")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Semaglutide Effects on Metabolic Outcomes in Diabetes Mellitus Patients — Real World Study
Authors Balcázar-Valencia CM , García-Ramos AF , Osorio-Toro LM , Ordoñez-Guzmán YA, Buitrago-Gómez N , Cabarcas-López WF , Vizcaino-Guerrero CJ, Daza-Arana JE , Ramírez-Rincón A , Restrepo-Erazo K
Received 21 October 2023
Accepted for publication 11 January 2024
Published 10 April 2024 Volume 2024:17 Pages 1667—1673
DOI https://doi.org/10.2147/DMSO.S443115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Carlos Mario Balcázar-Valencia,1 Andrés Felipe García-Ramos,2– 5 Luis Miguel Osorio-Toro,2,3,6 Yessica Alejandra Ordoñez-Guzmán,3 Nathalia Buitrago-Gómez,4 William Fernando Cabarcas-López,7 Carlos Javier Vizcaino-Guerrero,8 Jorge Enrique Daza-Arana,2,9 Alex Ramírez-Rincón,4 Katherine Restrepo-Erazo2,10
1Specialization in Internal Medicine, Faculty of Health Sciences, Universidad Libre, Santiago de Cali, Colombia; 2Specialization in Internal Medicine, Faculty of Health, Universidad Santiago de Cali, Santiago de Cali, Colombia; 3Research and Education Department, Clínica de Occidente S.A., Santiago de Cali, Colombia; 4Specialization in Endocrinology, Faculty of Health Sciences, Universidad Pontificia Bolivariana, Medellín, Colombia; 5Specialization in Internal Medicine, Faculty of Health, Universidad del Valle, Santiago de Cali, Colombia; 6Genetics, Physiology and Metabolism Research Group (GEFIME), Faculty of Health Sciences, Universidad Santiago de Cali, Santiago de Cali, Colombia; 7Master in Epidemiology, Faculty of Health, Universidad de Caldas, Manizales, Colombia; 8Specialization in Endocrinology, Faculty of Health, Fundación Universitaria Ciencias de la Salud FUCS, Bogotá, Colombia; 9Health and Movement Research Group, Faculty of Health Sciences, Universidad Santiago de Cali, Santiago de Cali, Colombia; 10Specialization in Endocrinology, Faculty of Health, Universidad Nacional de Colombia, Bogotá D.C., Colombia
Correspondence: Jorge Enrique Daza-Arana, Specialization in Internal Medicine, Faculty of Health, Universidad Santiago de Cali, Calle 5 # 62-00, Santiago de Cali, Colombia, Tel/Fax +57 3108923676, Email [email protected]
Purpose: Diabetes is a public health problem that requires strategies to impact glycemic control and reduce the risk of long-term medical complications. Pharmacological management is a necessary treatment for this disease. Therefore, semaglutide is an essential tool to achieve the treatment targets. The present study aimed to evaluate the semaglutide effects on a cohort with type 2 diabetes mellitus (T2DM) in Colombia.
Materials and Methods: The cohort included 49 patients with T2DM that have been treated in a specialized care center. Their glycemic outcomes, weight, renal function, and adverse events were evaluated through a 3-, 6- and 12-month follow-up.
Results: Significant differences were observed in the outcome evaluation: reduction of glycated hemoglobin levels (MD − 2.74 CI − 1.95 to − 3.52 in 6 months), fasting plasma glucose levels, body weight (MD − 7.11 CI − 5.97 to − 8.24), and the albumin-to-creatinine ratio. The results were maintained throughout the treatment period. The adverse event rate was 16.3%, predominating gastrointestinal events.
Conclusion: This real-world evidence shows the efficacy of semaglutide in achieving treatment goals in patients with T2DM.
Keywords: semaglutide, diabetes mellitus, glycated hemoglobin A, obesity, glycemic control
Introduction
Type 2 diabetes mellitus (T2DM) is a current public health problem due to its high disease burden.1 Since the first edition in 2000, the estimated prevalence of diabetes in adults aged 20–79 years has more than tripled, from an estimated 151 million (4.6% of the global population at the time) to 537 million (10.5%) today. Without sufficient action to address the situation, it is estimated that 643 million people will have diabetes by 2023 (11.3% of the population). If trends continue, the number will jump to a staggering 783 million (12.2%) by 2045.2 These figures are due to the chronicity of the disease and the emergence of new cases. T2DM is characterized by the complexity of its metabolic interactions, where insulin resistance and hyperglycemia play an essential role,3 resulting in an increased risk of microvascular and macrovascular complications.4 Because of its implications, DM management requires strategies to reduce risks, positively impact glycemic control, and decrease cardiovascular complications.5 In addition to structured and individualized nutritional interventions and regular physical activity, most T2DM patients should start a pharmacological treatment. The best-choice medication should be based on individualized targets for glycemic control, comorbidities, life expectancy, and cardiovascular risk.6
Recently published studies have positioned glucagon-like peptide-1 receptor agonists (GLP1-RAs) in a leading role in metabolic regulation by stimulating glucose-dependent insulin synthesis and secretion, inhibiting glucagon secretion, delaying gastric emptying, and increasing satiety.7 Semaglutide, a GLP1-RAs, has shown benefits in treating T2DM patients by reducing glycated hemoglobin (HBA1c) levels and body weight, with a low hypoglycemia risk.8–10 Hence, semaglutide is an option for T2DM patients with a high cardiovascular risk who cannot reach control with oral medications.11
Recently, semaglutide has been introduced to the Latin-American market. Our study aims to evaluate the response to semaglutide treatment in a cohort of T2DM patients regarding glycemic control, body weight, renal function, and safety in a Latin-American real-world setting.
Materials and Methods
Subjects and Study Design
We performed an observational and retrospective cohort study. We included adults diagnosed with T2DM under semaglutide treatment in a structured and comprehensive chronic care model in a specialized diabetes care center in Cali, Colombia, between March 2020 and September 2021. All subjects who received treatment for at least one year and had at least two follow-up visits were included. An investigator extracted information from medical records regarding baseline variables and follow-up consultations three, six, and twelve months after starting semaglutide treatment. Semaglutide was administered subcutaneously at a starting dose of 0.25 mg once weekly, and, after four weeks, the dose was increased to 0.5 mg once weekly, according to the indications for use. The primary outcomes were the change in the HbA1c absolute values and weight recorded in the follow-up visits compared to the values obtained at the first medical consultation where semaglutide was prescribed. The secondary outcomes were the proportion of subjects who achieved the target glycemic control (HbA1c ≤7%), change in the albumin-to-creatinine ratio (ACR), fasting plasma glucose, adherence, cause of treatment discontinuation, and adverse events.
Statistical Analysis
Central tendency and dispersion measures were calculated for quantitative variables according to their distribution. Absolute frequencies and percentages were calculated for qualitative variables. To measure changes over time in the quantitative variables of interest from baseline (t0), mean differences and their respective 95% confidence intervals were calculated and tested through repeated-measures ANOVA. In addition, the percentage of patients at HbA1c and ACR targets (according to the microalbuminuria and macroalbuminuria classification) was compared to baseline values through McNemar’s test. All statistical analyses were performed using R statistical software.
This study was conducted pursuant to the international recommendations for clinical research included in the Declaration of Helsinki. According to Resolution 8430 of 1993 issued by Ministerio de Salud de Colombia (Ministry of Health of Colombia), this study was classified as a risk-free research, since data was collected from secondary sources. This project was approved by our Ethics and Research Committee of the Universidad Libre (Minutes No. 010/2021). The Institutional Ethics Committee, in considering a risk-free study, did not consider the informed consent of the study subjects necessary.
Results
A total of 49 patients who met the study selection criteria were included in the study. 27 (55.1%) were women, the mean age was 60.8 years old, and 79.6% of patients participated in a patient support program focused on self-care, education, and treatment adherence. The mean basal weight was 84.2 kilograms, median fasting plasma glucose was 200 mg/dl, and ACR was 37.6 mg/g (Table 1).
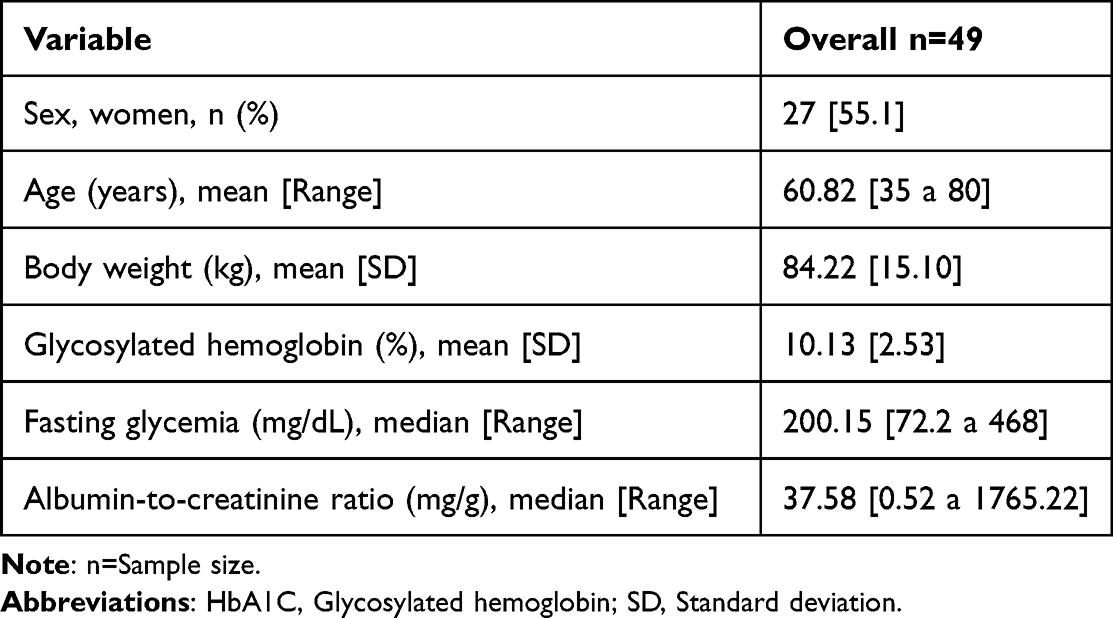 |
Table 1 Demographic and Basal Characteristics of the Studied Cohort |
At baseline, the HbA1c mean was 10.1%, with a progressive decrease during follow-up at three, six, and twelve months (8%, 7.4%, and 7.4%, respectively). Significative differences (p=0.000) from basal rates were detected at three, six, or twelve months (Figure 1). The percentage of patients that achieved the HbA1c targets was 12.2% at the beginning of the study. Then, it increased to 38.8% in month 3, and it reached 63.8% in month 6 when 96% of participants (n=47) were still treated with semaglutide. At month 12, the proportion of patients with HbA1c > 7% was significantly higher compared to the proportion of patients in goals at baseline (p=0.001).
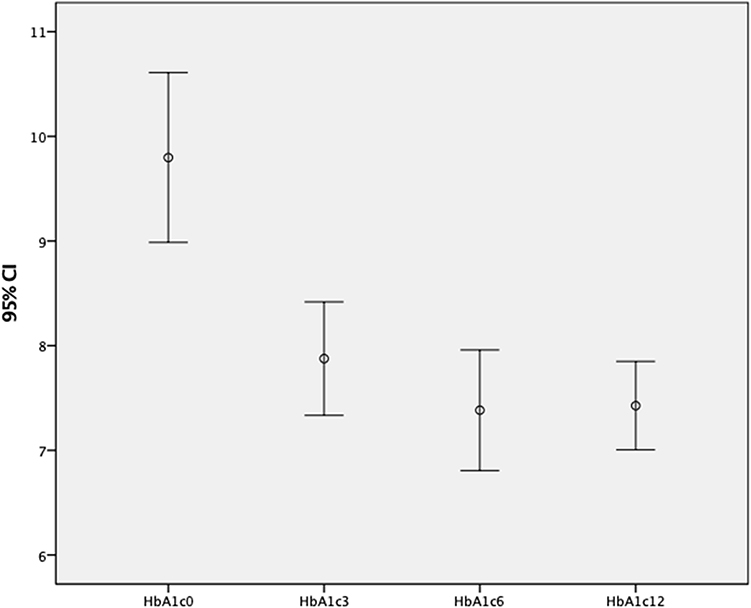 |
Figure 1 Glycosylated hemoglobin at baseline and 3-, 6-, and 12-months follow-up. Abbreviation: HbA1C, Glycosylated hemoglobin (5). Note: n=Sample size. |
Likewise, fasting plasma glucose (basal mean 221.4 mg/dl) showed a reduction during the follow-up (the estimated means were 153.8 mg/dl [month 3], 129.8 mg/dl [month 6], and 135.9 mg/dl [month 12]). The mean differences in fasting plasma glucose during follow-up were statistically significant (p=0.000). A post hoc Bonferroni correction showed that the fasting plasma glucose was statistically different in months 3 and 6, the fasting plasma glucose decreased by 67.6 mg/dl in month three compared to the beginning of the treatment, and the reduction was 91.6 mg/dl in month six compared to the basal rates.
The initial patients’ mean weight was 84 kg (a range between 59 kg and 122 kg). Then, it decreased in months 3 (mean=81.1 Kg), 6 (mean= 76.7 kg), and 12 (mean= 77.9 kg). The mean differences in basal weight rates were statistically significant (p=0.000) in all follow-up visits (Figure 2).
 |
Figure 2 Baseline body weight and at follow-up at 3, 6 and 12 months. Notes: Weight is expressed in kilograms, n=Sample size. |
The ACR mean was 184.3 mg/g at the beginning of the study. During months 3 and 6, this value decreased (the mean was 114.5 mg/g and 89.4 mg/g, respectively). By month 12, there was an increase compared to the previous follow-up (the mean was 92.4 mg/g); however, it maintained a 50% decrease compared to the baseline values. When classifying the ACR rates, statistically significant differences were found between the 3-month and 6-month visits compared to basal rates finding a larger proportion of patients who had normal values (Table 2).
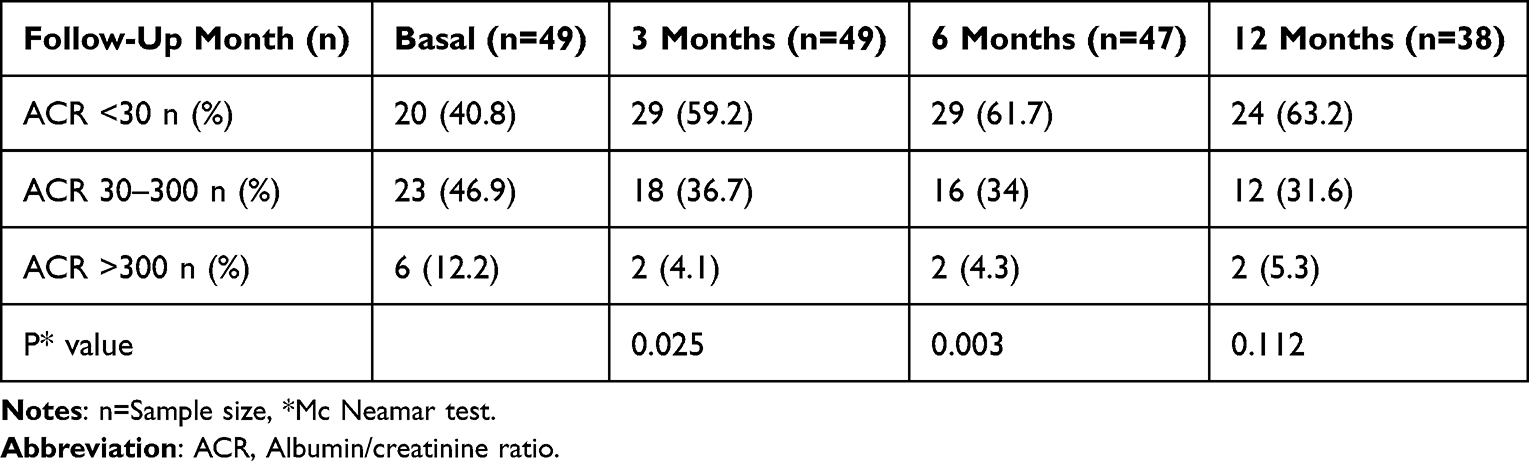 |
Table 2 ACR Index Classification Baseline and During the Follow-Up |
Regarding the safety of semaglutide treatment, 16.3% of patients (8 cases) presented some adverse events during the follow-up year, in half of the cases led to the treatment discontinuation (Table 3). The 20.4% of subjects discontinued the treatment due to barriers to access and distribution of the medication. 2 patients died of SARS-CoV-2 infection during the follow-up.
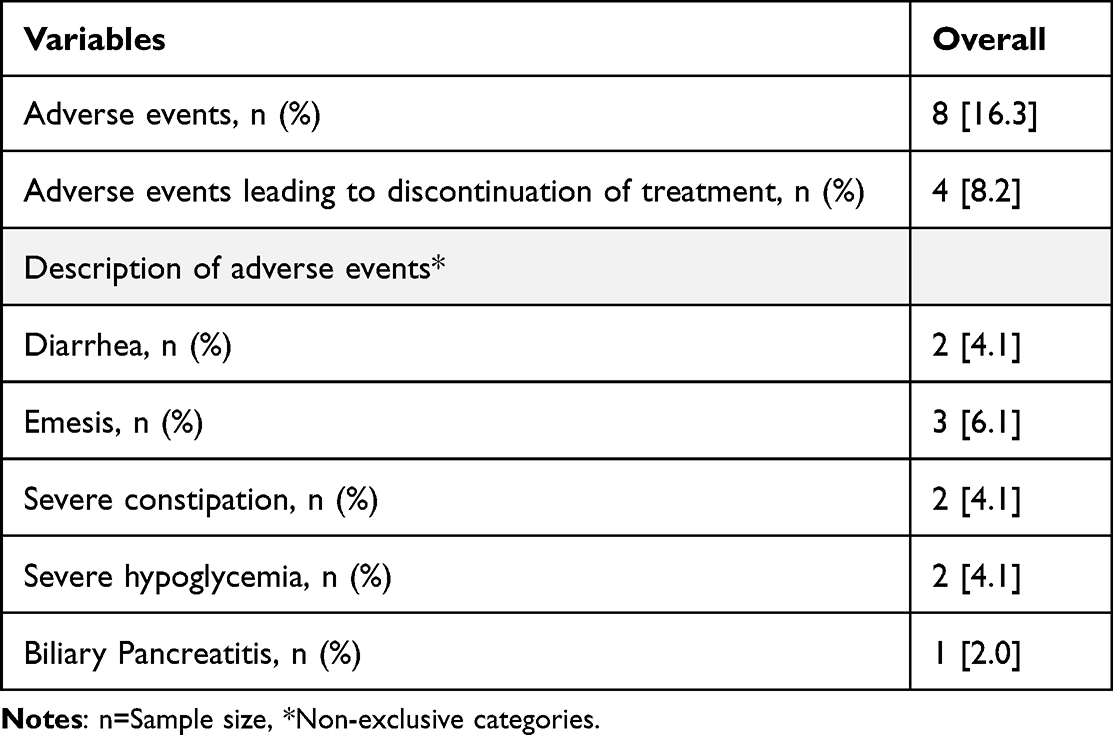 |
Table 3 Adverse Reactions Presented During the Study Time |
Discussion
Appropriate pharmacological management is an essential part of the treatment for T2DM because it allows the achievement of glycemic targets and, ideally, reduces the clinical impact and the disease burden.4 In different studies, GLP1-RAs have shown benefits in treating T2DM by achieving greater glycemic control12 and decreasing macrovascular complications.13,14
In this study, we observed a significant improvement in glycemic parameters: the net reduction of HbA1c at 12-month follow-up was 2.67%, and the decrease in the mean of fasting plasma glucose was 85.5 mg/dl. These results are similar to published reports from the SUSTAIN clinical trial program.12 Furthermore, semaglutide in doses of 0.5 and 1 mg has reduced HbA1c levels between 1.2–1.5% and 1.5–1.8%, respectively. It also reduces body weight between 3.5–4.6 kg (0.5 mg dose) and 4.5–6.5 kg (1 mg dose), demonstrating even better efficacy than Dulaglutide.14 Specifically, with Hb1AC, a substantial decrease at 12-month follow-up was achieved that was similar to the results of Frías et al15 the effects of two doses of semaglutide were evaluated, showing a reduction of HbA1c by 2.2 percentage points (2.0 mg dose) and −1.9 percentage points (1.0 mg dose) during a 40-week follow-up.
On the other hand, when evaluating the HbA1c values in controlled/uncontrolled categories following the reference of HbA1c less than or equal to 7%, it was found that a significantly high proportion of patients reached treatment targets in all evaluated periods (38.8% [month 3], 63.8% [month 6], and 48.6% [month 12]) compared to the initial rates (12.2% of the population at glycemia targets). These results coincide with a real-world evidence study conducted in Italy, where HbA1c targets were achieved at 6-month follow-up by 61% of patients and 12-month follow-up by 57% of patients.16
The follow-up results showed significant changes in HbA1c and fasting plasma glucose compared to the initial rates in months 3 and 6. Those values, as well as the body weight results, increased slightly towards month 12 may be due to alterations in adherence and medication discontinuation. The causes were not addressed in detail in this study.
In addition, statistically significant reductions in body weight were documented up to 7.1 kilograms on average during the follow-up period. This effect was similar to the results found in most studies of this medication. For example, Wilding et al found that weight decreased by 14.9% at a 68-week follow-up,17 while the research by Rubino et al documented an average weight decrease of 10.6% at a 20-week follow-up.18 These results support that semaglutide positively impacts body weight control with other metabolic variables such as abdominal circumference and lipid profile.19
The present study showed that the ACR decreased during the follow-up of patients treated with semaglutide. Therefore, it reduces the proportion of patients with microalbuminuria and macroalbuminuria. These findings coincide with the results from the subgroup analysis of the SUSTAIN 6 study, where it was documented a decrease in the nephropathy risk (HR 0.64 CI 95% 0.46–0.88).20 As an effect of the pharmacological group, GLP-1 RAs have shown a positive renal impact with a 17% reduction of renal function damage (HR 0.83 CI 95% 0.78–0.89 p<0.0001), mainly due to a reduction of urinary albumin excretion.21 A recent meta-analysis evaluating renal outcomes of GLP-1 RAs showed that each 1% reduction in HbA1c was associated with a decrease of 35% (p 0.040) in the risk of composite renal outcomes (macroalbuminuria onset, reduction in the estimated glomerular filtration rate, or increased creatinine).10
In the SUSTAIN studies, semaglutide had a safety profile similar to other GLP-1 RAs, where the most common adverse reactions were gastrointestinal, such as nausea, diarrhea, and vomiting. It caused to stop using this medication in almost half of the patient.15,22 Likewise, the most common adverse reactions were gastrointestinal in the present real-world evidence: (n=7) emesis, (n=3) diarrhea, (n=2) and constipation (n=2). Two patients presented severe hypoglycemia; thus, treatment was discontinued in both cases. An isolated case of pancreatitis was reported without suspected causality, considering that this outcome is rare in SUSTAIN studies. No association between the event and the semaglutide treatment was demonstrated.22,23
The semaglutide discontinuation happened in the 28.57% (14 patients) cases: four were due to the adverse reactions mentioned above, and ten were due to access issues. These figures are relevant because proper medication administration (frequency and dosage) is essential for the expected positive results.
This study has several limitations, including the small sample size and other biases inherent to data sourced by retrospective, observational, and real-world evidence studies. It should also be understood that semaglutide is a recently approved medication in the country and its medical practice. Despite that scenario, the study opens the door to further research that could generate different results on semaglutide performance. Also, new research can provide evidence for better clinical decisions and the comprehensive management of T2DM patients with short- and long-term targets. The present study provides scientific knowledge with interesting data on the application of this drug in the Latin American context, a region in which few studies are currently reported in the literature. In addition, it includes the results of the metabolic variables described in previous studies worldwide and allows us to observe their behavior in the local population.
Conclusion
The present real-world evidence study associates semaglutide treatment with improving fasting plasma glucose and HbA1c control. Besides, it improves ACR and decreases total body weight in T2DM patients. Furthermore, semaglutide treatment was well tolerated, and there were low rates of treatment discontinuation.
Abbreviations
T2DM, Type 2 diabetes mellitus; GLP1-Ras, glucagon-like peptide-1 receptor agonists; HBA1c, glycated hemoglobin; ACR, albumin-to-creatinine ratio; HR, Hazard Ratio.
Acknowledgments
This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 01-2024.
Funding
The research team’s activities were sponsored by clinical institution and the Universidad Santiago de Cali. However, the authors declare full autonomy when conducting all phases of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lovic D, Piperidou A, Zografou I, Grassos H, Pittaras A, Manolis A. The growing epidemic of diabetes mellitus. Curr Vasc Pharmacol. 2020;18(2):104–109. doi:10.2174/1570161117666190405165911
2. International Diabetes Federation. IDF Diabetes Atlas, 10th edn. Brussels, Belgium: International Diabetes Federation; 2021. Available from: https://www.diabetesatlas.org.
3. Pearson ER. Type 2 diabetes: a multifaceted disease. Diabetologia. 2019;62(7):1107–1112. doi:10.1007/s00125-019-4909-y
4. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
5. Damaskos C, Garmpis N, Kollia P, et al. Assessing cardiovascular risk in patients with diabetes: an update. Curr Cardiol Rev. 2020;16(4):266–274. doi:10.2174/1573403X15666191111123622
6. ElSayed NA, Aleppo G, Aroda VR, et al.; on behalf of the American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140–S157. doi:10.2337/dc23-S009
7. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740–756. doi:10.1016/j.cmet.2018.03.001
8. Christou GA, Katsiki N, Blundell J, Fruhbeck G, Kiortsis DN. Semaglutide as a promising antiobesity drug. Obes Rev. 2019;20(6):805–815. doi:10.1111/obr.12839
9. Smits MM, Van Raalte DH. Safety of semaglutide. Front Endocrinol. 2021;12:645563. doi:10.3389/fendo.2021.645563
10. Yoshiji S, Minamino H, Tanaka D, Yamane S, Harada N, Inagaki N. Effects of glucagon-like peptide-1 receptor agonists on cardiovascular and renal outcomes: a meta-analysis and meta-regression analysis. Diabetes Obes Metab. 2022;24(6):1029–1037. doi:10.1111/dom.14666
11. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. doi:10.1016/j.molmet.2020.101102
12. Aroda VR, Ahmann A, Cariou B, et al. Comparative efficacy, safety, and cardiovascular outcomes with once-weekly subcutaneous semaglutide in the treatment of type 2 diabetes: insights from the SUSTAIN 1–7 trials. Diabetes Metab. 2019;45(5):409–418. doi:10.1016/j.diabet.2018.12.001
13. Husain M, Bain SC, Jeppesen OK, et al. Semaglutide (SUSTAIN and PIONEER) reduces cardiovascular events in type 2 diabetes across varying cardiovascular risk. Diabetes Obes Metab. 2020;22(3):442–451. doi:10.1111/dom.13955
14. Pratley RE, Aroda VR, Lingvay I, et al.; SUSTAIN 7 investigators. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275–286. doi:10.1016/S2213-8587(18)30024-X
15. Frías JP, Auerbach P, Bajaj HS, et al. Efficacy and safety of once-weekly semaglutide 2·0 mg versus 1·0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double-blind, randomised, phase 3B trial. Lancet Diabetes Endocrinol. 2021;9(9):563–574. doi:10.1016/S2213-8587(21)00174-1
16. Marzullo P, Daffara T, Mele C, et al. Real-world evaluation of weekly subcutaneous treatment with semaglutide in a cohort of Italian diabetic patients. J Endocrinol Invest. 2022;45(8):1587–1598. doi:10.1007/s40618-022-01799-2
17. Wilding JPH, Batterham RL, Calanna S, et al.; STEP 1 Study Group. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183
18. Rubino D, Abrahamsson N, Davies M, et al.; STEP 4 Investigators. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414–1425. doi:10.1001/jama.2021.3224
19. Hjerpsted JB, Flint A, Brooks A, Axelsen MB, Kvist T, Blundell J. Semaglutide improves postprandial glucose and lipid metabolism, and delays first-hour gastric emptying in subjects with obesity. Diabetes Obes Metab. 2018;20(3):610–619. doi:10.1111/dom.13120
20. Verma S, McGuire DK, Bain SC, et al. Effects of glucagon-like peptide-1 receptor agonists liraglutide and semaglutide on cardiovascular and renal outcomes across body mass index categories in type 2 diabetes: results of the LEADER and SUSTAIN 6 trials. Diabetes Obes Metab. 2020;22(12):2487–2492. doi:10.1111/dom.14160
21. Kristensen SL, Rørth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019;7(10):776–785. doi:10.1016/S2213-8587(19)30249-9
22. Peter R, Bain SC. Safety of injectable semaglutide for type 2 diabetes. Expert Opin Drug Saf. 2020;19(7):785–798. doi:10.1080/14740338.2020.1772230
23. Andreadis P, Karagiannis T, Malandris K, et al. Semaglutide for type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Obes Metab. 2018;20(9):2255–2263. doi:10.1111/dom.13361
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.