")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Salivary Oxidative Stress and Antioxidant Capacity in Smokeless Tobacco (Naswar) Users
Authors Ahmad I, Binmadi N, Afridi SG, Aljohani S, Shah I, Saidal A , Shahzad M
Received 4 April 2023
Accepted for publication 29 June 2023
Published 12 July 2023 Volume 2023:15 Pages 121—132
DOI https://doi.org/10.2147/CCIDE.S415827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Iftikhar Ahmad,1 Nada Binmadi,2 Sahib Gul Afridi,1 Suad Aljohani,2 Inayat Shah,3 Ahsan Saidal,4 Muhammad Shahzad3,5
1Department of Biochemistry, Abdul Wali Khan University Mardan, Mardan, Khyber Pakhtunkhwa, 23200, Pakistan; 2Department of Oral Diagnostic Sciences, King Abdulaziz University Faculty of Dentistry, Jeddah, Saudi Arabia; 3Institute of Basic Medical Sciences, Khyber Medical University, Peshawar, 25110, Pakistan; 4Institute of Paramedical Sciences, Khyber Medical University, Peshawar, 24350, Pakistan; 5School of Biological Sciences, Health and Life Sciences Building, University of Reading, Reading, RG6 6AX, UK
Correspondence: Muhammad Shahzad, Institute of Basic Medical Sciences, Khyber Medical University, Hayat Abad Phase 5, Peshawar, 25100, Pakistan, Tel +92 91 9217703, Fax +92 91 9217704, Email [email protected]
Background: Naswar, a smokeless tobacco product, commonly consumed in Pakistan, is associated with a 10-fold increase in the risk of oral cancer. However, little is known about Naswar’s underlying toxicity mechanisms.
Objective: The current study aimed to investigate the effects of Naswar use on oral health and salivary parameters.
Methods: A case-control study was conducted among Naswar users (n=42) and age-matched healthy controls (n=42) in Pakistan in 2019. Participant data were collected using questionnaires. Decayed, missing, and filled teeth (DMFT) scores were computed during clinical examinations. Unstimulated whole saliva was collected to assess salivary flow rate, pH, and salivary total oxidative stress (TOS)/total antioxidant capacity (TAC) using commercially available kits. Participants’ oral health parameters were compared between cases and controls using ANOVA.
Results: No significant differences were observed between the two groups in terms of age, oral health, and hygiene practices and mean DMFT score. Mean salivary pH and the salivary flow rate was significantly (p< 0.001) higher in Naswar users (7.7 and 0.71 mL/minute, respectively) than in non-users (6.95 and 0.52 mL/minute, respectively). Although TOS and TAC were not significantly different between the groups, Naswar users generally had a higher TOS (51.6± 42 μmol/L) and lower TAC (0.55± 0.18 mmol/L) than non-users (TOS 45.5± 38.2 μmol/L and TAC 0.57± 0.17 mmol/L). Correlational analysis also revealed a significant positive correlation between DMFT score and Naswar use duration (r=0.796, p< 0.001) and the number of dips/units consumed each day (r=0.515; p< 0.001).
Conclusion: Habitual Naswar use is associated with increased salivary flow rate, pH, and TOS, and reduced TAC levels in Pakistani adults compared to non-users. The pro-oxidant changes may contribute toward deleterious effects of Naswar use including oral cancer.
Keywords: salivary flow rate, salivary pH, oxidative stress, antioxidant capacity, oral health
Introduction
Consumption of smokeless tobacco (ST), a type of tobacco product that is used without burning or combustion, is a global public health issue. According to recent estimates, ST products are used by more than 300 million people across the globe,1 the majority of which reside in South East Asian countries. In these countries, ST use is gradually on the rise2 primarily due to a lack of ST-specific tobacco control laws and legislation, insufficient scientific evidence on toxicity, and a general public belief that ST is a safer product.3
ST users are generally at a high risk of developing ST-related diseases such as cancer and ischemic heart diseases.4 In Pakistan, approximately 8% of the population consume at least one ST product, with the commonest being Naswar, paan, and gutka.5 Naswar is the most popular ST product used by the ethnic “Pashtun” population native to the Northwest areas of Pakistan (Khyber Pakhtunkhwa) and Afghanistan.6 In Peshawar city (the capital of Khyber Pakhtunkhwa province of Pakistan) and its peripheries, more than 60% of the tobacco consumed is in the form of Naswar.7 Naswar is usually a mixture of sundried tobacco leaves, slaked-lime, wood ash, flavorings (cardamom, menthol), and sometimes coloring agents (indigo).8 In Pakistan, the product is prepared in the local cottage industries and sold in polythene bags without any safety warning. It is used in the form of a small pellet placed in the buccal vestibule usually between the mandibular premolars and first molar teeth. The users gently suck the Naswar pellet intermittently for extended periods of time and spit out when desired.9
Naswar use, just like other ST products, is a common risk factor for oral cancer, the second most common type of cancer in Pakistan.10 A recent meta-analysis by Khan et al (2019) found that Naswar users have a ten-fold risk of developing oral cancer when compared to Naswar non-users.11 The risk has generally been attributed to the presence of a large number of toxic substances present in Naswar including nicotine, heavy metals such as arsenic, beryllium, cadmium, chromium, cobalt, lead, and nickel, and tobacco-specific nitrosamines (TSNAs).12 It is believed that habitual tobacco use (both smoking and smokeless tobacco) enhances free radical (reactive oxygen species) generation in the human body,13,14 leading to oxidative stress when the balance between reactive oxygen species (ROS) concentration and the body’s antioxidant defense mechanism is lost. Oxidative stress has been implicated as an important biological mechanism in carcinogenesis due to the direct damaging effect of reactive oxygen species on cellular DNA.15,16 The body’s antioxidant defense mechanism is vital in counteracting the damaging effects of oxidative stress, especially in tobacco users.17 However, active smokers and ST users have lower levels of protective antioxidants (superoxide dismutase, glutathione peroxidase, and catalase) compared to the general population and thus are at an increased risk of carcinogenesis.18,19 There is mounting research evidence suggesting tobacco use as a risk factor for enhanced oxidative stress and related complications in humans. For example, increased oxidative stress in Naswar users damages macromolecules such as DNA in the oral mucosa resulting in oral pre-malignant and malignant transformation.20,21 Thus, the high prevalence of oral cancer in Naswar users could be attributed to the oral mucosa being the first and most directly exposed site to the toxic effects of ST.11
The absorption of nicotine and other toxic constituents found systemically among ST users primarily occurs through the mucous membranes in the oral cavity.22 Therefore, the oral mucosa of ST users is under constant stress due to oxidative stress triggered by the toxic constituents. Indeed, the first exposed site for the constituents and emissions of tobacco in tobacco users is the oral cavity. Consequently, it is the most vulnerable site for clinical, immunologic, carcinogenic, and microbial effects of ST use.22 The oral mucosa can therefore be used as a site to evaluate the deleterious effects of nicotine and other toxic constituents present in ST. However, to the best of our knowledge, the impact of habitual Naswar use on oxidative stress and total antioxidant capacity of saliva is unknown. Therefore, the current study aimed to quantify the impact of habitual Naswar use on markers of salivary oxidative stress and antioxidant capacity in adult, healthy volunteers.
Methodology
Study Design and Setting
This case control study was conducted at the Medical Teaching Institute Hayat Medical Complex (MTI–HMC) Peshawar from February 2019 to July 2019. MTI–HMC is the second largest tertiary care teaching hospital of Peshawar, the capital city of Khyber Pakhtunkhwa province of Pakistan. In 2022, the hospital provided healthcare services to approximately 1.5 million patients including 30,000 Afghan refugees in 32 different specialties including oral and dental care.23
Study Population
Study participants were 84 male adults, aged 18 years and above and divided into two groups (cases and controls). Cases (n=42) were exclusive Naswar users who had used Naswar at least once each day in the 12 months preceding the interview date and had no apparent oral or systemic disease. Controls (n=42) were age- (±18 years) and ethnicity-matched healthy volunteers (n=42) who lived in the same area as cases and had never used any tobacco product in their entire life. Past smokers, those who were using other types of tobacco products, or those who were on antibiotics or prescription mouthwash at the time of the interview, or in the one month preceding the interview date, were ineligible to participate.
Participant Recruitment and Data Collection
Participants were identified by word of mouth and poster displays in areas surrounding the study site. Participant information sheets containing all the details about the study in the local language (Pashto) and the national language (Urdu) were provided to all the participants. The study procedures were also verbally explained to participants, and participants’ queries, if any, were answered by the researcher. Upon completion of the information session, consenting participants were asked to sign a written informed consent document which preceded data collection. An interviewer-administered structured questionnaire consisting of 32 open-ended and closed questions, developed in consultation with expert dental and public health professionals (n=4) and pre-tested on eight volunteers who did not take part in the study, was used for data collection. The questionnaire had four sections: section A included demographic information such as age, gender, ethnicity, etc.; section B collected information on socioeconomic status; and sections C and D had questions about participants’ Naswar intake and oral health and hygiene. Once the data were collected, the participants were instructed to schedule an appointment for free dental checkup with a dentist at a convenient date but preferably within one month of recruitment into the study.
Clinical Oral Examination
All participants underwent clinical oral examination in a well-equipped dental facility at MTI–HMC. The participants were first reclined comfortably in supine position on a dental chair. Clinical oral examination was carried out by a single, experienced dentist who did not know whether the participant was in case or control group. A separate set of disposable dental mirror and probe was used for each participant to limit the risk of cross-infection. The decayed, missing, filled teeth (DMFT) score was used to assess oral health status and document the presence of dental caries (enamel or dentine), missing teeth, and restorations24 on a data collection sheet. The DMFT score is the sum of the number of decayed, missing due to caries, and filled teeth in the permanent dentition.
Saliva Sample Collection and Onsite Analysis for pH and Flow Rate
Unstimulated, whole saliva samples were collected from all the participants following a standard procedure.25 Briefly, the participants were instructed not to brush their teeth on the day of sample collection. They were also advised to refrain from eating or drinking any fluid except water at least one hour before saliva collection to avoid dilution and contamination of saliva with food debris. Ten minutes before sample collection, the participants were asked to rinse the mouth thoroughly using distilled water to remove any food debris. Each participant was asked to tilt his head and slightly open his mouth to allow the saliva drool onto the floor of the mouth over a period of five minutes. The participant would then be asked to spit the collected saliva into a sterile tube (15 mL). Efforts were made to collect at least 5 mL of saliva sample from each participant. The salivary flow rate was calculated by dividing the volume collected by duration of collection and computed as mL/minute. Onsite analysis of pH was done using digital pH meter (InoLab WTW 7110). The samples were than aliquoted and stored at −80°C for further analyses.
Measurement of Total Oxidant Status and Antioxidant Capacity
The total oxidant status (TOS) and total antioxidant capacity (TAC) of the stored salivary samples for both the Naswar users and the control subjects were assessed using commercially available kits (Rel Assay Diagnostics, Turkey) following manufacturer instructions.
Statistical Analysis
Data were coded and analyzed using the Statistical Package for Social Science (SPSS, Windows version 24). The normality of the data was examined using Kolmogorov–Smirnov test and the Shapiro–Wilk test. Continuous variables were reported as mean and standard deviation (SD). Categorical data were reported as frequency and percentage. Comparisons between continuous variables were conducted using the independent t-test, and chi-square and Fisher exact tests were used to evaluate the difference between Naswar users and non-users in terms of categorical variables. An ANOVA was conducted to examine the effect of participant demographic and oral health characteristics on various oral health outcomes in parametric data. The Mann–Whitney test and Kruskal–Wallis test were used to assess the effect of participant characteristics on oral health outcomes in non-parametric data. A p-value of <0.05 was considered statistically significant.
Ethical Considerations
Ethical approval was granted by Ethics Board of the Khyber Medical University (DIR/KMU-EB/PR/00532).
Results
Demographic Characteristics and Oral Health and Hygiene Habits of Naswar Users and Non-Users
A total of 42 Naswar users and 42 non-tobacco users as healthy controls were enrolled. The mean age of all the participants was 29.64±9.98 years, the majority were of high school or college level education (52%), were employed (49%), lived in their own homes (76%) with more than 10 household members (62%). There was a significantly lower proportion of employed persons among Naswar users when compared to the the non-users (46% vs 52%; p=0.0031). Naswar users and non-users did not differ by age, education level, type of dwelling, duration lived at current residence, or number of household members.
Among all participants, the majority brushed their teeth twice a day (60%), in the morning and at bedtime (60%), using a toothbrush and toothpaste (56%). A minority complained of bleeding gums during brushing (30%) and teeth mobility (19%). Most participants (77%) only visited the dentist as needed. A lower proportion of Naswar users used toothbrushes and toothpaste to clean their teeth when compared to non-users (36% vs 76%; p=0.0009). Naswar users and non-users did not differ by other oral health habits (Table 1).
 |
Table 1 Characteristics and Oral Health Habits of Participants Who Were Enrolled in the Case Control Study to Compare Naswar Users to Non-users, Pakistan |
Laboratory and Clinical Outcomes
Clinical oral health status as assessed by DMFT score as well as lab-based salivary parameters were further compared between the two groups. Using independent samples t-test, we found elevated salivary pH (7.7) and flow rate (0.71 mL/minute) in Naswar user group compared to the non-user group (6.95 and 0.52 mL/minute, respectively), and the differences were statistically significant (p<0.001) (Figure 1A and B). In terms of clinical oral health status as assessed by DMFT score, no significant differences were found between the two groups (Figure 1C). Similary, Naswar users generally had a higher TOS (51.6±42 µmol/L) and lower TAC (0.55±0.18 mmol/L) than non-users (TOS 45.5±38.2 µmol/L and TAC 0.57±0.17 mmol/L) (Figure 1D and E), although there was no statistically significant difference.
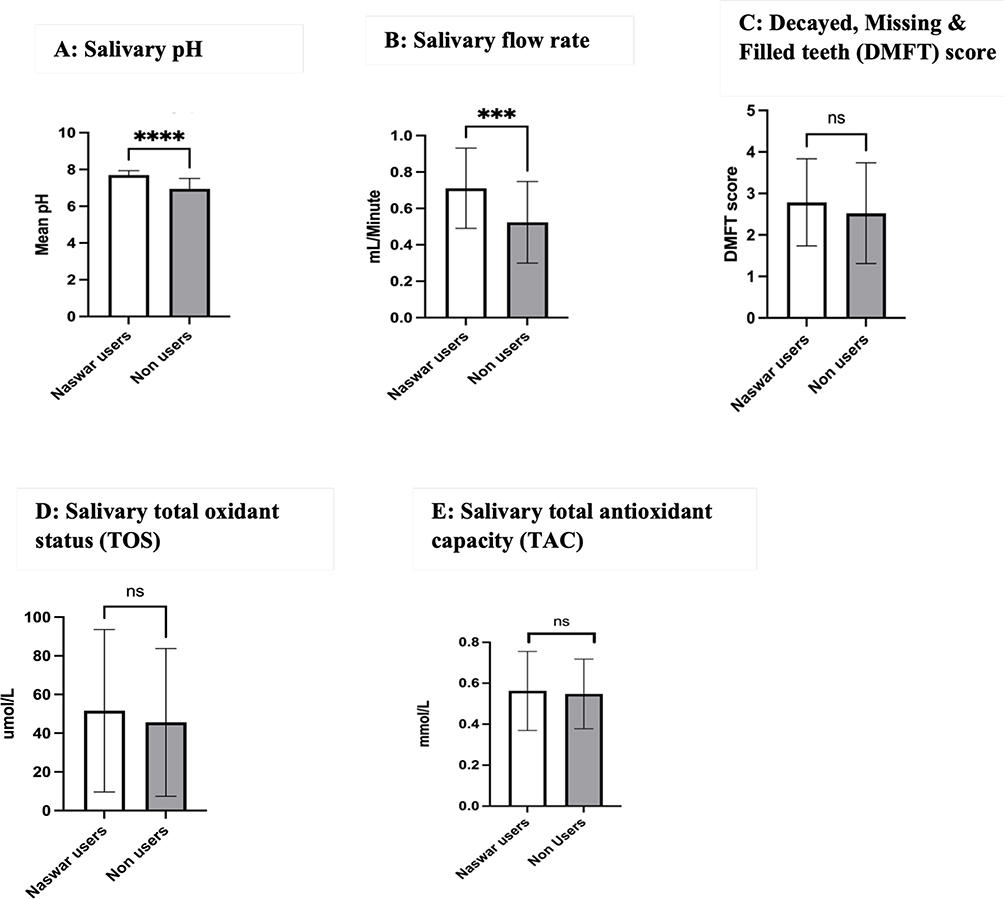 |
Figure 1 (A-E)Laboratory and clinical oral health status of the participants. (A) Salivary pH; (B) Sa livary flow rate; (C) Decayed, Missing and Filled teeth (DMFT) score; (D) Salivary total oxidant status (TOS); (E) Salivary total antioxidant capacity (TAC). Independent sample t-test was used. ****p<0.0001, ***p<0.001. Abbreviation: ns, non-significant. |
Naswar Use Characteristics and Oral Health Outcomes
Among Naswar users, the most common type used was the green moist type (62%), of the Bara brand (50%), which was placed in the lower right quadrant of the mouth (33%). Users dipped between 1 to 10 dips a day (45%) for a duration of 1 to 5 minutes (50%) and spat out the saliva (93%) (Table 2).
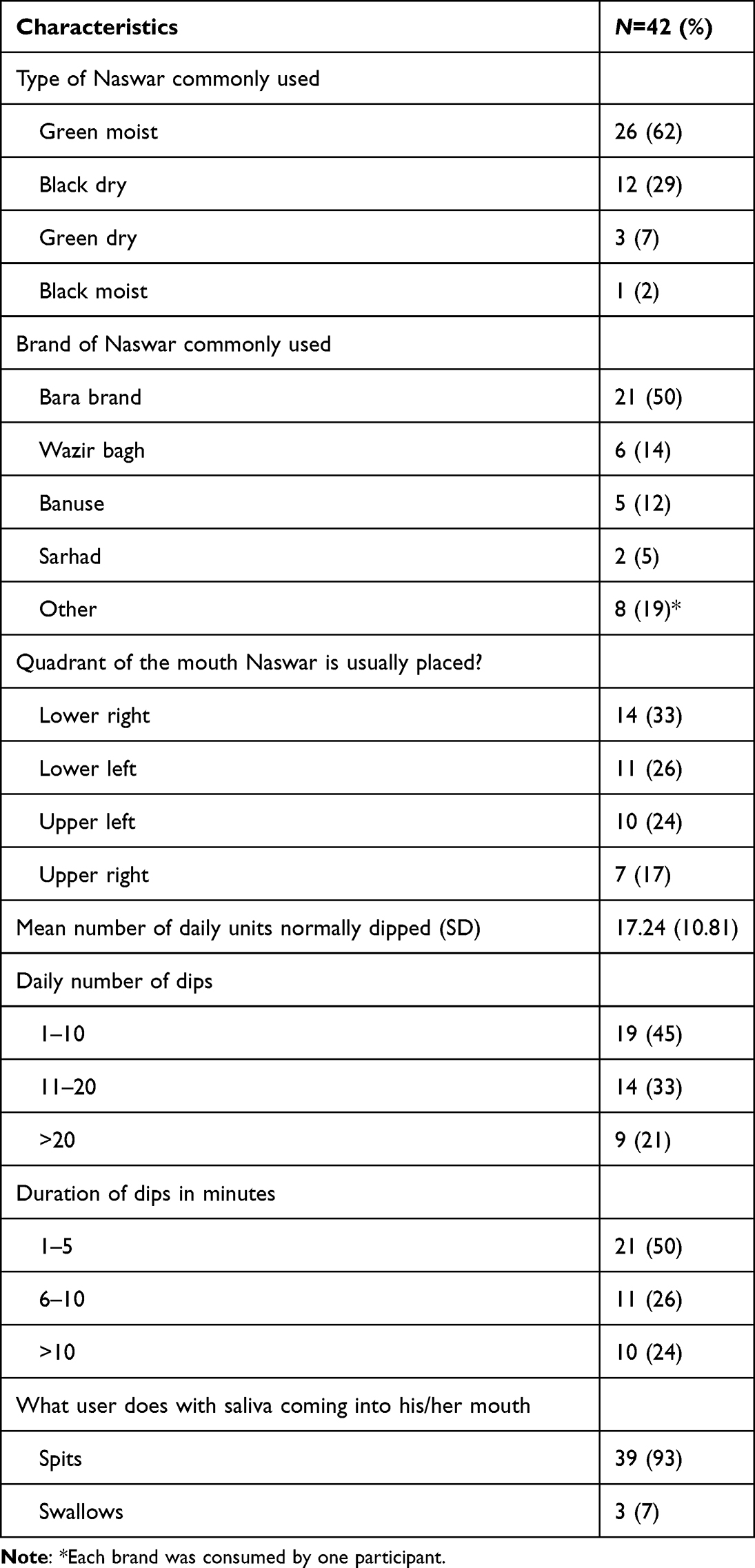 |
Table 2 Characteristics of Naswar Use by Cases, Pakistan |
Individuals who use 1–10 units of Naswar per day had significantly lower DMFT scores compared to those who used 11–20 or >20 units daily (p=0.005). Regarding the type of Naswar, individuals who consumed green moist Naswar had significantly higher DMFT scores than those who consumed other types (p=0.005). On the other hand, there was no significant association between the number of daily units and the salivary pH (p=0.545), salivary flow rate (p=0.491), total oxidant status (p=0.089), and total antioxidant capacity (p=0.403). Likewise, there was no association between duration of Naswar consumption or behaviors towards saliva after using Naswar and oral health outcomes (Table 3).
 |
Table 3 Association Between Oral Health Scores and Characteristics of Naswar Use for Cases, Pakistan |
Discussion
We set out to quantify the impact of habitual Naswar use on markers of oxidative stress and antioxidant status in adult healthy volunteers. There were more daily-wage workers among Naswar users. Naswar users mainly used 1 to 10 daily dips of the green moist type of Naswar of the Bara brand, which they spat out after chewing it. The DMFT scores, salivary pH, flow rate, TOS, and TAC were higher in the Naswar group than in the non-user group. Naswar users who consumed the green moist type had the highest DFMT scores when compared to users of other brands. Likewise, those who used a higher number of Naswar units per day also had higher DFMT scores.
The proportion of DFMT is known to increase with age.15,26,27 Tobacco products are also known to have an impact on dental health.28 Naswar use thus may have an impact on DFMT scores only at an advanced age; this impact could be related to duration of Naswar use since onset and is related to the quantity of Naswar use29 and type of Naswar use. However, in this study the Naswar users were young adults aged 18–34 years (64%). Moisture is known to increase the constituents of ST products.30 The impact of Naswar use on DFMT may be limited by the number of dental visits made by a Naswar user. The predominance of daily wage workers among Naswar users and a limited number of students among the Naswar users could be related to their education level. Naswar users were mainly those of lower educational level who could spend close to USD 1.00 a day on ST products.5
An important finding of the present study was that habitual Naswar use results in a significant increase in the salivary flow rate and pH. These findings contrast with the previously published studies among other types of smokeless tobacco users. For example, decreased salivary flow rate has been reported in smokeless tobacco users from Iran,31 Saudi Arabia,32 and India.33 Similarly, these studies have also reported decreased salivary pH in smokeless tobacco users compared to non-users. These differences in oral parameters between Naswar and other types of smokeless tobacco products may be due to differences in chemical composition of these products. Naswar, in addition to ground tobacco, also contains ash and slaked lime which greatly increases the pH of the oral cavity. The increased pH may also enhance nicotine absorption through the mucous membrane of the mouth.11 The increased salivary flow rate in Naswar users may also have a diluting effect and reduce the activity of salivary proteins and antioxidant enzymes as reported elsewhere.34
Excessive generation of free radicals and the resultant oxidative stress condition are commonly implicated as an important molecular mechanism underlying different diseases in humans including those commonly reported in ST users.13 The presence and detection of different oxidative stress markers in saliva are increasingly being discussed as an innovative, non-invasive, and advanced method in the risk assessment, diagnosis, and prognosis of different oral and systemic conditions. However, due to the extremely short half-life of the free radicals, measurement of oxidation products is most commonly used as an indicator of oxidative stress.35 Previously, research studies have shown that tobacco users have high levels of lipid peroxidation, protein oxidation, and DNA damage markers9,13 compared to non-users. However, among ST users, a test measuring salivary TOS36 and TAC is more appropriate and context-specific since saliva is the first component of the human body that comes in contact with ST during use.
The salivary TOS and TAC of Naswar users were higher than those of non-users, although these differences were not significant. Tobacco use is an important risk factor for enhanced oxidative stress and related complications in humans. Increased oxidative stress in Naswar users may damage macromolecules such as DNA in the oral mucosa, resulting in oral pre-malignant and malignant transformation.20,21 This hypothesis is reinforced by several in-vitro studies reporting genotoxic and DNA-damaging effects of different smokeless tobacco products that is mediated through production of reactive oxygen species.37 In fact, epidemiological studies have revealed higher odds of oral and upper aerodigestive tract cancers in tobacco users than in non-users.38 In the literature, TAC is reduced among smokers.39 However, we observed an increase in TAC. The increase in antioxidative capacity is an indicator of improved internal oxidative status and could also be an adaptation to increased oxidative states at an early age.40 Total antioxidant status is increased in states of oxidative stress.41
Since we did not collect Naswar use duration, it is challenging to link the changes in TAC to duration of Naswar use. The relationship between tobacco use and TAC is controversial, and this may be attributed to varied methods for antioxidant measurement, and genetic and ethnicity diversities. A study among male smokers in Iran showed an insignificant weak positive correlation between smoking duration and TAC,39 a relationship we could possibly liken to the observed insignificant increase in TAC levels with Naswar quantity. Total antioxidative capacity reduces as a function of human age.42 However, in the absence of a wide range of age groups in our study, we were unable to systematically assess for this relationship.
Although this is the first study of its kind assessing impact of Naswar use on oral health parameters, our study had some limitations. The current study, instead of comprehensive oral health assessments, employed only the DMFT index to assess the impact of Naswar use on oral health status. ST use including Naswar is a common risk factor for a number of other oral health diseases and conditions, including poor periodontal health and oral lesions, and a comprehensive oral health assessment would have been an advantage. Due to cultural constraints, our study was only limited to male participants; therefore, inferences cannot be made about gender-specific variations of the effects of ST on oral health parameters. Nevertheless, we were able to provide information that could be used to manage the largest proportion of ST users that are primarily males.36 Furthermore, the accuracy of our responses maybe limited by recall bias. Nevertheless, we limited our recruitment to recent ST use and used oral health assessment measures that could cater for the short-half lives of the tested parameters. Additionally, we relied on snowball sampling and word of mouth recruitment; it is possible that our participant selection may be biased. However, the study site has a large catchment area and is visited by a representative Pakistani population.
Conclusion
The changes in oral health parameters among Pakistani ST users could be associated with the increased cancer risk among this population. Although these markers could potentially serve as biomarkers for oxidative stress among ST users, our results were both congruent and incongruent with published literature, an observation that could be attributed to genetic and ethnic diversity, education level, chemical components within ST, oral health habits, assessment methods, or other factors. Further research should investigate the influence of other factors on oral health outcomes among ST users in diverse contexts, taking into consideration the chemical constituents of different ST products and assessment methods for oral health outcomes, with a view to recommend screening methods for potential cancer risk in this population.
Ethical Approval
The procedures were conducted according to the principles outlined in the Declaration of Helsinki and Ethical Conduct for Research with Human Beings and the Good Clinical Practice Guidelines. Ethical approval was granted by the Ethics Board of the Khyber Medical University (DIR/KMU-EB/PR/00532).
Consent to Participate
Informed consent was taken from all participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no fund from any institution or company.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hatsukami D, Zeller M, Gupta P, Parascandola M, Asma S. Smokeless Tobacco and Public Health: A Global Perspective. NIH Publication; 2014:14–7983.
2. Suliankatchi RA, Sinha DN, Rath R, et al. Smokeless tobacco use is “Replacing” the smoking epidemic in the South-East Asia Region. Nicotine Tob Res. 2019;21(1):95–100. doi:10.1093/ntr/ntx272
3. Wackowski OA, Lewis MJ, Delnevo CD, Ling PM. Smokeless tobacco risk comparison and other debate messages in the news. Health Behav Policy Rev. 2014;1(3):183–190. doi:10.14485/hbpr.1.3.2
4. Siddiqi K, Husain S, Vidyasagaran A, Readshaw A, Mishu MP, Sheikh A. Global burden of disease due to smokeless tobacco consumption in adults: an updated analysis of data from 127 countries. BMC Med. 2020;18(1):222. doi:10.1186/s12916-020-01677-9
5. Naz S, Naz S, Nadeem Saqib MA, Bashir F, Rafique I. Prevalence of smokeless tobacco use in Pakistan: insight from the Global Adult Tobacco Survey Pakistan (GATS Pakistan-2014). J Pak Med Assoc. 2018;68(Suppl 2):S7–S12.
6. Ahmad F, Khan Z, Siddiqi K, et al. Compliance of Oral Snuff (Naswar) packaging and sales practices with national tobacco control laws and the relevant articles of framework convention on tobacco control in Khyber Pakhtunkhwa Pakistan. Nicotine Tob Res. 2020;22(12):2224–2230. doi:10.1093/ntr/ntaa144
7. Ali S, Wazir MARK, Qadir S. Naswar; What do (A form of smokeless tobacco) users know about its harmful effects? Prof Med J. 2017;24(3):386–391. doi:10.17957/TPMJ/17.3683
8. Zakiullah SM, Muhammad N, Muhammad N, et al. Assessment of potential toxicity of a smokeless tobacco product (naswar) available on the Pakistani market. Tob Control. 2012;21(4):396–401. doi:10.1136/tc.2010.042630
9. Sajid F, Bano S. Effects of smokeless dipping tobacco (Naswar) consumption on antioxidant enzymes and lipid profile in its users. Pak J Pharm Sci. 2015;28(5 Suppl):1829–1833.
10. International Agency for Research on cancer global cancer observatory. Available from: https://gco.iarc.fr/.
11. Khan Z, Suliankatchi RA, Heise TL, Dreger S. Naswar (Smokeless Tobacco) use and the risk of oral cancer in Pakistan: a systematic review with meta-analysis. Nicotine Tob Res. 2019;21(1):32–40. doi:10.1093/ntr/ntx281
12. Abbasi ZA, Hadi NI, Zubairi AM, Hosein M. Salivary Interleukin 1-beta levels and clinical periodontal parameters in habitual naswar users and non-users. Pak J Med Sci. 2019;35(3):674–679. doi:10.12669/pjms.35.3.10
13. Caliri AW, Tommasi S, Besaratinia A. Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer. Mutat Res Rev Mutat Res. 2021;787:108365. doi:10.1016/j.mrrev.2021.108365
14. Li L, Zhou X, Wang Y. Smokeless tobacco extract inhibits proliferation and promotes apoptosis in oral mucous fibroblasts. Oncol Lett. 2018;16(4):5066–5074. doi:10.3892/ol.2018.9252
15. Naga Sirisha CV, Manohar RM. Study of antioxidant enzymes superoxide dismutase and glutathione peroxidase levels in tobacco chewers and smokers: a pilot study. J Cancer Res Ther. 2013;9(2):210–214. doi:10.4103/0973-1482.113352
16. Patel BP, Rawal UM, Shah PM, et al. Study of tobacco habits and alterations in enzymatic antioxidant system in oral cancer. Oncology. 2005;68(4–6):511–519. doi:10.1159/000086995
17. Sugiura T, Dohi Y, Takase H, Yamashita S, Fujii S, Ohte N. Oxidative stress is closely associated with increased arterial stiffness, especially in aged male smokers without previous cardiovascular events: a cross-sectional study. J Atheroscler Thromb. 2017;24(11):1186–1198. doi:10.5551/jat.39289
18. Block G, Dietrich M, Norkus EP, et al. Factors associated with oxidative stress in human populations. Am J Epidemiol. 2002;156(3):274–285. doi:10.1093/aje/kwf029
19. Ermis B, Ors R, Yildirim A, Tastekin A, Kardas F, Akcay F. Influence of smoking on maternal and neonatal serum malondialdehyde, superoxide dismutase, and glutathione peroxidase levels. Ann Clin Lab Sci. 2004;34(4):405–409.
20. Arbabi-Kalati F, Salimi S, Nabavi S, Rigi S, Miri-Moghaddam M. Effects of tobacco on salivary antioxidative and immunologic systems. Asian Pac J Cancer Prev. 2017;18(5):1215–1218. doi:10.22034/apjcp.2017.18.5.1215
21. Begum SF, Nagajothi G, Latha KS, et al. Possible role of nicotine and cotinine on nitroxidative stress and antioxidant content in saliva of smokeless tobacco consumers. Pract Lab Med. 2018;12:e00105. doi:10.1016/j.plabm.2018.e00105
22. Tomar SL, Hecht SS, Jaspers I, Gregory RL, Stepanov I. Oral health effects of combusted and smokeless tobacco products. Adv Dent Res. 2019;30(1):4–10. doi:10.1177/0022034519872480
23. Qayyum MA, Farooq Z, Yaseen M, et al. Statistical assessment of toxic and essential metals in the serum of female patients with lung carcinoma from Pakistan. Biol Trace Elem Res. 2020;197(2):367–383. doi:10.1007/s12011-019-01998-8
24. Amin MN, Siddiqui SA, Ibrahim M, et al. Inflammatory cytokines in the pathogenesis of cardiovascular disease and cancer. SAGE Open Med. 2020;8:2050312120965752. doi:10.1177/2050312120965752
25. Mathis C, Smart DJ, Xia W, et al. Chapter 20 - residual risk of nicotine. In: Peitsch MC, Hoeng J, editors. Toxicological Evaluation of Electronic Nicotine Delivery Products. Academic Press; 2021:513–587.
26. National Institute of Dental and Craniofacial Research Dental caries (Tooth decay) in adults (Ages 20 to 64 years). Available from: https://www.nidcr.nih.gov/research/data-statistics/dental-caries/adults.
27. National Institute of Dental and Craniofacial Research Dental caries (Tooth decay) in seniors (Ages 65 and older). Available from: https://www.nidcr.nih.gov/research/data-statistics/dental-caries/seniors.
28. Sham AS, Cheung LK, Jin LJ, Corbet EF. The effects of tobacco use on oral health. Hong Kong Med J. 2003;9(4):271–277.
29. Rahim A, Syed K, Ahad B, Farooq A, Ayub Z, Batool SM. Comparison of severity of periodontal clinical parameters among naswar/snuff users: cross sectional study. PLoS One. 2022;17(9):e0273288. doi:10.1371/journal.pone.0273288
30. Edwards SH, Hassink MD, Taylor KM, Vu AT. Quantitative measurement of harmful and potentially harmful constituents, pH, and moisture content in 16 commercial smokeless tobacco products. Regul Toxicol Pharmacol. 2022;133:105199. doi:10.1016/j.yrtph.2022.105199
31. Moradi G, Mohamadi Bolbanabad A, Moinafshar A, Adabi H, Sharafi M, Zareie B. Evaluation of oral health status based on the Decayed, Missing and Filled Teeth (DMFT) Index. Iran J Public Health. 2019;48(11):2050–2057. doi:10.17485/ijst/2016/v9i41/103895
32. Navazesh M, Kumar SK. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc. 2008;139:35s–40s. doi:10.14219/jada.archive.2008.0353
33. Akram Z, Abduljabbar T, Hosain M, et al. Comparison of periodontal inflammatory parameters among habitual gutka-chewers and naswar-dippers: a split-mouth retrospective clinical study. Acta Odontol Scand. 2018;76(2):141–147. doi:10.1080/00016357.2017.1394489
34. Javed F, Al-Kheraif AA, Al Amri MD, et al. Periodontal parameters and whole salivary cytokine profiles among habitual gutka chewers and non-chewers. J Periodontol. 2015;86(5):689–695. doi:10.1902/jop.2015.140556
35. Eskander SB, Saleh HM. Heavy metal-induced oxidative stress and related cellular process. In: Faisal M, Saquib Q, Alatar AA, Al-Khedhairy AA, editors. Cellular and Molecular Phytotoxicity of Heavy Metals. Cham: Springer International Publishing; 2020:99–123.
36. Colilla SA. An epidemiologic review of smokeless tobacco health effects and harm reduction potential. Regul Toxicol Pharmacol. 2010;56(2):197–211. doi:10.1016/j.yrtph.2009.09.017
37. Al-Ak’hali MS, Halboub ES, Mujam OH, Alahmar NM, Jerah SA, Mutawwam FA. Salivary parameters among Arabian snuff (Shammah) users. Saudi Med J. 2017;38(12):1201–1206. doi:10.15537/smj.2017.12.20973
38. Kanwar A, Sah K, Grover N, Chandra S, Singh R. Long term effect of tobacco on resting whole mouth salivary flow rate and pH: an institutional based comparative study. Eur J Gen Dent. 2013;2(03):296–299. doi:10.4103/2278-9626.116017
39. Ghazi A, Pakfetrat A, Hashemy SI, Boroomand F, Javan-Rashid A. Evaluation of antioxidant capacity and cotinine levels of saliva in male smokers and non-smokers. Addict Health. 2020;12(4):244–250. doi:10.22122/ahj.v12i4.278
40. Christou K, Gourgoulianis KI. Reactive oxygen metabolites (ROMs) as an index of oxidative stress in obstructive sleep apnea patients. In: Qureshi GA, Parvez SH, editors. Oxidative Stress and Neurodegenerative Disorders. Amsterdam: Elsevier Science B.V; 2007:247–265.
41. Tóthová L, Kamodyová N, Červenka T, Celec P. Salivary markers of oxidative stress in oral diseases. Front Cell Infect Microbiol. 2015;5:73. doi:10.3389/fcimb.2015.00073
42. Maurya PK. Animal biotechnology as a tool to understand and fight aging. In: Verma AS, Singh A, editors. Animal Biotechnology. San Diego: Academic Press; 2017:177–191.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.