")
Back to Journals » Integrated Pharmacy Research and Practice » Volume 11
Sudanese Medical Doctors’ Perceptions, Expectations, Experiences and Perceived Barriers Towards the Roles of Clinical Pharmacists: A Cross-Sectional Study
Authors Mahmoud MI , Maatoug MM, Jomaa AAAFA, Yousif M
Received 20 December 2021
Accepted for publication 13 July 2022
Published 18 July 2022 Volume 2022:11 Pages 97—106
DOI https://doi.org/10.2147/IPRP.S354717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jonathan Ling
Mohammed Ibrahim Mahmoud,1 Maha Mirghani Maatoug,1 Abd Alkareem Ahmed Fadal Allah Jomaa,2 Mirghani Yousif1
1Department of Clinical Pharmacy & Pharmacy Practice, University of Gezira, Wad Medani, Gezira State, Sudan; 2Department of Pharmacology, University of Gezira, Wad Medani, Gezira State, Sudan
Correspondence: Mohammed Ibrahim Mahmoud, Department of Clinical Pharmacy & Pharmacy Practice, Faculty of Pharmacy, 6 Jabra Ave, Al Khartoum, 11111, Sudan, Tel +249118208439, Fax +249183526178, Email [email protected]
Purpose: Interprofessional collaboration between physicians and clinical pharmacists has been shown to improve patients’ outcome by reduce medical errors, costs and patient adherence. Thus, the purpose of this study was to investigate the medical doctors’ perceptions, expectations, experiences, and perceived barriers regarding clinical pharmacists in Wad Medani.
Methods: A cross-sectional study was conducted at five major hospitals in Wad Medani, between April and June 2021 using a self-administered questionnaire. The questionnaire was distributed among 178 physicians. The questionnaire consists of four sections, in addition to a demographic section. These four sections measure physicians’ perceptions, expectations, experience, and perceived barriers.
Results: A total of 178 physicians were enrolled in the study. Physicians were comfortable with clinical pharmacists detecting and preventing prescription errors (55.1%); providing patient education (56.3%). Generally, physicians had high expectations with agreement rate of all the items ranged from 51.7% to 85.4%. Most physicians (79.8%) agreed that clinical pharmacists were a reliable source of general and clinical drug information. 64.0% and 59.0% of physicians perceive the unclear responsibility of clinical pharmacists and the lack of physicians’ experience with clinical pharmacists were barriers that can hinder clinical pharmacists’ contributions, respectively.
Conclusion: Physicians had positive perceptions, expectations, and experiences with clinical pharmacists, and pointed out some barriers clinical pharmacists face. It was suggested that hospitals should recruit more clinical pharmacists to cover each unit within the hospital with clear job description and provide them CPD.
Keywords: physicians, clinical pharmacists, perceptions, expectations, experiences, barriers
Introduction
Traditionally, it was known that physicians diagnose the disease and write the prescription, whereas the role of the pharmacists was limited to compounding and dispensing these prescriptions. However, since the emergence of the clinical pharmacy discipline in the 1960s, pharmacists have shifted from drug-centered orientation to patient-centered orientation.1–3 It was said that the reason for the emergence of clinical pharmacy discipline was that the pharmacists were displeased with their old practice and needed to professionally share in the healthcare field as unique experts in pharmacotherapy.4
The American College of Clinical Pharmacy (ACCP) is a professional and scientific society that provides leadership, education, advocacy, and resources enabling clinical pharmacists to achieve excellence in practice, research, and education. The ACCP, which contains over 15,000 members in more than 60 countries, defines Clinical Pharmacy as “a health science discipline in which pharmacists provide patient care that optimizes medication therapy and promotes health, wellness, and disease prevention”, and defines clinical pharmacists who
work directly with physicians, other health professionals, and patients to ensure that the medications prescribed for patients contribute to the best possible health outcomes. Clinical pharmacists practice in health care settings where they have frequent and regular interactions with physicians and other health professionals, contributing to better coordination of care.5
Clinical pharmacists are a primary source of scientifically valid information and advice regarding the safe, appropriate, and cost-effective use of medications.6 Also, they can offer complementary skills, knowledge and services to those that are provided by other health care professionals within a multidisciplinary team, specifically by preventing, identifying, or resolving drug-related problems; by ensuring the safe and efficacious use of medicines; by providing comprehensive drug information to patients and other health care professionals; and by promoting patient adherence to medications.7 Furthermore, several studies suggested that clinical pharmacists’ services reduce healthcare costs.8–10 Also, numerous studies had confirmed that clinical pharmacist’s interventions had a positive impact in cardiology, oncology, hematology, emergency, and pediatric departments.11–15
It was noted that integrating clinical pharmacists as part of the healthcare team is a viable solution for improving the quality of health care.16 A good collaboration between physicians and pharmacists is necessary to fully utilize pharmacists’ skills in managing drug therapy, and it has been shown to result in improved service delivery and enhanced patient outcomes.17,18
The perception of physicians towards clinical pharmacists or towards themselves has been studied extensively in the Arab region and across the world.17,19–28 Abdel-Latif had noted that in the Arab region, physicians’ acceptance of the clinical pharmacist’s role in clinical practice remains debatable.31 This may be due to the fact that the current roles of clinical pharmacists have not been clearly established and agreed.17
There are numerous factors that can impact clinical pharmacy services (CPS). One of which is, physicians’ attitude towards the clinical pharmacist that plays an important role either as a facilitator or detrimental when implementing CPS.32 Moreover, Penm and partners noted that the strongest facilitator for implementing CPS is the strong relationship with other health workers.33 This can explain why there is a lot of literature looking at this relationship. On the other hand, Penm and partners also mentioned some of the attitudes of physicians that have made the implementation of CPS challenging.33
In Sudan, clinical pharmacy discipline is still being considered as a relatively new specialization, where it was first introduced as an undergraduate pharmacy curriculum for the first time in 2001, and after a short time it was adopted in the post-graduate education programs in 2004 as a “2-year” Master’s degree at the University of Khartoum, and soon after, it had been opened in several pharmacy faculties as a higher education program.34
Since the start of the Master’s program at Gezira University, a number of hospitals in Wad Medani that set up CPS had been raised from one hospital to six hospitals: This implies that CPS is still new to Wad Medani. To the best of our knowledge, this is the first and may be the only study to be conducted in Wad Medani in order to evaluate the physicians’ perception of the roles of clinical pharmacists, and their interactions, and what they expect from them, and their opinion on the barriers hindering clinical pharmacists’ contributions.
Materials and Methods
Study Design and Settings
This study was a descriptive observational cross-sectional survey. It was conducted between April and June 2021.
The study was conducted in five major public hospitals in Gezira State, locality of Wad Medani. The hospitals were Wad Medani Hospital for Heart Diseases (WMHHD), Wad Medani Teaching Hospital (WMTH), National Cancer Institute (NCI), Wad Madani Paediatric Teaching Hospital (WMPTH), and Gezira Hospital for Renal Disease and Surgery (GHRDS). WMTH and WMPTH are teaching hospitals, and the WMHHD, NCI, GHRDS are specialized hospitals.
Each hospital has ward-based clinical pharmacists which go with the physicians in round. Only WMTH contains a Drug Information Centre (DIC) which is run by clinical pharmacists where physicians can get information about the drugs either in person or by phone.
Study Population and Sampling Technique
The total number of physicians in these hospitals was 328. A sample size of 178 was calculated using Raosoft®.35 The sample distribution of the five hospitals was as follows: WMHHD (n = 30), WMTH (n = 82), NCI (n = 17), WMPTH (n = 30), and GHRDS (n = 19). The total number of physicians in the five hospitals was as follows: WMHHD (n = 55), WMTH (n = 150), NCI (n = 31), WMPTH (n = 55), and GHRDS (n = 34). All the physicians in these five hospitals were included except some physicians who worked in WMTH and GHRDS, in particularly surgery and ear-nose-throat departments’ physicians, because the CPS are not available to them. The data were collected via convenience sampling.
Study Instrument
The questionnaire consists of five sections in addition to an introductory letter: section one describes the participants’ demographic profiles such as their gender, age, the country where qualification was obtained, hospital where they work in, current area of practice, current position, the frequency of interacting with pharmacists and a description of the reason(s) of this interaction. Section two measured the perceptions of physicians by using the level-of-comfort. Sections three, four, and five assessed physicians’ expectations, experiences, and perceived barriers towards the role of clinical pharmacists, respectively. Sections two, three, four, and five consist of eight items.
The perception, expectation, and experience domains were adopted from a study conducted in Sudan by Awad et al adaptation which has been validated by Smith et al in California.36,37 The perceived barriers domain and was adopted from Almazrou et al which has been reviewed by peers and experts.36 A pilot test was done with ten physicians to assess the clarity of the questionnaire.
Data Collection
The self-administered questionnaires were delivered directly to the physicians, and the data collector waited for the physician to fill them out to avoid mistakes. Due to the nature of their hard work, some questionnaires were left with the physicians and collected at a later date, which might result in some missing responses. There was an introductory letter explaining the purpose of the study and providing anonymity to participants. The questionnaires were distributed on different working days of the week to available physicians on these days. When each physician was identified, the data collector approached and asked them to participate after explaining the purpose of the study, and then explained the instructions for filling out the questionnaire.
Ethical Considerations
Ethical approval and verbal informed consent were obtained from the Health Research Ethical Committee of the University of Gezira, Wad Medani on 1/4/2021 (reference number: 25–21). Approval was obtained from the Gezira State’s Ministry of Health and each respective hospital to conduct the study prior to the data collection. Verbal consent was obtained before handing over the questionnaire.
Statistical Analysis
The data were entered into Excel sheet, coded, cleaned up, and then entered into SPSS version 26.0 (SPSS, Chicago, IL, USA) for analysis. The level-of-comfort was coded: 1 for uncomfortable, 2 for moderately uncomfortable, and 3 for comfortable. The expectations, experiences and perceived barriers were coded: 1 for strongly disagree to 5 strongly agree. To present the results more clearly, the “strongly agree” and “agree” responses were merged to “overall agree” and likewise for “strongly disagree” and “disagree” to “overall disagree”. The final coding was 1 “overall disagree”, 2 “neutral”, 3 “overall agree”. Frequency values were calculated.
Results
A total of 178 physicians were enrolled in this study (100% response rate). The majority of the physicians were female (60.1%). More than half of the respondents (55.6%) were in the range of 26–30 years old. Nearly all of the participants (98.9%) had received their medical qualification in Sudan. Most of physicians (47.2%) were medical staff members at WMTH. The most prominent area of practice was internal medicine, representing 66.9% of the sample. About two-thirds of the physicians were either medical-officers (32.6%); or registrars (34.8%). More than three-quarters of the enrolled participants (77.5%) had five or less years of experience (Table 1). Nearly half of the physicians either had never (10.7%) or rarely (41.0%) interacted with clinical pharmacists. The reasons of interactions with clinical pharmacists were drug-availability enquiries (53.5%); drug-alternative enquiries (46.5%); drug-dosage enquiries (58.6%); and drug-interaction enquiries (54.8%) (Table 2). Participants were most comfortable with clinical pharmacists providing patient education (55.1%); detecting and preventing prescription errors (55.1%) (Table 3). Generally, physicians had high expectation, with majority of physicians expect clinical pharmacists to: educate patients about the rational use of their medications (83.7%); to be knowledgeable experts regarding drug-therapy (85.4%); and to be available for consultation when they see patients (80.3%) (Table 4). Regarding physicians’ experience with clinical pharmacists, the majority of physicians agreed that clinical pharmacists: are a reliable source of general drug information (79.8%); are a reliable source of clinical drug information (79.8%); and routinely inform them if they detect clinical problems with their prescriptions (72.5%) (Table 5). The majority of physicians confirmed that there were some barriers hindering clinical pharmacists’ contributions and the highest were as follows: the specific responsibilities of a clinical pharmacist were not clearly defined (64.0%); physicians have no prior experience of working with a clinical pharmacist (59.0%); physicians were unaware of the benefits of having a clinical pharmacist on their team (58.4%). On the other hand, physicians do not believe that the involvement of clinical pharmacists in other tasks interrupts the continuity of patient care (53.6%); physicians have a low level of trust in the clinical pharmacist’s abilities (50.0%) were not hindering clinical pharmacists’ contributions (Table 6).
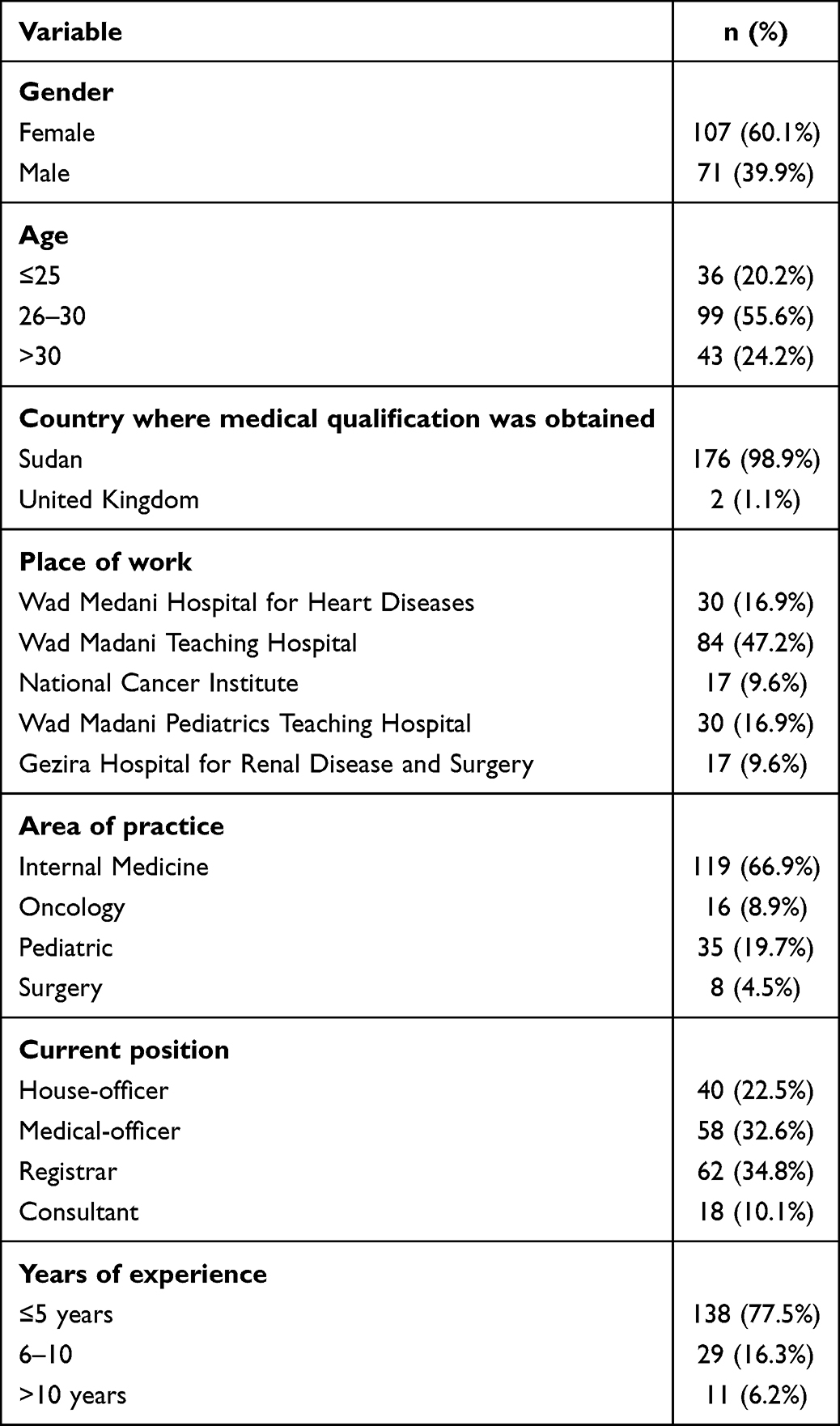 |
Table 1 Physicians’ Demographics and Relevant Characteristics (n = 178) |
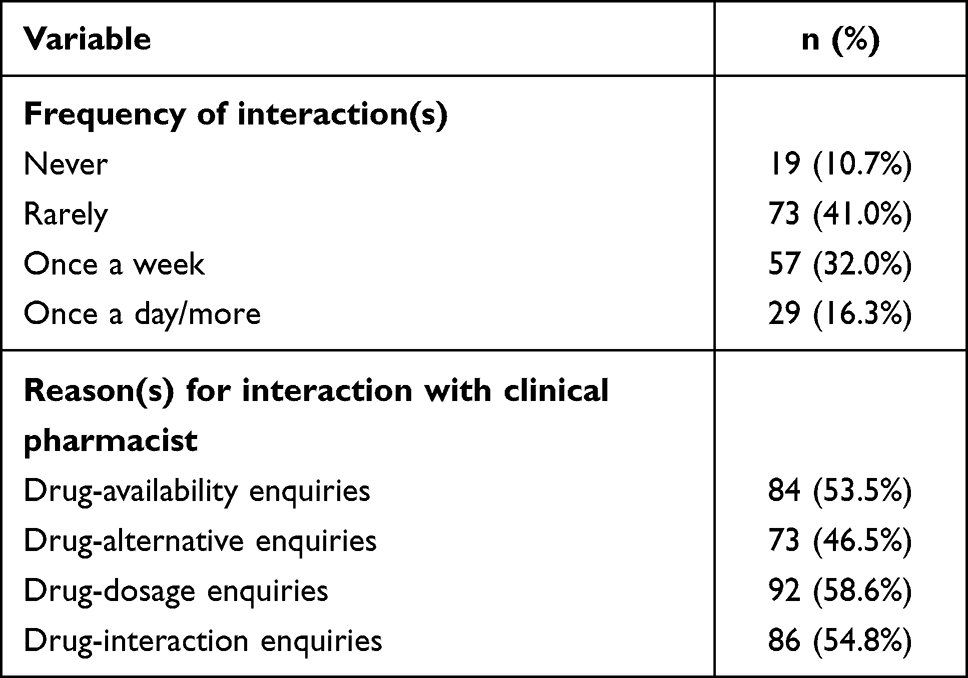 |
Table 2 The Reported Frequencies of Physicians’ Interactions with Clinical Pharmacists and Their Reasons (n = 178) |
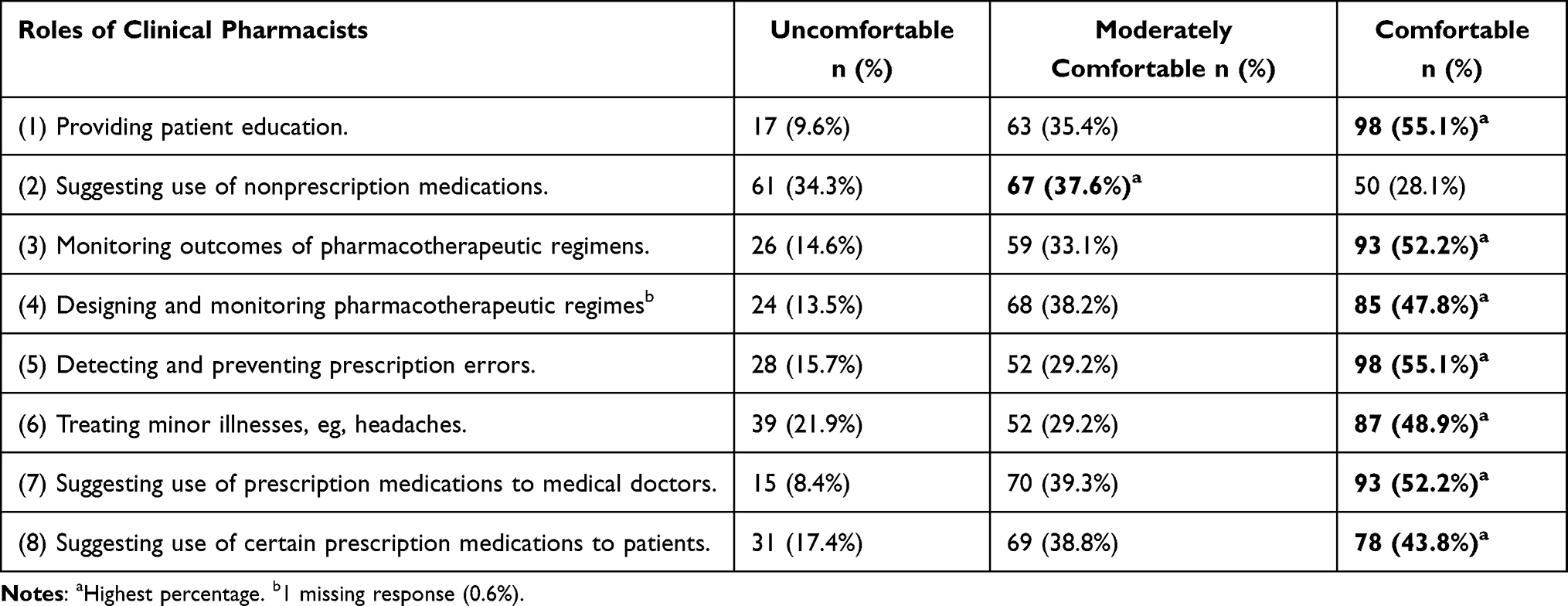 |
Table 3 Perceptions of Physicians Towards the Roles of Clinical Pharmacists (n = 178) |
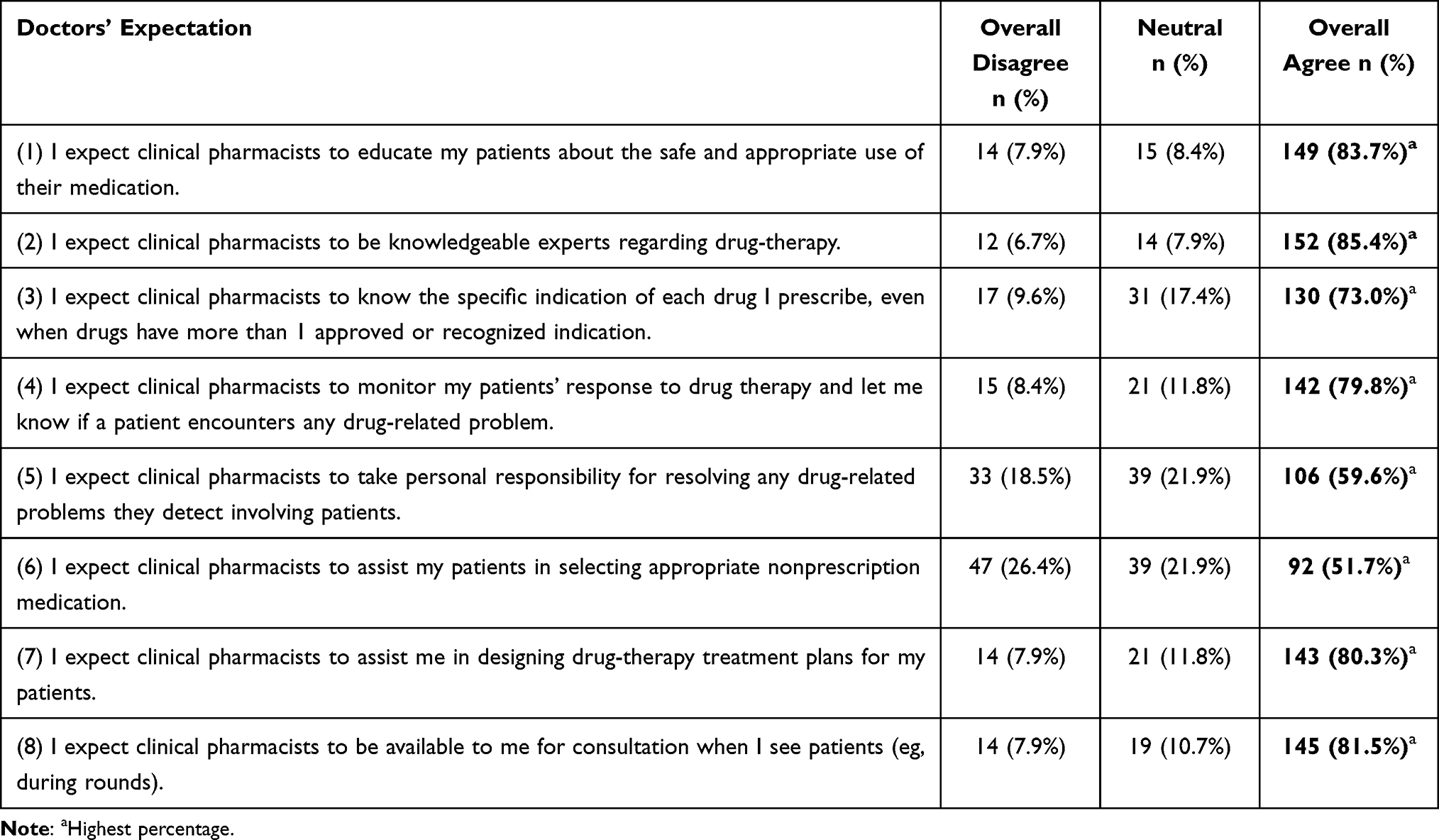 |
Table 4 Physicians’ Expectation of Clinical Pharmacists (n = 178) |
 |
Table 5 Physicians’ Actual Experiences with Clinical Pharmacists (n = 178) |
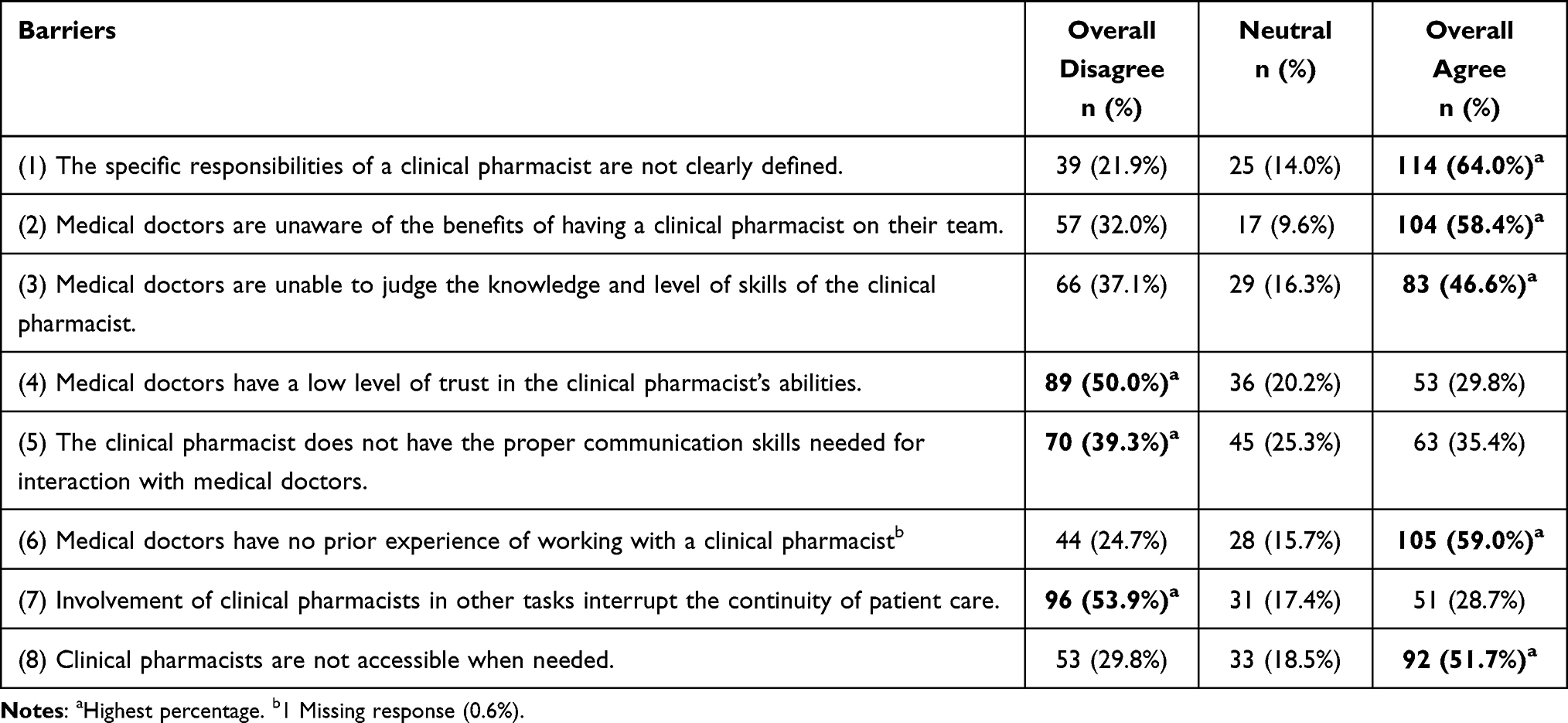 |
Table 6 Physicians’ Perceived Barriers That Can Hinder Clinical Pharmacists’ Contributions (n = 178) |
Discussion
One of the main factors affecting the implementation of CPS in the medical teams of the local hospitals is the nature of relationship between physicians and clinical pharmacists, and that good physicians’ attitude is the most important and strongest facilitator regarding the implementation of CPS in hospitals.33 Nevertheless, the CPS are relatively new to Wad Medani hospitals. Therefore, the purpose of the current study was to investigate the physicians’ perceptions, expectations, experiences, and perceived barriers with clinical pharmacists. By using a questionnaire that measures physicians’ perceptions, expectations, experiences, and perceived barriers towards the role of clinical pharmacists; the study found that physicians were quite convenient with some roles of clinical pharmacists and had high expectations and had good experience with clinical pharmacists. Also, physicians reported some barriers that can hinder clinical pharmacists’ contribution.
The perception was measured using level-of-comfort regarding the roles of clinical pharmacists. Slightly more than half of the physicians were comfortable with clinical pharmacists providing patient education, detecting and preventing prescription errors, and monitoring outcomes of pharmacotherapeutic regimens. These findings agree with observations elsewhere.29,30 These positive perceptions towards the roles of clinical pharmacists might indicate that clinical pharmacists can perform their established roles such as detecting and preventing prescription errors and some of the extended roles such as providing patient education activities with the support of physicians.
The majority of physicians had relatively high expectations towards clinical pharmacist with an overall statement of more than 50% rate of agreement. These findings are similar to studies done in several countries.27,29,37 This high expectation regarding clinical pharmacists educating patients about the safe and appropriate use of their medications was aligned with the positive perception of the role of clinical pharmacists in providing patients education. Clinical pharmacists must meet these high expectations. Although, clinical pharmacists do seek to improve their level of practice, they are faced with many obstacles and they need to overcome them, such as lack of Continuous Professional Development (CPD), and lack of clinical pharmacist staff which make it harder for them to get a spare time for the CPD.38
Physicians had good experience in nearly all the statements and reported that clinical pharmacists are reliable sources of both clinical and general drug information. The finding is observed elsewhere.30 This is in consensus with physicians who reported high expectation with clinical pharmacists’ being knowledgeable drug experts in this study. Half of the physicians in the current sample have reported that they never or rarely interact with clinical pharmacists, and yet we see high level of experiences with clinical pharmacists, which may indicate a contradiction. It is unclear why this contradiction exists, but it could be as a result of the DIC activities of clinical pharmacists that physicians may perceive it as an experience.
Physicians reported that the specific responsibilities of a clinical pharmacist are not clearly defined, and physicians have no previous experience of working with a clinical pharmacist, also physicians were unaware of the benefits of having a clinical pharmacist in their team are barriers hindering clinical pharmacists’ contributions. Similar finding was also reported in Saudi Arabia.34 Salim et al noted that clinical pharmacists in Khartoum reported that they lack a clear job description. Both clinical pharmacists and physicians agree with these results.24 The low frequency of interactions may explain why: physicians believe that physicians have no previous experience working with a clinical pharmacist; physicians were unaware of the benefits of having a clinical pharmacist in their team; and clinical pharmacists are not accessible when needed. These might reflect the inadequacy of hiring clinical pharmacists in hospitals. The high level of disagreement with “physicians have a low level of trust in the clinical pharmacist’s abilities” and “Involvement of clinical pharmacists in other tasks interrupts the continuity of patient care” can be explained by the good experiences physicians had with clinical pharmacists.
This study’s findings suggest that physicians in Wad Medani can support clinical pharmacists in performing their established and extended roles as seen by the positive perception and the high expectations and experience toward clinical pharmacists. Also, physicians had reported some challenges that can hinder clinical pharmacists’ contributions. Overcoming these challenges may require making clinical pharmacists available to physicians by increasing the working clinical pharmacists in the hospitals and providing them a clear job description.
Limitations
Generally, the study had faced two limitations. First, the findings cannot be generalized due to the study design of choosing the participants. Second, the number of the enrolled participants in this study did not necessarily reflect the full picture, since most of the targeted hospitals have an outdated or inaccurate employment list and even that some physicians do not attend to the hospitals even if they were listed in the employment list.
Conclusion
This study showed that most physicians were quite comfortable towards the roles of clinical pharmacists and reflected their high expectations and good experiences in collaboration with clinical pharmacists. It had also shown some of the perceived physicians’ barriers that can hinder clinical pharmacists’ contributions in Wad Medani hospitals. It was suggested that hospitals should recruit more clinical pharmacists in the hospital with clear job description and provide them CPD. Future research should focus on the impact of clinical pharmacists in Sudan.
Abbreviations
CPS, clinical pharmacy services; WMHHD, Wad Medani Hospital for Heart Diseases; WMTH, Wad Medani Teaching Hospital; NCI, National Cancer Institute; WMPTH, Wad Madani Paediatric Teaching Hospital; GHRDS, Gezira Hospital for Renal Disease and Surgery; CPD, Continuous Professional Development.
Acknowledgments
The authors would like to thank all the physicians who participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Miller RR. History of clinical pharmacy and clinical pharmacology. J Clin Pharmacol. 1981;21(4):195–197. doi:10.1002/j.1552-4604.1981.tb05699.x
2. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Health Syst Pharm. 1990;47(3):533–543. doi:10.1093/ajhp/47.3.533
3. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166(9):955–964. doi:10.1001/archinte.166.9.955
4. Ibrahim OM, Ibrahim R. Perception of physicians to the role of clinical pharmacists in United Arab Emirates (UAE). Pharmacol Pharm. 2014;5(9):895–902. doi:10.4236/pp.2014.59100
5. American College of Clinical Pharmacy. About American College of Clinical Pharmacy; 2008.
6. Sabry NA, Farid SF. The role of clinical pharmacists as perceived by Egyptian physicians. Int J Pharm Pract. 2014;22(5):354–359. doi:10.1111/ijpp.12087
7. Eltorki Y, Abdallah O, Omar N, Zolezzi M. Perceptions and expectations of health care providers towards clinical pharmacy services in a mental health hospital in Qatar. Asian J Psychiatr. 2019;42:62–66. doi:10.1016/j.ajp.2019.03.018
8. Han JM, Ah YM, Suh SY, et al. Clinical and economic impact of pharmacists’ intervention in a large volume chemotherapy preparation unit. Int J Clin Pharm. 2016;38(5):1124–1132. doi:10.1007/s11096-016-0339-9
9. Morgan SR, Acquisto NM, Coralic Z, et al. Clinical pharmacy services in the emergency department. Am J Emerg Med. 2018;36(10):1727–1732. doi:10.1016/j.ajem.2018.01.056
10. Dalton K, Byrne S. Role of the pharmacist in reducing healthcare costs: current insights. Integr Pharm Res Pract. 2017;6:37–46. doi:10.2147/IPRP.S108047
11. Farmer BM, Hayes BD, Rao R, Farrell N, Nelson L. The role of clinical pharmacists in the emergency department. J Med Toxicol. 2018;14(1):114–116. doi:10.1007/s13181-017-0634-4
12. Dunn SP, Birtcher KK, Beavers CJ, et al. The role of the clinical pharmacist in the care of patients with cardiovascular disease. J Am Coll Cardiol. 2015;66(19):2129–2139. doi:10.1016/j.jacc.2015.09.025
13. Naseralallah LM, Hussain TA, Jaam M, Pawluk SA. Impact of pharmacist interventions on medication errors in hospitalized pediatric patients: a systematic review and meta-analysis. Int J Clin Pharm. 2020;42(4):979–994. doi:10.1007/s11096-020-01034-z
14. de Grégori J, Pistre P, Boutet M, et al. Clinical and economic impact of pharmacist interventions in an ambulatory hematology–oncology department. J Oncol Pharm Pract. 2020;26(5):1172–1179. doi:10.1177/1078155220915763
15. Gatwood J, Gatwood K, Gabre E, Alexander M. Impact of clinical pharmacists in outpatient oncology practices: a review. Am J Health Syst Pharm. 2017;74(19):1549–1557. doi:10.2146/ajhp160475
16. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists’ effect as team members on patient care: systematic review and meta-analyses. Med Care. 2010;48(10):923–933. doi:10.1097/MLR.0b013e3181e57962
17. Lo U, Hu H, Ung C. Physicians’ and pharmacists’ experience and expectations of the roles of pharmacists: insights into hospital setting in Macau. Trop J Pharm Res. 2014;12(6):1077. doi:10.4314/tjpr.v12i6.32
18. Mubarak N, Hatah EM, Khan TM, Zin CS. A systematic review and meta-analysis of the impact of collaborative practice between community pharmacist and general practitioner on asthma management. J Asthma Allergy. 2019;12:109–153. doi:10.2147/JAA.S202183
19. Al-Arifi M, Alghamdi B, Al-Saadi M, et al. Attitudes and perceptions of healthcare providers towards clinical pharmacy services at a tertiary care hospital in Riyadh, Saudi Arabia. Trop J Pharm Res. 2015;14(5):913. doi:10.4314/tjpr.v14i5.23
20. Abu-Gharbieh E, Fahmy S, Rasool BA, Abduelkarem A, Basheti I. Attitudes and perceptions of healthcare providers and medical students towards clinical pharmacy services in United Arab Emirates. Trop J Pharm Res. 2010;9(5):421–430. doi:10.4314/tjpr.v9i5.61050
21. Kabel AM, Bakr MM, Alshanbari AM, et al. Perceptions and attitudes towards clinical pharmacy services and their impact on the management of cancer in Taif, Saudi Arabia. Asian Pac J Cancer Prev. 2020;21(2):531–538. doi:10.31557/APJCP.2020.21.2.531
22. Mekonnen AB, Yesuf EA, Odegard PS, Wega SS. Pharmacists’ journey to clinical pharmacy practice in Ethiopia: key informants’ perspective. SAGE Open Med. 2013;4(2):571–574. doi:10.1177/2050312113502959
23. Khan N, McGarry K, Naqvi AA, Holden K. Doctors’ perceptions, expectations and experience regarding the role of pharmacist in hospital settings of Pakistan. Int J Clin Pharm. 2020;42(2):549–566. doi:10.1007/s11096-020-00991-9
24. Salim AA, Elhada AA, Elgizoli B. Exploring clinical pharmacists’ perception of their impact on healthcare in Khartoum State, Sudan. J Res Pharm Pract. 2016;5(4):272. doi:10.4103/2279-042x.192459
25. Tahaineh L, Wazaify M, Alomoush F, Nasser SA, Alrawashdh N, Abraham I. Physicians’ perceptions, expectations, and experiences of clinical pharmacists in Jordan-2017. Int J Clin Pharm. 2019;41(5):1193–1201. doi:10.1007/s11096-019-00884-6
26. Alsuhebany N, Alfehaid L, Almodaimegh H, Albekairy A, Alharbi S. Attitude and perception of physicians and nurses toward the role of clinical pharmacists in Riyadh, Saudi Arabia: a qualitative study. SAGE Open Nurs. 2019;5:1–8. doi:10.1177/2377960819889769
27. Omar NE, Elazzazy S, Abdallah O, et al. Perceptions and expectations of health care providers towards clinical pharmacy services at a tertiary cancer centre in Qatar. J Oncol Pharm Pract. 2020;26(5):1086–1096. doi:10.1177/1078155219882076
28. Zaidan M, Singh R, Wazaify M, Tahaineh L. Physicians’ perceptions, expectations, and experience with pharmacists at Hamad Medical Corporation in Qatar. J Multidiscip Healthc. 2011;4:85–90. doi:10.2147/JMDH.S14326
29. Alipour F, Peiravian F, Mehralian G. Perceptions, experiences and expectations of physicians regarding the role of pharmacists in low-income and middle-income countries: the case of Tehran hospital settings. BMJ Open. 2018;8(2):e019237. doi:10.1136/bmjopen-2017-019237
30. Khdour MR, Alayasa KS, Alshahed QN, Hawwa AF. Physicians’ perceptions, attitudes and expectations regarding the role of hospital-based pharmacists in the West Bank, Palestine. Int J Pharm Pract. 2013;21(3):178–184. doi:10.1111/j.2042-7174.2012.00246.x
31. Abdel-Latif MMM. Hospital doctors’ views of, collaborations with and expectations of clinical pharmacists. Eur J Hosp Pharm. 2017;24(6):343–348. doi:10.1136/ejhpharm-2016-001075
32. Trinh HT, Nguyen HTL, Pham VTT, et al. Hospital clinical pharmacy services in Vietnam. Int J Clin Pharm. 2018;40(5):1144–1153. doi:10.1007/s11096-018-0633-9
33. Penm J, Moles R, Wang H, Li Y, Chaar B. Factors affecting the implementation of clinical pharmacy services in China. Qual Health Res. 2014;24(3):345–356. doi:10.1177/1049732314523680
34. Mohamed SSE. Current state of pharmacy education in the Sudan. Am J Pharm Educ. 2011;75(4):65a. doi:10.5688/ajpe75465a
35. Raosoft®. Raosoft sample size calculator; 2004. Available from: http://www.raosoft.com/samplesize.html.
36. Almazrou S, Alnaim L, Al-Kofide H. Perceptions, expectations and barriers of physicians towards working with clinical pharmacists in Saudi Arabia. J Sci Res Rep. 2015;6(5):404–415. doi:10.9734/jsrr/2015/11637
37. Awad A, Matowe L, Capps P. Medical doctors’ perceptions and expectations of the role of hospital pharmacists in Sudan. Pharm World Sci. 2007;29(5):557–564. doi:10.1007/s11096-007-9111-5
38. Elsadig H, Weiss M, Scott J, Laaksonen R. Exploring the challenges for clinical pharmacists in Sudan. Int J Clin Pharm. 2017;39(5):1047–1054. doi:10.1007/s11096-017-0521-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.