")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Servant Leadership in the Healthcare Literature: A Systematic Review
Authors Demeke GW , van Engen ML , Markos S
Received 13 September 2023
Accepted for publication 9 December 2023
Published 3 January 2024 Volume 2024:16 Pages 1—14
DOI https://doi.org/10.2147/JHL.S440160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Zhanming Liang
Getnet Worku Demeke,1,2 Marloes L van Engen,3 Solomon Markos1
1Department of Business Administration and Information Systems, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Management, Kotebe University of Education, Addis Ababa, Ethiopia; 3Institute for Management Research, Radboud University, Nijmegen, the Netherlands
Correspondence: Getnet Worku Demeke, Tel +251 911 57 13 25, Email [email protected]; [email protected]
Abstract: Servant leadership has received a growing consideration among scholars and practitioners as a viable leadership model capable of bringing positive changes in the increasingly complex healthcare system. The increasing servant leadership literature in healthcare requires an integrated research work that provides a holistic picture of the existing studies. This systematic review aims to synthesize servant leadership conceptualizations, theoretical frameworks, measurement tools, and nomological networks (antecedents, mediators, outcomes, and moderators) associated with prior research in healthcare. A systematic synthesis of 55 pertinent healthcare-specific conceptual and empirical studies demonstrated that servant leadership assumes a crucial role in developing a committed workforce that contributes towards the achievement of performance excellence in healthcare. The review uncovers that the Global Servant Leadership Scale is the most utilized measure of servant leadership in sector-specific studies in healthcare. Moreover, social exchange theory is the dominant underpinning mechanism explaining the influence of servant leadership on specific variables of interest. The findings further revealed that servant leadership has a positive relationship with a range of valued individual and organizational outcomes in healthcare. Our review contributes to the development of servant leadership theory and practice through ascertaining sector-specific studies in the territory of healthcare. We finally conclude by providing a detailed panorama for future healthcare-specific servant leadership research in terms of potential topics, methodological rigor, and less explored variables in prior studies.
Keywords: healthcare leadership, health care, healthcare sector, content analysis, nomological network, comprehensive review
Introduction
Servant leadership has attracted the attention of healthcare leaders and other stakeholders looking for mechanisms to achieve excellence in areas of leadership, management, service, and professional growth.1–3 The inherent servant nature of healthcare creates a fertile ground for the implementation of servant leadership in healthcare settings.4 Servant leadership is a moral-based leadership primarily driven by the idea that serving is a natural component (“altruistic calling”) or inner conviction of the servant leader where the focus is on the personal growth and well-being of others.5,6 In essence, servant leadership offers a leadership style that transcends self-interest to serve the needs of others.
Servant leaders assumed to bring the heart into everyone’s work in healthcare organizations.7 The theory of servant leadership uniquely embraces a combined motivation to be a leader with a strong conviction to serve.5,8 Research reveals that servant leadership has moral and professional alignment with the core values underpinning the healthcare working environment.9–12 Servant leadership offers a supportive supervisory experience for employees,13 shows caring and compassion for patients,14 and improves the safety performance of hospitals,11 which makes the theory congruent with the healthcare landscape.
Servant leadership has been consistently studied within multiple industrial and cultural contexts including healthcare.5,15 It continues to demonstrate positive relationships with valuable outcomes, such as patient satisfaction,16 service quality,17 quality of leader-follower relationships,18 and organizational performance.19 With a growing body of scientific publications demonstrating relationships between servant leadership and outcomes in healthcare, there is a compelling need to integrate the important details of existing studies in a systematic review. To the best of our knowledge, there is no comprehensive systematic review of studies that develops nomological networks of prior servant leadership research in healthcare.
Existing healthcare-specific reviews provide valuable insights into the leadership literature.4,20,21 Yet, there is a lack of integrated research work in the literature that provides a holistic picture of the journey of sector-specific servant leadership studies in healthcare. Our review ventures to advance research through a systematic analysis of theoretical frameworks, measurement tools, and nomological networks (antecedents, mechanisms, outcomes, and moderators) associated with servant leadership research in the domain of healthcare. We thus aim to provide a comprehensive picture of the value and positioning of servant leadership theory in healthcare through synthesizing and evaluating sector-specific conceptual and empirical studies that have explored servant leadership theory and research.
This review will be guided by the following research questions:
- How is servant leadership conceptualized in the healthcare literature?
- Which underpinning theories guide servant leadership research in healthcare?
- Which methodologies are used in studying servant leadership in healthcare?
- What antecedents, mediating mechanisms, outcomes, and boundary conditions of servant leadership are investigated in healthcare research?
The paper is structured as follows. First, a discussion of servant leadership theory and its position in the healthcare literature are provided. Next, a description of the review methods detailing search procedure and analysis approach is offered. Then, the results of the analysis are presented, along with mapping the nomological network of prior sector-specific servant leadership studies in healthcare. Subsequently, the discussion section synthesizes the main findings and presents an agenda for future research.
Theoretical Background
Servant Leadership
Greenleaf6 pioneered to set the foundation for the emergence of theories, frameworks, and models that enhance our understanding of servant leadership. He conceptualized servant leadership as a way of life that “begins with the natural feeling that one wants to serve, to serve first. Then conscious choice brings one to aspire to lead” (p. 7). Spears22 established ten essential characteristics of servant leadership: listening, empathy, healing, awareness, persuasion, conceptualization, foresight, stewardship, commitment to the growth of people, and building community. A proliferation of studies continued portraying different variations of these servant leadership characteristics.5,8,9,23–25
Eva et al’s5 comprehensive review provides a conceptual clarity of servant leadership vis-à-vis transformational leadership, authentic leadership, and ethical leadership. The authors defined servant leadership using the characteristics of motivation (“other-oriented approach to leadership”), mode (“one-on-one interactions between leaders and followers”), and mindset (“an overarching concern towards the wellbeing of others”). Yet, there is no consensus on the definition of servant leadership in the literature, and as a result, miscellaneous measurement tools were developed,15,26 which raises issues on the validity of empirical findings.
Servant Leadership in Healthcare
Appointment of healthcare leaders merely based on medical degree or technical skills is no more feasible in modern-day healthcare organizations.27 The presence of various disease areas, multidirectional goals, and complex non-linear interactions of multidisciplinary staff make the task of leadership challenging in healthcare.28,29 Mahon13 states that servant leadership may act as a “universal leadership language” justifiable in an increasingly over-burdened multicultural healthcare settings. A servant leadership mindset is believed to be a natural healthcare cultural-match21,30–32 relevant to addressing challenges in the complex healthcare sector.
While the leadership literature has observed a proliferation of healthcare-specific servant leadership studies, only little has been done in terms of establishing meaningful integrations. One of the prominent work here is Aij and Rapsaniotis’s20 review that integrated the evidence of existing studies on lean and servant leadership in healthcare. The review suggested that both are promising models that can contribute to the delivery of high-value patient care. This lays the impetus for the current systematic review to offer new insights into servant leadership theory through a comprehensive synthesis of sector-specific studies in healthcare.
Review Methods
Search Procedure
To ensure a replicable, scientific, and transparent process, the present review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.33 A systematic literature search of five scholarly electronic databases (Embase, Medline/PubMed, Science Direct, Scopus, and Web of Science) was conducted to identify standard published studies relevant to investigating leadership in healthcare.
The search was conducted using keywords grouped using the AND/OR Boolean terms. All research articles that include the words “servant leadership” AND (“health” OR “healthcare” OR “medical” OR “clinical” OR “pharmaceutical” OR “pharmacy” OR “nursing” OR “patient” OR “hospital” OR “community care” OR “primary care” OR “secondary care”) in the title were identified. These keywords were selected based on the literature to ensure a comprehensive coverage of relevant scientific literature across diverse settings in healthcare.
For an article to be included in this systematic literature review, it must (i) be published before April 2023; (ii) be written in the English language, and (iii) have an emphasis on servant leadership in the context of healthcare. Articles that explored servant leadership out of healthcare context and grey literature were excluded. The resulting articles in the search process were checked on titles and abstracts to ensure that they were focused on servant leadership in healthcare. Then, studies that were relevant by title and abstract were accessed in full text to settle on final articles relevant for addressing the predefined research questions of the current study.34
Analysis Approach
The reviewed articles were coded on article title, year of publication, study setting (country), study design (conceptual, empirical), sample (size, type), and findings. The parameters for the corresponding articles were summarized into Excel spread sheet to offer a systematic synthesis of healthcare-specific servant leadership studies.33,35
We conducted an in-depth content analysis of the articles on the conceptualization of servant leadership in the healthcare literature.35,36 Krippendorff35 underlines that content analysis enables to provide “replicable and valid inferences from texts (or other meaningful matter) to the contexts of their use” (p. 18). We thus started with generating first-order codes that describe servant leadership characteristics (eg, “soul of service”) using an inductive approach.37 Then, related first-order codes were clustered into themes (N = 23) that more generally denote servant leadership behaviors (eg, “exhibits humility and respect for others”). Finally, these themes (second-order codes) were condensed into nine general categories, including “ensuring autonomy”, “caring for others”, and “developing employees”.
To map the nomological network of servant leadership research in healthcare (cf),5 we extracted study variables (antecedents, mechanisms, outcomes, and moderators), along with servant leadership measures and underpinning theoretical lenses utilized from the subsample of quantitative articles (N = 32).
Results
The electronic database search procedure resulted in a subset of 162 published scientific records. After removing duplicate records (n = 93), 69 articles were subject to the screening process. The screening process yields a sample population of 55 eligible scientific manuscripts to be included in the qualitative synthesis (Figure 1).
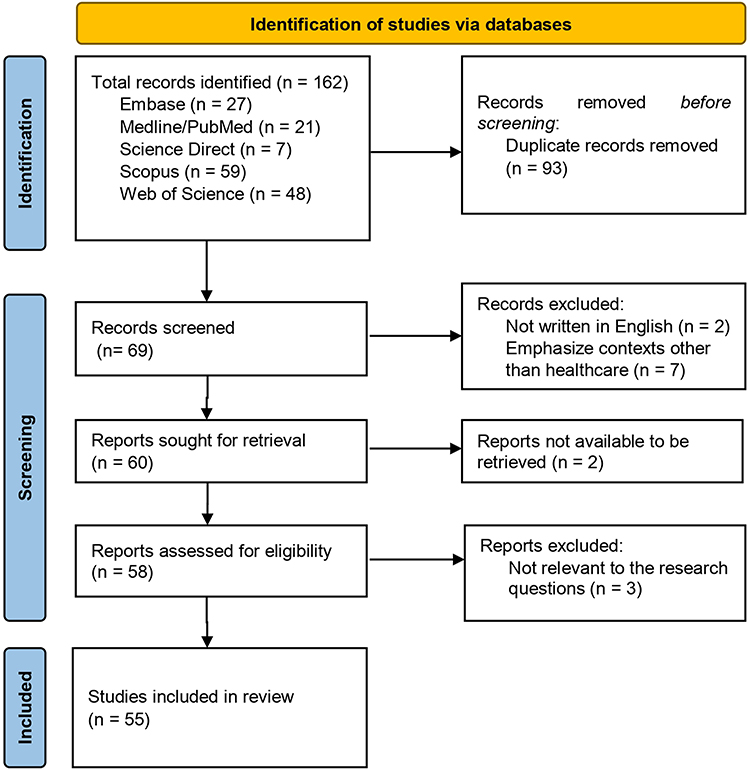 |
Figure 1 PRISMA-2020 review process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. http://creativecommons.org/licenses/by/4.0/.33 |
Characteristics of the Sample Healthcare-Specific Servant Leadership Studies
The sample population* was composed of seventeen conceptual papers and reviews (eg, Aij & Rapsaniotis,20 Neville et al),12 five qualitative (interview, case, and ethnographic) studies (eg, Sturm,1 Vanderpyl),38 thirty-two quantitative studies (eg, Hosseini et al),39 and one study that employed a mixed methods design.40
Some conceptual papers emphasized the association of servant leadership with various variables, such as creativity and innovation,10 equity and diversity,41 and sustainable research capacity.42 Other conceptual papers discussed the importance of servant leadership in building hospital-physician relationships,43 effective medical missions,44 and positive coping in medical school leadership roles.45 Review papers presented servant leadership as a prominent model in healthcare46 that enables employees to become effective lean leaders.20 Moreover, a few conceptual papers10,12 noted that servant leadership is not widely taught in healthcare leadership education programs.
Empirical research on servant leadership in healthcare has been conducted across sixteen countries, with the majority (23.7%) coming from the USA, followed by Pakistan and Indonesia (15.8%). In terms of continental distribution, the largest number of articles originated from Asia (n=23). North America had the second largest number of published articles (n=10), followed by Africa (n=3), and Europe (n=2). Table 1 presents the geographic distribution and research design of the reviewed empirical studies.
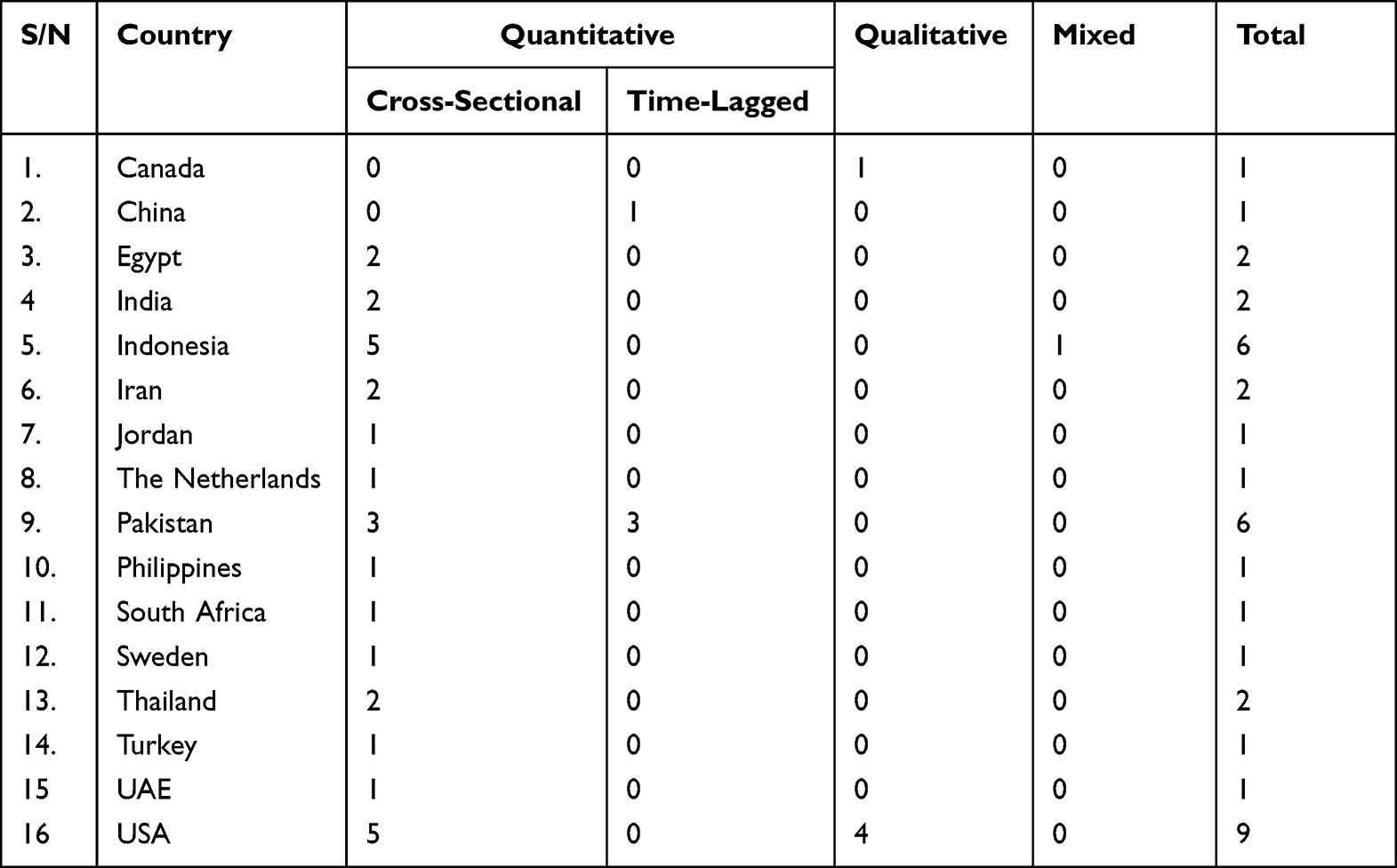 |
Table 1 Geographic Distribution and Research Design of Empirical Studies |
The qualitative healthcare-specific servant leadership studies (n = 5) employed case study and ethnographic design (participant observation, interview, document analysis). The sample sizes considered in the qualitative studies ranged from (n = 8) to (n = 24) comprising nurses, physicians, residents, supervisors, chief executive officers, practitioners, managers, administrators, and other staff members. Qualitative papers discussed the importance of servant leadership in supporting personal and professional growth,1 organizational recovery,47 and innovation.38 The only mixed-method research published on servant leadership in healthcare40 examined the role of servant leadership in promoting training effectiveness.
The reviewed survey-based quantitative studies on servant leadership (n = 32) analyzed data measured at different levels in multiple healthcare settings, which confirms the heterogeneity of the sample. Two of these studies48,49 collected data from employees and supervisors to scrutinize dyadic relationships through structural equation modeling techniques. Four of the reviewed studies used multiple time points (two waves of survey with a one-week interval50 and three waves of survey with; a ten-day interval,51 a two-week interval,49 and a two-month interval)52 to test their research models. The samples considered in the survey-based quantitative studies ranged from 66 to 1713 participants (Mean = 360, Median = 312).
Servant Leadership Conceptualization in the Healthcare Literature
To provide a synthesis of servant leadership conceptualizations in the healthcare literature, we extracted themes that subsequently distilled into categories representing servant leadership descriptions across the reviewed sector-specific studies (Table 2).
 |
Table 2 Themes of Servant Leadership in the Reviewed Healthcare-Specific Studies |
Our content analysis produced second-order themes (N = 23), eventually clustered into nine categories (“ensuring autonomy”, “fostering relationships”, “caring for others”, “giving recognition”, “promoting equity”, “nurturing collaboration”, “prioritizing others’ needs”, “developing employees”, and “involving in decision-making”). These broad themes (categories) deemed to sufficiently represent servant leadership descriptions in the reviewed healthcare-specific studies.
Servant Leadership Measures in Healthcare
Servant leadership studies in healthcare employed both self-assessment (eg, Page & Wong)24 and follower-assessment (eg, Irving)62 measures of servant leadership characteristics (Table 3). In the table, the percent of usage of corresponding servant leadership measures in healthcare research is provided.
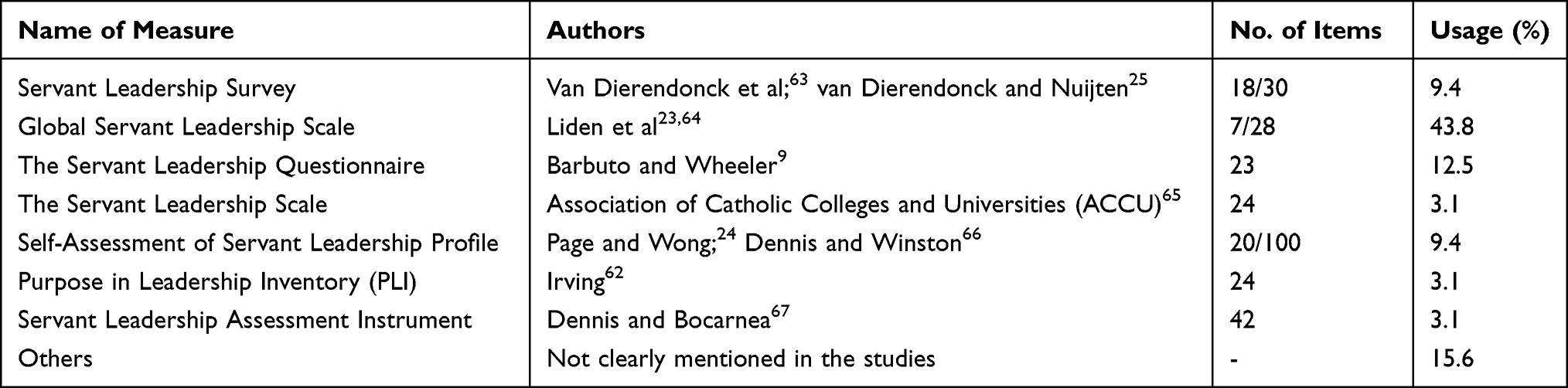 |
Table 3 The Measurement of Servant Leadership in Healthcare Research |
Theories Utilized in Servant Leadership Research in Healthcare
The theoretical frameworks for empirical research on servant leadership in healthcare draw from different theories including social-based theories, resource-based theories, and motivational theories (Table 4). In the table, we provide a description of theoretical lenses employed and conceptual frameworks tested in the corresponding empirical studies.
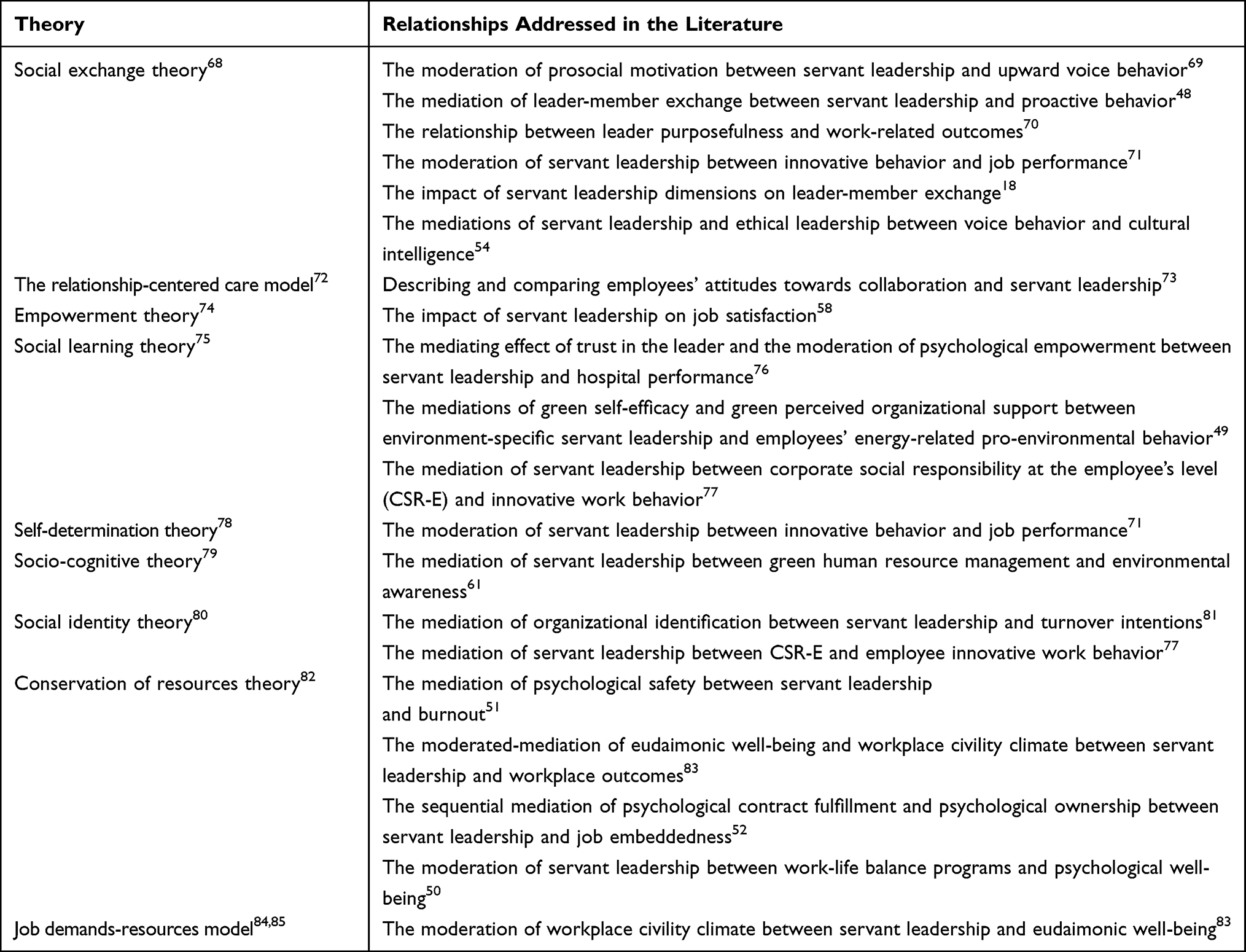 |
Table 4 Underpinning Theories Governing Healthcare-Specific Servant Leadership Studies |
Nomological Network of Servant Leadership Research in Healthcare
We mapped our sample of quantitative healthcare-specific servant leadership studies in terms of antecedents, mediating mechanisms, outcomes, and boundary conditions. In the nomological network, variables associated with employees (eg, voice behavior), teams (eg, collaboration), leaders (eg, perceived leadership effectiveness), and organizations (eg, organizational justice) are portrayed (Figure 2). Arrows indicate the direction of relationships among the considered variables of interest. In addition, the (+) and (-) signs indicate whether a positive or negative relationship was found in the reviewed healthcare-specific quantitative studies, respectively.
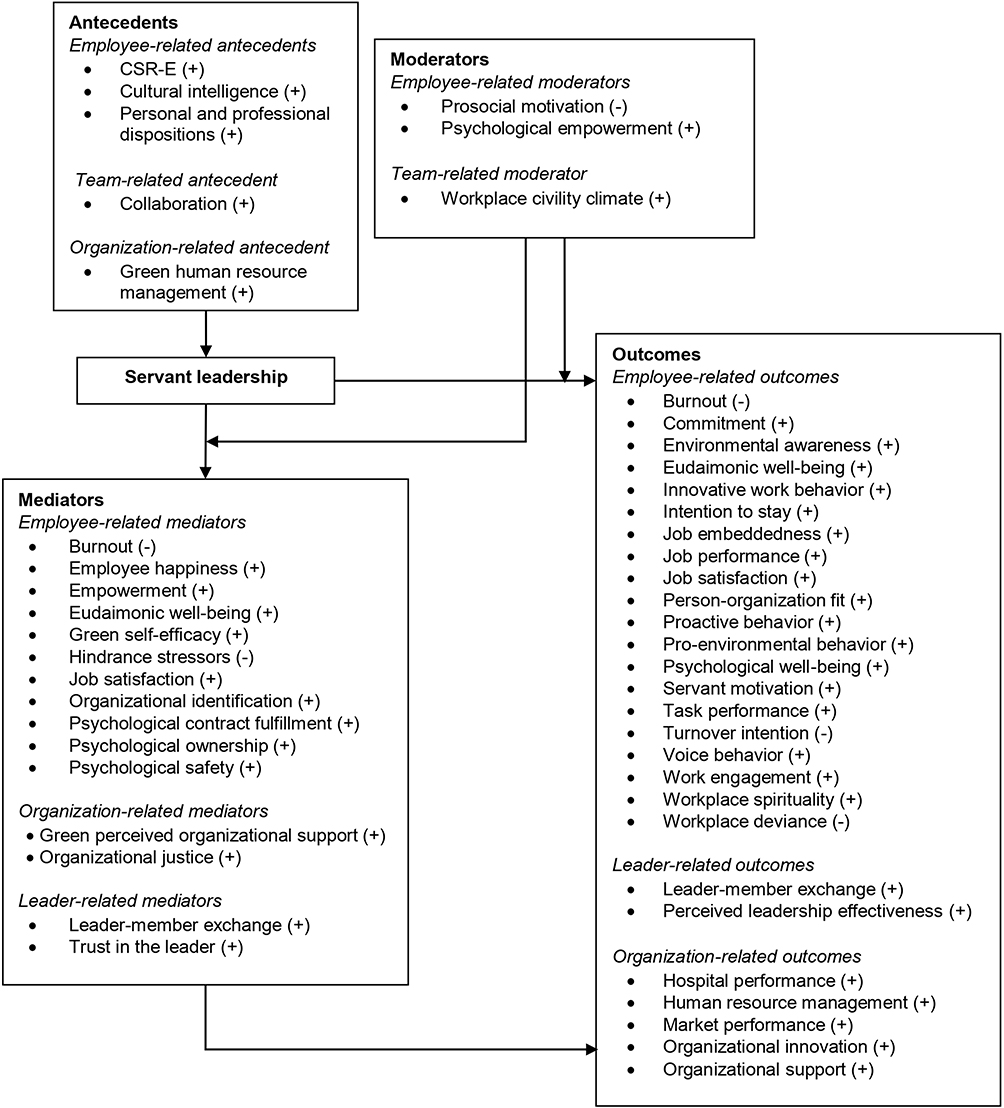 |
Figure 2 The nomological network of servant leadership research in healthcare. Notes: Figure adapted from Eva N, Robin M, Sendjaya S, et al. Servant leadership: a systematic review and call for future research. Leadership Q. 2019;30(1):111-132. Creative Commons.5 |
Antecedents of Servant Leadership in Healthcare Research
Personal and professional attributes such as age, gender, educational attainment, length of service as a manager, position, and rank were antecedents of servant leadership disposition.59 Administrators who are senior in age and position appeared higher in servant first orientation and instructive transformative relating. Corporate social responsibility at the employee level,77 cultural intelligence,54 and green human resource management61 were also studied as antecedent variables of servant leadership. Moreover, Garber et al73 showed a weak positive correlation between collaboration and servant leadership.
Mediators of Servant Leadership in Healthcare Research
Servant leadership enhances job performance through the mediation of employee happiness53 and increases employees’ intention to stay in the organization through empowerment.60 Servant leaders also promote proactive behavior through enhancing the quality of exchange relationships48 and elevates organizational performance through instilling trust.76 Further, studies reveal that a servant leader with environmental inclinations could significantly improve the energy-specific pro-environmental behavior of hospital employees through the mediating mechanisms of green self-efficacy and green perceived organizational support.49
Moreover, servant leadership reduces workplace deviance through organizational justice86 and decreases burnout through psychological safety.51 In addition, organizational identification mediated the negative impact of servant leadership on the turnover intentions of employees in healthcare.81
Psychological contract fulfilment and psychological ownership sequentially mediated the relationship between servant leadership and job embeddedness.52 Moreover, hindrance stressors, burnout, and job satisfaction mediated the relationship of servant leadership and performance and turnover.87 Servant leadership positively influences workplace outcomes (task performance, innovative work behavior, and work engagement), partially through eudaimonic well-being, and this mediation varies across different levels of workplace civility climate.83
Finally, servant leadership mediated the relationship between green human resource management and environmental awareness by promoting employee learning and engagement in pro-environmental behaviors.61 Servant leadership also partially mediated the relationship between CSR-E and employee innovative behavior in times of crisis.77
Moderators of Servant Leadership in Healthcare Research
Employee-related moderators of psychological empowerment and prosocial motivation influence the effectiveness of servant leadership. The relationship between servant leadership and nurses’ upward voice was found stronger for those lower in prosocial motivation than for those higher in prosocial motivation.69 The relationship between follower trust in the leader and the performance of the hospital organization has been found stronger when follower psychological empowerment is high.76 Further, servant leadership had a stronger relationship with eudaimonic well-being when the workplace civility climate was high.83
In addition, Kul and Sonmez71 demonstrated that servant leadership behaviors of nurse managers strengthen the positive relationship between nurses’ innovative behaviors and their job performance. However, servant leadership did not have a moderating role between work-life balance programs and psychological well-being.50
Outcomes of Servant Leadership in Healthcare Research
Servant leadership can successfully foster employee commitment,70,88,89 job embeddedness,52 servant motivation,40 psychological well-being,50 voice behavior,69 person-organization fit,70 proactive behavior,48 and satisfaction at work.70,86,87,90 Furthermore, servant leadership is positively associated with innovative behavior,71 job performance,53,71,86 and pro-environmental behavior.49 The findings also showed that servant leadership reduces workplace deviance,86 burnout,51,86 and turnover intentions.81,86
Hanse et al18 demonstrated the presence of significant correlations between servant leadership dimensions and leader-member exchange among healthcare professionals. Similarly, Irving and Berndt70 showed the effect of leader purposefulness within servant leadership (follower perspectives on servant leadership, leader follower-focus, leader goal orientation, and leader purposefulness) on work-related outcomes (job satisfaction, organizational commitment, person-organization fit, and perception of leadership effectiveness).
Moreover, servant leadership is linked with organizational performance,76,91 market performance,92 and the human resources management system93 of healthcare facilities. Further, servant leadership is found to increase spirituality39,94 and organizational support of nurses,39 which in turn improve healthcare effectiveness.
Servant leadership is also studied along with transformational leadership,58 ethical leadership,54 green leadership and digital leadership,55 and corporate social responsibility practices.60 The findings revealed the unique contribution of servant leadership to organizational performance and job satisfaction,58 market performance,55 and employees’ intention to stay in the organization.60 However, servant leadership style did not have a role in the relationship between cultural intelligence and voice behavior.54
Discussion
The present comprehensive systematic review adds to the leadership literature through synthesizing conceptual and empirical sector-specific servant leadership studies in the healthcare domain. Our discussion below addresses research design, servant leadership conceptualizations, measurement tools, theoretical mechanisms, and nomological networks in prior healthcare-specific servant leadership studies.
The conceptual and empirical studies in healthcare enabled us to obtain a deeper understanding into the construct of servant leadership. Our review shows the emergence of empirical research across the various healthcare contexts of sixteen different countries, which contributes to the cross-cultural validity of servant leadership theory.8 However, many of the empirical studies in healthcare use a cross-sectional design with the risk of common method bias and unclarity of causal directionality more likely.95,96
The review uncovers the variety in conceptualizations of servant leadership in healthcare, which accompanying utilization of different measures. This limits across study comparisons. The emerging themes of servant leadership (ie, promoting equity, fostering relationships, giving recognition, developing employees, and involving in decision-making) share similarities with the conceptualizations of inclusive leadership.97 The overlapping themes identified here offers opportunities for further research and application.
Social exchange theory dominates the contribution in explaining the relationship between servant leadership and other variables in the healthcare literature. Further, just a few studies integrated multiple theoretical lenses. Self-determination theory helps us explain the effect of servant leadership on specific variables of interest based on employee-related intrinsic motivation factors. Self-determination posits that the satisfaction of innate psychological needs for competence, autonomy, and relatedness determine the conditions for individuals to completely realize their human potentials.78 Moreover, resource-oriented theories such as conservation of resources theory help explain the influence of servant leadership based on personal characteristics or conditions valued by the individual employee. Conservation of resources theory assumes that employees attempt to gain valued resources (eg, supportive colleagues) to defend against resource loss.5,82
The nomological network of this systematic review identified that variables related to individual employees (eg, voice behavior) are dominant in healthcare research, followed by organization-related (eg, hospital performance) variables. Nonetheless, scholars gave less emphasis to the investigation of team dynamics, which would give new avenues for the increasingly interpersonal context of healthcare. Antecedents and boundary conditions of servant leadership also remain less explored, leaving a knowledge gap in relation to establishing fertile grounds for the development of servant leadership behaviors in healthcare.
Servant leadership is predominantly viewed as an exogenous variable predicting multiple outcomes of interest in the context of healthcare. The results of the current review are consistent with the theory and research outcomes of servant leadership across various sectors.5,98,99 Further, the positive follower and organizational outcomes demonstrated in the reviewed sector-specific studies stand to witness that servant leadership is particularly promising in healthcare where adherence to moral codes of conduct is essential to providing professional healthcare services.20,21 Servant leadership facilitates the process of shaping psychological good functioning across individual, organizational, and societal realms in the territory of healthcare.47,83
Suggestions for Future Research
Research on context-specific antecedents of servant leadership is needed to further shed light on the motivations of healthcare employees to become servant leaders. In addition, considering important follower-related mediating mechanisms such as compassion and work engagement would contribute to the dynamics of servant leadership-outcome relationships in healthcare. Future studies might also investigate less explored relationships in healthcare between servant leadership and outcomes such as patient safety, employee well-being, knowledge sharing, and innovative behaviors to provide insights on the role of the theory to sustainable performance in healthcare.
Researchers should look to venture into qualitative studies to complement the quantitative investigations in servant leadership research and offer additional insights into the field. For instance, how servant leadership could foster carers motivation in establishing a patient safety culture. Furthermore, mixed-methods research involving a broad range of participants including patients would be valuable to validate actions and behaviors that drive positive outcomes in healthcare. Conducting multi-source, time-lagged studies using the Global Servant Leadership Scale would be indispensable to make results more comparable.
This systematic review had certain limitations. The search process in the current systematic literature review is restricted to journal articles published by five of the most prominent electronic databases, which might have limited the results on the servant leadership phenomenon in healthcare. Future scholars can extend the research to include other relevant servant leadership articles available in other electronic databases such as the grey literature, dissertations, and other unpublished projects (eg, hospital internal research projects) to elicit a more compelling argument for servant leadership theory in healthcare.
Implications for Practitioners
The consistent positive relationships found between servant leadership and valued outcomes provide compelling evidence supporting the relevance of practicing servant leadership in healthcare. We believe healthcare organizations can benefit from cultivating servant leadership that promotes a working climate where employees embark beyond defined day-to-day role descriptions. We specifically suggest the adoption of servant leadership in public healthcare organizations seeking to achieve a more sustainable healthcare system that offers high quality care at reasonable costs.
Leadership training exposure is associated with increased servant leadership scores in healthcare.56 We thus suggest the delivery of specific need-based training (eg, ensuring autonomy, caring for others, nurturing collaboration, giving recognition) to develop the servant leadership capabilities of managers in contemporary healthcare organizations.
While servant leadership is associated with positive outcomes in healthcare, practitioners should be cautious that embedding such behaviors within healthcare organizations is not an easy task. Garber et al73 revealed attitude differences toward collaboration and servant leadership between nurses, physicians, and residents. Avoiding such differences requires potential servant leaders in healthcare to be more transparent in their actions and to be able to balance self-interest and the needs of other staff.
Conclusion
The review has shown that servant leadership research has made considerable progress in the healthcare literature. Consistent across other non-healthcare domains, scholars predominantly approach servant leadership as an exogenous variable that directly and indirectly influences various individual and organizational outcomes in healthcare. Social exchange theory is the dominant underpinning mechanism; with few studies on servant leadership in healthcare that integrated multiple theoretical lenses. The findings draw attention to the importance of embracing servant leadership in healthcare as it promises above-the-norm job in developing a committed workforce that contributes towards the achievement of performance excellence. Hence, effective implementation of servant leadership in healthcare can be an essential requirement to bring positive employee and patient outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. *Sturm BA. Principles of servant-leadership in community health nursing: management issues and behaviors discovered in ethnographic research. Home Health Care Manag Prac. 2009;21(2):82–89. doi:10.1177/1084822308318187
2. Swearingen S, Liberman A. Nursing leadership: serving those who serve others. Health Care Manag. 2004;23(2):100–109. doi:10.1097/00126450-200404000-00002
3. Tropello PD, Jane DeFazio J. Servant leadership in nursing administration and academia shaping future generations of nurses and interdisciplinary team providers to transform healthcare delivery. Nurse Leader. 2014;12(6):59–66. doi:10.1016/j.mnl.2014.09.010
4. *Schwartz RW, Tumblin TF. The power of servant leadership to transform health care organizations for the 21st-century economy. Arch Surg. 2002;137(12):1419–1427. doi:10.1001/archsurg.137.12.1419
5. Eva N, Robin M, Sendjaya S, van Dierendonck D, Liden RC. Servant leadership: a systematic review and call for future research. Leadersh Q. 2019;30(1):111–132. doi:10.1016/j.leaqua.2018.07.004
6. Greenleaf RK. Servant Leadership: A Journey into the Nature of Legitimate Power and Greatness. New York: Paulist Press; 1977.
7. *Mustard RW. Servant leadership in the veterans health administration. Nurse Leader. 2020;18(2):178–180. doi:10.1016/j.mnl.2019.03.019
8. Van Dierendonck D. Servant leadership: a review and synthesis. J Manag. 2011;37(4):1228–1261. doi:10.1177/0149206310380462
9. Barbuto JE, Wheeler DW. Scale development and construct clarification of servant leadership. Group Organ Manag. 2006;31(3):300–326. doi:10.1177/1059601106287091
10. *Cottey L, McKimm J. Putting service back into health care through servant leadership. Br J Hosp Med. 2019;80(4):220–224. doi:10.12968/hmed.2019.80.4.220
11. *Malak H, Mirza B, Rundio A, Mirza M. Impact of practicing servant leadership style among Chief Nursing Officers (CNOs) in nursing organizations. J Interprof Educ Prac. 2022;29:100562. doi:10.1016/j.xjep.2022.100562
12. *Neville KL, Conway K, Maglione JL, Connolly KA, Foley MC, Re S. Understanding servant leadership in nursing: a concept analysis. Int J Hum Caring. 2021;25(1):22–29. doi:10.20467/HumanCaring-D-20-00022
13. *Mahon D. Can using a servant -leadership model of supervision mitigate against burnout and secondary trauma in the health and social care sector? Leadersh Health Serv. 2021;34(2):198–214. doi:10.1108/LHS-01-2021-0001
14. *Anderson D. Servant leadership, emotional intelligence: essential for baccalaureate nursing students. Creat Nurs. 2016;22(3):176–180. doi:10.1891/1078-4535.22.3.176
15. Parris DL, Peachey JW. A systematic literature review of servant leadership theory in organizational contexts. J Bus Ethics. 2013;113(3):377–393. doi:10.1007/s10551-012-1322-6
16. Neubert MJ, Hunter EM, Tolentino RC. A servant leader and their stakeholders: when does organizational structure enhance a leader’s influence? Leadersh Q. 2016;27(6):896–910. doi:10.1016/j.leaqua.2016.05.00
17. Kwak WJ, Kim HK. Servant leadership and customer service quality at Korean hotels: multilevel organizational citizenship behavior as a mediator. Soc Behav Pers. 2015;43(8):1287–1298. doi:10.2224/sbp.2015.43.8.1287
18. *Hanse JJ, Harlin U, Jarebrant C, Ulin K, Winkel JT. The impact of servant leadership dimensions on leader–member exchange among health care professionals. J Nurs Manag. 2016;24(2):228–234. doi:10.1111/jonm.12304
19. Liden RC, Wayne SJ, Liao C, Meuser JD. Servant leadership and serving culture: influence on individual and unit performance. Acad Manag J. 2014;57(5):1434–1452. doi:10.5465/amj.2013.0034
20. *Aij KH, Rapsaniotis S. Leadership requirements for lean versus servant leadership in health care: a systematic review of the literature. J Healthc Leadersh. 2017;18(9):1–14. doi:10.2147/JHL.S120166
21. *Trastek VF, Hamilton NW, Niles EE. Leadership models in health care: a case for servant leadership. Mayo Clin Proc. 2014;89(3):374–381. doi:10.1016/j.mayocp.2013.10.012
22. Spears L. Tracing the past, present, and future of servant leadership. In: Spears L, Lawrence M, editors. Focus on Leadership: Developments in Theory and Research. New York: Palgrave Macmillan; 2002:1–6.
23. Liden RC, Wayne SJ, Zhao H, Henderson D. Servant leadership: development of a multidimensional measure and multi-level assessment. Leadersh Q. 2008;19(2):161–177. doi:10.1016/j.leaqua.2008.01.006
24. Page D, Wong TP. A conceptual framework for measuring servant-leadership. In: Adjibolosoo S, editor. The Human Factor in Shaping the Course of History and Development. Boston: University Press of America; 2000.
25. Van Dierendonck D, Nuijten I. The servant leadership survey: development and validation of a multidimensional measure. J Bus Psychol. 2011;26(3):249–267. doi:10.1007/s10869-010-9194-1
26. Beck CD. Antecedents of servant leadership: a mixed methods study. J Leadersh Organ Stud. 2014;21(3):299–314. doi:10.1177/1548051814529993
27. Moustafa N, Sayed I. Systematic analysis regarding leadership in healthcare. Int J of Bus Cont Risk Manag. 2021;11(2/3):224–236. doi:10.1504/IJBCRM.2021.116281
28. Al-Sawai A. Leadership of healthcare professionals: where do we stand? Oman Med J. 2013;28(4):285–287. doi:10.5001/omj.2013.7
29. Kumar RDC, Khiljee N. Leadership in healthcare. Anaesth Intensive Care Med. 2016;17(1):63–65. doi:10.1016/j.mpaic.2015.10.012
30. *Alam HV, Miharjab M, Astarinac I, Dewid P. Servant leadership: its impact and relationship on organizational performance & organizational learning in physicians. Int J Innov Creat Change. 2019;9(5):338–363.
31. *Belton LW, Anderson P. Servant leadership: a journey, not a race. Health Manag. 2017;17(4):268–270.
32. *Shalaby ME Servant leadership for healthcare organizations. Linkdin; 2015. Available from: https://www.linkedin.com/pulse/servant-leadership-healthcare-organizations-mohamed-e-shalaby/.
33. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. doi:10.1136/bmj.n71
34. Hiebl MRW. Sample selection in systematic literature reviews of management research. Organ Res Method. 2023;26(2):229–261. doi:10.1177/1094428120986851
35. Downe-Wamboldt B. Content analysis: method, applications, and issues. Health Care Women Int. 1992;13(3):313–321. doi:10.1080/07399339209516006
36. Krippendorff K. Content Analysis: An Introduction to Its Methodology. California: Sage Publications; 2004.
37. Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2:8–14. doi:10.1016/j.npls.2016.01.001
38. *Vanderpyl TH. Servant leadership: a case study of a Canadian health care innovator. J Healthc Leadersh. 2012;4:9–16. doi:10.2147/JHL.S28810
39. *Hosseini SM, Hosseini SS, Maher A. The relationship between servant leadership and spirituality in the workplace and perceived organizational support among nurses of medical and educational centers in Kermanshah. Int J Med Res Health Sci. 2016;5(9S):94–99.
40. *Nadeak B. Effects of servant leadership and training programs on servant motivation of hospital medical personnel. Ind J Public Health Res Dev. 2019;10(9):1772–1775. doi:10.5958/0976-5506.2019-02709.8
41. *Mezu-Ndubuisi OJ. Unmasking systemic racism and unconscious bias in medical workplaces: a call to servant leadership. J Am Heart Asson. 2021;10(7):e018845. doi:10.1161/JAHA.120.018845
42. *Jackson D. Servant leadership in nursing: a framework for developing sustainable research capacity in nursing. Collegian. 2008;15(1):27–33. doi:10.1016/j.colegn.2007.10.001
43. *Anderson RJ. Building hospital-physician relationships through servant leadership. Front Health Serv Manag. 2003;20(2):43–54. doi:10.1097/01974520-200310000-00007
44. *Johanson L. Building effective medical missions with servant leadership skills. J Christ Nurs. 2017;34(2):122–126. doi:10.1097/CNJ.0000000000000372
45. *Gorsky D, Barker JR, MacLeod A. Servant and supervisor: contrasting discourses of care and coercion in senior medical school leadership roles. Stud High Educ. 2017;43(12):2238–2250. doi:10.1080/03075079.2017.1318366
46. *Allen GP, Moore WM, Moser LR, Neill KK, Sambamoorthi U, Bell HS. The role of servant leadership and transformational leadership in academic pharmacy. Am J Pharm Educ. 2016;80(7):113. doi:10.5688/ajpe807113
47. *Yancer DA. Betrayed trust: healing a broken hospital through servant leadership. Nurs Adm Q. 2012;36(1):63–80. doi:10.1097/NAQ.0b013e31823b458b
48. *Mostafa AMS, El-Motalib EAA. Servant leadership, leader–member exchange, and proactive behavior in the public health sector. Public Person Manag. 2019;48(3):309–324. doi:10.1177/0091026018816340
49. *Peng J, Samad S, Coomite U, et al. Environmentally specific servant leadership and employees’ energy-specific pro-environmental behavior: evidence from a healthcare sector of a developing economy. Int J Environ Res Public Health. 2022;19(13):7641. doi:10.3390/ijerph19137641
50. *Xiao Q, Liang X, Liu L, Klarin A, Zhang C. How do work-life balance programmes influence nurses’ psychological well-being? The role of servant leadership and learning goal orientation. J Advanced Nurs. 2023;79(2):2720–2731. doi:10.1111/jan.15654
51. *Ma Y, Faraz N, Ahmed F, et al. Curbing nurses’ burnout during COVID-19: the roles of servant leadership and psychological safety. J Nurs Manag. 2021;29(8):2383–2391. doi:10.1111/jonm.13414
52. *Faraz NA, Xiong ZD, Mehmood SA, Ahmed F, Pervaiz K. How does servant leadership nurture nurses’ job embeddedness? Uncovering sequential mediation of psychological contract fulfillment and psychological ownership. J Nurs Manag. 2023;7294334. doi:10.1155/2023/7294334
53. *Alahbabi AMF, Robani AB, Zainudin MZB. A framework of servant leadership impact on job performance: the mediation role of employee happiness in UAE healthcare sector. Quality Access to Success. 2023;24(194):69–79. doi:10.47750/qas
54. *Hidayati T, Zainurossalamia S. Cultural intelligence as a pre-requisite for voice behavior of pharmaceutical sector employees in Indonesia: mediating role of servant and ethical leadership styles. Syst Rev Pharm. 2020;11(5):216–225. doi:10.31838/srp.2020.5.33
55. *Fahmi K, Kurniawan T, Cahyono Y, et al. Did servant, digital, and green leadership influence market performance? Evidence from Indonesian Pharmaceutical Industry. Syst Rev Pharm. 2020;11(9):642–653. doi:10.31838/srp.2020.9.95
56. *Murphy C, Campbell E, Boland P, Sick B. The leadership baseline: assessing servant leadership and leadership self-efficacy in first-year health professions students. J Interprof Educ Prac. 2020;20(11):100354. doi:10.1016/j.xjep.2020.100354
57. *Downs FC. The servant-leadership worldview in long-term care nursing. Ann Longterm Care. 2007;15(8):36–39.
58. *Siriattakul P, Jermsittiparsert K. Impact of transformational and servant leadership on organizational performance and job satisfaction: an empirical assessment of pharmaceutical firms in Thailand. Int J Innov Creat Change. 2019;6(11):73–101.
59. *Biag AD. Servant leadership in nursing service administration: the case of government hospitals in Pampanga and Tarlac. Philipp J Nurs. 2011;81(2):12–19.
60. *Pranee S, Pungnirund B, Saeng-on P, Pulphon S. The influence of servant leadership and CSR practices on the Employee’s intention of stay in the pharmacy firms: mediating role of empowerment. Sys Rev Pharm. 2020;11(3):10–18. doi:10.5530/srp.2020.3.02
61. *Yadav M, Yadav R, Tokas S, Farooq R. Environmental awareness in Indian Pharmaceutical Industry: role of green HRM and servant leadership. J Pharm Negative Results. 2022;13(8):1660–1664. doi:10.47750/pnr.2022.13.S08.201
62. Irving JA. The development & initial testing of the purpose in leadership inventory: a tool for assessing leader goal-orientation, follower-focus, and purpose-in-leadership. Servant Leadersh Theory Prac. 2014;1(1):53–67.
63. Van Dierendonck D, Sousa M, Gunnarsdottir A, et al. The cross-cultural invariance of the servant leadership survey: a comparative study across eight countries. Adm Sci. 2017;7(2):8. doi:10.3390/admsci7020008
64. Liden RC, Wayne SJ, Meuser JD, Hu J, Wu J, Liao C. Servant leadership: validation of a short form of the SL-28. Leadersh Q. 2015;26(2):254–269. doi:10.1016/j.leaqua.2014.12.002
65. Association of Catholic Colleges and Universities (ACCU). Toolkit for assessing servant leadership. University of St Francis. Available from: https://studylib.net/doc/9078102/toolkit-for-assessing-servant-leadership.
66. Dennis R, Winston BE. A factor analysis of page and Wong’s servant leadership instrument. Leadersh Organ Dev J. 2003;24(8):455–459. doi:10.1108/01437730310505885
67. Dennis RS, Bocarnea M. Development of the servant leadership assessment instrument. Leadersh Organ Dev J. 2005;26(8):600–615. doi:10.1108/01437730510633692
68. Blau PM. Exchange and Power in Social Life. New York: Wiley; 1964.
69. *Abdelmotaleb M, Metwally A, Saha SK. Servant leadership and nurses’ upward voice behavior in an Egyptian hospital: does prosocial motivation matter? Hum Syst Manag. 2021;41(4):1–12. doi:10.3233/HSM-201134
70. *Irving JA, Berndt J. Leader purposefulness within servant leadership: examining the effect of servant leadership, leader follower-focus, leader goal-orientation, and leader purposefulness in a large U.S. healthcare organization. Adm Sci. 2017;7(2):1–20. doi:10.3390/admsci7020010
71. *Kul S, Sonmez B. The effect of nurse managers’ servant leadership on nurses’ innovative behaviors and job performances. Leadersh Organ Dev J. 2021;42(8):1168–1184. doi:10.1108/LODJ-07-2020-0318
72. Tresolini CP. Health Professions Education and Relationship-Centered Care. San Francisco, CA: Pew Health Professions Commission; 1994.
73. *Garber JS, Madigan EA, Click ER, Fitzpatrick JJ. Attitudes towards collaboration and servant leadership among nurses, physicians, and residents. J Interprof Care. 2009;23(4):331–340. doi:10.1080/13561820902886253
74. Wilkinson A. Empowerment: theory and practice. Personnel Rev. 1998;27(1):40–56. doi:10.1108/00483489810368549
75. Bandura A. Social Learning Theory. Englewood Cliffs, NJ: Prentice-Hall; 1977.
76. *Saleem S, Tourigny L, Raziq MM, Shaheen S, Goher A. Servant leadership and performance of public hospitals: trust in the leader and psychological empowerment of nurses. J Nurs Manag. 2022;30(5):1206–1214. doi:10.1111/jonm.13622
77. *Ahmad N, Scholz M, Arshad MZ, et al. The inter-relation of corporate social responsibility at the employee level, servant leadership, and innovative work behavior in the time of crisis in the healthcare sector of Pakistan. Int J Environ Res Public Health. 2021;18(9):4608. doi:10.3390/ijerph18094608
78. Deci EL, Ryan RM. Self-determination theory: a macro theory of human motivation, development, and health. Canadian Psychol. 2008;49(3):182–185. doi:10.1037/a0012801
79. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52(1):1–26. doi:10.1146/annurev.psych.52.1.1
80. Tajfel H. Social Identity and Intergroup Relations. Vol. 7. Cambridge, UK: Cambridge University Press; 2010.
81. *Omanwar SP, Agrawal RK. Servant leadership, organizational identification, and turnover intention: an empirical study in hospitals. Int J Organ Analysis. 2022;30(2):239–258. doi:10.1108/IJOA-08-2020-2374
82. Hobfoll SE. The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. J Appl Psychol. 2001;50(3):337–421. doi:10.1111/1464-0597.00062
83. *Der Kinderen S, Valk A, Khapova SN, Tims M. Facilitating eudaimonic well-being in mental health care organizations: the role of servant leadership and workplace civility climate. Int J Environ Res Public Health. 2020;17(4):1173. doi:10.3390/ijerph17041173
84. Bakker AB, Demerouti E, Euwema MC. Job resources buffer the impact of job demands on burnout. J Occup Health Psychol. 2005;10(2):170–180. doi:10.1037/1076-8998.10.2.170
85. Demerouti E, Nachreiner F, Bakker AB, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. doi:10.1037/0021-9010.86.3.499
86. *Yasir M, Jan A. Servant leadership in relation to organizational justice and workplace deviance in public hospitals. Leadersh Health Serv. 2023;36(2):164–185. doi:10.1108/LHS-05-2022-0050
87. *Westbrook KW, Nicol D, Nicol JK, Orr DT. Effects of servant leadership style on hindrance stressors, burnout, job satisfaction, turnover intentions, and individual performance in a nursing unit. J Health Manag. 2022;24(4):670–684. doi:10.1177/09720634221128100
88. *Raoush A. Relationship between adopting servant leadership style and employee commitment: empirical evidence from Jordanian governmental hospitals. Probl Perspect Manag. 2022;20(1):299–309. doi:10.21511/ppm.20(1).2022.25
89. *Uktutias SAM, Iswati S, Hadi C, Suhariadi F. Servant leadership and job satisfaction and organizational commitment: empirical evidence from surabaya health care sector. Open Access Maced J Med Sci. 2022;10(E):1082–1093. doi:10.3889/oamjms.2022.9237
90. *Farrington SM, Lillah R. Servant leadership and job satisfaction within private healthcare practices. Leadersh Health Serv. 2019;32(1):148–168. doi:10.1108/LHS-09-2017-0056
91. *Hattab S, Kornelius Y. Effect of servant leadership on the performance of a regional general hospital. Probl Perspect Manag. 2021;19(2):507–518. doi:10.21511/ppm.19(2).2021.40
92. *Cahyono Y, Jihadi M, Arifin Z, et al. Do servant leadership influence market performance? Evidence from Indonesian Pharmacy Industries. Sys Rev Pharm. 2020;11(9):439–451. doi:10.31838/srp.2020.9.62
93. *Sharifizadeh G, Ghavam A, Barzabad PA. Examining the impact of servant leadership on human resources management in Yasouj University of Medical Sciences. Biosci Biotech Res Comm. 2017;1:153–157.
94. *Maglione JL, Neville K. Servant leadership and spirituality among undergraduate and graduate nursing students. J Relig Health. 2021;60(6):4435–4450. doi:10.1007/s10943-021-01311-9
95. Jordan PJ, Troth AC. Common method bias in applied settings: the dilemma of researching in organizations. Aust J Manag. 2020;45(1):3–14. doi:10.1177/0312896219871976
96. Podsakoff PM, MacKenzie SB, Podsakoff NP. Sources of method bias in social science research and recommendations on how to control it. Annu Rev Psychol. 2012;63(1):539–569. doi:10.1146/annurev-psych-120710-100452
97. Korkmaz AV, Van Engen ML, Knappert L, Schalk R. About and beyond leading uniqueness and belongingness: a systematic review of inclusive leadership research. Human Res Manag Rev. 2022;32(4):100894. doi:10.1016/j.hrmr.2022.100894
98. Canavesi A, Minelli E. Servant leadership: a systematic literature review and network analysis. Employ Respons Rights J. 2022;34(6):267–289. doi:10.1007/s10672-021-09381-3
99. Lee A, Lyubovnikova J, Tian AW, Knight C. Servant leadership: a meta-analytic examination of incremental contribution, moderation, and mediation. J Occup Organ Psychol. 2020;93(1):1–44. doi:10.1111/joop.12265
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.