")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Reduction of Inflammatory RANTES/CCL5 Serum Levels by Surgery in Patients with Bone Marrow Defects of the Jawbone
Authors Diederich J , Schwagten H, Biltgen G, Lechner J , Müller KE
Received 1 May 2023
Accepted for publication 1 September 2023
Published 8 September 2023 Volume 2023:15 Pages 181—188
DOI https://doi.org/10.2147/CCIDE.S417783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Joé Diederich,1 Hendrik Schwagten,2 Georges Biltgen,3 Johann Lechner,4 Kurt E Müller5
1Center for General, Clinical Environmental and Functional Medicine, Colmar-Berg, Luxembourg; 2Private Practice, Center for Biological Dentistry, Luxembourg-City, Luxembourg; 3Private Practice, Center for Biological Dentistry, Diekirch, Luxembourg; 4Private Practice, Centre for Integrative Dentistry, Munich, Germany; 5Dermatology, Clinical Environmental Medicine, Functional Medicine, Preventive Medicine, Dresden International University, Kempten, Germany
Correspondence: Joé Diederich, 4b, Avenue G. Smith, Colmar-Berg, L-7740, Luxembourg, Tel +352 268866-1, Fax +352 268866-66, Email [email protected]
Purpose: The presence of bone marrow defects of the jawbone (BMDJ) is associated with increased levels of inflammatory cytokines such as RANTES/CCL5. The purpose of this study was to analyze if BMDJ therapy under real-world conditions reduces RANTES/CCL5 serum levels in BMDJ patients.
Patients and Methods: During this retrospective study, 113 BMDJ patients received either no treatment (n = 57), BMDJ surgery (n = 25), tooth extraction (n = 20), or root canal treatment (n = 11). Serum concentrations of RANTES/CCL5, C-reactive protein (CRP), and Tumor Necrosis Factor-α (TNF-α) were assessed before and after treatment (interventional group) and at the beginning and end of the study period (control group). Statistical analyses of the results were performed by the two-sample t-test and Bonferroni post hoc test with ANOVA for multiple comparisons.
Results: BMDJ were detected in all patients with 4.42 ± 2.75 BMDJ findings per patient. RANTES/CCL5 levels were significantly reduced by any treatment when compared to no treatment (p < 0.001; effect size d = 0.90). This effect was most pronounced in the BMDJ surgery group (p < 0.001; effect size d = 1.30). In contrast, RANTES/CCL5 serum concentrations further increased in untreated patients. Mean duration between pre- and post-treatment RANTES/CCL5 measurements was 22.86 ± 19.36 weeks, with no correlation with RANTES/CCL5 levels in any interventional group or in the total sample (p = 0.104).
Conclusion: BMDJ surgery, tooth extraction, and root canal treatment significantly reduce RANTES/CCL5 serum concentrations in BMDJ patients, with surgery being most beneficial. Further research is required to establish regular RANTES/CCL5 assessments as part of an improved diagnosis, monitoring, and evaluation of therapy success in BMDJ patients.
Keywords: bone marrow defect of the jawbone, osteolysis, osteonecrosis of the jaw, RANTES, dental
A Letter to the Editor has been published for this article.
A Response to Letter by Professor Keith has been published for this article.
Introduction
There is growing evidence for the association between dental health and non-oral conditions and chronic diseases such as facial neuralgia1 and cardiovascular disease.2,3 One dental disorder potentially involved in the development of chronic disease is the formation of bone marrow defects of the jawbone (BMDJ). BMDJ mostly occur in the periphery of implants and dental buds as well as after tooth extraction and root resection. They initially develop from fibrosis and chronic intraosseous inflammation, followed by bone destruction and bone marrow loss, initiating cavitation formation.1 The process of developing BMDJ may involve the accumulation of degenerative fatty tissue and may lead to neuralgia-inducing cavitational osteonecrosis, but can also be asymptomatic for years.1 BMDJ has been suspected to interfere with the immune system and to induce chronic inflammation resulting in a series of chronic diseases, but systematically collected data are limited.4
In BMDJ, increased levels of inflammatory messengers have been found, with RANTES/CCL5 (chemotactic cytokine ligand 5) being the most prominent in different patient populations, whereas tissue concentrations of other cytokines like CRP or TNF- α remain low.4–9 As a proinflammatory cytokine, RANTES/CCL5 is produced at high levels by platelets, macrophages, eosinophils, and fibroblasts, as well as endothelial, epithelial, and endometrial cells in response to a broad array of infectious and inflammatory stimuli to guide the recruitment of immune cells into the damaged or infected tissue.10 During BMDJ, an initially compensatory local inflammation occurs in response to tissue damage by tooth extraction, root resection, and dental implantation. This localized inflammation may then develop into a chronic inflammatory response that involves significantly elevated RANTES/CCL5 levels.11 The significance of RANTES/CCL5 expression for multiple inflammatory processes and disorders12 suggests a potential contributing role of BMDJ in the pathogenesis of systemic disorders.4–6,8,9
In BMDJ tissue samples derived from patients with different diseases, RANTES/CCL5 levels are up to 30-fold increased when compared to healthy controls.4–6,8 Preliminary results suggesting that BMDJ therapy reduces RANTES/CCL5 serum levels6 have not been confirmed so far, and there are no systematic assessments on appropriate treatment strategies. Basically, tooth extractions and primary or secondary root canal treatments might be indicated. Another more comprehensive approach is the surgical removal of dead tissue, debris, and diseased bone, followed by the reconstruction of bone tissue by the use of platelet-rich plasma.13
In this article, we therefore asked if BMDJ therapy under real-world conditions significantly reduces serum levels of RANTES/CCL5 and other inflammatory cytokines. In this respect, we retrospectively compared the efficacy of different approaches, including specific BMDJ surgery involving bone tissue reconstruction and micronutrient supplementation, tooth extractions, and root canal treatments in 113 walk-in patients of a general practice between November 2020 and February 2022.
Materials and Methods
Study Design
The study period of this retrospective assessment was between November 2020 and February 2022. Walk-in patients of a general practice were eligible to participate if the patient’s dental history was obtained by means of a standardized questionnaire, if the oral cavity was examined during the visit, and if RANTES/CCL5 serum concentrations were assessed at least twice during the study period (before and after the intervention). Patients with any malignant disease were excluded.
In the interventional group, BMDJ was treated by BMDJ surgery, tooth extraction, or root canal treatment. Patients of the control group received no dental treatment during the time period between the two assessments of RANTES/CCL5 serum concentrations. The appropriate BMDJ therapy was chosen by the treating dentist. All treatment decisions were independent of the study participation, and all patients provided informed consent before participation. Biosamples and patient data were collected during routine medical care. Ethical approval was qualified as unnecessary by the committee in charge (Luxembourg National Research Ethics Committee, CNER) due to the retrospective character of the study. The study complies with the standards of the Declaration of Helsinki.
In this study, the BMDJ incidence in the study population and the RANTES/CCL5 serum concentrations before and after treatment were assessed as outcome parameters. The differences of RANTES/CCL5 serum concentrations were compared between untreated (patients not or not yet assessed or treated by the dentist) and treated patients as well as among differentially treated patients.
Procedures
BMDJ Diagnosis
BMDJ was suspected on the basis of the patient’s dental history and dental examinations (history of tooth extraction, root resection, dental implantation, amalgam fillings), X-ray examinations of the jaw, and elevated serum concentrations of RANTES/CCL5, C-reactive protein (CRP), and Tumor Necrosis Factor-α (TNF-α). BMDJ diagnosis was then confirmed by imaging techniques such as computed tomography, digital volume tomograms or through-transmission alveolar ultrasonography. Figure 1 shows the outcome of an X-Ray in comparison to a CT-scan, whereas Figure 2 shows a BMDJ adjacent to an implantation site.
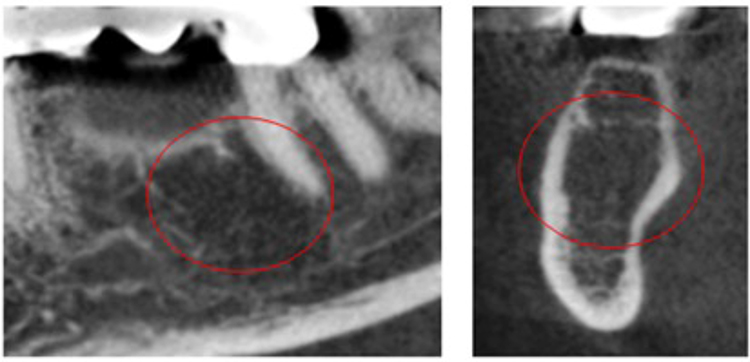 |
Figure 1 BMDJ barely detected on X-Ray (left, area in the red circle), confirmed by CT-scan (right, area in the red circle). |
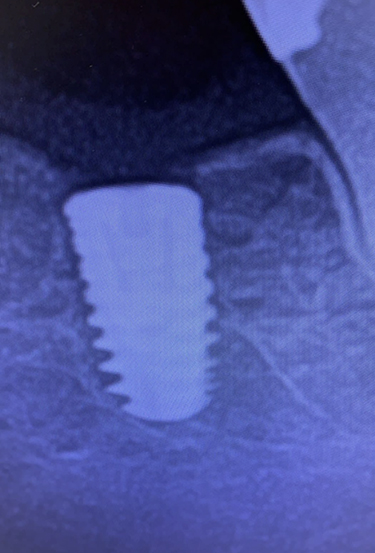 |
Figure 2 X-Ray of a BMDJ of an implantation site. |
Interventions
BMDJ therapies delivered during the study period consisted of BMDJ surgery, tooth extraction, and root canal treatment. BMDJ surgery was performed by three independent dentists and involved the supplementation with micronutrients to support healing after surgery, beginning several weeks before surgery and continuing for 6 months after surgery (target range of 25-hydroxy vitamin D: 70–100 ng/mL; LDL-cholesterol ≤120 mg/dl). During surgery, the gingiva and bone were cut and opened under local anesthesia to expose the affected tooth area. Dead tissue, debris, and diseased bone tissue were surgically removed. Local anesthesia was extended by covering the treated area with a procaine-soaked compress for 20 minutes, followed by thorough disinfection with ozone.14 Bone defects were then repaired by applying platelet-rich fibrin (PRF) that had been obtained by centrifugation of the patient’s blood as described.15,16 The wound was then closed with absorbable material. The other procedures, tooth extractions and root canal treatments, were performed by the treating dentist. Although root canal treatments were not performed by the authors of the study, it is safe to assume that all treatments were performed in accordance with current treatment techniques and quality standards.17,18 Figures 3 and 4 depict the through-transmission alveolar ultrasound findings before and after surgery.
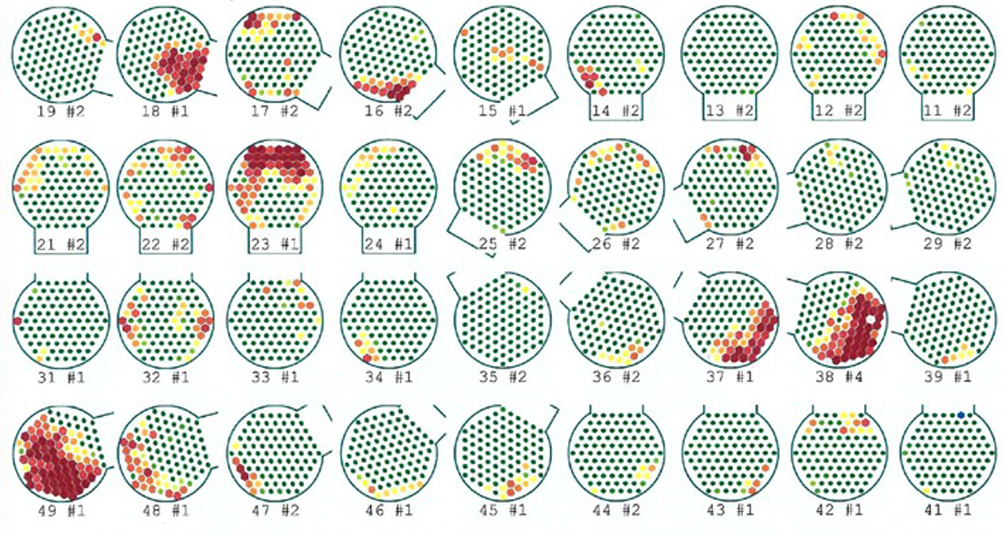 |
Figure 3 Through-transmission alveolar ultrasound screening on a patient presenting a normal X-Ray: confirmation of several BMDJ (red areas). |
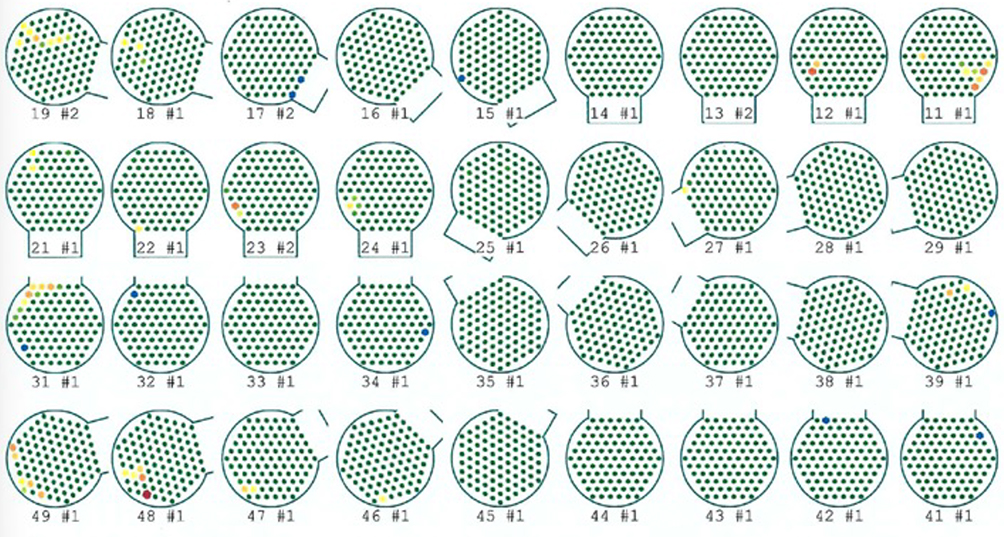 |
Figure 4 Post-treatment through-transmission alveolar ultrasound on the same patient confirming normal bone density. |
Cytokine and Chemokine Levels
During the study period, peripheral blood was drawn at any time before and after treatment (interventional group) and at the beginning and end of the study (control group) for the analysis of RANTES/CCL5, CRP, and TNF-α serum levels using standard laboratory techniques. The time between end of treatment and follow-up assessments was recorded.
Statistics
Statistics were mostly descriptive (mean ± standard deviation). Significant differences between independent variables were determined by the two-sample t-test. The outcomes of the different treatment modalities were additionally assessed by Bonferroni post hoc tests with ANOVA for multiple comparisons. The latest version of SPSS Statistics was used.
Results
Patient Characterization
Out of 1471 registered participants, 113 fulfilled the inclusion criteria of two available RANTES/CCL5 measurements (755 participants provided only one RANTES/CCL5 measurement). The characteristics of the included patient population are depicted in Table 1. Out of the 113 patients included, 57 received no treatment, 25 were treated by BMDJ surgery, and 20 and 11 patients were treated by tooth extraction and root canal treatment, respectively.
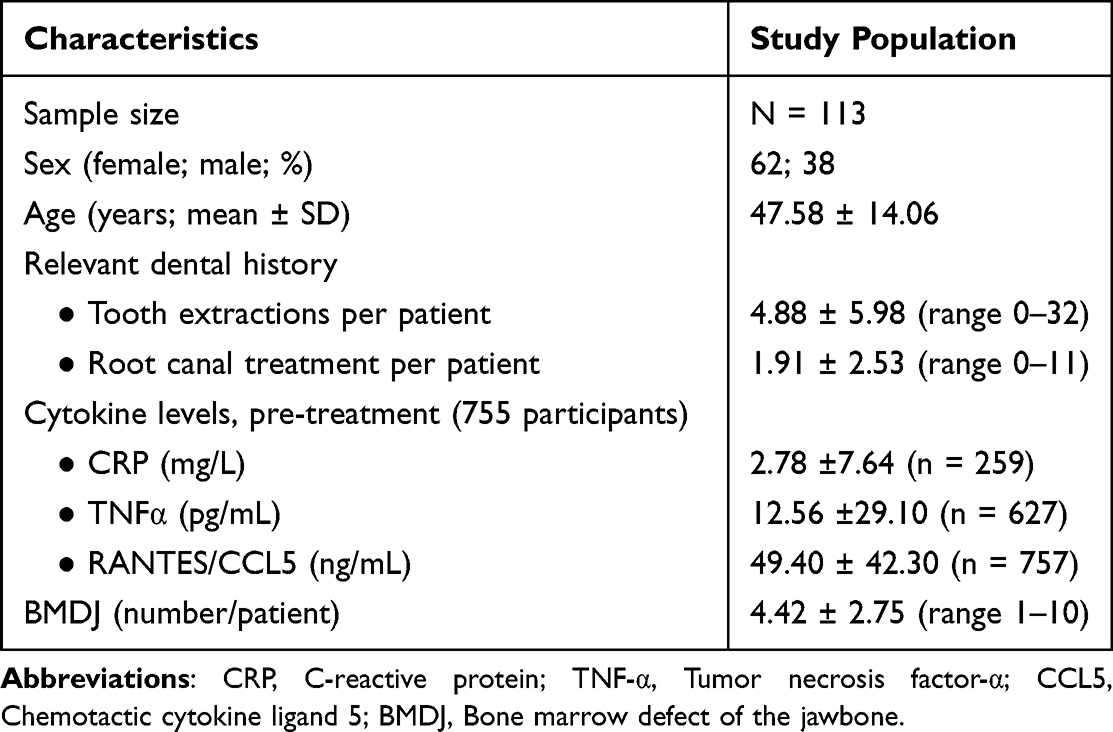 |
Table 1 Characteristics of Patients |
Correlation analyses revealed that increased age positively correlated with both dental history (number of tooth extractions and root canal treatment) and higher RANTES/CCL5 serum concentrations before treatment (p < 0.001). RANTES/CCL5 concentrations correlated with CRP levels (p < 0.001). BMDJ were detected in virtually all patients included. The number of BMDJ per patient was 4.42 ± 2.75. The number of BMDJ per patient did not correlate with RANTES/CCL5 serum levels.
RANTES/CCL5 Serum Levels Before and After Treatment
BMDJ surgery, tooth extraction, and root canal treatment markedly reduced RANTES/CCL5 serum concentrations (Figure 5). It is important to note that RANTES/CCL5 levels further increased during the study period in untreated control subjects, with a mean increase of 8 ng/mL at the second measurement.
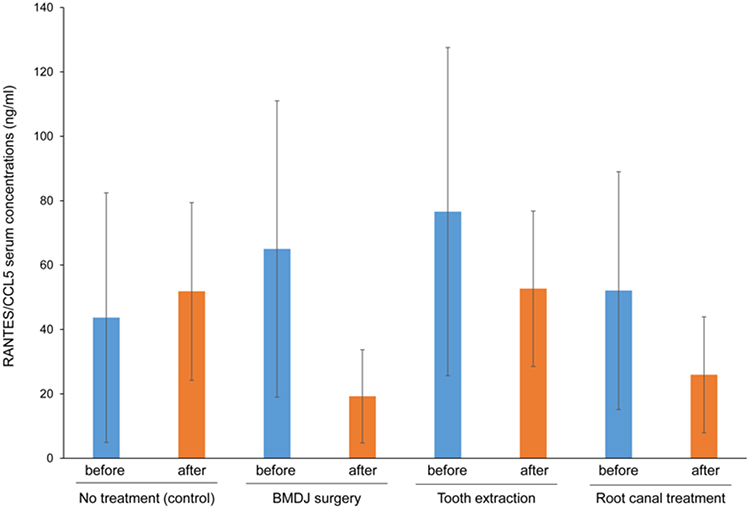 |
Figure 5 RANTES/CCL5 serum concentrations before and after dental therapy. Abbreviation: BMDJ, Bone marrow defect of the jawbone. |
Comparison of RANTES/CCL5 levels obtained before and after treatment revealed a significant reduction of RANTES/CCL5 serum levels by any treatment when compared to no treatment (p < 0.001; effect size d = 0.90). This effect was even more pronounced if BMDJ surgery was directly compared with no treatment (p < 0.001; effect size d = 1.30; Figure 6).
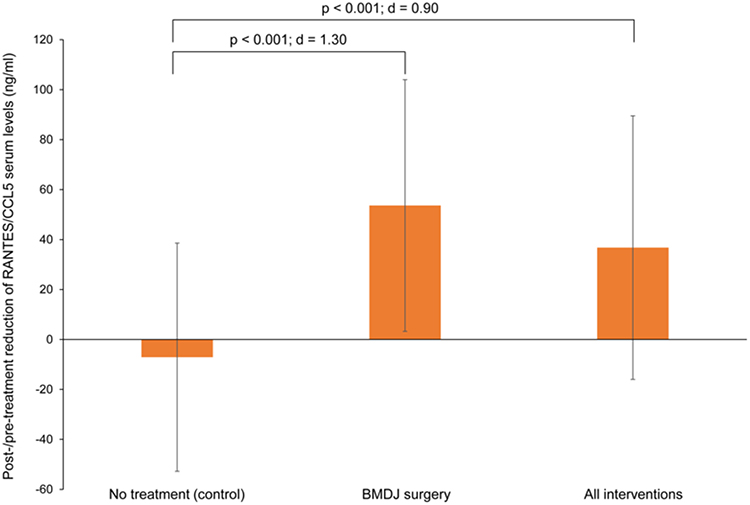 |
Figure 6 Post-/pre-treatment reduction of RANTES/CCL5 serum concentrations. Abbreviation: BMDJ, Bone marrow defect of the jawbone. |
Interestingly, statistically significant effects on RANTES/CCL5 serum levels as assessed by Bonferroni-corrected post-hoc analyses were exclusively found for BMDJ surgery (p < 0.001) and tooth extraction (p = 0.014). The mean duration between pre- and post-treatment RANTES/CCL5 measurements was 22.86 ± 19.36 weeks. However, the length of the time interval between both measurements did not correlate with the extent of RANTES/CCL5 reduction in any interventional group and in the total sample (p = 0.104).
Discussion
Here, we report that in real-world practice, BMDJ surgery, tooth extraction, and root canal treatment markedly reduce RANTES/CCL5 serum concentrations in BMDJ patients. Among these therapeutic approaches, BMDJ surgery showed the most beneficial effect on RANTES/CCL5 levels. In untreated BMDJ patients, however, RANTES/CCL5 levels further increased during the study period.
In most publications, RANTES/CCL5 concentrations have been assessed in necrotic tissue samples of the diseased jawbone. In comparison to healthy control jawbone tissue, RANTES/CCL5 levels were increased in BMDJ tissue samples, in a range from 17-fold6 to 36-fold.9 In most of these studies, patients had different systemic and local diseases such as atypical facial and trigeminal pain, neurodegenerative diseases, tumors, rheumatism, chronic fatigue syndrome5,8,9,19 or malignancies such as breast cancer.6 Serum levels of RANTES/CCL5 in BMDJ patients have only been reported in a single publication. This publication showed the reduction of serum RANTES/CCL5 by BMDJ surgery in a very small group of patients.6 In our study, we now demonstrate that different BMDJ surgical and dental treatment approaches significantly reduce RANTES/CCL5 serum concentrations. BMDJ surgery seems to outperform tooth extraction and root canal treatment. However, this effect might not be clearly attributable to methodological differences in, for example, surgical procedures and supplementation with micronutrients, as patients of other interventional groups as well as control patients may have also received, for example, vitamin D supplementation. Our study was performed under real-world conditions, with individual treatment decisions being made exclusively by the dentist.
Considering the involvement of RANTES/CCL5 in various pathological processes, there is no reasonable potential for low RANTES/CCL5 serum levels as an exclusion marker for BMDJ diagnosis. It is conceivable, however, that RANTES/CCL5 serum levels might support imaging-based BMDJ diagnosis and might help monitor treatment success, whereby no definite cut-off value of RANTES/CCL5 serum concentrations could be identified in our study. Nonetheless, individual comparisons between pre- and post-treatment RANTES/CCL5 serum levels would provide good indications for treatment failure or success.
We recognized the following two major limitations in our study. First, the low sample size of each experimental group might limit the generalizability of our results, as RANTES/CCL5 values generally show a high degree of individual variability. Second, the fact that BMDJ was observed in all patients contradicts earlier study results which demonstrate an incidence of jaw osteonecrosis in, for example, 5% of cancer patients receiving high-dose intravenous bisphosphonates.20 This discrepancy might result from the heterogeneity of both the diagnostic modalities employed and the experience of the dentists involved. It further underlines the need for an improved guidance on BMDJ diagnostic procedures.
Conclusion
The authors hypothesize that BMDJ surgery, tooth extraction, and root canal treatment reduce RANTES/CCL5 serum concentrations in BMDJ patients. BMDJ surgery showed the most beneficial effect on RANTES/CCL5 levels. Further research and is now required to establish RANTES/CCL5 assessments as part of improved diagnostic and therapeutic strategies for BMDJ therapy.
Acknowledgments
We thank Dr Stefan Lang for his assistance during the development of this paper.
Disclosure
The authors report no conflicts of interest related to this study.
References
1. Bouquot JE, Roberts AM, Person P, Christian J. Neuralgia-inducing cavitational osteonecrosis (NICO). Osteomyelitis in 224 jawbone samples from patients with facial neuralgia. Oral Surg Oral Med Oral Pathol. 1992;73(3):307–319. doi:10.1016/0030-4220(92)90127-c
2. Naderi S, Merchant AT. The association between periodontitis and cardiovascular disease: an update. Curr Atheroscler Rep. 2020;22(10):52. doi:10.1007/s11883-020-00878-0
3. Sanz M, Marco Del Castillo A, Jepsen S, et al. Periodontitis and cardiovascular diseases: consensus report. J Clin Periodontol. 2020;47(3):268–288. doi:10.1111/jcpe.13189
4. Lechner J, von Baehr V. RANTES and fibroblast growth factor 2 in jawbone cavitations: triggers for systemic disease? Int J Gen Med. 2013;6:277–290. doi:10.2147/ijgm.s43852
5. Lechner J, Schmidt M, von Baehr V, Schick F. Undetected jawbone marrow defects as inflammatory and degenerative signaling pathways: chemokine RANTES/CCL5 as a possible link between the jawbone and systemic interactions? J Inflamm Res. 2021;14:1603–1612. doi:10.2147/jir.s307635
6. Lechner J, Schulz T, Lejeune B, von Baehr V. Jawbone cavitation expressed RANTES/CCL5: case studies linking silent inflammation in the jawbone with epistemology of breast cancer. Breast Cancer. 2021;13:225–240. doi:10.2147/bctt.s295488
7. Lechner J, Schulz T, von Baehr V. Immunohistological staining of unknown chemokine RANTES/CCL5 expression in jawbone marrow defects-osteoimmunology and disruption of bone remodeling in clinical case studies targeting on predictive preventive personalized medicine. EPMA J. 2019;10(4):351–364. doi:10.1007/s13167-019-00182-1
8. Lechner J, von Baehr V. Peripheral neuropathic facial/trigeminal pain and RANTES/CCL5 in jawbone cavitation. Evid Based Complement Alternat Med. 2015;2015:582520. doi:10.1155/2015/582520
9. Lechner J, von Baehr V, Schick F. RANTES/CCL5 signaling from jawbone cavitations to epistemology of multiple sclerosis - research and case studies. Degener Neurol Neuromuscul Dis. 2021;11:41–50. doi:10.2147/dnnd.s315321
10. Griffith JW, Sokol CL, Luster AD. Chemokines and chemokine receptors: positioning cells for host defense and immunity. Annu Rev Immunol. 2014;32:659–702. doi:10.1146/annurev-immunol-032713-120145
11. Turner MD, Nedjai B, Hurst T, Pennington DJ. Cytokines and chemokines: at the crossroads of cell signalling and inflammatory disease. Biochim Biophys Acta. 2014;1843(11):2563–2582. doi:10.1016/j.bbamcr.2014.05.014
12. Zeng Z, Lan T, Wei Y, Wei X. CCL5/CCR5 axis in human diseases and related treatments. Genes Dis. 2022;9(1):12–27. doi:10.1016/j.gendis.2021.08.004
13. Liu Y, Sun X, Yu J, et al. Platelet-rich fibrin as a bone graft material in oral and maxillofacial bone regeneration: classification and Summary for better application. Biomed Res Int. 2019;2019:3295756. doi:10.1155/2019/3295756
14. Domb WC. Ozone therapy in dentistry. A brief review for physicians. Interv Neuroradiol. 2014;20(5):632–636. doi:10.15274/inr-2014-10083
15. You JS, Kim SG, Oh JS, Kim JS. Effects of platelet-derived material (Platelet-Rich Fibrin) on bone regeneration. Implant Dent. 2019;28(3):244–255. doi:10.1097/id.0000000000000877
16. Ghanaati S, Herrera-Vizcaino C, Al-Maawi S, et al. Fifteen years of platelet rich fibrin in dentistry and oromaxillofacial surgery: how high is the level of scientific evidence? J Oral Implantol. 2018;44(6):471–492. doi:10.1563/aaid-joi-D-17-00179
17. European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921–930. doi:10.1111/j.1365-2591.2006.01180.x
18. Jain A. Principles and Techniques of Exodontia. In: Bonanthaya K, Panneerselvam E, Manuel S, Kumar VV, Rai A, editors. Oral and Maxillofacial Surgery for the Clinician. Springer Nature Singapore; 2021:259–297.
19. Lechner J, Aschoff J, Rudi T. The vitamin D receptor and the etiology of RANTES/CCL-expressive fatty-degenerative osteolysis of the jawbone: an interface between osteoimmunology and bone metabolism. Int J Gen Med. 2018;11:155–166. doi:10.2147/ijgm.s152873
20. Reid IR, Cornish J. Epidemiology and pathogenesis of osteonecrosis of the jaw. Nat Rev Rheumatol. 2011;8(2):90–96. doi:10.1038/nrrheum.2011.181
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.