adjuvant administration of sorafenib after local ablation on the primary endpoint time-to-recurrence (TTR) was investigated. See also chapter “Neoadjuvant and adjuvant systemic treatment”, page 12.
These heterogeneous results on the combination of sorafenib with TACE or SIRT indicate that further studies may be needed here, also considering the novel agents approved for HCC.
Transarterial Chemoembolization Plus Immune Checkpoint Inhibitors
Further studies are currently in progress to evaluate the efficacy and safety of supplementing TACE with systemic administration of ICI and anti-angiogenic drugs. In DEMAND trial A+B prior to or in combination with TACE is evaluated with regard to the primary end point 24-month survival rate and the secondary end points including objective response rate, progression-free survival, safety and quality of life (NCT04224636).
Both studies, EMERALD-1 and -3 compare a therapeutic regimen containing an antiangiogenic agent to a treatment regimen without an anti-angiogenic effect. After TACE, angiogenesis can be induced by hypoxia via VEGF, causing recurrence and progression. Thus, the biology of carcinogenesis suggests that the outcome of TACE may benefit from supplementation by antiangiogenic agents.41,42 Phase 3 trial EMERALD-3 compares the outcome of combining TACE with the STRIDE regimen with or without lenvatinib versus TACE alone (NCT05301842).
Phase 3 trial EMERALD-1 investigates efficacy and safety of TACE in combination with durvalumab monotherapy or durvalumab plus bevacizumab versus TACE alone (NCT03778957). The trial met the primary endpoint with a significantly prolonged mPFS in the cohort with durvalumab plus bevacizumab plus TACE compared to TACE alone (15.0 vs 8.2 months; HR 0.77; 95% CI 0.61–0.98; p = 0.032).43
In light of the significant increase in progression-free survival in intermediate stage HCC patients in the EMERALD-1 trial, the use of durvalumab after TACE might become a standard of care soon. However, in the case of approval of durvalumab plus bevacizumab plus TACE, data on subsequent immunotherapy-based therapy after progression under this regimen will be lacking.
Neoadjuvant and Adjuvant Systemic Treatment
HCC recurrence after curative resection or ablation occurs in 70–80%.3,44,45 In order to evaluate their effectiveness on recurrence free survival (RFS), neoadjuvant and adjuvant therapies were performed in the context of clinical trials: Sorafenib failed to demonstrate benefit in the neoadjuvant and adjuvant setting alone and in combination with conventional cytostatic agents.46,47 A+B was assessed for efficacy and safety in the adjuvant setting after resection or ablation of HCC at high risk for recurrence in a multinational, randomized (1:1 A+B adjuvant versus active surveillance), two-arm, open-label trial (IMbrave 050).3,48 The 668 patients enrolled either received adjuvant therapy with A+B lasting up to a maximum of 12 months or received active surveillance. The primary endpoint, independent review facility–assessed recurrence free survival (IRF-RFS), was met. Over a median follow-up of 17.4 months median IRF-RFS was not evaluable in both arms (95% CI 22.1 months – not evaluable vs 21.4 months – not evaluable; HR 0.72; p = 0.012).48 Treatment-related grade 5 adverse events occurred in 2 patients (0.6%) of the A + B cohort. Overall, the results imply that whether a patient can benefit from the adjuvant therapy with A + B depends primarily on the risk of HCC recurrence and the individual risk profile for side effects on A + B (eg gastrointestinal bleeding events or liver dysfunction). It is now important to wait for a longer follow-up of the RFS and OS in order to assess if the benefit of adjuvant therapy also persists over the period of application of A + B.
A+B is the subject of further research on perioperative administration:
Currently ongoing is DYNAMIC, a study investigating the efficacy of neoadjuvant A+B in patients with potentially resectable BCLC stage B/C or high risk resectable HCC (NCT04954339). In AB-LATE02 phase 2 trial, atezolizumab monotherapy before and A+B after radiofrequency ablation is currently being investigated for its effect on RFS (NCT04727307).
Perioperative nivolumab monotherapy and nivolumab plus ipilimumab have demonstrated adequate safety and feasibility in a single-center, randomized, open-label phase 2 trial.5 Of the 27 patients enrolled, thirteen were randomized to the nivolumab alone arm and fourteen to the combination arm, which received a single dose of ipilimumab neoadjuvant and ipilimumab every six weeks adjuvant in addition to nivolumab. Immunotherapy-related adverse events occurred more frequently in the combination cohort than in the nivolumab alone cohort. The benefit of therapy may also depend on the extent of pre-existing T-cell infiltrates.5 Valid biomarkers predicting adequate response to immuno-oncologic therapy are currently not sufficiently established.49
Phase 3 trial CA209-9DX investigates the impact of nivolumab on RFS administered after resection or ablation with high risk of recurrence (NCT03383458) and KEYNOTE-937 evaluates efficacy and safety of pembrolizumab versus placebo in an adjuvant setting (NCT03867084). First data on these phase 3 studies are expected later this year.
In the local ablation cohort of SORAMIC trial, patients were randomized 1:1 to local ablation + sorafenib versus local ablation + placebo.
The primary endpoint time-to-recurrence (TTR) showed no significant difference with a median TTR of 15.2 months in the local ablation + sorafenib arm versus 16.4 months in the local ablation + placebo arm,50 so that no benefit can be assumed for TTR by adjuvant administration of sorafenib currently.
Systemic Treatment in Intermediate Stage HCC
In intermediate stage, locoregional therapy with transarterial chemoembolization (TACE) is the standard of care so far.
The remarkable response rates of atezolizumab and bevacizumab raise the question of whether patients can be expected to benefit from therapy with atezolizumab and bevacizumab even with HCC at intermediate stage (BCLC B). Particularly in patients at high risk for recurrence after TACE (eg, large or multifocal bilobar HCC, high AFP), a potential benefit of systems therapy versus TACE needs to be reevaluated.
ABC-HCC (NCT04803994) is a phase 3b, randomized, multicenter trial comparing efficacy and safety of A+B versus TACE in intermediate stage HCC with high tumor burden exceeding the Milan criteria.
Systemic Treatment of HCC in Organ Transplant Recipients
By liver transplantation, hepatocellular carcinoma (HCC) can be treated curatively while simultaneously eliminating the usually underlying liver disease. Although organ allocation criteria consider factors that are suggestive of high risk for HCC recurrence, such as macroscopic vascular invasion, HCC recurrence after liver transplantation still occurs in 10% to 20%.51
HCC recurrence may be considered a systemic disease due to persistence of malignant cells after resection of the affected liver. Thus, HCC recurrence after liver transplantation often requires systemic therapy. Since ICIs have played a central role in the therapy of HCC, the question arises whether these therapeutic options can also be offered to organ transplant recipients. As patients with a previous organ transplant are usually excluded from clinical trials investigating ICI, there are scarce data on their application in transplant recipients.52
On the one side, simultaneous use of immunosuppressants reduces the effect of ICI. On the other side, there is an increased risk of rejection due to the mode of action, which is based on enhancement of an immune response. In particular, the PD1/PD-L1 pathway, which is inhibited by many ICI, contributes to the development of allograft tolerance.53
A summary of fourteen cases of liver transplant recipients treated with ICI (pembrolizumab, nivolumab or ipilimumab) shows that four of these patients (28.6%; three melanomas, one HCC) were responding to therapy. Four patients had graft rejection during therapy with PD1 inhibitor, three of those were fatal. The three patients treated with CTLA-4 inhibitor ipilimumab showed no rejection.54
While ICI have gained immense importance in the therapy of HCC, ICI should only be administered as ultima ratio in recurrent HCC after liver transplantation only in exceptional cases considering the risk of potentially fatal graft failure.
Conclusion
The increasing number of options in systemic therapy of HCC requires more complex clinical decisions with regard to the treatment sequence.
More and more ICIs are gaining approval for the treatment of HCC. Currently, there is no reliable and accessible biomarker that predicts response to ICI.49 Further research is certainly needed to identify a tumor microenvironment that is well addressable by ICI. It also remains to be investigated at what tumor stage the patient will benefit from switching to systemic therapy. The results of ABC-HCC may help us to define which patients with HCC at stage BCLC B should be initially treated with TACE and which should be initially treated with A+B.
A benefit for a combination of TACE with TKI could not be detected in the past 20 years. Final data on the combination of TACE with ICI are still pending. It remains to be seen whether additive or even synergistic effects can be demonstrated.
The results of studies examining the effectiveness of triple combination therapy (EMERALD-3: TACE ± Durvalumab/Tremelimumab ± Lenvatinib; LEAP-012: TACE ± Pembrolizumab ± Lenvatinib), may also be of interest in learning more about the limitations of liver function.
Regarding the use of A+B in adjuvant settings, more mature data are certainly to be awaited. Data of IMbrave 050 were read out very early. Indeed, there are indications that adjuvant application of A+B can prevent early recurrences. However, long-term RFS and especially long-term overall survival remain vague.3,55
A+B will remain the standard of care in the treatment of advanced HCC in the foreseeable future. STRIDE regimen is now available especially for patients with impaired liver function or high risk of bleeding events. As a consequence of the positive results of mainly Asian CARES-310 trial on the efficacy of camrelizumab + rivoceranib versus sorafenib, approval by the FDA was requested.
Lenvatinib will be the first choice if no ICI can be provided, eg for patients with poorly controlled autoimmune diseases or after organ transplantation. Subgroup analysis in IMbrave-150 has demonstrated inferiority in mOS for non-viral HCC compared to viral HCC12 and preclinical models provided indications for a reduced efficacy of ICI in NASH-HCC.56 However, for genesis to become a leading factor in treatment decisions, the current data are insufficient.57–59 Cabozantinib can be administered in second and third-line, ramucirumab can be used in second-line for patients with AFP ≥ 400 ng/mL.
Disclosure
Dr Christine Koch reports personal fees/grants from Astra Zeneca, MSD, and BMS; travel supports from Servier, Merck, and Ipsen, outside the submitted. Prof. Dr. Jörg Trojan reports personal fees from AstraZeneca, BMS, Ipsen, and Roche, during the conduct of the study. Prof. Dr. Fabian Finkelmeier reports personal fees from IPSEN, AstraZeneca, AbbVie, and MSD, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1). doi:10.1038/s41572-020-00240-3
2. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
3. Hack SP, Spahn J, Chen M, et al. IMbrave 050: a Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020;16(15):975–989. doi:10.2217/fon-2020-0162
4. Marron TU, Fiel MI, Hamon P, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):219–229. doi:10.1016/S2468-1253(21)00385-X
5. Kaseb AO, Hasanov E, Cao HST, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):208–218. doi:10.1016/S2468-1253(21)00427-1
6. Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734–1739. doi:10.1016/S0140-6736(02)08649-X
7. Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111(2):255–264. doi:10.1038/bjc.2014.199
8. Kulik L, Heimbach JK, Zaiem F, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta‐analysis. Hepatology. 2018;67(1):381–400. doi:10.1002/hep.29485
9. Yao FY, Mehta N, Flemming J, et al. Downstaging of hepatocellular cancer before liver transplant: long‐term outcome compared to tumors within Milan criteria. Hepatology. 2015;61(6):1968–1977. doi:10.1002/hep.27752
10. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008. doi:10.1056/NEJMoa0708857
11. Kudo M, Finn R, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018. doi:10.1016/S0140-6736(18)30207-1
12. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/nejmoa1915745
13. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
14. Himmelsbach V, Pinter M, Scheiner B, et al. Efficacy and safety of atezolizumab and bevacizumab in the real-world treatment of advanced hepatocellular carcinoma: experience from four tertiary centers. Cancers. 2022;14(7). doi:10.3390/cancers14071722
15. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
16. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/nejmoa1717002
17. Zhu A, Finn R, Galle P, et al. Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma (HCC) and elevated alpha-fetoprotein (AFP) following first-line sorafenib: pooled efficacy and safety across two global randomized Phase 3 studies (REACH-2 and REACH). Ann Oncol. 2018:
18. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1(8). doi:10.1056/evidoa2100070
19. Kudo M, Finn RS, Edeline J, et al. Updated efficacy and safety of KEYNOTE-224: a Phase II study of pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib. Eur J Cancer. 2022;167:1–12. doi:10.1016/j.ejca.2022.02.009
20. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
21. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2019;38:193–202. doi:10.1200/JCO.19
22. Qin S, Chen Z, Fang W, et al. Pembrolizumab versus placebo as second-line therapy in patients from Asia with advanced hepatocellular carcinoma: a randomized, double-blind, phase III trial. J Clin Oncol. 2022;41:1434–1443. doi:10.1200/JCO.22
23. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. 2020;6:e204564. doi:10.1001/jamaoncol.2020.4564
24. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
25. Qin S, Kudo M, Meyer T, et al. LBA36 Final analysis of RATIONALE-301: randomized, phase III study of tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Ann Oncol. 2022;33:S1402–S1403. doi:10.1016/j.annonc.2022.08.033
26. Qin S, Finn RS, Kudo M, et al. RATIONALE 301 study: tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Future Oncol. 2019;15(16):1811–1822. doi:10.2217/fon-2019-0097
27. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
28. Kelley RK, Rimassa L, Cheng AL, et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2022;23(8):995–1008. doi:10.1016/S1470-2045(22)00326-6
29. Finn RS, Kudo M, Merle P. LBA34 - Primary results from the phase III LEAP-002 study: lenvatinib plus pembrolizumab versus lenvatinib as first-line (1L) therapy for advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2022;33:S1401.
30. Ribas A, Puzanov I, Dummer R, et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. Lancet Oncol. 2015;16(8):908–918. doi:10.1016/S1470-2045(15)00083-2
31. Gul A, Stewart TF, Mantia CM, et al. Salvage ipilimumab and nivolumab in patients with metastatic renal cell carcinoma after prior immune checkpoint inhibitors. J clin oncol. 2020;38(27):3088–3094. doi:10.1200/JCO.19.03315
32. Ravi P, Mantia C, Su C, et al. Evaluation of the safety and efficacy of immunotherapy rechallenge in patients with renal cell carcinoma. JAMA Oncol. 2020;6(10):1606. doi:10.1001/jamaoncol.2020.2169
33. Scheiner B, Roessler D, Phen S, et al. Efficacy and safety of immune checkpoint inhibitor rechallenge in individuals with hepatocellular carcinoma. JHEP Rep. 2023;5(1):100620. doi:10.1016/j.jhepr.2022.100620
34. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J clin oncol. 2021;39(36):4073–4126. doi:10.1200/JCO.21.01440
35. Sangro B, Chan SL, Meyer T, Reig M, El-Khoueiry A, Galle PR. Diagnosis and management of toxicities of immune checkpoint inhibitors in hepatocellular carcinoma. J Hepatol. 2020;72(2):320–341. doi:10.1016/j.jhep.2019.10.021
36. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
37. Kudo M, Ikeda M, Ueshima K, et al. Response Evaluation Criteria in Cancer of the Liver version 5 (RECICL 2019 revised version). Hepatol Res. 2019;49(9):981–989. doi:10.1111/hepr.13394
38. Kudo M, Ueshima K, Ikeda M, et al. TACTICS: final overall survival (OS) data from a randomized, open label, multicenter, phase II trial of transcatheter arterial chemoembolization (TACE) therapy in combination with sorafenib as compared with TACE alone in patients (pts) with hepatocellular carcinoma (HCC). J clin oncol. 2021;39(3 suppl):270. doi:10.1200/JCO.2021.39.3
39. Lencioni R, Llovet JM, Han G, et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: the SPACE trial. J Hepatol. 2016;64(5):1090–1098. doi:10.1016/j.jhep.2016.01.012
40. Ricke J, Klümpen HJ, Amthauer H, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J Hepatol. 2019;71(6):1164–1174. doi:10.1016/j.jhep.2019.08.006
41. Shim JH, Park JW, Kim JH, et al. Association between increment of serum VEGF level and prognosis after transcatheter arterial chemoembolization in hepatocellular carcinoma patients. Cancer Sci. 2008. doi:10.1111/j.1349-7006.2008.00909.x
42. Kudo M. Implications of the TACTICS trial: establishing the new concept of combination/sequential systemic therapy and transarterial chemoembolization to achieve synergistic effects. Liver Cancer. 2022;11(6):487–496. doi:10.1159/000527404
43. Lencioni R, Kudo M, Erinjeri J, et al. EMERALD-1: A Phase 3, Randomized, Placebo-Controlled Study of Transarterial Chemoembolization Combined with Durvalumab with or Without Bevacizumab in Participants with Unresectable Hepatocellular Carcinoma Eligible for Embolization. American Society of Clinical Oncology; 2024. doi:10.1200/JCO.2024.42.3_suppl.LBA432
44. Saito A, Toyoda H, Kobayashi M, et al. Prediction of early recurrence of hepatocellular carcinoma after resection using digital pathology images assessed by machine learning. Mod Pathol. 2021;34(2):417–425. doi:10.1038/s41379-020-00671-z
45. Chen HY, Lu SN, Hung CH, et al. Predicting outcomes for recurrent hepatocellular carcinoma within Milan criteria after complete radiofrequency ablation. PLoS One. 2020;15(11):1–15. doi:10.1371/journal.pone.0242113
46. Williet N. Neoadjuvant sorafenib combined with gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma. World J Gastroenterol. 2011;17(17):2255. doi:10.3748/wjg.v17.i17.2255
47. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
48. Qin S, Chen M, Cheng AL, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402(10415):1835–1847. doi:10.1016/S0140-6736(23)01796-8
49. Macek Jilkova Z, Aspord C, Decaens T. Predictive factors for response to PD-1/PD-L1 checkpoint inhibition in the field of hepatocellular carcinoma: current status and challenges. Cancers. 2019;11(10):1554. doi:10.3390/cancers11101554
50. Seidensticker M, Öcal O, Schütte K, et al. Impact of adjuvant sorafenib treatment after local ablation for HCC in the phase II SORAMIC trial. JHEP Rep. 2023;5(5):100699. doi:10.1016/j.jhepr.2023.100699
51. Fernandez‐Sevilla E, Allard M, Selten J, et al. Recurrence of hepatocellular carcinoma after liver transplantation: is there a place for resection? Liver Transpl. 2017;23(4):440–447. doi:10.1002/lt.24742
52. Pinter M, Scheiner B, Peck-Radosavljevic M. Immunotherapy for advanced hepatocellular carcinoma: a focus on special subgroups. Gut. 2021;70(1):204–214. doi:10.1136/gutjnl-2020-321702
53. Riella LV, Paterson AM, Sharpe AH, Chandraker A. Role of the PD-1 pathway in the immune response. Am J Transplant. 2012;12(10):2575–2587. doi:10.1111/j.1600-6143.2012.04224.x
54. Munker S, De Toni EN. Use of checkpoint inhibitors in liver transplant recipients. United Eur Gastroenterol J. 2018;6(7):970–973. doi:10.1177/2050640618774631
55. Hoffmann-La Roche Ltd F. Media & investor release ad hoc announcement pursuant to art. 53 lr roche’s tecentriq plus avastin is the first treatment combination to reduce the risk of cancer returning in people with certain types of early-stage liver cancer in a phase III trial pivotal phase III IMbrave050 study investigating tecentriq plus avastin in people with early-stage Hepatocellular Carcinoma (HCC) at high risk of recurrence following surgery met primary endpoint of recurrence-free survival. Available from: www.roche.com.
56. Pfister D, Núñez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592:450. doi:10.1038/s41586-021-03362-0
57. Pinter M, Jain RK, Duda DG. The current landscape of immune checkpoint blockade in hepatocellular carcinoma. JAMA Oncol. 2021;7(1):113. doi:10.1001/jamaoncol.2020.3381
58. Pinter M, Pinato DJ, Ramadori P, Heikenwalder M. NASH and hepatocellular carcinoma: immunology and immunotherapy. Clin Cancer Res. 2023;29(3):513–520. doi:10.1158/1078-0432.CCR-21-1258
59. Kudo M. Lack of response to immunotherapy in non-alcoholic steatohepatitis related hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2021;10(4):522–525. doi:10.21037/hbsn-21-203
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.