")
Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Request for Antimalarial Medicines and Their Dispensing Without a Prescription in Community Pharmacies in Rwanda
Authors Nsengimana A , Biracyaza E , Isimbi J, Uwambajimana C, Hategekimana JC , Kagisha V, Asingizwe D, Nyandwi JB
Received 29 June 2023
Accepted for publication 20 October 2023
Published 31 October 2023 Volume 2023:12 Pages 195—212
DOI https://doi.org/10.2147/IPRP.S428105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Walid Al-Qerem
Amon Nsengimana,1 Emmanuel Biracyaza,2,3 Joyce Isimbi,4 Charles Uwambajimana,4 Jean Claude Hategekimana,4 Vedaste Kagisha,4 Domina Asingizwe,5,6 Jean Baptiste Nyandwi4,6
1US Agency for International Development Global Health Supply Chain Program, Procurement and Supply Chain Management, Kigali, Rwanda; 2School of Rehabilitation, Faculty of Medicine, Université de Montréal, Québec, Canada; 3Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR), Montreal, Canada; 4Department of Pharmacy, University of Rwanda, Kigali, Rwanda; 5Department of Physiotherapy; University of Rwanda, Kigali, Rwanda; 6East African Community Regional Centre of Excellence for Vaccines, Immunization and Health Supply Chain Management, University of Rwanda, Kigali, Rwanda
Correspondence: Amon Nsengimana, Email [email protected]
Purpose: This study aimed to explore the request and dispensing of antimalarial medicines without a prescription in community pharmacies in Rwanda, as well as factors associated.
Methods: We employed an embedded mixed-methods design that involved a convenience sample of 235 licensed community pharmacists between February and April 2022. To simultaneously collect qualitative and quantitative data, we used a self-administered questionnaire containing a combination of close and open-ended questions. Bivariate and multivariate regression analyses were performed to examine the relationship between dispensing antimalarial medicines without a prescription and the selected independent variables. Statistical significance was set at p< 0.05, and a 95% confidence interval was applied. The factors influencing the dispensing of antimalarial medicines without a prescription were analyzed using thematic content analysis as a qualitative analysis approach.
Results: Most respondents (88.5%) were asked to dispense antimalarial medicines by clients without a prescription. More than half of them (54%) agreed, but 34.5% refused; instead, they referred clients to malaria diagnostic testing facilities. Those who had rapid diagnostic tests for malaria in stock (OR=2.08, 95% CI:1.1– 3.94), and thought that antimalarials were over-the-counter medicines (OR=7.03, 95% CI:2.01– 24.5) were more likely to dispense antimalarial medicines without prescriptions. The primary reasons reported by community pharmacists for dispensing antimalarial medicines without prescriptions included their prior knowledge of malaria diagnosis, client pressure, and fear of losing clients. However, non-adherence to negative results obtained from formal health facilities and long queues at these institutions have also been cited as additional factors driving clients to seek antimalarial medicines without prescriptions.
Conclusion: Dispensing antimalarial medicines without prescriptions is a common practice in community pharmacies in Rwanda. The main factors contributing to this practice include lack of awareness regarding the classification of antimalarials as prescription medicines, the availability of malaria diagnostic tests, client pressure, and fear of losing clients.
Keywords: request, antimalarial medicines, dispensing, community pharmacies, Rwanda
Introduction
In 2021, the World Health Organization (WHO) reported 247 million cases and 619 thousand deaths due to malaria.1 The global public health threat posed by this communicable disease is most prominent in Africa, with 234 million cases, accounting for about 95% of global cases in 2021.1,2 Of particular concern, only four countries, namely Nigeria, the Democratic Republic of Congo, Uganda, and Mozambique, accounted for almost half of all reported cases worldwide, while more than 50% of all malaria deaths occurred in Nigeria, the Democratic Republic of Congo, Niger, and the United Republic of Tanzania.1 Rwanda like any other African country, malaria remains one of its foremost public health problems.1–3 In Rwanda and most Sub-Saharan African (SSA) countries, plasmodium falciparum malaria remains the leading cause of malaria cases and deaths.1,4
Before the emergence of molecular markers indicating resistance to chloroquine was detected in 2001, the first-line treatment for uncomplicated falciparum malaria in SSA involved the administration of chloroquine.4 Since then, countries in which P. falciparum malaria was endemic have updated their treatment policy from the use of monotherapy with drugs such as chloroquine to artemisinin-based combination therapies (ACTs).5,6 These ACTs are now the WHO recommended first-line treatment to address resistance to monotherapies.5–7 They continue to exhibit effectiveness in most regions with high malaria prevalence.1,8 Rwanda has also adopted ACTs, specifically Artemether + Lumefantrine, as the preferred initial treatment option for uncomplicated malaria.9
In SSA, community pharmacies remain the key providers of malaria treatment,10,11 with a significant market share of antimalarial sales volume ranging from 33% to 95%.12 For instance, half of all antimalarial medicines in Uganda are distributed through private drug stores.13 In Tanzania, a study reported that 21% of clients in community pharmacies sought malaria treatment.14 Such treatment-seeking behaviors in community pharmacies are common because public health facilities in SSA face frequent stock-outs of essential medicines including antimalarials.15 However, in Ghana, 73% of clients chose community pharmacies because they were close to their households.16 Recognizing the importance of community pharmacies in malaria diagnosis and treatment, the WHO has recommended strengthening their role.17
As in the public health sector, the WHO recommends that for all suspected malaria cases, a parasitological test (microscopy or rapid diagnostic test) should be performed to confirm the diagnosis.5 However, many community pharmacies in SSA do not traditionally provide diagnostic services, potentially leading to overtreatment with antimalarial medicines, unnecessary potential side effects, incorrect treatment of non-malaria fever, and the emergence of antimalarial drug resistance.18,19 Across SSA, the rate between presumptive and actual parasitological malaria cases has been estimated to range from 10% to 60%.2
Anti-malarial drug resistance is a significant global concern.20 Notably, in Africa, Rwanda’s confirmation of artemisinin partial resistance is alarming.20,21 While the causes and development of antimalarial drug resistance are complex and multifaceted, dispensing antimalarials without malaria confirmation is among the main contributing factors.22 Regrettably, little is known about the magnitude of requests for antimalarial medicines and their dispensing without a prescription in community pharmacies in Rwanda. To address this research gap, this study aimed to explore the request and dispensing of antimalarial medicines without a prescription in community pharmacies across Rwanda and the possible contributing factors.
In malaria-endemic countries, because the scope of pharmacy practice differs from one country to another, regulations on over-the-counter (OTC) antimalarial dispensing also differ.23 For instance, while community pharmacists in the same region as Kenya can sell antimalarial medicines after performing malaria rapid diagnostic tests (m-RDTs),22 this is not yet allowed in Rwanda; thus, antimalarials remain prescription medicines. On the other hand, studies have shown that in countries where malaria diagnostic services in community pharmacies are restricted, antimalarial medicines are often dispensed without a prescription, increasing the risk of antimalarial drug resistance.2,18,22 Therefore, this study is considered important because the findings will inform policymakers and healthcare providers about the extent of antimalarial medicines being dispensed without a prescription and the contributing factors to be addressed in their strategies. This information can be used to develop interventions and policies to improve the appropriate use of antimalarial medicines and to reduce the risk of drug resistance. It can also inform strategies for strengthening the regulation and oversight of community pharmacies to ensure safe and effective use of antimalarial medicines.
Methods
Study Design
This was an embedded mixed methods study that was carried out between February 11, 2022, and April 1, 2022, among 235 licensed community pharmacists in Rwanda. This study simultaneously compared the findings of quantitative and qualitative methods to determine their mutual confirmation or contradiction. Furthermore, by triangulating the results obtained from both quantitative and qualitative analyses, this study aimed to gain a comprehensive understanding of this research phenomenon.
Settings, and Population
This study was conducted in Rwanda, a landlocked country in East-Central Africa. Rwanda is divided into four administrative provinces (East, West, South, and North), plus the capital city called Kigali. With a population of 13.2 million people in 2022, Rwanda is a relatively small nation often referred to as “The Land of a Thousand Hills”.3 The Rwandan pharmaceutical workforce consists of pharmacists and pharmacy technicians. Most pharmacists work in the private sector, particularly community pharmacies, whereas only 39% work in the public health sector.24 The private sector mainly encompasses wholesale and community pharmacies. Pharmacy is a regulated profession in Rwanda, and the Rwanda Food and Drugs Authority (Rwanda FDA) grants approval for the operation of a community pharmacy upon presentation of a licensed and registered pharmacist by the Rwanda National Pharmacy Council (NPC). Throughout the study period, 612 community pharmacies across the country were Rwanda FDA licensed.25
Sample Size
The researchers obtained a list of licensed community pharmacies from the Rwanda FDA, indicating that there were 612 licensed community pharmacies during the study period. The sample size for the study was determined using Yamane’s formula ( ),26 which considers the population size (N), desired confidence interval (e = 0.05) at a 95% confidence level, and sample size (nY). Using the aforementioned formula, the sample size was calculated as
),26 which considers the population size (N), desired confidence interval (e = 0.05) at a 95% confidence level, and sample size (nY). Using the aforementioned formula, the sample size was calculated as

The resulting sample size of 242 licensed community pharmacists was selected across the country using a convenience sampling method. The study included all licensed community pharmacists employed in community pharmacies. However, unlicensed pharmacists and those who chose not to participate voluntarily were excluded. Out of the 242 community pharmacists who met the eligibility criteria, 235 (equivalent to 97%) filled the self-administered questionnaire. The first fifteen participants who consented to take part in this quantitative part were additionally invited to participate in the qualitative part. As a result, eleven of them agreed. Nonetheless, the final sample size was reduced to nine participants because no novel themes or insights emerged after the eighth participant.
Data Collection and Research Instruments
Five data collectors, all holding bachelor’s Degrees in pharmacy, before commencing data collection, they underwent a two-day initiation training that focused on the topic guide for semi-structured methods, embedded study designs, data collections tools and participant protection. They collected data under supervision from the first and second authors. For the qualitative part, two data collectors who had different responsibilities conducted the semi-structured interview. One data collector was to interview whereas the other had to take notes and audio-recording. Qualitative data were collected using the local language (Kinyarwanda). Each semi-structured interview lasted 21 to 33 minutes.
In Rwanda, it is mandatory for a community pharmacy to have a premise license displayed within the pharmacy, along with the name of the licensed pharmacist responsible for managing the pharmacy. Consequently, the pharmacist’s name listed on the premise license was used to identify participating licensed pharmacists. Eligible pharmacists were selected via convenience sampling. Data collection utilized a semi-structured questionnaire that included both open-ended questions for the qualitative phase and close-ended questions for the quantitative phase. Participants were conveniently recruited from their workplaces, and those who agreed to take part were immediately given the questionnaires. The questionnaire was designed to explore the prevalence and factors influencing the dispensing of antimalarial medicines without a prescription among community pharmacists. The questionnaire encompassed four main sections: (a) Socio-demographic characteristics (gender, age, education, marital status) and information about the pharmacy/pharmacist (level of education, year of graduation, pharmacy ownership, location, working experience, availability of other healthcare professionals); (b) Request and dispensing of antimalarial medicines without a prescription, exploring such practices in the past week; (c) assessment of community pharmacists’ knowledge of malaria diagnosis and prescription status of antimalarial medicines in Rwanda, and (d) exploration of reasons for dispensing antimalarial medicines without a prescription through an open-ended question.
Qualitative data collection continued until saturation was achieved, indicating that no further insights or issues were being identified, and additional data collection would be redundant, confirming an adequate sample size. The questionnaire was initially prepared in English and then translated into Kinyarwanda, the native language of the participants, widely spoken among community pharmacists and community members.
Data Analysis
The collected quantitative data was imported into Microsoft Excel for cleaning. After data cleaning, the cleaned dataset was imported into the Statistical Package for Social Sciences (SPSS) version 25.0 for Windows. The imported data were double-checked for accuracy to ensure reliability. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to present quantitative data. Furthermore, bivariate logistic regression analyses were conducted to identify significant variables associated with the practice of dispensing antimalarial medicines without a prescription. The odds ratio was used as a measure of the strength and direction of the relationship between the variables. All variables found to be significant in the bivariate analyses were included in multivariate logistic regression models. Multivariate analysis also used the odds ratio to determine the factors associated with the dispensing of medicines without a prescription. Statistical significance was considered at a p-value of less than 0.05, indicating a significant relationship between the variables.
Following the completion of data collection, the qualitative data —which had been audio-recorded— underwent verbatim transcription employing the Microsoft Office 365 dictation-transcription tool. Transcription was effectuated by the first, second, and seventh authors who were fluent in English and Kinyarwanda languages with sufficient experiences in data collection and analyses of the qualitative research. In addition to this step, manual editing was undertaken by the sixth, seventh, and eighth authors who were fluent in English and Kinyarwanda languages. Subsequently, the data were translated into English by the first author for subsequent analysis. The transcribed narratives underwent coding procedures facilitated by Nvivo software version 12. Commencing the analysis, the first and fifth authors generated the preliminary code set, informed by emerging themes and sub-themes that were in alignment with the research inquiries. The initial list of codes subsequently underwent review and refinement by the final author. This revised code list was then subject to collective scrutiny and refinement by all authors, culminating in the establishment of the definitive set of codes for analysis. Noteworthy is the expertise of the second and seventh authors, who possess proficiency in qualitative research and public health. The transcripts underwent meticulous reading and coding to facilitate in-depth analysis. The data were subjected to deductive analysis through the application of thematic analysis techniques. Following analysis, pertinent quotations were employed to elucidate the research findings.
Validity and Reliability of the Study
A pilot study involving 15 community pharmacists confirmed the validity and reliability of a data collection instrument for the quantitative part. The sub-component with a Cronbach’s Alpha greater than 0.6 was considered consistent. Three untrustworthy questions were revised for better understanding. The instrument showed good internal consistency, with Cronbach’s Alpha (α)=0.88. For the qualitative part, a pilot interview with a community pharmacist, similar to the study population selected through purposive sampling, was conducted. The interviewee provided no negative input, ensuring the interview guide’s applicability among the participants.
Ethics
The Institutional Review Board (IRB) of the College of Medicine and Health Sciences, University of Rwanda approved this study (Ref. CMHS/IRB/014/2022). Every participant received a consent form outlining the details of the study and the age requirement for participation, which was set at 18 years or older. Those who provided a valid, written informed consent were then given access to the research survey. The protection of confidentiality was safeguarded. Further, participation in the study was entirely voluntary and participants did not receive any compensation for their involvement in this research. Special precautions were taken to protect the identities of the respondents. In the consent form, the participants agreed that their identities would remain anonymous when reports or articles about the study are published. Moreover, participants provided consent for their direct quotes to be included in the publication of the study, with the understanding these quotations would be presented anonymously . This commitment to anonymity has been instrumental in maintaining privacy and confidentiality between the researchers and participants.
Results
Characteristics of Community Pharmacists and Pharmacies
There were 242 CPs invited to participate in this study, but seven declined because they were unavailable (n=3), requested compensation (n=2), and (n=2) had unidentified reasons. Of the 235 CPs who agreed to participate in the study, 72.8% (n=171) were men and 27.2% (n=64) were women. Their ages ranged from 20 to 50 years, with an average age of 29.43. The majority, 92.3% (n=217), had a bachelor’s degree and 7.7% (n=18) had a master’s degree. Moreover, the majority 71.9% (n=169) had less than 6 years of experience working in community pharmacies. During the study period, more than half 54.9% (n=129) were working in Kigali city and 90.6% (n=213) were working with a nurse in the pharmacy (Table 1).
 |
Table 1 Demographic Characteristics of Community Pharmacists and Pharmacies (n=235) |
Request and Dispensing of Antimalarial Medicines Without a Prescription
The study found that most community pharmacists 88.5% (n=208) were consulted by clients seeking antimalarial artemisinin-based combination therapy (ACT) without a prescription. Of the 88.5% (n=208) who were consulted, 51.1% (n=120) reported being consulted for malaria treatment three or more times per week. More than a half (n=127, 54%) of the community pharmacists reported dispensing ACTs without a prescription, while 46% (n=108) referred clients to malaria diagnostic testing facilities. Almost all 97% (n=228) of the community pharmacies had the first-line antimalarial (artemether-Lumefantrine) in stock, which was the only antimalarial medicine dispensed without a prescription 100% (n=208). Further results showed that 48% (n=61) of the community pharmacists who dispensed antimalarial medicines without a prescription did so two to three times per week while the data were being collected (Table 2).
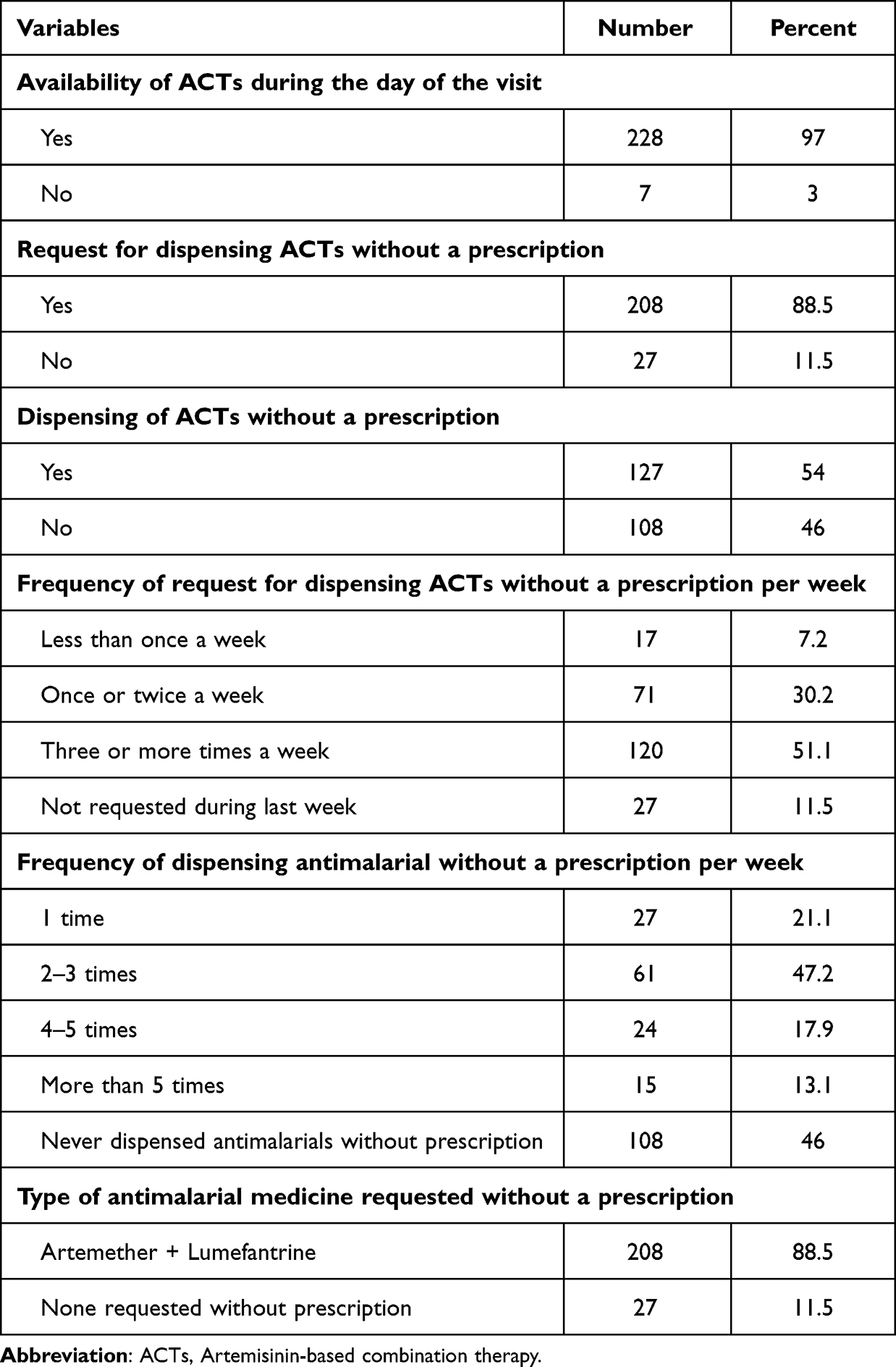 |
Table 2 Request and Dispensing of Antimalarial Medicines Without a Prescription (n=235) |
Of the community pharmacists who did not dispense antimalarial medicines to clients without a prescription, 108 respondents (46%) advised their clients to undergo a malaria diagnostic test first. They advised clients to go to a hospital, health center, clinic, dispensary, or community health worker for malaria testing. Some participants stated the following:
I advise them to get a test first, then tell the client to take antipyretics or NSAIDs while they wait for the results of the diagnostic test. (Community Pharmacist, aged 36)
Because malaria tests are inexpensive, pharmacists have no reason to dispense antimalarials without a prescription. They can instead find ways to get the rapid test to the pharmacy so that any incoming client without a prescription can use it to confirm positivity or negativity. (Community Pharmacist aged 29)
Knowledge of Community Pharmacists on Malaria and Prescription Status of Antimalarials
When community pharmacists were asked about malaria symptoms that clients present prior to asking for antimalarial medicines, 96% (n=225) reported fever, 74.5% (n=176) reported headache, and 63.7% (n=150) reported body weakness (Table 3).
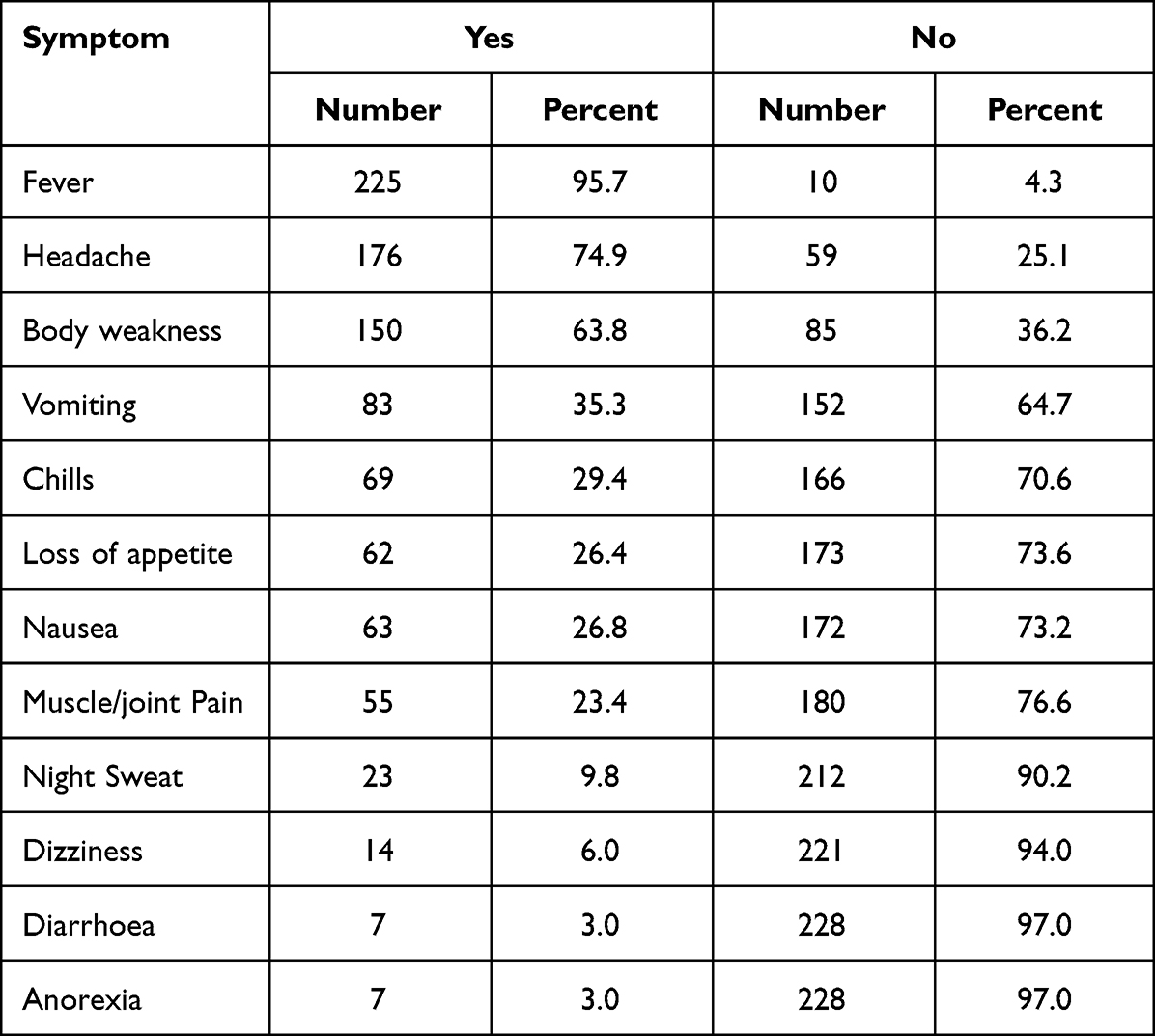 |
Table 3 Symptoms of Malaria (n=235) |
We found that 63.4% (n=149) of respondents were aware that antimalarial medicines are prescription medicines but are sometimes dispensed without a prescription. Only 20.9% (n=49) of the respondents stated that antimalarial medicines are only available by prescription and must always be accompanied by one. More than a half (66.4%, n=156) agreed that dispensing antimalarial medicines without malaria confirmation was a serious problem. As a result, the majority of 86.8% (n=204) suggested that antimalarial medicines be given only after a positive malaria diagnostic test(Table 4)
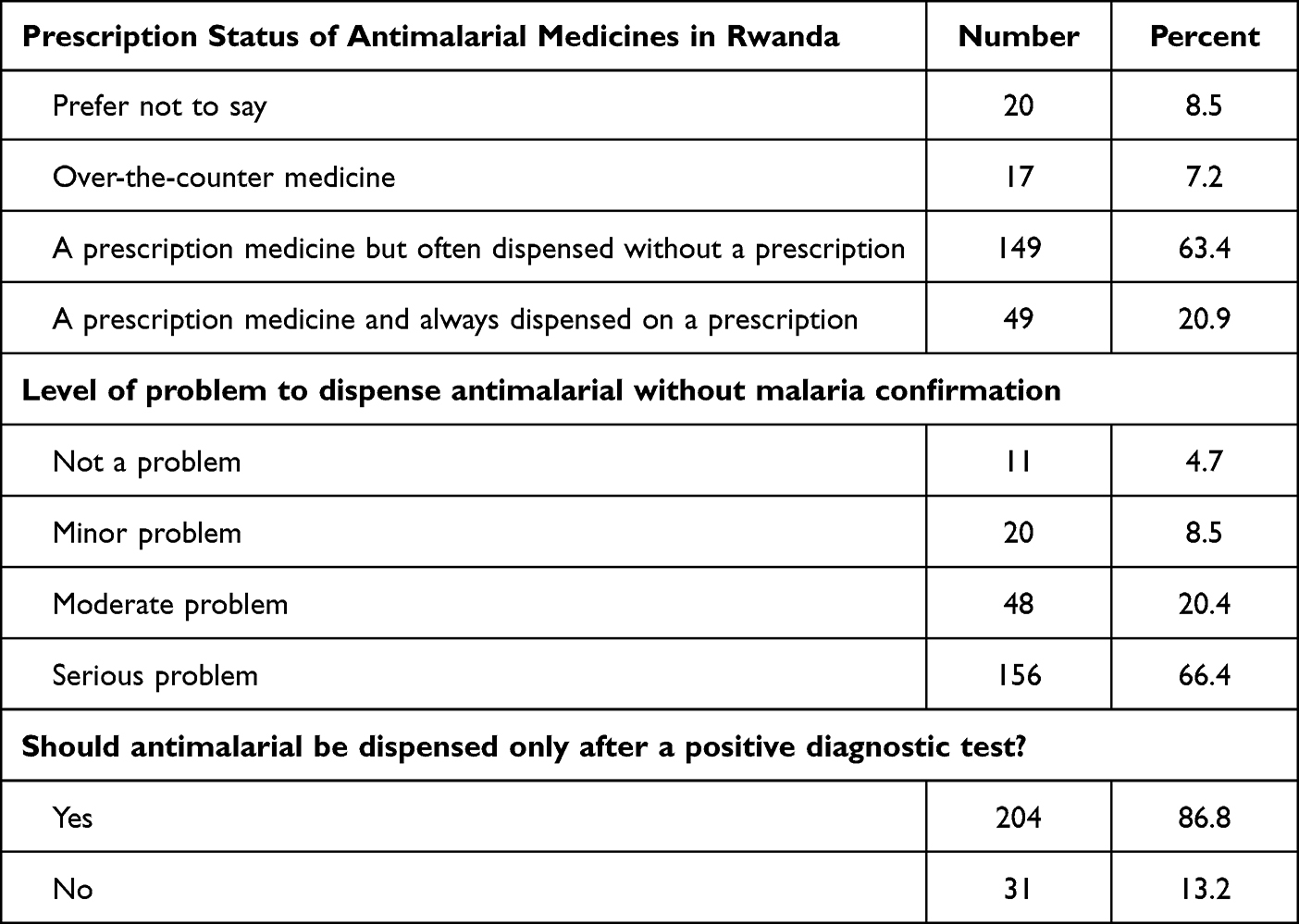 |
Table 4 Perceptions of Community Pharmacists on Prescription Status of Antimalarial Medicines (n=235) |
Bivariate Logistic Regression Analyses for the Associated Factors of Dispensing Antimalarial Medicines Without a Prescription
Bivariate logistic regression analyses revealed that respondents who reported that being aware of the negative effects of dispensing antimalarial medicines without a prescription, having knowledge of the prescription status of antimalarial medicines, and having access to m-RDTs in pharmacies were significantly associated with dispensing non-prescribed antimalarial medicines (Table 5).
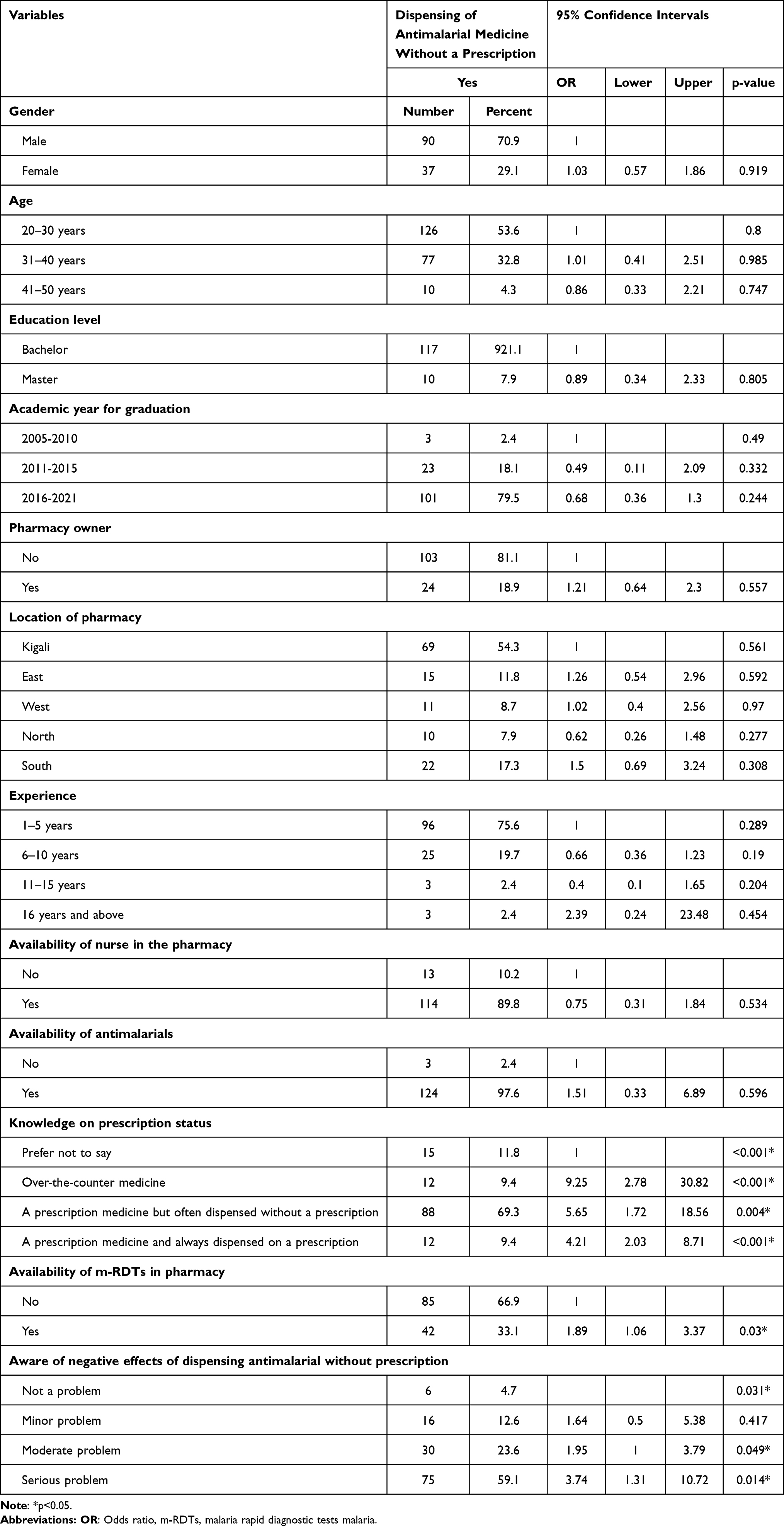 |
Table 5 Bivariate Logistic for Associated Factors of Dispensing Antimalarial Without Prescription (n=127) |
Logistic Regression Analyses for the Associated Factors of Dispensing Antimalarial Medicines Without a Prescription
Multivariate analysis revealed that respondents who reported that antimalarials were over-the-counter medicines [OR=7.03; 95% CI, (2.01; 24.56), p=0.002], prescription medicines but sometimes dispensed without a prescription [OR=5.71; 95% CI, (1.65; 19.78), p=0.006], prescription-only medicines, and always dispensed on a prescription [OR=4.17; 95% CI, (1.95; 8.91)), and those who had m-RDTs available in pharmacies [OR=2.08; 95% CI, (1.1; 3.94), p=0.02] were more likely than their counterparts to provide non-prescribed antimalarial medicines. However, the dispensing of non-prescribed antimalarial medicines was not significantly associated with awareness of the negative effects of dispensing antimalarial drugs without a prescription (Table 6).
 |
Table 6 Multivariate Logistic for Associated Factors of Dispensing Antimalarial Without a Prescription (n=127) |
Factors Contributing to Over-the Counter Antimalarial Seeking and Dispensing
These factors were identified by CPs and divided into two categories: factors influencing clients to seek over-the-counter antimalarial medicines and factors influencing CPs to dispense over-the-counter antimalarial medicines. These factors are discussed in the following sections:
Factors Influencing Clients to Seek Over-The Counter Antimalarial Medicines
The factors influencing clients to seek over-The-counter antimalarial medicines, as reported by CPs, were divided into (1) long queues at public health facilities, (2) non-adherence to the test results, and (3) lack of health insurance. This is discussed in detail in the next section.
Long Queue at Health Facilities
The main reason given by CPs for clients preferring to seek malaria treatment in community pharmacies is that public health facilities have many clients, thus causing a long queue and a long waiting time to provide healthcare services. However, some clients also have pressing travel plans to malaria-endemic countries or have had long working days and do not have time to visit public health institutions. The community pharmacists expressed the following:
Some clients do not like to spend a long time at health centers or hospitals. Also, clients don’t need to consult a physician because of the huge number of clients. (Community pharmacist, aged 32 years)
Some clients do come to community pharmacies because they are traveling back to Europe or elsewhere thinking that they may need it later when they are there. (Community pharmacist, aged 32 years)
Similarly, respondents expressed that community pharmacists are accessible because they provide healthcare services as quickly as possible compared to hospitals and health centers where they can spend much time so that they can receive healthcare services.
Another respondent said,
Access to public health institution is difficult due to long queue, thus clients prefer getting antimalarial medicines from community Pharmacies as they are more accessible. (Community pharmacist, aged 32 years)
Non-Adherence to the Negative Test Results
Our findings showed that CPs observed clients who did not trust the negative malaria results provided by public health facilities, so they went to community pharmacies to purchase antimalarial medicines on their own thinking that the results obtained were false negatives. In addition, community pharmacists showed that some malaria tests are not accurate and provide inaccurate results during the diagnosis, which impeded an effective diagnosis and discouraged clients from being prescribed medicines for malaria and pharmacists from providing medicines without prescription. A respondent expressed:
Sometimes clients test negative at hospitals or from community health workers, yet they feel like they have malaria, as a result they visit community pharmacies to get antimalarial medicines. Thus, rapid tests are not always trustworthy. (Community pharmacist aged 29 years)
Lack of Health Insurance
Some clients, particularly those from rural areas, fail to pay community-based health insurance (CBHI); as a result, when they become ill, they seek treatment from CPs because they do not charge consultation fees and cannot afford hospital or clinic bills. One of the CP stated:
Some clients especially in rural areas do not have enough money to pay for a hospital consultation or other laboratory tests because they do not have health insurance. Therefore, they are afraid of going to a health facility because they could not afford the bill when they were charged 100%. When these come, they claim to be aware of the symptoms they are experiencing, so they come to ask for antimalarial medicines. (Community pharmacist aged 32years)
In relation to this, some people who travel abroad and do not have local insurance prefer buying these antimalarial medicines for future use.
Some local and international citizens who do not have insurance prefer to obtain antimalarial medicines from community pharmacies prior to traveling abroad because they can not get it from a formal health facility. (Community pharmacist aged 36 years)
Factors Influencing CPs’ Dispensing of Over-the-Counter Antimalarial Medicines
Factors influencing CPs to dispense over-The-counter antimalarial medicines were identified and classified into four categories: (1) knowledge of CPs to diagnose malaria, (2) client pressure, (3) ability to perform a malaria diagnostic test, and (4) fear of losing clients. This is discussed in detail in the following sections.
Knowledge of Community Pharmacists to Diagnose Malaria
Community pharmacists’ decisions to dispense antimalarial medicines over-the-counter were heavily influenced by their knowledge of malaria diagnosis. They claimed that simple malaria is easy to diagnose, and that even community health workers with no specialized training can do so. They emphasized that malaria can be treated presumptively based on symptoms and the client’s history, including whether they are from an endemic area. In addition, some community pharmacists indicated that they dispense antimalarial medicines because they want to help clients who do not have the time or means to go to a health facility. Some of the participants elaborated the following:
The malaria seasons are known and when working from a malaria endemic region or the clients have said they don’t sleep under mosquito net, it is easy to presume malaria. (Community Pharmacist aged 36 years)
Pharmacists are qualified to diagnose and treat malarial diseases. Some doctors also prescribe antimalarial medicines based on symptoms through a client-doctor discussion. (Community Pharmacist aged 33 years)
We do it to reduce rates of mortality related to malaria among the community. But also, some people do not have enough time to seek services in public health facilities. (Community Pharmacist aged 29)
Sometimes community pharmacists are helping the clients because the clients don’t want to go the hospital (due to different reasons) for diagnosis and prefer to buy it over-the-counter. (Community Pharmacist aged 41years)
The Influences of the Clients and Pressure
The CPs agreed to supply antimalarial medicines over-the-counter in response to client requests and pressures. They went on to say that since most clients had already experienced malaria, they also knew about it. According to community pharmacists, clients’ beliefs that their ailments were mild enough not to require attention led them to request antimalarial medicines without a prescription. They also mentioned that clients thought they would receive the same prescription if they visited a doctor because they had previously been treated for a condition of similar nature. Participants stated:
I think most are influenced by client because most of time client comes in retail pharmacies and he/ she tells the nurse or pharmacist that she knows her state when he/ she have malaria and same times he might give out the signs and symptoms. (Community Pharmacist aged 29years)
First, clients have had the same symptoms in the past and got the same treatment, so they are in most cases pretty much sure that what they have is malaria. (Community Pharmacist aged 36 years)
Some clients say give me the medicines; I already know how I feel when I get infected with malaria. (Community Pharmacist, aged 43 years)
Ability to Perform a Malaria Test
Some CPs stated that they dispensed antimalarials after performing a malaria rapid diagnostic test for clients, although it has not yet been allowed for use in community pharmacies. One community pharmacist expressed the following:
I think the Test of Malaria is simple and can be performed in retail/Community pharmacy. When the client presents malaria signs and is confirmed by malaria rapid diagnostic test. (Community Pharmacist aged 25 years)
Fear of Losing the Client
Some CPs claimed that they dispensed antimalarial medicines out of fear of losing customers, because community pharmacies compete with one another to attract customers. If they did not, they would go to the next pharmacy to receive the same medicines, which would irritate pharmacy owners because pharmacies are also meant to make a profit. A participant said:
High request, many competing pharmacies impeding professionalism (you don’t provide them while others do), antimalarials are commonly used in the community by CHWs. Clients are insisting that if you don’t give it to them, they will go to another pharmacy. (Community Pharmacist aged 29 years)
Another respondent said,
If you deny delivering the client will go elsewhere and they will give him the medicine. Some pharmacy owners are afraid of losing the client, thus putting pressure on the pharmacist to dispense antimalarial medicines despite the lack of confirmed presence of malaria. (Community pharmacist aged 36 years)
Discussion
Our study explored the request and dispensing of antimalarials without a prescription in community pharmacies, as well as factors that influence it. The request for antimalarials without a prescription was 88.5%. This rate is comparable to that reported in a Nigerian study, where more than 60% of individuals sought malaria treatment in community pharmacies.27 The request for antimalarials without a prescription in the current study could be attributed to the preference of individuals to seek treatment in community pharmacies rather than public health facilities, which has been documented in previous studies in SSA.22,28,29 The findings of the current study suggest that a high proportion of individuals in Rwanda are seeking antimalarials without a prescription, which may have implications for the efficacy of malaria treatment and the emergence of drug resistance. Although community pharmacists in some countries within the same region, such as Kenya, can dispense antimalarials without a prescription after conducting an m-RDT,22 the regulations in Rwanda do not allow it. This highlights the need for interventions that promote the appropriate use of antimalarials and encourage individuals to seek attention before taking any medicines. Alternatively, the current results could also inform a need to develop strategies that extend access to malaria diagnostic services in community pharmacies in Rwanda.
In our study, factors such as long queues at public health facilities, non-adherence to the test results, and lack of health insurance were reported as reasons clients seek antimalarials in community pharmacies. These results concurred with those of a study conducted in Kenya and Egypt, where consultation fees and time to formal health facilities were among the main factors leading clients to seek antimalarial self-medication.30,31 These findings imply that improving the accessibility and affordability of healthcare services, including diagnostic tests and consultations, may help to reduce the burden of self-medication and improve the appropriate use of medication. In SSA, community pharmacies are important in the treatment of minor ailments and reduce the request for more costly healthcare options like appointments with doctors.16,32,33 However, as in the present study, previous studies conducted in Kenya and Nigeria revealed that clients who expected positive malaria test results were likely to request antimalarials despite their negative test results.12,19 Therefore, strategies to improve client education may help to address this issue and improve the appropriate use of antimalarial medicines. Furthermore, the factors identified in the present study could provide a strong foundation for the Rwandan healthcare system to improve access to malaria diagnosis and treatment services in community pharmacies, which are a popular choice among the public.
The WHO recommends that all suspected cases of malaria should undergo parasitological testing (microscopy or Rapid Diagnostic Test) to confirm the diagnosis.5 However, the current study found that 54% of community pharmacists dispensed antimalarials without conducting a parasitological test. Similarly, another study in SSA reported that community pharmacists dispensed antimalarials even when clients did not have a prescription or a confirmed malaria diagnosis.2 Treating malaria without prior diagnostic confirmation promotes self-medication, which can lead to antimalarial resistance, a global concern.34–37 Thus, this finding illustrates a potential risk of malaria misdiagnosis, which may accelerate the burden of antimalarial drug resistance reported in Rwanda as the first African country.21 The current finding is yet another demonstration that those community pharmacies facilitate self-medication, which was similarly reported in a study in Rwanda.38 Importantly, the rate in the current study was found to be low compared to studies in Ghana and Tanzania, where 66% and 98% of clients were treated without an RDT.22,39 Our findings suggest that there should be more effort at extending malaria case detection and management in community pharmacies, leveraging on the already existing healthcare workers, with benefits in people seeking to buy antimalarial without a prescription.
In Kenya, pharmacy retailers have suggested that increasing the use of m-RDTs would increase rational malaria treatment in private retail drug outlets.12 This is like the current study, where 66.4% community pharmacists agreed that dispensing antimalarials without prior diagnostic confirmation is a serious problem, thus proposed licensing use of m-RDTs in community pharmacies to promote rational treatment of malaria. This is supported by a previous study where Rwandan community pharmacists suggested a regulatory authority to license the use of rapid diagnostic tests such as m-RDTs in community pharmacies.40 Rational dispensing ensures that the client receives the medication appropriate for their diagnosis at the correct dose and at the right time, and that there is no unnecessary use of drugs.41 Thus, the national regulatory bodies that prohibit retail providers from performing consultations and offering an RDT pose an additional barrier to promoting rational dispensing. In Ghana, m-RDT reduced the likelihood of purchasing antimalarial medicines by 42%.19 So, this barrier should be overcome, especially considering studies showing that community pharmacists are willing to incorporate RDTs into their business and that customers are likely to accept testing before requesting treatment in community pharmacies.2 Access to primary health should be understood more broadly than simply locating a healthcare setting within or close to communities.42
In the current study, community pharmacists with m-RDTs in stock were more likely to dispense antimalarial medicines without prescription. This is substantiated by a study in Nigeria, where health workers felt that m-RDTs increased their tendency to prescribe more ACTs.43 They are also supported by a study in Burkina Faso, which reported that the prescription of antimalarials was affected by the performance of malaria diagnostic tests.44 The reported likelihood in our study could be attributed to the fact that 16.5% admitted that they performed m-RDTs before dispensing antimalarials to clients without a prescription. However, this rate is low compared to a study in Nigeria, where 28.5% of community pharmacists carried out malaria diagnosis before initiating treatment.27 This difference might be because the use of diagnostic services is an unlicensed practice in community pharmacies in Rwanda. Our results also agreed with those of a study conducted in Tanzania, which stated that the availability of reliable, easy-to-use, and affordable m-RDTs allows a realistic switch from presumptive treatment to laboratory-confirmed diagnosis and treatment.36 Though community pharmacists who were not aware that antimalarials are prescription medicines were more likely to dispense antimalarial medicines without prescription in the current study, the majority 86.8% admitted that antimalarials should be dispensed only after a positive test. The perceptions of community pharmacists in the current study were positive, as in a study in Nigeria where 91.4% of health workers agreed that febrile clients must be tested prior to treatment.45 In a country like Rwanda, where artemisinin resistance has been reported, it is critical to reinforce national regulations through educational programs tailored to the availability of reference material for non-prescription medicines.
Further factors identified to influencing CPs to dispense over-the counter antimalarial medicines were (1) knowledge of CPs to diagnose malaria, (2) client pressure, (3) being able to perform a malaria diagnostic test, and (4) fear of losing clients. Regarding their knowledge to diagnose malaria, most cited fever, and headache as the main symptoms of malaria. Similarly, in Ghana, fever is the most common symptom that often leads to presumptive treatment.35 As in the current study, in Ethiopia, continued customer pressure was the major reason for maintaining the counter-sale of antibiotics.46 Similar to our study, client pressure has been identified as a factor behind dispensing antibiotics among community pharmacists in Sudan.47 Another study in SSA countries reported that most healthcare workers acknowledged pressure as a factor leading to inappropriate dispensing of antimalarials to RDT-negative clients.48 In agreement with the current study, in Italy, Vietnam, and Saudi Arabia,49–51 community pharmacists dispensed antibiotics without prescription because of fear of losing clients, affecting their sales, and decreasing profit margins. Hence, the healthcare system in Rwanda needs to develop a working relationship with community pharmacies to ensure that malaria diagnosis and treatment are equally accessible in community pharmacies to guide appropriate treatment in these settings. Existing laws are yet to recognize the added roles of community pharmacists in the healthcare system, as they are restricted in their roles and can assist clients with minor ill health.
Strengths and Limitations
Our study had two major strengths. First, the use of an embedded mixed-methods approach, combining qualitative and quantitative data collection and analysis simultaneously, enhanced the consistency and validity of our findings. Second, our study was the first to explore the prevalence of dispensing antimalarial medicines without a prescription in Rwanda, as well as the determinants associated with this practice among community pharmacists. However, our study had some limitations. First, there is a scarcity of literature specifically focusing on community pharmacists in Rwanda and sub-Saharan Africa as a whole. Second, we did not directly interview clients who sought antimalarial medicines without a prescription from community pharmacies. Additionally, due to the nature of our embedded design, we were unable to establish causal relationships, highlighting the need for future longitudinal studies to explore causality in this context. Future qualitative studies are recommended to get an in-depth understanding of community pharmacies’ attitudes towards demand for antimalarial medicines and their difficulties in dispensing them without a prescription.
Public Health Implications
Our study underscores the potential of community pharmacists as accessible healthcare providers. Policymakers should consider measures to further integrate community pharmacists into the healthcare system to enhance patients’ access to essential services. Policymakers may also prioritize continuous education and training programs for community pharmacists, ensuring they are equipped with the latest knowledge and skills necessary to handle various health issues effectively. Our study also highlights the need for updates in the legal and regulatory framework governing the practice of community pharmacists. Current regulations should be reviewed to allow community pharmacists an expanded scope of practice, especially in dealing with diseases like malaria when appropriate. This can lead to quicker diagnosis, treatment, and referral, ultimately reducing the burden on secondary healthcare facilities. To achieve that, promoting collaboration between community pharmacists and other healthcare providers is crucial. Therefore, policies should encourage inter-professional teamwork to optimize patient care and outcomes. Health policy makers should consider revising and modernizing these regulations to reflect the evolving roles of community pharmacists. Policymakers may also invest in public health campaigns to raise awareness about the expanded roles of community pharmacists. This can help patients make informed decisions about seeking healthcare services from community pharmacists.
Conclusion
Request and dispensing of antimalarial medicines without a necessary prescription are frequent in community pharmacies in Rwanda. Community pharmacists indicated that non-adherence to negative malaria diagnostic tests obtained from formal health facilities, long queues, and lack of affordability at these facilities were the main reasons clients without prescriptions sought antimalarials in community pharmacies. On the other hand, being unaware that antimalarials are prescription medicines and prior knowledge of the use of malaria diagnostic tests significantly led community pharmacists to dispense antimalarial medicines without a prescription. However, they are aware that such practices lead to overuse of antimalarial medicines and antimalarial drug resistance. Moreover, they had positive attitudes as far as dispensing antimalarial medicines upon a diagnostic test was concerned and were ready to improve their contribution to malaria management. Therefore, they suggested licensing the use of m-RDTs to limit the presumptive treatment of malaria.
Acknowledgments
The authors gratefully acknowledge the participants who consented to participate.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World malaria report 2022; 2022. Available from: https://www.who.int/teams/global-malaria-programme.
2. Ladner J, Davis B, Audureau E, Saba J. Treatment-seeking patterns for malaria in pharmacies in five sub-Saharan African countries. Malar J. 2017;16(1). doi:10.1186/s12936-017-1997-3
3. National Institute of Statistics of Rwanda. Rwanda demographic and health survey 2019–2020; 2019. Available from: https://www.statistics.gov.rw/datasource/demographic-and-health-survey-201920.
4. Maiga FO, Wele M, Toure SM, et al. Artemisinin-based combination therapy for uncomplicated Plasmodium falciparum malaria in Mali: a systematic review and meta-analysis. Malar J. 2021;20. doi:10.1186/s12936-021-03890-0
5. World Health Organization. WHO Guidelines for malaria – 3; 2022. Available from: http://apps.who.int/bookorders.
6. Davis B, Ladner J, Sams K, et al. Artemisinin-based combination therapy availability and use in the private sector of five AMFm Phase 1 countries; 2013. Available from. http://www.malariajournal.com/content/12/1/135.
7. World Health Organization. Artemisinin resistance and artemisinin-based combination therapy efficacy; 2010.
8. Pousibet-Puerto J, Salas-Coronas J, Sánchez-Crespo A, et al. Impact of using artemisinin-based combination therapy (ACT) in the treatment of uncomplicated malaria from Plasmodium falciparum in a non-endemic zone. Malar J. 2016;15(1). doi:10.1186/s12936-016-1408-1
9. Ministry of health, R. National guidelines for the treatment of malaria in Rwanda; 2013.
10. Tougher S, Hanson K, Goodman C. What happened to anti-malarial markets after the affordable medicines facility-malaria pilot? Trends in ACT availability, price and market share from five African countries under continuation of the private sector co-payment mechanism. Malar J. 2017;16(1). doi:10.1186/s12936-017-1814-z
11. Kizito J, Kayendeke M, Nabirye C, Staedke SG, Chandler CIR. Improving access to health care for malaria in Africa: a review of literature on what attracts patients. Malar J. 2012;11(1). doi:10.1186/PREACCEPT-2317562776368437
12. Rusk A, Goodman C, Naanyu V, et al. Expanding access to malaria diagnosis through retail shops in western Kenya: what do shop workers think? Malar Res Treat. 2013;2013. doi:10.1155/2013/398143
13. Kaula H, Buyungo P, Opigo J. Private sector role, readiness and performance for malaria case management in Uganda, 2015. Malar J. 2017;16(1). doi:10.1186/s12936-017-1824-x
14. Kagashe GAB, Minzi O, Matowe L. An assessment of dispensing practices in private pharmacies in Dar-es-Salaam, Tanzania. Int J Pharm Pract. 2011;19(1):30–35. doi:10.1111/j.2042-7174.2010.00075.x
15. Cohen J, Cox A, Dickens W, et al. Determinants of malaria diagnostic uptake in the retail sector: qualitative analysis from focus groups in Uganda. Malar J. 2015;14(1). doi:10.1186/s12936-015-0590-x
16. Okai GA, Abekah-Nkrumah G, Asuming PO. Perceptions and trends in the use of community pharmacies in Ghana. J Pharm Policy Pract. 2019;12(1). doi:10.1186/s40545-019-0186-x
17. Alba S, Hetzel MW, Goodman C, et al. Improvements in access to malaria treatment in Tanzania after switch to artemisinin combination therapy and the introduction of accredited drug dispensing outlets - A provider perspective. Malar J. 2010;9(1). doi:10.1186/1475-2875-9-164
18. Visser T, Bruxvoort K, Maloney K, et al. Introducing malaria rapid diagnostic tests in private medicine retail outlets: a systematic literature review. PLoS One. 2017;12(3):1–24. doi:10.1371/journal.pone.0173093
19. Ikwuobe JO, Faragher BE, Alawode G, Lalloo DG. The impact of rapid malaria diagnostic tests upon anti-malarial sales in community pharmacies in Gwagwalada, Nigeria. Malar J. 2013;12(1). doi:10.1186/1475-2875-12-380
20. World Health Organization(WHO). World malaria report 2021. Available from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021.
21. Uwimana A, Legrand E, Stokes BH, et al. Emergence and clonal expansion of in vitro artemisinin-resistant Plasmodium falciparum kelch13 R561H mutant parasites in Rwanda. Nat Med. 2020;26(10):1602–1608. doi:10.1038/s41591-020-1005-2
22. Amankwa CE, Bonful HA, Agyabeng K, Nortey PA. Dispensing practices for anti-malarials in the la nkwantanang-madina municipality, greater Accra, Ghana: a cross-sectional study. Malar J. 2019;18(1). doi:10.1186/s12936-019-2897-5
23. Frempong BK, Amalba A, Donkor N, Akuffo KO. Regulatory compliance among over-The-counter medicine sellers facilities within the Upper East Region of Ghana. J Pharm Policy Pract. 2021;14(1). doi:10.1186/s40545-021-00363-2
24. Ministry of Health. National Pharmacy Policy; 2016. Available from: https://www.moh.gov.rw/fileadmin/templates/policies/Pharmacy-Policy_Rwanda-2016.pdf.
25. Rwanda food and drugs. List of licensed human retail pharmacies; 2021.
26. Naing NN. Determination of sample size. Malays J Med Sci. 2003;10:84–86.
27. Peace Chukwuzurum E, Obi Daniel E, Olukayode Popoola I, et al. Malaria diagnosis and treatment: perception of community pharmacists in Abuja metropolis, Nigeria. Int J Infect Dis Ther. 2021;6(1):6. doi:10.11648/j.ijidt.20210601.12
28. Hirko N, Edessa D. Factors influencing the exit knowledge of patients for dispensed drugs at outpatient pharmacy of hiwot fana specialized university hospital, Eastern Ethiopia. Patient Prefer Adherence. 2017;11:205–212. doi:10.2147/PPA.S128658
29. Buabeng KO, Duwiejua M, Dodoo ANO, Matowe LK, Enlund H. Self-reported use of anti-malarial drugs and health facility management of malaria in Ghana. Malar J. 2007;6(1). doi:10.1186/1475-2875-6-85
30. Kimoloi S, Okeyo N, Ondigo BN, et al. Choice and sources of antimalarial drugs used for self-medication in Kisumu, Western Kenya. J Pharmacol Ther. 2013;2:124–129.
31. Ghazawy ER. Self-medication among adults in Minia, Egypt: a cross sectional community-based study. Health N Hav. 2017;09:883–895.
32. Anderson S. Community pharmacy and public health in Great Britain, 1936 to 2006: how a Phoenix rose from the ashes. J Epidemiol Community Health. 2007;61(10):844–848. doi:10.1136/jech.2006.055442
33. Hughes, Dyfrig. & Pharmacy Practice Research Trust. Medicines and People (Programme). Investigating Factors Influencing User Choices to Visit Either General Practitioners or Community Pharmacists in the Management of Minor Ailments: Piloting a Discrete Choice Experiment. Pharmacy Practice Research Trust; 2008.
34. Mwita S, Meja O, Katabalo D, Richard C. Magnitude and factors associated with anti-malarial self-medication practice among residents of Kasulu Town Council, Kigoma-Tanzania. Afri Health Sci. 2019;19(3):2457. doi:10.4314/ahs.v19i3.20
35. Babayara MNK, Addo B. Presumptive treatment of malaria in Ghana: was it ever useful? Evidence from the Kassena-Nankana District of Northern Ghana. Malar Res Treat. 2018;2018:1–6. doi:10.1155/2018/3408089
36. D’Acremont V, Kahama-Maro J, Swai N, et al. Reduction of anti-malarial consumption after rapid diagnostic tests implementation in Dar es Salaam: a before-after and cluster randomized controlled study. Malar J. 2011;10:1.
37. Attinsounon CA, Sissinto Y, Avokpaho E, et al. Self-medication practice against malaria and associated factors in the City of Parakou in Northern Benin: results of a population survey in 2017. Adv Infect Dis. 2019;09:263–275.
38. Tuyishimire J, Okoya F, Adebayo AY, Humura F, Lucero-Prisno DE. Assessment of self-medication practices with antibiotics among undergraduate university students in Rwanda. Pan Afr Med J. 2019;33. doi:10.11604/pamj.2019.33.307.18139
39. Masanja MI, McMorrow M, McElroy PD, Kachur SP, McElroy PD. Health workers’ use of malaria rapid diagnostic tests (RDTS) to guide clinical decision making in rural dispensaries, Tanzania. Am J Trop Med Hyg. 2010;83(6):1238–1241. doi:10.4269/ajtmh.2010.10-0194
40. Nsengimana A, Biracyaza E, Hategekimana JC, et al. Attitudes, perceptions, and barriers of community pharmacists in Rwanda towards health promotion: a cross sectional study. Arch Public Health. 2022;80(1). doi:10.1186/s13690-022-00912-4
41. Kamuhabwa AAR, Silumbe R. Knowledge among drug dispensers and antimalarial drug prescribing practices in public health facilities in Dar es Salaam. Drug Healthc Patient Saf. 2013;5:181–189. doi:10.2147/DHPS.S50071
42. Davy C, Harfield S, McArthur A, Munn Z, Brown A. Access to primary health care services for Indigenous peoples: a framework synthesis. Int J Equity Health. 2016;15(1):1–9. doi:10.1186/s12939-016-0450-5
43. Uzochukwu BSC, Onwujekwe E, Ezuma NN, et al. Improving rational treatment of malaria: perceptions and influence of RDTs on prescribing behaviour of health workers in Southeast Nigeria. PLoS One. 2011;6(1):e14627. doi:10.1371/journal.pone.0014627
44. Bonko MDA, Kiemde F, Tahita MC, et al. The effect of malaria rapid diagnostic tests results on antimicrobial prescription practices of health care workers in Burkina Faso. Ann Clin Microbiol Antimicrob. 2019;18(1). doi:10.1186/s12941-019-0304-2
45. Obi IF, Sabitu K, Olorukooba A, et al. Health workers’ perception of malaria rapid diagnostic test and factors influencing compliance with test results in Ebonyi state, Nigeria. PLoS One. 2019;14(10):e0223869. doi:10.1371/journal.pone.0223869
46. Gebretekle GB, Serbessa MK. Exploration of over the counter sales of antibiotics in community pharmacies of Addis Ababa, Ethiopia: pharmacy professionals’ perspective. Antimicrob Resist Infect Control. 2016;5(1). doi:10.1186/s13756-016-0101-z
47. Abdelrahman Hussain M, Osman Mohamed A, Sandel Abkar A, Siddig Mohamed F, Khider Elzubair H. Knowledge, attitude and practice of community pharmacists in relation to dispensing antibiotics without prescription in Sudan: a cross-sectional study. Integr Pharm Res Pract. 2022;11:107–116. doi:10.2147/IPRP.S363079
48. Boyce MR, O’Meara WP. Use of malaria RDTs in various health contexts across sub-Saharan Africa: a systematic review. BMC Public Health. 2017;17(1). doi:10.1186/s12889-017-4398-1
49. Bianco A, Licata F, Trovato A, Napolitano F, Pavia M. Antibiotic-dispensing practice in community pharmacies: results of a cross-sectional study in Italy. Antimicrob Agents Chemother. 2021;65(6). doi:10.1128/AAC.02729-20
50. Hadi MA, Karami NA, Al-Muwalid AS, et al. Community pharmacists’ knowledge, attitude, and practices towards dispensing antibiotics without prescription (DAwP): a cross-sectional survey in Makkah Province, Saudi Arabia. Int J Infect Dis. 2016;47:95–100. doi:10.1016/j.ijid.2016.06.003
51. Nga Do TT, Chuc NT, Hoa NP, et al. Antibiotic sales in rural and urban pharmacies in northern Vietnam: an observational study. BMC Pharmacol Toxicol. 2014;15(6). doi:10.1186/2050-6511-15-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.