")
Back to Journals » International Journal of Women's Health » Volume 16
Risk Factors and Patient-Reported Outcomes in Chinese Women with Postpartum Diastasis Recti Abdominis: An Observational Study
Authors Zhu Y, Jiang L, Ye T, Liu Y, Sun L, Xiao L, Chen J, Wang T, Ren Y, Xu H, Zhao H, Mao X, Shen T
Received 25 August 2023
Accepted for publication 22 January 2024
Published 31 January 2024 Volume 2024:16 Pages 179—192
DOI https://doi.org/10.2147/IJWH.S437088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ying Zhu,1 Liyuan Jiang,2 Tiantian Ye,3 Yan Liu,4 Li Sun,2 Lijuan Xiao,5 Jiayu Chen,6 Ting Wang,7 Yinghua Ren,8 Hongjun Xu,8 Huihui Zhao,8 Xiaozhen Mao,8 Tiantian Shen9
1School of Basic Medical Sciences, Zhejiang Chinese Medical University, Hangzhou, 310053, People’s Republic of China; 2Department of Acupuncture and Rehabilitation, Hangzhou Hospital of Traditional Chinese Medicine, Hangzhou, 310005, People’s Republic of China; 3The 1st Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, 310053, People’s Republic of China; 4The 2nd Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, 310053, People’s Republic of China; 5Department of Rehabilitation, Chun’an County Hospital of Traditional Chinese Medicine, Chun’an, 311799, People’s Republic of China; 6Department of Rehabilitation, Huzhou Central Hospital, Huzhou, 313099, People’s Republic of China; 7The 3rd Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, 310053, People’s Republic of China; 8Department of Acupuncture and Tuina, Community Health Service Center of Zhuantang Street, Hangzhou, 310024, People’s Republic of China; 9Department of Acupuncture and Rehabilitation, Shengzhou Municipal Hospital of Traditional Chinese Medicine, Hangzhou, 312499, People’s Republic of China
Correspondence: Liyuan Jiang, Department of Acupuncture and Rehabilitation, Hangzhou Hospital of Traditional Chinese Medicine, No. 453, Stadium Road, Xihu District, Hangzhou, 310005, People’s Republic of China, Tel +86-13018976755, Email [email protected]
Purpose: Diastasis recti abdominis (DRA) is a condition in which the linea alba is stretched and widened, and the abdominal muscles are separated from each other. DRA typically occurs in pregnant and postpartum women. We aimed to determine the risk factors and patient-reported outcomes (PROs) of DRA in Chinese postpartum women.
Methods: This observational study was conducted in Hangzhou Hospital of Traditional Chinese Medicine, and involved 534 women who filled out the following risk-factor and PRO questionnaires: SF-MPQ-2, SF-ICIQ, LDQ, EPDS, MBIS, HerQles, and SF-36 (all Chinese versions). The inter-recti distance was measured by palpation. Statistical analyses were performed using SPSS v25.0 software and the Mann–Whitney U-test, chi-square test, binary logistic regression analysis (for risk factors of DRA), and the Kendall and Spearman tests (for correlation analysis).
Results: After childbirth, 78.1% (417/534) of the enrolled women had DRA. Abdominal surgery (P = 0.002), number of pregnancies (P = 0.035), parity (P = 0.012), number of births (P = 0.02), fetal birth weight (P = 0.014), and waist-to-hip ratio in the supine position (P = 0.045) significantly differed between the DRA and non-DRA groups. Caesarean delivery was an independent risk factor for DRA. The PROs were significantly worse in the DRA group than in the non-DRA group.
Conclusion: Caesarean delivery was an independent risk factor for DRA. Women with DRA are more likely to have limited physical activity or function after childbirth, lower self-confidence, and a decreased quality of life.
Keywords: risk factors, patient-reported outcome measures, diastasis recti abdominis, postpartum period
Introduction
Diastasis recti abdominis (DRA) is a condition in which the linea alba is stretched and widened, and the abdominal muscles are separated from each other, typically due to pregnancy. DRA greatly affects patients’ quality of life (QoL) during pregnancy and the postpartum period, and imposes a financial burden on patients and their families. Moreover, DRA is not always reversible; the global prevalence of DRA is 70% in the final trimester, 60% at 6 weeks postpartum, and more than 30% at 1 year after giving birth.1 A recent study found that postpartum DRA affects 28.4% of Chinese women in the ages of 18 to 90 years (average age, 58 years).2
DRA can occur at the supraumbilical, umbilical, and sub-umbilical levels, and typically develops first at the umbilical level; however, the normal ranges of inter-recti distance (IRD) vary from site to site.3 Various approaches can be used to measure the IRD, including palpation,1,4 digital caliper,5 ultrasonography,6 and computed tomography,2 of which the palpation method is most commonly used in clinical practice.4
Although DRA has been extensively researched, the results obtained are conflicting. Some studies have found that DRA is not associated with maternal age,1,4,7 ethnicity,4 height,1,4 preconception weight,1,4 gestational weight gain,1,4 exercise habits,7 or history of abdominal surgery.4 However, other studies have reported that age,2,8,9 cesarean section,8 body mass index (BMI) before and after childbirth,8,9 and parity9 are significant risk factors for DRA. Furthermore, no specific indicators have been identified for the comprehensive evaluation of DRA. Therefore, the present study aimed to determine the physiological, psychological, and social effects of maternal DRA after childbirth by investigating several clinically relevant patient-reported outcomes (PROs) collected by administering multiple questionnaires. The objectives of this study were two-fold: (1) to identify the potential risk factors for DRA and (2) to summarize the PROs of women with postpartum DRA.
Materials and Methods
Ethics and Consent
This comparative, non-interventional, observational study was approved by the ethics committee of Hangzhou Hospital of Traditional Chinese Medicine (approval code: 2020KY082). All study procedures were performed in accordance with the Declaration of Helsinki (2008). Before formally entering the study, all subjects signed written informed consent forms. None of the subjects received any financial compensation or other benefits for participating in this study.
Sample Size Estimation
According to a previous study,1 an exercise frequency of ≥20 times/week is the main risk factor for DRA, and the probability of this exercise frequency in postpartum women without DRA is 17.5%. The bilateral test was established with an odds ratio of 2.18, an α level of 0.05, and test efficiency (1 – β) of 0.90, and a total of 2 subject groups were required for this study. Using Power Analysis and Sample Size (PASS v11.0) software (NCSS), we estimated that a sample size of 194 was required for each group. Assuming a loss to follow-up rate of 10%, we concluded that each group should be no less than 210 subjects, which yielded a total sample size of no less than 420 subjects for this study.
Inclusion and Exclusion Criteria
Women who visited the Postpartum Clinic at the Department of Acupuncture and Rehabilitation, Hangzhou Hospital of Traditional Chinese Medicine, Dingqiao District, between May 29th, 2020 and December 9th, 2022, were eligible for enrollment in this study provided they met the following inclusion criteria:10 (1) they were between the ages of 20 and 55 years; (2) they had given birth at least 42 days prior to enrollment; and (3) they were not currently undergoing and had not previously undergone treatment for DRA.
The exclusion criteria10 were suspected or diagnosed severe spinal lesions or neurological injuries (such as bone fractures, metastases, inflammatory or infectious diseases, cauda equina syndrome, and widespread neurological disorder); motor contraindications; and severe infectious diseases (such as severe cardiovascular disease and cancer).
Diagnosis of DRA
All measurements were taken with the subject lying in a supine position, with the abdomen exposed. The women were instructed to slightly flex the upper body through abdominal muscle contraction during expiration to keep the shoulder blades lifted off the bed. According to a previous study,11 DRA was diagnosed if the IRD was more than 2 cm when measured by palpation at the level of the umbilicus. Van de Water and Benjamin5 have demonstrated that this measurement method shows good intra-rater and inter-rater reliability (weighted kappa = 0.73–0.77 for test-retest reliability; weighted kappa = 0.53 for validity). In the present study, all IRD measurements were performed by a single physiotherapist (Li Sun, who has 5 years of clinical experience).
Basic Information, Risk Factors, and PROs
We collected the following demographic and clinical data from the enrolled subjects: age, days after the end of childbirth, disease history, medicine history, allergy history, education background, occupation, pelvic girdle pain (PGP), low back pain (LBP), urinary incontinence (UI), frequent urination, sexual dysfunction, and chronic pelvic pain (CPP).
Possible risk factors were selected by referring to the available literature1–4,7,12–14 and consisted of the following: maternal height, weight, weight gain during pregnancy, body mass index (BMI), number of pregnancies, number of births, number of cesarean deliveries, number of vaginal deliveries, number of gestational weeks at the time of delivery, fetal birth weight, waist circumference at the umbilical level in the supine position, hip circumference in the supine position, skinfold thickness at the umbilical level, waist-to-hip ratio (WHR, defined as the ratio of the waist circumference at the umbilical level to the hip circumference, both measured with the subject lying in a supine position), history of abdominal surgery, parity, delivery method, twin/multiple births, exercise frequency, and weight-bearing frequency. The subjects’ height, waist and hip circumferences, and left and right skinfold thicknesses at the umbilical level were recorded by physiotherapist Li Sun in the Rehabilitation Clinic.
All subjects were asked to complete the risk-factor questionnaires and PRO forms by themselves in the clinic. The information collected was summarized in the form of fill-in-the-blanks style questionnaires, scanned, and uploaded as a PDF by Ying Zhu and Lijuan Xiao. The completed questionnaires were checked by Jiayu Chen and Ting Wang, using EpiData and Excel. The following questionnaires were used.
Short-Form McGill Pain Questionnaire-2
The Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2) was used to assess LBP in the previous month during the postpartum period.15 The Chinese version of this questionnaire was developed and verified by the Pain Branch of the Chinese Medical Association, and its reliability and validity were found to be good (Cronbach α > 0.70).16 The questionnaire is divided into 3 areas: pain rating index (PRI), visual analog scale (VAS), and present pain intensity (PPI).
Short-Form International Consultation on Incontinence Questionnaire
The Short-Form International Consultation on Incontinence Questionnaire (SF-ICIQ) is an easy-to-use tool for evaluating the impact of UI on QoL. This questionnaire can be applied to patients with different etiologies and types of UI. The Chinese version of the SF-ICIQ has good stability and internal consistency, and is consistent with the results of urodynamic tests (kappa = 0.77).17 This questionnaire includes 3 scored items on UI frequency, diafiltration volume, and impact on daily life and a 4th non-scored item that evaluates UI types.
Leeds Dyspepsia Questionnaire
The Leeds Dyspepsia Questionnaire (LDQ) was modified with a 5-point system formulated by the Spleen and Stomach Disease Professional Committee of the Chinese Association of Traditional Chinese Medicine.18,19 The main symptoms of indigestion (epigastric pain, postprandial fullness and discomfort, early satiety, burning sensation in the upper abdomen, postprandial nausea, and belching) are evaluated at 4 levels.18,19 The LDQ has a sensitivity of 80% (95% confidence interval [CI]: 65–91%), a specificity of 79% (95% CI: 66–89%), and good internal consistency (kappa = 0.90).20
The 10-Item Edinburgh Postnatal Depression Scale
The 10-item Edinburgh Postnatal Depression Scale (EPDS) was compiled by Cox et al to screen for postpartum depression. This questionnaire is widely used, and has good reliability and validity.21 Guo et al revised the EPDS to align with the language and culture of the people in Mainland China; the Chinese version of the EPDS was reported to have an internal consistency of 0.76, a content validity of 0.93, and a recommended cutoff score of 9.5 points.22
Modified Body Image Scale
The original 10-item Body Image Scale was first used for women with breast cancer.23,24 This scale was modified for patients with pelvic organ prolapse by Jelovsek and Barber,25 and its Chinese version was derived by Wang Xiaoqian.26 We conducted a reliability and validity study of the Chinese version of the Modified Body Image Scale (MBIS) in 150 postpartum women (Supplement 1). The Kaiser-Meyer-Olkin value of this questionnaire was 0.897 (Cronbach α = 0.906), and the test-retest reliability was 0.841 (95% CI: 0.784–0.881).
Hernia-Related Quality-of-Life Survey
The 12-question Hernia-Related Quality-of-Life Survey (HerQles-12) is a modified version of the original HerQles,27 and was first used to evaluate disease-specific QoL by evaluating abdominal wall function.4,28–30 The Chinese version of this questionnaire came from Professor Huang Yonggang,31 and we obtained approval from Professor Huang to use the Chinese version by e-mail. Similar to the MBIS, the Chinese version of the HerQles showed a Kaiser-Meyer-Olkin value of 0.802 (Cronbach α = 0.872), and a test-retest reliability of 0.758 (95% CI: 0.681–0.819).
The 36-Item Short-Form Health Survey
The 36-item Short-Form Health Survey (SF-36) is regarded as the universal standard among QoL assessments. The total score of the SF-36 corresponds to the sum of the scores of its 8 dimensions. Zhejiang University translated the SF-36 into Chinese, and the translated version has shown good reliability and validity (Cronbach α = 0.838, Spearman-Brown coefficient = 0.828).32,33
Blinding
The evaluators of this study were blinded to the clinical group. The assessment to detect the presence of DRA was performed by a physiotherapist in a private office. The recruitment of the patients, and the collection, entry, and verification of the questionnaires were all done by other doctors and medical students, who were not in the same office as the one used for the DRA assessments. Data analysis was performed by personnel from other colleges of the same university, and was independent of the medical staff of Hangzhou Hospital of Traditional Chinese Medicine in order to ensure complete blinding with no overlap between the evaluators.
Statistical Analysis
Yan Liu and Tiantian Ye performed all the statistical analyses with the SPSS v25.0 software (SPSS Inc., Chicago, IL, USA). Continuous quantitative variables that conformed to normality were expressed as mean ± standard deviation, and skewed quantitative data were described as median and interquartile range. Continuous variables were compared using the independent-samples t-test when normally distributed and the Mann‒Whitney U-test when non-normally distributed. The chi-square test was used to analyze dichotomous qualitative data, and the appropriate χ2 and P values were selected according to the n and T values. Binary logistic regression analysis was performed to identify variables that were significantly associated with DRA. The selected variables included parameters that showed statistically significant differences in the univariate analysis and well-known clinical factors. The Spearman test was used to perform correlation analysis to determine the correlations between continuous variables and ordinal data. The Kendall test was used to determine the correlations between ordinal data. P < 0.05 was considered to indicate statistical significance.
Results
Demographic and Clinical Characteristics of the Participants
A flowchart of patient selection is shown in Figure 1. A total of 666 postpartum women met the selection criteria and participated in this study. Of them, 132 women were excluded for not completing the questionnaires; the remaining 534 women were included in this analysis. DRA was diagnosed in 417 of the 534 women (78.1%); the remaining 117 (21.9%) women did not have DRA. We found no differences in age, days after the end of childbirth, disease history, medicine history, allergy history, education background, and occupation between the DRA and non-DRA groups, which indicated good comparability of the groups at the baseline (Table 1). During the IRD measurement, no adverse events occurred in the patients.
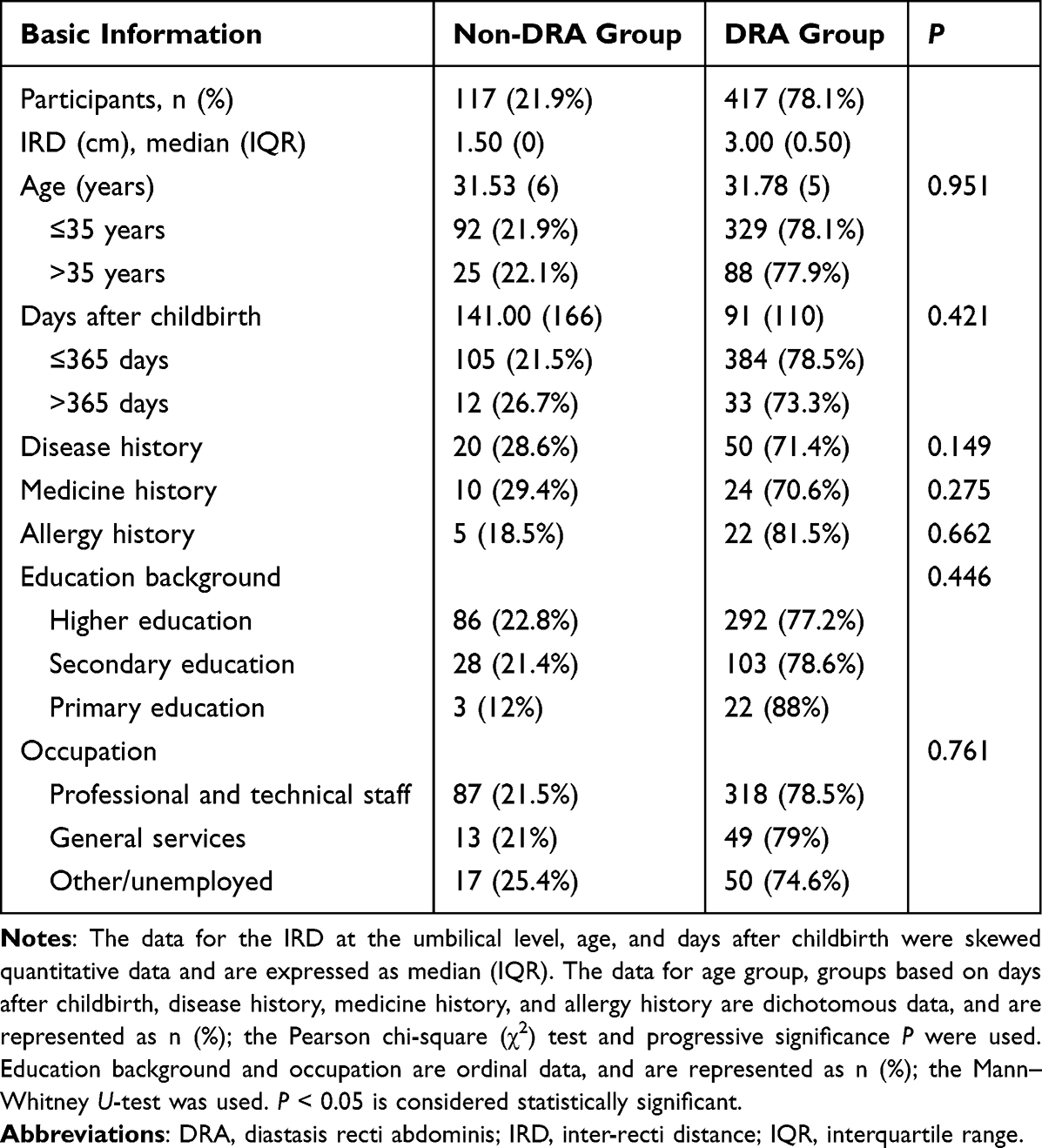 |
Table 1 Demographic and Clinical Characteristics of the Study Subjects |
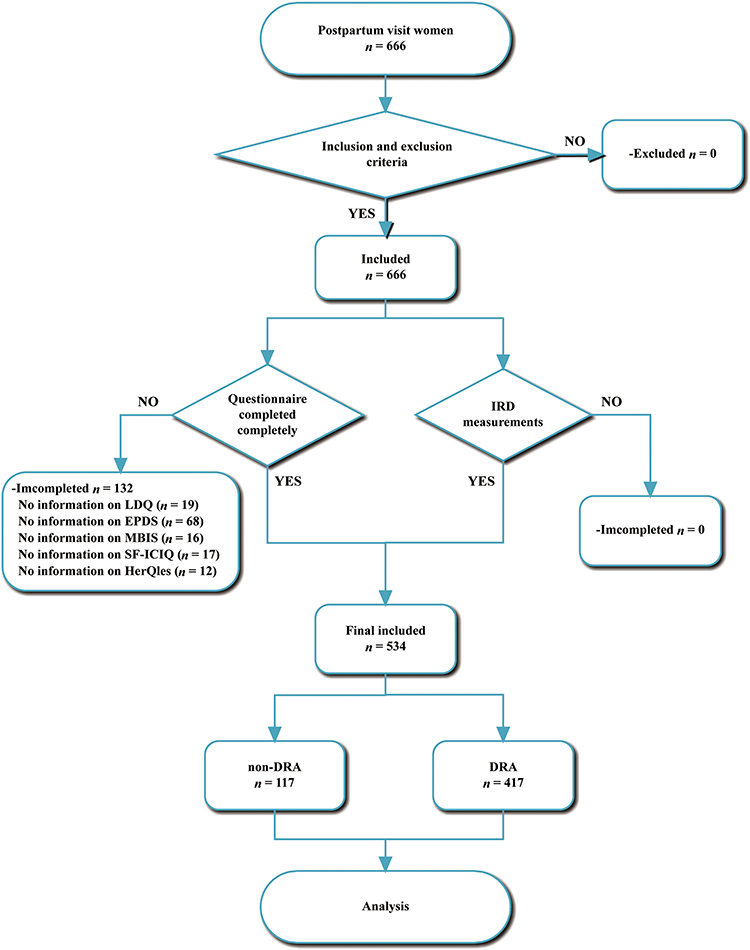 |
Figure 1 Flow chart of subject selection. |
Risk Factors
Abdominal surgery (P = 0.002), number of pregnancies (P = 0.035), parity (P = 0.012), number of births (P = 0.02), number of fetuses delivered by cesarean section (P = 0), number of vaginal births (P = 0.015), delivery mode (P = 0), fetal birth weight (P = 0.014), and WHR (P = 0.045) all significantly differed between the DRA and non-DRA groups. Exercise frequency (P = 0.058) was also a possible risk factor for DRA. Height, weight, weight gain during pregnancy, BMI, number of gestational weeks at delivery, waist circumference in the supine position, hip circumference in the supine position, skinfold thickness at the umbilical level, twin/multiple births, and weight-bearing frequency did not significantly differ between the DRA and non-DRA groups (P > 0.05; Table 2).
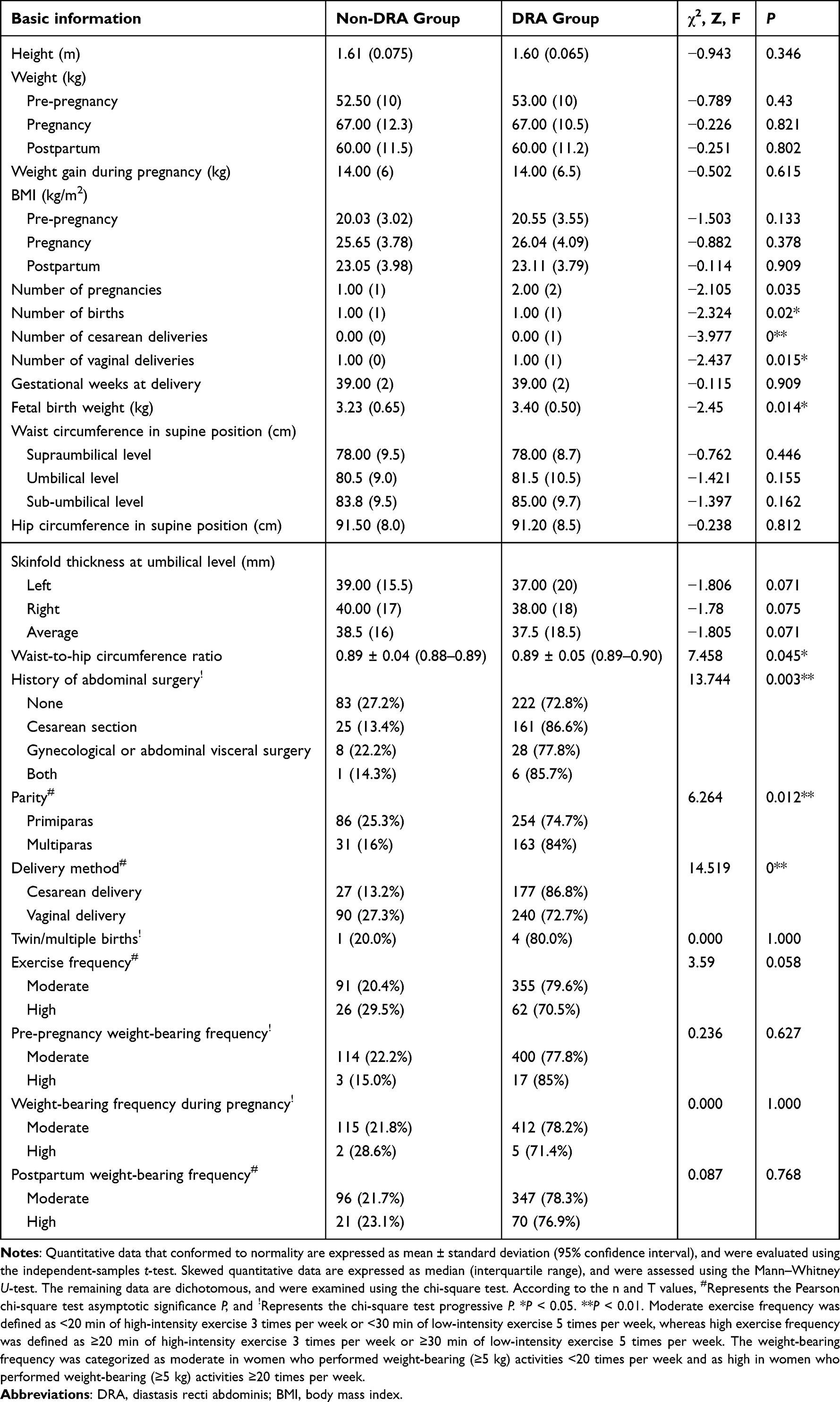 |
Table 2 Possible Risk Factors for DRA in the Study Subjects |
The Kendall rank correlation analysis showed that exercise frequency was related to postpartum weight-bearing frequency (r = 0.134, P = 0.002; Table S1 in Supplement 2).
Relationships Between DRA, Pelvic Symptoms, and LBP
Pre-Pregnancy to 42 Days Postpartum
The rate of severe PGP, which was defined as PGP that limits mobility, during pregnancy significantly differed between the DRA and non-DRA groups (P = 0.041). The rates of PGP before pregnancy and postpartum periods did not differ between the DRA and non-DRA groups (P > 0.05). The frequency of LBP did not differ between the DRA and non-DRA groups during the pre-pregnancy, pregnancy, and postpartum periods (P > 0.05). Pelvic floor symptoms, including UI, frequent urination, sexual dysfunction, and CPP, from the pregnancy to the postpartum period, did not differ between the DRA and non-DRA groups (P > 0.05; Table 3).
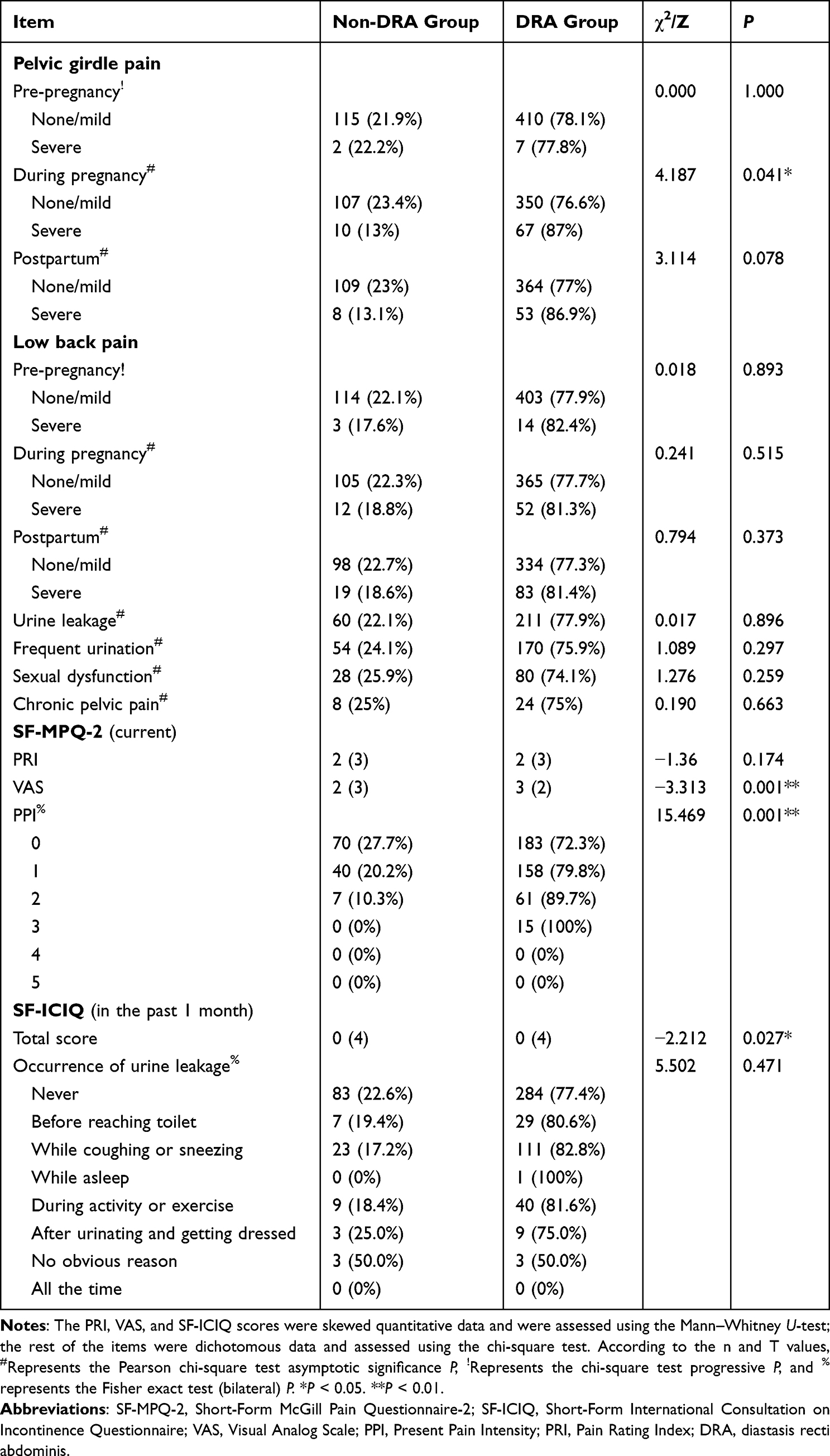 |
Table 3 Comparison of Pelvic Symptoms, Low Back Pain, and SF-MPQ-2 and SF-ICIQ Scores |
The Kendall rank correlation test showed that LBP was significantly correlated with severe PGP in the same period as well as with pelvic symptoms such as UI, frequent urination, sexual dysfunction, and CPP (0 < |r| < 0.4, P < 0.05). This suggests that severe LBP may be correlated with severe PGP during the same puerperal period and other pelvic floor symptoms (Table S2 in Supplement 2).
In the Past Month During the Postpartum Period
The SF-MPQ-2, especially the VAS, can evaluate current LBP. The VAS and PPI scores were significantly higher in the DRA group than in the non-DRA group (P < 0.05), whereas the PRI was not different (P > 0.05). This indicates that patients with postpartum DRA are more likely to have postpartum LBP. The SF-ICIQ was used to assess UI over the past month. The DRA group had higher overall scores in the 3 scored items of the SF-ICIQ (P = 0.027); in the fourth question, the occurrence of urine leakage did not significantly differ between the 2 groups (P > 0.05; Table 3).
Spearman correlation analysis of LBP and SF-ICIQ scores showed that the PRI and PPI of current LBP were significantly correlated with the SF-ICIQ scores (0.1 < |r| < 0.2, P < 0.05), which indicated a positive correlation between LBP and UI after puerperium (Table S3 in Supplement 2).
Binary Logistic Regression Model
We established a binary logistic regression model based on the risk factors that showed significant differences in the univariate analysis, the related symptoms of DRA, as well as previously considered clinical risk factors. Cesarean delivery and the PPI of the SF-MPQ-2 were found to be independent risk factors for DRA. The incidence of DRA was 2.297 times higher in women who had undergone a caesarean section than in women who had never undergone a caesarean section, and the probability of DRA increased by 0.455 times for each increment in the PPI score for LBP (Table 4).
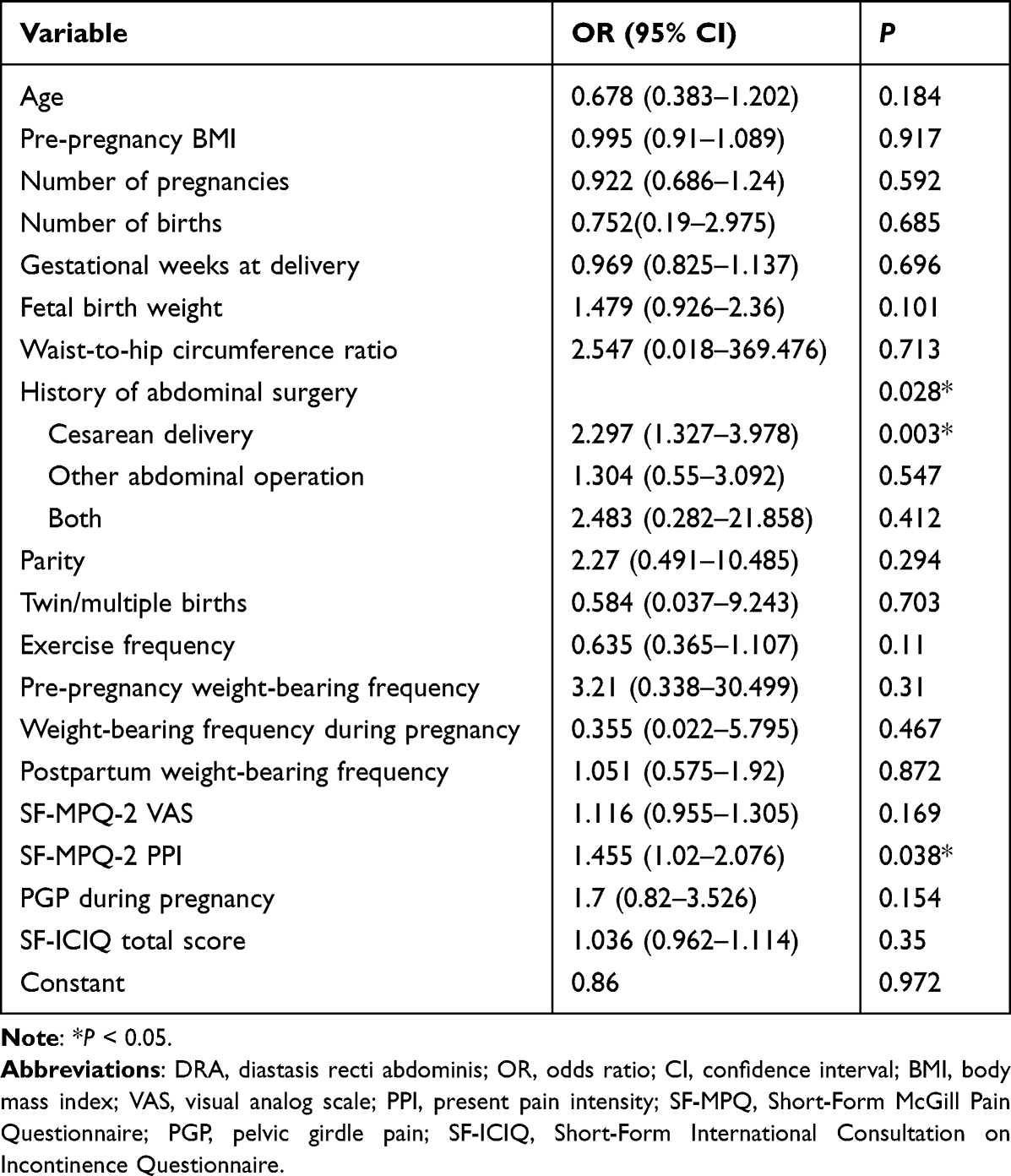 |
Table 4 Binary Logistic Regression Model for DRA |
Other PROs
Among the PROs, higher scores on the MBIS, HerQles, LDQ, and EPDS and lower scores on the SF-36 indicated more severe symptoms. The MBIS and HerQles scores were significantly higher in the DRA group than in the non-DRA group (P < 0.05). Compared to the women without DRA, those with DRA had worse scores in the self-image and abdominal wall function assessments. Regarding QoL, every dimension score of the SF-36 was lower in the DRA group than in the non-DRA group, and the scores in the Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), Vitality (VT), and Health Transition (HT) subscales were significantly lower in the DRA group than in non-DRA group (P < 0.05). The LDQ and EPDS scores did not differ between the 2 groups, indicating that there were no between-group differences in gastrointestinal symptoms and postpartum depression, respectively (Table 5).
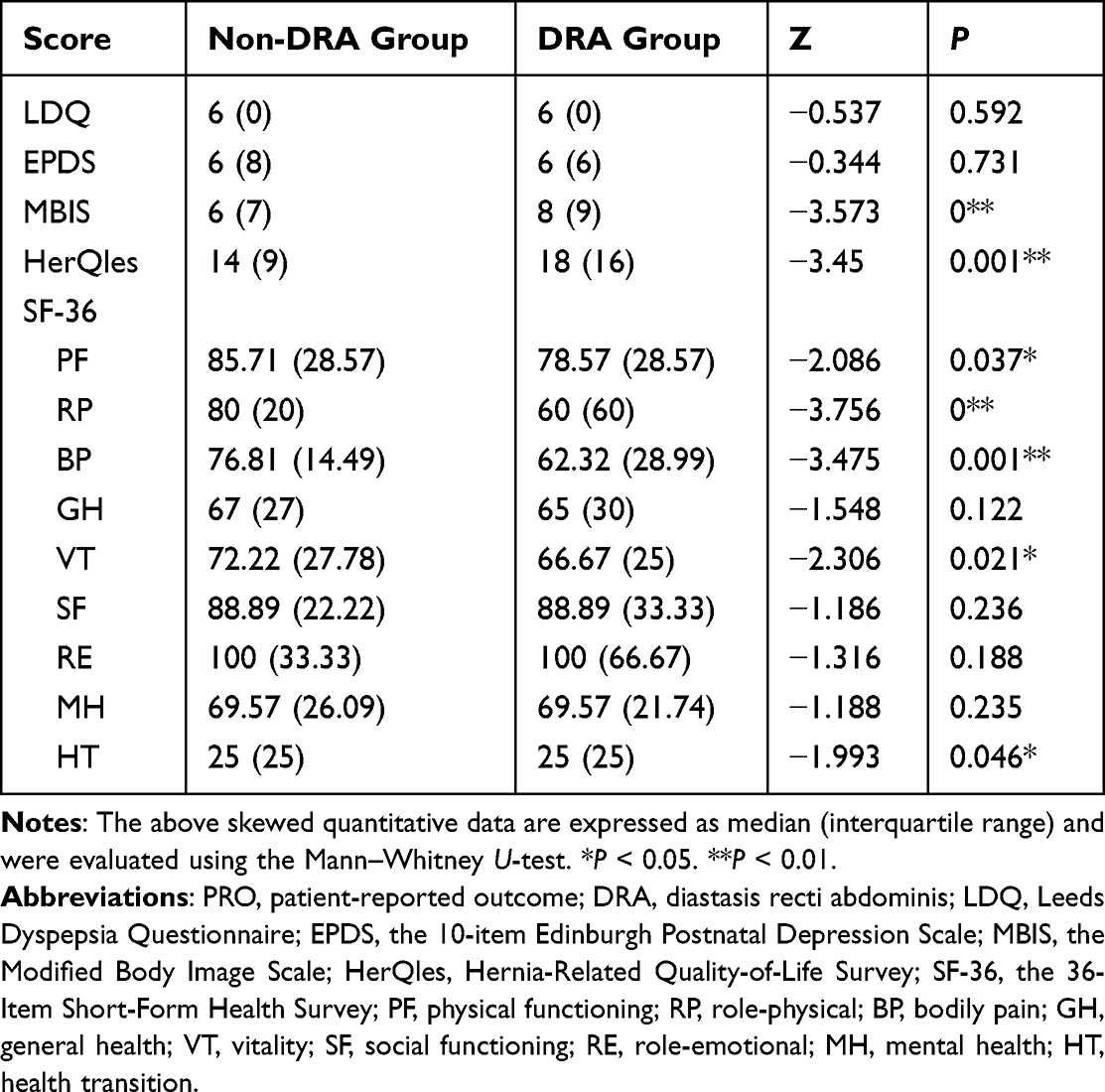 |
Table 5 Comparison of PROs of DRA |
The Spearman correlation test showed that the PF, RP, and BP subscale scores were moderately related (0.4 < |r| < 0.6, P < 0.05) with each other, and the VT, Role-Emotional (RE), Social Functioning (SF), and Mental Health (MH) subscale scores were strongly associated with each other (0.4 < |r| < 0.8, P < 0.05). The VT score was correlated with the PF, RP, and BP scores (0 < |r| < 0.2, P < 0.05). Similarly, the HT score was correlated with the PF, RP, and BP scores (0.3 < |r| < 0.4, P < 0.05). The LDQ score was negatively correlated with the PF, RP, BP, and VT scores (0 < |r| < 0.2, P < 0.05), and the EPDS and MBIS scores were negatively correlated with the PF, RP, BP, and HT scores (0.2 < |r| < 0.4, P < 0.05). The HerQles score was correlated with the PF, RP, BP, and HT scores on the SF-36 (0.2 < |r| < 0.6, P < 0.05). In addition, the LDQ, EPDS, MBIS, and HerQles scores were all correlated with each other (0.2 < |r| < 0.6, P < 0.05). These associations showed that postpartum abdominal wall function mildly affected self-image and physiological functional activity, and negatively impacted digestion, depression, and QoL. The PRI and VAS scores for current LBP were correlated with the PF, RP, BP, and HT scores of the SF-36 as well as with the LDQ, EPDS, MBIS, and HerQles scores (0.2 < |r| < 0.6, P < 0.05). The SF-ICIQ score was not correlated with the SF-36 scores, but was correlated with the MBIS and HerQles scores (0 < |r| < 0.2, P < 0.05; Table S3 in Supplement 2).
Discussion
To the best of our knowledge, this is the first study to investigate the risk factors for DRA and its related PROs in China. The study showed that compared to women without DRA, women with DRA had poorer abdominal wall function, self-image perception, and QoL. It also showed that DRA is closely associated with severe PGP during pregnancy, severe LBP, and urinary leakage during the postpartum period.
Consistent with earlier studies, we discovered that abdominal surgery,14 number of pregnancies,2,12,13 parity,12,13 number of births,12 fetal birth weight,8 and WHR were risk factors for DRA. Interestingly, we observed that in some women, the waist and hip circumferences changed due to gravity after switching from a supine to a standing position. Therefore, we suggest that postural differences in the waist and hip circumferences be investigated in future studies.
As univariate analysis does not account for confounding factors, we conducted a binary regression analysis, which yielded results that were consistent with those of previous studies;1,12 however, we found a greater effect of cesarean delivery on DRA and a less pronounced effect of other abdominal procedures. The PPI for LBP was closely correlated with DRA in this study, which has not been reported previously.
According to the findings of our study, the imbalance in the myofascial stress of the anterior abdominal wall caused by DRA can change the overall abdominal fascial tone. Without intervention, the process of normalization of the abdominal wall myofascial tone may fail or take longer than expected in some DRA patients. Therefore, we recommend that DRA should be promptly managed.
Using a previously reported cutoff for exercise frequency,1 we found that women who performed moderate-intensity general exercises had a lower incidence of DRA (14.9%), demonstrating that maintaining a regular exercise routine is advantageous. However, we found no increase in the likelihood of postpartum DRA in women who performed weight-bearing activities (≥5 kg) ≥20 times per week, which might be related to recall bias.
Women with DRA were more likely to experience severe PGP during pregnancy, and had higher VAS and PPI scores, which is consistent with a previous study.34 Thus, the incidence of these types of pain during pregnancy may indicate a higher risk of postpartum DRA. Our study demonstrated a limited but positive correlation between severe painful diseases and other PFD symptoms from pre-pregnancy to the postpartum period. We also discovered that LBP was more likely to be physiologically triggered and was closely related to the psychological subscales in the QoL assessment. In addition, the VAS score, unlike the PPI and PRI subtotals for painful diseases, could more subjectively indicate the degree of pain and distress in patients. Unfortunately, we did not conduct real-time monitoring and could not observe dynamic changes in the PROs.
PFD is common in the postpartum period, and thus far, there is no consensus over whether DRA is related to PFD.8 Given the timelines of the PRO questionnaires, we gathered descriptions of symptoms from preconception to 1 month postpartum, and analyzed PROs from the past month to the present postpartum period. Our findings showed that DRA patients had higher SF-ICIQ scores, supporting the abdominal tank theory about abdominal and pelvic floor coordination and unity.35 Correlation analysis showed an association between pain and other pelvic floor symptoms, which is consistent with previous results.36
Our results indicated that DRA was unlikely to lead to a digestive tract response. Functional dyspepsia is associated with diaphragm contraction and anterior abdominal wall protrusion. One study37 has demonstrated that the muscle contraction strongly affected the intra-abdominal oblique muscles (P = 0.037) and not the rectus abdominis muscles (P = 0.140–0.695). Our results showed no correlation between the SF-ICIQ and LDQ scores (r = −0.001, P = 0.977), which is consistent with a previous report that PFD is not associated with dietary irregularities.38
To verify that DRA harms the abdominal, physical, and mental health of postpartum women, we investigated the applicability of MBIS and HerQles among 150 postpartum women (Supplement 1). We found that the DRA group showed current PROs (MBIS and HerQles) that were comparable to those in the non-DRA group, which is consistent with an earlier study.4 Furthermore, the PF, RP, BP, VT, and HT scores of the SF-36 indicated that the mental and psychological effects were greater in the DRA group than in the non-DRA group, which is consistent with previous studies.33 We also performed a correlation analysis of these PROs, and the results showed that most aspects of the SF-36 were correlated with each other. Since other physical discomforts may accompany DRA, we analyzed the MBIS and HerQles scores, which were moderately associated with which each other.39 Among the remaining PROs, we observed correlations between low back pain, digestion, abdominal function, UI, psychological symptoms, and physiological factors (PF, RP, BP, and VT; Table S3 in Supplement 2). Digestion (LDQ score) was strongly correlated with physiological factors (PF, RP, BP, and VT); abdominal function (HerQles score) was strongly correlated with physiological factors (PF, RP, and BP), digestion (LDQ score), and emotion (EPDS and HT scores); and UI (SF-ICIQ score) was strongly correlated with self-image (MBIS score) and low back pain (SF-MPQ PRI and PPI). These findings serve as reminders that despite the theory that the body returns to its pre-pregnancy state after puerperium, numerous physiological issues and discomforts continue to have an impact on the mental and physical well-being of women long after puerperium.
In this study, we identified the risk factors associated with postpartum DRA, analyzed its symptoms, and clarified the relationships between PROs. Our findings support the assessment of low body image satisfaction and are in line with those of previous studies. This research study shows that it is critical to increase the awareness of DRA and educate people about DRA-related symptoms, particularly in light of the introduction of the three-child policy in the Chinese mainland. The prevention of DRA and the examination, treatment, and management of DRA and its related symptoms should be urgently improved for the sake of the well-being of women who are planning to become pregnant and those in the postpartum period.
Strengths and Limitations
To the best of our knowledge, this is the first study to investigate multi-dimensional PROs in Chinese postpartum women. The limitations of this study are as follows: (1) The questionnaires were very long, and the respondent needed to be patient. The answers to some questions needed to be recalled by the patient, which took a long time. (2) Although the IRD measurements were straightforward and performed by a trained professional, their accuracy was not as high as that of objective instruments, so we recommend the use of ultrasonography for more accurate measurements. In addition, the measurements can be evaluated in multiple postures, such as the standing and supine positions. (3) Some information, such as weight-bearing, was not very accurate, and we need to improve the data on weight-bearing type, duration, and frequency. (4) Some indicators (eg, time since delivery) were evaluated in a time-sensitive manner, but subsequent assessments of the same symptoms need to be uniform. (5) The study was conducted during the COVID-19 pandemic, and was subject to the associated limitations of collecting population-based information. The non-DRA group consisted of less than 210 subjects. We had no follow-up with the participants, and the number of days after delivery recorded in this study was inconsistent. To collect accurate information, it is necessary to optimize data-collection methods and better collaborate with sonologists and other investigators.
Conclusion
The prevalence of DRA is as high as 78.1%. Risk factors for DRA include abdominal surgery, number of pregnancies, parity, number of births, fetal birth weight, WHR, and exercise frequency. Caesarean delivery is an independent risk factor for DRA. Women with DRA are more likely to experience physical limitations, have lower self-image scores, poor abdominal wall functioning, and decreased QoL, especially psychological QoL.
Abbreviations
DRA, Diastasis recti abdominis; PROs, patient-reported outcomes; SF-MPQ-2, Short-Form McGill Pain Questionnaire-2; SF-ICIQ, Short-Form International Consultation on Incontinence Questionnaire; LDQ, Leeds Dyspepsia Questionnaire; EPDS, 10-item Edinburgh Postnatal Depression Scale; MBIS, Modified Body Image Scale; HerQles, Hernia-Related Quality-of-Life Survey; SF-36, 36-Item Short-Form Health Survey; IRD, inter-recti distance; PGP, pelvic girdle pain; VAS, visual analog scale; PPI, present pain intensity; PF, physical functioning, RP, role-physical; BP, bodily pain; VT, vitality; HT, health transition; QoL, quality of life; BMI, body mass index; LBP, low back pain; PFD, pelvic floor dysfunction; UI, urinary incontinence; CPP, chronic pelvic pain; PRI, pain rating index; WHR, waist-to-hip ratio.
Adverse Events Reporting and Safety Monitoring
During the IRD measurements, no adverse events or side effects, such as falls or joint sprains, occurred.
Data Sharing Statement
All data have been uploaded as supplements materials.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of Hangzhou Hospital of Traditional Chinese Medicine (approval code: 2020KY082). All study procedures were in accordance with the tenets of the Declaration of Helsinki (2008). Before formally entering the study, all subjects signed written informed consent forms.
Acknowledgments
We thank Dr. Yonggang Huang from the Department of Hernia and Abdominal Surgery, Hangzhou First People’s Hospital, Zhejiang University School of Medicine, who provided the Chinese version of the HerQles form. We thank Medjaden Inc. for its assistance in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Zhejiang Traditional Chinese Medicine Science and Technology Plan Project (project number: 2021ZQ065), Hangzhou Medical and Health Science and Technology (project number: A20200483), and Medical Scientific Research Foundation of Zhejiang Province, China (grant number: 2024KY1383).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, K B. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. 2016;50(17):1092–1096. doi:10.1136/bjsports-2016-096065
2. Wu L, Gu Y, Gu Y, et al. Diastasis recti abdominis in adult women based on abdominal computed tomography imaging: prevalence, risk factors and its impact on life. J Clin Nurs. 2021;30(3–4):518–527. doi:10.1111/jocn.15568
3. Mota P, Pascoal AG, Carita AI, Bo K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskelet Sci Pract. 2018;35:34–37. doi:10.1016/j.msksp.2018.02.004
4. Cardaillac C, Vieillefosse S, Oppenheimer A, Joueidi Y, Thubert T, Deffieux X. Diastasis of the rectus abdominis muscles in postpartum: concordance of patient and clinician evaluations, prevalence, associated pelvic floor symptoms and quality of life. Eur J Obstet Gynecol Reprod Biol. 2020;252:228–232. doi:10.1016/j.ejogrb.2020.06.038
5. van de Water AT, Benjamin DR. Measurement methods to assess diastasis of the rectus abdominis muscle (DRAM): a systematic review of their measurement properties and meta-analytic reliability generalisation. Man Ther. 2016;21:41–53. doi:10.1016/j.math.2015.09.013
6. Qu E, Wu J, Zhang M, et al. The ultrasound diagnostic criteria for diastasis recti and its correlation with pelvic floor dysfunction in early postpartum women. Quant Imaging Med Surg. 2021;11(2):706–713. doi:10.21037/qims-20-596
7. da Mota PG F, Pascoal AG, Carita AI, K B. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015;20(1):200–205. doi:10.1016/j.math.2014.09.002
8. Wang Q, Yu X, Chen G, Sun X, Wang J. Does diastasis recti abdominis weaken pelvic floor function? A cross-sectional study. Int Urogynecol J. 2020;31(2):277–283. doi:10.1007/s00192-019-04005-9
9. Kaufmann RL, Reiner CS, Dietz UA, Clavien PA, Vonlanthen R, Käser SA. Normal width of the linea alba, prevalence, and risk factors for diastasis recti abdominis in adults, a cross-sectional study. Hernia. 2021;26(2):609–618. doi:10.1007/s10029-021-02493-7
10. Liu Y, Zhu Y, Jiang L, et al. Efficacy of electro-acupuncture in postpartum with diastasis recti abdominis: a randomized controlled clinical trial. Front Public Health. 2022;10:1003361–1003391. doi:10.3389/fpubh.2022.1003361
11. Manetti G, Lolli MG, Belloni E, Nigri G. A new minimally invasive technique for the repair of diastasis recti: a pilot study. Surg Endosc. 2021;35(7):4028–4034. doi:10.1007/s00464-021-08393-2
12. Cavalli M, Aiolfi A, Bruni PG, et al. Prevalence and risk factors for diastasis recti abdominis: a review and proposal of a new anatomical variation. Hernia. 2021;25(4):883–890. doi:10.1007/s10029-021-02468-8
13. Liaw LJ, Hsu MJ, Liao CF, Liu MF, Hsu AT. The relationships between inter-recti distance measured by ultrasound imaging and abdominal muscle function in postpartum women: a 6-month follow-up study. J Orthop Sports Phys Ther. 2011;41(6):435–443. doi:10.2519/jospt.2011.3507
14. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(3):321–328. doi:10.1007/s00192-006-0143-5
15. Melzack R, Bélanger E. Labour pain: correlations with menstrual pain and acute low-back pain before and during pregnancy. Pain. 1989;36(2):225–229. doi:10.1016/0304-3959(89)90027-4
16. Li J, Feng Y, Han J, et al. Multi-centered linguistic adaptation and validation of short-form McGill pain questionnaire-2. Chin J Pain Med. 2013;19(01):42–46. doi:10.3969/j.issn.1006-9852.2013.01.014
17. Zebo C, Yongqing L, Qunduo C, Shuolei S, Bentao S, Zhizhen G. The relevance study of Chinese short form of international consultation on Incontinence questionnaire(ICIQ-SF) and urodynamics. J Modern Urology. 2011;16(05):403–405.
18. Zhang S, Wang H, Li Q. Functional Dyspepsia TCM Diagnosis and Treatment Specifications. Chin J Int Tradit West Med Dig. 2002;4:194.
19. Xiaoyu Z. Guidelines for clinical research of new Chinese medicine drugs (Trial). In: Beijing: Traditional Chinese Medicine Pharm Press. World Scientific; 2002:1397.
20. Moayyedi P, Duffett S, Braunholtz D, et al. The leeds dyspepsia questionnaire: a valid tool for measuring the presence and severity of dyspepsia. Aliment Pharm Ther. 1998;12(12):1257–1262. doi:10.1046/j.1365-2036.1998.00404.x
21. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psych. 1987;150(6):782–786. doi:10.1192/bjp.150.6.782
22. Xiujing G, Yuqiong W, Ying L, Jing C, Xiaofen P. Study on the optimal critical value of the Edinburgh postnatal depression scale in the screening of antenatal depression. Chin J Nurs. 2009;44(09):808–810.
23. Hopwood P. The assessment of body image in cancer patients. Eur J Cancer. 1993;29a(2):276–281. doi:10.1016/0959-8049(93)90193-j
24. Bhattacharya IS, Haviland JS, Kirby AM, et al. Patient-reported outcomes over 5 years after whole- or partial-breast radiotherapy: longitudinal analysis of the IMPORT LOW (CRUK/06/003) Phase III randomized controlled trial. J Clin Oncol. 2019;37(4):305–317. doi:10.1200/jco.18.00982
25. Jelovsek JE, Barber MD. Women seeking treatment for advanced pelvic organ prolapse have decreased body image and quality of life. Am J Obstet Gynecol. 2006;194(5):1455–1461. doi:10.1016/j.ajog.2006.01.060
26. Wang X Reliablity and Validity Of The Chinese Version Of The Mbis, I-Qol And Ufs-Hrql In Patients with POP, Urinary Incontinence And Uterine Fibroid. [doctoral thesis]. Peking Union Medical College; 2013.
27. Krpata DM, Schmotzer BJ, Flocke S, et al. Design and initial implementation of HerQLes: a hernia-related quality-of-life survey to assess abdominal wall function. J Am Coll Surg. 2012;215(5):635–642. doi:10.1016/j.jamcollsurg.2012.06.412
28. Patel V, Cunning JR, Rios-Diaz AJ, et al. Prospective assessment of the abdominal hernia-Q (AHQ)-patient burden, reliability, and longitudinal assessment of quality of life in hernia repair. Ann Surg. 2020;276:1039–1046. doi:10.1097/sla.0000000000004713
29. Nissen AT, Henn D, Moshrefi S, Gupta D, Nazerali R, Lee GK. Health-related quality of life after ventral hernia repair with biologic and synthetic mesh. Ann Plast Surg. 2019;82(5S Suppl 4):332–338. doi:10.1097/sap.0000000000001768
30. Hutchison CE, Rhemtulla IA, Mauch JT, et al. Cutting through the fat: a retrospective analysis of clinical outcomes, cost, and quality of life with the addition of panniculectomy to ventral hernia repair in overweight patients. Hernia. 2019;23(5):969–977. doi:10.1007/s10029-019-02024-5
31. Huang Y, Ye J, Zhang F, et al. Application value of obliquus externus abdominis pedicle flap graft technique in repair of giant abdominal incisional hernia. Chin J Dig Sur. 2020;19(07):757–761. doi:10.3760/cma.j.cn115610-20200516-00358
32. Ren XS, Amick B, Zhou L, Gandek B. Translation and psychometric evaluation of a Chinese version of the SF-36 health survey in the United States. J Clin Epidemiol. 1998;51(11):1129–1138. doi:10.1016/s0895-4356(98)00104-8
33. Li L. Chinese SF-36 Health Survey: translation, cultural adaptation, validation, and normalisation. J Epidemiol Community Health. 2003;57(4):259–263. doi:10.1136/jech.57.4.259
34. Yuan S, Wang H, Zhou J. Prevalence and risk factors of low back and pelvic pain in women with rectus abdominis diastasis: a multicenter retrospective cohort study. Korean J Pain. 2022;35(1):86–96. doi:10.3344/kjp.2022.35.1.86
35. Lee D, Hodges PW. Behavior of the linea alba during a curl-up task in diastasis rectus abdominis: an observational study. J Orthop Sports Phys Ther. 2016;46(7):580–589. doi:10.2519/jospt.2016.6536
36. Yi J, Tenfelde S, Tell D, Brincat C, Fitzgerald C. Triathlete risk of pelvic floor disorders, pelvic girdle pain, and female athlete triad. Female Pelvic Med Reconstr Surg. 2016;22(5):373–376. doi:10.1097/spv.0000000000000296
37. Burri E, Barba E, Huaman JW, et al. Mechanisms of postprandial abdominal bloating and distension in functional dyspepsia. Gut. 2014;63(3):395–400. doi:10.1136/gutjnl-2013-304574
38. Starzec-Proserpio M, Rejano-Campo M, Szymańska A, Szymański J, Baranowska B. The association between postpartum pelvic girdle pain and pelvic floor muscle function, diastasis recti and psychological factors-a matched case-control study. Int J Environ Res Public Health. 2022;19(10):6236–6251. doi:10.3390/ijerph19106236
39. Fuentes Aparicio L, Rejano-Campo M, Donnelly GM, Vicente-Campos V. Self-reported symptoms in women with diastasis rectus abdominis: a systematic review. J Gynecol Obstet Hum Reprod. 2021;50(7):101995–102027. doi:10.1016/j.jogoh.2020.101995
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.