")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Simultaneous Determination of Celecoxib, Dezocine and Dexmedetomidine in Beagle Plasma Using UPLC-MS/MS Method and the Application in Pharmacokinetics
Authors Hu J, Su XJ, Si HL, Song RX, Zhang F, Qiu XJ , Chen XP
Received 19 April 2021
Accepted for publication 28 May 2021
Published 15 June 2021 Volume 2021:15 Pages 2529—2541
DOI https://doi.org/10.2147/DDDT.S314562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Jie Hu,1,2 Xin-juan Su,2 Hui-Ling Si,2 Rui-Xiang Song,3 Fang Zhang,3 Xiang-Jun Qiu,3 Xing-Peng Chen2
1Department of Anesthesiology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, 710049, People’s Republic of China; 2Department of Anesthesiology, Luoyang Central Hospital, Luoyang, Henan Province, 471003, People’s Republic of China; 3School of Basic Medical Sciences, Henan University of Science and Technology, Luoyang, 471023, People’s Republic of China
Correspondence: Xiang-Jun Qiu
School of Basic Medicine, Henan University of Science and Technology, Luoyang, 471023, People’s Republic of China
Email [email protected]
Xing-Peng Chen
Luoyang Central Hospital, Luoyang, Henan Province, 471003, People’s Republic of China
Email [email protected]
Background: An efficient, fast and sensitive ultra high-performance liquid chromatography-mass spectrometry (UPLC-MS/MS) method for simultaneous determination of celecoxib (CEL), dezocine (DEZ) and dexmedetomidine (DEX) in beagle plasma were established.
Methods: The beagle dogs plasmawas precipitated by acetonitrile. The column was Acquity UPLC BEH C18 column and the mobile phase was acetonitrile-formic acid with gradient mode, and the flow rate was set at 0.4 mL/min. Under the positive ion mode, CEL, DEZ, DEX and Midazolam (internal standard, IS) were monitored by multiple reaction monitoring (MRM) as the following mass transition pairs: m/z 381.10→ 282.10 for CEL, m/z 246.20→ 147.00 for DEZ, m/z 201.10→ 94.90 for DEX, and m/z 326.10→ 291.10 for IS.
Results: This UPLC-MS/MS method had good linearity for CEL, DEZ and DEX. The RSDs of inter-day and intra-day precision were the values of 0.31– 7.66% and 0.11– 9.63%, respectively; the RE values were from − 6.05% to 10.98%. The extraction recovery was more than 79%, and the matrix effect was around 100%. The RSDs of stability were less than 8.96%. All of them met the acceptance standard of biological analysis method recommended by FDA.
Conclusion: This UPLC-MS/MS method is an effective tool for the simultaneous determination of CEL, DEX and DEX, and has been successfully applied to the study of pharmacokinetics in beagle dogs.
Keywords: celecoxib, dezocine, dexmedetomidine, UPLC-MS/MS, pharmacokinetics, beagles
Introduction
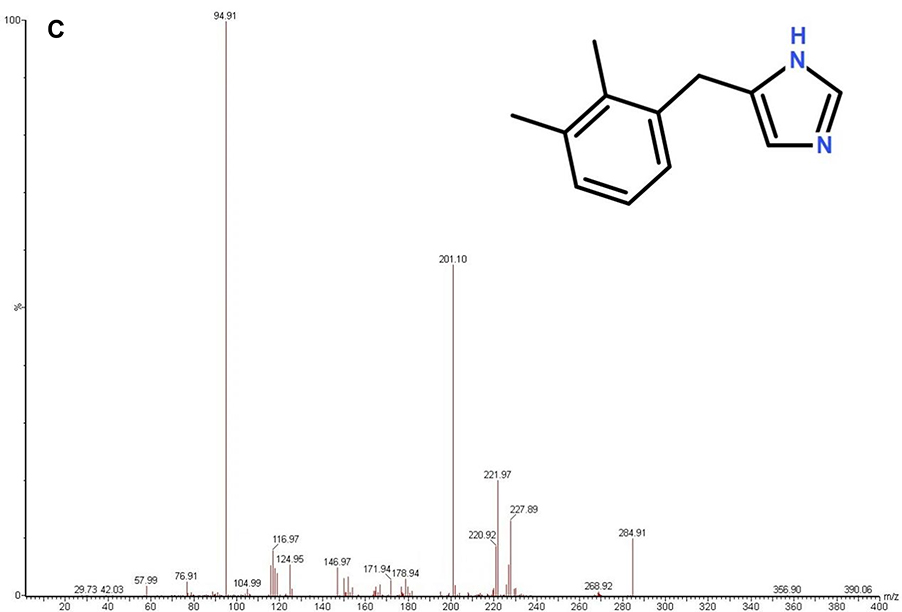
Pain is undoubtedly an unpleasant feeling, which affects the lifestyle of many people in the world. There are several treatments available for effective pain management, including the use of drugs and alternative measures. Postoperative pain is very frequent and difficult to treat.1 Postoperative pain after periodontal surgery is a common clinical symptom, which may vary greatly according to the gender, age and type of surgery.2 Pain can be defined as a complex sensory and emotional experience related to actual or potential tissue injury, which is subjective and unique. Pain perception may be influenced by many factors, such as duration, degree and complications of surgery, anxiety, past experience, stress and smoking.3,4 Nonsteroidal anti-inflammatory drugs (NSAIDs) and nonopioid analgesics are usually the first choice for postoperative pain management, especially due to the less side effects compared with other drugs.5 Figure 1 Continue. Figure 1 The chemical structure and the ion transitions from parent ion to daughter ion of CEL, DEZ and DEX (A)-CEL, (B)-DEZ, (C)-DEX.
Celecoxib (CEL, Figure 1A) is a NSAID that selectively inhibits COX-2, which is an enzyme that causes inflammation and pain.6 CEL, as well as other NSAIDs, has not been approved for use as preemptive analgesia, but only for postoperative analgesia.7 Even low-dose celecoxib administration with an adequate multimodal analgesic strategy was not inferior to the transversus abdominis plane (TAP) block and provided simple and effective preemptive analgesia for laparoscopic transabdominal preperitoneal inguinal hernia repair (LTAPP).8 Fentanyl for 24 hours and celecoxib for 4 days are safe and effective in pain relief after laparoscopic gastrectomy. Fentanyl plus celecoxib can replace epidural anesthesia for pain management after minimally invasive surgery.9
Dezocine (DEZ, Figure 1B) is a partial agonist/antagonist of opioid μ receptor, which is widely used because of its efficacy and safety. DEZ is widely used in perioperative pain treatment due to its good tolerance, mild adverse reactions and good curative effect.10 Postoperative hyperalgesia is very frequent and hard to treat, DEZ offers a significant anti-hyperalgesic and analgesic effect in patients undergoing elective open gastrectomy for up to 48 hours postoperatively.11 DEZ can effectively reduce the incidence of propofol injection pain, including mild, moderate and severe pain, and has no significant difference with lidocaine.12
Dexmedetomidine (DEX, Figure 1C), as a highly selective α 2-adrenoceptor agonist, has the characteristics of anti anxiety, sedation and analgesia. It is widely used in the auxiliary sedation during general anesthesia and postoperative mechanical ventilation.13 Different from other sedatives, DEX exerts sedative effect through endogenous sleep promoting pathway and maintains preclinical sleep structure to a certain extent. In elderly patients with non-mechanical ventilation and ICU patients after non-cardiac surgery, prophylactic low-dose DEX infusion can improve the overall sleep quality.14 DEX can attenuate perioperative stress and inflammation induced by surgical trauma, protect the immune function, and exhibit multifaceted protective effects when administered as an anaesthesia adjuvant. In elderly patients admitted to the ICU after non-cardiac surgery, prophylactic low-dose dexmedetomidine infusion significantly decreases the prevalence of postoperative delirium. The administration of low-dose dexmedetomidine did not significantly increase the prevalence of bradycardia or hypotension, but significantly decreased the prevalence of hypertension, tachycardia, and hypoxaemia.15 All these indicate that DEX may give benefits to surgical patients during the perioperative period and may improve the clinical outcomes of surgical patients.16
All the three drugs are anesthetic adjuncts and can be used in clinical practice at the same time. In the current research, an efficient, fast and sensitive UPLC-MS/MS method for the simultaneous determination of CEL, DEZ and DEX was developed using Midazolam (MDZ) as the internal standard (IS). At last, the pharmacokinetics profiles of CEL, DEZ and DEX after administration of three drugs in beagle dogs were described in our study.
Materials and Methods
Reagents and Drugs
CEL (purity more than 98.0%), DEZ (purity more than 98.0%), and DEX (purity more than 98.0%) were purchased from Sigma-Aldrich Chemical Co. (St. Louis, MO, USA). MDZ (purity more than 98.0%, IS) were obtained from China Academy of pharmaceutical and biological products. Celecoxib capsules (product batch number: DX7405, package lot number: ED5001) were purchased from Pfizer Pharmaceuticals Ltd. Dezocine Injection (product batch number: 18042731) were purchased from Yangtze River Pharmaceutical Group Co., Ltd. Dexmedetomidine Hydrochloride Injection (product batch number: 180222BP) was obtained from Hengrui medicine Co., Ltd. Methanol and acetonitrile of HPLC-grade were provided by Tianjin Kermel Chemical Reagent Co., Ltd. Formic acids were procured from Sigma-Aldrich Chemical Co. (St. Louis, MO, USA).
Instruments
Waters ACQUITY UPLC instrument is equipped with four element pump, online degasser, automatic sampler (Waters Corp., Milford, MA, USA). XEVO TQD triple quadrupole mass spectrometer is equipped with an electrospray ion source (Waters Corp., Milford, MA, USA). Other instruments included ultra-pure water equipment (Millipore, Bedford, USA), electronic analytical balance and vortex mixer, etc.
Solutions Preparation
10 mg of CEL, DEZ, DEX and IS were accurately weighed and dissolved in different volumetric flasks with methanol to obtain 1 mg/mL standard stock solution, respectively. The standard working solutions of different concentrations for the calibration curve and quality control (QC) were prepared by diluting the stock solution with methanol. 10 μL standard working solution was added to 90 μL blank plasma of beagle plasma to obtain the plasma standard solution in polypropylene tubes. The calibration curves with eight different concentrations of CEL, DEZ and DEX were prepared, and the concentration of calibration curve in plasma was as follows: 10, 25, 50, 100, 250, 500, 1000 and 2000 ng/mL for CEL; 1, 2.5, 5, 10, 25, 50, 100 and 200 ng/mL for DEZ; 0.1, 0.25, 0.5, 1, 2.5, 5, 10, 20 ng/mL for DEX. The QC samples in plasma were similarly prepared and the concentrations were set at 25, 500, 1500 ng/mL for DEZ, 2.5, 50, 150 ng/mL for DEZ and 0.25, 5, 15 ng/mL for DEX, respectively. The concentration of IS working solution was 100 ng/mL. All the solutions were stored in a refrigerator at −20 °C.
Experimental Animals and Drug Administration
Six beagle dogs weighing from 6.3 to 8.2 kg were obtained from the Laboratory Animal Center of Henan University of Science and Technology (Henan, China) and were used to study the pharmacokinetics of CEL, DEX, and DEX. All experimental procedures and protocols were approved by the Institutional Animal Care and Use Committee of Henan University of Science and Technology and were in accordance with the Guide for the Care and Use of Laboratory Animals. 12 hours before the experiment, Beagle dogs began to fast, but they could drink freely. The blood samples (1.0 mL) were collected from the veins of the forelimb or hind limb into heparinized tubes at 0.08, 0.17, 0.33, 0.67, 1, 1.5, 2, 3, 4, 6, 9, 12, 24, 48 h after simultaneous administration of the three drugs. CEL was given orally at a dose of 6.67 mg/kg, DEZ was given intramuscularly at a dose of 0.33 mg/kg, DEX was given by slow intravenous injection with a dose of 2 µg/kg. The blood samples were collected from the veins of the front and rear limbs of beagle dogs. Then, the blood samples were centrifuged for 10 min at 10,000 rpm and the plasma were collected and kept frozen at −20 °C until UPLC-MS/MS detection.
Preparation of Samples
The beagle plasma samples were taken out from the refrigerator and thawed at room temperature. 50 μL of plasma was taken into a 1.5 mL EP tube, and 10 μL IS working solution (100 ng/mL) was added and followed by vortexing for 15 s. Then, 200 μL acetonitrile was added to precipitate the plasma protein, and then vortexed for 1.0 min. At last, the supernatant was obtained by centrifuging at 15,000×g for 15 min. The supernatant was put into the autosampler sample bottle, and 2 μL supernatant was set to inject for analysis by the UPLC-MS/MS system.
UPLC-MS/MS Conditions
An Acquity UPLC BEH C18 column (2.1 mm × 50 mm, 1.7 μm) was used as the chromatographic column. Acetonitrile (A) −0.1% formic acid aqueous solution (B) were used as the mobile phase. The gradient elution procedure was as follows: 0.00–0.50 min, 10% A; 0.50–1.00 min, 10–90% A; 1.00–2.00 min, 90% A; 2.00–2.10 min, 90–10% A; 2.10–3.00 min, 10% A. The flow rate was 0.4 mL/min. The column temperature was set at 45 °C, and the injection volume was 2 μL.
A triple quadrupole tandem mass spectrometer equipped with electrospray ionization (ESI) was used to monitor in positive mode by multiple reactions monitoring (MRM) of the transitions at m/z 381.10→282.10 for CEL, m/z 246.20→147.00 for DEZ, m/z 201.10→94.90 for DEX, and m/z 326.10→291.10 for IS, respectively. The software used for data acquisition and instrument control was masslynx 4.1 (waters Corp., Milford, Ma, USA).
Method Validation
Methodology validation included specificity, linearity, precision, accuracy, recovery and stability. According to the guidelines for nonclinical pharmacokinetics of drugs of CFDA (China Food and Drug Administration) and the principles of Industry Bioanalytical Method Validation proposed by FDA, the UPLC-MS/MS method was validated in this experiment.17,18
The specificity was evaluated by comparing chromatograms of six individual blank beagle plasma samples, beagle blank plasma spiked with CEL, DEZ, DEX and IS, and beagle plasma sample after simultaneous administration of drugs.
The plasma standard solution with the concentration of 10, 25, 50, 100, 250, 500, 1000, 2000 ng/mL of CEL and 1, 2.5, 5, 10, 25, 50, 100, 200 ng/mL of DEZ and 0.1, 0.25, 0.5, 1, 2.5, 5, 10, 20 ng/mL of DEX was prepared and tested after treatment according to the plasma sample treatment method. The peak areas of CEL, DEZ, DEX and IS were recorded, respectively. The ratio of the peak area of the object to be measured to the IS peak area was y, the concentration of each point was x, and the standard curve of each analyte was drawn with the least square method. The lowest concentration of the calibration curve was the lower limit of quantification (LLOQ).
Prepare plasma standard solutions of low, medium and high concentrations (25, 500, 1500 ng/mL of CEL, 2.5, 50, 150 ng/mL of DEZ and 0.25, 5, 15 ng/mL of DEX), 6 in parallel. On the same day, after treatment of plasma samples, the intra-day precision was calculated. In the same operation for three consecutive days, the inter-day precision was calculated. The precision was expressed by relative standard deviation (RSD, %) and the accuracy was expressed by relative error (RE, %).
The extraction recovery was determined at three QC levels (low, medium and high) by comparing peak area ratios of extracted QC samples with those of reference QC solutions reconstituted in blank plasma extracts (n = 6).
The Matrix effect evaluation method was used to compare the response of the extracted sample and pure solution. The calculation method was as follows: without considering the recovery rate, compare the response of the analyte in the presence of matrix component and without matrix component, that is, the response of the extracted blank matrix added to the analyte/the response of the analyte in the pure solution. In this experiment, the matrix effects of analytes with low, medium and high concentrations were investigated.
The stability of plasma samples with low, medium and high concentrations was investigated under several different storage conditions: at room temperature for 12 h, at −20°C for 4 weeks, after three freeze-thaw cycles (−20 to 25 °C), and for 12 h in processed samples at 4°C in autosampler tray.
Pharmacokinetic Study
The pharmacokinetic parameters were calculated by DAS (Drug And Statistics, version 2.0), and then was expressed as arithmetic mean ± standard deviation, Mean ± SD. The time to reach the peak concentration (Tmax) and the maximum plasma concentration (Cmax) were measured values. Then, the mean concentration–time curves of CEL, DEZ and DEX were drawn, respectively.
Results and Discussion
UPLC MS/MS has the characteristics of high sensitivity, high throughput, high precision, reproducibility and high stability. And it is often used in the determination of drug concentration in biological samples, pharmacokinetic and drug–drug interactions (DDIs) studies.19,20
In this study, we evaluated the Acquity UPLC BEH C18 column, CSH C18 column and HSS C18, and found that the Acquity UPLC BEH C18 column had better peak shape, response and chromatographic behavior. Using acetonitrile and water as mobile phase, and adding 0.1% formic acid in water, the gradient elution mode was adopted to further improve the chromatogram and mass response curve. The higher the column temperature, the higher the separation rate.
ESI in both positive and negative modes were tested in the method development. The results show that CEL, DEZ and DEX have greater specificity in the positive mode. At the same time, through infusion and flow injection analysis, the MS parameters were optimized. In the process of optimization, MDZ was stable and have greater specificity in the positive mode. The peak shape of MDZ was good, so MDZ was selected as the internal standard (IS).
Sample Preparation
In our pre-experiment, the organic solvent extraction was used to extract analytes from plasma samples, such as n-hexane, ethyl acetate and methyl tert butyl ether, due to the different physicochemical properties of analytes and internal standard, the extraction recovery of each substance had a large deviation. Since protein precipitation is a simpler and faster method to remove potential interference from protein and sample preparation,19,20 different types of precipitants (methanol, acetonitrile) were tested to extract analytes from plasma samples. The results showed that acetonitrile precipitation had high protein precipitation efficiency and good repeatability.
Method Validation
Under the above experimental conditions, CEL, DEZ, DEX and IS were well separated from endogenous substances. Due to multi-channel detection, there was no interference between analytes and internal standards. The representative chromatograms of a blank beagle plasma sample (A), a beagle plasma sample spiked with CEL, DEZ, DEX and IS (B), and a beagle sample (C) were shown in Figure 2. The mean retention times of CEL, DEZ, DEX and IS were 1.46, 1.19, 1.14 and 1.23 min, respectively. The total running time for each sample was 3.0 min.
 |
Figure 2 The representative chromatograms of CEL, DEZ, DEX and IS in positive ion mode. (A) a blank plasma sample; (B) a blank plasma sample spiked with 250 ng/mL CEL, 25 ng/mL DEZ, 2.5 ng/mL DEX and 100 ng/mL IS; (C) a beagle plasma sample 1.5 h after administration. |
When the concentration of CEL was between 10 and 2000 ng/mL, the typical regression equations of CEL were y=1.46×10−2 x + 8.40×10−3 (r = 0.999 2). When the concentration of DEZ was between 1 and 200 ng/mL, the typical regression equations of DEZ were y=1.52×10−2 x + 1.63×10−2 (r = 0.999 1). When the concentration of DEX was between 0.1 and 20 ng/mL, the typical regression equations of DEX were y=2.08×10−2 x + 6.60×10−3 (r = 0.9987), and y represents the peak area ratio and x represents the plasma concentration. The LLOQ for CEL, DEZ and DEX in beagle plasma was 1.00 and 0.10 ng/mL, respectively.
The results obtained for the intra- and inter-day precision and accuracy of CEL, DEZ and DEX are shown in Table 1. The precision (% RSD) did not exceed 10%. Accuracy (% RE) was in the range from −6.05% to 10.98% at low, medium and high concentrations and met the requirements of validation.
 |
Table 1 Precision and Accuracy of CEL, DEZ and DEX in Beagle Dog Plasma (n=6, Mean ± SD) |
The Recoveries and ME results were investigated and shown in Table 2, which were accepted according to FDA method validation guidelines to differentiate and identify analytes in the sample. No effect of ME on the determination of each analyte in beagle plasma was observed.
 |
Table 2 The Recoveries and ME of CEL, DEZ and DEX in Beagle Dog Plasma (n=6, Mean ± SD) |
All the results of the stability are summarized in Table 3, and they were within the acceptable criteria of ± 15%, indicating that CEL, DEZ and DEX were stable under the conditions described above.
 |
Table 3 The Stability of CEL, DEZ and DEX in Beagle Dog Plasma (n=6, Mean ± SD) |
Application of the Method in Pharmacokinetic Study
The method described above was successfully applied to a pharmacokinetic study of CEL, DEZ and DEX, in which the plasma concentration was determined after simultaneous administration of the three drugs in beagles (CEL 6.67 mg/kg oral administration, DEZ 0.33 mg/kg intramuscular injection, DEX 2 µg/kg slow intravenous injection). The mean plasma concentration-time profiles of CEL, DEZ and DEX are shown in Figure 3A–C, and the pharmacokinetic parameters of CEL, DEZ and DEX including t1/2, maximum plasma concentration (Cmax), time to reach the maximum concentration (Tmax), area under concentration–time curve (AUC(0−t) and AUC(0−∞)) calculated by noncompartmental are listed in Table 4.
 |
Table 4 Pharmacokinetic Parameters of CEL, DEZ and DEX After Administration of Three Drugs to 6 Beagle Dogs (n=6, Mean ± SD) |
 |
Figure 3 (A) The mean plasma concentration–time curve of CEL after 6.67 mg/kg CEL oral administration to 6 beagle dogs (n=6). (B) The mean plasma concentration–time curve of DEZ after 0.33 mg/kg DEZ intramuscular administration to 6 beagle dogs (n=6). (C) The mean plasma concentration–time curve of DEX after 2 μg/kg DEX slow intravenous administration to 6 beagle dogs (n=6). |
Due to the short half-life of dezocine and dexmedetomidine, these two drugs could not be detected in plasma 6 hours after administration. Therefore, the concentration–time curve of dezocine and dexmedetomidine was a curve from 0 to 6 hours, and all pharmacokinetic parameters were calculated according to 6 hours after administration, separately. The half-life of celecoxib was longer, and it could still be detected 36 hours after administration, so the concentration–time curve of celecoxib was a curve from 0 to 36 hours, and the pharmacokinetic parameters were calculated according to 36 hours after administration.
In SD rats, the t1/2 after intravenous injection of DEX (20 µg/kg), DEZ (80 µg/kg), and MID (400 µg/kg) were 141.25 min, 225.39 min, and 80.51 min, respectively. The Cmax values were 23.24 ng/mL, 22.37 ng/mL and 645.68 ng/mL, respectively.21 DEX was a strong inhibitor of CYP P450 enzyme.22 DEX could inhibit the metabolism of DEZ, midazolam and valdecoxib in beagle dogs.23,24 The results of pharmacokinetics study showed that after a single dose of CEL, DEZ and DEX administration to beagle dogs, the Cmax of CEL, DEZ and DEX were (984.37 ± 168.58) ng/mL, (50.37 ± 11.97) ng/mL and (2.99 ± 0.87) ng/mL, respectively, the t1/2 were (8.51 ± 1.34) h, (1.08 ± 0.30) h and (2.98 ± 0.87) h, respectively. Although the study is a single-dose administration, the possible interaction between drugs should also be considered.
Conclusions
In this study, a sensitive UPLC-MS/MS method was developed for the simultaneous determination of CEL, DEZ and DEX in beagle plasma. This method requires a simple Acetonitrile precipitation procedure and the analysis time was 3.0 min per sample. After validation, the method has been successfully applied to the pharmacokinetic study.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding authors upon request. The corresponding authors: Xing-peng CHEN [email protected].
Acknowledgments
This study was supported by grants from the Key Scientific and Technological Projects in Henan Province (192102310128) and the Medical science and technology project of Henan Province (2018020904, LHGJ20191213).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared that no competing interests exist.
References
1. Khan H, Eto B, Vincenzo DF, et al. Evidence based alternative medicines in pain management. Evid Based Complement Alternat Med. 2015:313821. doi:10.1155/2015/313821
2. Mei CC, Lee FY, Yeh HC. Assessment of pain perception following periodontal and implant surgeries. J Clin Periodontol. 2016;43(12):1151–1159. doi:10.1111/jcpe.12618
3. Canakçi CF, Canakçi V. Pain experienced by patients undergoing different periodontal therapies. J Am Dent Assoc. 2007;138(12):1563–1573. doi:10.14219/jada.archive.2007.0105
4. Riley JL, Tomar SL, Gilbert GH. Smoking and smokeless tobacco: increased risk for oral pain. J Pain. 2004;5(4):218–225. doi:10.1016/j.jpain.2004.03.003
5. Moore PA, Hersh EV. Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions: translating clinical research to dental practice. J Am Dent Assoc. 2013;144(8):898–908. doi:10.14219/jada.archive.2013.0207
6. Johnson C, Stephens J, Walker C, Cappelleri JC, Shelbaya A. Economic outcomes related to persistence and dosing of celecoxib in patients with osteoarthritis (OA) using a retrospective claims database analysis. Clinicoecon Outcomes Res. 2020;12:56–67. doi:10.2147/CEOR.S199145
7. Mammoto T, Fujie K, Mamizuka N, et al. Effects of postoperative administration of celecoxib on pain management in patients after total knee arthroplasty: study protocol for an open-label randomized controlled trial. Trials. 2016;17(1):45. doi:10.1186/s13063-015-1106-2
8. Saito T, Iwamoto S, Murotani K, et al. Efficacy of celecoxib as preemptive analgesia for patients undergoing laparoscopic inguinal hernia repair: a randomized trial. Surg Today. 2021. doi:10.1007/s00595-020-02199-w
9. Shibasaki S, Kawamura H, Homma S, et al. A comparison between fentanyl plus celecoxib therapy and epidural anesthesia for postoperative pain management following laparoscopic gastrectomy. Surg Today. 2016;46(10):1209–1216. doi:10.1007/s00595-015-1290-4
10. O’Brien JJ, Benfeld P. Dezocine, A preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic efcacy. Drugs. 1989;38(2):226–248. doi:10.2165/00003495-198938020-00005
11. Fang Y, Zhou J, Xia S, et al. Dezocine prevents postoperative hyperalgesia in patients undergoing open abdominal surgery. Evid Based Complement Alternat Med. 2015;2015:Article ID. 946194. doi:10.1155/2015/946194
12. Zhou C, Yang Y, Zhu Y, Ruan L. Effects of dezocine on prevention of propofol injection pain: a meta-analysis. J Pain Res. 2017;10:1369–1375. doi:10.2147/JPR.S128889
13. Xue L, Yang J, Nie X-L. et al. Impact of dexmedetomidine on the incidence of delirium in elderly patients after cardiac surgery: a randomized controlled trial. PLoS One. 2017;12(2):e0170757. journal.pone. 0170757. doi:10.1371/journal.pone.0170757
14. Xin-Hai W, Cui F, Zhang C, et al. Low-dose dexmedetomidine improves sleep quality pattern in elderly patients after noncardiac surgery in the intensive care unit. Anesthesiology. 2016;125(5):979–991. doi:10.1097/ALN.0000000000001325
15. Wang K, Mengge W, Jian X, et al. Effects of dexmedetomidine on perioperative stress, inflammation, and immune function: systematic review and meta-analysis. Br J Anaesth. 2019;123(6):777–794. doi:10.1016/j.bja.2019.07.027
16. Su X, Meng Z-T, Wu X-H, et al. Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery: a randomised, double-blind, placebo-controlled trial. Lancet. 2016;388(10054):1893–1902. doi:10.1016/S0140-6736(16)30580-3
17. The technical guidelines for non clinical pharmacokinetics of drugs. Available from: http://www.nmpa.gov.cn/gsz05106/15.pdf.
18. US Food and Drug Administration. Guidance for industry: bioanalytical method validation. Rockville, MD, USA: US Department of Health and Human Services, US FDA, Center for Drug Evaluation and Research; 2018. Available from: https://www.fda.gov/regulatoryinformation/search-fda-guidance-documents/bioanalyticalmethodvalidation-guidance-industry.
19. Shuang-long L, Zhu Y-L, Zhu C-Y, et al. Simultaneous determination of parecoxib and its metabolite valdecoxib concentrations in beagle plasma by UPLC-MS/MS and application for Pharmacokinetics Study. Drug Des Devel Ther. 2020;14:1117–1125. doi:10.2147/DDDT.S226349
20. Shuang-long L, Zhang Y, Cheng Q-S, et al. UPLC-MS/MS measurement of the effect of isavuconazole, itraconazole and fluconazole on the pharmacokinetics of selinexor in rats. Infect Drug Resist. 2020;13:3153–3161. doi:10.2147/IDR.S269831
21. Cui W, Liu Q, Xiong S, Qiao L. LC-MS/MS method for simultaneous quantification of dexmedetomidine, dezocine, and midazolam in rat plasma and its application to their Pharmacokinetic Study. J Anal Methods Chem. 2018;2018:1–7. Article ID 3184759. doi:10.1155/2018/3184759
22. Zhou W, Shuang-long L, Zhao T, et al. Effects of dexmedetomidine on the pharmacokinetics of dezocine, midazolam and its metabolite 1-hydroxymidazolam in beagles by UPLC-MS/MS. Drug Des Devel Ther. 2020;14:2595–2605. doi:10.2147/DDDT.S254055
23. Jie H, Bing-feng L, Guo W-J, et al. Effects of dexmedetomidine on the pharmacokinetics of parecoxib and its metabolite valdecoxib in beagles by UPLC-MS/MS. Biomed Res Int. 2020;2020:Article ID 1563874. doi:10.1155/2020/1563874
24. Chang X, YU CC, Hua L, et al. Pharmacokinetics and sedation of sufentanil and dexmedetomidine combination in rats. Chin J Pharmacol Toxicol. 2019;33(1):63–69. doi:10.3867/j.issn.1000-3002.2019.01.009
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.