")
Back to Journals » Journal of Healthcare Leadership » Volume 15
Senior Hospital Physician Leaders’ Perspectives on Factors That Impact Physician Engagement: A Qualitative Interview Study
Authors Simard J, Shea C , Cho V, Perrier L , Prokopy M, Moshirzadeh E, Sodhi S, Karsan A, Perreira TA
Received 7 June 2023
Accepted for publication 29 July 2023
Published 16 August 2023 Volume 2023:15 Pages 161—167
DOI https://doi.org/10.2147/JHL.S424741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Julie Simard,1 Christine Shea,1 Veronica Cho,2 Laure Perrier,1 Melissa Prokopy,1,2 Emitis Moshirzadeh,2 Sundeep Sodhi,1,2 Alia Karsan,2 Tyrone A Perreira1,2
1Dalla Lana School of Public Health, Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada; 2Ontario Hospital Association, Toronto, Ontario, Canada
Correspondence: Tyrone A Perreira, Ontario Hospital Association, 200 Front St West, Suite 2800, Toronto, Ontario, M5V 3L1, Canada, Email [email protected]
Background: Physicians are essential in health-care delivery. Physician engagement, defined as active participation in administrative and leadership activities in their organization, is a useful metric for hospital leaders to evaluate as they develop and implement strategy. The purpose of this study was to gain insight into the perspectives of senior hospital physician leaders on factors impacting physician engagement.
Methods: Semi-structured interviews were conducted virtually. A purposive sample was used. Hospital physician senior leaders were recruited from Ontario public hospitals in Canada. The interviews were recorded, transcribed verbatim, and analyzed.
Results: Ten participants in senior hospital physician leadership positions were interviewed. Seven themes were identified as impacting physician engagement: being seen and being heard, accountability, trust, leadership engagement, intercommunication, organizational stability, and discord within the organization. Saturation of themes was achieved.
Conclusion: Two-way communication is essential to physician engagement. Physician input in decision-making processes is a vital way to improve engagement. For this to work, leadership must also be engaged. Trust and accountability are critical attributes for senior hospital physician leaders, especially during times of organizational instability. For physicians whose remuneration model is fee-for-service, new compensation models are required for them to actively participate in hospital decision-making.
Keywords: physician engagement, hospitals, leadership, interviews as a topic, qualitative research
Background
Health systems face social, economic, and political challenges, which demand continual adjustments, transformations, and adaptations.1–3 One problem increasingly requiring attention is workforce issues.1,4 Significant challenges exist, including shortages, unequal distribution of health workers, limited resources, and fiscal constraints.1,3,4 Hospital leadership plays an essential role in personnel management, including fostering commitment from the workforce to improve health-care services.5 Employee engagement is critical to create and sustain harmonious work environments. Kleine et al found supportive leadership behaviour, commitment, and perceived organizational support are associated with an employee thriving at work.6 Hospital leaders must consider strategies to measure and enhance physician engagement, which is defined as the active involvement and participation of physicians in administrative and/or leadership activities in their organization.7,8 Limited studies exist on this topic, and few examine efforts to measure, plan, or improve physician engagement.7,9 The purpose of this study was to gain insight into the perspectives of senior hospital physician leaders on factors impacting physician engagement.
Methods
Recruitment and Data Collection
Semi-structured interviews were conducted with individuals currently employed in leadership positions at hospitals in Ontario, Canada. Ontario houses more than a third of Canada’s population and presently has 140 public hospital corporations operating over 220 sites.10,11 Recruitment efforts were optimized to include participants from different regions and hospital sizes, and written consent was obtained from each participant in this purposive sample. Participant informed consent included publication of anonymized responses. The study team met to design the study, select participants, and refine the semi-structured interview guide.12,13 All interviews were conducted virtually by team members (JS, EM) in May 2022. Participants were first provided with a definition of physician engagement: active participation of physicians in deciding how their work is done, making suggestions for improvement, goal setting, planning, and monitoring of their performance in activities targeted at the patient, organization, and/or health system levels.7 Participants were then specifically asked to describe physician engagement at their site and identify factors that impacted engagement, whether positive or negative. The study was approved by the University of Toronto Research Ethics Board (RIS Human Protocol Number 40771).
Data Analysis
Interviews were recorded and transcribed. Two investigators (VC and LP) read and reviewed the transcripts to achieve immersion.14 A sensitizing framework was used whereby the researchers entered the study with open minds and no preconceived theories or hypotheses. Using content analysis and constant comparison to analyze the data, a thematic approach was applied.15,16 Two investigators (VC and LP) independently coded the first two transcripts, and following this, a meeting was held to compare the codes generated. Commonalities, wording, and inconsistencies were discussed to reach a consensus and generate a final set of codes to code further transcripts. Transcripts were coded in groups of two or three, and a meeting was held to resolve coding discrepancies for each set. When coding was completed, all data were put into Microsoft Excel (Microsoft, USA) to organize data by codes and review. A third investigator (TP) provided verification and review of codes. To establish trustworthiness, referential adequacy, peer review, and triangulation were used. The interviewers (JS and EM) reviewed the final codes to ensure accurate reflection of interviews. An independent, qualified, and impartial colleague (CS) reviewed and assessed transcripts, methodology, and findings. Finally, researchers (TP, MP, CS, and JS) reviewed recent quantitative physician engagement survey results from each participant’s site to verify alignment of qualitative and quantitative data.
Rigour and Quality
Lincoln and Guba’s framework were used to enhance the rigour and quality of the study, and the following triangulation process ensured findings arose from investigator consensus.17 All procedures were documented so that coding development could be traced. Transcripts were coded and analyzed independently by two investigators who discussed all discrepancies until agreement was reached. For transparency, participants’ quotes are provided to support themes and allow the reader to determine if the findings reflect participants’ perceptions.
Results
We interviewed six females and four males holding senior hospital physician leadership positions in Ontario, Canada (Table 1). Saturation of themes was achieved after coding the second transcript. We used a method to determine the saturation of themes validated by Guest et al,18 and the calculations can be reviewed in Supplementary Material. Seven themes were identified: being seen and being heard, accountability, trust, leadership engagement, intercommunication, organizational stability, and discord within the organization. Each theme is described below, and illustrative quotes are provided in Table 2.
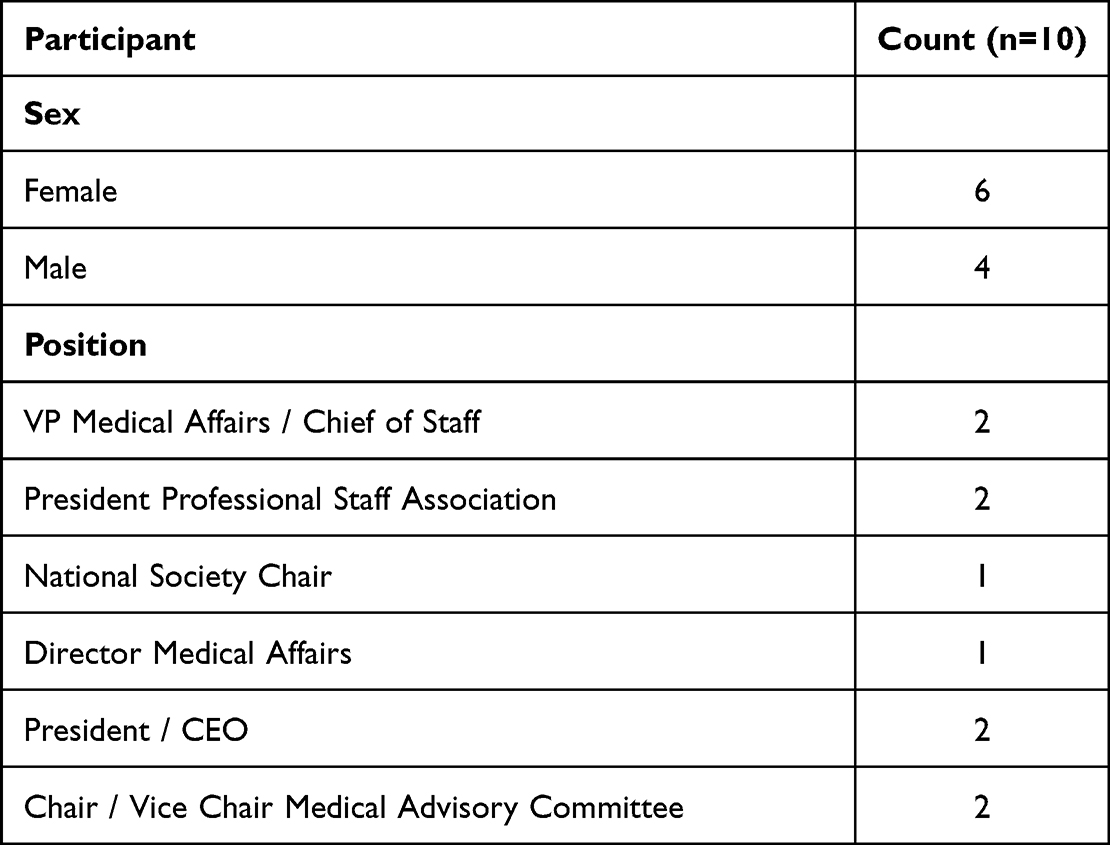 |
Table 1 Participant Characteristics |
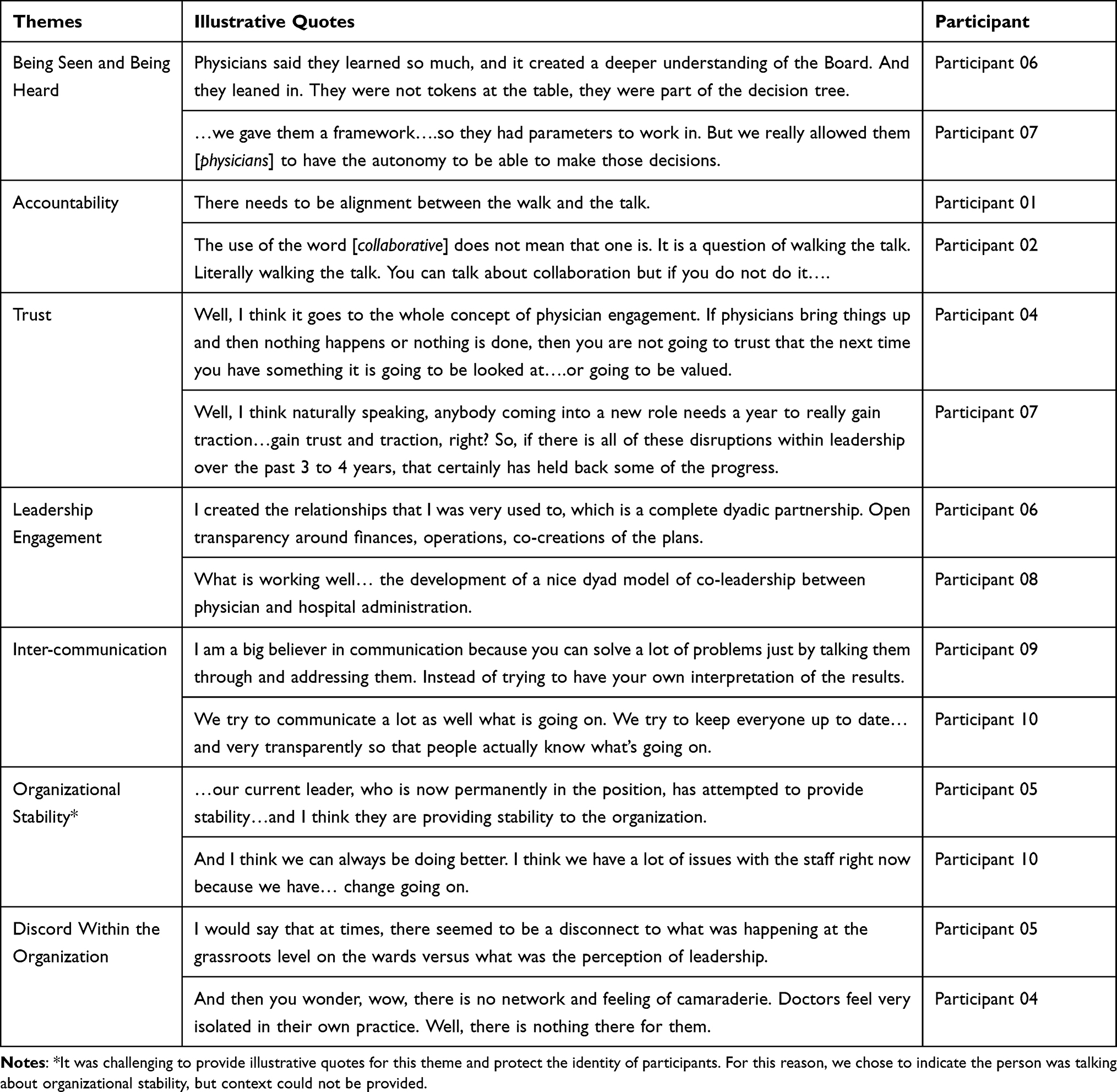 |
Table 2 Themes Derived and Illustrative Quotes |
Being Seen and Being Heard
Being seen and being heard describes instances when physician input was explicitly sought by hospital leadership, and physician perspectives were heard and respected. This was portrayed as contributing to enhanced physician engagement. This encompasses physicians perceiving their position and input/feedback to be well represented and valued. This does not always equate with decisions being favorable to physicians. It does signify that physicians were included in the decision-making process.
Accountability
Accountability was identified as an essential component of building relationships and fostering physician engagement. Accountability included instances of hospital leadership acknowledging their responsibility to deliver and follow up on requests. More than one participant specifically stated the importance of senior leaders “walking the talk”. The failure of senior leadership to take responsibility and to be accountable was seen as undermining physician engagement. An example of this provided by one participant was hospital leaders who continually blamed external groups over a period of years for failing to deliver equipment requested by physicians that hospital leadership agreed to provide.
Trust
Hospital leaders listed trust as key to building relationships and facilitating physician engagement. Lack of trust was identified as eroding physician confidence in hospital leadership. Once trust was broken, e.g., making promises that were not fulfilled, it took a long time to rebuild. In contrast, maintaining an “open door” policy that encouraged conversations with physicians was an example provided by one participant as a way to build trust [Participant 06].
Leadership Engagement
Engagement is a two-way street, and leadership engagement indicates efforts and initiatives by hospital leaders to meet physicians halfway. It denotes efforts on the part of leadership to reach common goals with physicians by engaging and working with physicians. This includes fostering environments of inclusion by explicitly asking for physician input on solutions to current challenges, accommodating physician schedules by arranging meetings at times convenient for physicians, and proactively anticipating issues or challenges such as arranging alternate resting quarters for physicians to sleep during the COVID pandemic.
Intercommunication (Two-Way Communication)
Participants offered numerous general statements about communication to indicate its importance as a staple of relationships necessary as an essential element in physician engagement (e.g., “we try to communicate a lot”) [Participant 10], “communication is important” [Participant 03)]. We created this separate code because, in these instances, there were no tangible or concrete examples attached to the statements. Rather, they were broad generalizations about relationships with no specific actions associated with them. It differs from being seen and being heard, where the focus of communication is specifically on physician input and discord within the organization where relationships were fractured and, in some cases, a lack of communication was mentioned.
Organizational Stability
Stability identifies unstable institutional environments that threaten physician engagement. Examples included major institutional change or transformations (e.g., hospital mergers or unexpected changes in top leadership), change with resources (e.g., budget constraints resulting in items requested by physicians not being obtained), or system (e.g., a “regulation that comes from the Ministry” that creates a constraint in the system resulting in friction with physicians [Participant 09]).
Discord Within the Organization
Discord within the organization denoted a fracture in relationships with hospital leadership that was damaging to physician engagement. These are instances where participants described a lack of support or harmony at an institutional level, including indifference (e.g., management holding meetings important to physicians at times when physicians could not attend; leadership choosing not to involve physicians in decision-making), misaligned views (e.g., expecting physicians to take on duties outside of practice; forced continuing education on topics unrelated to physician practice), and alienation (e.g., negatively targeting physicians). These difficulties were often a result of diverging priorities or agendas.
Discussion
The purpose of this study was to gain insight into the perspectives of senior hospital physician leaders on factors impacting physician engagement. We interviewed ten participants in senior hospital physician leadership positions and asked about their perceptions of factors that impact physician engagement. Analysis of the transcripts generated seven themes. One theme is directly related to physician presence and voice (being seen and being heard). Four themes explicitly focus on behaviours and actions of hospital leaders (accountability, trust, communication, and leadership engagement), and two were related to organizational factors (organizational stability and discord within the organization).
Physician Presence and Voice
Being seen and being heard, which describes positive relationships and high engagement when physicians have opportunities to provide input into decision-making, and this input is listened to. Participants indicated that the expectation was not that physicians thought they should always receive what they requested, but rather that they were part of the decision-making process. Being part of this process provided a more extensive understanding of the organization’s inner workings. This helps to avoid situations whereby “suggestions might not get implemented. But people never know why. And then after a while, they stop talking” [Participant 04]. Inviting physicians to sit at the table and participate in decision-making allowed for “a lot of learning on both sides” [Participant 06] and help ensure that
the doctors know the process – and what a capital project looks like with the Ministry (of Health)…they were completely unaware of the time frames, the stages we had to go through, all of the approval processes. [Participant 07]
Current literature suggests that leaders may want to consider “listening sessions” as a great way to get feedback and input from physicians, however, these sessions must be carefully planned and facilitated to ensure they are constructive and do not turn into simply complaint sessions with no resolve.19
Behaviours and Actions of Hospital Leaders
Accountability, trust, leadership engagement, and intercommunication are the themes most closely associated with hospital leaders. These themes align with the results of a physician engagement concept analysis, which identifies accountability, communication, and interpersonal relations as precursors of physician engagement.7 This concept analysis also indicates defining attributes of physician engagement include physicians having regular participation in (i) deciding how their work is done, (ii) making suggestions for improvement, and (iii) planning.7 The results of our current study reinforce these components of physician engagement as we report on the importance physicians place in being actively involved in decision-making.
Organizational Factors
The two themes related to organization factors, discord within the organization and organizational stability, were associated with decreased physician engagement. Discord within the organization describes an erosion of confidence in leadership and physician’s perceived lack of sincerity. This code represents the friction between hospital leaders and physicians, including instances such as the absence of physician representation in decision-making. One aspect of the discord within the organization theme highlighted a tension that is challenging to resolve within hospitals, compensation. Ensuring physicians are invited to sit at the table to make decisions can require commitment to committee work, which is typically unpaid work for practicing physicians who are remunerated using a fee-for-service model. This was mentioned as potentially contributing to burnout, particularly during the COVID pandemic. While our theme being seen and being heard strongly indicates physicians want to provide input into hospital decisions, they may be required to give up their free time to provide that input. This is not a new issue in Canada and has been discussed in the literature for many years.20
Organizational stability highlights instances of internal turmoil or external forces that limit the institution’s impact on physician engagement and identifies aspects of physician engagement that may be difficult to manage. Hospital mergers are an example of times of change when attention can be diverted to other activities. Similarly, public hospitals are bound to work with government bodies, and their control may be restricted, for example, in making decisions or fulfilling timelines on capital projects. While hospitals have limited influence in these circumstances, our data provide cases where institutions actively engaged physicians in decision-making, resulting in them having a better understanding of processes relating to external groups such as government bodies. This aligns with the literature on hospital mergers, which suggests that more time should be spent following up and engaging with staff after mergers to ensure the success of the merger process and other organizational changes.21
Limitations
Two of our themes, discord within the organization and organizational stability, touched on unfavourable circumstances in organizations. Given that we conducted interviews during the COVID pandemic, this raises the question of whether the pandemic played a role in generating these themes that may not have emerged otherwise. However, when we reviewed the data, participants provided examples and pointed to situations independent of the COVID pandemic (e.g., hospital mergers; leadership changes) and none of the participants described the COVID pandemic as a sole factor to organizational discord and instability. Furthermore, given our findings suggest that engagement is enhanced by senior leaders with strong people skills, this study may be generalizable to other health-care settings in the province of Ontario, Canada, and globally.
Directions for Future Research
These findings build on previous work,7 adding to the knowledge on physician engagement precursors, specifically communication, accountability, and interpersonal relations. Additional research is warranted on remuneration models and physician engagement. Our data support that physicians strongly want to participate in hospital decision-making; however, those being compensated using a fee-for-service model, are often required to do so without compensation. This area requires further exploration to identify what is being compromised and possible missed opportunities for hospitals when the fee-for-service model is used.
Conclusion
Most hospital leaders in our study conveyed that two-way communication was essential to physician engagement. Seeking input from physicians and including them in decision-making processes were also identified as vital ways to improve engagement. For this to work, leadership must also be engaged. Trust and accountability emerged as critical attributes for senior hospital physician leaders, especially during times of organizational instability. For physicians whose remuneration model is fee-for-service, new compensation models are required for them to actively participate in hospital decision-making.
Acknowledgments
We would like to thank all participants that volunteered for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. World Health Organization. Global strategy on human resources for health: workforce 2030. Geneva: World Health Organization; 2016. Available from: https://www.who.int/publications/i/item/9789241511131.
2. American Hospital Association. Data brief: health care workforce challenges threaten hospitals’ ability to care for patients. Available from: https://www.aha.org/system/files/media/file/2021/11/data-brief-health-care-workforce-challenges-threaten-hospitals-ability-to-care-for-patients.pdf.
3. Boniol M, Kunjumen T, Nair TS, Siyam A, Campbell J, Diallo K. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Glob Health. 2022;7(6):e009316. doi:10.1136/bmjgh-2022-009316
4. West M, Dawson J. Employee Engagement and NHS Performance. London: King’s Fund; 2012.
5. Reich MR, Javadi D, Ghaffar A. Introduction to the special issue on “effective leadership for health systems”. Health Syst Reform. 2016;2(3):171–175. doi:10.1080/23288604.2016.1223978
6. Kleine AK, Rudolph CW, Zacher H. Thriving at work: a meta‐analysis. J Organ Behav. 2019;40(9–10):973–999. doi:10.1002/job.2375
7. Perreira TA, Perrier L, Prokopy M, Neves-Mera L, Persaud DD. Physician engagement: a concept analysis. J Healthc Leadersh. 2019;11:101–113. doi:10.2147/JHL.S214765
8. Kaissi A. Enhancing physician engagement: an international perspective. Int J Health Serv. 2014;44(3):567–592. doi:10.2190/HS.44.3.h
9. Reinertsen JL, Gosfield AG, Rupp W, Whittington JW. Engaging physicians in a shared quality agenda. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement; 2007. Available from: www.ihi.org/resources/Pages/IHIWhitePapers/EngagingPhysiciansWhitePaper.aspx.
10. Statistics Canada. Population and dwelling counts: Canada, provinces and territories. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=9810000101.
11. Ministry of Health. Questions and answers. Available from: https://www.health.gov.on.ca/en/common/system/services/hosp/faq.aspx.
12. Patton MQ. Qualitative Research and Evaluation Methods: Integrating Theory and Practice. Thousand Oaks: Sage; 2014.
13. Britten N. Qualitative interviews in medical research. BMJ. 1995;311(6999):251–253. doi:10.1136/bmj.311.6999.251
14. Braun V, Clark V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
15. Hsieh H, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
16. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–111. doi:10.1111/j.1365-2648.2007.04569.x
17. Lincoln Y, Guba E. Naturalistic Inquiry. Newbury Park, CA: Sage Publications; 1985.
18. Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. 2020;15(5):e0232076. doi:10.1371/journal.pone.0232076
19. Shanafelt TD, Larson D, Bohman B, et al. Organization-wide approaches to foster effective unit-level efforts to improve clinician well-being. Mayo Clin Proc. 2023;98(1):163–180. doi:10.1016/j.mayocp.2022.10.031
20. Dubìnsky IL, Greengarten M, Grossman L, Hundert M, Sawatzky D, Whittaker B. Implementing a physician leader compensation program at a major community hospital. Healthc Q. 2008;11(2):58–61. doi:10.12927/hcq.2008.19617
21. Sisti LG, Mariani M, De Vito C, et al. Paying attention to personnel in organizational changes: the impact of hospital mergers. Eur J Public Health. 2019;29(Supplement_4). doi:10.1093/eurpub/ckz186.381
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.