")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
Prosthodontic Management of a Patient with Ectodermal Dysplasia: Case Report
Authors Nejabi MB, Anwari A , Shadab H, Mtawakel N, Omarzad F, Ahmadi ME
Received 22 May 2023
Accepted for publication 2 August 2023
Published 7 August 2023 Volume 2023:15 Pages 133—141
DOI https://doi.org/10.2147/CCIDE.S419939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mohammad Bashir Nejabi,1 Abdurrahman Anwari,2 Hassina Shadab,3 Nargis Mtawakel,1 Fariha Omarzad,1 Mohammad Eissa Ahmadi3
1Prosthodontics Department, Kabul University of Medical Sciences (KUMS), Kabul, Afghanistan; 2Operative/ Restorative Dentistry and Endodontics Department, Kabul University of Medical Sciences (KUMS), Kabul, Afghanistan; 3Periodontics Department, Kabul University of Medical Sciences (KUMS), Kabul, Afghanistan
Correspondence: Abdurrahman Anwari, Operative/ Restorative Dentistry and Endodontics Department, Kabul University of Medical Sciences (KUMS), Jamal Mena, 3rd District, Kabul, Afghanistan, Tel +93795125522, Email [email protected]
Abstract: Ectodermal dysplasia (ED) is an inherited disorder that affects the ectoderm of a developing embryo and impacts structures that originate from it. It typically presents as a triad of missing teeth (anodontia/hypodontia), sparse hair (atrichosis/hypotrichosis), and lack of sweat glands (hypohidrosis), often accompanied by nail dystrophy and palmoplantar hyperkeratosis. There are two main types of this condition: X-linked anhidrotic or hypohidrotic and hidrotic (autosomal type). The oral manifestation of ED may include anodontia or hypodontia, with or without cleft lip and palate. Tooth loss leads to a decrease in the height of the alveolar ridges, resulting in a reduction of the vertical dimension of the lower face, disappearance of the vermilion border, and prominent lips. As a result, the affected person’s face may resemble that of an elderly individual. The current case report aims to illustrate the prosthodontic rehabilitation of 16-year-old male patient with ectodermal dysplasia and complete anodontia, visiting Dentistry Teaching Hospital, Kabul, Afghanistan. Fortunately, this patient was acceptably managed with the collaboration of several disciplines.
Keywords: prosthodontic management, ectodermal dysplasia, anodontia, case report
Introduction
Ectodermal dysplasia syndrome is a genetic disorder that affects multiple structures derived from the ectoderm during fetal development.1 These structures include hair, nails, teeth, sweat glands, sebaceous glands, and skin.1,2 There are different types of ectodermal dysplasias, but they typically present with lack of teeth, thin hair, and inadequate sweat gland function.1 There are two main clinical variations of EDs: Hypohidrotic/Anhidrotic (X-linked recessive) and Hidrotic (autosomal inherited).3–5 When at least two ectodermal structures are affected, a diagnosis of ED is made, clinical presentation can include abnormal teeth, fine and dry hair, and a lack of sweat glands.3,4
The developing embryo has 3 layers: endoderm, mesoderm and ectoderm which are the basis for the formation of all body structures; these layers arise through a process known as gastrulation. The endoderm gives rise to the gastrointestinal system’s epithelial lining, pancreas, thyroid, lungs, and liver, while the mesoderm produces organs such as the heart, circulatory system, genitourinary system, gonads, muscles, bone, and cartilage. The ectoderm layer is responsible for the development of structures like mammary glands, skin, hair, nails, teeth, external ear, melanocytes, cornea, conjunctiva, lacrimal system, and central/peripheral neural system.6 Any disruption in the formation of organs from these layers can result in developmental genetic defects and lifelong complications. The Ectodermal Dysplasia Syndrome is a collection of inherited disorders that can cause defects in two or more structures derived from the ectoderm. This can result in incomplete formation of associated structures and specific clinical manifestations.1
To cover all clinical conditions of ectodermal dysplasia, various classifications have been made. One classification divides ectodermal dysplasia into nine classes based on the structures involved (Table 1).7
 |
Table 1 Types of Ectodermal Dysplasia |
Ectodermal dysplasia is caused by genetic mutations that affect the coding of ectoderm, resulting in errors in signal transmission. Specific genes, including ectodysplasin, wingless, and p63/sonic hedgehog, are commonly affected by genetic mutations in this disorder. Ectodermal dysplasia can be transmitted through different genetic patterns, including autosomal recessive, autosomal dominant, and x-linked modes.8
Christ-Siemens-Touraine syndrome, also referred to as Hypohidrotic or Anhidrotic, is a genetic disorder that follows an X-linked recessive pattern of inheritance. This condition predominantly affects males, while women act as carriers.9,10 The syndrome is characterized by a triad of symptoms including fine, dry hair (hypotrichosis, atrichosis), insufficient sweat gland function and missing teeth (hypodontia, oligodontia, anodontia) or misshapen teeth.1,3,4,10 It is estimated that the incidence of the syndrome in men is approximately 1 in 100,000 births, while carriers have an incidence of around 17 in 100,000 women.3,11 Diagnosis is typically made based on clinical symptoms and radiographic evidence.7 However, the ideal way to confirm this is to have a skin biopsy that shows absence or hypoplasia of sweat glands. In addition, numerous genetic tests are also available to diagnose subtypes of ED.12 Patients with this condition often experience negative impacts on their appearance, particularly in regard to their facial features and missing teeth.1 Ectodermal dysplasia can be devastating, both physically and emotionally, to patients.13 Appropriate rehabilitative procedures can improve quality of life for patients with ectodermal dysplasia.14 The most effective treatment option for improving both function and aesthetics is prosthodontic rehabilitation.15
This report details the prosthetic rehabilitation of a 16-year-old boy with hypohidrotic ectodermal dysplasia and complete anodontia. Treatment options were discussed with dentists of multidiscipline and patient’s father. The feasible treatment option was complete dentures for maxillary and mandibular arches. Alginate primary impressions were taken from both arches. Study casts were poured from these impressions. Final impressions with condensation silicone were taken using custom trays. Complete dentures were made on master casts.
Case Presentation
On February/10/2023, registration no 8932, a 16-year-old male patient, accompanied by his father, was referred to the Prosthodontics Department, Dentistry Teaching Hospital, Kabul University of Medical Sciences “Abu Ali Ibn Sina”. The patient’s main complaint was his unpleasant appearance and lack of teeth in both his upper and lower jaws, which led to difficulties in chewing. The family history revealed that the patient’s mother, father, grandmother and grandfather were all in good health and had no known medical issues. Furthermore, no consanguinity was involved in his parent’s marriage history. However, upon further investigation, it was discovered that the patient’s 21-year-old sister and 11-year-old brother exhibited abnormal characteristics in their oral cavity. Specifically, they both presented with hypodontia and micro-shaped teeth.
The patient’s mother divulged the occurrence of recurring hyperthermia in her offspring’s infancy and present time.
Clinical Findings
The clinical manifestations exhibited by the patient were indicative of hypohidrotic ectodermal dysplasia. Upon conducting an extraoral assessment, the patient’s attributes comprised widespread alopecia of the scalp, characterized by fragile, parched, and hypochromic hair, arid skin, prominent forehead, sparse eyebrows and eyelashes, pigmented skin around the mouth with wrinkles, a pronounced lower lip, and a straight facial profile (Figures 1 and 2).
 |
Figure 1 Frontal view showing typical clinical manifestations of ED. |
 |
Figure 2 Side view with straight facial profile. |
Intraoral examination showed that the patient did not have any baby or adult teeth. The ridges were thin, and there was less space for the teeth to fit in. The tissue inside the mouth was sticky and not normal (Figures 3 and 4).
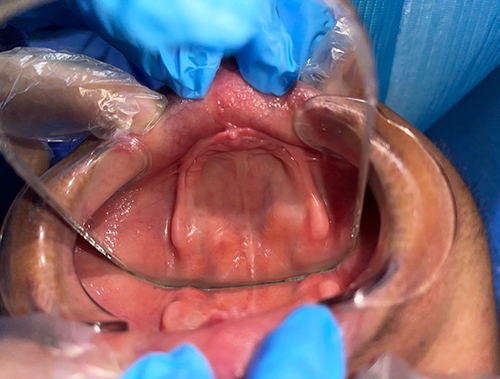 |
Figure 3 Narrow upper ridge with compromised height. |
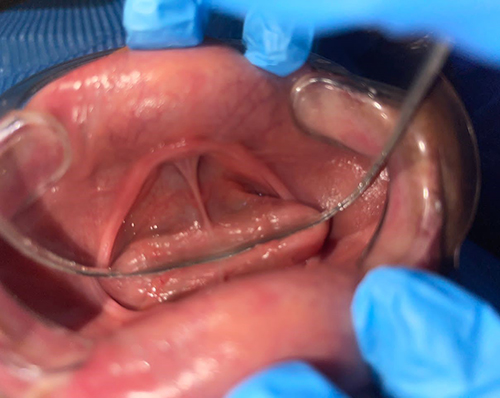 |
Figure 4 Vertical reduction of lower ridge with very adherent frenulum. |
Diagnostic Assessment
The panoramic x-ray also confirmed that there were no signs of any tooth buds (Total Anodontia) (Figure 5). The model of the mouth showed that the ridges were not fully developed and had lost their height. Lower and upper jaws fall in Type IV and Type C of ACP classification system for completely edentulous patients, respectively.
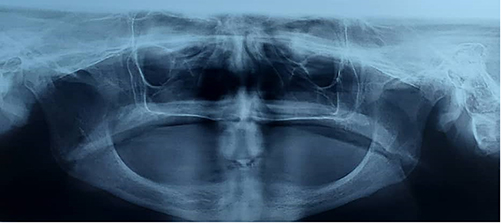 |
Figure 5 Panoramic Radiography confirming complete anodontia. |
Therapeutic Intervention
According to the hospital’s policy, the patient’s father signed an informed consent form and authorized the proposed treatment.
In order to improve patient’s appearance, ability to chew, and speaking proficiency it was decided to create full dentures for both upper and lower jaws.
The patient had a surgical procedure (Frenectomy) performed by the periodontal team to address the issue of the labial frenulum being tightly attached in both jaws, which hindered the proper placement of the prosthesis.
Then, the process of creating dentures begun and involved the following steps: To begin the process of creating dentures, firstly made an initial impression of the patient’s mouth using alginate material. Custom trays were fabricated with cold cure acrylic resin for final impression. Final impression was taken with condensation silicone using functional impression technique with the intention of preventing from further ridge resorption. The acrylic bases and wax rims were created on the working casts. The mandible’s physiological rest position was used to determine vertical dimension of occlusion (VDO). Both jaws were recorded and mounted in an articulator. The dentist selected acrylic, anatomical shape, B2 shade teeth to address all of the patient’s concerns, and the dentures were constructed from heat-cured acrylic resin in balanced occlusion. After the dentures were completed (as shown in Figures 6 and 7), the patient was given instructions for proper hygiene and advised to remove the dentures overnight and clean it properly. If any issues arose, the patient was encouraged to visit the dentist for assistance.
 |
Figure 6 After prosthetic rehabilitation, final look. |
 |
Figure 7 Post treatment full mouth view. |
Follow-Up and Outcomes
After providing the patient with dentures and monitoring his progress for three weeks, he reported a decrease in his previous concerns and expressed contentment with the treatment. No adverse and unanticipated event was noted.
Discussion and Conclusions
Despite years of investment and useful resource, medical care in Afghanistan stays seriously constrained and is “frequently non-existent, prohibitively not affordable or inaccessible” where it is wanted most.16 71.8% (545/759) of Afghan patients had barriers in accessing medical facilities. A combination of long distances, high costs, and conflict has deprived people of life-saving medical care. The nearest public clinics were underutilized due to lack or low quality of staff, services and medicines.17 Access to dental care is limited like medical care and even more so. Meanwhile, it is clear that the quality of life and general well-being is affected by oral health status.18 Despite the above problems and limitations, in this case, an appropriate dental care has been provided to a patient with ectodermal dysplasia.
The order and category of dental therapies for ED vary from one patient to another. The aims of these therapies encompass improving functionality, speech, facial looks, and dental esthetics by bringing back to norm the vertical measurement and supporting soft tissues of the face.19,20 Maintaining the existing dentition, improving acceptance by family and peers and promoting psychological well-being are other aims of dental therapy for ED patients.9 According to the type and severity of teeth abnormality, extent of teeth loss, orthopedic abnormalities and age of patients with ED, therapies such as complete dentures (CD),19–24 removable partial dentures,19,22,23,25–28 conventional or resin fixed partial dentures,27,29,30 implant supported prosthesis,29,31 auto transplantation,32 direct restorations,25 orthodontic therapy,33 orthopedic and orthognathic treatment34 have been provided individually or in combination, so far.
Complete removable denture and implant supported denture are two oral rehabilitation options for ED patients with total anodontia. For adult patients with ED, dental implants are the treatment of choice because of stability of growth and can be used to support, maintain and stabilize dentures.35 However, determining the best time for pediatric implant treatment seems to be very difficult because many aspects need to be considered in finding the optimal treatment strategy for each individual.36 Patients with ED who had tooth replacement therapy with dental implants were satisfied with the results.37 Regardless of age, a high survival rate (20-year CSR 84.6%) of dental implants placed in patients with ED has been seen.38
On the other hand, full dentures are simple, affordable and reversible treatment for patients with ED. Several case reports have demonstrated the successful use of full dentures in these patients.39 Alteration of alveolar height, betterment of musculocutaneous profile and significant improvement in mastication, esthetics, phonetics and psychological well-being are major benefits of complete dentures.40 In patients with ectodermal dysplasia, underdevelopment of the maxillary tuberosity and alveolar ridge make it difficult to achieve adequate resistance to lateral and anterior-posterior displacement of the prosthesis.41
In this case report, a 16-year-old boy with hypohidrotic ectodermal dysplasia with total anodontia and a family history of the disorder is discussed. The patient sought treatment to address issues with his appearance, as well as difficulties with chewing and speaking. A team of specialists, including a pedodontist, maxillofacial surgeon, orthodontist, and prosthodontist, collaborated to determine treatment options. The options considered included implant surgery and the use of removable prostheses. However, due to limitations such as the patient’s age, weakened jaw bone, financial constraints, and input from pediatric and orthodontic experts, implant surgery was deemed unsuitable. Therefore, the focus turned to the use of removable prostheses as a feasible solution. Due to thin alveolar ridges and high frenal attachment, we faced a challenge in gaining ideal retention for complete denture. Frenectomy was all we did to partially overcome the problem. In addition to enhancing esthetics, the treatment improved patient’s chewing ability, speech, social and psychological health. However, this denture’s retention and stability is much less than an implant supported prosthesis.
This case report discusses the oral rehabilitation of an ED patient with total anodontia with complete dentures in Afghanistan, where even access to basic health care is limited. The basic objectives were to improve patient’s esthetics, speech, chewing ability and confidence in social life, which were achieved to some extent.
Consent to Publication
The patient's father gives his consent for the publication of identifiable details, which can include photograph(s) and/or case history and/or details within the text (“Case Report”) to be published in the Dove Press Journal and Article. The Dentistry Teaching Hospital Management Board has authorized publication of these case details.
Patient Perspective
I express my gratitude to all the doctors who contributed to my treatment. I no longer worry about missing teeth when laughing and talking. My confidence in the community has increased. Of course, it takes time to get used to the prosthesis completely.
Funding
This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kargül B, Alcan T, Kabalay U, Atasu M. Hypohidrotic ectodermal dysplasia: dental, clinical, genetic and dermatoglyphic findings of three cases. J Clin Pediatr Dent. 2001;26(1):5–12. PMID: 11688814. doi:10.17796/jcpd.26.1.g156r02u66w30729
2. Halai T, Stevens C. Ectodermal dysplasia: a clinical overview for the dental practitioner. Dent Update. 2015;42(8):779–80, 783–4, 787–8 passim. PMID: 26685476. doi:10.12968/denu.2015.42.8.779
3. Dhanrajani PJ, Jiffry AO. Management of ectodermal dysplasia: a literature review. Dent Update. 1998;25(2):73–75. PMID: 9791211.
4. Bartstra HL, Hulsmans RF, Steijlen PM, Ruige M, de Die-Smulders CE, Cassiman JJ. Mosaic expression of hypohidrotic ectodermal dysplasia in an isolated affected female child. Arch Dermatol. 1994;130(11):1421–1424. PMID: 7979445. doi:10.1001/archderm.1994.01690110087014
5. Ladda R, Gangadhar S, Kasat V, Bhandari A. Prosthodontic management of hypohidrotic ectodermal dysplasia with anodontia: a case report in pediatric patient and review of literature. Ann Med Health Sci Res. 2013;3(2):277–281. PMID: 23919206; PMCID: PMC3728879. doi:10.4103/2141-9248.113679
6. Solnica-Krezel L, Sepich DS. Gastrulation: making and shaping germ layers. Annu Rev Cell Dev Biol. 2012;28:687–717. PMID: 22804578. doi:10.1146/annurev-cellbio-092910-154043
7. Tape MW, Tye E. Ectodermal dysplasia: literature review and a case report. Compend Contin Educ Dent. 1995;16(5):524–528. PMID: 8624991.
8. Reyes-Reali J, Mendoza-Ramos MI, Garrido-Guerrero E, Méndez-Catalá CF, Méndez-Cruz AR, Pozo-Molina G. Hypohidrotic ectodermal dysplasia: clinical and molecular review. Int J Dermatol. 2018;57(8):965–972. PMID: 29855039. doi:10.1111/ijd.14048
9. Nunn JH, Carter NE, Gillgrass TJ, et al. The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J. 2003;194(5):245–251. PMID: 12658298. doi:10.1038/sj.bdj.4809925
10. Tarjan I, Gabris K, Rozsa N. Early prosthetic treatment of patients with ectodermal dysplasia: a clinical report. J Prosthet Dent. 2005;93(5):419–424. PMID: 15867750. doi:10.1016/j.prosdent.2005.01.012
11. Pinheiro M, Freire-Maia N. Ectodermal dysplasias: a clinical classification and a causal review. Am J Med Genet. 1994;53(2):153–162. PMID: 7856640. doi:10.1002/ajmg.1320530207
12. Clauss F, Manière MC, Obry F, et al. Dento-craniofacial phenotypes and underlying molecular mechanisms in hypohidrotic ectodermal dysplasia (HED): a review. J Dent Res. 2008;87(12):1089–1099. PMID: 19029074. doi:10.1177/154405910808701205
13. Hashem A, Kelly A, O’Connell B, O’Sullivan M. Impact of moderate and severe hypodontia and amelogenesis imperfecta on quality of life and self-esteem of adult patients. J Dent. 2013;41(8):689–694. PMID: 23778130. doi:10.1016/j.jdent.2013.06.004
14. Abadi B, Herren C. Clinical treatment of ectodermal dysplasia: a case report. Quintessence Int. 2001;32(9):743–745. PMID: 11695142.
15. Gopinath VK, Manoj KM, Mahesh K. Hypohidrotic ectodermal dysplasia-a case report. J Indian Soc Pedod Prev Dent. 1999;17(3):90–92. PMID: 10863497.
16. Vogel L. Afghan people risk their lives to obtain health care: MSF. CMAJ. 2014;186(6):411. PMID: 24616140; PMCID: PMC3971023. doi:10.1503/cmaj.109-4751
17. Nic Carthaigh N, De Gryse B, Esmati AS, et al. Patients struggle to access effective health care due to ongoing violence, distance, costs and health service performance in Afghanistan. Int Health. 2015;7(3):169–175. PMID: 25492948; PMCID: PMC4427534. doi:10.1093/inthealth/ihu086
18. Kramer PF, Feldens CA, Ferreira SH, Bervian J, Rodrigues PH, Peres MA. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent Oral Epidemiol. 2013;41(4):327–335. PMID: 23330729. doi:10.1111/cdoe.12035
19. Al-Qadasy NE, Al-Khorasani MA, Qahhar MA, et al. Dental management in a child with ectodermal dysplasia: a case report along with review. Biosc Biotech Res Comm. 2021;14(3). doi:10.21786/bbrc/14.3.8
20. Chugh A, Gupta N, Chugh VK. Ectodermal dysplasia with total anodontia: case report with review. Indian J Multidiscip Dent. 2016;6:124–128. doi:10.4103/2229-6360.197777
21. Vieira KA, Teixeira MS, Guirado CG, Gavião MB. Prosthodontic treatment of hypohidrotic ectodermal dysplasia with complete anodontia: case report. Quintessence Int. 2007;38(1):75–80. PMID: 17216912.
22. Mittal M, Srivastava D, Kumar A, Sharma P. Dental management of hypohidrotic ectodermal dysplasia: a report of two cases. Contemp Clin Dent. 2015;6(3):414–417. Erratum in: Contemp Clin Dent. 2016 Jan-Mar;7(1):122. PMID: 26321846; PMCID: PMC4549998. doi:10.4103/0976-237X.161907
23. Srivastava VK. Ectodermal dysplasia: a case report. Int J Clin Pediatr Dent. 2011;4(3):269–270. PMID: 27678241; PMCID: PMC5034093. doi:10.5005/jp-journals-10005-1124
24. Manuja N, Passi S, Pandit IK, Singh N. Management of a case of ectodermal dysplasia: a multidisciplinary approach. J Dent Child. 2011;78(2):107–110. PMID: 22041116.
25. Di Lanaro M, Faker K, Cancio V. Ectodermal dysplasia: case report of aesthetic and functional rehabilitation. Braz Dent Sci. 2017;20(1):110–114. doi:10.14295/bds.2017.v20i1.1299
26. Sood A, Mishra D. Ectodermal dysplasia: case report and molecular review. Polymorphism. 2020;6:26.
27. Pinto AS, Conceição Pinto ME, Melo Do Val C, Costa Oliveira L, Costa de Aquino C, Vasconcelos DF. Prosthetic management of a child with hypohidrotic ectodermal dysplasia: 6-year follow-up. Case Rep Dent. 2016;2016:2164340. PMID: 27822392; PMCID: PMC5086375. doi:10.1155/2016/2164340
28. Hekmatfar S, Jafari K, Meshki R, Badakhsh S. Dental management of ectodermal dysplasia: two clinical case reports. J Dent Res Dent Clin Dent Prospects. 2012;6(3):108–112. PMID: 22991648; PMCID: PMC3442425. doi:10.5681/joddd.2012.023
29. Koyuncuoglu CZ, Metin S, Saylan I, Calısir K, Tuncer O, Kantarci A. Full-mouth rehabilitation of a patient with ectodermal dysplasia with dental implants. J Oral Implantol. 2014;40(6):714–721. PMID: 25506662. doi:10.1563/AAID-JOI-D-12-00072
30. Aragon C. Prosthodontic rehabilitation of an adult patient with hypohidrotic ectodermal dysplasia: a case report. Oral Health Group; 2020. Available from: https://www.oralhealthgroup.com/features/prosthodontic-rehabilitation-of-an-adult-patient-with-hypohidrotic-ectodermal-dysplasia-A-case-report/.
31. Nakayama Y, Baba Y, Tsuji M, et al. Dentomaxillofacial characteristics of ectodermal dysplasia. Congenit Anom. 2015;55(1):42–48. PMID: 25181309. doi:10.1111/cga.12073
32. Terheyden H, Wüsthoff F. Occlusal rehabilitation in patients with congenitally missing teeth-dental implants, conventional prosthetics, tooth autotransplants, and preservation of deciduous teeth-a systematic review. Int J Implant Dent. 2015;1(1):30. PMID: 27747652; PMCID: PMC5005685. doi:10.1186/s40729-015-0025-z
33. Wimalarathna AAAK, Weerasekara WBMCRD, Herath EMUCK. Comprehensive management of ectodermal dysplasia with interceptive orthodontics in a young boy who was bullied at school. Case Rep Dent. 2020;2020:6691235. PMID: 33489382; PMCID: PMC7790564. doi:10.1155/2020/6691235
34. Ruhin B, Martinot V, Lafforgue P, Catteau B, Manouvrier-Hanu S, Ferri J. Pure ectodermal dysplasia: retrospective study of 16 cases and literature review. Cleft Palate Craniofac J. 2001;38(5):504–518. PMID: 11522173. doi:10.1597/1545-1569_2001_038_0504_pedrso_2.0.co_2
35. Pigno MA, Blackman RB, Cronin RJ Jr, Cavazos E. Prosthodontic management of ectodermal dysplasia: a review of the literature. J Prosthet Dent. 1996;76(5):541–545. PMID: 8933447. doi:10.1016/s0022-3913(96)90015-3
36. Kramer FJ, Baethge C, Tschernitschek H. Implants in children with ectodermal dysplasia: a case report and literature review. Clin Oral Implants Res. 2007;18(1):140–146. PMID: 17224035. doi:10.1111/j.1600-0501.2006.01180.x
37. Stanford CM, Guckes A, Fete M, Srun S, Richter MK. Perceptions of outcomes of implant therapy in patients with ectodermal dysplasia syndromes. Int J Prosthodont. 2008;21(3):195–200. PMID: 18548955.
38. Chrcanovic BR. Dental implants in patients with ectodermal dysplasia: a systematic review. J Craniomaxillofac Surg. 2018;46(8):1211–1217. PMID: 29884311. doi:10.1016/j.jcms.2018.05.038
39. Bidra AS, Martin JW, Feldman E. Complete denture prosthodontics in children with ectodermal dysplasia: review of principles and techniques. Compend Contin Educ Dent. 2010;31(6):426–33; quiz 434, 444. PMID: 20712106.
40. Bhargava A, Sharma A, Popli S, Bhargava R. Prosthodontic management of a child with ectodermal dysplasia: a case report. J Indian Prosthodont Soc. 2010;10(2):137–140. PMID: 21629459; PMCID: PMC3081263. doi:10.1007/s13191-010-0026-9
41. Shaw RM. Prosthetic management of hypohidrotic ectodermal dysplasia with anodontia. Case report. Aust Dent J. 1990;35(2):113–116. PMID: 2346400. doi:10.1111/j.1834-7819.1990.tb05873.x.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.