")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Role of Diabetes Mellitus in Acute Coronary Syndrome Patients with Heart Failure and Midrange Ejection Fraction Who Have Undergone Percutaneous Coronary Intervention: A 3-Year Case-Series Follow-Up Retrospective Study
Authors Li L, Li G, Chen H, Feng Z, Zhang L, Chen L, Fan L
Received 26 September 2021
Accepted for publication 4 November 2021
Published 29 December 2021 Volume 2021:14 Pages 4931—4944
DOI https://doi.org/10.2147/DMSO.S339209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Lieyou Li,1,* Ganyang Li,2,* Huang Chen,1 Zhihai Feng,1 Lin Zhang,1 Lianglong Chen,1 Lin Fan1
1Department of Cardiology, Fujian Medical University Union Hospital Institute of Coronary Heart Disease, Fuzhou, Fujian, People’s Republic of China; 2Department of Cardiology, Longyan First Hospital Affiliated with Fujian Medical University, Longyan, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Fan Tel +86 591 8335-7896
Fax +86 591 83308713
Email [email protected]
Background: Data are limited on the effect of diabetes mellitus (DM) on the prognosis of acute coronary syndrome (ACS) patients with heart failure with midrange ejection fraction (HFmrEF) who have undergone percutaneous coronary intervention (PCI). This study aimed to investigate the relationship between type 2 DM (T2DM) and 3-year outcomes in such a population.
Methods: A total of 377 ACS patients with HFmrEF (left ventricular EF 40%– 49%) who had undergone PCI (132 diabetic and 245 nondiabetic patients) were included in the analysis. The primary outcome was a composite end point of all-cause death or HF rehospitalization. Cox proportional-hazard regression analysis and Kaplan–Meier tests were used to assess the effect of DM on the primary outcome. Sensitivity analysis was conducted with propensity score–matching analysis.
Results: During a follow-up of 3 years, diabetic patients had higher incidence of the primary outcome than nondiabetic patients (96.1 vs 44.6 per 1,000 patient-years, incidence ratio 2.301, 95% CI 1.334– 3.969; P=0.002). Multivariate analysis showed that DM was associated with a significant increase in the composite outcome of all-cause death or HF rehospitalization (adjusted HR 2.080, 95% CI 1.115– 3.878; P=0.021). Sensitivity analysis further confirmed that DM was an independent prognostic factor of long-term adverse outcomes for ACS patients with HFmrEF who had undergone PCI (adjusted HR 3.792, 95% CI 1.802– 7.980; P< 0.001).
Conclusion: Among ACS patients with HFmrEF who had undergone PCI, T2DM comorbidity was significantly associated with worse long-term outcomes.
Keywords: diabetes mellitus, acute coronary syndrome, heart failure with midrange ejection fraction, percutaneous coronary intervention, outcome
Background
Acute coronary syndrome (ACS) is the acute manifestation of ischemic heart disease. Despite optimal antithrombotic therapies and timely revascularization, ACS remains a major cause of morbidity and mortality worldwide, and can lead to the development of de novo acute heart failure (HF) or worsening of chronic HF.1 Diabetes mellitus (DM) is a complex, chronic metabolic disease, often complicated by coronary artery disease (CAD) and other atherosclerosis-related cardiovascular diseases, and is also a major risk factor of HF, especially for ACS patients. Epidemiological and clinical data from the last two decades have proven that DM increases the mortality of patients with HF with reduced ejection fraction (HFrEF).2 HF with midrange EF (HFmrEF), a distinct phenotype, was first defined as left ventricular EF (LVEF) of 40%–49% in the 2016 European Society of Cardiology (ESC) HF guidelines.3 Recent observational studies have focused only on description of its characteristics and prognosis of HFmrEF, and patients enrolled in these clinical trials had different HF etiology. In view this, our study concentrated on ACS patients using a 3-year retrospective analysis to investigate the role of DM in ACS patients with HFmrEF who had undergone percutaneous coronary intervention (PCI).
Methods
Patient Selection
ACS patients with HFmrEF who had undergone PCI were retrospectively (registered from January 2014 to June 2017) screened from the Coronary Angiography and Angioplasty Registry Database of Fujian Medical University Union Hospital. Inclusion criteria were hospitalization for ACS and had undergone PCI, survived to discharge following first admission, met HFmrEF diagnostic criteria according to the 2016 ESC guidelines,4 reviewed by an expert cardiologist during hospitalization, presence of symptoms and/or signs of HF, LVEF 40%–49%, BNP >35 and/or NT-proBNP >125pg/mL, objective evidence of other cardiac functional and structural alterations underlying HF, and a minimum 3-year follow-up completed. Exclusion criteria were echocardiography data or other clinical information not available, echocardiography-confirmed LVEF ≥50% or <40%, lost to follow-up, and HF due to nonischemic heart disease (such as valvular heart disease, alcoholic cardiomyopathy). Through the screening process, 377 HFmrEF patients were successfully enrolled in this analysis. This study was approved by the Ethics Committee of Fujian Medical University Union Hospital and conformed to the principles outlined in the Declaration of Helsinki (2021KY009). Informed consent was obtained from all patients. The flowchart is shown in Figure 1.
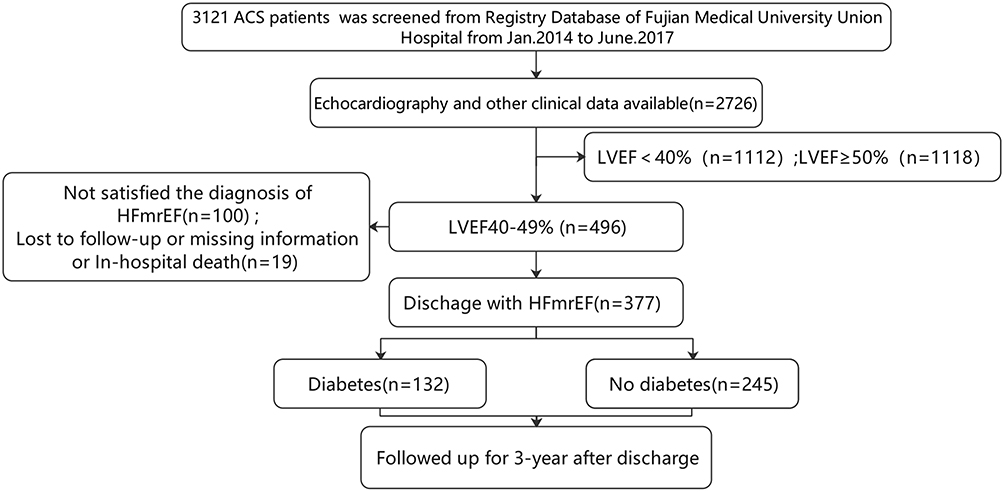 |
Figure 1 Patient-selection flowchart. Abbreviations: ACS, acute coronary syndrome; LVEF, left ventricular ejection fraction; HFmrEF, heart failure with midrange ejection fraction. |
Definition of Type 2 Diabetes Mellitus
Patients were considered to have type 2 DM (T2DM) if they had been previously informed of the diagnosis by a physician or were on glucose-lowering therapy, ie, insulin, oral hypoglycemic agents, diet, and exercise. Patients without previously diagnosed T2MD who required initiation of antihyperglycemic therapy during their hospital stay were also considered to have DM.5
Data Collection
Patient information and coronary angiography procedural details were collected by independent trained reviewers blinded to group assignment from hospital databases and recorded in a computerized database. Baseline data comprised demographics, clinical status, complications, comorbidities, electrocardiographic findings, angiographic and intervention status, and treatment, including discharge medications. Patients were divided into diabetic and nondiabetic groups at discharge from the index hospitalization.
Follow-Up and End Points
All patients were followed up and clinical end points occurring within the 3 years following index admission registered and recorded. Follow-up data were collected from review of hospital charts, discharge summary reviews, clinical visits, or telephone interviews conducted by the reviewers. The primary outcome was a composite of all-cause death or rehospitalization for HF. Secondary end points were a composite of cardiovascular death or rehospitalization for HF, all-cause death, cardiovascular death, rehospitalization for HF, and unplanned revascularization.6 Cardiovascular death was defined as death due to HF, myocardial infarction, cardiogenic shock, sudden cardiac death, death related to stroke, or other cardiac causes. Unexplained death was also regarded as cardiovascular in origin, unless obvious noncardiovascular causes could be identified. Rehospitalization for HF was defined as an admission for decompensated HF after discharge from the index hospitalization. Decompensated HF was defined on the basis of symptoms and signs, such as dyspnea, rales, and ankle edema, and the need for intravenous drug therapy, hemodialysis, and mechanical circulatory or respiratory support.7 Unplanned revascularization was repeat PCI or coronary artery–bypass grafting of any vessels, excluding staged PCI.8
Statistical Analysis
Continuous variables are presented as means ± SD or medians with interquartile ranges. Differences were assessed using Student’s t-test or Wilcoxon rank-sum test. Categorical variables are described as percentages, with differences analyzed with Pearson χ2 or Fisher’s exact test. For analysis of associations between DM and outcomes, incidence per 1,000 patient-years and incidence ratio were calculated for each outcome. Cumulative incidence of outcomes was estimated using regression estimates from a Cox proportional-hazard model including covariates that were either statistically significant (P<0.20) on univariate analysis or clinically relevant. Adjusted HRs were estimated by Cox regression and are presented with 95% CIs. Covariates taken into adjusted HR analysis were age, sex, hypertension, history of myocardial infarction, Killip functional class (III–IV vs I–II), atrial fibrillation or atrial flutter, diagnosis at admission (STEMI vs NSTE-ACS), coronary disease status (multivessel vs single-vessel disease), complete revascularization, statins, angiotensin converting–enzyme inhibitors (ACEIs)/angiotensin-receptor blockers (ARBs), and mineralocorticoid-receptor antagonists (MRAs). Survival curves were constructed using Kaplan–Meier estimates for time to first event and compared using log-rank tests.
For sensitivity analysis, a propensity score was estimated by fitting a logistic regression model adjusted for age, sex, Killip functional class (III–IV vs I–II), hypertension, atrial flutter, coronary disease status (multivessel vs single-vessel disease), complete revascularization, ACEIs or ARBs, and calcium-channel blockers (CCBs). Pair matching (1:1) between the two groups was performed by nearest-neighbor matching without replacement. The same analysis was performed for the propensity-matched cohorts. All tests were two tailed, and P<0.05 was considered statistically significant. All analyses were performed using SPSS 23.0.
Results
Baseline Characteristics
In sum, 377 ACS patients with HFmrEF who had undergone PCI and survived to discharge were enrolled and divided into diabetic and nondiabetic groups. Baseline characteristics are shown in Table 1. Mean age was 63.2 years, and 85.9% of patients were male. Diabetic patients were older than nondiabetic patients (63.83±11.29 vs 62.89±11.07 years, P=0.025), Comorbidities were comparable, except for higher prevalence of hypertension (75.8% vs 5 4.3%, P<0.001) in the diabetic group. However, NT-proBNP at admission between two groups was not significantly different (959.0 [301.5–2,013.0] vs 1,133.0 [336.0–2,693.5], P=0.307). With regard to medication at discharge, ACEIs/ARBs and CCBs were more frequently prescribed in the nondiabetic group (57.6% vs 70.2%, P=0.017 and 6.1% vs 13.5%, P=0.036, respectively). Compared with nondiabetic patients, diabetic patients showed higher prevalence of multivessel disease (57.6% vs 47.5%, P=0.015) and required longer stents (43.5 [29–69.75] vs 33 [24–60] mm; P=0.038). However, they received less complete revascularization (47% vs 62%, P=0.006). There was no significant difference between the groups with respect to the proportion of drug-eluting stent use, stent number, or minimum stent diameter. Because the baseline characteristics were in disequilibrium, we used 1:1 propensity-score matching, after which no significant differences were observed between the groups, as also shown in Table 1.
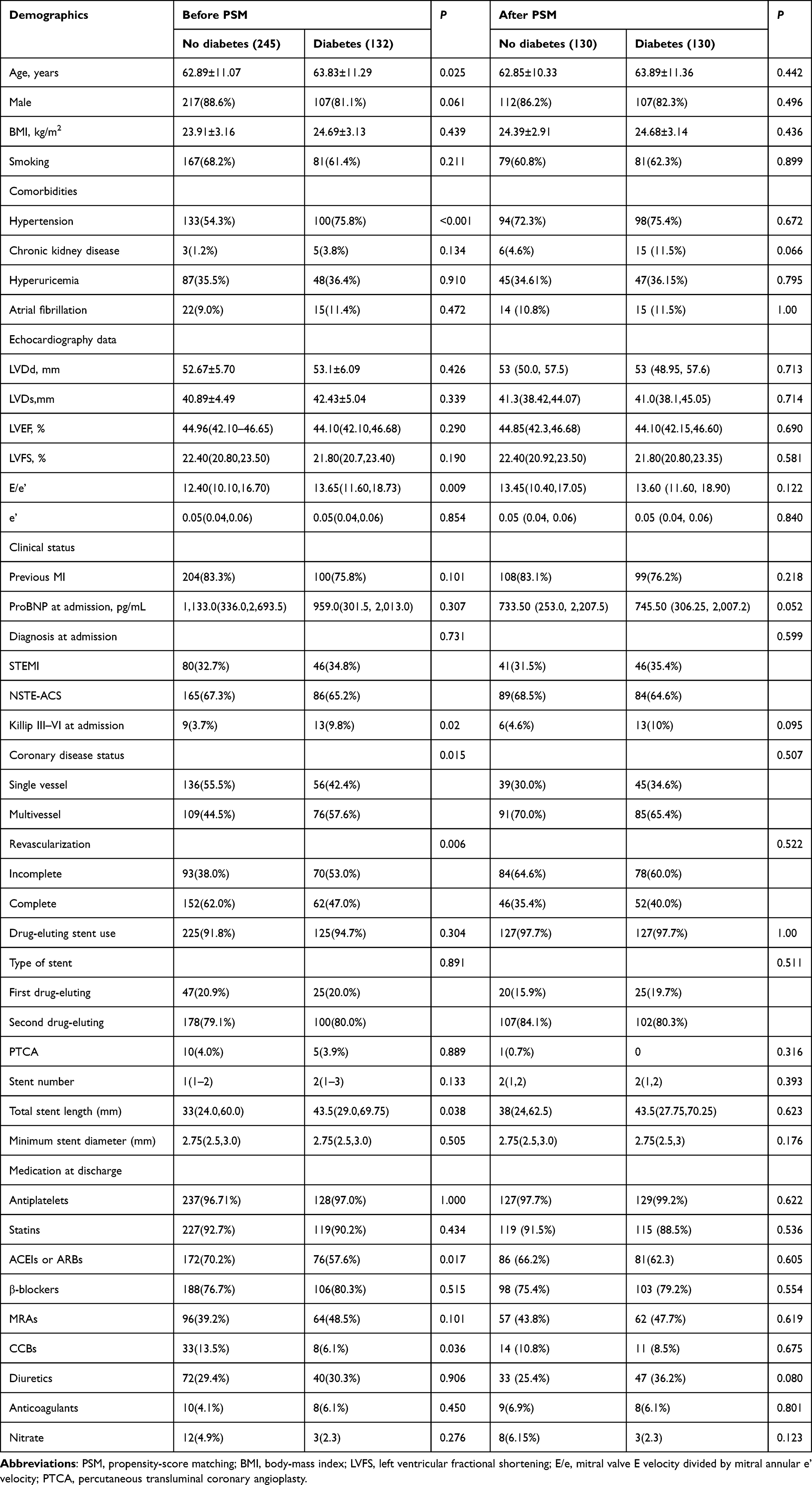 |
Table 1 Baseline characteristics |
Comparison of 3-Year Outcomes Between Diabetic and Nondiabetic Patients
During a follow-up of 3 years, incidence of the primary outcome was higher in diabetic patients than nondiabetic patients (33 [25%] vs 31 [12.6%], P=0.002). Incidence of the composite outcome of all-cause death/HF rehospitalization, composite outcome of cardiovascular death/HF rehospitalization, all-cause death, cardiovascular death, HF rehospitalization, and unplanned revascularization per 1,000 patient-years were 96.1 vs 44.6, 88.6 vs 41.6, 49.5 vs 20.8, 43.7 vs 14.9, 82.4 vs 35.7, and 92.9 vs 48.4 for the diabetic and nondiabetic groups, respectively (Table 2). Incidence ORs were 2.301 (95% CI 1.334–3.969, P=0.002), 2.055 (95% CI 1.291–3.272, P=0.003), 2.254 (95% CI 1.148–4.260, P=0.019), 2.784 (95% CI 1.287–6.023, P=0.009), 2.320 (95% CI 1.417–3.800, P=0.001) and 2.056 (95% CI 1.196–3.532, P=0.010) for each outcome (Table 2).
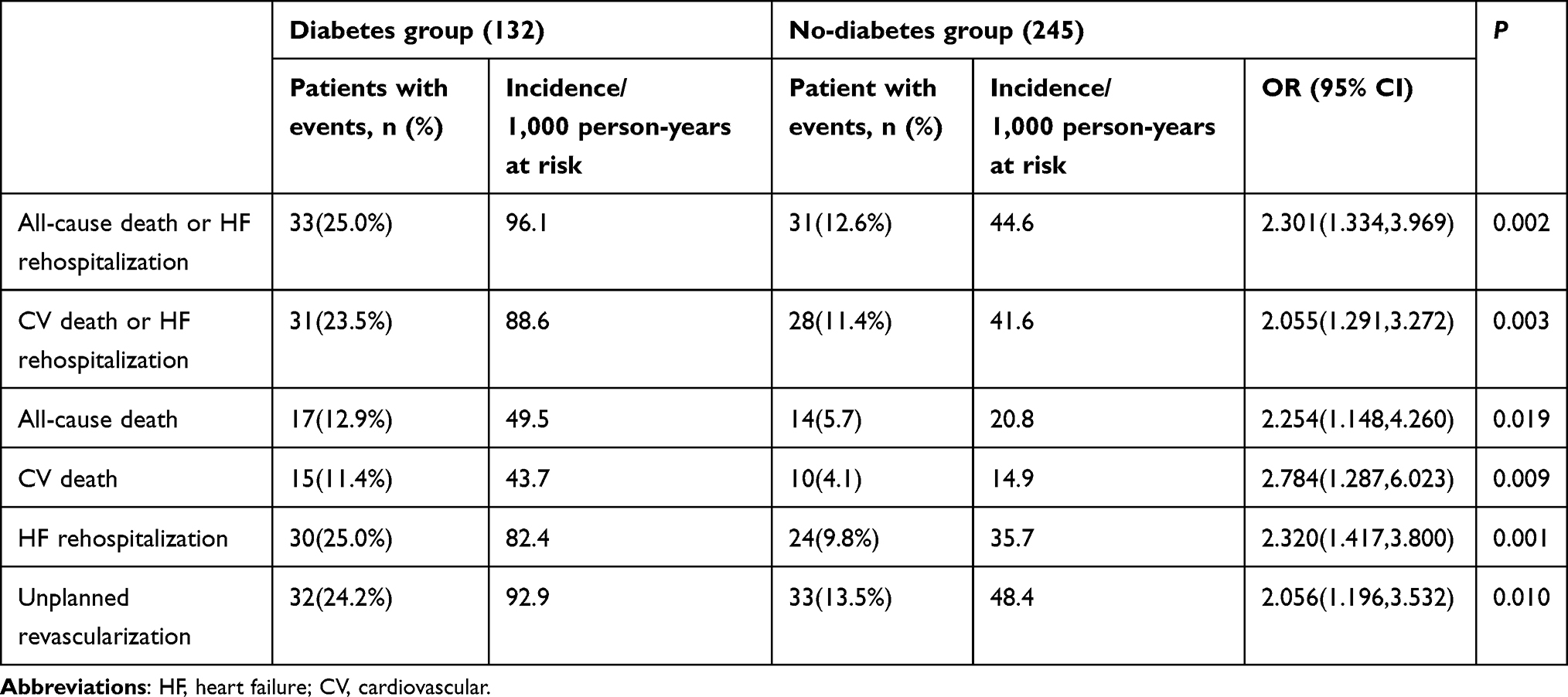 |
Table 2 Incidence and prevalence |
Univariate analysis of the composite of all-cause death or HF rehospitalization using Cox regression demonstrated that DM, age, sex, Killip functional class III–IV at admission, complete revascularization, and atrial fibrillation were significantly associated with the primary outcome. Multivariate analysis of these factors showed that DM (adjusted HR 2.080, 95% CI 1.115–3.878; P=0.021), age (adjusted HR 1.038, 95% CI 1.007–1.069; P=0.015), Killip III–VI at admission (adjusted HR 1.268, 95% CI 1.006–2.213; P=0.032), multivessel disease (adjusted HR 3.146, 95% CI 1.210–8.185; P=0.019), complete revascularization (adjusted HR 0.149, 95% CI 0.057–0.391; P<0.001), and atrial fibrillation (adjusted HR 3.411, 95% CI 1.510–7.702; P=0.003) were associated with worse prognosis (Table 3). After propensity-score matching, DM (adjusted HR 3.792, 95% CI 1.802–7.980; P<0.001) was still significantly associated with the primary outcome on multivariate analysis (Table 4).
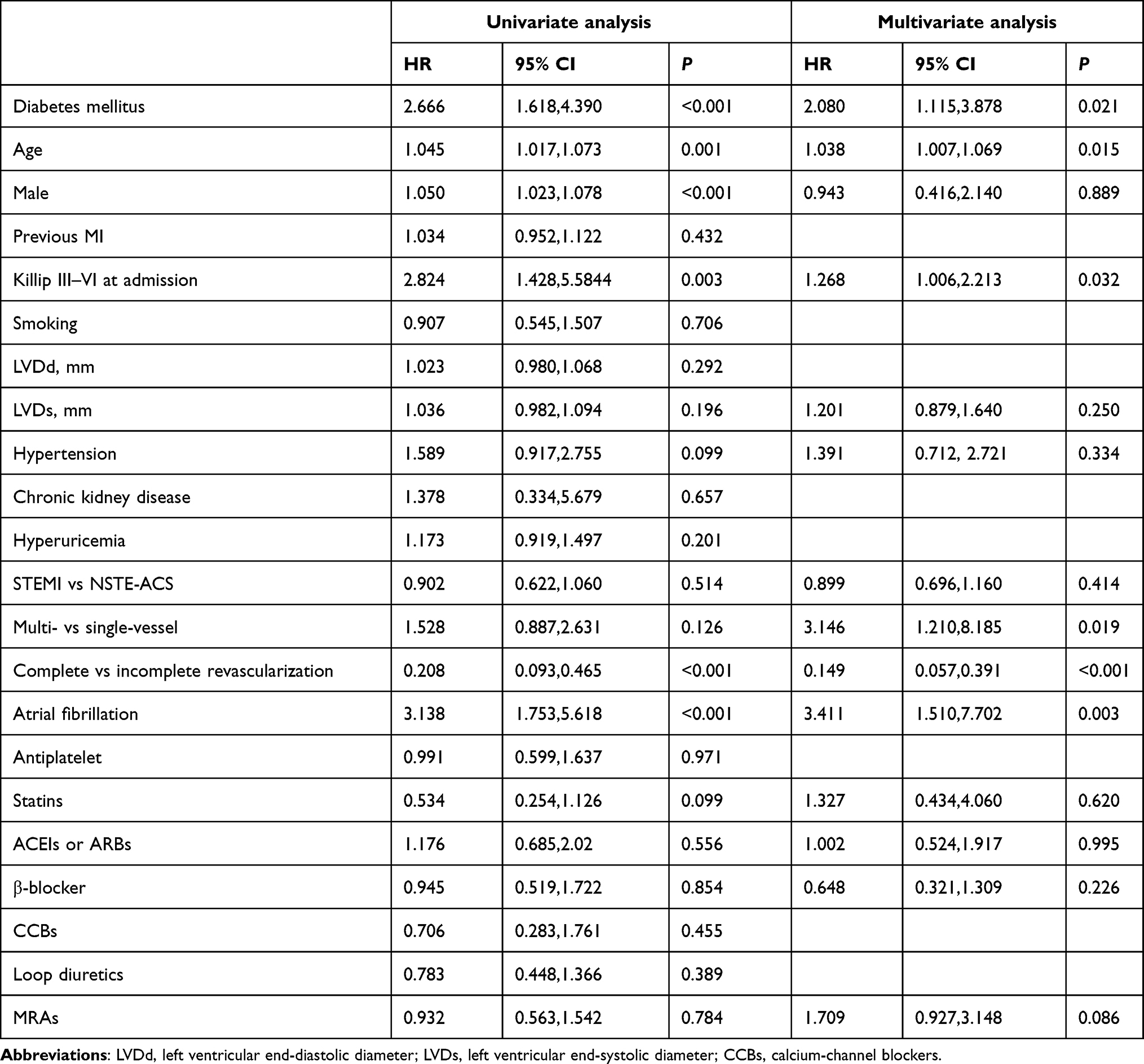 |
Table 3 Unadjusted and adjusted HRs for primary outcome |
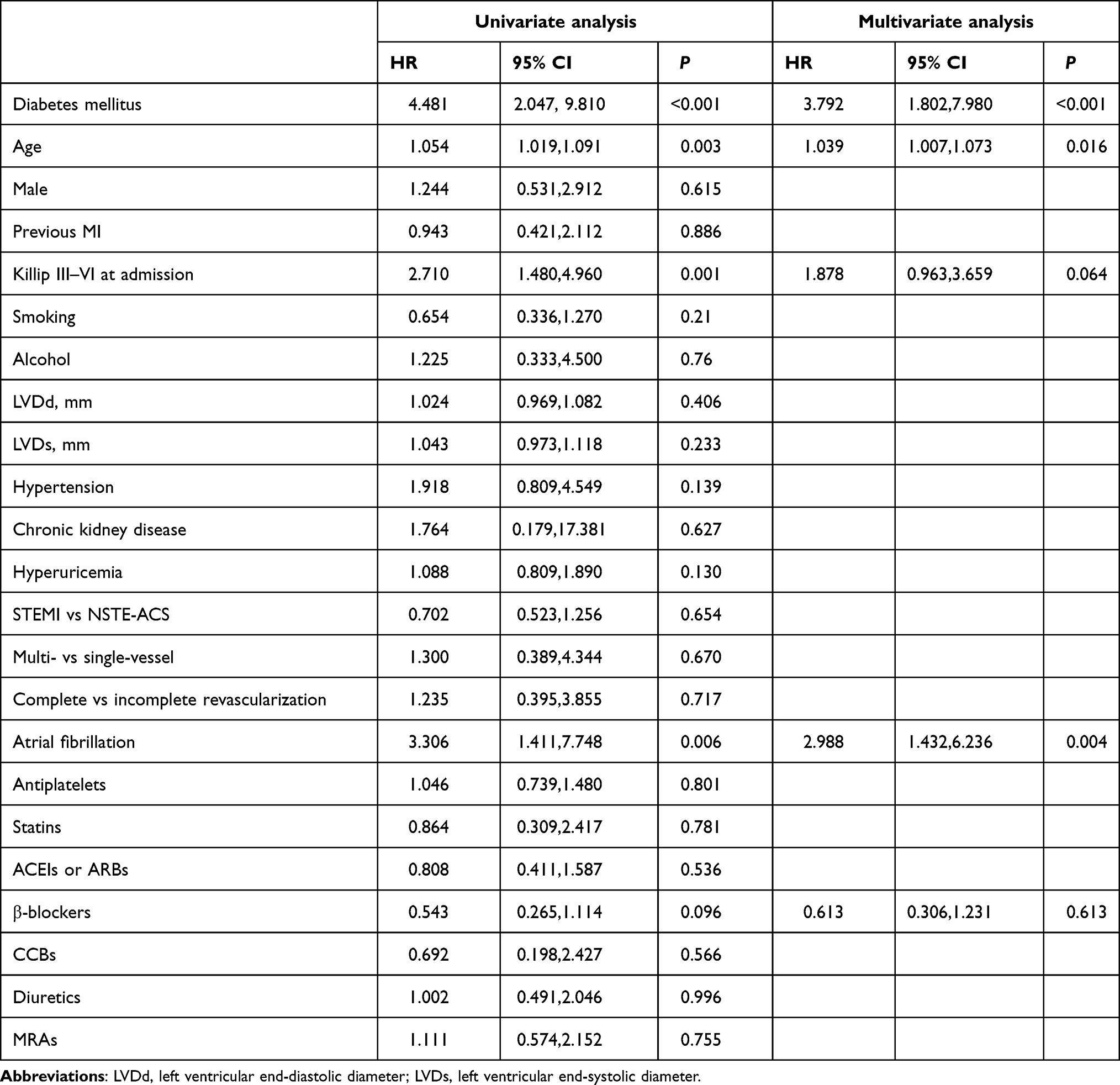 |
Table 4 Unadjusted and adjusted HRs for primary outcome in propensity score–matched cohorts |
Figure 2 shows survival curves constructed using Kaplan–Meier estimates for time to first event and the cumulative incidence of each outcome. Cumulative incidence of the composite of all-cause death/HF rehospitalization (P=0.0023, Figure 2A), composite of cardiovascular death/HF rehospitalization (P=0.0028, Figure 2B), all-cause death (P=0.0163, Figure 2C), cardiovascular death (P=0.0071, Figure 2D), HF hospitalization (P=0.0006, Figure 2E), and unplanned revascularization (P=0.0081, Figure 2F) were significantly higher in the diabetic patients. After adjustment by propensity-score matching, DM still increased the cumulative incidence of the composite of all-cause death/HF rehospitalization (P=0.0001, Figure 3A), composite of cardiovascular death/HF rehospitalization (P=0.0004, Figure 3B), all-cause death (P=0.0004, Figure 3C), cardiovascular death (P=0.0004, Figure 3D), and HF rehospitalization (P=0.0003, Figure 3E), but no significant association was found between DM and cumulative incidence of unplanned revascularization (P=0.1189, Figure 3F).
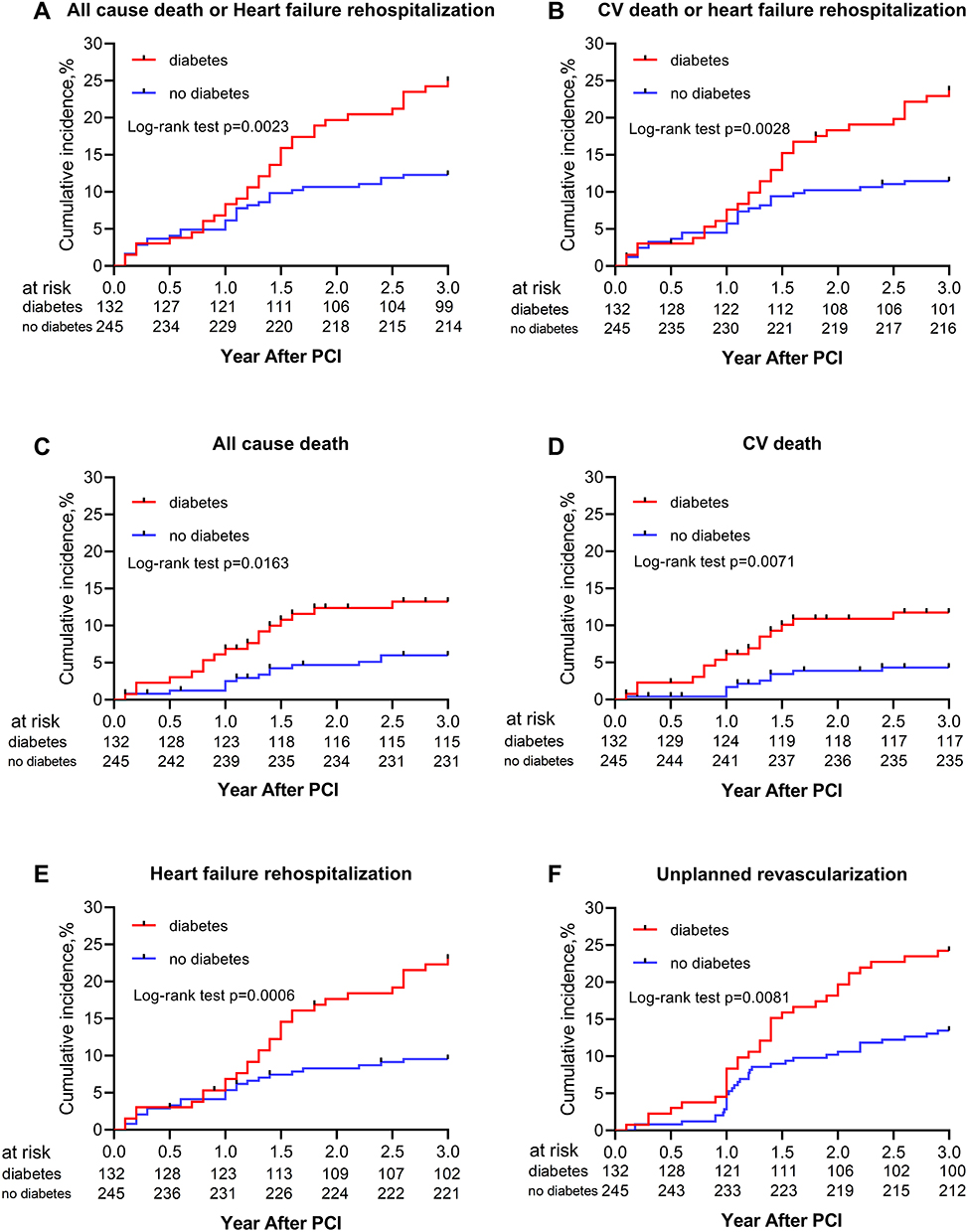 |
Figure 2 Comparison of estimated event rates: (A) all-cause death and heart-failure hospitalization; (B) CV death and heart-failure hospitalization; (C) all-cause death; (D) CV death; (E) heart-failure hospitalization; (F) unplanned revascularization between diabetes group (red dotted line) and nondiabetes group (solidblue line) after PCI. |
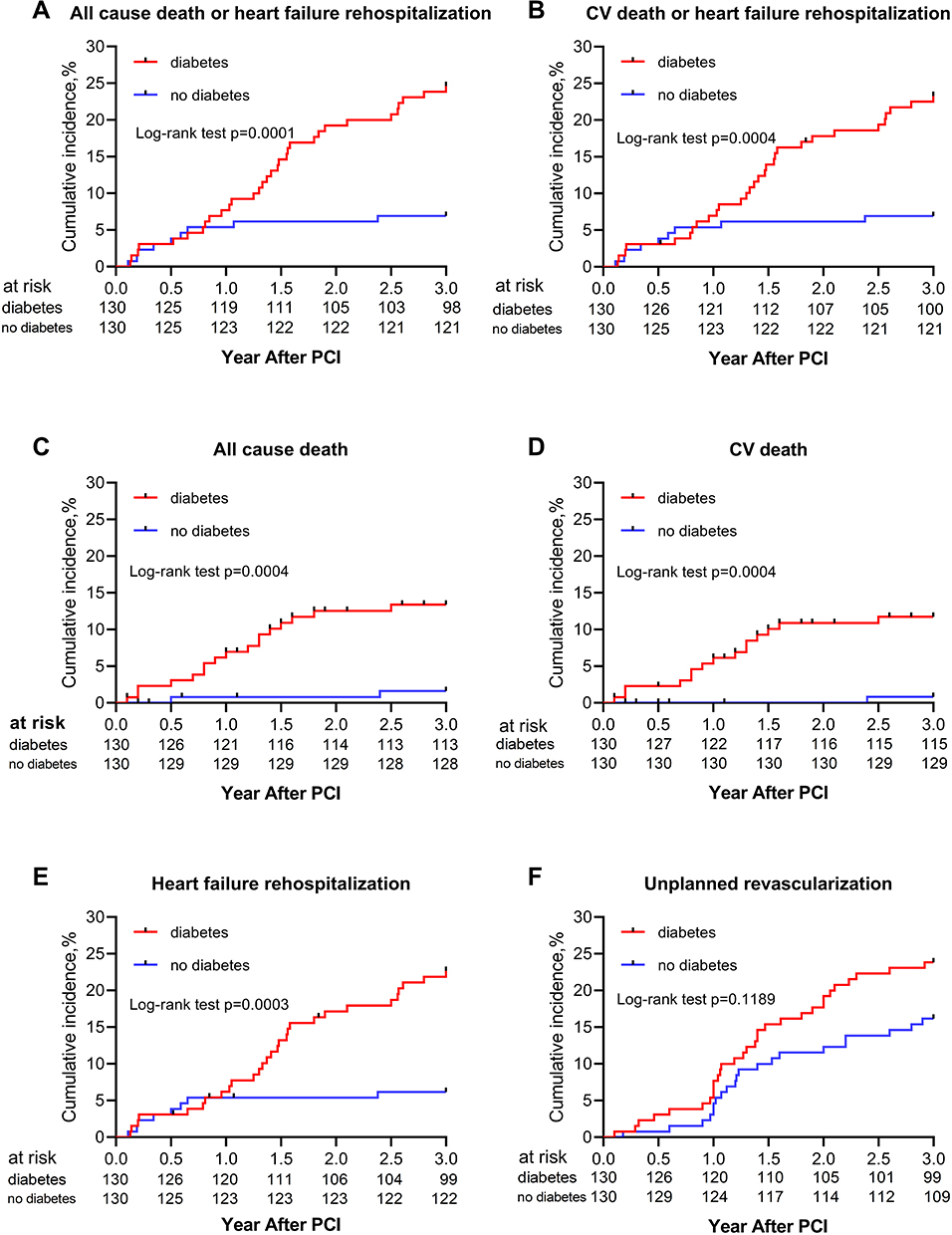 |
Figure 3 Comparison of estimated event rates: (A) all-cause death and heart-failure hospitalization; (B) CV death and heart-failure hospitalization; (C) all-cause death; (D) CV death; (E) heart-failure rehospitalization; (F) unplanned revascularization between diabetes group (dotted red line) and nondiabetes group (solid blue line) after PCI in propensity score–matched cohorts. |
Subgroup Analysis
To confirm the association between DM and the composite of all-cause death/HF rehospitalization across various subgroups, we performed post hoc subgroup analyses. As Figure 4 shows, despite complete revascularization having been done, DM patients still suffered a higher risk of the primary outcome (OR 0.24, 95% CI 0.10–0.59; P<0.05). No difference between groups was found for patients with incomplete revascularization. DM also increased the risk of adverse outcomes in patients with multivessel disease (OR 0.45, 95% CI 0.22–0.94; P<0.05), hypertension (OR 0.45, 95% CI 0.23–0.87; P<0.05), or left anterior descending artery as target vessel (OR 0.42, 95% CI 0.22–0.80; P<0.05), but not among patients with single-vessel disease or right coronary/left circumflex artery as target vessel (all P≥0.05). The effect of DM on ACS patients with HFmrEF who had undergone PCI was not related to age or creatinine-clearance rate on subgroup analysis (all P≥0.05). Similar results were found in propensity score–matched cohorts, except for the fact that regardless of revascularization having been performed or not, DM still increased the risk of the composite end point (as shown in Figure 5). To further study the effect of glycemic control status on prognosis, we divided diabetic patients into two groups: well controlled (HbA1c <7.5%) and poorly controlled (HbA1c ≥7.5%), according to the level of glycosylated hemoglobin tested at baseline and at the end of 1-year follow-up. As the survival curves show in Figure 6, compared with well-controlled diabetic patients, cumulative incidence of the composite of all-cause death/HF rehospitalization was significantly higher in poorly controlled diabetic patients (all P<0.05).
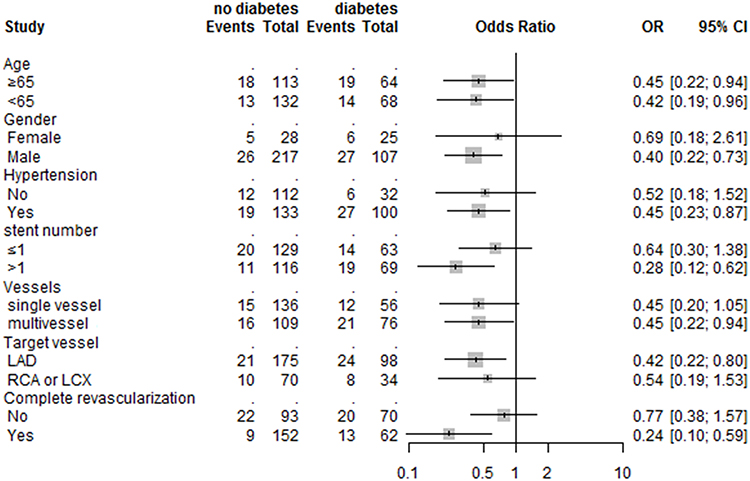 |
Figure 4 Comparative unadjusted ORs of primary outcome between diabetes group and nondiabetes group for each subgroup in the overall population. |
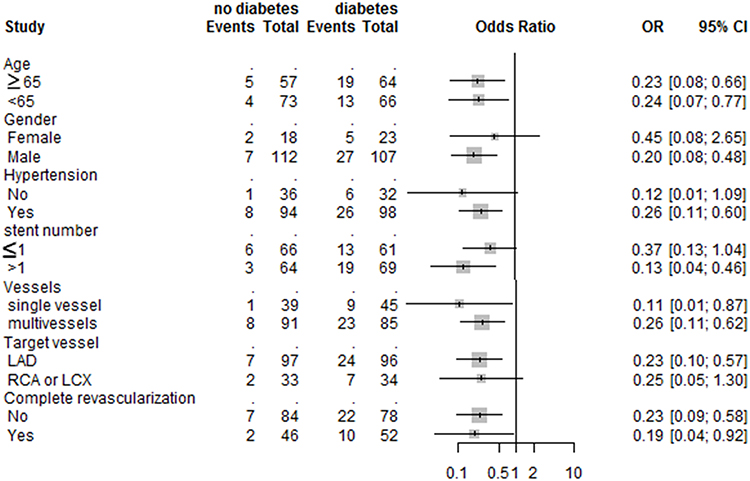 |
Figure 5 Comparative unadjusted ORs of primary outcome between diabetes group and nondiabetes group for each subgroup in propensity score–matched cohorts. |
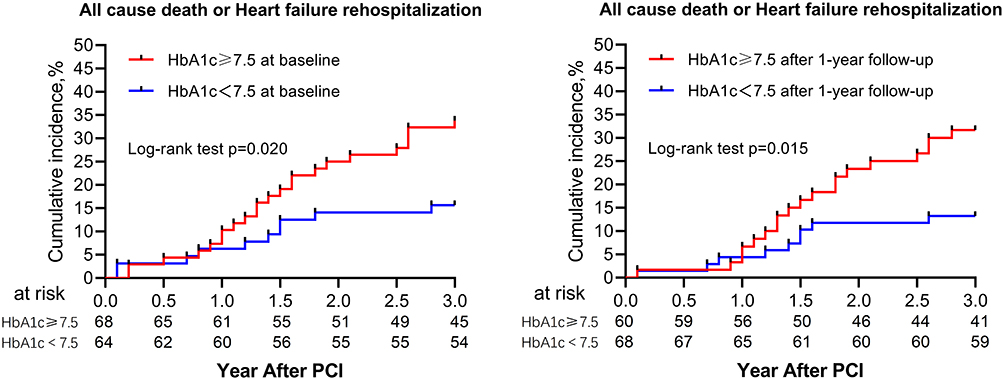 |
Figure 6 Comparison of estimated event rates of all-cause death and heart-failure rehospitalization diabetes patients stratified by HbA1c ≥7.5% tested at baseline and 1-year follow-up. |
Discussion
HF with LVEF of 40%–49% is a gray area existing between HFrEF and HFpEF that the 2016 ESC HF guidelines termed HFmrEF.4 In view of the fact that previous studies had focused only on describing its characteristics with no focus on etiology,9–11 our study concentrated on ACS patients in a 3-year retrospective analysis to further investigate the relationship between DM and long-term outcomes in the ACS patients with HFmrEF after PCI. The major finding of the present study was that DM significantly increased the risk of the composite of all-cause death/HF rehospitalization in this population, especially in ACS patients with poorly controlled glycemic status. This is an another in-depth report to identify such a relationship between DM and ACS patients with HFmrEF who have undergone PCI.
There is a consensus that patients with HF often have higher DM prevalence. The proportion of T2DM in chronic HF patients is about 30%, irrespective of HF phenotype (ie, HFrEF and HFpEF),12–14 and 30%–40% in clinical trials on acute HF. We found similar results: approximately 35% of our HFmrEF patients had DM. Although a majority of data in the past suggested that DM significantly increased the risk of HF secondary to CAD, most of those data were limited to patients with HF whose EF was reduced or preserved.13,15,16 Maybe our research has provided some data to fill the lack of knowledge on HFmrEF and furthers exploration of the pathophysiological mechanisms of DM increasing the risk of adverse prognoses for HFmrEF patients.
Knowledge about pathophysiological aspects of myocardial dysfunction in T2DM has increased enormously in recent years. Widely accepted is the fact that DM patients develop CAD more easily and suffer more diffuse coronary disease. As shown in Table 1, the prevalence of multivessel disease in the diabetic group was higher and stents longer, demonstrating that T2DM causes accelerated atherosclerosis and more diffuse atherosclerosis in the coronary arteries, which may partly explained why DM is associated with adverse prognoses. Complete revascularization in diabetic patients was proportionally lower (47% vs 62%, P<0.05), which suggests that complete revascularization may help to protect HF patients from adverse events. Evidence-based data on the importance of complete revascularization in HF cases are limited, but randomized data provide evidence suggesting CAD patients with HF may benefit from complete revascularization (SYNTAX and FAME trials).17,18 However, the worse prognosis of diabetic patients did not change in the propensity score–matched cohort after differences in complete revascularization had been balanced. Subgroup analyses also demonstrated that whether revascularized or not, DM patients still suffered a higher risk of adverse outcomes (Figures 4 and 5), suggesting that revascularization alone is not enough to change the prognosis of diabetic patients.
Neurohormonal antagonists (ACEIs, MRAs, and β-blockers) are recommended and have been shown to improve survival in patients with HF. However, few differences were observed between the diabetic and nondiabetic groups in respect of medication at discharge (MRAs and β-blockers, but not ACEIs/ARBs) for HF in this study, especially in propensity score–matched cohorts. In other words, HF patients with DM had not received individualized or optimal treatment different from those without DM, which may be one of the reasons for the worse prognosis for these patients. Thus far, there have been no clinical trials of HF treatment to include only patients with T2DM, so the evidence available is from subgroup analyses of mixed populations. The embarrassing situation of there being no specific recommendations on HF treatment in T2DM patients needs solving urgently.
Many clinical trials have observed that T2DM-related processes can cause myocardial dysfunction in certain diabetic patients, but in the absence of CAD. Rubler et al came up with a new theory named “diabetic cardiomyopathy” to explain such a phenomenon.19 Hyperglycemia and insulin resistance are the two major consequences of DM responsible for cardiovascular disorders in patients with DM.20 Their detrimental effects interact with each other and exert a potentiating effect, leading to several maladaptive responses and resulting in myocyte alteration, a common element in these chains being that ROS production increases diabetic cardiomyocytes. Hyperglycemia and insulin resistance affect myocardial function by breaking the balance of ROS production in cardiomyocytes, leading to impaired cellular function and cardiovascular pathology.21 Subgroup analysis revealed that DM was associated with adverse outcomes independently of age, sex, and hypertension (Figures 4 and 5). Figure 6 shows that compared with diabetic patients with well-controlled glycemic status (HbA1c <7.5%), diabetic patients with poorly controlled glycemic status (HbA1c ≥7.5%) were more at risk of composite end-point events, demonstrating that hyperglycemia itself has an important impact on the prognosis of HF patients with DM, indirectly indicating that optimized antidiabetic treatment and strict blood-glucose control is of great significance in improving the prognosis. However, old antidiabetic drugs used widely, such as insulin and sulfonylureas, have not been proved safe in HF patients with T2DM,22,23 and some drugs have even been shown to increase the risk of HF hospitalization (ie, rosiglitazone, pioglitazone, and saxagliptin).24–27 Inappropriate antidiabetic treatment not only fails to benefit patients but may also lead to adverse outcomes. Fortunately, some new antidiabetic drugs, such as GLP1-receptor agonists and DPP4 inhibitors, have no impact on the risk of HF hospitalization.28–32 In addition, SGLT2 inhibitors (eg, empagliflozin and canagliflozin) have demonstrated a significant reduction in the risk of HF hospitalization in patients with T2DM, and are currently being investigated as a potential addition to the optimal medical treatment of HF, especially in patients with T2DM.33,34 Therefore, we speculate that combined use of optimized hypoglycemic drugs and anti-HF drugs may bring the greatest improvement to HF patients with DM in prognosis.
Limitations
Several limitations of this study should be acknowledged. Firstly, this was a single-center, retrospective, observational study, the sample was limited, and the number of subjects with DM modest (132), but it still provides meaningful evidence for clinical practice. Secondly, we attempted to explore the impact of complete revascularization on the prognosis of ACS patients with HFmrEF, and found that it may be one of the factors affecting prognosis, but not the only one. In view of this, we tried to study whether optimization of drug treatment, including anti-HF and antidiabetic drugs, may be more important for the prognosis of such a population, but the limited data are not enough to support our conjecture. More large-scale randomized controlled trials are required to verify such a conjecture. Thirdly, the details of antidiabetic therapy were not collected, so the effects of such therapy on the prognosis of HFmrEF complicated with DM was not completed.
Conclusion
Taken together, our data suggested that T2DM was associated with adverse outcomes in ACS patients with HFmrEF who had undergone PCI and significantly increased the risk of mortality and HF rehospitalization compared to HF patients without T2DM. For management of this population, in addition to effective revascularization, optimal medication including the optimization of hypoglycemic therapy and anti-HF therapy was probably more significant.
Abbreviations
T2DM, type 2 diabetes mellitus; ACS, acute coronary syndrome; HFmrEF, heart failure with midrange ejection fraction; HFrEF, HF with reduced EF; HFpEF, HF with preserved EF; LVEF, left ventricular EF; PCI, percutaneous coronary intervention; CAD, coronary artery disease; MI, myocardial infarction; STEMI, ST-elevation MI; NSTE, non–ST segment elevation; ACEI, angiotensin converting–enzyme inhibitor; ARB, angiotensin-receptor blocker; CCB, calcium-channel blocker; MRA, mineralocorticoid-receptor antagonist.
Data Sharing
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics and Consent
The study (2021KY009) was approved by the Clinical Research Ethics Committee of Union Hospital, Fujian Medical University, Fuzhou, Fujian, China.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the Natural Science Foundation of Fujian Province (2020J011028) and partially sponsored by the Fujian Provincial Health Technology Project (2020CXB015).
Disclosure
The authors declare that they have no competing interests.
References
1. Eisen A, Giugliano RP, Braunwald E. Updates on acute coronary syndrome: a review. JAMA Cardiol. 2016;1(6):718–730. doi:10.1001/jamacardio.2016.2049
2. Lehrke M, Marx N. Diabetes mellitus and heart failure. Am J Med. 2017;130(6S):S40–S50. doi:10.1016/j.amjmed.2017.04.010
3. van der Meer P, Gaggin HK, Dec GW. ACC/AHA versus ESC guidelines on heart failure: JACC guideline comparison. J Am Coll Cardiol. 2019;73(21):2756–2768. doi:10.1016/j.jacc.2019.03.478
4. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. doi:10.1002/ejhf.592
5. Aronson D, Musallam A, Lessick J, et al. Impact of diastolic dysfunction on the development of heart failure in diabetic patients after acute myocardial infarction. Circ Heart Fail. 2010;1:125–131. doi:10.1161/CIRCHEARTFAILURE.109.877340
6. Enzan N, Matsushima S, Ide T, et al. Spironolactone use is associated with improved outcomes in heart failure with mid-range ejection fraction. ESC Heart Fail. 2020;7(1):339–347. doi:10.1002/ehf2.12571
7. Shiga T, Suzuki A, Haruta S, et al. Clinical characteristics of hospitalized heart failure patients with preserved, mid- range, and reduced ejection fractions in Japan. ESC Heart Fail. 2019;6(3):475–486. doi:10.1002/ehf2.12418
8. Sen S, Ahmad Y, Dehbi HM, et al. Clinical events after deferral of LAD revascularization following physiological coronary assessment. J Am Coll Cardiol. 2019;73(4):444–453. doi:10.1016/j.jacc.2018.10.070
9. Chioncel O, Lainscak M, Seferovic PM, et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017;19(12):1574–1585. doi:10.1002/ejhf.813
10. Kapoor JR, Kapoor R, Ju C, et al.Precipitating clinical factors, heart failure characterization, and outcomes in patients hospitalized with heart failure with reduced, borderline, and preserved ejection fraction. JACC Heart Fail. 2016;(6):464–472. doi:10.1016/j.jchf.2016.02.017
11. Guisado-Espartero ME, Salamanca-Bautista P, Aramburu-Bodas Ó, et al.; RICA investigators group. Heart failure with mid-range ejection fraction in patients admitted to internal medicine departments: findings from the RICA registry. Int J Cardiol. 2018;255:124–128. doi:10.1016/j.ijcard.2017.07.101
12. McMurray JJ, Packer M, Desai AS, et al.; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993–1004. doi:10.1056/NEJMoa1409077
13. Banks AZ, Mentz RJ, Stebbins A, et al. Response to exercise training and outcomes in patients with heart failure and diabetes mellitus: insights from the HF-ACTION trial. J Card Fail. 2016;22(7):485–491. doi:10.1016/j.cardfail.2015.12.007
14. Sarma S, Mentz RJ, Kwasny MJ, et al.; EVEREST investigators. Association between diabetes mellitus and post-discharge outcomes in patients hospitalized with heart failure: findings from the EVEREST trial. Eur J Heart Fail. 2013;15(2):194–202. doi:10.1093/eurjhf/hfs153
15. Kristensen SL, Preiss D, Jhund PS, et al.; PARADIGM-HF Investigators and Committees. Risk related to pre-diabetes mellitus and diabetes mellitus in heart failure with reduced ejection fraction: insights from prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial. Circ Heart Fail. 2016;9(1):e002560. doi:10.1161/CIRCHEARTFAILURE.115.002560
16. MacDonald MR, Petrie MC, Varyani F, et al.; CHARM Investigators. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: assessment of reduction in mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29(11):1377–1385. doi:10.1093/eurheartj/ehn153
17. Head SJ, Mack MJ, Holmes DR, et al. Incidence, predictors and outcomes of incomplete revascularization after percutaneous coronary intervention and coronary artery bypass grafting: a subgroup analysis of 3-year SYNTAX data. Eur J Cardiothorac Surg. 2012;41(3):535–541. doi:10.1093/ejcts/ezr105
18. Tonino PA, De Bruyne B, Pijls NH, et al.; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213–224. doi:10.1056/NEJMoa0807611
19. Rubler S, Dlugash J, Yuceoglu YZ, et al. New type of cardiomyopathy associated with diabetic glomerulosclerosis. Am J Cardiol. 1972;30(6):595–602. doi:10.1016/0002-9149(72)90595-4
20. Shah MS, Brownlee M. Molecular and cellular mechanisms of cardiovascular disorders in diabetes. Circ Res. 2016;118(11):1808–1829. doi:10.1161/CIRCRESAHA.116.306923
21. Nathan C, Cunningham-Bussel A. Beyond oxidative stress: an immunologist’s guide to reactive oxygen species. Nat Rev Immunol. 2013;13(5):349–361. doi:10.1038/nri3423
22. Carrasco-Sánchez FJ, Gomez-Huelgas R, Formiga F, et al.; RICA investigators. Association between type-2 diabetes mellitus and post-discharge outcomes in heart failure patients: findings from the RICA registry. Diabetes Res Clin Pract. 2014;104(3):410–419. doi:10.1016/j.diabres.2014.03.015
23. MacDonald MR, Petrie MC, Hawkins NM, et al. Diabetes, left ventricular systolic dysfunction, and chronic heart failure. Eur Heart J. 2008;29(10):1224–1240. doi:10.1093/eurheartj/ehn156
24. Komajda M, McMurray JJ, Beck-Nielsen H, et al. Heart failure events with rosiglitazone in type 2 diabetes: data from the RECORD clinical trial. Eur Heart J. 2010;31(7):824–831. doi:10.1093/eurheartj/ehp604
25. Lago RM, Singh PP, Nesto RW. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: a meta-analysis of randomised clinical trials. Lancet. 2007;370(9593):1129–1136. doi:10.1016/S0140-6736(07)61514-1
26. MacDonald MR, Eurich DT, Majumdar SR, et al. Treatment of type 2 diabetes and outcomes in patients with heart failure: a nested case-control study from the U.K. general practice research database. Diabetes Care. 2010;33(6):1213–1218.
27. Scirica BM, Braunwald E, Raz I, et al.; SAVOR-TIMI 53 Steering Committee and Investigators. Heart failure, saxagliptin, and diabetes mellitus: observations from the SAVOR-TIMI 53 randomized trial. Circulation. 2015;132(15):e198. doi:10.1161/CIRCULATIONAHA.115.015511
28. Marso SP, Daniels GH, Brown-Frandsen K, et al.; LEADER Steering Committee. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–322. doi:10.1056/NEJMoa1603827
29. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXA Investigators. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247–2257. doi:10.1056/NEJMoa1509225
30. Holman RR, Bethel MA, Mentz RJ, et al.; EXSCEL Study Group. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228–1239. doi:10.1056/NEJMoa1612917
31. Jorsal A, Kistorp C, Holmager P, et al. Effect of liraglutide, a glucagon-like peptide-1 analogue, on left ventricular function in stable chronic heart failure patients with and without diabetes (LIVE)-A multicentre, double-blind, randomised, placebo-controlled trial. Eur J Heart Fail. 2017;19(1):69–77. doi:10.1002/ejhf.657
32. Margulies KB, Hernandez AF, Redfield MM, et al.; NHLBI Heart Failure Clinical Research Network. Effects of liraglutide on clinical stability among patients with advanced heart failure and reduced ejection fraction: a randomized clinical trial. JAMA. 2016;316(5):500–508. doi:10.1001/jama.2016.10260
33. Neal B, Perkovic V, Mahaffey KW, et al.; CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
34. Zinman B, Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi:10.1056/NEJMoa1504720
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.