")
Back to Journals » International Journal of Women's Health » Volume 16
“SO FAR AWAY” How Doctors Can Contribute to Making Endometriosis Hell on Earth. A Call for Humanistic Medicine and Empathetic Practice for Genuine Person-Centered Care. A Narrative Review
Authors Cetera GE , Facchin F , Viganò P, Merli CEM, Frassineti A, Fiorini J, Somigliana E, Vercellini P
Received 16 September 2023
Accepted for publication 13 December 2023
Published 19 February 2024 Volume 2024:16 Pages 273—287
DOI https://doi.org/10.2147/IJWH.S440542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Giulia Emily Cetera,1,2 Federica Facchin,3 Paola Viganò,2,4 Camilla Erminia Maria Merli,1 Annalisa Frassineti,5 Jessica Fiorini,5 Edgardo Somigliana,2,4 Paolo Vercellini1,2
1Gynecology Unit, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy; 2Academic Center for Research on Adenomyosis and Endometriosis, Department of Clinical Sciences and Community Health, Università degli Studi di Milano, Milan, Italy; 3Department of Psychology, Catholic University of the Sacred Heart, Milan, Italy; 4Infertility Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy; 5Associazione Progetto Endometriosi Organizzazione di Volontariato, Reggio Emilia, Italy
Correspondence: Giulia Emily Cetera, Gynecology Unit, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, via della Commenda 12, Milano, 20122, Italia, Tel +392550352318, Email [email protected]
“SO FAR AWAY” * How Doctors Can Contribute to Making Endometriosis Hell on Earth
[* by Knopfler M. In Dire Straits. Brothers in Arms. Vertigo Records, U.K., 1985]
Abstract: The distance physicians may create within the relationship with their patients by not having a humanistic approach to their practice may strongly influence clinical outcomes. The purpose of this paper is to convey the well-known narrative of patient dissatisfaction into pro-action by discussing the aspects of dehumanization, which may occur in the relationship between physicians and women with endometriosis. Eight dimensions of dehumanization are examined and related to everyday scenarios occurring in endometriosis care settings and the possible downstream consequences on patients’ clinical outcomes are described. Objectification, which may come across as minimization of pain, may not only increase patients’ perception of pain but also lead to undertreatment of unrecognized forms of endometriosis, especially among adolescents. Passivity, that is not favoring shared decision-making nor self-management, may compromise adherence to treatment, reducing patients’ trust in physicians and quality of life. The same consequences may result from homogenization, that is giving for granted that all patients have the same access to care. Both isolation, ie not practicing therapeutic empathy, and loss of meaning, ie not supporting patients in the re-definition of their life plans, may affect women’s psychological wellbeing and further increase pain perception. Ignoring women’s personal journey by not providing clear information on the consequences endometriosis may have on their lives may favor women’s self-silencing. Not promoting an un-biased communication and not setting aside scientific polarization are the main features of dislocation, which may jeopardize patient empowerment. Lastly, having a reductionist approach to the body may contribute to chronicization of pain, thus compromising quality of life. This considered, taking time to listen to women with endometriosis and tailoring decisions on the basis of their individual needs should be fostered as a moral duty. Physicians should always keep in mind that they are not only deliverers of treatment; they are a form of treatment themselves.
Keywords: endometriosis, dehumanization, patient-centered care, treatment, phsycians’ role
Introduction
It has been estimated that around 50% of women with endometriosis are dissatisfied with the care they receive.1 Ineffective communication and a lack of centeredness on patients’ needs often strain the patient–physician relationship. Thereby, distance is created between the parties, determining a one-way dynamic in which women struggle to be listened to or to be believed, chasing a diagnosis or a satisfactory treatment, which often only the most enduring or fortunate are able to achieve.2,3
Although physicians appear to be partially aware of such a dysfunctional relationship, and although more attention in these regards has been recommended by the scientific community for the last twenty years,4,5 no substantial improvement seems to have occurred, thus suggesting that junior doctors are perpetuating their predecessors’ dehumanizing attitude.5–7
What has advanced in the last decades is patients’ ability to resort to alternative solutions. Social networks are a popular source of health information for many, especially for younger generations, which are also those who experience endometriosis care as less person-centered.8 Around 40% of young people search TikTok or Instagram before Google6 and among the top 100 TikTok videos on endometriosis – which account for more than 300 million views – 24% highlight distrust in healthcare and 80% of those discussing hormonal treatment do so in a negative way.9 Making up only 5% of content creators, physicians appear to be one step behind their patients, who, as a result, may search for solutions outside traditional healthcare channels, further increasing the communication gap.9,10
It must be remarked that it is undoubtedly challenging for physicians to be able to adequately support all of their patients and to efficiently address each of their individual needs, considering hospitals’ strict time schedules, the burden of paperwork and not least the fear of litigation. Moreover, the expression of therapeutic empathy and humanizing practices requires not only physicians’ will to facilitate personal interaction but also patients’ openness to communication and healthcare managers being committed to value the time clinicians spend caring for their patients.11
However, patient satisfaction with medical support is essential, as it strongly influences quality of life, compliance to treatment and patients’ ability to cope with their disease.1,8,12,13 Physicians are de facto a form of treatment themselves and as such it is fundamental they realize that, like any other kind of therapy, they entail benefits and harms.
The purpose of this paper is to discuss all aspects of dehumanization, which may occur in the relationship between physicians and patients with endometriosis, thus jeopardizing its intrinsic therapeutic role. Raising clinicians’ awareness towards the need of person-centered care may in fact shorten the distances within this often dysfunctional, yet critical relationship. Our aim is to convey the well-known narrative of diagnostic delay and of patient dissatisfaction into pro-action.
Dehumanizing and Corresponding Humanizing Aspects in Endometriosis Management
Philosophically, dehumanization is defined as the denial to people of their humanness,14 which may be considered in terms of uniquely human qualities (ie, cognitive skills, ethics, moral sensitivity, socialization and intelligence) or in terms of characteristics that constitute human nature (ie, emotionality, warmth, curiosity, agency). The denial of uniquely human attributes represents individuals as animal-like, while the denial of human nature represents others as objects.15
Translated into clinical practice, dehumanization consists in the impoverishment of communication and interaction, which instead sustain and enrich the patient–physician relationship.16 Practically, dehumanization makes patients unworthy of moral concern, of compassionate care, of a dialectical encounter and of shared decision-making. Clearly, dehumanization in medical practice is usually not a deliberate choice, rather a coping strategy17 or the result of the passive perpetuation of the paternalistic attitude, which traditionally has often characterized the medical professional.18,19
In 2009, Todres and co-workers described eight dimensions of dehumanization in healthcare (objectification, passivity, homogenization, isolation, loss of meaning, loss of personal journey, dislocation and reductionist body) (Table 1) and a corresponding number of humanizing dimensions (insiderness, agency, uniqueness, togetherness, sense-making, personal journey, sense of place, embodiment). The authors suggest physicians use the humanizing dimensions not as dogmas, rather as touch-stones for awareness, while keeping in mind the complexity of lived situations.18 In fact, the eight couples of dehumanizing/humanizing dimensions are not separate but imply one another and within clinical practice they are more easily found along a spectrum of possibilities which go from one extreme (total dehumanization) to another (total humanization) than in their absolute form.18
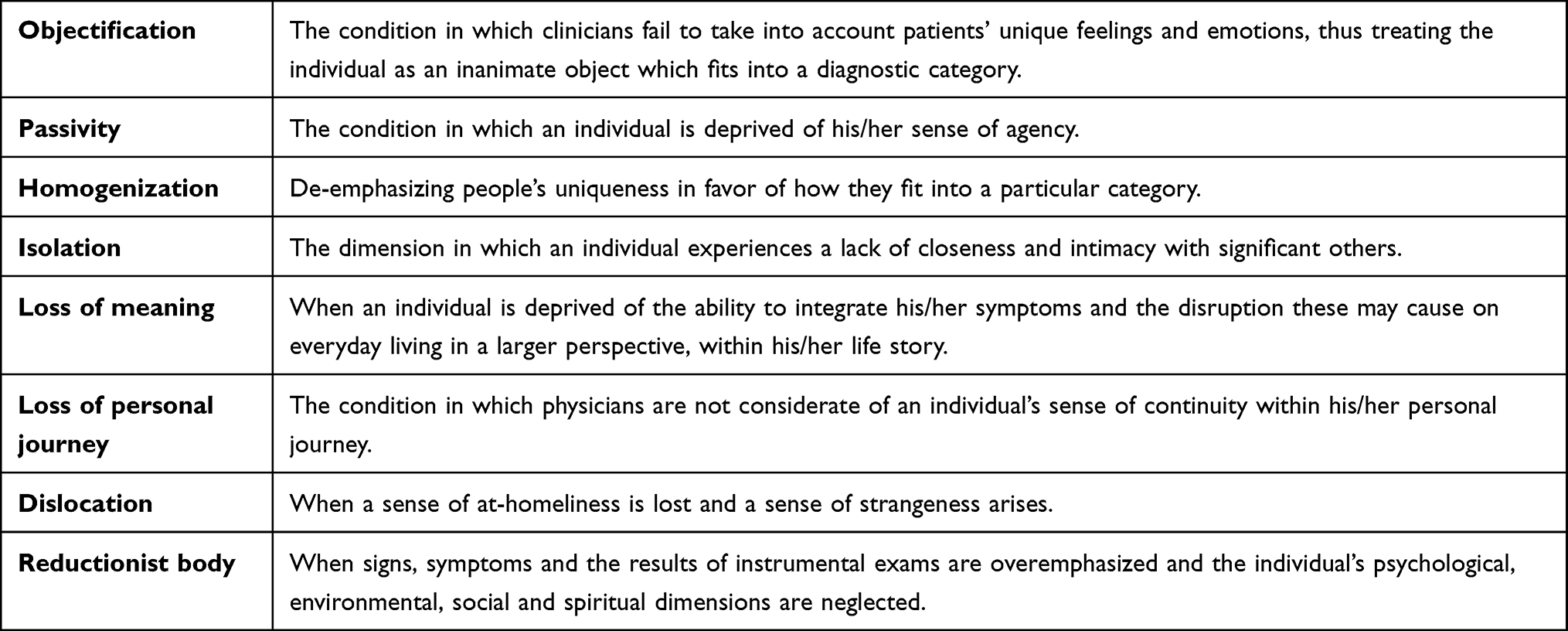 |
Table 1 The Eight Dimensions of Dehumanization as Described by Todres and Co-Workers |
Moving from Todres and colleagues’ work, we herein analyze in which terms the eight dimensions of dehumanization apply to the clinical management of women with endometriosis (Figure 1) and examine the possible downstream consequences they may determine on patients’ clinical outcomes, suggesting pro-active solutions.
 |
Figure 1 Women with endometriosis’ perception of dehumanization in clinical practice. (A) objectification; (B) passivity; (C) homogenization; (D) isolation; (E) loss of meaning; (F) loss of personal journey; (G) dislocation; (H) reductionist body. |
Objectification
Todres and co-workers define objectification as the condition by which clinicians fail to take into account individuals’ unique feelings and emotions, thus treating the individual as an inanimate object which fits into a diagnostic category. Only individuals themselves are authorities on the entity of their inner feelings and on the consequences such feelings determine on their every day life. Overstepping such authority is a further feature of objectification.18
Common examples of objectification in the management of women with endometriosis are normalization and psychologization of pain.19 These two concepts are expressions of the same phenomenon that is minimization of pain. Much has been said already in this regard, being the literature and the media overflowing of data and opinions. Our aim is to discuss minimization from a pro-active perspective.
Although it appears that compared to men, women have lower pain thresholds,19–21 and although it is culturally more accepted for women to show pain,22 it has been proven that women receive less pain relief22–24 and more antidepressants25,26 and referrals to mental health professionals27 than men. Accordingly, despite up to 61% of women with endometriosis experience difficulties in daily activities and self-care due to endometriosis-related symptoms,28,29 chronic pelvic pain is often trivialized by clinicians30,31 and sometimes normalized by women themselves.1
Minimizing pain may entail two main consequences: misdiagnosis (and as such perpetuation of pain; missing out on proper treatment; and chronicization of pain contributors); and the establishment of a vicious circle by which individuals who feel psychologized by health professionals are more prone to distress, which further increases physicians’ conviction their pain “is all in their heads”.24
Minimization of pain may be particularly frequent in cases of superficial endometriosis and among adolescents.32 In the former case, minimization may arise from the fact that lesions are less easily detectable. In the latter, it may origin from a low awareness of endometriosis in teenagers, both among medical professionals33 and among patients, who often consider menstrual pain an inevitable manifestation of menses.34 Moreover, in young girls with endometriosis, the disease is frequently in an early stage.35
In Martire and co-workers’ study on 270 adolescents, 21% of those reporting dysmenorrhea, 33% of those with dyspareunia and dyschezia and 44% of those with bowel symptoms had ultrasonographic signs of endometriosis.32 Together with nausea, dizziness and headache during menses, bowel symptoms are in fact considered red flags for endometriosis in adolescents.33,36 A positive family history for endometriosis, frequent absenteeism from school during menses, prolonged use of non-steroidal anti-inflammatory drugs and prescription of oral contraceptives before 18 years of age to treat severe dysmenorrhea are further red flags.35,37 These findings should be kept in mind when evaluating young individuals with chronic pelvic pain, as an earlier detection of endometriosis could yield better outcomes in terms of pain, fertility and mental health.38
Authors suggest that a progestin monotherapy or a combined estro-progestin therapy should be commenced in all presumptive diagnoses of endometriosis, ie in those situations in which a clinical suspicion of endometriosis (suggestive symptoms and/or anamnesis) is not supported by clinical or radiologic findings.39 In these cases, endometriosis should be considered as the cause of the individual’s pelvic pain until proven otherwise and both adolescents and adults should be treated accordingly.40
According to some, prescribing empiric hormonal treatment to individuals with a presumptive diagnosis of endometriosis may perpetuate the significant delay in diagnosis by masking symptoms.41 It may be argued, however, that an early treatment has a greater beneficial effect on clinical outcomes, as compared to an early diagnosis.
In any case, an early diagnosis should always be considered as a clinical goal as it allows the treatment of all pain contributors, which include chronic systemic inflammation, peripheral sensitization, central sensitization (CS), myofascial contributors and psychological contributors, alongside nociception.42 These factors are strictly intertwined and influence one another in such a way that the treatment of one pain contributor should not preclude the treatment of the others.43 In Sieberg and co-workers’ words, “conceptualizing chronic pelvic pain associated with endometriosis as a peripherally driven phenomenon is a disservice to the millions of women suffering from this disease. Simply removing lesions […] is not going to fix the problem”.44 As such, pain management should be tailored and include variable combinations of hormonal treatment, surgery, psychological therapy, physical therapy, sexual therapy and pharmacological treatment of central pain.45 Multimodal treatment for endometriosis will be discussed more extensively further on in the manuscript.
Passivity
Passivity is defined as the condition in which an individual is deprived of his/her sense of agency. Experiencing oneself as making choices and being held accountable for one’s actions is closely linked to the human sense of dignity and being deprived of such dignity determines a diminished sense of personhood.18
In the management of women with endometriosis, passivity may come across as not promoting shared decision-making and as not enabling self-management. The difference between the two may appear subtle but is substantial. Shared decision-making requires the patient to express her preferences and priorities and to contribute to the definition of the approach which best fits her needs, whereas self-management is a consequence of shared decision-making and consists in the patient actively taking part in her own therapeutic process.
Although traditionally the patient and his/her body have been seen as passively subjected to internal (diseases) and external (physician’s decisions) forces,18 awareness regarding the need for greater patient empowerment is increasing at a global scale. The call is also on junior doctors, who are often taught and feel that “the correct thing to do” is to follow guidelines, rather than making decisions tailored to individuals’ needs and preferences.46
In fact, patient empowerment appears to positively influence not only quality of life and patient satisfaction, regardless of symptom reduction,47 but also trust in physician competence, adherence to treatment and the ability to remain integrated in society despite suffering from a chronic pain condition.48,49
Taking into account individual needs, personal beliefs and life projects during the medical encounter is the groundwork for shared decision-making.
The establishment of an open and sincere conversation may sometimes be challenging, however it has been proven that when patients perceive that their clinician cares about them and is interested in them as a person, they are more prone to be active in the encounter and are also more adherent to treatment.50,51
Consciousness should be raised to a further sly element, which may compromise the patient–physician encounter that is stereotyping. Categorizing is an adaptive strategy all humans use to make the world more manageable,52 especially in complex situations, as is the context within physicians' work, having to make quick judgments and carry out complex tasks in a limited amount of time.53,54 Although physicians expect themselves to be untouched by patients’ social and demographic characteristics, research suggests that these do influence their judgments.55,56 For example, individuals with a lower socioeconomic status are more often rated by clinicians as being at risk of non-compliance with medical advice and black people are less likely to be perceived as being intelligent and educated than white people.57 This may create a vicious circle by which individuals with a lower socioeconomic status are discouraged from actively engaging with their physician, thus reinforcing his/her beliefs regarding their cognitive ability.58–60
Self-management comes with providing individuals with comprehensive knowledge on their condition, supporting their acquisition of skills to manage symptoms and by promoting coping mechanisms, including social and emotional adjustments, when needed.47 The objective is to contrast patients’ dependency upon medical decisions by facilitating a proactive attitude and by helping the woman see her disease not as a dominating force but rather as a –certainly uninvited – life companion. A trusting alliance and collaboration between woman and physician are essential for such processes to take place.61
As many as 76% of Australian women with endometriosis use self-management strategies, including heat, rest, meditation, cannabis and diet modifications to cope with pain.62–64 Evidence regarding the efficacy and the potential harms of these self-management strategies is scarce, however their use should not be discouraged in principle, as they appear to be associated to an improvement in women’s quality of life.65
Moreover, as what specifically regards dyspareunia, coping may be promoted by actively including patients in the clinical examination. In fact, helping patients identify the location of specific painful areas enables them to adopt sexual positions that do not provoke the mechanical stimulation of endometriotic foci or of muscular tender points. For example, avoiding rear entry positions, which stimulate the posterior fornix and the rectum, potentially reduces nociception deriving from endometriotic lesions infiltrating the posterior compartment.66,67
Homogenization
According to Todres and co-workers, homogenization consists in de-emphasizing people’s uniqueness in favor of how they fit into a particular category. Patients are often considered as epiphenomena of their own illness rather than as individuals and as such may be treated as similar or interchangeable with other individuals who belong to their same diagnostic category.18
Applied to women with endometriosis, homogenization may translate both into a lack of attention to patients’ needs and priorities, as has been extensively analyzed in the previous paragraph, and in a scarce promotion of inclusive healthcare.
Although in countries with a national health system the pressure of the economics of treatments may be less tangible, it should never be given for granted that all persons have the same access to care. It has been estimated that in 2021 in the USA 8% of adults were not compliant to prescribed treatments due to their cost and that women and black people were the most vulnerable in such sense.68 Women and people with a low socio-economic status are also the individuals among which chronic pain conditions are more prevalent.69
There are two main ways in which physicians may be bearers of more inclusive healthcare: by making sure prescribed treatments are accessible for all individuals and by promoting a rational use of healthcare resources.
Socioeconomic factors influence access to care not only at an individual level but also at a national level. Less wealthy public health services may not be able to afford prolonged treatments with expensive drugs for everyone70 and, in general, favoring costly treatments which are not justified by ascertained and long-lasting benefits may dissipate health systems’ resources which could be invested in a more efficient manner.
As regards endometriosis specifically, both second-line medical treatments such as GnRH agonists and antagonists and surgical treatment are burdened by considerable costs, as compared to first-line medical treatment.71 Moreover, such treatments are often insufficient on their own. Thus, considering that the incremental benefit of such treatments is yet to be clearly defined, their use on a large scale may not be justified, especially in low-income countries.71
Instead, authors recommend the adoption of a stepwise approach, prescribing GnRH agonists and antagonists only when first-line medical treatment with low-dose combined contraceptives and progestins is ineffective or contraindicated and reserving surgery to selected cases.72,73 Moreover, the cost of pharmacological treatment with GnRH agonists may be cut up to 30% by adopting depot formulations with extended-interval dosing regimens.71
Attention should be paid not only to expensive treatments but also to diagnostic tools. In the last years, there has been an increasing interest in the development of novel non-invasive tests for the detection of endometriosis using biological samples such as blood, urine and saliva.74 Although the availability of simple, easy to perform and supposedly accurate bio-molecular tests may seem attractive, at a closer glance their utility appears unclear. Among symptomatic individuals with clinical signs of endometriosis, a non-invasive test would be superfluous. Among asymptomatic women with no clinical signs of the disease, it is uncertain whether such a diagnostic tool would change clinical management. At the present moment, the only certainty is that it would increase the number of women with a diagnosis of asymptomatic endometriosis, presumably determining considerable psychological consequences and possibly causing overtreatment and financial opportunities for test manufacturers and dealers, pharmaceutical industries, private health services and many others. This said, the utility of non-invasive molecular tests would be restricted to the population of symptomatic women with a presumptive diagnosis of superficial peritoneal endometriosis. It is arguable, however, that in these cases, a thorough collection of medical history and a correct physical examination should be more than sufficient.74
This considered, it is desirable that the training of physicians includes a heightened awareness of both the impact different types of diagnostic tools and treatments have on healthcare resources and of the degree to which the choice of a specific diagnostic test or medical prescription can tip the balance in favor of an elitist or socially inclusive healthcare.
Isolation
Isolation is a dimension in which individuals experience a lack of closeness and intimacy with significant others. Everyday social connections are disrupted and a sense of alienation arises.18
Inevitably, diseases determine varying degrees of isolation and individuals with endometriosis are not exempt. Women often report a lack of understanding from family and friends due to the social stigma both on gynecological diseases and on chronic pain conditions.75,76 However, clinicians also play a critical role in patients’ feeling of alienation. Lack of eye contact, of expressivity and of touch, standing at the end of the patients’ bed rather than beside them, not remembering personal details are all determinants of isolation.77
Facilitating the typically human dimension of togetherness is possible by encouraging both empathy and social support.
Therapeutic empathy begins with active listening.11 Physicians have historically been trained to approach consultations using interrogative questioning, in order to frame patients’ issues in medical terms and limit time loss and digressions. However, this kind of attitude, which puts clinicians in a position of power, where they can steer the conversation, my potentially leave out critical information and silence patients’ version of reality.78 In 2000, Charon introduced the term “narrative medicine” to describe the discipline that conjugates humanities and medicine and aims to train clinicians in a reflective practice.79 Listening to patients’ entire story, as opposed to a list of symptoms, not only is possible but is vastly preferable. In fact, what physicians see in the time of the clinical consultation is just a moment of the story of a lifetime and attending to individuals’ health concerns means bringing together the events of their lives that form the context of the medical problem.80
Giving patients time to tell their story and express their feelings, emphasizing that they are being listened to, makes them feel validated, supported and respected,81 as well as reducing the entity of symptoms and down-regulating nociceptive processing, as reported in neuroimaging studies.82,83
However, carrying out therapeutic empathy is often more easily said than done. It has been estimated that 50% of clinicians’ time is spent updating electronic health records and that such use of time is an important contributor to burnout.84 Lack of time, having to constantly look at a screen rather than being able to make eye contact, as well as having difficulty managing one’s own emotions certainly does not facilitate the expression of therapeutic empathy. In any case, this should not be an invitation to remain oblivious to patients’ needs.
Clinicians are not the only ones involved in therapeutic empathy. It has been proven that among patients suffering from pain, the presence of a supportive other may be pivotal, regardless of his relation with the patient, being a clinician, a romantic partner, a friend or a stranger alike.85 It may in fact reduce patients’ pain-related stress response86 and alter neuroendocrine and haemodynamic responses, alleviating negative emotions87 and as such should never be discouraged.
Loss of Meaning
Sense making is a typically human characteristic. In varying forms and degrees, all human beings are motivated to find significance for events and experiences, connecting patterns and making wholes out of parts. In other words, humans are storytellers.18
In the medical context, patients feel the need to integrate their symptoms and the disruption these may cause on their everyday living in a larger perspective, within their life story. When such sense making is taken away, individuals can experience a sense of meaningless.18
Like all chronic illnesses, endometriosis may be a disruptive event, which leads to a rethinking of biography and to a shift from a perceived normal life trajectory to an abnormal trajectory. Up to 50% of women report that endometriosis has a negative effect on their work and career, 50% on their personal relationships and 16% on their education.88 Expectations and plans for the future may in some cases have to be re-examined89 and such interference on biographical continuity may be an important source of anxiety and depression.90 What is critical to safeguard mental health and to support individuals in the re-definition of their life plans, once again, is communication.
It has been proven that patients who find coping strategies are able to manage their pain better and experience a higher quality of life compared to those with a more passive attitude to the disease.47 It has also been proven that being well informed about one’s chronic disease supports coping.5
Endometriosis is characterized by uncertainty regarding its diagnosis, its treatment and its prognosis. However, not all of the uncertainty is inherent to the disease. Part of it originates from lack of communication.91
The importance of gaining feedback from patients regarding their perception of their disease is often overlooked48 and little attention is paid to how well they have understood what has happened, what is happening and will probably happen in their lives.92 Patients may feel it is best not to disclose their queries and fears, either because they believe nothing can be done, or they are reluctant to burden the doctor, who may manifest a blocking behavior, making patients feel it is not legitimate for them to express their concerns, or because they do not want to seem pathetic, or even for fear their worries will be confirmed.93 As a consequence, they may seek for pain relief by visiting the emergency room,94 or independently resort to alternative sources of information, such as the Internet, patient support groups or family and friends.91
However, independent access to information may be mined by two main issues: health literacy, ie, the degree to which individuals are capable to access, understand and use basic health information to promote good health;95 and the absence of established assurances of the quality of the vast quantity of health information which is easily accessible to the general public.96 As a consequence, independent collection of information may result in misinformation, which may lead to fear or negative expectations towards prognosis and treatments, mining the adherence to such treatments and their effectiveness.97,98
Thus, delivering clear, comprehensible, accurate, quantitative information through an honest encounter becomes an ethically significant act. Communicating the uncertainty inherent to endometriosis is also a moral duty.96 In these regards, Maguire’s six key tasks in communication with patients should always be kept in mind during the medical encounter: 1) defining the patient’s main problems, his/her perception of these and their impact on his/her life; 2) tailoring information and checking the patient has understood; 3) eliciting the patient’s reactions and concerns regarding the information he/she has received; 4) establishing how much the patient wants to be involved in decision-making; 5) discussing treatment options and their implications; 6) maximizing the chance the patient will be adherent to treatment and lifestyle changes.93
Lastly, recognizing the need for and suggesting psychological support to those who struggle to cope with their disease is a further task physicians should attain to.91
Personal Journey
Tightly connected to the concept of loss of meaning is the concept of personal journey. Humans are connected to a sense of continuity with the past while living in their present and while walking into their future. People look for the meaningfulness of their personal journey.18
In the medical encounter, there is often little space for consideration of patients’ sense of continuity, of how it is maintained or disrupted by their disease. The emphasis is usually on how the person is, more than on who the person is and this does not help patients feel how their care is linked to their history.18
The reasons for such behavior have been extensively analyzed in the previous paragraphs of this manuscript. Physicians are often burdened by paperwork, have to work on tight time-scales and often feel there is no time for biographical digressions. Patients, on the other hand, may feel dismissed, and dismissal leads to feelings of distrust and invalidation, negatively affecting the patient–physician relationship.77
In the modern society, women juggle between being workers, partners, mothers and care-givers.99 As it is, balancing work and family may be stressful and, in some cases, may be a source of anxiety, depression, insomnia and personal and work conflicts.100 By determining varying degrees of chronic pain, sexual dysfunction and infertility, endometriosis may jeopardize all aspects of a woman’s life, thus enhancing the work-family conflict.
Weather women are diagnosed with endometriosis in adolescence or in adulthood, it is physicians’ role to acquaint patients in these regards, providing clear and quantitative information on the consequences the disease may have on their future lives. For example, an alert about possible infertility may motivate women not to excessively procrastinate their desire for motherhood.32 In fact, although it is estimated that around 30–50% of women with endometriosis experience infertility, patients do not know if they lie within such percentage or not until they do not start trying to get pregnant.101 Deciding to try to conceive and when to do so entails a revision of one’s biography not only at an individual level but also at a couple level and as such requires negotiation, joint reflection and an adjustment of the romantic relationship.102,103 Informing women timely enables such decision processes to occur.
On the other hand, it must always be kept in mind that not all women wish to be mothers and different types of treatment addressing different aspects of the disease (pain versus infertility) should be prioritized accordingly.104 Moreover, it should always be taken into account that discussing motherhood and potential infertility may uncover patients’ sense of inadequacy and failure in their role as women and as such physician’s tact is never enough.103
Regardless of motherhood and regardless of their culture and of their religion, women are expected to be caring and self-sacrificing, even when in discomfort.105 This pressure may be emphasized by the taboo associated with gynecological conditions and menstruation in particular106 and may lead women to choose self-silencing over self-care.107 This may occur with cultural variations, depending on gender roles and expectations in different societies.108 The consequences of self-silencing may include poor mental health and quality of life,109 reduced treatment adherence,110 a feel of guilt for burdening significant others, and self-sacrifice.111 As such, it is physicians’ role to recognize these patterns, when they occur, to adjust patients’ treatment accordingly and, if needed, to help them obtain social support.
Dislocation
All humans need a habitat, which is a place where the feeling of at-homeliness becomes meaningful. Feeling at-home provides comfort, a sense of security and of unreflective ease. Dislocation occurs when such a sense of at-homeliness is lost and a sense of strangeness arises.18
In clinical settings, the quality of spaces is a determinant of privacy, dignity and of homeliness. However, spaces are not only created by their architecture but also by what happens within them.112
During the medical encounter, the perimeter of non-physical space is delimitated by two main actors (ie, the physician and his/her patient), both of whom may condition the sense of homeliness. Given the physician’s role of power in such encounter, it is his/her duty to make sure such sense of homeliness is safeguarded. Thus, his/her focus should be both on putting the patient at ease and on establishing an honest dialogue.
Each human being experiences the world in a different way, through the lenses that are determined by his/her biography. Rendering clinical information in a way that the recipient understands and feels as his/her own, intuiting what is meaningful for him/her is a first way to prevent the sense of dislocation, which may occur in the medical context.113
Once the patient is at ease, an honest dialogue may be established by conveying precise, quantitative information, by unveiling those issues for which certainty may not be established (ie, by addressing uncertainty), but also by setting aside scientific polarization and potential conflicts of interest.
According to Ploug and Holm, scientific polarization occurs when a scientific community is segregated into opposing groups, which are headed by reputable scientist with radically different views on selected arguments.114 Such a dualistic attitude may threaten objectivity and create a conflict of interest which may not be clearly identifiable by the public, the media or by political decision-makers.114
In the field of endometriosis, the notorious debate between advocates of medical treatment and advocates of surgery is an example of scientific polarization.115,116 When these divergent views are transferred into the medical encounter as if they were the only piece of available scientific evidence, physicians arrogate to themselves the right to decide what is best for their patients. Thus, although it is patients who bear the burden of symptoms, side effects and surgical complications, it is not always in their power to make a truly informed choice.117
Conveying honest, transparent advice should always be physicians’ responsibility as it enables true patient empowerment, whilst reducing confusion and uncertainty regarding the best treatment for each specific individual.
Reductionist Body
A reductionist view of the body consists in overemphasizing signs, symptoms and the results of instrumental exams, whilst neglecting the individual’s psychological, environmental, social and spiritual dimensions.18
Although it is now accepted that endometriosis is a systemic, inflammatory condition and that endometriosis-related pain is caused by a variety of factors, ranging from organic contributors to neuro-psychological ones,43 the treatment of all such contributors is often considered by physicians superfluous, if not unorthodox. However, times are changing, and it should be no longer acceptable for women’s psychological health and sexual function not to be addressed in the medical encounter.
Psychology is a major determinant of pain-related disability, that is the way an individual understands, experiences and manages pain.118 Catastrophizing in particular is correlated to lower perceived effectiveness of analgesics, elevated stress and lower quality of life.118 In fact, it may influence the hypothalamic–pituitary–adrenal axis, magnifying inflammatory responses,119 and is associated with a reduction in both the activity and the grey-matter volume of brain areas involved in the inhibition of pain signals.120
In fact, together with selective attention, sleep disturbances and anxiety and depression, catastrophic misinterpretation has been observed in chronic pain patients with signs of CS.121 Central sensitization is a neurobiological phenomenon characterized by an increased sensitivity to peripheral stimuli due to alterations in central neural mechanisms. These probably derive from a continued peripheral input, such as inflammation, and are similar to those underlying the generation of memory.122 Endometriosis has been included among the Chronic Overlapping Pain Conditions (COPCs), a set of conditions, which often co-occur and appear to share CS as a common underlying mechanism.45 Women with endometriosis with a greater central component to pain appear to have more severe symptoms and are less likely to respond to first-line hormonal treatment.123,124
Further contributors to anxiety and depression among persons with endometriosis may be represented by pain itself, especially in its non-cyclical form,125 by impaired self-esteem and perception of body image126 and by the uncertainty regarding infertility.44
Although evidence in this regard is still limited, psychological interventions seem to be effective in reducing endometriosis-related pain, even long term, irrespective of the presence of CS.127,128
Quality of sexual life should also be addressed. Despite sexual dysfunction may be present in up to 70% of women with endometriosis,129 independently of disease severity,130 the quality of physician/patient communication on sexual issues remains poor.131
Impairment in sexual function may arise from mechanical pressure on endometriotic lesions, traction of scarred tissue, inflammation, but also from a vicious circle which connects dyspareunia, fear and anticipation of pain, inhibition of the sexual response cycle, mood disorders and CS.132 Central elaboration of pain may in fact induce viscero-somatic reflexes which can generate painful pelvic myofascial trigger points in as many as 60–90% of women with endometriosis.45,133
Treatment of sexual dysfunction should be addressed through an interdisciplinary cooperation of gynecologists, sexologists, psychologists and pelvic floor therapists.132 Alongside medical and surgical treatment, when needed, cognitive behavioral therapy and physical therapy have been found to reduce pain, anxiety, depression, stress and fatigue and consequently to improve quality of life.90,134,135
Conclusions
The shift in endometriosis research from the evaluation of pathological classification improvement to the analysis of patient reported outcomes has unveiled an increasing distance between physicians and their patients and, as a consequence, the need for a more humanizing, person-centered care. Understanding patients’ unique point of view as well as relying on scientific knowledge, taking time to listen, recognizing individual needs and tailoring decisions on the basis of individual beliefs should be part of medical education programs and should be fostered throughout medical practice as a moral duty.
In persons with endometriosis, quality of care has been associated with better treatment satisfaction, and the adoption of humanizing practices has been found to improve clinical outcomes. Physicians are not only deliverers of treatment; they are a form of treatment themselves and as such they should always keep in mind how their attitude towards their patients is a major determinant of their patients’ quality of life.
Acknowledgments
We are extremely grateful to Francesca Guadagno for creating the vignettes in Figure 1. Her artwork is a great added value to our manuscript.
Funding
This study was partially funded by the Italian Ministry of Health, Current Research IRCCS Ca’ Granda, Ospedale Maggiore Policlinico Milano.
Disclosure
P.V. serves as Associate Editor for Human Reproduction; is a member of the Editorial Board of the Journal of Obstetrics and Gynaecology Canada, of the Italian Journal of Obstetrics and Gynaecology, and of the International Editorial Board of Acta Obstetricia et Gynecologica Scandinavica; he has received royalties from Wolters Kluwer for chapters on endometriosis management in the clinical decision support resource UpToDate and maintains both a public and private gynaecological practice. E.S. discloses payments from Ferring for research grants and honoraria from Merck-Serono for lectures, grants from Ibsa, and personal fees from Gedeon Richter. All other authors declare they have no conflict of interest.
References
1. Lukas I, Kohl-Schwartz A, Geraedts K., et al. Satisfaction with medical support in women with endometriosis. PLoS One. 2018;13(11):e0208023. doi:10.1371/journal.pone.0208023
2. Facchin F, Saita E, Barbara G, Dridi D, Vercellini P. “Free butterflies will come out of these deep wounds”: a grounded theory of how endometriosis affects women’s psychological health. J Health Psychol. 2018;23(4):538–549. doi:10.1177/1359105316688952
3. Rowe HJ, Hammarberg K, Dwyer S, Camilleri R, Fisher JR. Improving clinical care for women with endometriosis: qualitative analysis of women’s and health professionals’ views. J Psychosom Obstet Gynaecol. 2021;42(3):174–180. doi:10.1080/0167482X.2019.1678022
4. Facchin F, Barbara G, Buggio L, Dridi D, Frassineti A, Vercellini P. Assessing the experience of dyspareunia in the endometriosis population: the Subjective Impact of Dyspareunia Inventory (SIDI). Hum Reprod. 2022;37(9):2032–2041. doi:10.1093/humrep/deac141
5. Cox H, Ski CF, Wood R, Sheahan M. Endometriosis, an unknown entity: the consumer’s perspective. Int J Consum Stud. 2003;27:200–209. doi:10.1046/j.1470-6431.2003.t01-1-00302.x
6. Huang K, For Gen Z TikTok is the new search engine. New York: New York Times; 2022.
7. Pettersson A and Berterö CM. (2020). How women with endometriosis experience health care encounters. Women’s Health Reports, 1(1), 529–542. 10.1089/whr.2020.0099
8. Strömberg C, Olovsson M and Grundström H. (2022). Age-related differences in experienced patient-centred care among women with endometriosis. J Obstet Gynaecol, 42(7), 3356–3361. 10.1080/01443615.2022.2125796
9. Wu J, Greene M, Bickett A, Song AH, Swartz JJ. Period pain is not normal: a content analysis of endometriosis-related videos on the social media platform TikTok. BJOG. 2023;00:1–2.
10. Geukens E, Apers S, Meuleman C, D’Hooghe T and Dancet E. (2018). Patient-centeredness and endometriosis: definition, measurement, and current status. Best Pract Res Cl Ob, 50 11–17. 10.1016/j.bpobgyn.2018.01.009
11. Howick J, Bizzari V, Dambha-Miller H. Oxford Empathy Programme. Therapeutic empathy: what it is and what it isn’t. J R Soc Med. 2018;111(7):233–236. doi:10.1177/0141076818781403
12. Bertakis KD, Callahan EJ, Helms LJ, Azari R, Robbins JA, Miller J. Physician Practice Styles and Patient Outcomes: differences between Family Practice and General Internal Medicine. Med Care. 1998;36(6):879–891. doi:10.1097/00005650-199806000-00011
13. Cofini V, Muselli M, Lolli C, Fabiani L, Necozione S. Does Quality of Care (QoC) Perception Influence the Quality of Life (QoL) in Women with Endometriosis? Results from an Italian Nationwide Survey during Covid Pandemic. Int J Environ Res Public Health. 2022;20(1):625. doi: 10.3390/ijerph20010625
14. Haslam N. Dehumanization: an integrative review. Pers Soc Psychol Rev. 2006;10:252–264. doi:10.1207/s15327957pspr1003_4
15. Lekka D, Richardson C, Madoglou A, et al. Dehumanization of Hospitalized Patients and Self-Dehumanization by Health Professionals and the General Population in Greece. Cureus. 2021;13(12):e20182. doi:10.7759/cureus.20182
16. Maskrey N. Shared decision making: why the slow progress? An essay by Neal Maskrey. BMJ. 2019;367(l6762). doi:10.1136/bmj.l6762
17. Haque OS, Waytz A. Dehumanization in Medicine: causes, Solutions, and Functions. Perspect Psychol Sci. 2012;7(2):176–186. doi:10.1177/1745691611429706
18. Todres L, Galvin K, Holloway I. The humanization of healthcare: a value framework for qualitative research. International Journal of Qualitative Studies on Health and Well-Being. 2009;4(2):68 77. doi:10.1080/17482620802646204
19. Tsang A, Von Korff M, Lee S, et al. Common chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2008;9(10):883–891. doi:10.1016/j.jpain.2008.05.005
20. Keogh E. Sex and gender differences in pain: past, present, and future. Pain. 2022;163(Suppl 1):S108–S116.
21. Bimpong K, Thomson K, Mcnamara CL, et al. The Gender Pain Gap: gender inequalities in pain across 19 European countries. Scand J Public Health. 2022;50(2):287–294. doi:10.1177/1403494820987466
22. Hoffmann DE, Tarzian AJ. The girl who cried pain: a bias against women in the treatment of pain. J Law Med Ethics. 2001;29(1):13–27. doi:10.1111/j.1748-720X.2001.tb00037.x
23. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
24. Tait RC, Chibnall JT, Kalauokalani D. Provider judgments of patients in pain: seeking symptom certainty. Pain Med. 2009;10(1):11–34. doi:10.1111/j.1526-4637.2008.00527.x
25. Racine M, Dion D, Dupuis G, Guerriere DN, Zagorski B, Choinière M. The Canadian STOP-PAIN project: the burden of chronic pain-does sex really matter? Clin J Pain. 2014;30(5):443–452. doi:10.1097/AJP.0b013e3182a0de5e
26. Hirsh AT, Hollingshead NA, Matthias MS, Bair MJ, Kroenke K. The influence of patient sex, provider sex, and sexist attitudes on pain treatment decisions. J Pain. 2014;15(5):551–559. doi:10.1016/j.jpain.2014.02.003
27. Bernardes SF, Costa M, Carvalho H. Engendering pain management practices: the role of physician sex on chronic low-back pain assessment and treatment prescriptions. J Pain. 2013;14(9):931–940. doi:10.1016/j.jpain.2013.03.004
28. Fourquet J, Báez L, Figueroa M, Iriarte RI, Flores I. Quantification of the impact of endometriosis symptoms on health-related quality of life and work productivity. Fertil Steril. 2011;96(1):107–112. doi:10.1016/j.fertnstert.2011.04.095
29. Simoens S, Dunselman G, Dirksen C, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod. 2012;27(5):1292–1299. doi:10.1093/humrep/des073
30. Manderson L, Warren N, Markovic M. Circuit breaking: pathways of treatment seeking for women with endometriosis in Australia. Qual Health Res. 2008;18(4):522–534. doi:10.1177/1049732308315432
31. Markovic M, Manderson L, Warren N. Endurance and contest: women’s narratives of endometriosis. Health. 2008;12(3):349–367. doi:10.1177/1363459308090053
32. Martire FG, Lazzeri L, Conway F, et al. Adolescence and endometriosis: symptoms, ultrasound signs and early diagnosis. Fertil Steril. 2020;114(5):1049–1057. doi:10.1016/j.fertnstert.2020.06.012
33. Greene R, Stratton P, Cleary SD, Ballweg ML, Sinaii N. Diagnostic experience among 4334 women reporting surgically diagnosed endometriosis. Fertil Steril. 2009;91(1):32–39. doi:10.1016/j.fertnstert.2007.11.020
34. Centini G, Lazzeri L, Dores D, et al. Chronic pelvic pain and quality of life in women with and without endome- triosis. J Endometr Pelvic Pain Disord. 2013;5:27–33.
35. Shah DK, Missmer SA. Scientific investigation of endometriosis among ado- lescents. J Pediatr Adolesc Gynecol. 2011;24(Suppl):S18–9. doi:10.1016/j.jpag.2011.07.008
36. DiVasta AD, Vitonis AF, Laufer MR, Missmer SA. Spectrum of symptoms in women diagnosed with endometriosis during adolescence vs adulthood. Am J Obstet Gynecol. 2018;218(3):324.e1–324.e11. doi:10.1016/j.ajog.2017.12.007
37. Chapron C, Lafay-Pillet MC, Monceau E, et al. Questioning patients about their adolescent history can identify markers associated with deep infiltrating endometriosis. Fertil Steril. 2011;95(877):88. doi:10.1016/j.fertnstert.2010.10.027
38. Sieberg CB, Lunde CE, Shafrir AL, et al. Quantitative somatosensory testing of the abdomen: establishing initial reference values across developmental age and biological sex. Pain. 2023.
39. Solnik MJ. Chronic pelvic pain and endometriosis in adolescents. Curr Opin Obstet Gynecol. 2006;18(5):511–518. doi:10.1097/01.gco.0000242953.94749.2b
40. Wüest A, Limacher JM, Dingeldein I, et al. Pain Levels of Women Diagnosed with Endometriosis: is There a Difference in Younger Women? J Pediatr Adolesc Gynecol. 2023;36(2):140–147. doi:10.1016/j.jpag.2022.10.011
41. Dunselman GA, Vermeulen N, Becker C, et al. European Society of Human Reproduction and Embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412. doi:10.1093/humrep/det457
42. Nasyrova RF, Sotnikova LS, Baystrukova NV, et al. Psychoimmune interactions in women of reproductive age with endometriosis. Bull Exp Biol Med. 2011;152(1):93–97. doi:10.1007/s10517-011-1463-0
43. Cetera GE, Merli CEM, Facchin F, et al. Non-response to first-line hormonal treatment for symptomatic endometriosis: overcoming tunnel vision. A narrative review. BMC Women's Health. 2023;23(1):347. doi:10.1186/s12905-023-02490-1
44. Sieberg CB, Lunde CE, Borsook D. Endometriosis and pain in the adolescent- striking early to limit suffering: a narrative review. Neurosci Biobehav Rev. 2020;108:866–876. doi:10.1016/j.neubiorev.2019.12.004
45. Till SR, Nakamura R, Schrepf A, As-Sanie S. Approach to Diagnosis and Management of Chronic Pelvic Pain in Women: incorporating Chronic Overlapping Pain Conditions in Assessment and Management. Obstet Gynecol Clin North Am. 2022;49(2):219–239. doi:10.1016/j.ogc.2022.02.006
46. Driever EM, Tolhuizen IM, Duvivier RJ, Stiggelbout AM, Brand PLP. Why do medical residents prefer paternalistic decision making? An interview study. BMC Med Educ. 2022;22(1):155. doi:10.1186/s12909-022-03203-2
47. O’Hara R, Rowe H, Fisher J. Managing endometriosis: a cross-sectional survey of women in Australia. J Psychosom Obstet Gynaecol. 2022;43(3):265–272. doi:10.1080/0167482X.2020.1825374
48. Stewart MA, Roter D, editors. Communicating with Medical Patients. Newbury Park, CA: Sage Publications; 1989.
49. Lancet T. Patient empowerment--who empowers whom? Lancet. 2012;379(9827):1677. doi:10.1016/S0140-6736(12)60699-0
50. Ben-Sira Z. The function of the professional’s affective behavior in client satisfaction: a revised approach to social interaction theory. J Health Soc Behav. 1976;17(1):3–11. doi:10.2307/2136462
51. Di Matteo MR, Taranta A, Friedman HS, Prince LM. Predicting patient satisfaction from physicians’ nonverbal communication skills. Med Care. 1980;18(4):376–387. doi:10.1097/00005650-198004000-00003
52. Hamilton DL, Ed. Cognitive Processes in Stereotyp- Ing and Intergroup Behavior. Hillsdale, NJ: Erlbaum; 1981.
53. Bodenhausen GV, Lichtenstein M. Social stereotypes and information-processing strategies: the impact of task complexity. J Pers Soc Psychol. 1987;52(5):871–880. doi:10.1037/0022-3514.52.5.871
54. MacRae HM, Cohen R, Regehr G, Reznick R, Burnstein M. A new assessment tool: the patient assessment and management examination. Surgery. 1997;122(2):335–343. doi:10.1016/S0039-6060(97)90025-8
55. Daniel J. The Poor: Aliens in an Affluent Society: Cross- Cultural Communication. Today’s Speech; 1970.
56. Hooper EM, Comstock LM, Goodwin JM, Goodwin JS. Patient characteristics that influence physician behavior. Med Care. 1982;20(6):630–638. doi:10.1097/00005650-198206000-00009
57. Phelan SM, Puhl RM, Burgess DJ, et al. The role of weight bias and role-modeling in medical students’ patient-centered communication with higher weight standardized patients. Patient Educ Couns. 2021;104(8):1962–1969. doi:10.1016/j.pec.2021.01.003
58. Cartwright A. Human Relations and Hospital Care. London: Routledge & Kegan Paul; 1964.
59. Boreham P, Gibson D. The informative process in private medical consultations: a preliminary investigation. Soc Sci Med. 1978;12(5A):409–416.
60. Matthews J. The communication process in clinical settings. Soc sci med. 1983;17:1371. doi:10.1016/0277-9536(83)90197-1
61. Clarke IM. Chronic-pain patients must cope with chronic lack of physician understanding. CMAJ. 1991;145(6):620.
62. Marziali M, Venza M, Lazzaro S, Lazzaro A, Micossi C, Stolfi VM. Gluten-free diet: a new strategy for management of painful endometriosis related symptoms? Minerva Chir. 2012;67(6):499–504.
63. Moore JS, Gibson PR, Perry RE, Burgell RE. Endometriosis in patients with irritable bowel syndrome: specific symptomatic and demographic profile, and response to the low FODMAP diet. Aust N Z J Obstet Gynaecol. 2017;57(2):201–205. doi:10.1111/ajo.12594
64. Krabbenborg I, de Roos N, van der Grinten P, Nap A. Diet quality and perceived effects of dietary changes in Dutch endometriosis patients: an observational study. Reprod Biomed Online. 2021;43(5):952–961. doi:10.1016/j.rbmo.2021.07.011
65. Armour M, Sinclair J, Chalmers KJ, Smith CA. Self-management strategies amongst Australian women with endometriosis: a national online survey. BMC Complement Altern Med. 2019;19(1):17. doi:10.1186/s12906-019-2431-x
66. Schultz WGM, Van Andel P, Sabelis I, Mooyart E. Magnetic reso- nance imaging of male and female genitals during coitus and female sexual arousal. Br Med J. 1999;319:1596–1600. doi:10.1136/bmj.319.7225.1596
67. Faix A, Lapray JF, Callede O, Maubon A, Lanfrey K. Magnetic resonance imaging (MRI) of sexual intercourse: second experience in missionary position and initial experience in posterior position. J Sex Marital Ther. 2002;28(Suppl 1):63–76. doi:10.1080/00926230252851203
68. Mykyta L, Cohen RA. Characteristics of Adults Aged 18-64 Who Did Not Take Medication as Prescribed to Reduce Costs: United States, 2021. NCHS Data Brief. 2023;5(470):1–8.
69. Bonathan C, Hearn L, Williams AC. Socioeconomic status and the course and consequences of chronic pain. Pain Manag. 2013;3(3):159–162. doi:10.2217/pmt.13.18
70. Fourquet J, Zavala DE, Missmer S, Bracero N, Romaguera J, Flores I. Disparities in healthcare services in women with endometriosis with public vs private health insurance. Am J Obstet Gynecol. 2019;221(6):623.e1–623.e11. doi:10.1016/j.ajog.2019.06.020
71. Vercellini P, Bandini V, Buggio L, et al. Mitigating the economic burden of GnRH agonist therapy for progestogen-resistant endometriosis: why not? Hum Reprod Open. 2023;2023(2):hoad008. doi:10.1093/hropen/hoad008
72. Vercellini P. Introduction: management of endometriosis: moving toward a problem-oriented and patient-centered approach. Fertil Steril. 2015;104(4):761–763. doi:10.1016/j.fertnstert.2015.09.004
73. Vercellini P, Donati A, Ottolini F, et al. A stepped-care approach to symptomatic endometriosis management: a participatory research initiative. Fertil Steril. 2018;109(6):1086–1096. doi:10.1016/j.fertnstert.2018.01.037
74. Viganò P, Somigliana E, Chapron C, et al. “I’m looking through you”: what consumers and manufacturers need to know about non-invasive diagnostic tests for endometriosis. J Endometriosis Uterine Disorders. 2023;100031. doi:10.1016/j.jeud.2023.100031
75. Schreurs AMF, Dancet EAF, Apers S, et al. The relation between patient-centered care and quality of life in women with endometriosis. Gynecol Obstet Invest. 2023;13:1.
76. Grundström H, Engman L, Rimhagen E, Söderstierna C, Flink I. Experiences of communication in women with endometriosis: perceived validation and invalidation in different contexts, and associations with health-related quality of life. J Psychosom Obstet Gynaecol. 2023;44(1):2264483. doi: 10.1080/0167482X.2023.2264483
77. Blasini M, Peiris N, Wright T, Colloca L. The Role of Patient-Practitioner Relationships in Placebo and Nocebo Phenomena. Int Rev Neurobiol. 2018;139:211–231.
78. Goldie JGS. The ethics of listening and responding to patients’ narratives: implications for practice. Br J Gen Pract. 2011;61(585):306–307. doi:10.3399/bjgp11X568143
79. Charon R. Literature and medicine: origins and destinies. Acad Med. 2000;75(1):23–27. doi:10.1097/00001888-200001000-00008
80. Glasberg 2003. Available from: https://news.columbia.edu/news/narrative-medicine-teaches-doctors-how-listen-patients-stories.
81. Thiel P, Burke MJ, Bridge-Cook P, Leonardi M. Nocebo effects in the treatment of endometriosis. Reprod Fertil. 2021;2(4):C35–C38. doi:10.1530/RAF-21-0040
82. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. BMJ. 2008;336(7651):999–1003. doi:10.1136/bmj.39524.439618.25
83. Ellingsen DM, Isenburg K, Jung C, et al. Brain-to-brain mechanisms underlying pain empathy and social modulation of pain in the patient-clinician interaction. Proc Natl Acad Sci U S A. 2023;120(26):e2212910120. doi:10.1073/pnas.2212910120
84. Adler-Milstein J, Zhao W, Willard- Grace R, Knox M, Grumbach K. Electron- ic health records and burnout: time spent on the electronic health record after hours and message volume associated with exhaustion but not with cynicism among primary care clinicians. J Am Med Inform Assoc. 2020;27:531–538. doi:10.1093/jamia/ocz220
85. Brown JL, Sheffield D, Leary MR, Robinson ME. Social support and experimental pain. Psychosom Med. 2003;65:276–283. doi:10.1097/01.PSY.0000030388.62434.46
86. Heinrichs M, Baumgartner T, Kirschbaum C, Ehlert U. Social support and oxytocin interact to suppress cortisol and subjective responses to psychosocial stress. Biol Psychiatry. 2003;54(12):1389–1398. doi:10.1016/S0006-3223(03)00465-7
87. Kamarck TW, Shiffman SM, Smithline L, et al. Effects of task strain, social conflict, and emotional activation on ambulatory cardiovascular activity: daily life consequences of recurring stress in a multiethnic adult sample. Health Psychol. 1998;17(1):17–29. doi:10.1037/0278-6133.17.1.17
88. De Graaf R, van Dorsselaer S, Tuithof M, ten Have M. Sociodemographic and psychiatric predictors of attrition in a prospective psychiatric epidemiological study among the general population. Result of the Netherlands Mental Health Survey and Incidence Study-2. Compr Psychiatry. 2013;54(8):1131–1139. doi:10.1016/j.comppsych.2013.05.012
89. Bury 1982: ‘Chronic illness as biographical disruption’.
90. Buggio L, Barbara G, Facchin F, Frattaruolo MP, Aimi G, Berlanda N. Self-management and psychological-sexological interventions in patients with endometriosis: strategies, outcomes, and integration into clinical care. Int J Women's Health. 2017;9:281–293. doi:10.2147/IJWH.S119724
91. Yoon Y, Park MA, Park S. Seeking adaptation from uncertainty: coping strategies of South Korean women with endometriosis. Res Nurs Health. 2021;44(6):970–978. doi:10.1002/nur.22186
92. Silverman J, Kurtz S, Draper J. Skills for Communicating with Patients. Oxford: Radcliffe Medical Press; 1998.
93. Maguire P, Pitceathly C. Key communication skills and how to acquire them. BMJ. 2002;325(7366):697–700. doi:10.1136/bmj.325.7366.697
94. Ng N, Wahl K, Orr NL, et al. Endometriosis and negative perception of the medical profession. J Obstet Gynaecol Can. 2020;42(3):248–255. doi: 10.1016/j.jogc.2019.08.034. Erratum in: J Obstet Gynaecol Can. 2020;42(8):1063.
95. Nutbeam D. Health promotion glossary. Health Promot Int. 1998;13:349–364. doi:10.1093/heapro/13.4.349
96. Ishikawa H, Kiuchi T. Health literacy and health communication. Biopsychosoc Med. 2010;4:18. doi:10.1186/1751-0759-4-18
97. Nestoriuc Y, von Blanckenburg P, Schuricht F, et al. Is it best to expect the worst? Influence of patients’ side-effect expectations on endocrine treatment outcome in a 2-year prospective clinical cohort study. Ann Oncol. 2016;27(10):1909–1915. doi:10.1093/annonc/mdw266
98. Petrie KJ, Rief W. Psychobiological Mechanisms of Placebo and Nocebo Effects: pathways to Improve Treatments and Reduce Side Effects. Annu Rev Psychol. 2019;70:599–625. doi:10.1146/annurev-psych-010418-102907
99. Loezar-Hernández M, Briones-Vozmediano E, Ronda-Pérez E, Otero-García L. Juggling during Lockdown: balancing Telework and Family Life in Pandemic Times and Its Perceived Consequences for the Health and Wellbeing of Working Women. Int J Environ Res Public Health. 2023;20(6):4781. doi:10.3390/ijerph20064781
100. Antino M, Ruiz-Zorrilla P, Sanz-Vergel AI, Leon-Perez JM, Rodriguez-Muñoz A. The Role of Job Insecurity and Work-Family Conflict on Mental Health Evolution during COVID-19 Lockdown. Eur J Work Org Psychol. 2022;31:667–684. doi:10.1080/1359432X.2022.2049251
101. Meuleman C, Vandenabeele B, Fieuws S, Spiessens C, Timmerman D, D’Hooghe T. High prevalence of endometriosis in infertile women with normal ovulation and normospermic partners. Fertil Sterility. 2009;92(1):68–74. doi:10.1016/j.fertnstert.2008.04.056
102. Wilson S. When you have children, you’re obliged to live’: motherhood, chronic illness and bio- graphical disruption. Sociol Health Illness. 2007;29(4):610–626. doi:10.1111/j.1467-9566.2007.01008.x
103. Hudson N, Culley L, Law C, Mitchell H, Denny E, Raine-Fenning N. ‘We needed to change the mission statement of the marriage’: biographical disruptions, appraisals and revisions among couples living with endometriosis. Sociol Health Illn. 2016;38(5):721–735. doi:10.1111/1467-9566.12392
104. Yong PJ. Deep dyspareunia: a narrative review of impact on sexual function and quality of life. Minerva Obstet Gynecol. 2022;74(3):222–233. doi:10.23736/S2724-606X.22.04974-0
105. Ussher M, West R, Hibbs N. A survey of pregnant smokers’ interest in different types of smoking cessation support. Patient Educ Couns. 2004;54(1):67–72. doi:10.1016/S0738-3991(03)00197-6
106. Chrisler JC. Leaks, lumps, and lines: stigma and women’s bodies. Psychol Women Quart. 2011;35(2):202–214. doi:10.1177/0361684310397698
107. Cole JM, Grogan S, Turley E. “The most lonely condition I can imagine”: psychosocial impacts of endometriosis on women’s identity. Feminism Psychol. 2021;31(2):171–191. doi:10.1177/0959353520930602
108. Beauboeuf-Lafontant T. Listening past lies: a voice-centered analysis of strength and depression among black women. Qualitative Sociology. 2008;31(4):391–406. doi:10.1007/s11133-008-9113-1
109. Sormanti M, Smith E. Intimate partner violence screening in the emergency department: u.S. medical residents’ perspectives. Int Q Community Health Educ. 2009;30(1):21–40. doi:10.2190/IQ.30.1.c
110. Brody LR, Stokes LR, Kelso GA, et al. Gender role behaviors of high affiliation and low self-silencing predict better adherence to antiretroviral therapy in women with HIV. AIDS Patient Care and STDs. 2014;28(9):459–461. doi:10.1089/apc.2014.0068
111. West C, Zimmerman DH. Doing gender. Gender Soc. 1987;1(2):125–151. doi:10.1177/0891243287001002002
112. Arman M, Ranheim A, Rehnsfeldt A, Wode K. Anthroposophic health care--different and home-like. Scand J Caring Sci. 2008;22(3):357–366. doi:10.1111/j.1471-6712.2007.00536.x
113. Von Unwerth M. Listening to the patient: a perspective from narrative medicine. Int J Psychiatry Med. 2020;55(1):16–24. doi:10.1177/0091217419894470
114. Ploug T, Holm S. Conflict of interest disclosure and the polarisation of scientific communities. J Med Ethics. 2015;41(4):356–358. doi:10.1136/medethics-2014-102114
115. Canis M, Guo SW. In the thicket of fears, doubts, and murky facts: some reflections on treatment modalities for endometriosis-associated pain. Hum Reprod. 2023;38(7):1245–1252. doi:10.1093/humrep/dead061
116. Vercellini P. Are combined hormonal contraceptives the neglected treatment for symptomatic endometriosis? Fertil Steril. 2018;110(1):61–62. doi:10.1016/j.fertnstert.2018.03.038
117. Bretthauer M, Kalager M. What is my risk, doctor? How to convey disease risk and treatment effects. BMJ. 2023;381:e075289. doi:10.1136/bmj-2022-075289
118. Joseph K, Mills J. Unmet treatment needs in patients with chronic pelvic pain in a New Zealand gynaecology service. Aust N Z J Obstet Gynaecol. 2019;59(6):856–860. doi:10.1111/ajo.13059
119. Edwards RR, Kronfli T, Haythornthwaite JA, Smith MT, McGuire L, Page GG. Association of catastrophizing with interleukin-6 responses to acute pain. Pain. 2008;140(1):135–144. doi:10.1016/j.pain.2008.07.024
120. Seminowicz DA, Davis KD. Cortical responses to pain in healthy individuals depends on pain catastrophizing. Pain. 2006;120(3):297–306. doi:10.1016/j.pain.2005.11.008
121. Ezra Y, Hammerman O, Shahar G. The four-cluster spectrum of mind-body interrelationships: an integrative model. Front Psychiatry. 2019;10. doi:10.3389/fpsyt.2019.00039
122. Ren K, Dubner R. Pain facilitation and activity-dependent plasticity in pain modulatory circuitry: role of BDNF-TrkB signaling and NMDA receptors. Molecular Neurobiology. 2007;35(3):224–235. doi:10.1007/s12035-007-0028-8
123. Orr NL, Wahl KJ, Lisonek M, et al. Central sensitization inventory in endometriosis. Pain. 2022;163(2):e234–e245. doi:10.1097/j.pain.0000000000002351
124. Raimondo D, Raffone A, Renzulli F, et al. Prevalence and Risk Factors of Central Sensitization in Women with Endometriosis. J Minim Invasive Gynecol. 2023;30(1):73–80.e1. doi:10.1016/j.jmig.2022.10.007
125. Rodríguez-Lozano DC, Meza-Rodríguez MDP, Cruz-Orozco OP, et al. Emotional dysregulation in women with endometriosis with cyclical and non-cyclical chronic pelvic pain. BMC Women's Health. 2022;22(1):525. doi:10.1186/s12905-022-02066-5
126. Vannuccini S, Lazzeri L, Orlandini C, et al. Mental health, pain symptoms and systemic comorbidities in women with endometriosis: a cross-sectional study. J Psychosom Obstet Gynaecol. 2018;39(4):315–320. doi:10.1080/0167482X.2017.1386171
127. Meissner K, Schweizer-Arau A, Limmer A, et al. Psychotherapy With Somatosensory Stimulation for Endometriosis-Associated Pain: a Randomized Controlled Trial. Obstet Gynecol. 2016;128(5):1134–1142. doi:10.1097/AOG.0000000000001691
128. Hansen KE, Brandsborg B, Kesmodel US, et al. Psychological interventions improve quality of life despite persistent pain in endometriosis: results of a 3-armed randomized controlled trial. Qual Life Res. 2023;32(6):1727–1744. doi:10.1007/s11136-023-03346-9
129. Vercellini P, Somigliana E, Consonni D, Frattaruolo MP, De Giorgi O, Fedele L. Surgical versus medical treatment for endometriosis-associated severe deep dyspareunia: i. Effect on pain during intercourse and patient satisfaction. Hum Reprod. 2012;27(12):3450–3459. doi:10.1093/humrep/des313
130. Chêne G, Jaffeux P, Lasnier C, et al. Existe-t-il une corrélation anatomoclinique entre endométriose minime et endométriose sévère? Premiers résultats du registre régional d’Auvergne de l’endométriose [Are there anatomical and clinical correlations between minimal and deep endometriosis? First results of Auvergne’s Registry of Endometriosis]. Gynecol Obstet Fertil. 2008;36(1):17–22. doi:10.1016/j.gyobfe.2007.11.005
131. Witzeman K, Antunez Flores O, Renzelli-Cain RI, et al. Patient-Physician Interactions Regarding Dyspareunia with Endometriosis: online Survey Results. J Pain Res. 2020;13:1579–1589. doi:10.2147/JPR.S248887
132. Vannuccini S, Maseroli E, Vignozzi L, Petraglia F. The challenge of endometriosis for female sexual health. J Sex Med. 2023;20(3):240–246. doi:10.1093/jsxmed/qdad004
133. Aredo JV, Heyrana KJ, Karp BI, Shah JP, Stratton P. Relating Chronic Pelvic Pain and Endometriosis to Signs of Sensitization and Myofascial Pain and Dysfunction. Semin Reprod Med. 2017;35(01):088–097. doi:10.1055/s-0036-1597123
134. Evans S, Fernandez S, Olive L, Payne LA, Mikocka-Walus A. Psychological and mind-body interventions for endometriosis: a systematic review. J Psychosom Res. 2019;124:109756. doi:10.1016/j.jpsychores.2019.109756
135. Del Forno S, Arena A, Alessandrini M, et al. Transperineal Ultrasound Visual Feedback Assisted Pelvic Floor Muscle Physiotherapy in Women With Deep Infiltrating Endometriosis and Dyspareunia: a Pilot Study. J Sex Marital Ther. 2020;46(7):603–611. doi:10.1080/0092623X.2020.1765057
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.