")
Back to Journals » Infection and Drug Resistance » Volume 17
Species Distribution, Typical Clinical Features and Risk Factors for Poor Prognosis of Super-Elderly Patients with Bloodstream Infection in China
Authors Cui J, Li Y, Du Q, Wei Y, Liu J, Liang Z
Received 14 October 2023
Accepted for publication 9 February 2024
Published 1 March 2024 Volume 2024:17 Pages 779—790
DOI https://doi.org/10.2147/IDR.S444694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jiewei Cui,1,* Yang Li,2,* Qingyan Du,3,* Yuanhui Wei,1 Jinxia Liu,1 Zhixin Liang1
1College of Pulmonary & Critical Care Medicine, 8th Medical Center of Chinese PLA General Hospital, Beijing, 100091, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, The First Hospital of Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 3Jiamei Dental Hospital, Beijing, 100143, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhixin Liang, Email [email protected]
Objective: Bloodstream infection (BSI) is characterized by high mortality, especially among these increasing super-elderly patients (≥ 85 years), and this study was conducted to understand the species distribution, typical clinical features and risk factors for poor prognosis of super-elderly patients with BSI.
Methods: Based on previous work, this retrospective study was performed by reviewing an ongoing prospective medical database in a comprehensive tertiary center in China, and all super-elderly patients with BSI in the past 6 years were enrolled in this study.
Results: Out of 5944 adult-patients with BSI, there were totally 431 super-elderly patients (≥ 85 years old) enrolled in this study and age ≥ 90 years accounted for 31.1% (134/431). Among these 431 super-elderly patients with BSI, 40 patients (9.3%) were diagnosed with BSI and the remained 401 super-elderly patients (90.7%) were defined as hospital-acquired BSI. The typical feature of these super-elderly patients with BSI was the high proportion of patients with various comorbidities, such as cardiovascular disease (83.8%), ischemic cerebrovascular disease (63.3%) and pulmonary infection (61.0%). The other typical feature was that most (60.1%) of these patients had been hospitalized for long time (≥ 28 days) prior to the onset of BSI, and most patients had received various invasive treatments, such as indwelling central venous catheter (53.1%) and indwelling urinary catheter (47.1%). Unfortunately, due to these adverse features above, both the 7-day short-term mortality (13.2%, 57/431) and the 30-day long-term mortality (24.8%, 107/431) were high. The multivariate analysis showed that both chronic liver failure (OR 7.9, 95% CI 2.3– 27.8, P=0.001) and indwelling urinary catheter (OR 2.3, 95% CI 1.1– 4.7, P=0.023) were independent risk factors for 7-day short-term mortality, but not for 30-day long-term mortality. In addition, the microbiology results showed that the most common species were associated with nosocomial infection or self-opportunistic infection, such as Staphylococcus hominis (18.3%), Staphylococcus epidermidis (11.8%), Escherichia coli (9.7%), Klebsiella pneumoniae (9.3%) and Candida albicans (8.6%, fungi).
Conclusion: Super-elderly patients with BSI had typical features, regardless of the pathogenic species distribution and their drug resistance, or clinical features and their risk factors for poor prognosis. These typical features deserved attention and could be used for the prevention and treatment of BSI among super-elderly patients.
Keywords: bloodstream infection, elderly, species, risk factor, mortality, aging, central venous catheter, clinical feature
Introduction
Bloodstream infection (BSI) has a high mortality and the number of BSI has been increasing for various risk factors, such as the widely application of central venous catheter (CVC).1–3 According to the report from the China Antimicrobial Surveillance Network (CHINET), the number of specimens of BSI in China had increased from 296,052 in 2018 to 325,016 in 2021 (the report from the China National Drug Resistance Monitoring Network, https://www.carss.cn/sys/Htmls/dist/index.html#/distribution?type=specimens). Our previous research also reported that the episodes of BSI had increased from 2010 to 2019 in the hospital where this study was conducted.4 And among various risk factors for BSI, age is an important risk factor for BSI. Compared with young people, the elderly people (age ≥ 65 years old) are more prone to BSI due to various risk factors, such as weakened immunity and more comorbidities.5,6 Furthermore, the prognosis among elderly patients with BSI is even worse and the mortality is much higher, especially among those super-elderly patients (age ≥ 85 years old).7,8 However, due to the increasingly serious aging in the current society,9 there are more and more super-elderly patients without and with BSI, and the prevention for poor prognosis of super-elderly patients with BSI have been attracting more and more attention.
About risk factors for the poor prognosis of BSI, although previous studies had already pointed out that many risk factors were be associated the mortality of various BSI such as severity of illness,10,11 the risk factors leading to poor prognosis of super-elderly patients with BSI may have their typical features. For example, the super-elderly patient might have multiple risk factors at the same time, such as multiple comorbidities, or a certain risk factor may be more serious, such as liver failure rather than just liver injury. Similarly, as to be known, timely and early appropriate empirical antimicrobial therapy is the critical protective factor for the prognosis of BSI,12,13 while the microbiology about the species distribution and their antibiotic resistance profiles used to guide empirical antimicrobial therapy should be also specific among super-elderly patients with BSI. However, there were few specific studies that focused on these typical risk factors and microbiology among super-elderly patients with BSI currently.
Therefore, in order to understand the latest and special microbiology features about the species distribution and their antibiotic resistance of BSI among super-elderly patients, we conducted this study in one of the largest tertiary hospitals in China. And simultaneously, we also hoped that we could find out the special risk factors for the poor prognosis (death) so as to give the super-elderly patients more targeted treatment to improve their prognosis.
Methods
Previous Work for This Study
This study was undertaken at the Chinese People’s Liberation Army (PLA) General Hospital. The center is one of the largest comprehensive tertiary medical centers in China and there are more than 140,000 hospitalized patients per year. Just as descripted in our previous study,4 all hospitalized patients who were suspected of BSI by clinicians would receive a set of blood cultures only when they had symptoms and signs related to BSI such as fever, chills, and unexplained hypotension. Each set of blood cultures in our hospital included an aerobic blood culture bottle and an anaerobic blood culture bottle. A positive blood culture was defined as at least one isolation of microorganisms for a set of blood cultures, including bacterial, fungal and other rare pathogens. All hospitalized patients with positive blood cultures were considered as being suspicious for BSI, but only patients who had at least one BSI-related clinical symptom and (or) elevated levels of at least one BSI-related molecular marker were diagnosed with BSI by reviewing the real-time nosocomial infection surveillance system (RT-NISS) in the hospital. Otherwise, the positive blood culture was considered a contaminant or colonization.
Identification of the detected strain from blood cultures: Blood cultures were performed at the hospital’s clinical microbiology laboratory. The blood culture was processed using the BacT/ALERT 3D Microbial Detection System (Becton-Dickinson, Sparks, MD, USA), and the species identification was performed using the VITEK 2 System (BioMérieux, Marcy 1′Étoile, France). The implementation standard of the antimicrobial susceptibility test was performed in accordance with the Clinical and Laboratory Standards Institute (CLSI) standards updated annually.
Inclusion and exclusion of BSI: The RT-NISS system identified repeated and identical BSI in the same patient. If the patient who was diagnosed with BSI had two or more positive blood cultures caused by an identical specie within 14 consecutive days, only the first blood culture was used to diagnose an episode of BSI, and the other cultures were excluded. However, if the identical BSI recurred after 14 days, the recurrent BSI was considered a new episode of BSI by the RT-NISS system. Additionally, if the patient had one or more positive blood cultures caused by two or more different species and each of the species in the blood culture could be diagnosed as BSI, then each species that caused the BSI was considered as a separate episode of BSI.
Design and Purpose of This Study
In our previous study mentioned above, we had collected 9381 adult-hospitalized patients diagnosed with BSI in this hospital from January 1, 2010 to December 31, 2019.4 And our purpose and design of this study was to separately screen those super-elderly patients with BSI from these 9381 adult-hospitalized patients with BSI and conducted this study. For this purpose, in this study, the super-elderly patient was defined as patient aged 85 years or older. Bloodstream infection (BSI) was defined as a patient who had detected pathogenic microorganisms by blood culture, and also showed symptoms and/or signs of infection. The study period was from January 1, 2014 to December 31, 2019.
According to the purpose of this study, out of those 9381 patients diagnosed with BSI mentioned above, there were 5944 adult-patients with BSI from January 1, 2014 to December 31, 2019. And out of 5944 adult-patients with BSI, there were 431 super-elderly patients (7.3%, 431/5944) aged 85 years or older (≥85 years old) enrolled in this study. Those patients admitted prior to 2014 were not enrolled in this study because many data related to clinical characteristics required for statistical analysis in this study were not available. And all the following clinical and the microbiological data of these 431 super-elderly patients with BSI were respectively collected by reviewing the RT-NISS system mentioned above.
Clinical Features of These 431 Super-Elderly Patients with BSI
All the following clinical data were collected from the medical database by reviewing the RT-NISS system. (1) Demographics: age (grouped as 85–89, 89–94 and ≥95 group), gender (male or female), body mass index (BMI), and the onset date of BSI (the date when the positive blood culture was drawn). (2) qSOFA score (quick sepsis related organ failure assessment score), which was evaluated based on medical records within 24 h after the onset of BSI. (3) Comorbidities at the onset of BSI: ischemic cerebrovascular disease, cardiovascular disease (insufficient cardiovascular blood supply with clinical evidence, such as electrocardiogram and myocardial enzyme abnormalities), pulmonary infection, diabetes mellitus, chronic liver failure with abnormal serum alanine aminotransferase (ALT), chronic renal failure with abnormal serum creatinine (SCr), haematologic malignancy, and neutropenia, solid tumor such as lung cancer and liver cancer. (4) Treatments within 14 days prior to the onset of BSI: indwelling central venous catheter (CVC), indwelling urinary catheter, surgery (including trauma), invasive mechanical ventilation (tracheostomy or tracheal intubation), chemotherapy, renal replacement therapy including hemofiltration and dialysis, total parenteral nutrition, glucocorticoid therapy (defined to the use of methylprednisolone > 1 mg·kg−1·day−1 or equivalent glucocorticoid for at least 2 days), and broad-spectrum antibiotics (defined as the third-fourth generation cephalosporins and carbapenems). (5) Laboratory test results: inflammatory markers within 24 hours before and after the onset of BSI including the numbers of leukocyte counts and neutrophils counts. (6) Antibiotics used for empirical antimicrobial therapy within 72 h after the onset of BSI. Additionally, empirical antimicrobial therapy was also considered appropriate if the clinical symptom (temperature > 38°C) recovered to normal (temperature < 38°C) within 72 h after empirical antibiotic therapy. (7) Outcomes (poor prognosis): 7-day short-term mortality and the 30-day long-term mortality. Some patients lacked the data about the outcome in the database because they had been discharged before 7 days or 30 days, and their outcome data were obtained by telephone follow-up.
Microbiological Data of These 431 Super-Elderly Patients with BSI
The microbiological data to be collected mainly including the species that caused the BSI among these 431 super-elderly patients and drug susceptibility to antibiotics of these species. The BSI were divided into fungaemia or bacteraemia, and the bacteria were mainly categorized as gram-positive cocci, gram-negative bacilli and a few other types of bacteria. In addition, the antibiotic susceptibility profiles of the bacteria were also collected and presented in detail in this study.
Statistical Analysis
Categorical variables were exhibited as frequency counts and percentages (n, %). According to whether the data met normality, continuous variables were exhibited as the mean (standard deviation, SD) or median (interquartile range, IQR). To explore the risk factors for the 7-day mortality and the 30-day mortality, we used univariate regression analysis to screen for the possible risk factors and used multivariate regression analysis to identify the independent risk factors. All variables significant (P<0.05) in univariate analysis were included in the multivariate logistic regression analysis. All statistical analyses were performed using SPSS 22.0 software (IBM Corp., Armonk, NY, USA) and all results with a 2-tailed P-value < 0.05 were considered significant.
Results
Typical Clinical Features of These 431 Super-Elderly Patients with BSI
At last, out of 5944 adult-patients with BSI, there were totally 431 super-elderly patients enrolled in this study from January 1, 2014 to December 31, 2019. In this study, all the clinical data of these 431 super-elderly patients with BSI was collected by reviewing the electrical medical database (the RT-NISS system). As shown in Table 1, all these super-elderly patients with BSI were 85 years or older, and the mean age was 88.4 (2.7) years old. Among these patients, age ≥90 years old accounted for 31.1% (134/431). In addition, 40 out of these 431 super-elderly patients (9.3%, 40/431) were diagnosed with BSI within 48 hours after the admission and were defined as community-acquired BSI. The remained 401 super-elderly patients (90.7%, 401/431) were defined as hospital-acquired BSI because they were diagnosed with BSI after 48 hours of hospitalization.
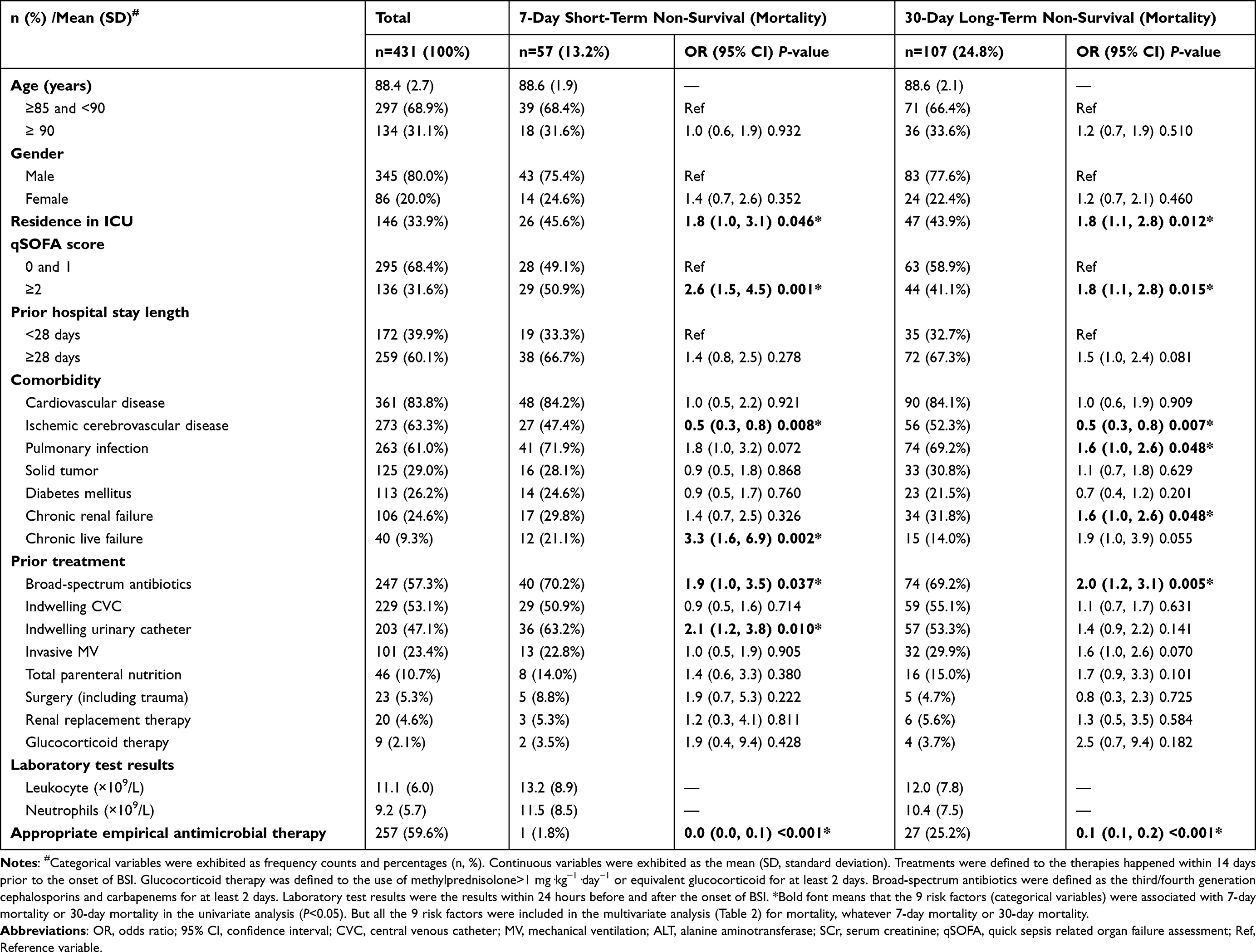 |
Table 1 The Typical Clinical Features and Univariate Analysis of Risk Factors for 7-Day Short-Term Mortality and 30-Day Long-Term Mortality Among These Super-Elderly Patients with BSI |
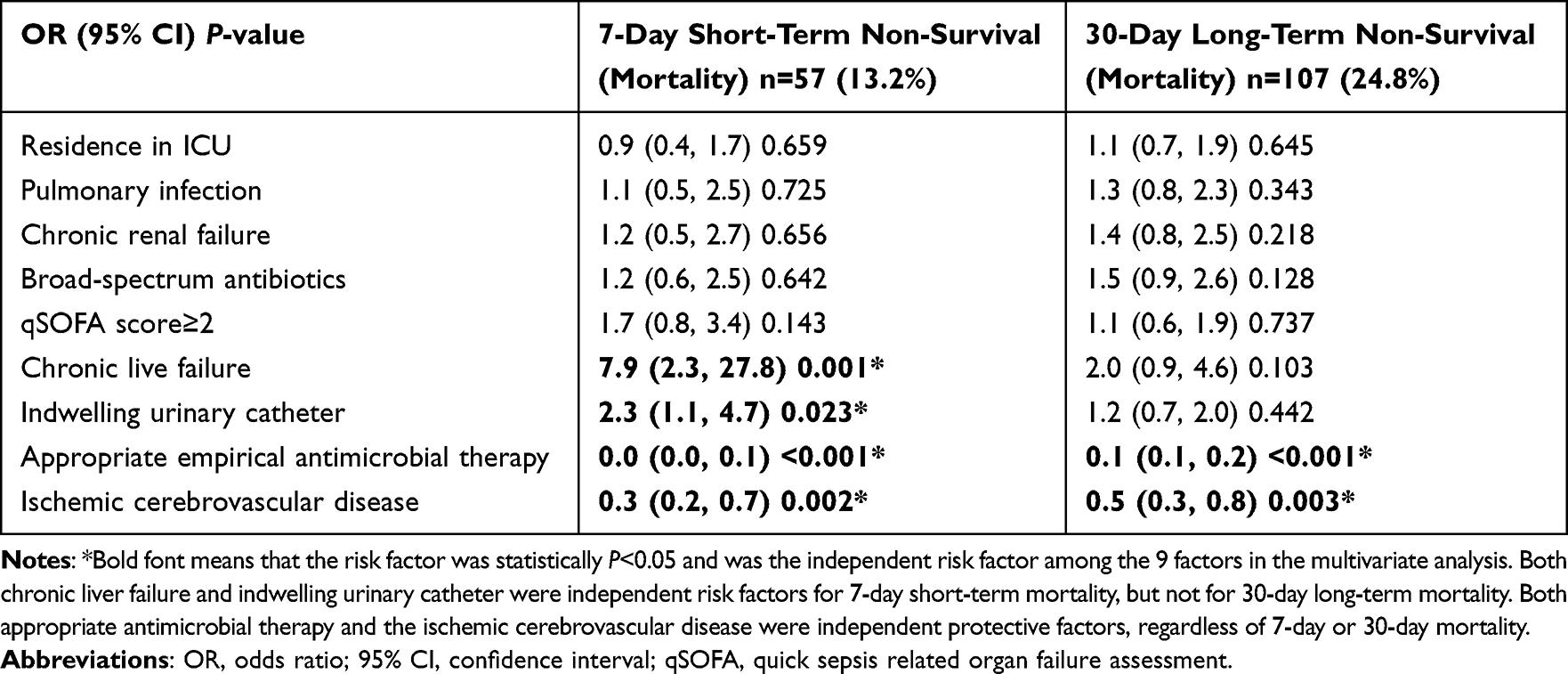 |
Table 2 The Multivariate Logistic Regression Analysis of Risk Factors for 7-Day Short-Term Mortality and 30-Day Long-Term Mortality Among These Super-Elderly Patients with BSI |
These super-elderly patients with BSI were typically characterized by the high proportion of patients with various underlying comorbidities, such as cardiovascular disease (83.8%, 361/431), ischemic cerebrovascular disease (63.3%, 273/431), pulmonary infection (61.0%), chronic renal failure (24.6%), diabetes mellitus (26.2%), chronic liver failure (9.3%), and solid tumor (29.0%). The proportion of these super-elderly patients who had been hospitalized for ≥28 days prior to the onset of BSI was up to 60.1% (60.1%, 259/431), and the residence in ICU at the onset of BSI accounted up to 33.9% (33.9%, 146/431).
In addition, the proportion of these super-elderly patients who had used broad-spectrum antibiotics for more than 2 days within 14 days before the onset of BSI was high up to 57.3% (247/431), and the proportions of patients who had received various invasive treatments were also high, such as indwelling CVC (53.1%, 229/431), indwelling urinary catheters (47.1%, 203/431), invasive mechanical ventilation (23.4%, 101/431), and total parenteral nutrition support (10.7%, 46/431). Unfortunately, due to all of the above features, these super-elderly patients with BSI were relatively severe, and the proportion of patients with a qSOFA score ≥2 was up to 31.6% (136/431).
Mortality of These Super-Elderly Patients with BSI and Associated Risk Factors
Due to the above clinical characteristics of these super-elderly patients with BSI, the mortality of these super-elderly patients after the onset of BSI was extremely high, regardless of the short-term 7-day mortality (13.2%, 57/431), or the long-term 30-day mortality (24.8%, 107/431).
As shown in Table 1, about the risk factors associated with the high mortality, the univariate analysis showed that residence in ICU, the qSOFA score≥2, ischemic cerebrovascular disease, chronic liver failure, the use of broad-spectrum antibiotics for more than 2 days within 14 days before the onset of the BSI, indwelling urinary catheter, and appropriate empirical antimicrobial therapy were all associated with the 7-day short-term mortality (P<0.05). And except these risk factors above, both pulmonary infection and chronic liver failure were also associated with 30-day mortality (P<0.05).
To assess the independent value of these potentially risk factors for mortality after the onset of BSI among these super-elderly patients, we included all the 9 risk factors described above into the multivariate logistic regression analysis to screen the independent risk factors for 7-day short-term and 30-day long-term mortality. As shown in Table 2, among these super-elderly patients, both the chronic liver failure (OR 7.9, 95% CI 2.3–27.8, P=0.001) and indwelling urinary catheter (OR 2.3, 95% CI 1.1–4.7, P=0.023) were independent risk factors for 7-day short-term mortality after the onset of the BSI. However, both the chronic liver failure (OR 2.0, 95% CI 0.9–4.6, P=0.103) and indwelling urinary catheter (OR 1.2, 95% CI 0.7–2.0, P=0.442) were no longer independent risk factors for 30-day long-term mortality. And simultaneously, the multivariate logistic regression analysis also showed that both appropriate empirical antimicrobial therapy and the ischemic cerebrovascular disease were independent protective factors, regardless of 7-day or 30-day mortality.
The Microbiology results of the 431 Super-Elderly Patients with BSI
The 431 species distribution caused the BSI among these 431 super-elderly patients were shown in Figure 1. The results showed that there were totally 391 bacteria strains (81.4%, 391/431) and were classified as Gram-positive cocci (GPC, 58.5%), Gram-negative bacilli (GNB, 29.9%) and few other types of bacteria (3.0%, Gram-negative cocci and Gram-positive bacilli). The rest were Fungi (8.6%, 37/431), but all these fungi were Candida albicans in this study. The top four most common species of GPC were Staphylococcus hominis (18.3%, 79/431), Staphylococcus epidermidis (11.8%, 51/431), Enterococcus faecium (6.5%, 28/431) and Staphylococcus aureus (4.2%, 18/431). The four most common species of GNB were Escherichia coli (9.7%, 42/431), Klebsiella pneumonia (9.3%, 40/431), Acinetobacter baumannii (2.3%, 10/431) and Pseudomonas aeruginosa (2.3%, 10/431). In addition, the antimicrobial susceptibility detailed results of the resistance to all the 8 antibiotic categories of all the 391 strains were shown in Table 3. The result showed that the resistance rate of each antibiotic was high among these 391 bacteria strains; however, none of these 391 strains was resistant to linezolid or vancomycin.
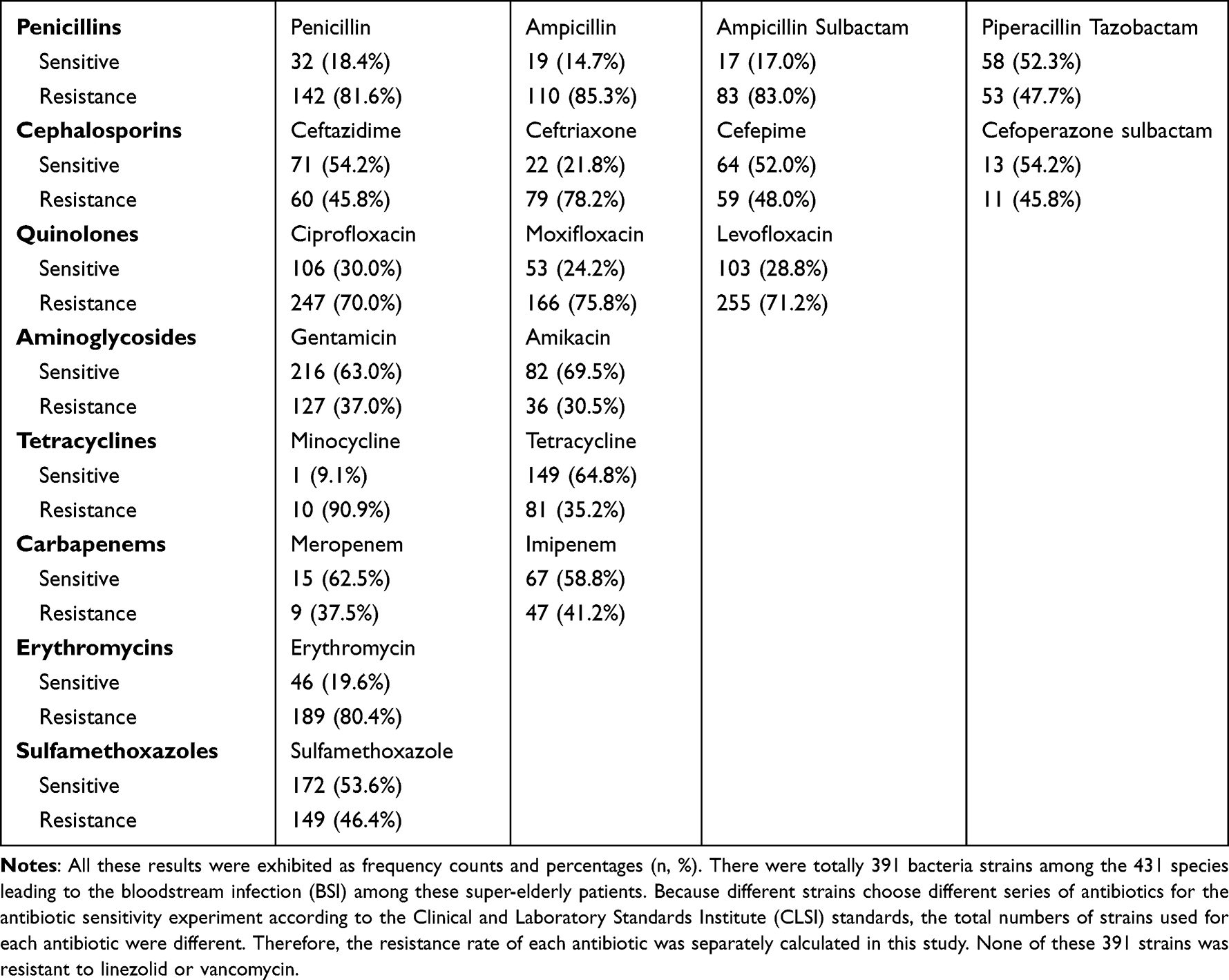 |
Table 3 The Antibiotic Susceptibility of All the 391 Bacteria Strains Out of 431 Pathogenic Species Leading to These Super-Elderly Patients with BSI |
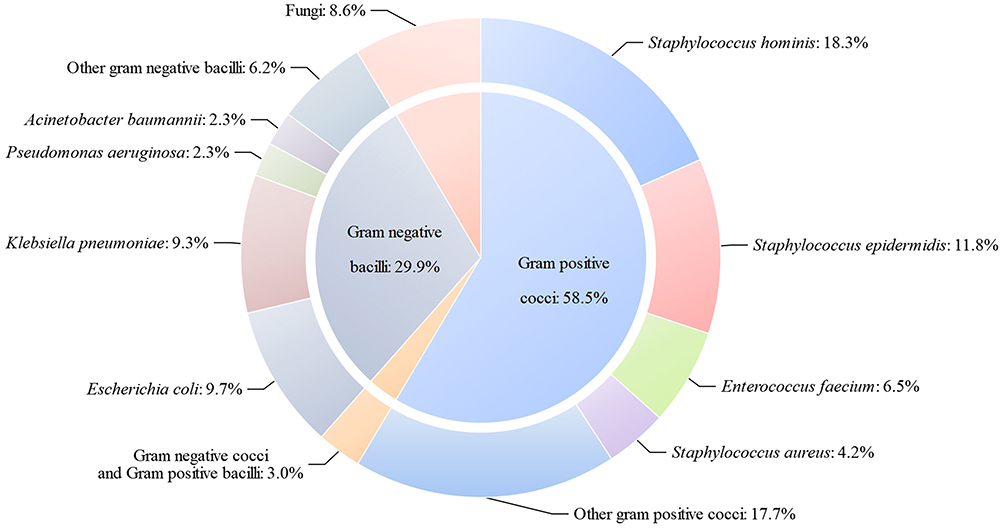 |
Figure 1 The species distribution caused the BSI among these 431 super-elderly patients. There were totally 391 bacteria strains (81.4%, 391/431) and were classified as Gram-positive cocci (58.5%), Gram-negative bacilli (29.9%) and few other types of bacteria (3.0%, Gram-negative cocci and Gram-positive bacilli). The rest were Fungi (8.6%, 37/431), but all these fungi were Candida albicans in this study. |
Discussion
Aging becomes more and more serious and brings challenges to the world with the increased average human life expectancy.14–16 Characterized by rapid progression and high mortality, bloodstream infection (BSI) are more lethal for super-elderly patients who are relatively more vulnerable. And the prevention and treatment of BSI among super-elderly patients have been attracting more and more attention in modern aging society. For the above reasons, we conducted this study among super-elderly patients with BSI, and at last, a total of 431 super-elderly patients with BSI in the past 6 years were included in the study.
Our research data showed that these 431 super-elderly patients with BSI were all over 85 years old and nearly 1/3 were over 90 years old. Just due to their super-elderly age, the proportion of patients with one or more underlying comorbidities was very high, which is a typical common feature of these super-elderly patients with BSI. Our data showed that far more than half of these patients had a history of various cardiovascular diseases (83.8%), ischemic cerebrovascular diseases (63.3%) and/or pulmonary infection (61.0%). Apart from these comorbidities, the other typical feature of these super-elderly patients with BSI was that most (60.1%) of these patients had been hospitalized in the hospital for long time (>28 days) before the onset of BSI, and these patients who had received invasive various treatments were also more than other ordinary younger patients, such as indwelling central venous catheters (53.1%), indwelling urinary catheter (47.1%), invasive mechanical ventilation (23.4%) and total parenteral nutrition (10.7%). In addition, most (57.3%) of these super-elderly patients had used broad-spectrum antibiotics for various infectious diseases within 14 days before the onset of BSI.
All of these adverse features above are risk factors for causing BSI and may make super-elderly patients with low immunity more vulnerable to BSI, just has been proved in many literatures.17–20 And simultaneously, these adverse risk factors above were also related to the more severity of these super-elderly patients. Our results showed that the proportion of patients with a qSOFA score ≥ 2 was high up to 31.6% (136/431), which is a score closely associated with poor prognosis of various infection, including BSI,21 especially sepsis and sepsis shock.22 As a result, these super-elderly patients with BSI were also more prone to be residence in ICU (66.1%, 285/431) at the onset of BSI, which was also a risk factor for the development and mortality of BSI.5,23 And for the severity, the 30-day mortality reached high to nearly 1/4 (24.8%, 107/431) and the 7-day mortality rate also reached 13.2% (13.2%, 57/431) among these super-elderly patients with BSI.
The qSOFA score above we used in this study was a fast and simple scoring system used to evaluate the severity and prognosis of sepsis patients, the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) and several validation studies have proven that the ability of the qSOFA score to predict in-hospital mortality.24,25 In addition, further research had also suggested that a qSOFA score ≥2 was strongly associated with mortality among patients with infections and patients with pneumonia.26,27 However, a systematic review and meta-analysis found that positive qSOFA scores had a high specificity (0.83) for in-hospital mortality and could be used as a clinical tool to promptly identify patients with infection likely to develop adverse outcomes in patients with suspected or confirmed infection outside the ICU, but its sensitivity was very low (0.51). Similarly, the sensitivity of positive qSOFA scores in predicting acute organ dysfunction and predicting ICU admission were also low.25 Fortunately, this study also points out that the sensitivity of a positive qSOFA score would be enhanced when critically ill patients with sepsis or septic shock, and the sensitivity would also be increased when the overall mortality >10%. Due to the low sensitivity of a positive qSOFA score, the use of the qSOFA score to evaluate the morality or severity also had the corresponding limitation in our study. Some patients with severe illness or poor prognosis might mistakenly display as low qSOFA score, which might lead to bias in our research results. However, because the majority of our patients were hospital acquired BSI and a large portion of them reside in the ICU, with an overall mortality rate of 13.2% within the short-term 7 days and up to 24.8% within long-term 30 days, the low sensitivity of a positive qSOFA score might be increased in our study and should not be too low to affect the accuracy of our results.
About the extremely high mortality, we also screened the potential risk factors associated with the poor prognosis of these super-elderly patients with BSI. Based on the 9 the potential associated risk factors screened by the univariate analysis (Table 1), the multivariate analysis revealed that both the chronic liver failure (OR 7.9, 95% CI 2.3–27.8, P=0.001) and indwelling urinary catheter (OR 2.3, 95% CI 1.1–4.7, P=0.023) were independent risk factors for 7-day short-term mortality after the onset of the BSI (Table 2).
About chronic liver failure, its important role in mortality could be understood and accepted from the perspective of the normal function of liver and the adverse impact of chronic liver failure. Due to chronic liver failure, the liver detoxification function and the synthesis of essential nutrients and energy and are impaired, such as albumin, resulting in low immunity and easy acquisition of various infections including BSI.28 Simultaneously, many effective antibiotics that require liver metabolism cannot be used to cure BSI, which affects the treatment options and prognosis after infection. All these effects above might make liver failure an independent risk factor for poor prognosis of BSI, which had been confirmed in many BSI-related studies.29,30
Similarly, as the other independent risk factor, the indwelling urinary catheter was also easy to understand about its potential clinical value for 7-day mortality. A large number of studies had shown that indwelling urinary catheter itself was the main iatrogenic factor for urinary tract infection, and indwelling urinary catheter could easily cause urinary tract injury and spread urinary tract infection into blood, causing BSI.31,32 Moreover, because super-elderly patients often need long-term continuous use of indwelling urinary catheters and up to 47.1% of these super-elderly patients had been indwelling urinary catheters as showed in this study, urinary tract infections are more difficult to control because most pathogenic bacteria are hospital-acquired MDR bacteria and/or fungi.33 However, although chronic liver failure and indwelling urinary catheter were independent risk factors for 7-day short-term mortality after the onset of these super-elderly patients with BSI, both of them were not the independent risk factors for 30-day long-term mortality. The reason for this might was that the long-term prognosis of BSI was related to many factors, and there are various clinical interference factors of uncertain or unexpected in 30 days. Therefore, it is inappropriate and unreliable to evaluate the long-term prognosis of BSI by only two or several factors.
In addition to the clinical characteristics above, we had also summarized the pathogenic species causing BSI among these super-elderly patients. As shown in Figure 1, the common species were gram-positive cocci (GPC) (58.5%), while the Gram-negative bacilli (GNB) only accounted for 29.9%. This result was different with many previous literature reports. An investigation conducted in 10 large teaching hospitals from seven geographic regions across China in 2016 based on China Antimicrobial Surveillance Network (CHINET) showed that Gram-negative bacteria (67.5%) was far more than Gram-positive bacteria (29.6%), but the BSI in that study was the result of only blood cultures without ruling out contamination and colonization.34 Some studies had also shown that the proportions of Gram-negative bacteria and Gram-positive bacteria were similar, with Gram-negative bacteria slightly more than Gram-positive bacteria, regardless of community-acquired bloodstream infection35 or nosocomial bloodstream infection.36,37 However, all the mean ages of patients in those studies were far below 85 years old, while these super-elderly enrolled in this study were all over 85 years old. Similarly, reported in our previous study, which included all these super-elderly patients in this study, the proportions of GPC (45.9%) and GNB (42.8%) among 9381 episodes of patients with BSI of all ages were almost equal.4 Contrary to those researches above, there were far more GPC (58.5%) than GNB (29.9%) among these pathogenic bacteria causing these super-elderly patients with BSI in this study. This result clearly exhibited the typical feature of the species distribution among these super-elderly patients with BSI, which might be precisely related to the super-elderly age of these patients themselves. Of course, it might also be related to other reasons, such as weakened immunity or more invasive procedures, including indwelling central venous catheters, indwelling urinary catheters, indwelling gastric catheters, etc. However, for any reason, the typical feature about the species distribution among these super-elderly patients with BSI deserved more attention and further research.
Among these pathogenic species causing BSI among these super-elderly patients, we could find that many of them were the most common pathogenic species causing current nosocomial infections in China, such as Escherichia coli, Klebsiella pneumoniae and Staphylococcus aureus.38 At the same time, we also found that most of these pathogenic bacteria were related to various invasive treatments, and/or bacterial flora imbalance caused by broad-spectrum antibiotics, especially various opportunistic pathogenic species, which mainly lead to infection in immunocompromised conditions, such as CoNS, Enterococcus faecalis and Candida albicans. Moreover, as shown in Table 3, these pathogenic species were mostly resistant to common antibiotics. Therefore, all these results above indicated that these super-elderly patients were quite vulnerable to BSI and were also difficult to get effective anti-infection antibiotics.
Limitations
Since this study was a retrospective analysis of clinical data, there was a potential for bias and the bias was hard to completely control in this study. For example, the 30-day mortality in this study was nearly up to 1/4 (24.8%), but some mild or low-risk elderly patients with good prognosis who were actually BSI might not be diagnosed with BSI from the beginning because their condition was insufficient for blood culture, which might have increased the mortality in this study. In addition, this study was a single-center study with a limited number of patients, which might also cause bias in the statistical analysis of the results. However, we believe that, even if the mortality was overestimated due to these limitations, the potentially increased mortality will encourage us to pay more attention to the prevention and treatment of BSI among super-elderly patients to improve outcomes, and could serve as a reference data for further prospective studies to other researchers.
Conclusion
As a global social problem, aging is becoming increasingly serious in many countries, and the prevention and treatment of bloodstream infection (BSI) among super-elderly patients are relatively vulnerable. Through these super-elderly patients over 85 years old diagnosed as BSI in the past 6 years, we found that as the most immunocompromised population, these super-elderly patients with BSI had typical features, regardless of the significant high proportion of Gram-positive cocci about species distribution and their high antibiotic resistance to common antibiotics, or typical clinical features and their risk factors for poor prognosis after the onset of BSI. We believed that these typical features deserved more attention from clinical medical staff and might be useful for the prevention and treatment of BSI among super-elderly patients, especially in the current aging society with an increasing number of super-elderly patients in the hospital.
Abbreviations
BSI, bloodstream infection; CI, confidence intervals; OR, odds ratio; CVC, central venous catheter; MDR, multidrug resistance; SD, standard deviation; IQR, interquartile range; qSOFA, quick sepsis-related organ failure assessment; GPC, Gram-positive cocci; GNB, Gram-negative bacilli; ICU, intensive care unit.
Data Sharing Statement
The data of this study are not publicly available to avoid violating the privacy rules of the medical database in our hospital, but all data are available from the corresponding author for any reader if necessary.
Ethics Approval and Consent to Participate
This study complies with the Declaration of Helsinki and the Clinical Trial Ethics Review Committee of the Chinese PLA General Hospital approved this study. Since this study was a retrospective study and private information such as patient name and address, was not involved in the study, and therefore, formal consent was waived in our hospital.
Acknowledgments
We thank Dr Miaoyu Wang and Zhenfei Mo from the First Medical Center of Chinese PLA General Hospital for their important advice and suggestions on this work.
Funding
This research was supported by the National Key R&D Program of China (No. 2022YFA1104704).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Chen J, Ma H, Huang X, et al. Risk factors and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary-care hospital in China: an eight-year retrospective study. Antimicrob Resist Infect Control. 2022;11(1):161. doi:10.1186/s13756-022-01204-w
2. Mattei D, Baretta V, Mazzariol A, et al. Characteristics and outcomes of bloodstream infections in a tertiary-care pediatric hematology-oncology unit: a 10-Year Study. J Clin Med. 2022;11(3):880. doi:10.3390/jcm11030880
3. Sabé N, Maristany M, Tuells M, et al. Risk factors and outcomes of acute graft pyelonephritis with bacteremia due to multidrug-resistant gram-negative bacilli among kidney transplant recipients. J Clin Med. 2022;11(11):3165. doi:10.3390/jcm11113165
4. Cui J, Li M, Cui J, Wang J, Qiang X, Liang Z. The proportion, species distribution and dynamic trends of bloodstream infection cases in a tertiary hospital in China, 2010–2019. Infection. 2022;50(1):121–130. doi:10.1007/s15010-021-01649-y
5. Chen Y, Chen Y, Liu P, et al. Risk factors and mortality for elderly patients with bloodstream infection of carbapenem resistance Klebsiella pneumoniae: a 10-year longitudinal study. BMC Geriatr. 2022;22(1):573. doi:10.1186/s12877-022-03275-1
6. Lin H, Gao Y, Qiu Y, et al. Impact of age group on bloodstream infection risk evaluation in immunosuppressed patients: a retrospective, single-centre, 5-year cohort study. Aging Clin Exp Res. 2022;35(2):357–366. doi:10.1007/s40520-022-02299-2
7. Laupland KB, Pasquill K, Steele L, Parfitt EC. Burden of bloodstream infection in older persons: a population-based study. BMC Geriatr. 2021;21(1):31. doi:10.1186/s12877-020-01984-z
8. Posteraro B, De Angelis G, Menchinelli G, et al. Risk factors for mortality in adult COVID-19 patients who develop bloodstream infections mostly caused by antimicrobial-resistant organisms: analysis at a large teaching hospital in Italy. J Clin Med. 2021;10(8). doi:10.3390/jcm10081752
9. da Silva N, da Rocha JA, Do Valle FM, Silva A, Ehrlich S, Martins IS. The impact of ageing on the incidence and mortality rate of bloodstream infection: a hospital-based case-cohort study in a tertiary public hospital of Brazil. Trop Med Int Health. 2021;26(10):1276–1284. doi:10.1111/tmi.13650
10. Brooks D, Polubothu P, Young D, Booth MG, Smith A. Sepsis caused by bloodstream infection in patients in the intensive care unit: the impact of inactive empiric antimicrobial therapy on outcome. J Hosp Infect. 2018;98(4):369–374. doi:10.1016/j.jhin.2017.09.031
11. Chen X, Yang Y, Li Y, Chen J. Clinical characteristics and risk factors for death in patients with Candida bloodstream infection in intensive care unit. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021;46(7):719–724. doi:10.11817/j.issn.1672-7347.2021.201012
12. Zhang Y, Du M, Chang Y, Chen LA, Zhang Q. Incidence, clinical characteristics, and outcomes of nosocomial Enterococcus spp. bloodstream infections in a tertiary-care hospital in Beijing, China: a four-year retrospective study. Antimicrob Resist Infect Control. 2017;6:73. doi:10.1186/s13756-017-0231-y
13. Wang X, Guo Z, Zhang X, et al. Inappropriate empirical antibiotic therapy was an independent risk factor of pediatric persistent S. aureus bloodstream infection. Eur J Pediatr. 2022;182(2):719–729. doi:10.1007/s00431-022-04729-9
14. de Azeredo Passos VM, Champs A, Teixeira R, et al. The burden of disease among Brazilian older adults and the challenge for health policies: results of the Global Burden of Disease Study 2017. Popul Health Metr. 2020;18(Suppl 1):14. doi:10.1186/s12963-020-00206-3
15. Blagosklonny MV. No limit to maximal lifespan in humans: how to beat a 122-year-old record. Oncoscience. 2021;8:110–119. doi:10.18632/oncoscience.547
16. Iijima K, Arai H, Akishita M, et al. Toward the development of a vibrant, super-aged society: the future of medicine and society in Japan. Geriatr Gerontol Int. 2021;21(8):601–613. doi:10.1111/ggi.14201
17. Sakihama T, Tokuda Y. Use of peripheral parenteral nutrition solutions as a risk factor for bacillus cereus peripheral venous catheter-associated bloodstream infection at a Japanese tertiary care hospital: a Case-Control Study. Jpn J Infect Dis. 2016;69(6):531–533. doi:10.7883/yoken.JJID.2015.489
18. Liu Y, Cui BC, Pi CM, et al. Analysis of prognostic risk factors of bloodstream infections in Beijing communities: a retrospective study from 2015 to 2019. Mediterr J Hematol Infect Dis. 2021;13(1):e2021060. doi:10.4084/MJHID.2021.060
19. Huang F, Shen T, Hai X, et al. Clinical characteristics of and risk factors for secondary bloodstream infection after pneumonia among patients infected with methicillin-resistant Staphylococcus aureus. Heliyon. 2022;8(12):e11978. doi:10.1016/j.heliyon.2022.e11978
20. Moriyama K, Ando T, Kotani M, et al. Risk factors associated with increased incidences of catheter-related bloodstream infection. Medicine. 2022;101(42):e31160. doi:10.1097/MD.0000000000031160
21. Angioni D, Hites M, Jacobs F, De Breucker S. Predictive factors of in-hospital mortality in older adults with community-acquired bloodstream infection. J Frailty Aging. 2020;9(4):232–237. doi:10.14283/jfa.2019.45
22. Chen FC, Ho YN, Cheng HH, Wu CH, Change MW, Su CM. Does inappropriate initial antibiotic therapy affect in-hospital mortality of patients in the emergency department with Escherichia coli and Klebsiella pneumoniae bloodstream infections. Int J Immunopathol Pharmacol. 2020;34:2058738420942375. doi:10.1177/2058738420942375
23. Kumar A, Chaudhry D, Goel N, Tanwar S. Epidemiology of intensive care unit-acquired infections in a tertiary care hospital of North India. Indian J Crit Care Med. 2021;25(12):1427–1433. doi:10.5005/jp-journals-10071-24058
24. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
25. Song JU, Sin CK, Park HK, Shim SR, Lee J. Performance of the quick sequential (sepsis-related) organ failure assessment score as a prognostic tool in infected patients outside the intensive care unit: a systematic review and meta-analysis. Crit Care. 2018;22(1):28. doi:10.1186/s13054-018-1952-x
26. Jiang J, Yang J, Mei J, Jin Y, Lu Y. Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: a meta-analysis. Scand J Trauma Resusc Emerg Med. 2018;26(1):56. doi:10.1186/s13049-018-0527-9
27. Jiang J, Yang J, Jin Y, Cao J, Lu Y. Role of qSOFA in predicting mortality of pneumonia: a systematic review and meta-analysis. Medicine. 2018;97(40):e12634. doi:10.1097/MD.0000000000012634
28. Chang YC, Chen JS, Yin CH, Shin-Jung Lee S, Chen WC. Candidemia in hospitalized cirrhotic patients with bloodstream infection: a retrospective analysis and brief summary of published studies. J Chin Med Assoc. 2022;85(3):295–303. doi:10.1097/JCMA.0000000000000695
29. Cui J, Liang Z, Mo Z, Zhang J. The species distribution, antimicrobial resistance and risk factors for poor outcome of coagulase-negative staphylococci bacteraemia in China. Antimicrob Resist Infect Control. 2019;8(1):65. doi:10.1186/s13756-019-0523-5
30. Ngamchokwathana C, Chongtrakool P, Waesamaae A, Chayakulkeeree M. Risk factors and outcomes of non-albicans Candida bloodstream infection in patients with candidemia at Siriraj Hospital-Thailand’s largest national tertiary referral hospital. J Fungi. 2021;7(4):269. doi:10.3390/jof7040269
31. Choi MH, Kim D, Park Y, Jeong SH. Impact of urinary tract infection-causative microorganisms on the progression to bloodstream infection: a propensity score-matched analysis. J Infect. 2022;85(5):513–518. doi:10.1016/j.jinf.2022.08.039
32. Li C, Wang J, Wang Q, et al. Predictive value of a quick pitt bacteremia score for prognosis of patients with bloodstream infection secondary to urinary tract infection: a Retrospective Cohort Study. Infect Drug Resist. 2022;15:4381–4391. doi:10.2147/IDR.S373998
33. Gudiol C, Albasanz-Puig A, Laporte-Amargós J, et al. Clinical predictive model of multidrug resistance in neutropenic cancer patients with bloodstream infection due to Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2020;64(4). doi:10.1128/AAC.02494-19
34. Hu F, Yuan L, Yang Y, et al. A multicenter investigation of 2773 cases of bloodstream infections based on China antimicrobial surveillance network (CHINET). Front Cell Infect Microbiol. 2022;12:1075185. doi:10.3389/fcimb.2022.1075185
35. An R, Ou Y, Pang L, et al. Epidemiology and risk factors of community-associated bloodstream infections in Zhejiang Province, China, 2017–2020. Infect Drug Resist. 2023;16:1579–1590. doi:10.2147/IDR.S400108
36. Jiang ZQ, Wang SD, Feng DD, Zhang BX, Mao SH, Wu JN. Epidemiological risk factors for nosocomial bloodstream infections: a four-year retrospective study in China. J Crit Care. 2019;52:92–96. doi:10.1016/j.jcrc.2019.04.019
37. Cai L, Chen H, Wei Y, et al. Changing epidemiology, microbiology and mortality of bloodstream infections in patients with haematological malignancies before and during SARS-CoV-2 pandemic: a retrospective cohort study. BMJ Open. 2023;13(12):e078510. doi:10.1136/bmjopen-2023-078510
38. Hu F, Zhu D, Wang F, Wang M. Current status and trends of antibacterial resistance in China. Clin Infect Dis. 2018;67(suppl_2):S128–S134. doi:10.1093/cid/ciy657
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.