")
Back to Journals » International Medical Case Reports Journal » Volume 17
Surgical Treatment of Chest Deformity in a Patient with Poland Syndrome. Clinical Case Report
Authors Kazbekov A , Bekarisov O, Tazhin K
Received 27 October 2023
Accepted for publication 7 March 2024
Published 27 March 2024 Volume 2024:17 Pages 247—252
DOI https://doi.org/10.2147/IMCRJ.S441944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Ablaikhan Kazbekov,1,2 Olzhas Bekarisov,1 Kairat Tazhin1
1National Scientific Center for Traumatology and Orthopedics Named After Academician N.D. Batpenov, Ministry of Health of the Republic of Kazakhstan, Astana, Kazakhstan; 2Astana Medical University, Astana, Kazakhstan
Correspondence: Ablaikhan Kazbekov, Email [email protected]
Introduction: Poland syndrome is a rare congenital syndrome that is characterized by partial or complete unilateral absence of the pectoralis major muscle, congenital malformation of the hand and deformation of the chest. Often the patients has abnormalities of the nipple-areolar complex. Here, we present a case of surgical treatment of local chest deformity with patient with Poland syndrome.
Case Presentation: We observed a patient, an 18-year-old man. The parents noticed the deformation of the chest from birth. The patient did not receive any treatment until adulthood. The patient contacted our clinical research center to correct chest deformity. After clinical and diagnostic procedures, the patient underwent surgical operation: open thoracoplasty with installation of a wire-frame construction. The early postoperative period was uneventful. Early postoperative outcome was assessed 6 months after surgery.
Conclusion: Our experience shows that thoracoplasty using a wire-frame construction is a good method for correcting local chest deformities in patients with Poland syndrome.
Keywords: Poland syndrome, chest deformity, surgery, case report
Introduction
Poland syndrome is a congenital syndrome characterized more often by one-sided (less often bilateral) hypoplasia (aplasia) large pectoral muscle and ribs (usually from 2 to 5), atelia, amastia, thinning of the subcutaneous fat layer of the chest, lack of hair growth in the axillary area and on the chest on the affected side, as well as congenital malformations of the upper limb (usually in the form of symbrachydactyly). The incidence of Poland syndrome is 1 case per 10–100 thousand people.1 The male sex prevails over the female sex in a ratio of 2–3: 1.2 Etiology and pathogenesis of Poland syndrome so far unknown for sure. Currently the generally accepted theory development of Poland syndrome is a disorder blood flow along the subclavian or vertebral arteries and their branches at the 6th week of intrauterine development. The severity of the syndrome manifestations determined by duration and intensity circulatory disorders in the data pool arteries.3
Case Presentation
An 18-year-old patient came to our clinical center for correction of local chest deformity. This patient’s chest deformity is congenital. The patient did not receive any treatment. When examining the chest, there is a complete absence of the pectoralis major muscle on the right, local retraction at the level of the 3rd and 4th intercostal spaces, incomplete development of the right nipple, and thinning of the subcutaneous fat layer of the skin (Figure 1).
 |
Figure 1 Patient’s appearance before operation. |
The patient is asthenic, height - 184 cm, weight - 59 kg. BMI - 17.4. After hospitalization, the patient underwent a computed tomography scan of the chest, which revealed local depression of the chest at the level of the third and fourth ribs and deformation of the cartilaginous parts of the ribs. After preoperative preparation, the patient underwent thoracoplasty with the installation of a wire-frame structure (Figure 2).
 |
Figure 2 CT of thorax before operation. |
The operation took place under intubation anesthesia. After processing the surgical field, an arcuate incision was made along the anterior wall of the chest from the level of the second rib on the right to the fifth intercostal space on the right. The skin is dissected, subcutaneous fat, periosteum and soft tissues are mobilized to the outer boundaries of the deformity. A defect in the third and fourth ribs on the right is visually noted. After skeletonizing the II to V rib on both sides to the outer boundaries of the deformation, the ends of the III and IV ribs were skinned. An autograft was taken from the cartilaginous part of the 5th rib. Then a frame structure is formed using Kirschner wires (Figure 3).
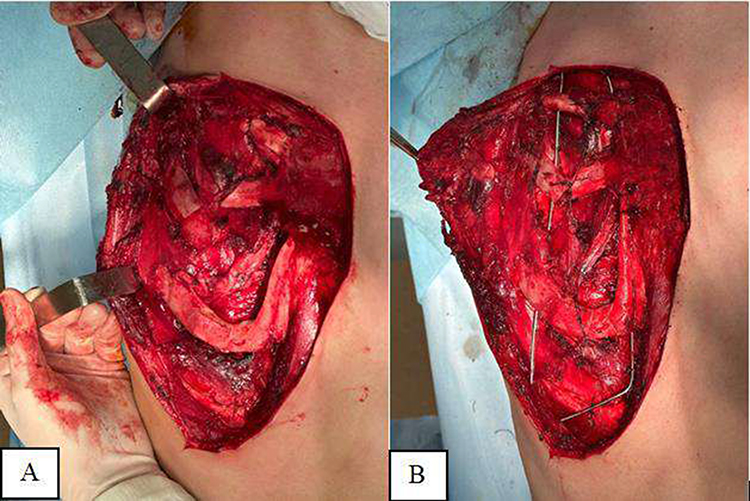 |
Figure 3 Intraoperative view. (A) View of right hemithorax after sketetalization of the deformed ribs; (B) Installed wire-frame construction. |
Additional costotomies of the third and fourth ribs on the right were also performed. The wound is washed and sutured tightly in layers, leaving a drainage tube. The operation time was 80 minute, intraoperative blood loss was 2000 mL. The next day after the operation, the patient was activated and rehabilitation measures were started (breathing exercises, inhalations). The drainage tube was removed on the second day after surgery. The patient was discharged 4 days after surgery. The sutures were removed 14 days after the operation. A follow-up examination of the patient was carried out 6 months after the operation. Clinical and tomographic results are satisfactory (Figures 4 and 5). Removal of metal structures is planned no earlier than 2 years after the operation. The purpose of our operational manual is to restore the frame structure of the cage. The second stage of surgical treatment is the replacement of the pectoralis major muscle defect with a silicone prosthesis. However, this operation is performed by aesthetic surgeons.
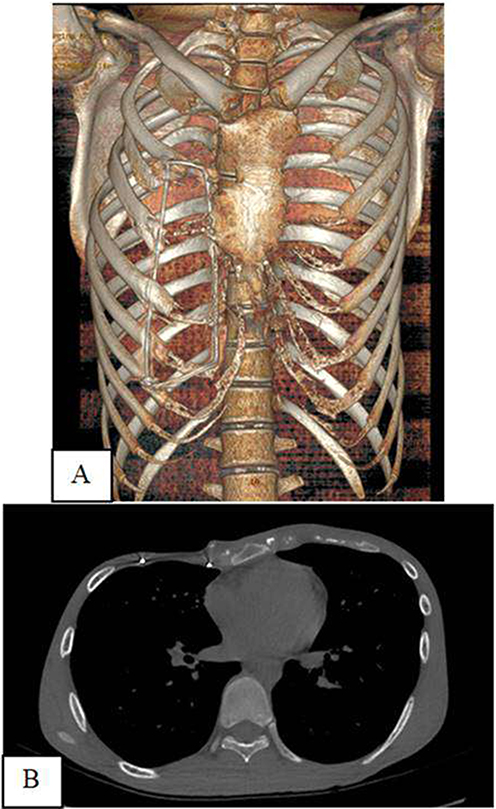 |
Figure 4 CT scans after operation: (A) 3D reconstruction; (B) Transversal section of thorax. |
 |
Figure 5 Patient’s appearance 6 months after operation. |
Discussion
The choice of treatment tactics for patients with Poland syndrome depends on the type of the deformity and the severity of the anatomical and functional state of the chest. If the defect is limited only to soft tissues, reconstructive interventions are performed only for aesthetic reasons. If there is a deformity or defect of the ribs and sternum, then surgical intervention is performed aimed at restoring the chest frame.4
Currently, there is no exact opinion at what age it is necessary to perform surgical interventions for deformities. Some authors believe that it is advisable to perform the operation after adolescence.5 Other authors believe that operations performed at an earlier age give better results.6,7
Surgical procedures used for chest deformities in patients with Poland syndrome can be divided into the following groups: 1. Restoration of chest contours (autotransplantation of skin-fat and muscle flaps; lipografting; injections of polymer polyacrylamide solution, prosthetics); 2. Reconstruction of the mammary gland (autotransplantation of skin-fat and muscle flaps; prosthetics; lipografting; formation of the nipple-areolar complex); 3. Restoration of the frame function of the chest (restoration of rib defects, elimination of lung hernia, as well as deformation of the sternum).
Today, in the world when reconstructing the pectoralis major muscle in patients with Poland syndrome, preference is given to transposition of the latissimus dorsi muscle (free and non-free version) in the position of the pectoralis major muscle.2
An alternative method for aesthetic correction of chest deformity in Poland syndrome is the use of silicone implants. G. Soccorso et al reported their experience in treating pectus excavatum in a child with Poland syndrome with a silicone implant, and the authors obtained a good cosmetic result.7
One of the methods of cosmetic correction of chest deformities is microinjection autotransplantation of adipose tissue, or lipografting. This is a procedure in which the patient’s fat tissue is removed from the thighs, abdomen, and buttocks using liposuction and injected into the area where it is needed. The main advantages of this method of correction are the absence of a rejection reaction, minimally invasiveness, and a minimal rehabilitation period.8 However, due to the resorption of adipose tissue, multiple interventions are required to obtain a satisfactory aesthetic result.9
In cases where patients have severe developmental anomalies of the sternum and ribs, causing functional or gross cosmetic disturbances, reconstructive operations are initially performed on the chest frame: thoracoplasty according to Ravich, its modification,5 replacement of defects with cartilaginous autografts, osteochondral allografts, artificial materials, modified thoracoplasty according to Nuss.6
Conclusion
Thus, our experience shows that thoracoplasty using a wire frame design is a good method for correcting local chest deformities in patients with Poland syndrome.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper, including publication of any accompanying images. Institutional approval was not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was conducted within the framework of the scientific and technical program of program-targeted financing by the Ministry of Health of the Republic of Kazakhstan (No. BR11065157).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yiyit N, Işıtmangil T, Öksüz S. Clinical analysis of 113 patients with Poland syndrome. Ann Thorac Surg. 2015;99(3):999–1004. doi:10.1016/j.athoracsur.2014.10.036
2. Papadopulos NA, Eder M, Stergioula S, et al. Women’s quality of life and surgical long-term outcome after breast reconstruction in Poland syndrome patients. Womens Health. 2011;20(5):749–756. doi:10.1089/jwh.2010.2211
3. Bavinck JNB, Weaver DD, Opitz JM, et al. Subclavian artery supply disruption sequence: hypothesis of a vascular etiology for Poland, Klippel-Feil, and Möbius anomalies. Am J Med Genet. 1986;23(4):903–918. doi:10.1002/ajmg.1320230405
4. De Palma A, Sollitto F, Loizzi D, et al. Chest wall stabilization and reconstruction: short and long-term results 5 years after the introduction of a new titanium plates system. J Thoracic Dis. 2016;8(3):490–498. doi:10.21037/jtd.2016.02.64
5. Baratte A, Bodin F, Del Pin D, et al. Poland’s syndrome in women: therapeutic indications according to the grade. Apropos of 11 cases and review of the literature. Ann Chir Plast Esthet. 2011;56(1):33–42. doi:10.1016/j.anplas.2010.10.016
6. Koizumi T, Mitsukawa N, Saiga A, et al. Clinical application of nuss procedure for chest wall deformity in Poland syndrome. Kardiochir Torakochirurgia Pol. 2014;4(4):421–423. doi:10.5114/kitp.2014.47343
7. Soccorso G, Anbarasan R, Singh M, et al. Management of large primary spontaneous pneumothorax in children: radiological guidance, surgical intervention and proposed guideline. Pediatr Surg Int. 2015;31(12):1139–1144. doi:10.1007/s00383-015-3787-8
8. Yang H, Lee H. Successful use of squeezed-fat grafts to correct a breast affected by Poland syndrome. Aesthetic Plast Surg. 2011;35(3):418–425. doi:10.1007/s00266-010-9601-z
9. Dionyssiou D, Demiri E, Batsis G, et al. Revision breast and chest wall reconstruction in Poland and pectus excavatum following implant complication using free deep inferior epigastric perforator flap. Indian J Plast Surg. 2015;48(1):85–88. doi:10.4103/0970-0358.155277
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.