")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Recommendations to Improve Services and Supports for Domestically Sex Trafficked Persons Derived from the Insights of Health Care Providers
Authors Du Mont J, Montemurro F, Bruder R, Kelly CE, Recknor F, Mason R
Received 3 November 2023
Accepted for publication 8 March 2024
Published 10 April 2024 Volume 2024:17 Pages 1577—1583
DOI https://doi.org/10.2147/JMDH.S448037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Janice Du Mont,1,2 Frances Montemurro,1 Rhonelle Bruder,1,2 C Emma Kelly,1 Frances Recknor,1 Robin Mason1,2
1Women’s College Research Institute, Women’s College Hospital, Toronto, ON, M5S 1B2, Canada; 2Dalla Lana School of Public Health, University of Toronto, Toronto, ON, M5T 3M7, Canada
Correspondence: Janice Du Mont, Women’s College Research Institute, Women’s College Hospital, 76 Grenville St, Toronto, ON, M5S 1B2, Canada, Email [email protected]
Abstract: Health care providers are highly likely to encounter persons who have been domestically sex trafficked and, therefore, possess valuable insights that could be useful in understanding and improving existing services and supports. In-depth interviews were conducted with 31 health care providers residing and working in Canada’s largest province, Ontario. Results were analyzed using Braun and Clarke’s analytical framework. Across providers, a key theme was identified: “Facilitators to improve care”, which was comprised of two sub-themes, “Address needs in service provision” and “Center unique needs of survivors”. From these results, eight wide-ranging recommendations to improve services and supports were developed (eg, Jointly mobilize an intersectoral, collaborative, and coordinated approach to sex trafficking service provision; Employ a survivor-driven approach to designing and delivering sex trafficking services). These recommendations hold the potential to enhance services in Canada and beyond by reducing barriers to access and care, facilitating disclosure, aiding in recovery, and empowering those who have been domestically sex trafficked.
Keywords: domestic, human trafficking, health care, recommendations, sex trafficking, social services
Introduction
Sex trafficking is among the fastest growing and most profitable crimes globally.1,2 Federal and provincial governments in Canada have prioritized the development of strategies to respond to sex trafficking, reduce its incidence, and identify its victims.1,2 Despite the difficulty in gathering reliable data on this largely hidden crime, existing police-reported statistics indicate that trafficking in persons is an issue of concern in Canada. Ontario, Canada’s largest province, in particular has been an acknowledged center of domestic sex trafficking,1,3,4 a form of trafficking that takes place entirely within a single country.5 However, responses to address domestic sex trafficking vary across regions and among professions, with limited and underdeveloped best practices to facilitate work with this service population. Moreover, there is a lack of evidence on how to improve services for domestically sex trafficked persons within the Canadian context. Canada’s universal health care system differs from that of many other countries – particularly the United States where much previous research has been conducted.6,7 As health care providers fill diverse roles across professional health care settings and are likely to come into contact with sex trafficked persons,8,9 they can hold valuable information that may aid in transforming supports provided to sex trafficked persons. This study therefore explored Canadian health care providers’ perceptions of what is needed to improve care, from which wide-ranging recommendations to better services and supports were generated.
Methods
Women’s College Hospital’s Research Ethics Board approved a program of research on domestic sex trafficking, of which this study is one part, in December 2021 (REB# 2021–0133-E).10–14 A semi-structured interview guide was developed by multidisciplinary team members with diverse expertise in qualitative research, gender-based violence, sex trafficking, women’s health, psychology, social work, and public health. Open-ended questions were crafted to understand health care providers’ knowledge, attitudes, and practices regarding domestic sex trafficking, several of which were modified from those that comprise the Human Trafficking Myth Scale.10,15 Other questions included, for example, “What do you believe patients who have been sex trafficked need most in general and also from you specifically as a health care provider?” and “What challenges stand in the way of you being able to provide the patient with appropriate support?”. Participants were recruited via the researchers’ networks, direct contact with health care organizations, and social media platforms. Recruitment ended when interviews no longer yielded new information.16 Eligibility criteria included living and working as a health care provider in a health care setting in Ontario, Canada at the time of the interview. A sociodemographic questionnaire documented providers’ unique characteristics, including their social identity (eg race, age, gender), education, occupation, and years in occupation. Prior to scheduling interviews, consent was discussed; outstanding questions were answered; and completed consent forms, providing for publication of anonymized responses, were returned via email. Between November 2022 and February 2023, 31 semi-structured interviews were conducted via Zoom, each lasting 1–2 hours (see Table 1). Interviews were transcribed verbatim and uploaded to Dedoose, a software program, for analysis using Braun and Clarke’s thematic qualitative analytic approach.17 After repeat reading of all transcripts, initial codes were developed and applied. Coded excerpts of the transcripts were reviewed and subsequently clustered into larger groupings, referred to here as code categories. From these emerged final themes and sub-themes (see10 for further methodological detail).
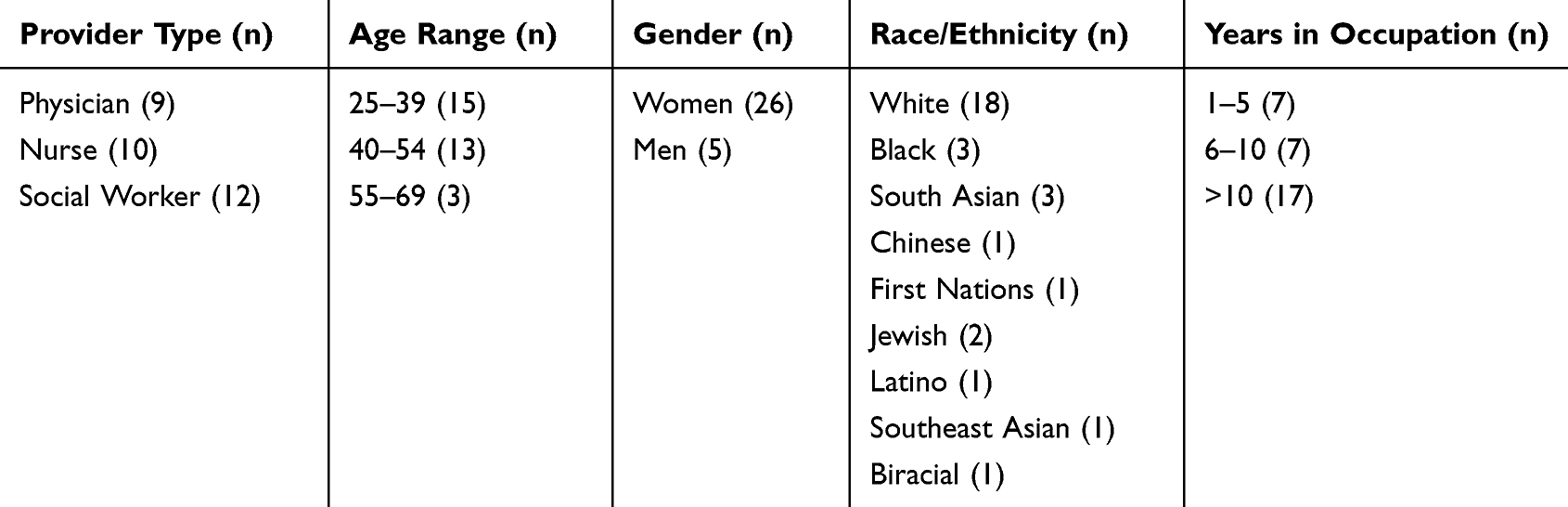 |
Table 1 Sociodemographic Information of Participants |
Results
Health care providers shared their perspectives on “Facilitators to improve care” for domestically sex trafficked persons as shaped by their work experiences. Within this theme, two sub-themes were identified: Address needs in service provision, which included several related code categories that acknowledged gaps in services and supports; and Center unique needs of survivors, in which the related code categories documented survivor-centered considerations for care. Example supporting quotations relevant to each sub-theme and code category are highlighted below; additional quotes can be found in Supplemental Table 1: Facilitators to improve care for domestically sex trafficked persons: sub-themes, code categories, and supporting quotations.
Address Needs in Service Provision
Within this sub-theme, health care providers noted several significant aspects of service provision that provide opportunities to improve domestic sex trafficking care. Here, the descriptive code categories included: Collaborative, coordinated supports across social, health care, and community settings; Integrated, team-based, wrap-around, co-located services; Attainable specialized expertise; Available, suitable shelters and housing; Curriculum, training, toolkits, and protocols; and Funds for survivors, services, and supports.
Collaborative, Coordinated Supports Across Social, Health Care, and Community Settings
Having [social service] partnerships with health agencies, so they [the health care provider] have a secure trusted agency they can make that call [...] to talk to, to consult with. [...] Just like we have with [name of social service organization], we have those different services where we can reach out and ask and inquire about or have partnerships with, then that would be helpful. (HCP 14)
[I]t needs to be a holistic approach. You cannot just try and rescue somebody [out] of the sex trafficking industry unless you address the underlying components and barriers to that. Like you said, home, food, security, if there’s drug addiction, safety issues, the fact that they may lose their entire support system because their support system is within that network. [...] There needs to be [...] a systematic effort. (HCP 17)
Integrated, Team-Based, Wrap-Around, Co-Located Services
We do not have one spot that does everything and I think that’s kind of the big missing piece. [...] [T]hese people need that anchor, that one place that knows everything about them and can get to them, the social work, the money, the housing, the physical health needs, and the mental health needs that they need. (HCP 2)
I just do not feel like it’s one area that needs to be addressed. I think it’s complex, human trafficking, and I do not know if it just falls on one type of team member or it’s definitely not, it’s not an individual approach. I do not think working in silos would be helpful, either. [I] need a team to help this client and support them. That’s what I mean by wrap-around, [a] multi-disciplinary approach to helping a client. [...] One person [...] can only [do so much]. (HCP 5)
Attainable Specialized Expertise
I think ideally it would be somebody whose role in the hospital, or maybe shared amongst several hospitals, knowing who to pick up the phone and call for that support to really discuss the case and receive the advice in real time would be helpful. [...] [T]hey’re giving you tailored advice on how to approach the issues that you are having particular difficulty with. (HCP 23)
Having allied health professionals who have [sex trafficking] expertise and paying for those allied health professionals to be designated for this kind of work, because in that moment, when someone discloses, I do not want to lose that opportunity if they are ready to talk about it. (HCP 31)
Available, Suitable Shelters and Housing
[R]ight now shelters are filled with people who are homeless, people who are coming out of domestic violence, and there is no space for anybody right now, not even for people who are being trafficked. [...] Right now, people are being put into hotels and sometimes it’s not safe in there either, because I have clients who do not feel safe in a hotel. They want to be within a shelter where people cannot enter and access their rooms. (HCP 6)
I think there needs to be more shelters, less co-ed shelters, more gender-orientated shelters. [...] [W]hen I had that one patient, the transgender patient, there [were no] women’s shelters that are accepting of transgender females to make sure that they have a safe environment. [...] I think it is less safe for someone who’s trying to escape from their traffickers to go into a shelter where they have to sleep next to a guy that they do not know; it’s traumatizing to them. (HCP 8)
Curriculum, Training, Toolkits, and Protocols
We want to do everything we can to help them [sex trafficked person]. But I think there’s just a [...] knowledge gap or maybe just we do not always know how to best help these people. I think just [...] having more education is [...] important, because a lot of times people [who] are being trafficked are going to come through the ED [emergency department] at some point. [...] [T]here’s gonna’ be so many opportunities to intervene if you are astute enough to pick it up. (HCP 22)
If we had [sex trafficking training] modules where we could kind of combine the generalities of a lot of the different cases, like here’s what tipped this person off to the fact that this person may have been trafficked. We just do not see enough of the cases for each person to develop that list of red flags. If we were able to share the information and compile a module of what we have noticed at all these different sites, that may be more helpful. (HCP 25)
Funds for Survivors, Services, and Supports
Our funding just got cut at our center, it boggles my mind [...] at a time when people are just absolutely struggling. So, that would be a huge one, if there’s any way to get more funding for more help. And maybe that would mean there’d be more individual counseling, groups as well, group therapy where people can feel connected. (HCP 4)
Money is necessary; sometimes it takes a while to get somebody on [social assistance] or get them any kind of support. Sometimes you need money just to get people to a safe place [...], [but] most of the time people do not have access to money and without money you can have all the information in the world, but [that does not matter if] you do not have access to funding. [...] I am not talking [about] funding for the organization. I am talking [...] help to people directly. (HCP 6)
Center Unique Needs of Survivors
Health care providers also noted that survivor-centered approaches to care can best serve the needs of domestically sex trafficked persons. Here, the descriptive code categories included: Survivor-led and informed approaches and the Primacy of trust, rapport, and safety.
Survivor-Led and Informed Approaches
A lot of it is trust [...] and I have to work towards that [...] [by] making them a part of the plan. So [asking the patient] [...], “Would you be open to going to a women’s shelter?” [T]hen you get their reason why [they] do not, and [then asking], “What other ideas do you have?” So, one came up with go[ing] to [her] sister’s for the weekend. [I agreed] that [was] a good idea. (HCP 16)
It would be nice to know what are some of the factors that we need to be on the lookout for and go from there, but also how to support people from the client perspective. Like, what are things they want from their health care provider, because sometimes we have our approach of what we think they need to know. But maybe they are not ready to hear that or maybe that’s not what their priority is. (HCP 24)
Primacy of Trust, Rapport, and Safety
We do not have time, which sounds really bad and I feel like it’s really hard to build a trusting relationship with somebody that is like this [sex trafficked]. Nobody’s going to come out and tell you, “Oh, yes, I have been sex trafficked.” (HCP 10)
They need care. They need somebody that is compassionate with them and they need somebody that is going to [...] be like, “Okay, we need to figure out something safe for you.” (HCP 10)
[It’s] [h]ard to identify [sex trafficking] because of the limited time people [doctors] have with their clients or patients, the rush in the waiting room, and [patients] feeling uncomfortable talking to someone who they do not feel safe with. There used to be posters on walls, [...] in sexual health clinics and stuff like that [...] [saying] this is a safe place. Maybe all doctors’ offices need to have that. [...] Maybe [saying] something [to the patient] about, “If you have anything that you need to talk about as well, whatever, this is a safe place to do it. We will not do harm [...] and if you need help in any way, [we are here].” Something that [lets] people know that they can [disclose]. Because it’s scary to go into a doctor’s office for people and young women. (HCP 20)
Discussion
In this study, we drew upon the insights of health care providers to understand what is needed to improve health and other services and supports for domestically sex trafficked patients. The study builds on our earlier work documenting the challenges social service workers identified as impeding their practices with sex trafficked persons12 and contributes to the nascent scholarly research on domestic sex trafficking in Canada.18 Here, analysis of the 31 interviews with physicians, nurses, and social workers resulted in two key sub-themes: 1. Address needs in service provision and 2. Center unique needs of survivors. From these sub-themes, we developed eight recommendations, extensive in scope, to guide future systems and organizational change (see Table 2). Three of the recommendations are focused on the importance of implementing sex trafficking specific models of care including those that are intersectoral, multidisciplinary, or draw on in-house specialized expertise and supports, while others focus on the education and training needs of providers, provision of appropriate shelter and housing options, funding required, and practices to meet survivors’ particular needs. Collectively, these recommendations hold the potential to improve services by reducing barriers to access and care, facilitating disclosure, aiding in recovery, and empowering survivors (see Table 2 for anticipated impacts of recommendations).9,19,20
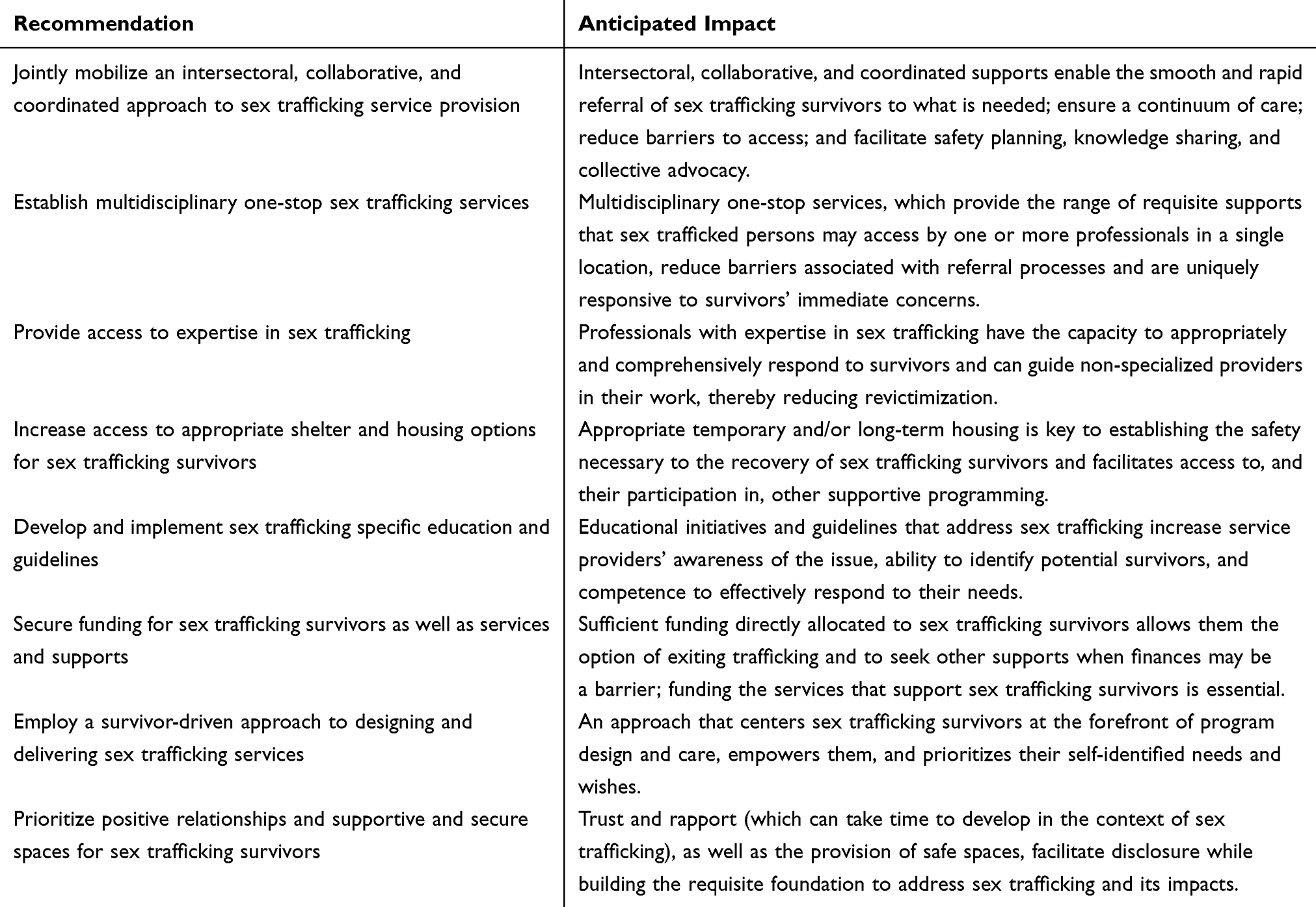 |
Table 2 Recommendations to Improve Services and Supports for Domestically Sex Trafficked Persons Derived from the Insights of Health Care Providers |
While the recommendations generated are derived from the valuable insights of Ontario health care providers, their perceptions would have been shaped by their individual experiences and the communities they served. Participants may not have fully represented the diverse range of health care services and settings across Ontario and elsewhere. Further, although the recommendations, if implemented, could meet some noted sex trafficked persons’ self-described needs (eg, building trust and rapport through positive relationships; collaborative, multidisciplinary, and community-based care; provider education on identifying sex trafficking),9,21,22 more research is needed to confirm the adequacy of these recommendations for diverse survivors (eg, Indigenous, Black, youth, sexual and gender minorities).
Data Sharing Statement
Data supporting the conclusions of this study are included in the published article with additional detail in a Supplementary Information File (see Supplemental Table 1. Facilitators to improve care for domestically sex trafficked persons: sub-themes, code categories, and supporting quotations).
Acknowledgments
This study would not have been possible without the health care providers who participated in interviews. We are thankful for their participation, as well as the funding support provided by the HART Foundation. Our gratitude also extends to Danielle Jacobson for her contributions to the larger program of research.
Funding
This work was supported by the HART Foundation. The views expressed in this article are solely those of the authors and do not necessarily reflect those of the funder.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Government of Ontario. Ontario’s anti-human trafficking strategy 2020–2025. Ontario; 2022. Available from: https://www.ontario.ca/page/ontarios-anti-human-trafficking-strategy-2020-2025.
2. Public Safety Canada. National strategy to combat human trafficking 2019–2024. Government of Canada; 2019. Available from: https://www.publicsafety.gc.ca/cnt/rsrcs/pblctns/2019-ntnl-strtgy-hmnn-trffc/index-en.aspx.
3. Conroy S. Trafficking in persons in Canada, 2021. Statistics Canada; 2022. Available from: https://www150.statcan.gc.ca/n1/en/pub/85-005-x/2022001/article/00001-eng.pdf?st=tcMUkcCq.
4. Royal Canadian Mounted Police. Domestic human trafficking for sexual exploitation in Canada. Government of Canada; 2013. Available from: https://publications.gc.ca/collections/collection_2014/grc-rcmp/PS64-114-2014-eng.pdf.
5. Government of British Columbia. What is human trafficking? British Columbia. date unknown. Available from: https://www2.gov.bc.ca/gov/content/justice/criminal-justice/victims-of-crime/human-trafficking/what-is-it.
6. Recknor FH, Gemeinhardt G, Selwyn BJ. Health-care provider challenges to the identification of human trafficking in health-care settings: a qualitative study. JHT. 2017;4(3):213–230. doi:10.1080/23322705.2017.1348740
7. Beck ME, Lineer MM, Melzer-Lange M, Simpson P, Nugent M, Rabbitt A. Medical providers’ understanding of sex trafficking and their experience with at-risk patients. Pediatrics. 2015;135(4):e895–902. doi:10.1542/peds.2014-2814
8. Richie-Zavaleta AC, Villanueva A, Martinez-Donate A, Turchi RM, Ataiants J, Rhodes SM. Sex trafficking victims at their junction with the healthcare setting—a mixed-methods inquiry. JHT. 2020;6(1):1–29. doi:10.1080/23322705.2018.1501257
9. Lederer LJ, Wetzel CA. The health consequences of sex trafficking and their implications for identifying victims in healthcare facilities. Ann of Health Law. 2014;23(1):61–91.
10. Jacobson D, Mason R, Bruder R, Du Mont J. A protocol for a qualitative study on sex trafficking: exploring knowledge, attitudes, and practices of physicians, nurses, and social workers in Ontario, Canada. PLoS One. 2022;17(9):e0274991. doi:10.1371/journal.pone.0274991
11. Jacobson D, Du Mont J, Montemurro F, Bruder R, Mason R. Social service providers’ knowledge of domestic sex trafficking in the Canadian context. Qual Res Health. 2023;3. doi:10.1016/j.ssmqr.2023.100279
12. Recknor F, Mason R, Jacobson D, et al. Challenges to supporting domestically sex trafficked persons: in-depth interviews with service providers. JHT. 2023. doi:10.1080/23322705.2023.2219224
13. Recknor F, Kelly CE, Jacobson D, et al. Impacts of the COVID-19 public health crisis on caring for sex trafficked persons. HPP. 2023. doi:10.1177/15248399231186639
14. Elliot S, Kelly CE, Jacobson D, et al. Identification of domestically sex trafficked persons in social service settings in Canada: a qualitative study. SSR. 2023;49(5):569–584. doi:10.1080/01488376.2023.2242886
15. Cunningham KC, DeMarni Cromer L. Attitudes about human trafficking: individual differences related to belief and victim blame. JIV. 2016;31(2):228–244. doi:10.1177/0886260514555369
16. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. Hodgins E, Mutis J, Mason R, Du Mont J. Sex trafficking of women and girls in Canada: a scoping review of the scholarly literature. TVA. 2023;24(4):2363–2378. doi:10.1177/15248380221094316
19. Chisolm-Straker ML, Miller C, Duke G, Stoklosa HA. Framework for the development of healthcare provider education programs on human trafficking part two: survivors. JHT. 2020;6(4):410–424. doi:10.1080/23322705.2019.1635333
20. Corbett A. The voices of survivors: an exploration of the contributing factors that assisted with exiting from commercial sexual exploitation in childhood. J Child Youth. 2018;85:91–98. doi:10.1016/j.childyouth.2017.12.009
21. Lorvinsky J, Pringle J, Filion F, Gagnon AJ. Sex trafficking survivors’ experiences with the healthcare system during exploitation: a qualitative study. PLoS One. 2023;18(8):e0290067. doi:10.1371/journal.pone.0290067
22. Murdock L, Hodge-Williams C, Hardin K, Rood CJ. Youth survivor perspectives on healthcare and sex trafficking. PNJ. 2022;66:95–103. doi:10.1016/j.pedn.2022.05.020
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.