")
Back to Journals » Orthopedic Research and Reviews » Volume 15
Reconstruction After En Bloc Resection of a Distal Radius Tumor. An Updated and Concise Review
Authors Chobpenthai T , Poosiripinyo T , Warakul C
Received 22 May 2023
Accepted for publication 31 July 2023
Published 8 August 2023 Volume 2023:15 Pages 151—164
DOI https://doi.org/10.2147/ORR.S416331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Thanapon Chobpenthai,1 Thanate Poosiripinyo,2 Chawin Warakul1
1Princess Srisavangavadhana College of Medicine, Chulabhorn Royal Academy, Bangkok, Thailand; 2Department of Orthopaedics, Khon Kaen Hospital, Khon Kaen, Thailand
Correspondence: Thanapon Chobpenthai, Princess Srisavangavadhana College of Medicine, Chulabhorn Royal Academy, 906 Kamphaengphet 6 Road, Talat Bang Khen, Lak Si, Bangkok, 10210, Thailand, Tel +662-576-6000, Fax +662-576-6904, Email [email protected]
Abstract: The distal radius is rarely affected by either primary or metastatic bone cancers. The most frequent tumors of the distal radius are giant cell tumors, which are benign tumors with the propensity to invade. En bloc excision of giant cell tumors of the distal radius achieves a low recurrence rate but compromises the wrist joint, necessitates a significant reconstruction, and has functional consequences. Reconstruction after en bloc resection of a distal radius bone tumor is challenging. Furthermore, orthopedic oncologists disagree on treating such long bone anomalies most effectively. The present article summarizes the various biological and non-biological reconstruction techniques performed after en bloc resection of a distal radius tumor, discusses the advantages and disadvantages of each reconstruction strategy, and summarizes several case studies and case reports.
Keywords: benign bone tumor, giant cell tumor, en bloc resection, reconstruction technique, distal radius tumor
Introduction
Giant cell tumors (GCTs) comprise only 5% of primary bone tumors and 20% of benign bone tumors.1 GCT most frequently affects adults between the ages of 20 and 40 and is more common in females than males.2,3 The cell types most frequently contained in GCTs are mononuclear histiocytic cells, large multinucleated cells resembling osteoclasts, and neoplastic stromal cells, the significant proliferative cell populations.4,5 The condition is typically regarded as low-grade or borderline and has certain invasive traits supported by biological activities.6,7 The main issue with treating GCT is local recurrence after surgery. The recurrence rate is 27–65% following isolated curettage, 0–12% after en bloc resection, and 12–27% after curettage in addition to adjuvants like phenol, high-speed burring, polymethyl methacrylate, or liquid nitrogen.6
The distal ulna and radius are the fourth most frequent site for bone GCTs (9% of cases), following the distal femur, proximal tibia, and proximal femur.8,9 Numerous studies have reported that the distal ulna and radius are especially susceptible to GCT recurrence after resection. The best way to treat GCTs of the distal ulna and radius remains controversial.10,11 En bloc excision of a GCT in the distal radius achieves decreased recurrence rates but compromises the wrist joint, necessitates a significant reconstruction, and negatively affects the wrist function. Even when combined with surgical adjuvants like phenol, liquid nitrogen, or cement, intralesional excision (curettage) still carries a significant risk of local recurrence.10,12 For malignant tumors of the distal radius, cancer surgery guidelines recommend en bloc excision of the tumor with substantial margins.
As the wrist has high functional requirements, wrist reconstruction after en bloc a distal radius bone tumor is quite difficult for orthopedic oncologists (Figure 1). Long bone defects have been repaired using various methods; however, orthopedic oncologists disagree on the best strategy.13,14 The present article summarizes the different reconstruction techniques performed after en bloc distal radius tumors (Figure 2).
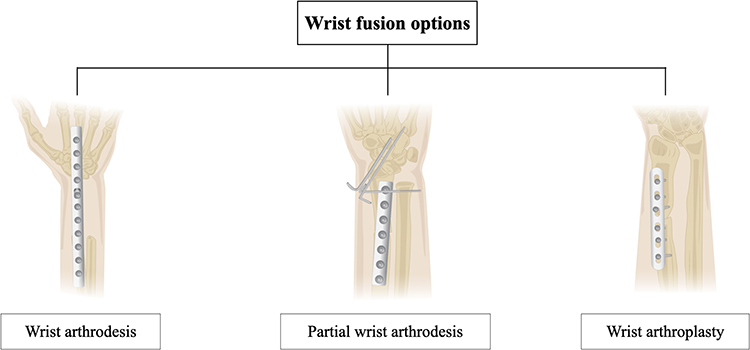 |
Figure 1 Wrist fusion options. |
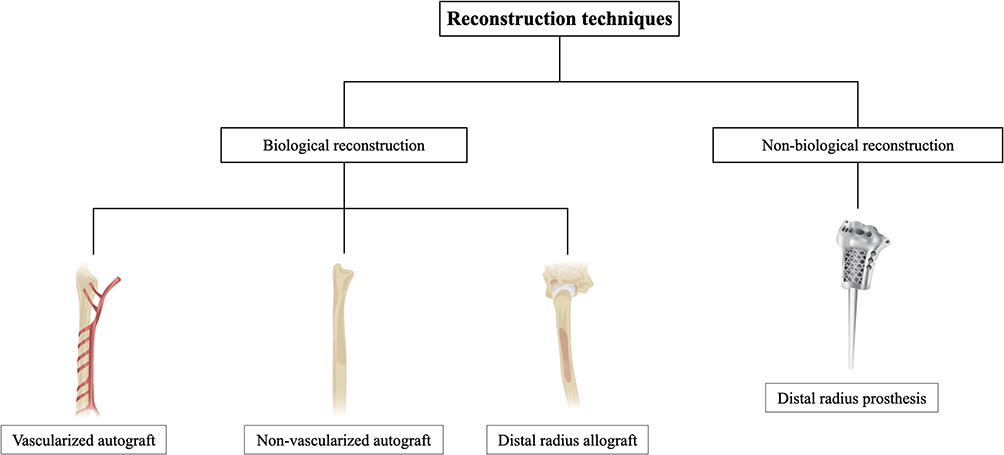 |
Figure 2 Reconstruction techniques for distal radius. |
Reconstruction Techniques
Biological Reconstruction
Non-Vascularized Fibular Graft
The fibula has been used as an autogenous graft in limb reconstruction for many years. The fibula has been used to reconstruct the distal radius following GCT removal.15 The fibrous fibular autograft has also provided mechanical support for the cervical spine after a corpectomy for spondylotic disease.16 Furthermore, fibular grafts have been used to reconstruct a wide variety of anatomical features, including the humerus, metatarsus, pelvis, and hip,17,18 and for mandibular repair after the removal of cancerous maxillofacial tumors.19 The fibular graft may be vascularized or non-vascularized, depending on whether a blood supply is transferred along with the bone graft. The optimal type of reconstruction graft is not established in the literature. One study reported that non-vascularized fibular autograft reconstruction and extensive excision of benign and malignant aggressive GCTs of the distal radius in 13 patients achieved satisfactory functional outcomes without jeopardizing the prognosis.20
Fibrous autografts have long been used to restore traumatic and non-traumatic bone abnormalities in adult and pediatric populations.21 Non-vascularized graft reconstructions are less expensive, quicker, and easier to carry out than vascularized fibular graft reconstructions.22 Another benefit of the non-vascularized graft method is subperiosteal dissection, which speeds up the regeneration of the resected fibula.23 Non-vascularized fibular autografts are widely used to successfully reconstruct massive bone defects from malignant pediatric bone tumors.21 Non-vascular fibular autografts retain the carpus architecture and wrist functionality. Using a non-vascularized fibular autograft also has no chance of viral transmission.24
Vascularized Fibular Graft
Pho was the first to use a free vascularized fibular head graft to rebuild a long bone defect after removing a tumor of the distal radius.25 The free vascularized fibular graft has been widely used to reconstruct the significant bone defect and articular surface after the surgical removal of the distal radius.26,27 The vascularized fibular head autograft also has intrinsic vascularity, which is particularly important if the lesion is larger than 10 cm.28 As well as achieving comparable functional results to non-vascularized fibular head autograft restoration, the vascularized fibular head autograft method minimizes bone collapse brought on by limited blood flow from the transplanted fibular head and promotes fast healing. In distal radius reconstruction following tumor resection, the vascularized fibular head autograft reportedly produces satisfactory treatment outcomes, with a short fusion time, high fusion rate, and no complications such as bone resorption or transplanted fibular head disintegration.29,30 However, this technique is highly time-consuming, technically challenging, and requires a high skill level.
The best type of graft for reconstruction is not demonstrated in the literature. Vascularized grafts may raise complications’ risk without enhancing union rates.31 However, a study of 53 adult and pediatric patients who underwent reconstruction after resection of primary bone sarcoma found no discernible difference in the union rates of vascularized versus non-vascularized grafts (p = 0.167).32
Ulnar Translocation
Ipsilateral ulnar translocation is a simple and cheap method that does not require microvascular expertise and can be completed more quickly than free vascularized fibular grafting. Skin closure following tumor excision is facilitated by the loss in forearm volume caused by the radial displacement of the ulna, mainly when there has been considerable soft tissue. Morbidity is decreased because the surgical process is limited to the same limb. Infection may be reduced by the relatively short surgical procedure and by using a graft with a continuous blood supply. Maintaining the vascularity of the graft also increases the likelihood of union, which occurs more quickly than with a non-vascularized graft.33,34
The most frequent complication of ipsilateral ulnar translocation is delayed union or non-union of the proximal radio-ulnar junction. This necessitates autogenous cancellous bone grafting and modification of the internal fixation.35 The reduced union rate is likely due to micromovement at the osteotomy site caused by the placement of a longitudinal pin to stabilize the radio-ulnar junction. As plates and screws offer more excellent fixation and provide a favorable biological and mechanical environment for bony union, these are frequently used to stabilize the construct.36 One patient with a GCT of the distal radius was effectively treated with a large local excision, ulnar translocation, and wrist arthrodesis;37 the patient exhibited an outstanding functional performance after two years of follow-up, with good supination and pronation ranges of motion and no localized recurrence.
Tibial Cortical Strut
A tibial cortical strut may preserve the wrist extensors and is recommended for minor forearm resections.38 Lauthe et al performed a study of 104 patients who underwent reconstruction of extended bone defects with a tibial strut autograft.39 Four patients experienced morbidity at the donor site. One patient had a stress-fractured tibia that required an osteotomy to be repaired using varus distortion. Two patients’ evacuation of hematoma was needed, while one patient required fasciotomies to treat anterior compartment syndrome. At five years postoperatively, the overall likelihood of union was 90%. Time to union was correlated with the bone integrity (p = 0.006), reconstruction technique (p = 0.018), and tibial graft size (p = 0.037).
Iliac Crest Autograft
An iliac crest autograft possesses the crucial traits of being osteoconductive, osteoinductive, and osteogenic and is frequently regarded as the gold standard for defect reconstruction. However, the most frequent donor site morbidity associated with iliac crest autografting is pain at the graft harvest site. Numerous bone graft extenders have been created to reduce pain at the iliac autograft site, but there is only weak evidence to support their usefulness. Many patients do not consent to the harvest of iliac crest autografts because of the potential pain.40 Furthermore, the results of harvesting the anterior and posterior crests vary. Compared with posterior iliac crest autograft harvests, anterior iliac crest autograft harvests are associated with a higher rate of complications, including more iliac wing fractures, postoperative hematomas, and sensory abnormalities. The patient frequently feels more pain owing to the harvest than the treatment itself, with the posterior route being associated with greater levels of postoperative pain than the anterior method. A significant amount of autogenous bone can be obtained from the all-cancellous iliac crest bone graft harvest for various surgeries, such as spinal fusion and bony reconstruction. The primary steps of this method mainly involve offsetting the surgical incision, exposing the iliac crest while attempting to avoid neurologic systems, locating and performing an iliac crest corticotomy, harvesting the cancellous bone graft using curettes, and achieving hemostasis followed by completing a faceted closure. It is crucial to initiate weight-bearing as soon as tolerated postoperatively.41
Approximately 6% to 39% of patients who undergo posterior iliac crest bone graft (ICBG) harvest report chronic donor site pain.42,43 These figures demonstrate that morbidity related to autologous iliac crest harvest is very common. However, Banwart et al reported that severe and numerous minor ICBG-related problems could be prevented with appropriate procedural improvements.44 Other studies have emphasized how challenging it is for patients to distinguish between donor site discomfort and lingering lower back pain after surgery.45,46 Therefore, the current literature may have exaggerated the discomfort associated with posterior ICBG harvesting.
Vascularized Ulnar Transposition
The mucoperiosteal cuff is composed of the abductor pollicus longus, ulnar head of the deep digital flexor, and pronator quadratus, and is essential to the ipsilateral vascularized ulnar transposition technique. The ulnar transposition technique can reduce the radius by up to 40%. As the styloid processes and radius are removed concurrently, there is no need to dissect the styloid process and the tumor. Most of the ulnar transplant (90%) is implanted into the defect.47 The ulnar head of the deep digital flexor is unaltered distally and proximally, the pronator quadratus is transected both distally and proximally, and the abductor pollicus is transected both distally and proximally. An appropriately sized dynamic compression plate connects the distal side of the third or fourth metacarpal bone to the proximal radius. The ulnar graft is then placed using two screws.47
The position of an ipsilateral vascularized ulnar autograft has numerous potential benefits. The graft accomplishes clinical union quickly and results in minimal bone resorption because of its preserved blood supply. Furthermore, the graft experiences hypertrophy and have good resistance to infection. As the graft is extracted from the same limb, there is minor morbidity and a short surgical time, and microvascular anastomosis is not required. These factors may lower the possibility of fatigue fractures, implant failure, and infection. However, using an ipsilateral vascularized ulnar autograft may have disadvantages such as incomplete tumor removal, caudal interosseous artery and vein injury during tapping, drilling, and screw placement, and limb shortening because of the removal of a portion of the styloid process along with the ulna. Furthermore, the surgical margins of the tumor may be compromised to protect the soft tissue connections on the ulna and the caudal interosseous blood vessels.48
One case report describes radioulnoscapholunate fusion facilitated by reconstruction with a vascularized ulnar transposition flap that was fixed with the help of a long-stem contralateral variable angle by locking the volar distal radius plate in a dorsal position.49 This case demonstrated the interdisciplinary handling of a complex reconstructive challenge and a unique fixation method that repurposed well-known, easily accessible hardware to produce the best possible osteosynthesis.
Allograft
Surgeons often choose allograft reconstruction to cover the bone defect following resection. This method carries a significant risk of non-union of the host-to-graft bone interface, with reported non-union rates ranging from 8.3% to 25% for a transverse cut.50 However, one study reported a non-union rate for distal radius allograft reconstruction using a step-cut technique of 0% in 11 patients after a mean follow-up duration of 153 months.51 Furthermore, an excellent long-term survival rate has been reported after osteoarticular allograft reconstruction and en bloc GCT excision.52
Non-Biological Reconstruction
Wrist Prosthetic Replacement
Prosthetic wrist repair is less commonly used than other reconstruction techniques. Still, it may be an option for patients who are apprehensive about the morbidity of harvesting fibular head autografts or in situations where there are no available allografts. Patients with a short life expectancy should consider a prosthetic replacement. This reconstructive approach primarily benefits repairing extended bone defects without graft-related problems like non-union, bone absorption, donor-site morbidity, and delayed union.53 3D-printed prostheses can restore bone anatomy after precise and thorough removal of tumors; In addition, when it is necessary to increase the stability of the prosthesis and the bone, fixation holes can be prefabricated in the prosthesis to maximize the recovery of normal limb function after surgery.
The two types of wrist prostheses are the unipolar prosthesis and the complete wrist prosthesis.54,55 Although unipolar prostheses reportedly achieved adequate postoperative functional results in early trials, the relatively high complication rate must be considered. One study reported that wrist reconstruction using a specially constructed unipolar prosthesis achieved a normal hand grip strength of around 68%; however, 60% of patients developed problems related to their prosthesis.56 Contrary to the findings of several other studies, Zhang et al found no issues related to the prosthesis in patients who underwent wrist reconstruction using personalized unipolar prostheses.57
One of the most frequent adverse effects after unipolar hemiarthroplasty is subluxation. After resecting the distal radius, the wrist is rebuilt using a whole wrist prosthesis to achieve a more secure wrist joint. The entire wrist prosthesis achieves a stable wrist joint and satisfactory postoperative performance.58,59 However, one study reported two patients who required revision surgery due to a failed wrist arthroplasty using a complete wrist prosthesis.60
The most frequent reason for prosthesis replacement failure is aseptic displacement. Three-dimensional technology based on mechanical-biological reconstruction may significantly lower the rate of prosthesis loosening.61 One study reported that wrist reconstruction using a three-dimensional, printed, uncemented tailored prosthesis produced satisfactory postoperative functional results without problems related to the prosthesis.62 However, the average duration of follow-up was just 14.45 months. Additionally, degenerative alterations in the restored wrist were imminent and may be brought on by decreased wrist motion and unfavorable prosthetic-bone contact.
Total Wrist Arthrodesis
Total wrist arthrodesis may result in a stable wrist with no discomfort; this method can also minimize several issues related to arthroplasty, such as subluxation, displacement, and degenerative alterations in the wrist joint, and therefore avoids the pain induced by these issues. As a result, this reconstructive procedure is frequently used in patients who must perform strenuous physical activities. Total wrist arthrodesis is the preferred treatment when wrist arthroplasty fails.63,64
Total wrist arthrodesis with a large allograft has some benefits, including a technically easy surgery and no donor-site-related morbidity. However, using an allograft has disadvantages, such as higher rates of non-union and fracture.50,65 Therefore, some surgeons oppose allograft reconstruction, and autogenous grafts are more widely used.
Partial Wrist Arthrodesis
Although total wrist arthrodesis achieves a strong and secure wrist joint, patients may find it challenging to carry out everyday tasks due to the lack of wrist motion. In contrast, partial wrist arthrodesis preserves the metacarpal joint, improving quality of life. The three types of partial wrist arthrodesis are radio-lunate fusion, radio-scaphoid-lunate fusion, and radio-scaphoid fusion.66
Zhu et al reported that partial wrist arthrodesis and wrist arthroplasty produce different functional and radiological results. Partial wrist fusion reportedly achieves a stable and robust wrist with good motion, long-term function, and a minimal complication rate.67
The various surgical techniques used for reconstruction after distal radius resection and the associated outcomes reported in the literature are presented in Table 1.
 |
Table 1 Surgical Reconstruction Techniques and Outcomes After Distal Radius Resection |
Wrist Arthroplasty
The real benefit of a wrist arthroplasty over a wrist arthrodesis is that it creates a more movable wrist joint, which enhances the patient’s quality of life. However, in multiple studies, the Disability of Arm, Shoulder, and Hand (DASH) and Musculoskeletal Tumor Society (MSTS) scores indicate that wrist arthrodesis may be preferable to wrist arthroplasty. This may be because wrist motion is not evaluated in the DASH or MSTS scoring methods. The Mayo wrist score may be more reliable and accurate in assessing wrist function after reconstruction.80
Following the removal of the distal radius, a sizeable osteoarticular allograft is recommended for wrist reconstruction due to its excellent wrist-specific compatibility, lack of donor site morbidity, and fair to exceptional functional outcomes. Duan et al reported that osteoarticular allograft reconstruction after the removal of a distal radius tumor produced adequate wrist functionality in all 15 included patients.71 Scoccianti et al reported satisfactory wrist functionality after distal radius tumor resection and reconstruction in 17 patients, with a mean International Society of Limb Salvage-MSTS score of 86% after a mean follow-up of 58.9 months.80
Because of the anatomical commonalities between the proximal fibula and the distal radius, the fibular head autograft is preferred for reconstructing distal radius defects. A non-vascularized fibular head autograft in wrist arthroplasty has produced good and excellent outcomes in numerous studies. Still, it has also been linked to non-union, delayed graft union, bone resorption, and secondary bony collapse of the grafted fibular head.81 The vascularized fibular head autograft may be a good option because of its independent vascularity, mainly if the defect is larger than 10 cm.28 Along with offering comparable functional results to non-vascularized fibular head autograft restoration, the vascularized fibular head autograft promotes fast healing. It minimizes bone collapse by inadequate blood flow from the grafted fibular head.
The vascularized fibular head autograft reportedly produces a favorable functional outcome for reconstructing the distal radius after tumor removal, with a shortened fusion time, greater fusion rate and no complications related to bone resorption or fibular head collapse.30 However, this technique is very time-consuming, technically demanding, and requires a high level of competence. Wrist instability is the most frequent adverse effect of vascularized/non-vascularized fibular head autograft repair. Soft tissue repair techniques have been applied to improve wrist stabilization.10 In addition, an imbalance between the proximal carpal row and the fibular head results in persistent degenerative alterations. However, as young patients undergo joint-surface remodeling, the degenerative changes in such patients are likely to be minimal.
Conclusion
Various procedures have been used to reconstruct the wrist after en bloc resection of distal radius bone tumors (Figure 3). Each strategy has benefits and disadvantages. According to previous reviews and personal experiences, wrist arthroplasty using a vascularized fibular head autograft may be a reasonable choice because this method achieves increased wrist function, sufficient grip strength, and a relatively low complication rate. However, this method requires a microvascular team and prolonged operative time. Vascularized ipsilateral ulnar transposition with partial wrist arthrodesis does not require a microvascular surgeon and takes a shorter operation time but results in limited wrist motion. Tumor recurrence is an essential indicator for selecting reconstruction options that are concerning for one more time of surgery. Orthopedic oncologists should be well-informed about each procedure to choose the most suitable reconstruction approach based on each patient’s specific conditions.
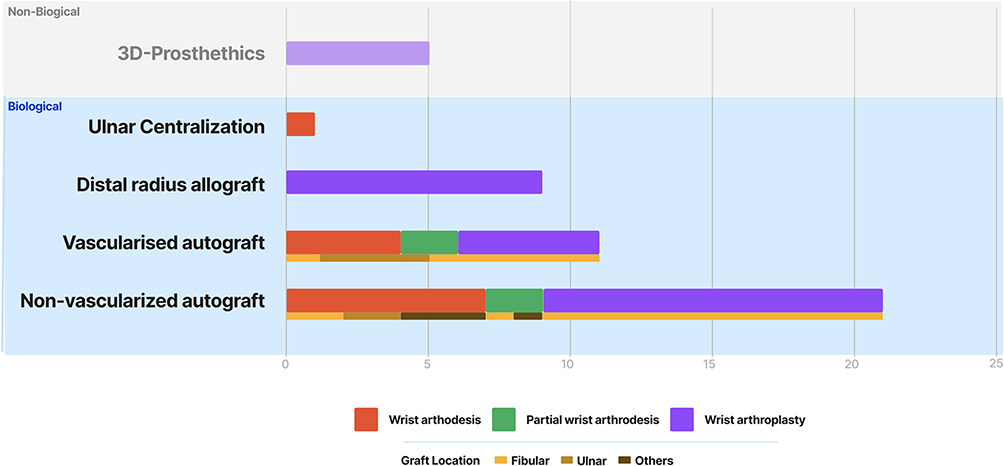 |
Figure 3 Distal radius reconstruction procedures described in the literature. |
Acknowledgments
We thank Kelly Zammit, BVSc, from Edanz (https://www.edanz.com/ac) for editing a draft of this manuscript.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Disclosure
The Authors have no conflicts of interest to declare.
References
1. Vanni D, Pantalone A, Andreoli E, Caldora P, Salini V. Giant cell tumor of the distal ulna: a case report. J Med Case Rep. 2012;6(1):143. doi:10.1186/1752-1947-6-143
2. Raskin KA, Schwab JH, Mankin HJ, Springfield DS, Hornicek FJ. Giant cell tumor of bone. J Am Acad Orthop Surg. 2013;21(2):118–126. doi:10.5435/JAAOS-21-02-118
3. Abramowicz S, Padwa BL. Pediatric head and neck tumors. In: Current Therapy in Oral and Maxillofacial Surgery. Elsevier; 2012:813–820.
4. Werner M. Giant cell tumour of bone: morphological, biological and histogenetical aspects. Int Orthop. 2006;30(6):484–489. doi:10.1007/s00264-006-0215-7
5. Klenke FM, Wenger DE, Inwards CY, Rose PS, Sim FH. Giant cell tumor of bone: risk factors for recurrence. Clin Orthop Relat Res. 2011;469(2):591–599. doi:10.1007/s11999-010-1501-7
6. Chakarun CJ, Forrester DM, Gottsegen CJ, Patel DB, White EA, Matcuk GR. Giant cell tumor of bone: review, mimics, and new developments in treatment. Radiographics. 2013;33(1):197–211. doi:10.1148/rg.331125089
7. Balke M, Schremper L, Gebert C, et al. Giant cell tumor of bone: treatment and outcome of 214 cases. J Cancer Res Clin Oncol. 2008;134(9):969–978. doi:10.1007/s00432-008-0370-x
8. Errani C, Ruggieri P, Asenzio MAN, et al. Giant cell tumor of the extremity: a review of 349 cases from a single institution. Cancer Treat Rev. 2010;36(1):1–7. doi:10.1016/j.ctrv.2009.09.002
9. Niu X, Zhang Q, Hao L, et al. Giant cell tumor of the extremity: retrospective analysis of 621 Chinese patients from one institution. J Bone Joint Surg Am. 2012;94(5):461–467. doi:10.2106/JBJS.J.01922
10. Liu Y-P, K-H L, Sun B-H. Which treatment is the best for giant cell tumors of the distal radius? A meta-analysis. Clin Orthop Relat Res. 2012;470(10):2886–2894. doi:10.1007/s11999-012-2464-7
11. Pazionis TJC, Alradwan H, Deheshi BM, Turcotte R, Farrokhyar F, Ghert M. A systematic review and meta-analysis of en-bloc vs intralesional resection for Giant Cell Tumor of Bone of the distal radius. Open Orthop J. 2013;7(1):103–108. doi:10.2174/1874325001307010103
12. Prosser GH, Baloch KG, Tillman RM, Carter SR, Grimer RJ. Does curettage without adjuvant therapy provide low recurrence rates in giant cell tumors of bone? Clin Orthop Relat Res. 2005;435(435):211–218. doi:10.1097/01.blo.0000160024.06739.ff
13. Saini R, Bali K, Bachhal V, Mootha AK, Dhillon MS, Gill SS. En bloc excision and autogenous fibular reconstruction for aggressive giant cell tumor of distal radius: a report of 12 cases and review of literature. J Orthop Surg Res. 2011;6(1):14. doi:10.1186/1749-799X-6-14
14. Aldekhayel S, Govshievich A, Neel OF, Luc M. Vascularized proximal fibula epiphyseal transfer for distal radius reconstruction in children: a systematic review: Vascularized Fibular Epiphyseal Transfer. Microsurgery. 2016;36(8):705–711. doi:10.1002/micr.22521
15. Murray JA, Schlafly B. Giant-cell tumors in the distal end of the radius. Treatment by resection and fibular autograft interpositional arthrodesis. J Bone Joint Surg Am. 1986;68(5):687–694. doi:10.2106/00004623-198668050-00008
16. Fernyhough JC, White JI, LaRocca H. Fusion rates in multilevel cervical spondylosis comparing allograft fibula with autograft fibula in 126 patients. Spine. 1991;16:S561–S564. doi:10.1097/00007632-199110001-00022
17. Rengsen P, Tiong K, Teo Y, Goh T, Sivapathasundram N. Reconstruction of the second metatarsal with non-vascularised fibular graft following en-bloc resection for giant cell tumour: a case report. Malays Orthop J. 2013;7(3):15–17. doi:10.5704/MOJ.1311.001
18. Akiyama T, Clark JCM, Miki Y, Choong PFM. The non-vascularised fibular graft: a simple and successful method of reconstruction of the pelvic ring after internal hemipelvectomy. J Bone Joint Surg Br. 2010;92(7):999–1005. doi:10.1302/0301-620X.92B7.23497
19. Devireddy SK, Senthil Murugan M, Kishore Kumar RV, Gali R, Kanubaddy SR, Sunayana M. Evaluation of non-vascular fibula graft for mandibular reconstruction. J Maxillofac Oral Surg. 2015;14(2):299–307. doi:10.1007/s12663-014-0657-1
20. Maruthainar N, Zambakidis C, Harper G, Calder D, Cannon SR, Briggs TW. Functional outcome following excision of tumours of the distal radius and reconstruction by autologous nonvascularized osteoarticular fibula grafting. J Hand Surg Br. 2002;27(2):171–174. doi:10.1054/JHSB.2001.0707
21. Sheridan GA, Cassidy JT, Donnelly A, Noonan M, Kelly PM, Moore DP. Non-vascularised fibular autograft for reconstruction of paediatric bone defects: an analysis of 10 cases. Strategies Trauma Limb Reconstr. 2021;15(2):84–90. doi:10.5005/jp-journals-10080-1462
22. Krieg AH, Hefti F. Reconstruction with non-vascularised fibular grafts after resection of bone tumours. J Bone Joint Surg Br. 2007;89(2):215–221. doi:10.1302/0301-620X.89B2.17686
23. Lenze U, Pohlig F, Knebel C, et al. Autologous fibular transplantation for reconstruction of bone defects. Der Orthopäde. 2017;46(8):648–655. doi:10.1007/s00132-017-3442-2
24. Taraz-Jamshidi MH, Gharadaghi M, Mazloumi SM, Hallaj-Moghaddam M, Ebrahimzadeh MH. Clinical outcome of en-block resection and reconstruction with nonvascularized fibular autograft for the treatment of giant cell tumor of distal radius. J Res Med Sci. 2014;19(2):117–121.
25. Pho RW. Malignant giant-cell tumor of the distal end of the radius treated by a free vascularized fibular transplant. J Bone Joint Surg Am. 1981;63(6):877–884. doi:10.2106/00004623-198163060-00003
26. Saikia KC, Borgohain M, Bhuyan SK, Goswami S, Bora A, Ahmed F. Resection-reconstruction arthroplasty for giant cell tumor of distal radius. Indian J Orthop. 2010;44(3):327–332. doi:10.4103/0019-5413.65134
27. Miyamura S, Shigi A, Kraisarin J, et al. Impact of distal ulnar fracture malunion on distal radioulnar joint instability: a biomechanical study of the distal interosseous membrane using a cadaver model. J Hand Surg Am. 2017;42(3):e185–e191. doi:10.1016/j.jhsa.2017.01.008
28. Clarkson PW, Sandford K, Phillips AE, et al. Functional results following vascularized versus nonvascularized bone grafts for wrist arthrodesis following excision of giant cell tumors. J Hand Surg Am. 2013;38(5):935–940.e1. doi:10.1016/j.jhsa.2012.12.026
29. Chung DW, Han CS, Lee JH, Lee SG. Outcomes of wrist arthroplasty using a free vascularized fibular head graft for Enneking stage II giant cell tumors of the distal radius: free Vascularized Fibular Head Graft for Giant Cell Tumor. Microsurgery. 2013;33(2):112–118. doi:10.1002/micr.22028
30. Yang Y-F, Wang J-W, Huang P, Xu Z-H. Distal radius reconstruction with vascularized proximal fibular autograft after en-bloc resection of recurrent giant cell tumor. BMC Musculoskelet Disord. 2016;17:17. doi:10.1186/s12891-016-1211-8
31. Allsopp BJ, Hunter-Smith DJ, Rozen WM. Vascularized versus nonvascularized bone grafts: what is the evidence? Clin Orthop Relat Res. 2016;474(5):1319–1327. doi:10.1007/s11999-016-4769-4
32. Schuh R, Panotopoulos J, Puchner SE, et al. Vascularised or non-vascularised autologous fibular grafting for the reconstruction of a diaphyseal bone defect after resection of a musculoskeletal tumour. Bone Joint J. 2014;96-B(9):1258–1263. doi:10.1302/0301-620X.96B9.33230
33. Cheng CY, Shih HN, Hsu KY, Hsu RW. Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res. 2001;383:221–228. doi:10.1097/00003086-200102000-00026
34. Minami A, Kato H, Iwasaki N. Vascularized fibular graft after excision of giant-cell tumor of the distal radius: wrist arthroplasty versus partial wrist arthrodesis. Plast Reconstr Surg. 2002;110(1):112–117. doi:10.1097/00006534-200207000-00020
35. Bhan S, Biyani A. Ulnar translocation after excision of giant cell tumour of distal radius. J Hand Surg Br. 1990;15(4):496–500. doi:10.1016/0266-7681(90)90102-A
36. Chalidis BE, Dimitriou CG. Modified ulnar translocation technique for the reconstruction of giant cell tumour of the distal radius. Orthopedics. 2008;31:1.
37. Agrawal AC, Garg AK, Choudhary R, Verma S, Dash RN. Giant cell tumor of the distal radius: wide resection, ulna translocation with wrist arthrodesis. Cureus. 2021. doi:10.7759/cureus.15034
38. van de Sande MAJ, van Geldorp NHW, Dijkstra PDS, Taminiau AHM. Surgical technique: tibia cortical strut autograft interposition arthrodesis after distal radius resection. Clin Orthop Relat Res. 2013;471(3):803–813. doi:10.1007/s11999-012-2555-5
39. Lauthe O, Soubeyrand M, Babinet A, Dumaine V, Anract P, Biau DJ. The indications and donor-site morbidity of tibial cortical strut autografts in the management of defects in long bones. Bone Joint J. 2018;100-B(5):667–674. doi:10.1302/0301-620x.100b5.bjj-2017-0577.r2
40. Pirris SM, Nottmeier EW, Kimes S, O’Brien M, Rahmathulla G. A retrospective study of iliac crest bone grafting techniques with allograft reconstruction: do patients even know which iliac crest was harvested? Clinical article. J Neurosurg Spine. 2014;21(4):595–600. doi:10.3171/2014.6.spine13902
41. Shaw KA, Griffith MS, Shaw VM, Devine JG, Gloystein DM. Harvesting autogenous cancellous bone graft from the anterior iliac crest. JBJS Essent Surg Tech. 2018;8(3):e20. doi:10.2106/jbjs.st.17.00068
42. Younger EM, Chapman MW. Morbidity at bone graft donor sites. J Orthop Trauma. 1989;3(3):192–195. doi:10.1097/00005131-198909000-00002
43. Silber JS, Anderson DG, Daffner SD, et al. Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine. 2003;28(2):134–139. doi:10.1097/01.BRS.0000041587.55176.67
44. Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine. 1995;20(9):1055–1060. doi:10.1097/00007632-199505000-00012
45. Howard JM, Glassman SD, Carreon LY. Posterior iliac crest pain after posterolateral fusion with or without iliac crest graft harvest. Spine J. 2011;11(6):534–537. doi:10.1016/j.spine.2010.09.001
46. Delawi D, Dhert WJA, Castelein RM, Verbout AJ, Oner FC. The incidence of donor site pain after bone graft harvesting from the posterior iliac crest may be overestimated: a study on spine fracture patients: a study on spine fracture patients. Spine. 2007;32(17):1865–1868. doi:10.1097/BRS.0b013e318107674e
47. Pooya HA, Séguin B, Mason DR, et al. Biomechanical comparison of cortical radial graft versus ulnar transposition graft limb-sparing techniques for the distal radial site in dogs. Vet Surg. 2004;33(4):301–308. doi:10.1111/j.1532-950X.2004.04044.x
48. Messina A, Messina JC. Transposition of the ulnar nerve and its vascular bundle for the entrapment syndrome at the elbow. J Hand Surg Br. 1995;20(5):638–648. doi:10.1016/s0266-7681(05)80126-3
49. Van Handel AC, Galvez MG, Brogan DM, et al. Vascularized ulnar transposition and radioulnoscapholunate fusion with volar locking plate in a dorsal position following resection of giant cell tumor of the distal radius. Tech Hand Up Extrem Surg. 2020;24(3):142–150. doi:10.1097/BTH.0000000000000282
50. Bianchi G, Donati D, Staals EL, Mercuri M. Osteoarticular allograft reconstruction of the distal radius after bone tumour resection. J Hand Surg Br. 2005;30(4):369–373. doi:10.1016/j.jhsb.2005.04.006
51. Wysocki RW, Soni E, Virkus WW, Scarborough MT, Leurgans SE, Gitelis S. Is intralesional treatment of giant cell tumor of the distal radius comparable to resection with respect to local control and functional outcome? Clin Orthop Relat Res. 2015;473(2):706–715. doi:10.1007/s11999-014-4054-3
52. Albergo JI, Farfalli GL, Cabas-Geat A, Roitman P, Ayerza MA, Aponte-Tinao LA. Does osteoarticular allograft reconstruction achieve long-term survivorship after en bloc resection of grade 3 giant cell tumor of bone? Clin Orthop Relat Res. 2020;478(11):2562–2570. doi:10.1097/corr.0000000000001337
53. Khattak MJ, Umer M, Umar M, Umar M. Autoclaved tumor bone for reconstruction: an alternative in developing countries: an alternative in developing countries. Clin Orthop Relat Res. 2006;447:138–144. doi:10.1097/01.blo.0000205876.05093.80
54. Natarajan MV, Chandra Bose J, Viswanath J, Balasubramanian N, Sameer M. Custom prosthetic replacement for distal radial tumours. Int Orthop. 2009;33(4):1081–1084. doi:10.1007/s00264-009-0732-2
55. Hatano H, Morita T, Kobayashi H, Otsuka H. A ceramic prosthesis for the treatment of tumours of the distal radius. J Bone Joint Surg Br. 2006;88(12):1656–1658. doi:10.1302/0301-620X.88B12.17989
56. Wang T, Chan CM, Yu F, Li Y, Niu X. Does wrist arthrodesis with structural iliac crest bone graft after wide resection of distal radius giant cell tumor result in satisfactory function and local control? Clin Orthop Relat Res. 2017;475(3):767–775. doi:10.1007/s11999-015-4678-y
57. Zhang S, Xu M-T, Wang X-Q, Wang -J-J. Functional outcome of en bloc excision and custom prosthetic replacement for giant cell tumor of the distal radius. J Orthop Sci. 2015;20(6):1090–1097. doi:10.1007/s00776-015-0763-z
58. Hariri A, Facca S, Di Marco A, Liverneaux P. Massive wrist prosthesis for giant cell tumour of the distal radius: a case report with a 3-year follow-up. Orthop Traumatol Surg Res. 2013;99(5):635–638. doi:10.1016/j.otsr.2013.04.001
59. Damert H-G, Altmann S, Kraus A. Custom-made wrist prosthesis in a patient with giant cell tumor of the distal radius. Arch Orthop Trauma Surg. 2013;133(5):713–719. doi:10.1007/s00402-013-1692-y
60. Sargazi N, Philpott M, Malik A, Waseem M. Ulna autograft for wrist arthrodesis: a novel approach in failed wrist arthroplasty. Open Orthop J. 2017;11(1):768–776. doi:10.2174/1874325001711010768
61. Gulati K, Prideaux M, Kogawa M, et al. Anodized 3D-printed titanium implants with dual micro- and nano-scale topography promote interaction with human osteoblasts and osteocyte-like cells: 3D Printed Titanium Implants with Dual Micro- and Nano-Scale Topography. J Tissue Eng Regen Med. 2017;11(12):3313–3325. doi:10.1002/term.2239
62. Lu M, Min L, Xiao C, et al. Uncemented three-dimensional-printed prosthetic replacement for giant cell tumor of distal radius: a new design of prosthesis and surgical techniques. Cancer Manag Res. 2018;10:265–277. doi:10.2147/cmar.s146434
63. Grandizio LC, Maschke S. Wrist arthrodesis with femoral head structural allograft after failed total wrist arthroplasty. Tech Hand Up Extrem Surg. 2017;21(3):116–120. doi:10.1097/bth.0000000000000165
64. Adams BD, Kleinhenz BP, Guan JJ. Wrist arthrodesis for failed total wrist arthroplasty. J Hand Surg Am. 2016;41(6):673–679. doi:10.1016/j.jhsa.2016.02.012
65. Asavamongkolkul A, Waikakul S, Phimolsarnti R, Kiatisevi P. Functional outcome following excision of a tumour and reconstruction of the distal radius. Int Orthop. 2009;33(1):203–209. doi:10.1007/s00264-007-0441-7
66. Brigstocke GHO, Hearnden A, Holt C, Whatling G. In-vivo confirmation of the use of the dart thrower’s motion during activities of daily living. J Hand Surg Eur Vol. 2014;39(4):373–378. doi:10.1177/1753193412460149
67. Zhu Z, Zhang C, Zhao S, Dong Y, Zeng B. Partial wrist arthrodesis versus arthroplasty for distal radius giant cell tumours. Int Orthop. 2013;37(11):2217–2223. doi:10.1007/s00264-013-2040-0
68. Szabo RM, Anderson KA, Chen JL. Functional outcome of en bloc excision and osteoarticular allograft replacement with the Sauve-Kapandji procedure for Campanacci grade 3 giant-cell tumor of the distal radius. J Hand Surg Am. 2006;31(8):461–467. doi:10.2106/JBJS.J.01922
69. Puri A, Gulia A, Agarwal MG, Reddy K. Ulnar translocation after excision of a Campanacci grade-3 giant-cell tumour of the distal radius: an effective method of reconstruction: an effective method of reconstruction. J Bone Joint Surg Br. 2010;92-B(6):875–879. doi:10.1302/0301-620X.92B6.23194
70. Jaminet P, Rahmanian-Schwarz A, Pfau M, Nusche A, Schaller H-E, Lotter O. Fibulo-scapho-lunate arthrodesis after resection of the distal radius for giant-cell tumor of the bone. Microsurgery. 2012;32(6):458–462. doi:10.1002/micr.21971
71. Duan H, Zhang B, Yang H-S, et al. Functional outcome of en bloc resection and osteoarticular allograft reconstruction with locking compression plate for giant cell tumor of the distal radius. J Orthop Sci. 2013;18(4):599–604. doi:10.1007/s00776-013-0394-1
72. McLean JM, Clayer M, Stevenson AW, Samson AJ. A modified ulnar translocation reconstruction technique for Campanacci grade 3 giant cell tumors of the distal radius using a clover leaf plate. Tech Hand Up Extrem Surg. 2014;18(3):705–711. doi:10.1002/micr.22521
73. Nagoba B, Malu RG, Jaju CR, Goyal V, Mali S. Giant cell tumor of distal radius treated by en-bloc resection and reconstruction by non vascularized fibular graft. Electron J Gen Med. 2015;12. doi:10.15197/sabad.1.12.39
74. Zhang W, Zhong J, Li D, Sun C, Zhao H, Gao Y. Functional outcome of en bloc resection of a giant cell tumour of the distal radius and arthrodesis of the wrist and distal ulna using an ipsilateral double barrel segmental ulna bone graft combined with a modified Sauve-Kapandji procedure. J Hand Surg Eur Vol. 2017;42(4):377–381. doi:10.1177/1753193416664291
75. Salunke AA, Shah J, Warikoo V. Giant cell tumor of distal radius treated with ulnar translocation and wrist arthrodesis: what are the functional outcomes? J Orthop Surg. 2017;25(1):230949901668497. doi:10.1177/2309499016684972
76. Dheeprajappa K. Resection and reconstruction of distal radius Giant cell tumour using avascular autogenous fibular graft. Univ J Surg Surg Spec. 2017;3:327–332.
77. Vyas A, Patni P, Saini N, Sharma R, Arora V, Gupta SP. Retrospective analysis of giant cell tumor lower end radius treated with en bloc excision and translocation of ulna. Indian J Orthop. 2018;52(1):10–14. doi:10.4103/ortho.IJOrtho_227_16
78. Kamal AF, Muhamad A. Outcomes of En bloc resection followed by reconstruction of giant cell tumor around knee and distal radius. A case series. Ann Med Surg. 2020;49:61–66. doi:10.1016/j.amsu.2019.11.019
79. Kuptniratsaikul V, Luangjarmekorn P, Charoenlap C, Hongsaprabhas C, Kitidumrongsook P. Anatomic 3D-printed endoprosthetic with multiligament reconstruction after en bloc resection in giant cell tumor of distal radius. J Am Acad Orthop Surg Glob Res Rev. 2021;5. doi:10.5435/JAAOSGlobal-D-20-00178
80. Scoccianti G, Campanacci DA, Beltrami G, Caldora P, Capanna R. The use of osteo-articular allografts for reconstruction after resection of the distal radius for tumour. J Bone Joint Surg Br. 2010;92-B(12):1690–1694. doi:10.1302/0301-620X.92B12.25121
81. Humail SM, Ghulam MKK, Zaidi IH. Reconstruction of the distal radius with non-vascularised fibular graft after resection of giant cell tumour of bone. J Orthop Surg. 2014;22(3):356–359. doi:10.1177/23094990140220031
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.