")
Back to Journals » Clinical Epidemiology » Volume 13
Prognostic Factors and a Nomogram Predicting Survival in Patients with Breast Ductal Carcinoma in situ with Microinvasion: A Population-Based Study
Authors Zheng YZ , Qin HB, Li ZZ, Jiang HS, Zhang G, Yang SW, Wang XM, Xu YC, Deng ZH , Liu GW
Received 16 October 2021
Accepted for publication 12 November 2021
Published 30 November 2021 Volume 2021:13 Pages 1095—1108
DOI https://doi.org/10.2147/CLEP.S341422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Yi-Zi Zheng,1,2 Hong-Bin Qin,1 Zi-Zheng Li,1 He-Sheng Jiang,3 Greg Zhang,4 Shi-Wei Yang,5 Xian-Ming Wang,2 Yang-Chun Xu,1 Zhen-Han Deng,6 Guo-Wen Liu2
1Department of Thyroid and Breast Surgery, The People’s Hospital of Hechi, Hechi, Guangxi, People’s Republic of China; 2Department of Thyroid and Breast Surgery, Shenzhen Breast Tumor Research Center for Diagnosis and Treatment, National Standardization Center for Breast Cancer Diagnosis and Treatment, The First Affiliated Hospital of Shenzhen University, Shenzhen Second People’s Hospital, Shenzhen, Guangdong, People’s Republic of China; 3Department of Surgery, Oregon Health & Science University, Portland, OR, USA; 4McGovern Medical School, University of Texas Health Science Center at Houston, Houston, TX, USA; 5Teaching Office, The First Affiliated Hospital of Shenzhen University, Shenzhen Second People’s Hospital, Shenzhen, Guangdong, People’s Republic of China; 6Department of Sports Medicine, the First Affiliated Hospital of Shenzhen University, Shenzhen Second People’s Hospital, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Yang-Chun Xu
Department of Thyroid and Breast Surgery, The People’s Hospital of Hechi, Middle 455 Jinchengjiang Road, Hechi, 547000, Guangxi, People’s Republic of China
Tel/Fax +86-778-2293900
Email [email protected]
Yi-Zi Zheng
Department of Thyroid and Breast Surgery, Shenzhen Breast Tumor Research Center for Diagnosis and Treatment, National Standardization Center for Breast Cancer Diagnosis and Treatment, The First Affiliated Hospital of Shenzhen University, Shenzhen Second People’s Hospital, 3002 Sungang West Road, Shenzhen, 518035, Guangdong, People’s Republic of China
Tel/Fax +86-755-83366388
Email [email protected]
Purpose: Ductal carcinoma in situ with microinvasion (DCISM) can be challenging to balance the risks of overtreatment versus undertreatment. We aim to identify prognostic factors in patients with DCISM and construct a nomogram to predict breast cancer-specific survival (BCSS).
Materials and Methods: A retrospective cohort study of women diagnosed with DCISM from 1988 to 2015 who were identified in the Surveillance, Epidemiology and End Results database. Clinical variables and tumor characteristics were evaluated, and Cox proportional-hazards regression was performed. A nomogram was constructed from the multivariate logistic regression to combine all the prognostic factors to predict the prognosis of DCISM patients at 5 years, 10 years, and 15 years.
Results: We identified 5438 total eligible breast cancer patients with a median and max survival time of 78 and 227 months, respectively. Here, patients with poorer survival outcomes were those diagnosed between 1988 and 2001, African-American race, under 40 years of age, higher tumor N stage, progesterone receptor-negative tumor, and received no surgery. The nomogram was constructed by the seven variables and passed the calibration and validation steps. The area under the receiver operating characteristic (ROC) curve (AUC) of both the training set and the validating set (5-year AUC: 0.77 and 0.88, 10-year AUC: 0.75 and 0.73, 15-year AUC: 0.72 and 0.65). Receiving chemotherapy was associated with a better BCSS (hazard ratio, HR=0.45, 95% confidence interval, 95% CI = 0.23– 0.89), especially in patients with estrogen receptor (ER) negative, progesterone receptor (PR) negative (HR = 0.35, 95% CI = 0.13– 0.97) and ER+PR-/ER-PR+ DCISM (HR = 0.07, 95% CI = 0.01– 0.59).
Conclusion: Our current study is the first to construct nomograms of patients with DCISM which could help physicians identify breast cancer patients that more likely to benefit from more intensive treatment and follow-up. Chemotherapy might benefit patients with ER-PR- and ER+PR-/ER-PR+ DCISM.
Keywords: breast cancer, ductal carcinoma in situ, microinvasion, nomogram, survival
Introduction
Ductal carcinoma in situ (DCIS) with microinvasion (DCISM) is a mostly preinvasive breast carcinoma with a small component of invasive disease (presence of one or more foci of stromal invasion, none exceeding 1 mm in size) and presumably has a low but plausible risk of metastasis.1,2 Tumors with any invasive foci of 1mm or larger in size are defined as invasive carcinoma.1,2 Microinvasive carcinoma is an uncommon disease, accounting for a mere 1% of all breast cancer diagnoses;3–5 furthermore, tumor microinvasion is found in association with only approximately 5–10% of DCIS cases.6–8 Microinvasive cancer is rarely ever seen in the absence of an adjacent in situ lesion.6 This may be due to difficulty visualizing an isolated 1-mm invasive component, whereas an adjacent in situ lesion will dramatically enhance its detectability. Consequently, microinvasive carcinoma is usually described as “DCIS with microinvasion” despite the presence of DCIS not being necessary. Although DCISM patients account for only a small proportion of total breast cancer cases, the incidence of DCISM continues to increase along with a very significant rise in DCIS as a result of increased detection of breast cancer with the widespread adoption of mammography screening.9,10
Current guidelines from the National Comprehensive Cancer Network (NCCN) recommend DCIS treatment and systemic therapy utilization for the majority of DCISM cases, which more closely reflects the therapeutic guidelines for DCIS than for that of invasive carcinoma.11 However, several years ago it was recommended that patients with microinvasive carcinoma be treated the same as patients with small invasive cancers.12 While surgery is the standard treatment in DCIS and the majority of invasive carcinomas, additional treatment options vary quite widely between the two entities. Most notably, adjuvant chemotherapy is part of the national treatment guidelines for many invasive breast cancers but is not recommended for DCIS.13 Given that DCISM is relatively rare compared to pure DCIS and most invasive ductal carcinomas, there exists limited and controversial data regarding its tumor biology and diseases prognosis that serves to guide disease management and patient counseling. Several single-institution retrospective studies have reported clinical features, management, and prognostic implications for DCISM, but yield conflicting results.14–16 Although DCIS, DCISM, and T1a invasive ductal carcinoma (invasive tumor size >0.1 cm but ≤0.5 cm in greatest dimension was classified as T1a) all have generally excellent prognosis, some population-based studies have revealed that DCISM more closely resembles small invasive carcinoma than pure DCIS and many practitioners are treating it accordingly as such.17,18 Breast cancer, even with microinvasion, is a very heterogeneous disease characterized by diverse histopathologic and molecular features that are associated with distinct clinical outcomes. As a result, it can be challenging to balance the potential risks of overtreatment versus undertreatment in DCISM.
The American Joint Committee for Cancer (AJCC) staging system is a widely used tool for clinicians to predict disease outcomes and guide therapeutic decision making.19,20 However, given the many variables that influence the course of cancer, a prognosis based on the AJCC staging system alone is simply insufficient. A precise estimate of DCISM mortality is required to evaluate the clinical implications of this early-stage cancer and guide individualized therapeutic approaches. Nomograms, with the ability to generate an individual probability of a clinical event by integrating biological and clinical variables, help fulfill this requirement and aid in the development of personalized medicine.21–23 There are currently no studies constructing a nomogram for DCISM female breast cancer. To address this issue, this study aims to establish a comprehensive and reliable prognostic model of DCISM by building a nomogram to better understand the risk factors and prognosis. And by risk regression analysis and propensity score matching method, we aim to deepen the understanding about chemotherapy, radiotherapy and surgery utility in DCISM patients. To obtain a sufficient number of DCISM cases, the Surveillance, Epidemiology and End Results (SEER) cancer database of the National Cancer Institute was used in this study.
Materials and Methods
Source of Data
Study data was obtained from the SEER database of the National Cancer Institute, an open access resource for epidemiologic and survival analyses of various cancers, consisting of a collection of 18 high quality population-based cancer registries with very high estimated completeness of reporting. All data is publicly available and de-identified, and therefore exempted from the review of an Institutional Review Board. SEER database data do not require informed consent.
The SEER*Stat software from the National Cancer Institute (Surveillance Research Program, National Cancer Institute SEER*Stat software, http://www.seer.cancer.gov/seerstat) (Version 8.1.5) was used to identify eligible patients with the following inclusion criteria: female, diagnosed between 1988–2015, pathological diagnosis of breast ductal carcinoma, unilateral breast cancer, stage T1mic (defined as presence of one or more foci of stromal invasion, none exceeding 1 mm in size), one primary site only, and known age at diagnosis. Information regarding the human epidermal growth factor receptor-2 (HER2/neu) status is only available in the SEER database from 2010 onwards; therefore, HER2 variable was not included in the analysis. Patients diagnosed with breast cancer after 2015 were excluded to ensure adequate follow-up time. The pathological diagnosis was based on the primary site and according to the International Classification of Disease for Oncology, Third Edition (ICD-O-3). Breast cancer-specific survival (BCSS) was the primary study outcome of the SEER data, which was calculated as the time period from the date of diagnosis to the date of breast cancer-specific death. The causes of death were categorized as either breast cancer related or non-breast cancer related. Patients who died of non–breast cancer related causes were censored regarding the date of death.
Nomogram Development
The following clinical variables were extracted for the study: year of diagnosis, age, marital status, race, N stage (derived from AJCC stage group 6th edition), primary site, laterality, grade, estrogen receptor (ER) status, progesterone receptor (PR) status, surgery, chemotherapy, radiation. Continuous predictors were tested for linearity and converted to categorical variables if the relationship was determined to be nonlinear. Categorical variables were collapsed over categories, with no significant differences. For nomogram construction and validation, all cases were randomly divided into training (n = 3,806) and validating (n = 1,632) cohorts with a ratio of 7:3.24 Univariate and multivariate Cox regression were then used to screen for variables that significantly correlated with BCSS in the training group. After backwards stepdown validation, predictors that remained in the model were year of diagnosis, age, race, N stage, PR status, surgery, and chemotherapy. The resulting multivariate Cox regression model was used to calculate risk score and build the final nomogram prognostic model.
Model Validation
The validity of the nomogram was tested by discrimination and calibration.21 The discrimination was estimated by the area under the receiver operating characteristic (ROC) curve (AUC).25 The theoretical value of the AUC is between 0 and 1; an AUC larger than 0.5 indicates prediction performance better than random chance. Calibration curves were plotted to evaluate the consistency between predicted and actual survival rates at 5, 10, and 15 years.22 A perfect prediction would result in a 45-degree calibration curve (ie, the identity line).
Other Statistical Methodologies
To account for differences in baseline characteristics across the groups, we matched each patient who received chemotherapy to another patient who did not using the following predetermined factors: year of diagnosis, age, marital status, race, N stage, primary site, laterality, grade, ER status, PR status, surgery, chemotherapy, radiation. Propensity score matching method was utilized and the matching quality was tested. Kaplan–Meier curves, with the corresponding results of Log rank tests, were constructed for breast cancer-specific survival. The same methodology was carried out for patients receiving radiation therapy. All statistical analyses were performed in SPSS (version 24.0; IBM Corp, Armonk, NY, USA) or R environment (version 3.4.0; Vienna, Austria; http://www.R-project.org). All tests were two-sided, and the results were presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
Results
Clinicopathological Characteristics of Patients
Application of the aforementioned inclusion and exclusion criteria resulted in a final study population of 5,438 DCISM cases (Figure 1). These cases were randomly divided into two distinct groups: 3,806 cases were used as the training cohort, while 1,632 cases were used as the validating cohort. The follow-up time ranged from 0 to 227 months (median 78 months) for the training cohort and from 0 to 226 months (median 78 months) for the testing cohort. Patient, disease, and treatment characteristics for the study population are summarized in Table 1. The demographic and clinical variables were similar in the training and validating groups. The majority of patients were diagnosed between 2002–2015, over 40 years of age, Caucasian, tumor grade II–III, ER positive, N0-N1 stage, had undergone surgery and had no chemotherapy.
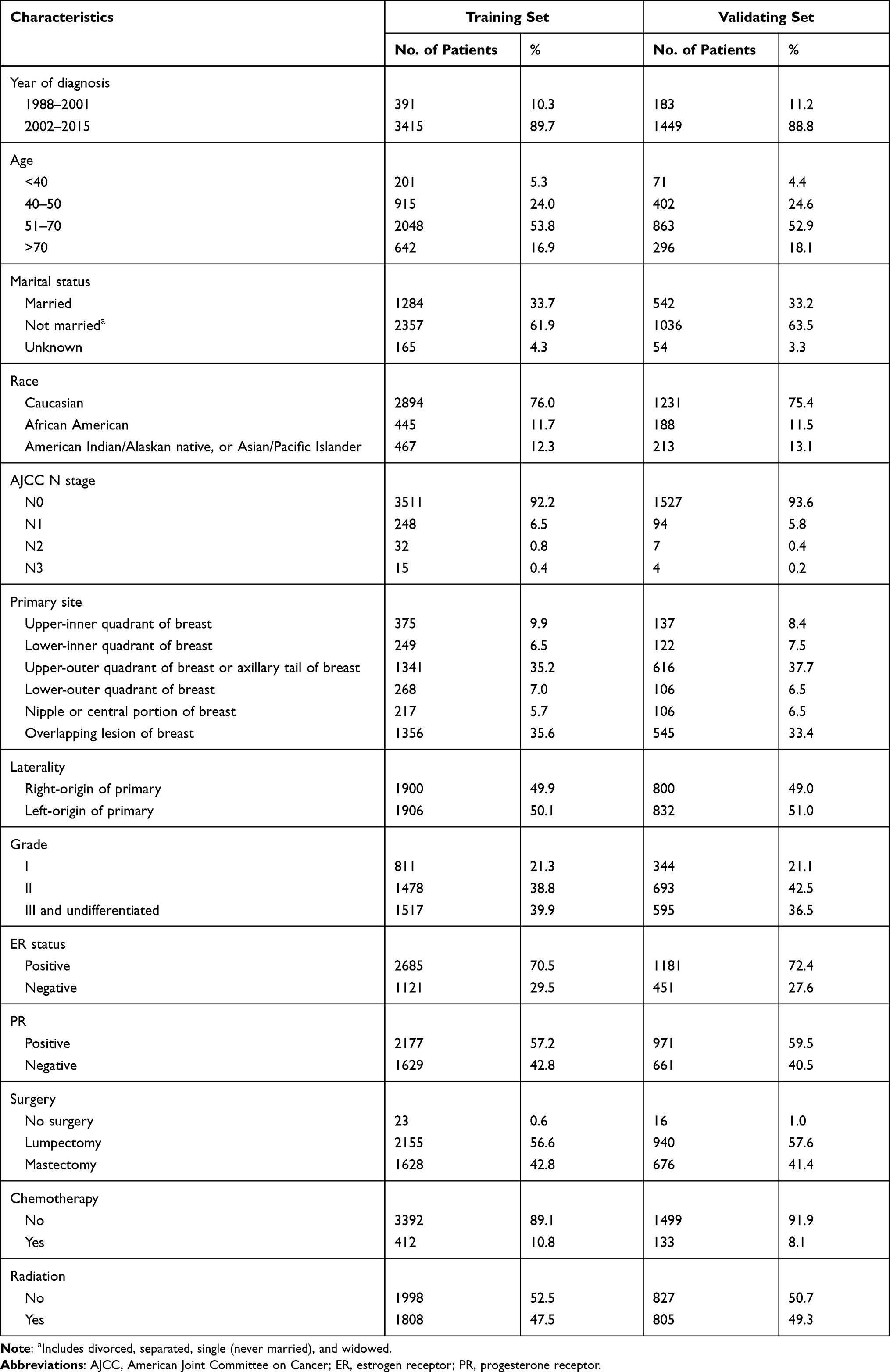 |
Table 1 The Individual Characteristics of Variables Involved in the Study |
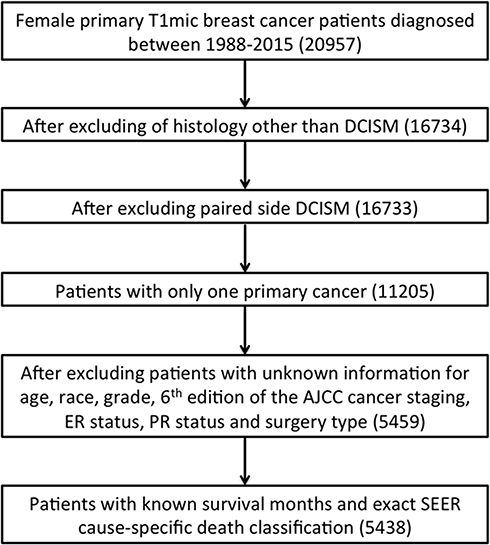 |
Figure 1 Flowchart of the case selection process in the study. Abbreviations: DCISM, ductal carcinoma in situ with microinvasion; ER, estrogen receptor; PR, progesterone receptor. |
Building Nomogram Prognostic Model in Training Cohort
In the univariate analysis, each of the following variables significantly increased the BCSS: “diagnosed in 2002–2015”, “age between 40 and 70”, “married”, “Caucasian”, “N0 stage”, “grade I and II”, “PR positive”, “received surgery”, “no chemotherapy” and “received radiotherapy” (Table 2). According to multivariate analysis, patients diagnosed between 2002–2015 were associated with decreased BCSS compared with patients diagnosed between 1988–2001 (HR=0.56, 95% CI=0.37–0.84). Older age at diagnosis showed association with better BCSS except for the group older than 70 (HR=0.41, 95% CI=0.22–0.78 for age 40–50; HR=0.53, 95% CI=0.30–0.96 for age 51–70; HR=1.40, 95% CI=0.72–2.74 for age over 70). African American patients had worse BCSS than Caucasian at 1.69 times (95% CI=1.06–2.68). More advanced in AJCC N stage corresponded to an increased risk of BCSS (HR=2.69, 95% CI=1.57–4.62 for N1; HR=4.29, 95% CI=1.64–11.19 for N2; HR=9.32, 95% CI=3.23–26.94 for N3). Patients with PR positive breast cancer had a significantly better BCSS than those who with PR negative cancer at 0.503 times (95% CI=0.32–0.80). Receiving surgery, whether lumpectomy or mastectomy, corresponded to significantly better BCSS (HR=0.11, 95% CI=0.04–0.28 for lumpectomy; HR=0.12, 95% CI=0.05–0.28 for mastectomy). Patients who received chemotherapy seemed to have worse BCSS (HR=2.21, 95% CI=1.29–3.76). After stepwise selection via multivariate analysis to further remove potential redundancies, the year of diagnosis, age, race, N stage, PR status, surgery, and chemotherapy were used in the final nomogram model (coefficients summarized in Table 2). The final risk scores for 5-year, 10-year, and 15-year BCSS were calculated by adding up the score of each item using the nomogram depicted in Figure 2. It was demonstrated that surgery contributed the most to prognosis, followed by N stage, age, race, chemotherapy, year of diagnosis, and lastly PR status. Based on this nomogram, some percent of patients would have a 5-year, 10-year or 15-year predicted BCSS under 90%.
 |
Table 2 Univariate and Multivariate Analyses of Breast Cancer-Specific Mortality |
 |
Figure 2 Nomogram to calculate risk score and predict 5-year, 10-year, and 15-year BCSS probability. By summing the points identified on the top scale for each independent variable and drawing a vertical line from the total points scale to the 5-year, 10-year, and 15-year BCSS, the corresponding survival probability can be obtained. Age, 1 = under 40 years, 2 = 41–50 years, 3 = 51–70 years, 4 = over 70 years; Race, 1 = Caucasian, 2 = African American, 3 = American Indian/Alaska Native or Asian/Pacific Islander; Year of diagnosis, 1 = 1988–2001, 2 = 2002–2015; AJCC 6th N stage, 0 = N0 stage, 1 = N1 stage, 2 = N2 stage, 3 = N3 stage; Surgery, 0 = no surgery, 1 = lumpectomy, 2 = mastectomy; Chemotherapy, 0 = no, 1 = yes; PR status, 0 = negative, 1 = positive. Abbreviations: BCSS, breast cancer-specific survival; PR, progesterone receptor.BCSS, breast cancer-specific survival; PR, progesterone receptor. |
Validation and Calibration of the Nomogram
The proposed nomogram was finally validated by discrimination and calibration measures in the independent testing set. The receiver operating characteristic (ROC) curves were plotted both internally and externally in the training and validating sets (Figure 3A and B). In the training set, the AUC for 5-year, 10-year, and 15-year BCSS were 0.77, 0.75 and 0.72, respectively. In the validating set, the AUC for 5-year, 10-year, and 15-year BCSS were 0.88, 0.73 and 0.65, respectively. This confirms the relatively strong prognostic power of the proposed nomogram. A calibration curve at 5 years (Figure 3C), 10 years (Figure 3D) or 15 years (Figure 3E) also showed high consistency between predicted probability and actual proportion of BCSS. The bias-corrected curve as well as the apparent curve were close to the ideal curve which falls along the 45-degree line, demonstrating the robustness of this nomogram. The 5-year, 10-year and 15-year BCSS of the whole study cohort were 98.5%, 96.7% and 95.2%, respectively (Figure 3F). The 5-year, 10-year and 15-year BCSS of the ER+PR+ subgroup were 99.1%, 97.5% and 95.5%, respectively (Figure 3F). The 5-year, 10-year and 15-year BCSS of the single hormone receptor positive (ER+PR- and ER-PR+) subgroup were 97.8%, 95.5% and 94.3%, respectively (Figure 3F). And The 5-year, 10-year and 15-year BCSS of the ER-PR- subgroup were 97.5%, 95.8% and 95%, respectively (Figure 3F).
 |
Figure 3 ROC curves and calibration plots for predicting BCSS. ROC curves of the nomogram predicting prognosis in the training set (A) and the validating set (B). Calibration curves comparing predicted and actual BCSS proportions at 5-year (C), 10-year (D), and 15-years (E), separately. Each point in the plot refers to a group of patients, with the nomogram predicted probability of survival shown on x axis and actual survival proportion shown on y axis. Distributions of predicted survival probabilities are plotted at the top. Error bars represent 95% confidence intervals. (F) 5-year, 10-year and 15-year BCSS in patients with each subtype of breast ductal carcinoma in situ with microinvasion. Abbreviations: AUC, area under the ROC curve; BCSS, breast cancer-specific survival; ER, estrogen receptor; PR, progesterone receptor; ROC, receiver operating characteristic curve. |
Statistical Matching for Chemotherapy and Radiotherapy
Chemotherapy and radiotherapy were both commonly applied adjuvant therapies for treatment of breast cancer. Therefore, survival analyses were additionally performed for these two important variables. To ensure that differences in outcome were not attributed to baseline differences in demographic and clinical characteristics across the therapeutic groups, we performed a 1:1 (chemotherapy: no chemotherapy) matched case-control analysis using the propensity score-matching method. We obtained a group of 726 patients with 363 patients from each chemotherapy group (Figure 4A). Here, we found that chemotherapy was associated with a better BCSS of DCISM (Figure 4A, HR=0.45, 95% CI=0.23–0.89). After stratified by ER and PR status, chemotherapy was not associated with BCSS in patients with ER+PR+ DCISM (Figure 4B, HR=1.66, 95% CI=0.35–7.86). However, benefit with chemotherapy was observed in patients with ER+PR-/ER-PR+ and ER-PR- DCISM (Figure 4C, ER+PR-/ER-PR+, HR=0.07, 95% CI=0.01–0.59; Figure 4D, ER-PR-, HR=0.35, 95% CI=0.13–0.97). Short-term and long term BCSS of patients with different hormone receptor types of DCISM were summarized in Table 3. In ER+PR-/ER-PR+ subgroup, the 5-year BCSS for patients in the chemotherapy and non-chemotherapy groups were 97.8% and 80.1%; the 10-year BCSS were 97.8% and 93.9%; the 15-year BCSS were 97.8% and 73.4%, respectively (Table 3). In ER-PR- subgroup, the 5-year BCSS for patients in the chemotherapy and non-chemotherapy groups were 95.1% and 81.1%; the 10-year BCSS were 89.7% and 81.1%; the 15-year BCSS were 89.7% and 81.1%, respectively (Table 3). The same analysis was performed for radiotherapy with a group of 1,588 patients with 794 patients in each radiotherapy group (Figure 4E). From this, we determined that radiotherapy was not associated with BCSS of DCISM (Figure 4E, HR=0.87, 95% CI=0.49–1.57).
 |
Table 3 BCSS of Patients with DCISM Between Statistically Matched Chemotherapy and Non-Chemotherapy Groups |
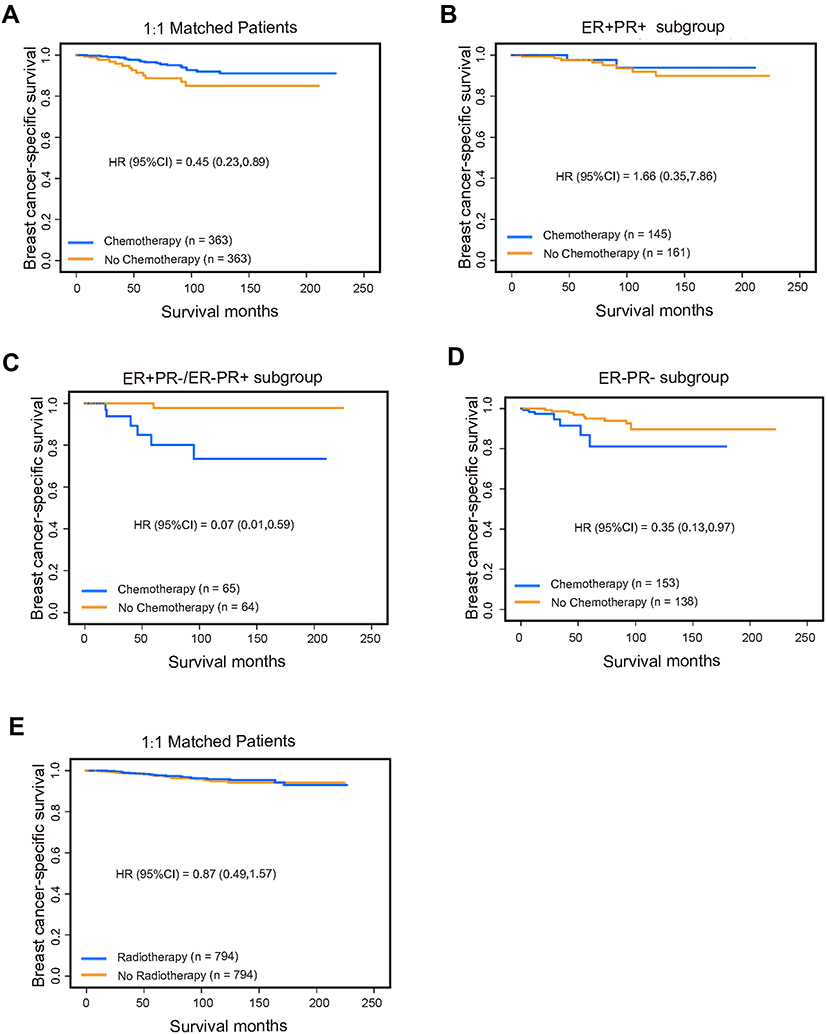 |
Figure 4 The survival curves for DCISM patients with and without chemotherapy and radiotherapy after 1:1 matching. (A) Kaplan-Meier curve depicting the association between chemotherapy and breast DCISM. Kaplan-Meier curve depicting the association between chemotherapy and breast DCISM in ER+PR+ (B), ER+PR-/ER-PR+ (C) and ER-PR- subgroup (D). (E) Kaplan-Meier curve depicting the association between radiotherapy and breast DCISM. Abbreviations: DCISM, ductal carcinoma in situ with microinvasion; ER, estrogen receptor; PR, progesterone receptor. |
Discussion
Because DCISM constitutes a small minority of cases of breast cancer, it has been difficult to definitively characterize its biological behavior, prognostic factors, and outcomes of multimodality therapy among patients. Previous studies have reported the prognostic implications and clinical management for DCISM, but the therapeutic recommendations proposed in microinvasive breast carcinomas are highly varied and remain controversial.14–16,26 Recent medical literature shows that current treatment patterns and prognosis of DCISM are comparable to those with small volume invasive ductal carcinoma.17,18 DCISM breast cancer is a quite heterogeneous disease and could be associated with distinct clinical outcomes. It remains challenging to find a proper, balanced treatment. In this study, a nomogram prognostic model was developed and validated using a large cohort of breast DCISM cases across the United States. Based on routinely available demographic, staging, and treatment information, this nomogram predicts the survival probability for individual DCISM patients and contributes to the development of personalized medicine.
In our present study, we constructed a comprehensive model based on a combination of various risk factors to predict prognosis of breast DCISM. The seven variables include age, race, year of diagnosis, AJCC N stage, PR status, chemotherapy, and surgery were kept in this nomogram after multivariate Cox regression screening and backward stepwise selection; these were all readily available information in the clinical database. Measured by the concordance index, the nomogram passed the discrimination step with an AUC of 0.77, 0.75 and 0.72 (for 5-, 10-, 15-year BCSS, respectively) in the training set and 0.88, 0.73 and 0.65 (for 5-, 10-, 15-year BCSS, respectively) in the validating set, suggesting a decent capability of discerning the breast cancer-specific death event most of the time. As characterized by the confidence intervals in calibration plots, there obviously lies an additional degree of uncertainty in a nomogram estimation. In general, this nomogram model is nevertheless quite reliable and robust in making accurate assessments and predictions but warrants external validation. As is illustrated in the nomogram, there are patients who would have a 5-year, 10-year or 15-year predicted BCSS less than 90%. Clinicians ought to determine more intensive treatment and follow-up strategy if predicted risk is sufficiently high.
The prognostic factors described in this study were basically consistent with findings of previous studies. Younger age, lymph node metastasis, multifocality, positive hormone receptor status have all previously been shown to be of significant relevance to the prognosis of DCISM patients.18,26–28 Diagnostic and therapeutic techniques have been improving over time and influencing prognosis of breast cancer. And the progress against cancer reflects large declines in mortality for breast cancer.9 Accordingly, patients diagnosed between 2002–2015 in this study had better BCSS than earlier cases did. Despite the increasing proportion of elderly patients with breast cancer, therapeutic guidelines for elderly patients are inconsistent, leading to challenges for clinicians in managing elderly patients.29 According to our analysis, patients over 70 showed similar BCSS to those who under 40. From previous publications, clinicians who manage elderly breast cancer patients should consider their comorbidities, functional status, clinical stages, biological characteristics of the cancer, and life expectancy, leading to the under-treatment of elderly patients compared with younger patients.30,31 Our study result was consistent with previous study that African Americans had a higher risk of death after a breast cancer diagnosis compared with women of other racial groups.32 Excluding the therapeutic factors, AJCC 6th edition N stage contributes the most to the final risk score (Figure 2), with HRs increasing with ascending N stages. The significant contribution of N stage to this nomogram strongly suggests that certain subsets of breast cancer may have an enhanced propensity to metastasize, exhibiting a worse prognosis even when the primary lesion is very small.33–35 However, the proportion of T1micN2-N3 stage cases (1.07% in this study cohort) was quite low. Despite a large initial study population, sub-stratification by AJCC N stage made the size of N2/N3 subgroup relatively small, yielding a limited statistical power. Consequently, it resulted in wide overlapping CIs and limited ability to detect differences precisely. It is evident from Figure 2 that patients with DCISM treated by lumpectomy had the same or even slightly lower risk scores than those who were treated by mastectomy. Data looking specifically at DCISM is quite limited. The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-06 has shown that stage I and II breast cancer patients who underwent lumpectomy with subsequent radiation had the same rate of survival as those who underwent mastectomies, which is consistent with the multivariate analysis results in our current study.36 A recent study based on well-matched, contemporary data revealed that breast-conserving therapy was associated with superior overall survival compared to mastectomy for early-stage breast cancer.37 Undergoing adjuvant chemotherapy in DCISM patients corresponded to a higher risk score according to the nomogram. This might be due to patients at higher risk of relapse being more likely to be selected for chemotherapy. After propensity score matching, patients treated with chemotherapy had better BCSS as expected, supporting the explanation that patients received chemotherapy had higher risk score was due to clinicopathological factors. In ER+PR+ subgroup analysis, we found no significant difference on BCSS between chemotherapy and non-chemotherapy groups. In ER+PR-/ER-PR+ and ER-PR- subgroup, however, BCSS was superior in the chemotherapy group compared with the other group. Study focusing on adjuvant chemotherapy received by DCISM patients is rare. As a small sample sized retrospective study reported, chemotherapy could improve the 5-year disease free survival of ER-/PR- DCISM patients (chemotherapy vs no chemotherapy, 95.8% vs 66.7%).38 And in our study, the 5-year, 10-year and 15-year BCSS of patients with ER+PR-/ER-PR+ were improved from 80.1%, 93.9% and 73.4% to 97.8%, 97.8% and 97.8%, respectively. Besides, the 5-year, 10-year and 15-year BCSS of patients with ER-PR- were improved from 81.1%, 81.1% and 81.1% to 95.1%, 89.7% and 89.7%, respectively. Although the precision was limited due to small sample size and insufficient events, the study results suggested the potential utility of this prognostic tool to identify candidates for chemotherapy if predicted risk is sufficiently high. Our data showed that patients with ER+PR+ DCISM had best short-term and long-term BCSS, patients with ER-PR- disease had worst short-term BCSS and patients with ER+PR-/ER-PR+ disease had worst long-term survival. From those results we can see that chemotherapy could benefit a certain subgroup of DCISM population with high risk of relapse, especially ER+PR-/ER-PR+ and ER-PR- subgroup. These results indicated that selecting the best implication of adjuvant chemotherapy for DCISM is important. In addition, there are some plausible explanations for why PR status passed the selection process and was kept in the nomogram while ER status did not. Firstly, our study supported the notion that ER positive, PR negative breast cancer is associated with reduced benefits from endocrine therapy39 and worse clinical outcomes.40 Secondly, ER positive breast cancers have a higher distant recurrence risk than triple-negative breast cancer,41 so these patients are mostly treated with endocrine therapy which would significantly reduce distant recurrence. Due to the lack of information about endocrine therapy, this therapeutic variable was not included during construction of the nomogram, which may have led to ER status being left out of the nomogram. Prognostic implications of applying adjuvant radiotherapy are further shown in Figure 4E. When statistically matched, radiotherapy showed no correlation with prognosis, indicating this adjuvant local-regional treatment might contribute more to local control than to BCSS. From NSABP B-17 and EORTC 10853 trials, radiotherapy reduced the risk of local recurrence instead of distant metastatic rate or overall survival in DCIS patients.42,43 For invasive breast cancer, however, radiotherapy to the conserved breast halves the rate at which the disease recurs and reduces the breast cancer death rate by about a sixth.44 In a sense, the significance of radiotherapy for DCISM is closer to DCIS than to invasive breast cancer.
There were several limitations in the study. Firstly, the information regarding the HER2/neu status is only available in the SEER database from 2010 onwards. If cases diagnosed before 2010 were excluded, the sample size would be dramatically reduced and follow-up time insufficient. Therefore, all cases diagnosed between 1988–2015 were enrolled and HER2 status was not included in the construction of the nomogram. Secondly, the SEER database lacks information about endocrine therapy, so this potential confounding factor could not be analyzed. Thirdly, the SEER database lacks information about surgical margin status or number of invasion foci, which might impact analysis. Fourthly, the retrospective nature of our study may have introduced a certain level of bias in our analysis results. Finally, the sequence of treatment was not considered. Because neither recurrence nor progression is recorded in SEER, we had to treat the therapies as baseline variables instead of time-varying covariates. As a result, it was assumed that the exact treatment combination was determined and given at the time point of diagnosis. Since the exact timing of the treatment is not available, relying on this assumption is necessary to incorporate the therapeutic information into the nomogram.
Conclusion
Controversy on DCISM is related to the limited information available on the prognosis of this disease. Our study comprehensively characterized prognostic factors and developed a nomogram prognostic model specifically for DCISM patients. Advanced AJCC N stage, no surgery, under 40 or over 70 years old, African American, diagnosed between 1988–2001, eligible for chemotherapy and PR negative were associated with worse BCSS. Chemotherapy might benefit patients with ER+PR-/ER-PR+ or ER-PR- DCISM. The Individualized risk score calculation method would help clinicians counsel patients more accurately about their prognosis and determine the best treatment strategy.
Abbreviations
DCISM, Ductal carcinoma in situ with microinvasion; DCIS, Ductal carcinoma in situ; BCSS, breast cancer-specific survival; AUC, area under the receiver operating characteristic curve; ROC, receiver operating characteristic; NCCN, National Comprehensive Cancer Network; AJCC, The American Joint Committee for Cancer; SEER, Surveillance, Epidemiology and End Results; HER2/neu, human epidermal growth factor receptor-2; ICD-O-3, International Classification of Disease for Oncology, Third Edition; ER, estrogen receptor; PR, progesterone receptor; NSABP, National Surgical Adjuvant Breast and Bowel Project; HR, hazard ratio; CI, confidence interval.
Data Sharing Statement
The datasets analyzed for this study can be found in the SEER database [http://www.seer.cancer.gov/ seerstat] Further inquiries can be directed to the corresponding author Yi-Zi Zheng.
Ethics Approval and Informed Consent
We obtained permission to access the SEER research data files using the reference number 15223-Nov2019. The data released by the SEER database do not require informed patient consent, and our study was approved by the Ethical Committee of Shenzhen Second People’s Hospital. The methods were performed in accordance with the principles stated in the Declaration of Helsinki.
Acknowledgments
We would like to thank Xian-Ming Wang for providing resources for this study.
Funding
This work was supported by the National Natural Science Foundation of China (Grant Numbers: 81902682, 81902303); Shanghai Sailing Program from Science and Technology Commission of Shanghai Municipality (Grant Number: 19YF1408900); Guangdong Basic and Applied Basic Research Foundation (Grant Number: 2021A1515011122, 2020A151501048); Shenzhen Science and Technology Project (Grant Number: JCYJ20210324103003010, JCYJ20190806170418445, JCYJ20190806164216661); and Clinical Research Project of Shenzhen Second People’s Hospital (Grant Number: 20203357028).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lakhani SR. Who Classification of Tumours of the Breast. International Agency for Research on Cancer; 2012.
2. Edge SB, Byrd DR, Carducci MA, et al. AJCC Cancer Staging Manual.
3. Hoda S, Chiu A, Prasad M, et al. Are microinvasion and micrometastasis in breast cancer mountains or molehills? Am J Surg. 2000;180:305–308.
4. Adamovich T, Simmons R. Ductal carcinoma in situ with microinvasion. Am J Surg. 2003;186:112–116.
5. Bianchi S, Vezzosi V. Microinvasive carcinoma of the breast. Pathol Oncol Res. 2008;14:105–111.
6. Shatat L, Gloyeske N, Madan R, et al. Microinvasive breast carcinoma carries an excellent prognosis regardless of the tumor characteristics. Hum Pathol. 2013;44:2684–2689.
7. Silver S, Tavassoli F. Mammary ductal carcinoma in situ with microinvasion. Cancer. 1998;82:2382–2390.
8. Padmore R, Fowble B, Hoffman J, et al. Microinvasive breast carcinoma: clinicopathologic analysis of a single institution experience. Cancer. 2000;88:1403–1409.
9. Siegel R, Miller K, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30.
10. Pfeiffer R, Webb-Vargas Y, Wheeler W, et al. Proportion of u.S. Trends in breast cancer incidence attributable to long-term changes in risk factor distributions. Cancer Epidemiol Biomark Prev. 2018;27:1214–1222.
11. Gradishar W, Anderson B, Abraham J, et al. Breast cancer, version 3.2020, NCCN clinical practice guidelines in oncology. J Natl Compreh Cancer Net. 2020;18:452–478.
12. Gradishar WJ, Anderson BO, Balassanian R, et al. Breast cancer version 2.2015. J Natl Compreh Cancer Net. 2015;13:448–475.
13. Goetz MP, Gradishar WJ, Anderson BO, et al. NCCN guidelines insights: breast cancer, version 3.2018. J Natl Compreh Cancer Net. 2019;17:118–126.
14. Parikh R, Haffty B, Lannin D, et al. Ductal carcinoma in situ with microinvasion: prognostic implications, long-term outcomes, and role of axillary evaluation. Int J Radiat Oncol Biol Phys. 2012;82:7–13.
15. Li Y, Zhang S, Wei X, et al. The clinical features and management of women with ductal carcinoma in situ with microinvasion: a retrospective cohort study. Int J Surg. 2015;19:91–94.
16. Wang W, Zhu W, Du F, et al. The demographic features, clinicopathological characteristics and cancer-specific outcomes for patients with microinvasive breast cancer: a seer database analysis. Sci Rep. 2017;7:42045.
17. Champion C, Ren Y, Thomas S, et al. DCIS with microinvasion: is it in situ or invasive disease? Ann Surg Oncol. 2019;26:3124–3132.
18. Sopik V, Sun P, Narod S. Impact of microinvasion on breast cancer mortality in women with ductal carcinoma in situ. Breast Cancer Res Treat. 2018;167:787–795.
19. Plichta JK, Ren Y, Thomas SM, et al. Implications for breast cancer restaging based on the 8th edition AJCC staging manual. Ann Surg. 2020;271:169–176.
20. Lee S, Sohn G, Kim J, et al. A retrospective prognostic evaluation analysis using the 8th edition of the American joint committee on cancer staging system for breast cancer. Breast Cancer Res Treat. 2018;169:257–266.
21. Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16:e173–e180.
22. Iasonos A, Schrag D, Raj G, et al. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26:1364–1370.
23. Xiong Z, Deng G, Huang X, et al. Score for the survival probability in metastasis breast cancer: a nomogram-based risk assessment model. Cancer Res Treatment. 2018;50:1260–1269.
24. Lei Z, Li J, Wu D, et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis b virus-related hepatocellular carcinoma within the Milan criteria. JAMA Surg. 2016;151:356–363.
25. Hanley J, McNeil B. The meaning and use of the area under a receiver operating characteristic (roc) curve. Radiology. 1982;143:29–36.
26. Kapoor N, Shamonki J, Sim M, et al. Impact of multifocality and lymph node metastasis on the prognosis and management of microinvasive breast cancer. Ann Surg Oncol. 2013;20:2576–2581.
27. Mamtani A, Nakhlis F, Downs-Canner S, et al. Impact of age on locoregional and distant recurrence after mastectomy for ductal carcinoma in situ with or without microinvasion. Ann Surg Oncol. 2019;26:4264–4271.
28. Si J, Guo R, Pan H, et al. In situ multiple microinvasion foci in ductal carcinoma is associated with an increased risk of recurrence and worse survival outcome. Front Oncol. 2020;10:607502.
29. Jeon Y, You S, Lee J, et al. Optimal treatment of breast cancer in women older than 75 years: a Korea breast cancer registry analysis. Breast Cancer Res Treat. 2019;178:693–701.
30. Bouchardy C, Rapiti E, Blagojevic S, et al. Older female cancer patients: importance, causes, and consequences of undertreatment. J Clin Oncol. 2007;25:1858–1869.
31. Ring A, Harder H, Langridge C, et al. Adjuvant chemotherapy in elderly women with breast cancer (AChEW): an observational study identifying MDT perceptions and barriers to decision making. Ann Oncol. 2013;24:1211–1219.
32. Bandera E, Qin B, Lin Y, et al. Association of body mass index, central obesity, and body composition with mortality among black breast cancer survivors. JAMA Oncol. 2021. doi:10.1001/jamaoncol.2021.1499
33. Foulkes WD, Reis-Filho JS, Narod SA. Tumor size and survival in breast cancer–a reappraisal. Nat Rev Clin Oncol. 2010;7:348–353.
34. Bernards R, Weinberg RA. A progression puzzle. Nature. 2002;418:823.
35. Zheng Y-Z, Wang X-M, Fan L, et al. Breast cancer-specific mortality in small-sized tumor with stage iv breast cancer: a population-based study. Oncologist. 2020;25:1–10.
36. Fisher B, Bauer M, Margolese R, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985;312:665–673.
37. Wrubel E, Natwick R, Wright GP. Breast-conserving therapy is associated with improved survival compared with mastectomy for early-stage breast cancer: a propensity score matched comparison using the national cancer database. Ann Surg Oncol. 2021;28:914–919.
38. Niu H, Wei L, Yu J, et al. Is adjuvant chemotherapy necessary for patients with microinvasive breast cancer after surgery? Cancer Biol Med. 2016;13:142–149.
39. Liu X-Y, Ma D, Xu X-E, et al. Genomic landscape and endocrine-resistant subgroup in estrogen receptor-positive, progesterone receptor-negative, and her2-negative breast cancer. Theranostics. 2018;8:6386–6399.
40. Li Y, Yang D, Yin X, et al. Clinicopathological characteristics and breast cancer-specific survival of patients with single hormone receptor-positive breast cancer. JAMA Net Open. 2020;3:e1918160.
41. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363:1938–1948.
42. Wapnir I, Dignam J, Fisher B, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103:478–488.
43. Donker M, Litière S, Werutsky G, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma in situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized Phase III trial. J Clin Oncol. 2013;31:4054–4059.
44. Darby S, McGale P, Correa C, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet (London, England). 2011;378:1707–1716.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.