")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Stimulating Students’ Interprofessional Teamwork Skills Through Community-Based Education: A Mixed Methods Evaluation
Authors Lestari E , Scherpbier A , Stalmeijer R
Received 14 June 2020
Accepted for publication 24 September 2020
Published 13 October 2020 Volume 2020:13 Pages 1143—1155
DOI https://doi.org/10.2147/JMDH.S267732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Endang Lestari,1 Albert Scherpbier,2 Renee Stalmeijer2
1Medical and Health Professions Education Unit, Faculty of Medicine, Universitas Islam Sultan Agung, Semarang, Indonesia; 2School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, the Netherlands
Correspondence: Endang Lestari Email [email protected]
Background: Interprofessional education (IPE) is suggested as a good means to prepare future healthcare professionals for collaborative work in interprofessional teams enabling them to solve complex health problems. Previous studies have advocated experiential IPE, including community-based IPE (CBIPE). This study aims to evaluate a CBIPE programme by exploring the students’ perception toward CBIPE design and toward groups’ teamwork.
Methods: To identify students’ perceptions of teamwork, the Interprofessional Teamwork Evaluation questionnaire was administered to 254 students of medical, nursing and midwifery programme. Three uni-professional focus group (FG) discussions were conducted to analyse the students’ perception of the design of community-based education and underlying reasons for teamwork.
Results: FGs reported three aspects that influence skills development in collaborative practice among students that shed light on why midwifery and nursing students held less positive perceptions of communication and mutual support: 1) communication gap due to lack of confidence, 2) contrasting ways of thinking affect communication in decision-making, and 3) the leadership culture in the health services.
Conclusion: A CBIPE programme was successfully implemented at Universitas Islam Sultan Agung. It demonstrated that students in the health professions can develop skills in collaborative practice despite having some problems with communication and mutual support.
Keywords: community-based interprofessional education, interprofessional education, interprofessional timework evaluation
Introduction
The increasing complexity of healthcare issues demands collaboration between various healthcare professions.1–3 However, it has been demonstrated that conducting collaborative care is not always self-evident and sometimes negatively influences patient safety and efforts to prevent health problems in the community.4–8
To better prepare future healthcare professionals for collaborative work in interprofessional teams, implementation of interprofessional education (IPE) in health professions education has been suggested.9,10 IPE in health care takes place when two or more healthcare professions learn about, from, and with each other with collaboration and improved health outcome as the end objectives.11
Future collaboration can be further enhanced by providing healthcare students from various professions with opportunities to actively learn and interact together.12 However, IPE formats situated in the classroom alone seem not always sufficient to develop some of the skills needed for collaborative health care.13–15 Consequently, the scope of IPE initiatives needs to be broadened.16 Several authors advocate for experiential IPE situated in practice-based settings.17–19
Community-based education (CBE) is suggested as a model for facilitating IPE in collaborative skills in the workplace.20–22 CBE is defined as learning activities that use the community extensively as a learning environment, in which not only students but also teachers, members of the community, and representatives of other sectors are actively engaged throughout the educational experience.23 Community-based IPE (CBIPE) is the process by which a group of two or more students from different health-related occupations with different educational backgrounds learn together while utilising the community as a learning environment, with collaboration and interaction as part of their learning goals.24 CBIPE students learn in the context of the community itself and are expected to work collaboratively in interprofessional teams to provide an expected health service despite limited resources.21 CBIPE programmes may also produce the added benefit of exposing students to concepts that might not be accounted for, or explicitly taught, in all health profession curricula, especially those dealing with family medicine, primary care, social determinants of health and cultural competence.25,26 Moreover, CBIPE helps stimulate social accountability in health profession students.27 Various approaches to CBIPE have been previously reported such as learning in rural and primary healthcare settings,24,28,29 community-based learning within broader community context16,22,30 and for specific community context; the commonly used model of CBIPE in the western countries.21,31–35 The nature of interprofessional learning activities is mainly to provide healthcare services primary healthcare setting, not in the community. Examples of CBIPE in specific community contexts have often been limited to specific settings like senior housing32 or child healthcare.34 To enable students to acquire comprehensive skills ranging from diagnosing health problems in the community, to formulating and implementing the problem-solving activities,20,22 designing a CBIPE program providing those learning opportunities needed to be designed.
Although CBIPE programmes have been implemented globally, there seem to be few reports on the implementation itself and result of these programmes in Asian contexts.21,24,36,37 Understanding the transferability of CBIPE in an Asian context might be especially important given the great need for interprofessional collaboration in this region.38 As most Asian countries, Indonesia has to deal with health problems of a very large and diverse population with different races, culture, ethnicities, religions, social strata, education and with relatively few resources for integrated community care system.39 Understanding what is needed for effective implement CBIPE in an Asian context could therefore have potential to improve future health practice. Moreover, healthcare setting in Asian is unique as it is influenced by strong culture of social hierarchy in the community. Although healthcare teams are often characterized by issues of hierarchy and power,40,41 these issues are exacerbated in Asian settings. Status in Asian culture is a pervasive organizing principle in all social relationships and is based on such criteria as family background, age, education level and professional rank.42 Regarding professional rank and educational level, doctors in Asian society are considered to have a high status compared to other health professionals such as nurses, midwives and so on. The Asian culture of status reported complicates effective interprofessional communication, teamwork and collaboration in healthcare teams,43–46 as the communication style applied is commonly paternalistic or one directional; which reflect doctor’s sense of superiority to the other healthcare professionals; rather than partnership style; which can be found in western context and reflect a culture with more bigger sense of “equity”.38,43
This study aims to evaluate the design of a CBIPE project implemented in an Indonesian university. As interprofessional collaboration is the main goal of IPE and teamwork is known to be an important aspect influencing collaboration,47 this study addresses the following research questions:
- How do students perceive teamwork during CBIPE?
- How do students’ experience the design of the CBIPE programme?
Context
Community Health Services in Indonesia
Community healthcare centres are at the forefront of public health services in Indonesia. They have the main task of improving the quality of health through community health development programmes and basic health services that involve community members. Each community healthcare centre serves 30,000–50,000 residents or a sub-district, with a population of 10,000–20,000, that has one community healthcare centre. In providing health services, if the community healthcare centre receives or treats cases of emergency or non-emergency (chronic illness) but the available health workers do not have the authority or are unable to provide certain medical treatment or supporting health services that are needed by patients, they must refer these patients to more capable health facilities, such as public/private hospitals. Thus, the referral system is based on medical indication, rather than patient request.
As the faced health problems are increasingly complex, health workers from various professions in community healthcare centres must work together. They must not only provide basic healthcare services but also diagnose health problems that exist in the community and provide appropriate interventions for respective problems by providing preventive programmes that involve community members. As these duties are the responsibility of health workers, students following health professional education must gain experience in them.
IPE at Universitas Islam Sultan Agung
Universitas Islam Sultan Agung began an IPE project in 2013. Since 2016, students in medicine, nursing, and midwifery have been participating in the IPE curriculum, which is spread over several semesters, starting in the 2nd year. During their pre-clinical year (50 hours), the main learning approaches are Interprofessional Problem-Based Learning tutorials and interprofessional clinical skill simulation training in the form of integrated patient management.
Previous Community-Based Experience of Participants
Before participating in CBIPE, all students from the three health programmes involved had previous experience in uni-professional CBE. Medical students had experienced conducting one community health survey and providing health education for the community on three occasions. Midwifery students had visited clients at home, with each student visiting three families on average, with two visits per patient. In addition, midwifery students had been apprenticed at rural midwifery clinics and Public Health Centres for 8–9 weeks, providing primary care services. Nursing students would have been immersed in primary health care at Public Health Centres, including 1 month of conducting home visits.
Community-Based Interprofessional Education
In 2016, CBIPE was introduced for clinical-year medical and nursing students and final-year pre-clinical phase midwifery students who were taking clinical rotations in Community Medicine. The Sultan Agung Community-Based Interprofessional Education (SACBIPE) programme starts with one-week training course for all participants in the form of lectures, discussions and simulations on topics such as the ethics of conducting surveys, interprofessional collaboration, cultural problems in health care and so forth. After this course, students are divided into groups of seven containing 2–3 medical and nursing students and two midwifery students. All groups are distributed in several villages in the District of Genuk, Semarang, Indonesia. Each group is responsible for a neighbourhood, normally consisting of 25–30 families with 3–8 members per family.
Students spend 2 weeks in the community, working on CBIPE activities as designed in the SACBIPE programme. They conduct a community health-problem survey, analysing the data to diagnose primary community health problems and determining and implementing interventions for the respective problems.
Students present the findings of their data collection and analysis as well as intervention proposals to a forum attended by the field supervisors of all programmes, the head or staff from the local public health centre and community leaders. The proposed intervention can be in the form of counselling and education for the community, collaboration with the community on disease prevention, training voluntary community health workers in certain topics, home visits for family education, and so forth. At this stage, students must be able to identify the roles and responsibilities of each profession and share the task based on their role and authority. When students find an overlap of the task between professions, they discuss giving the task to the more competent profession or they will accomplish the task together. Types of activities, content and schedules of interventions proposed by the group must be discussed in advance with the group’s field supervisor. Coming from various health professions, the field supervisors and health professionals in charge of community healthcare service in the area, such as village midwives or nurses, assist the team of students in implementing the interventions.
At the end of the programme the students reflect on all the conducted processes. During this step, students not only discuss the project but also reflect on the interprofessional collaboration. Students might describe what they have accomplished, their limitations, and their thoughts for future recommendation. Facilitated by the field supervisor, the reflections are done in the interprofessional group, whose members collaborate on writing the reflection report (Figure 1).
 |
Figure 1 Design of the Sultan Agung Community-Based Interprofessional Education (SACBIPE) programme. |
Methods
The current study to evaluate students’ experiences with CBIPE and their collaborative skills was conducted in 2017–2018. A total of 254 students (109 medical students, 61 midwifery students and 84 nursing students) had participated in two terms of SACBIPE.
Research Design
We applied an explanatory, sequential mixed methods design to answer the research questions.48 We first collected quantitative data on students’ self-perceived teamwork performance during the SACBIPE programme with the Interprofessional Teamwork Evaluation.47 The results of the scale were then used as input for qualitative data collection, consisting of uni-professional focus group (FG) discussions aimed at understanding the underlying reasons for students’ perceptions of teamwork and collaborative performance. Students’ perception of the CBIPE programme was also probed during the focus groups.
Quantitative Data Collection
Students’ perceptions of teamwork were assessed with Interprofessional Teamwork Evaluation47 which was adapted from the Teamwork Perception Questionnaire developed by TeamSTEPPS.49 The Interprofessional Teamwork Evaluation consists of 23 items divided into four subscales: team structure, leadership, situation monitoring, mutual support and communication. All items were assessed on a 1–5 Likert scale, from strongly disagree to strongly agree.
The Indonesian version of the Interprofessional Teamwork Evaluation had not been validated. Double-back translation by two language experts was applied in translating the questionnaire.
Quantitative Data Analysis
Factor analysis was used to explore the construct validity of the Indonesian version of the questionnaire, and Cronbach’s alpha was calculated to determine internal consistency using SPSS (version 20; IBM Corporation, Armonk, NY, USA). The Cronbach’s alpha was acceptable if it was >0.7. Suitability of the correlation matrix was determined by the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. The KMO score was considered good and applicable if it was >0.7 and Bartlett’s test of sphericity was significant with P<0.05. The numbers of factors retained for the initial solutions and entered into the rotation were determined with Kaiser’s criterion (eigenvalues >1). Initial factor extraction was performed using principal component analysis. Finally, we performed an exploratory factor analysis using Promax rotation to define the clearer structure. Kruskal–Wallis and Mann–Whitney U statistical analyses using IBM SPSS (version 23.0) were applied to evaluate the mean rank difference of total scores and subscale scores among subjects since the data were not normally distributed.
Qualitative Data Collection
To gain a better understanding of the students’ perception of interprofessional teamwork and collaboration performance, we organised three uni-professional focus groups. We deliberately chose not to mix students from different programmes to overcome potential barriers to communication and to encourage participation in the discussion.50 FG participation was voluntary. Students were invited to participate in FGs during the wrap-up session. Eight midwifery students, ten nursing students and ten medical students took parts. Lecturers in community medicine (AL and SY) who understood the concept and aims of the study facilitated the FGs with the aid of a discussion guide.51 The two facilitators took turns being the discussion facilitator because they had to handle three focus group discussions. When one was on duty, the other was observing. There was no power relationship between facilitators and students because the facilitators were not the CBIPE field supervisors. The FG guide included the following questions for students: (a) what is your perception of the design of the SACBIPE, (b) what needs to be improved in the SACBIPE, (c) what is your perception of the interprofessional teamwork and collaboration during the programme, (d) why did they score certain items on the questionnaire low or high? All FGs were tape recorded and transcribed verbatim by two experts in medical education.
Qualitative Data Analysis
The verbatim transcripts were coded and analysed by two experts (authors EL and SY), who independently evaluated the transcripts and developed coding categories. Afterward, they discussed the coding categories and agreed on the coding, which they finally applied to the data. After this process, all members of the research team discussed the findings up to the point of consensus on the overarching themes. For the thematic content analysis, ATLAS.Ti (version 7; ATLAS.ti Scientific Software Development GmbH, Berlin, Germany) was used.
Ethics
The study complied with the Declaration of Helsinki and was approved by the Bioethics Committee for Medical/Health Research Faculty of Medicine Islamic University of Sultan Agung Semarang (Letter No. 352/XII/2016/Komisi Bioetik) and was conducted at Universitas Islam Sultan Agung, Semarang, Indonesia. Taking part in the study posed no physical risks to participants. A cover letter explaining the study’s goal and confidentiality accompanied the questionnaire. Written informed consent obtained from participants included information concerning reproducing their responses. All students were informed that this project was part of an evaluation of the programme, that participation was voluntary and refusal to join the study would have no consequences. Consent was implied by the fact that students completed the questionnaire and took part voluntarily in the FGs. To ensure confidentiality we anonymised both the questionnaires and the transcripts of the FG interviews.
Results
Evaluation of the SACBIPE Programme
The SACBIPE programme was evaluated in focus group discussions. FGs were conducted with 26 voluntary participants from midwifery, nursing, medical programmes (Table 1). The findings indicate that students felt they benefited from the programme. Students enjoyed problem-solving and practising in real settings as they were interested in active learning. Students reported that by working together as a team in the community, they improved their “soft” skills, such as communication, leadership, conflict management, leadership and collaboration. The CBE format also helped students develop their skills in decision-making, planning and role sharing. Students said that they experienced identifying their own and other professions’ roles and the boundaries between them.
Discussing community problems with other health professional students was interesting. We had to discuss the problem, decide on possible interventions to solve it, schedule activities and share tasks among team members. Conflicts were discussed in the group. I think this was good practice for us to improve our collaboration skills. (Nursing student 3)
 |
Table 1 Characteristics of Uni-Professional FG Participants |
Students felt a stronger need to truly collaborate in the community-based interprofessional education activities, something which the interprofessional PBL they had previously experienced did not afford them.
Community-based IPE benefits us more than just PBL discussion in class, like we did in the pre-clinical phase. In this community-based IPE, we faced a real problem, not a scenario, that required us to collaborate and work together, and share roles in evaluating and solving the community health problem. (Medical student 6)
Students identified assessment of SACBIPE as in need of improvement. In the current design of SACBIPE, assessments are conducted by field supervisors and health professionals from the public health centre. Students suggested that it would be much fairer if assessments were also carried out by the community, such as family members who are visited or by voluntary community health workers who always collaborate with students in every intervention activity.
Quantitative Findings
Students’ perception of teamwork was evaluated with the Interprofessional Teamwork Scale. Of the 254 participants, 210 filled in the questionnaire completely (82.7%), 57 midwifery, 69 nursing, and 84 medical students (Table 2).
 |
Table 2 Characteristics of Subjects |
Factorial Analysis of the Questionnaire
The KMO index was 0.895, indicating sampling adequacy, while the Bartlett sphericity chi-square index was 2295.118, with p = 0.000 (<0.001) indicating that the correlation matrix was an identity matrix and therefore suitable for factor analysis. Exploratory factor analysis yielded three subscales which differed from the original questionnaire’s subscales by Shrader et al.52 Items of “communication” subscale converged with several items of the “mutual support” subscale, while all items of the “leadership” subscale converged with the items of the “team structure” subscale. Because the factorial analysis resulted in a different structure from the original questionnaire, the authors chose to rename the subscales as follows: subscale (a) “communication and mutual support” (13 items), subscale (b) “team structure and leadership” (7 items) and subscale (c) “situation monitoring” (3 items) with Cronbach’s alpha scores of 0.924, 0.853 and 0.712, respectively (Table 3).
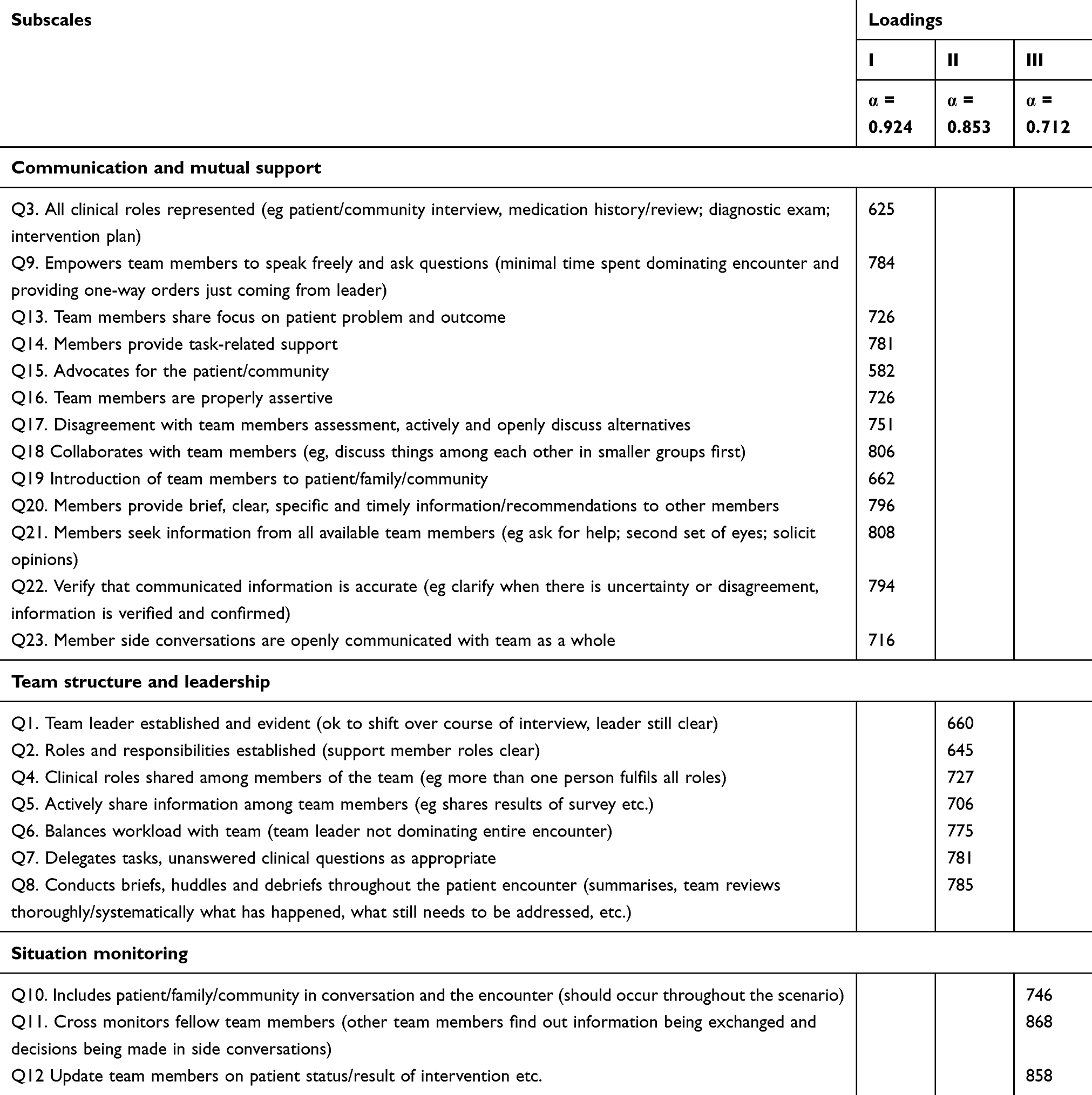 |
Table 3 Factor Loading of Each Item of Interprofessional Teamwork Evaluation (ITE) |
In general, medical students’ scores for interprofessional teamwork were higher than the scores of midwifery and nursing students. The Kruskal–Wallis statistical test results revealed significant differences in students’ mean rank scores on all items in subscale communication and mutual support, with the scores of midwifery students the lowest compared to the nursing and medical students. The results showed that midwifery students had a poor perception of interprofessional communication and the mutual support carried out by the group during the CBIPE activities. In addition, there were significant differences in students’ mean scores regarding “Team leader established and evident” and “Actively shares information among team members”, with the mean scores of nursing and medical students lower than midwifery students. These results indicate that the three groups of students assess leadership performance differently. Communication, mutual support and leadership are a problematic area of interprofessional teamwork (Table 4).
 |
Table 4 Mean Difference of Each Item |
Qualitative Findings
Focus groups discussions shed light on why midwifery and nursing students give less positive perceptions of communication and mutual support. The reasons were: communication gap due to lack of confidence, different ways of thinking affected communication in decision-making, and the leadership culture on collaborative practice in health services.
Communication Gap Due to Lack of Confidence
Some nursing and midwifery students felt insecure when collaborating with medical students. They felt inferior in terms of both social status and knowledge. This lack of confidence impeded communication and coordination between students during collaboration.
In our opinion communication is still a problem. We don’t feel so involved. We rarely propose anything at meetings, and sometimes we’re scared to even ask for information. We don’t know why, but we hesitate because we feel that our knowledge is not as important as the science of medical students. (Midwifery student 6)
Different Ways of Thinking and Level of Education Affected Decision-Making
Another communication problem was in decision-making. Medical students were often the ones to decide. Midwifery and nursing students complained that they wanted to contribute and provide alternative solutions, but, as medical students generally wanted a fast answer, they made quick decisions which the other professional students would have to agree with.
We really want to argue, but, while we’re still thinking of alternatives, the med students already make the decision, so finally we all have to agree with it. (Midwifery student 1)
Nursing students suggested that the differences may be influenced by how students from both health professions are educated to think in making decisions.
In our opinion there is difference in the way of thinking of medical and nursing students. We, nurses, are used to thinking holistically. Even when doing nursing care or nursing diagnostics, we make considerations such as from ‘head to toe’. For medical student it might be considered as taking time. So, what happens was that while we were still thinking they already made the decision. OK, finally we just followed. (Nursing student 7)
Level of education also influenced decision-making collaboration. As informed earlier that midwifery students were in their final year (3rd year) therefore they were in different grades with medical and nursing students who were in their clinical phase (year 5). Unequal level of education was reported by students as factors that might hinder communication.
We realised that communication problems arose because midwifery students are junior to us, so they might have a feeling of apprehensive when it comes to expressing opinions. Even though we have asked them to argue, they provided very few opinions. Finally, we decided lots and they followed (Medical student 5)
Leadership Culture in Health Services Influences the Choice of Team Leader
The other interesting finding was that all 30 groups of interprofessional teams in this study were led by medical students. This may be explained by the fact that the health profession culture places doctors in the highest hierarchical position of collaborations. Therefore, midwifery and nursing students tended to give leadership positions to medical students.
Yes, we appointed medical students as leaders in our group, that’s the culture, right? Even so, we still had opportunity to lead several smaller projects, related to our responsibilities. (Nursing student 2)
Discussion
This study aimed to evaluate students’ perception toward teamwork during CBIPE programme and how they experience the CBIPE educational design. To answer the first question, we did a survey using the Interprofessional Teamwork Evaluation Instrument and to answer the second question, we collected data from focus group discussions.
Students experienced the three weeks of IPE activities as successful in stimulating them to work in teams with the community to solve the community’s health problems. However, midwifery and nursing students had markedly different experiences. Although students had the opportunity to develop their communication skills with the SACBIPE programme, the quantitative data indicated that midwifery and nursing students did experience problems with communication and mutual support. The results of the FGs showed that the root of this issue was the lack of confidence and initiative in nursing and midwifery students. Previous studies have reported that midwifery students often lack confidence in their own abilities.53 Nursing and midwifery students are reported to consider themselves less competent than medical students in terms of knowledge and skills due to several factors, such as their status in society, competence and academic abilities.54,55 Tyastuti and colleagues (2013) recommend implementing non-scheduled extra-curricular activities for multi-professional students to help them improve their relations before they begin an IPE programme.56
Medical students were mostly the leaders of the community-based projects in our research, a situation similar to one reported by a previous study.54 The quantitative finding also reported that in general midwifery students and nursing students were satisfied with the way medical students lead the group. They reflected that it was natural to make medical students as leaders of the groups because in real healthcare team context doctors will lead the healthcare teams. This perception was affected by healthcare team culture which was developed based on hierarchical relationships and dominant–subordinate relationships40,57 and which always places doctors as the highest position and marginalized other professions. Yet with the complexity of current health problems, it is known that leadership must be collaborative and must focus on building trust and sharing power.41 Such collaborative efforts necessitate a shift away from vertical or hierarchical relationships of influence to horizontal power sharing.58 Considering that, healthcare professional students including nurses and midwives must be prepared with leadership competencies to enable them to meet the challenges of leading collaboratively with other professions. IPE is one approach that can be implemented to develop shared, transformational leadership skills.41,59,60
The uni-profession FGs revealed that students were satisfied with the design of SACBIPE and that it helped them to learn about IPC and community-based practice. Students argued that the learning design was more effective in fostering collaboration and teamworking skills compared to their experiences with interprofessional PBL. This finding suggests that active engagement in a workplace learning setting is a more effective way to expose students to IPC and help them learn about it. It also suggests that learning in real practice effectively fosters the culture that must be developed in the real situation and that learning with an IPE design will be effective if implemented in practice-based settings.17–19,61
CBIPE seems a potentially effective way to stimulate interprofessional collaborative learning for students. Our research indicates that successful implementation is possible but that the role of supervisor/teacher and assessment procedures both require close attention. Previous studies have highlighted the role of the supervisor/teacher in community-based IPE.24,56 In the IPE context, teaching staff must perform additional roles, including facilitating collaboration, sharing IPV values, such as showing respect, valuing other professions, collaboration, assessing collaboration and facilitating reflection on and evaluation of collaboration.62–64 This requires the faculty development programme to pay specific attention to developing equal perceptions and the teachers’ understanding of interprofessional education and collaboration so that they can develop, implement, and facilitate IPE activities.62,65–67
The literature has also paid attention to IPE assessment.68–70 Assessment of community-based education is known to be done by measuring problem-solving skills, communication, leadership and critical thinking capabilities. Assessment can be done by applying such methods as direct observation of particular skills during an intervention, the students’ report, and reflection sessions.71,72 These methods are also suitable for CBIPE, with the addition assessing the particular skills and attitudes that need to be developed in collaboration with other health workers.24,73 Our research suggests incorporating specifically the views of community members in the assessment since they have first-hand experience with the students’ activities.
The mixed methods approach to evaluate a model of community-based interprofessional education, this SACBIPE programme, and the resulting teamwork skills of the students can be considered strengths of this study. There is a limitation in that data were collected from schools of health profession of one university in Indonesia, which might restrict the generalizability of our findings. However, we aimed to increase transferability74 by providing a rich context description of the setting and programme so that others might interpret the value of the research for their own context. Future research could try to further unravel the influence of culture and power dynamics on interprofessional community-based education.
Conclusion
The SACBIPE programme was successfully implemented. It demonstrated that it could help health professional students develop their skills in collaborative practice. SACBIPE could provide learning activities that treat the community extensively as a learning environment, fostering active engagement not only in students but also members of the community throughout the educational experience. With CBIPE, students learn in the context of the community itself and work collaboratively in interprofessional teams to provide an expected health service despite limited resources. Nevertheless, problems are still found in communication and leadership skills, so that teaching in these skills needs improvement in the future. As complex learning, IPE needs a comprehensive approach in its implementation that includes various teaching methods and proper learning strategies. To this end, community-based education models seem promising.
Data Sharing Statement
Materials and supporting data are deidentified, however, they are available for download on the website: https://drive.google.com/drive/folders/1pH6iMwf43xI8JGCQGbha2vuKNRa_FtS3. All files may be used for research and education with further consent.
Acknowledgments
The authors wish to thank the Directorate General of Higher Education, Ministry of Research, Technology and Innovation, Republic of Indonesia, for funding the project; all teaching staff/field supervisors from the Nursing, Midwife and Medical departments of Universitas Islam Sultan Agung; all students who participated in the study; and Dian Apriliana Rachmawati (DAR) and Suryani Yulianti (SY), research associates of the Medical Education Unit of the Faculty of Medicine, Universitas Islam Sultan Agung, for their assistance in conducting the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Ministry of Research, Technology and Innovation of Republic of Indonesia funded this project.
Disclosure
The authors declare that they have no competing interests. The authors alone are responsible for the writing and content of this paper.
References
1. Baker MJ, Fowler-Durham C. Interprofessional education: a survey of student’s collaborative competency outcomes. J Nurs Educ. 2013;52(12):713–718. doi:10.3928/01484834-20131118-04
2. Bridges DR, Tomkowiak J. Allport’s intergroup contact theory as a theoretical base for impacting student attitudes in interprofessional education. J Allied Health. 2010;39(1):e29–33.
3. Makino T, Shinozaki H, Hayashi K, et al. Attitudes toward interprofessional healthcare teams: a comparison between undergraduate students and alumni. J Interprof Care. 2013;27(3):261–268. doi:10.3109/13561820.2012.751901
4. Olson R, Bialocerkowski A. Interprofessional education in allied health: a systematic review. Med Edu. 2014;48:236–246. doi:10.1111/medu.12290
5. Olupeliyawa AM, O’Sullivan AJ, Hughes C, Balasooriya CD. The teamwork mini-clinical evaluation exercise (T-MEX): a workplace-based assessment focusing on collaborative competencies in health care. Acad Med. 2014;899(2):1–7.
6. Rowland P, Kitto S. Patient safety and professional discourses: implications for interprofessionalism. J Interprof Care. 2014;28(4):331–338. doi:10.3109/13561820.2014.891574
7. Brock D, Abu-Rish E, Chia-Ru C, et al. Interprofessional education in team communication: working together to improve patient safety. BMJ Qual Saf. 2013;22(5):414–423. doi:10.1136/bmjqs-2012-000952
8. Thistlehwaite JE, Forman D, Matthews LR, Rogers GD, Steketee C, Yassine T. Competencies and frameworks in interprofessional education: a comparative analysis. Acad Med. 2014;89(6):869–875. doi:10.1097/ACM.0000000000000249
9. Derbyshire JA, Machin AI. Learning to work collaboratively: nurses’ views of their pre-registration interprofessional education and its impact on practice. Nurse Educ Pract. 2011;11(4):239–244. doi:10.1016/j.nepr.2010.11.010
10. Murray-Davis B, Marshall M, Gordon F. From school to work, promoting the application of pre-qualification of interprofessional education in the clinical workplace. Nurse Educ Pract. 2012;12:289–296. doi:10.1016/j.nepr.2011.10.009
11. WHO. Framework for Action on Interprofessional Education & Collaborative Practice. World Health Organization; 2010.
12. Thistlethwaite J, Moran M. Learning outcomes for interprofessional education (IPE): literature review and synthesis. J Interprof Care. 2010;24(5):503–513. doi:10.3109/13561820.2010.483366
13. Lestari E, Stalmeijer RE, Widyandana D, Scherpbier A. Does PBL deliver constructive collaboration for students in interprofessional tutorial groups? BMC Med Educ. 2019;19(1):1–13. doi:10.1186/s12909-019-1802-9
14. D’Eon M, Proctor P, Cassidy J, McKee N, Trinder K. Evaluation of an interprofessional problem-based learning module on care of persons living with HIV/AIDS. J Res Interprof Pract Educ. 2010;1(2):109–126.
15. McKee N, D’Eon M, Trinder K. Problem-based learning for inter-professional education: evidence from an inter-professional PBL module on palliative care. Can Med Educ J. 2013;4(1):e35–e48. doi:10.36834/cmej.36602
16. Stubbs C, Schorn MN, Leavell JP, et al. Implementing and evaluating a community-based, inter-institutional, interprofessional education pilot programme. J Interprof Care. 2017;31(5):652–655. doi:10.1080/13561820.2017.1343808
17. Paradis E, Whitehead CR. Beyond the lamppost: a proposal for a fourth wave of education for collaboration. Acad Med. 2018;93:1457–1463. doi:10.1097/ACM.0000000000002233
18. Frisby J, Mehdi Z, Birns J. Interprofessional learning on a stroke unit. Clin Teach. 2015;12:315–319. doi:10.1111/tct.12321
19. Vanderzalm J, Hall MD, McFarlane L-A, Rutherford L, Patterson SK. Fostering interprofessional learning in a rehabilitation setting: development of an interprofessional clinical learning unit. Rehabil Nurs. 2013;38:178–185.
20. Ahmad A, Yussof MSB, Mohammad WMZW, Nor MZM. Nurturing professional identity through a community based education program: medical students experience. J Taibah Univ Sci. 2018;13(2):113–122. doi:10.1016/j.jtumed.2017.12.001
21. Asakawa T, Kawabata H, Kisa K, Terashita T, Murakami M, Otaki J. Establishing community-based integrated care for elderly patients through interprofessional teamwork: a qualitative analysis. J Multidiscip Healthc. 2017;10:399–407. doi:10.2147/JMDH.S144526
22. Randita A, Widyandana W, Claramita M. IPE-COM:apilotstudyoninterprofessionallearningdesign for medical and midwifery students. J Multidiscip Healthc. 2019;12:767–775. doi:10.2147/JMDH.S202522
23. WHO. Learning Together to Work Together for Health. Switzerland: WHO; 1988.
24. Hosny S, Kamel MH, El-Wazir Y, Gilbert J. Integrating interprofessional education in community-based learning activities: case study. Med Teach. 2013;35:S68–S73. doi:10.3109/0142159X.2013.765550
25. Ohta R, Kamiyama Y, Makishi T. Inquiry into short-term learning on Japanese rural islands: a qualitative study. Educ Prim Care. 2019;1–8.
26. Ryan M, Vanderbilt AA, Mayer SD, Gregory A. Interprofessional education as a method to address health needs in a Hispanic community setting: a pilot study. J Interprof Care. 2015;29(5):515–517. doi:10.3109/13561820.2015.1020360
27. Boelen C. Why should social accountability be a benchmark for excellence in medical education? Educ Med. 2016;17(3):101–105.
28. Gum LF, Sweet L, Greenhill J, Prideaux D. Exploring interprofessional education and collaborative practice in Australian rural health services. J Interprof Care. 2019;1–11.
29. Haruta J, Yamamoto Y. Realist approach to evaluating an interprofessional education program for medical students in clinical practice at a community hospital. Med Teach. 2019.
30. Rhoda A, Laattoe N, Smithdorf G, Roman N, Frantz J. Facilitating community-based interprofessional education and collaborative practice in a health sciences faculty: student perceptions and experiences. Afri J Health Prof Educ. 2016;8(2):225–228. doi:10.7196/AJHPE.2016.v8i2.846
31. McCaffrey R, Ruth MT, Daniel ML, Friedland M. Interprofessional education in community-based Alzheimer’s disease diagnosis and treatment. J Interprof Care. 2013;27(6):534–536. doi:10.3109/13561820.2013.817384
32. Kurowski-Burt AL, Evans KW, Baugh GM, Utzman RR. A community-based interprofessional education fall prevention project. J Inter Prof Educ Pract. 2017;8:1–5. doi:10.1016/j.xjep.2017.04.001
33. Healey WE, Cygan HR, Reed M, Huber G. Physical therapist student, nursing student, and community partner perspectives of working together in a Chicago neighborhood after-school program. J Phys Ther Educ. 2018;32(2):191–198. doi:10.1097/JTE.0000000000000033
34. Isibela D, Bennington L, Boshier M, Stull S, Blando J, Claiborne D. Building interprofessional student teams for impactful community service learning. J Inter Prof Educ Pract. 2018;12:83–85. doi:10.1016/j.xjep.2018.07.002
35. Hays A, Schriever C, Rudzinski J, Lynch JL, Genrich E, Schriever A. Fostering interprofessional education through a multidisciplinary, community-based pandemic mass vaccination exercise. Am J Public Health. 2018;108:358–360. doi:10.2105/AJPH.2017.304240
36. Lestari E, Yuliyanti S. Community based interprofessional learning promotes equality of participation among health professions students. J Health Allied Sci. 2018;17:1–6.
37. Kristina TN, Syukriani Y. Community-based health-professions interprofessional education: a collaborative and sustainable model. Jurnal Pendidikan Kedokteran Indonesia. 2018;7(1):36–43.
38. Claramita M, Nugraheni MDF, Dalen J, Vleuten C. Doctor–patient communication in Southeast Asia: a different culture? Adv Health Sci Educ. 2013;18:15–31. doi:10.1007/s10459-012-9352-5
39. Tham TY, Tran TL, Prueksaritanond S, Isidro JS, Setia S, welluppillai V. Integrated health care systems in Asia: an urgent necessity. Clin Interv Aging. 2018;13:2527–2538. doi:10.2147/CIA.S185048
40. Whitehead C. The doctor dilemma in interprofessional education and care: how and why will physicians collaborate? Med Edu. 2007;41:1010–1016. doi:10.1111/j.1365-2923.2007.02893.x
41. Goldsberry JW. Advanced practice nurses leading the way: interprofessional collaboration. Nurse Educ Today. 2018;65:1–3. doi:10.1016/j.nedt.2018.02.024
42. Widiastuti A. Being Javanese a changing city. In: Ismail R, Shaw B, Ling OG, editors. Southeast Asian Culture and Heritage in a Globalising World. England: Ashgate Publishing Limited; 2009:115–128.
43. Claramita M, Susilo AP. Improving communication skills in the Southeast Asian health care context. Pers Med Educ. 2014;3:474–479. doi:10.1007/s40037-014-0121-4
44. Kim YM, Kols A, Bonnin C, Richardson P, Roter D. Client communication behaviors with healthcare providers in Indonesia. Patient Educ Couns. 2001;45(1):59–68. doi:10.1016/S0738-3991(01)00144-6
45. Houben V. Sociocultures of insular Southeast Asia: between history, area and social studies. Transcience. 2014;5(1):28–35.
46. Lestari E, Stalmeijer R, Widyandana D, Scherpbier AJJA. Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study. BMC Med Educ. 2016;16(1):1–11. doi:10.1186/s12909-016-0704-3
47. Shrader S, Kern D, Zoller J, Blue A. Interprofessional teamwork skills as predictors of clinical outcomes in a simulated healthcare setting. J Allied Health. 2013;42(1):e1–e6.
48. Johnson RB, Onwuegbuzie AJ. Mixed methods research: a research paradigm whose time has come. Educ Res. 2004;33(7):14–26. doi:10.3102/0013189X033007014
49. Battles J, King HB. TeamSTEPPS® Teamwork Perceptions Questionnaire Manual. Washington DC: American Institute for Research; 2010.
50. Boateng W. Evaluating the Efficacy of Focus Group Discussion (FGD) in qualitative social research. Int J Bus Soc Sci. 2012;3(7):54–57.
51. Sarantokos S. Social Research.
52. Shrader S, Farland MZ, Danielson J, Sicat B, Umland EM. A systematic review of assessment tools measuring interprofessional education outcomes relevant to pharmacy education. Am J Pharm Educ. 2017;81(6):1–20. doi:10.5688/ajpe816119
53. Skirton H, Stephen N, Doris F, Copper M, Avis M, Fraser DM. Preparedness of newly qualified midwives to deliver clinical care: an evaluation of pre-registration midwifery education through an analysis of key events. Midwifery. 2012;28:e660–e666. doi:10.1016/j.midw.2011.08.007
54. Rudland J, Mires G. Characteristics of doctors and nurses as perceived by students entering medical school: implications for shared teaching. Med Edu. 2005;39:448–455. doi:10.1111/j.1365-2929.2005.02108.x
55. Brown J, Lewis L, Ellis K, Stewart M, Freeman T, Kasperski M. Conflict on interprofessional primary health care teams–can it be resolved? J Interprof Care. 2011;25:4–10. doi:10.3109/13561820.2010.497750
56. Tyastuti D, Onishi H, Ekayanti F, Kitamura K. An educational intervention of interprofessional learning in community based health care in Indonesia: what did we learn from the pilot study? J Educ Pract. 2013;4(25):1–11.
57. Reeves S, Zwarenstein M, Zwarenstein M. Doctor-nurse game in the age of interprofessional care: a view from Canada. Nurs Inq. 2008;15(1):1–2. doi:10.1111/j.1440-1800.2008.00396.x
58. Wilson S. Collaborative leadership: it’s good to talk. J Healthc Manag. 2013;19(7):335–337. doi:10.12968/bjhc.2013.19.7.335
59. Chan K, Wong FKY, Chan LK, Ganotice FA. FAG. Interprofessional team-based learning: a revealing process for cultivating professional identity among nursing students. Open J Nurs. 2019;9:249–267. doi:10.4236/ojn.2019.93025
60. Schaik S, O’Brien B, Almeida S, Adler S. Perceptions of interprofessional teamwork in low-acuity settings: a qualitative analysis. Med Edu. 2014;48:583–592. doi:10.1111/medu.12424
61. Morphet J, Hood K, Cant R, Baulch J, Gilbee A, Sandry K. Teaching teamwork: an evaluation of an interprofessional training ward placement for health care students. Adv Med Educ Pract. 2014;5:197–204.
62. Grymonpre RE. Faculty development in interprofessional education (IPE): reflection from an IPE coordinator. J Taibah Univ Sci. 2016;11(6):510–519. doi:10.1016/j.jtumed.2016.10.006
63. Steinert Y. Learning together to teach together: interprofessional education and faculty development. J Interprof Care. 2005;19(Suppl 1):60–75. doi:10.1080/13561820500081778
64. Cooper H, Braye S, Geyer R. Complexity and interprofessional education. Health Soc Care. 2004;3(4):179–189. doi:10.1111/j.1473-6861.2004.00076.x
65. Watkins KD. Faculty development to support interprofessional education in healthcare professions: a realist synthesis. J Interprof Care. 2016;30(6):695–701. doi:10.1080/13561820.2016.1209466
66. Kwan D, Barker K, Richardson D, Wagner SJ, Austin Z. Effectiveness of a faculty development program in fostering interprofessional education competencies. J Res Interprof Pract Educ. 2009;1(1). doi:10.22230/jripe.2009v1n1a4
67. Freeman S, Wright A, Lindqvist S. Facilitator training for educators involved in interprofessional learning. J Interprof Care. 2010;24(4):375–385. doi:10.3109/13561820903373202
68. Healey AN, Undre S, Sevdalis N, Koutantji M, Vincent CA. The complexity of measuring interprofessional teamwork in the operating theatre. J Interprof Care. 2006;20(5):485–495. doi:10.1080/13561820600937473
69. Roberts SD, Lindsey P, Limon J. Assessing students’ and health professionals’ competency learning from interprofessional education collaborative workshops. J Interprof Care. 2018.
70. Simmons BS, Wagner SJ, Reeves S. Assessment of interprofessional education: key issues, ideas, challenges, and opportunities. In: Wimmers PF, Mentkowski M, editors. Assessing Competence in Professional Performance Across Disciplines and Professions. Vol. 13. Switzerland: Springer International Publishing; 2016.
71. Mpofu R, Imalingat A. The development of an instrument for assessing community-based education of undergraduate students of community and health sciences at the University of the Western Cape. Educ Health. 2006;19(2):166–178. doi:10.1080/13576280600783646
72. Mennin S, Petroni-Mennin R. Community-based medical education. Clin Teach. 2006;3:90–96. doi:10.1111/j.1743-498X.2006.00093.x
73. Hammick M, Freeth D, Koppel I, Reeves S, Baar H. A best evidence systematic review of interprofessional education: BEME Guide no. 9. Med Teach. 2007;29:735–751. doi:10.1080/01421590701682576
74. Frambach JM, Vleuten CPMVD, Durning SJ. AM last page: quality criteria in qualitative and quantitative research. Acad Med. 2013;88(4):552.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.