")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Profile of Sofosbuvir and Velpatasvir Combination in the Treatment of Chronic Hepatitis C in Children and Adolescents: Current Evidence
Authors Brigham D, Narkewicz MR
Received 15 August 2023
Accepted for publication 28 December 2023
Published 11 January 2024 Volume 2024:20 Pages 1—7
DOI https://doi.org/10.2147/TCRM.S326099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Dania Brigham, Michael R Narkewicz
Digestive Health Institute, Pediatric Liver Center, Children’s Hospital Colorado and University of Colorado School of Medicine, Section of Pediatric Gastroenterology, Hepatology and Nutrition, Aurora, CO, USA
Correspondence: Michael R Narkewicz, Email [email protected]
Abstract: Chronic hepatitis C (HCV) affects up to 3.25 million children and adolescents. Early treatment of HCV in children and adolescents reduces progression to advanced liver disease and cancer. Treatment for HCV has evolved to highly effective direct acting antiviral therapy in adults and now in children ≥ 3 years of age. This review focuses on the role of sofosbuvir and velpatasvir (SOF/VEL), a newer treatment of children and adolescents with chronic HCV. SOF/VEL is a pangenotypic DAA with primary clearance via the liver and biliary excretion. It has been studied in children and adolescents and is approved in the US for use in children and adolescents ≥ 3 years of age. Although the data are currently limited, SOF/VEL has demonstrated sustained viral response rates similar to comparable DAAs in the range of 95– 98%. To date, side effects have been minimal.
Keywords: pediatric hepatitis C, pediatric hepatitis C treatment
Introduction
Globally, approximately 3.25 million children aged under 18 years are estimated to be afflicted with active hepatitis C virus (HCV) infection.1 Vertical transmission is the principal route of HCV acquisition among children.2 Among children perinatally infected, an estimated 8% to 25% achieve spontaneous clearance of HCV infection, typically by age 7.3–5 However, the remaining individuals develop persistent chronic HCV infection, characterized by a slower progression of hepatic disease compared to adults.6 While pediatric HCV cases generally exhibit a more indolent course, liver disease progression has been reported, leading to severe complications such as liver cirrhosis,7–9 hepatocellular carcinoma,10,11 and advanced end-stage liver disease requiring liver transplantation.3,12 Recently, there has been an increase in HCV infection in adolescents, primarily related to IV drug use and other risk taking behaviors. The prevalence HCV infection may be as high as 5% in adolescents with high-risk behaviors.13
Early detection of chronic hepatitis C in children and adolescents is of paramount importance to prevent disease progression and its long-term consequences. Identifying infected individuals at an early stage allows for timely intervention, reducing the risk of developing advanced liver disease. Early detection also aids implementation of appropriate preventive measures to curb the spread of the virus.14 The timing of treatment initiation is a crucial consideration, especially for children with vertical HCV infection. Emerging evidence suggests that early treatment in this population can significantly improve outcomes and increase the likelihood of spontaneous viral clearance. Early intervention may prevent the establishment of chronic infection and minimize liver damage, providing a unique window of opportunity for effective therapy.
Current treatment options for chronic HCV in children and adolescents include interferon-based regimens and direct-acting antiviral (DAA) therapies. Interferon-based therapies, while effective, are associated with considerable side effects and limited efficacy in certain patient populations.15 In contrast, DAA therapies have revolutionized the landscape of pediatric HCV treatment, boasting higher efficacy rates and improved tolerability. These regimens offer high rates of virological cure, denoted by sustained virologic response (SVR) post-treatment, which is associated with diminished liver inflammation, decelerated fibrosis progression, and reduced risk of hepatocellular carcinoma. Additionally, SVR can contribute to the reversal of fibrosis or cirrhosis, and it plays a pivotal role in curtailing viral transmission.16–19
As the burden of chronic HCV in children and adolescents persists, the quest for more effective and safe treatment options continues. While DAA therapies have marked a significant breakthrough, ongoing research aims to evaluate the efficacy and safety in children, optimize dosing regimens, shorten treatment duration, and expand access to treatment. The development of novel antiviral agents and therapeutic strategies tailored to specific patient populations is paramount in achieving the goal of eradicating HCV infection in this vulnerable population.
Sofosbuvir and Velpatasvir Combination Therapy
Sofosbuvir (SOF), a potent HCV NS5B polymerase inhibitor, forms the basis of numerous antiviral regimens with low susceptibility to resistance.16 SOF and velpatasvir (VEL, SOF/VEL) combination therapy represents a breakthrough in the treatment of chronic hepatitis C in children and adolescents. This review will focus on what is known for SOF/VEL in pediatric and adolescents. Current published data are limited, and there are still gaps in our knowledge. This combination therapy consists of these two direct-acting antiviral agents, SOF and VEL, each targeting different stages of the HCV replication cycle, resulting in a potent and synergistic effect. SOF is a nucleotide analog inhibitor of the HCV NS5B polymerase, while velpatasvir is an NS5A inhibitor. This combination therapy effectively interferes with viral replication, leading to a sustained virologic response (SVR) and improved clinical outcomes in studies in adults.20–22 In adults, SOF/VEL combination therapy is a highly effective and well-tolerated treatment option for chronic hepatitis C with real-world studies demonstrating ~98% sustained viral response including individuals who were treatment experienced, those with HIV coinfection or renal disease or with compensated cirrhosis or advanced fibrosis.20,23,24 Preliminary data in children and adolescents suggest that it has similar efficacy to that seen in adults.25 Its unique mechanism of action, high efficacy rates across all HCV genotypes, and favorable safety profile make it a consideration for first-line therapy. Individualized dosing and treatment duration studies are still needed to ensure optimal outcomes in the pediatric population.
SOF/VEL therapy disrupts the viral life cycle at multiple points, leading to a significant reduction in viral load. SOF acts as a prodrug, converting to its active form (sofosbuvir triphosphate) within hepatocytes. This active metabolite acts as a chain terminator during HCV RNA replication, preventing further viral replication and propagation. VEL targets the NS5A protein, which plays a crucial role in viral assembly and replication. By inhibiting the NS5A protein, velpatasvir disrupts the formation of new viral particles, thus limiting the spread of the virus within the liver.
Regarding pharmacokinetics, both SOF and VEL are well-absorbed orally, allowing for convenient once-daily dosing. They exhibit favorable tissue penetration, particularly within the liver, the primary site of HCV replication. Their metabolism primarily occurs in the liver, with minimal renal excretion, making them suitable for use in children and adolescents with varying degrees of renal function.26
Clinical trials evaluating SOF/VEL therapy in children and adolescents have been limited to date but have demonstrated good efficacy as determined by SVR. In a multicenter registration study, published in abstract form, children and adolescents aged 3 to 17 years with chronic HCV infection were treated with SOF/VEL. The results revealed high SVR rates across different HCV genotypes, 83% among 3–5-year-olds, 93% among 6–11-year-olds, and 95% among 12–17-year-olds.27 In another multicenter registration study also in abstract form, SOF/VEL resulted in SVR rates >92% across HCV genotypes with a virologic failure rate of only 1% in both adolescents and children aged 6 to 11 years old.28 A single center open-label study of 50 children and adolescents 6–18 years of age with HCV treated with SOF/VEL demonstrated 100% SVR at 12 weeks.25 In this study, adverse events possibly or probably related to SOF/VEL were mild to moderate (headache, abdominal pain and asthenia were the most common) and were more common in the adolescents and none led to discontinuation of treatment. These observed virologic responses are comparable to the 95–99% SVR rates in the adult trials22,29 and demonstrate the potency and effectiveness of this combination in eradicating the virus and preventing disease progression. The lower response rate in younger children may be related to palatability of the preparations for children who cannot swallow tablets. SOF/VEL was initially approved by the FDA and EMA for children aged 6 and older with chronic HCV and extended by the FDA for children down to 3 years of age in 2021. Dosing is based on weight. For children ≥30 kg the dose is 400/110 mg of SOF/VEL daily. For individuals 17–29 kg, the dose is 200/50 mg daily and for those <17 kg it is 150/37.5 mg. Tablets are available for the first 2 dosing regimens, and oral granules are available for younger children. The standard treatment duration is 12 years. For the rare child or adolescent with decompensated cirrhosis, ribavirin (15 mg/kg/day divided into 2 doses) should be added to the regimen. The most recent guidelines for treatment and dosing can be found at https://www.hcvguidelines.org/unique-populations/children.
The safety profile of SOF/VEL available to date in pediatric patients has been consistently favorable. The limited data from the available clinical trials have shown that these medications are well tolerated, with the majority of adverse events being mild to moderate in severity. Serious adverse events were rare, and no new safety concerns have emerged during the course of these trials. The tolerability SOF/VEL is important in children and adolescents, as it can help with treatment adherence.
SOF/VEL has emerged as one of the several highly effective and safer alternatives to traditional interferon-based therapies. Interferon-based regimens, though effective in some cases, have been associated with significant side effects, including flu-like symptoms, anemia, and neuropsychiatric effects, which may be poorly tolerated, especially in pediatric patients. In contrast, SOF/VEL offers a shorter treatment duration, fewer side effects, and higher SVR rates, making it a potentially attractive treatment option for children and adolescents with chronic hepatitis C.
The dosing and duration of SOF/VEL is influenced by various factors, including the patient’s age, weight, and HCV genotype. Individualized dosing based on these factors is crucial to optimize treatment outcomes and ensure safety. Additionally, special populations, such as children under 12 years old and adolescents with comorbidities or HIV coinfection, may require further dose adjustments or close monitoring during treatment.26
The duration of therapy with SOF/VEL typically ranges from 12 to 24 weeks, depending on the patient’s HCV genotype and treatment history. The majority of pediatric patients achieve SVR after 12 weeks of therapy, reaffirming the efficacy of this regimen in a relatively short treatment period.27,30 However, in certain cases, especially in adolescents with advanced liver disease or previous treatment failures, a 24-week duration may be recommended to maximize treatment success.26 Glecaprevir/pibrentasvir (GLE/PIB) combination therapy does provide a similar SVR using a shorter duration of therapy (8 weeks) for treatment naïve children and adolescents than SOF/VEL.31 There is no significant difference in the duration of therapy between the 2 agents for treatment experienced children and adolescents31 (Table 1).
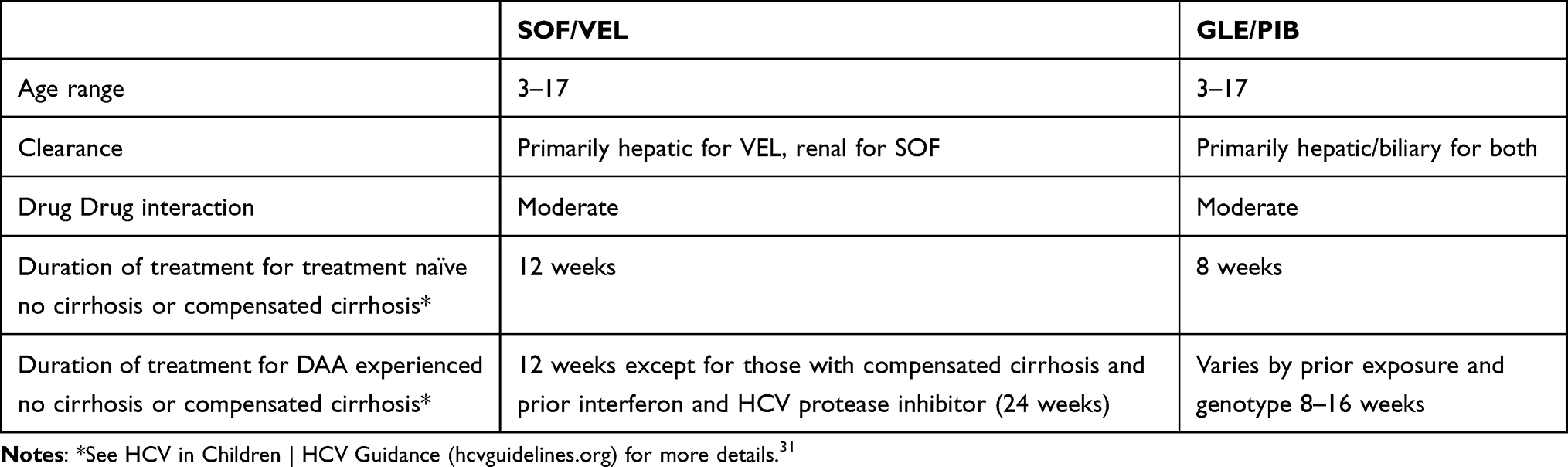 |
Table 1 Features of Pangenotypic DAA Therapies Available for Children and Adolescents |
Adverse Events and Safety Profile of Sofosbuvir and Velpatasvir Combination Therapy
The safety profile of SOF/VEL in pediatric patients with chronic hepatitis C is reassuring, with minimal serious adverse events and a low risk of drug–drug interactions. Given the limited published data, this should continue to be assessed in future studies. The mild and transient nature of common adverse events further supports its use as a well-tolerated treatment option for children and adolescents. However, close monitoring of patients, particularly those with pre-existing medical conditions or receiving concurrent medications, is essential to ensure optimal treatment outcomes and promote the successful eradication of the hepatitis C virus in this vulnerable population.
The most commonly reported adverse events associated with SOF/VEL in children and adolescents included mild and transient symptoms such as headache, fatigue, and gastrointestinal disturbances, including nausea and diarrhea.27,30,32 These adverse events were generally well tolerated and rarely lead to treatment discontinuation. The mild nature of these side effects is particularly important in pediatric populations, as it could enhance treatment adherence and minimizes the impact on the overall well-being of the young patients. Thus far, the incidence of severe adverse events leading to treatment discontinuation has been rare, emphasizing the overall safety of this treatment option in children and adolescents.
SOF/VEL has a moderate potential for drug–drug interactions similar to other pangenotypic DAA therapy, making it suitable for use in children and adolescents with comorbidities who may be on other medications. However, it is essential to consider potential interactions with other concomitant medications. For instance, certain anticonvulsants and herbal supplements may affect the pharmacokinetics of sofosbuvir or velpatasvir, necessitating dose adjustment and careful monitoring. Therefore, a comprehensive review of the patient’s current medication regimen is crucial to minimize the risk of drug interactions and ensure the safety of the combination therapy.26
Special Populations
Special populations, including children under 12 years old, adolescents with comorbidities, and adolescents with HIV coinfection, present unique challenges and considerations in the treatment of chronic hepatitis C with SOF/VEL. The limited data support the potential broader application of this treatment regimen in diverse patient groups, ensuring effective management of chronic hepatitis C and its associated complications in these vulnerable populations. However, close monitoring and individualized treatment plans remain essential to address specific clinical considerations and optimize treatment outcomes in each case.
The use of SOF/VEL in children under 12 years old has shown promising results in clinical trials. Studies by Jonas et al evaluated the safety and efficacy of this regimen in a cohort of pediatric patients aged 3 to 11 years.27,30 The study reported a high SVR rate of over 95% after 12 weeks of treatment, indicating its effectiveness in achieving viral clearance in this age group.27,30 Adverse events in children under 12 were consistent with those observed in older age groups and were generally mild and well tolerated. Similar data were found in the study by Pokorska-Spiewak et al for children 6–11 years of age.25 These findings support the consideration of the use of sofosbuvir and velpatasvir combination therapy as a viable treatment option for young children with chronic hepatitis C.
HIV and hepatitis C coinfection in adolescents can lead to liver disease progression and complications, necessitating effective antiviral therapy. Although there are no trials in children or adolescents, a large study in adults coinfected with HIV and HCC demonstrated high SVR rates and a favorable safety profile in this patient population. Treatment with SOF/VEL for 12 weeks resulted in SVR rates of 92–100% dependent on genotype. Importantly, the combination therapy did not adversely affect HIV control, and antiretroviral therapy remained effective during the course of hepatitis C treatment (Clinicaltrials.gov NCT02480712 results posting). This suggests that SOF/VEL combination therapy should be studied in adolescents coinfected with HIV and hepatitis C.
Cost-Effectiveness and Access to Treatment
Currently, no published data exist concerning the cost-effectiveness of SOF/VEL for pediatric hepatitis C. However, this topic has been a subject of investigation to determine the economic viability of this treatment approach in the adult population. A pertinent cost-effectiveness study by Ruggeri et al found that the extension of HCV treatment with SOF/VEL to patients in the early stages of infection, characterized by early fibrosis, rather than reserving treatment for those in more advanced disease stages, was a cost-effective strategy from the vantage point of the Italian Healthcare System.33 Consequently, one could infer that if SOF/VEL were utilized in children and adolescents, the majority of whom would be in the early stages of infection, it could also prove cost-effective. This study considered various factors, encompassing the direct medical costs of the medications, monitoring, adverse events, and the long-term impact of achieving sustained virologic response (SVR) in terms of averting liver-related complications and the associated healthcare expenditures. By considering these elements, the research provided valuable insights into the economic feasibility of using SOF/VEL in a broader context, which could potentially extend to the pediatric population.
Despite the proven cost-effectiveness of SOF/VEL in the adult literature, access to treatment remains a crucial concern. Insurance coverage plays a pivotal role in determining the accessibility of this therapy for pediatric patients with hepatitis C. Efforts are being made to expand insurance coverage to include this treatment regimen and ensure that more children and adolescents can benefit from its efficacy and safety. Advocacy for policy changes and inclusion of direct-acting antiviral treatments, including SOF/VEL, in insurance coverage guidelines are essential steps to improve access to treatment.
Global availability and affordability of SOF/VEL are also important considerations, particularly for resource-limited regions with a high burden of pediatric hepatitis C. The cost of these medications has been a barrier to widespread adoption in some countries. However, initiatives such as voluntary licensing agreements, differential pricing, and generic production have contributed to improving access and reducing costs in certain regions. Additionally, efforts by organizations like the World Health Organization (WHO) and pharmaceutical companies to expand access to affordable treatments for hepatitis C have shown progress in making these therapies more widely available.
Future Direction of Pediatric Hepatitis C
The field of pediatric HCV continues to evolve with ongoing research aimed at further improving treatment outcomes and expanding therapeutic options. Clinical trials are investigating novel antiviral agents, including pan-genotypic drugs such as SOF/VEL and recently SOF/VEL and voxilaprevir,32 to simplify treatment regimens and increase the efficacy of therapy in children and adolescents. Additionally, there is a growing focus on optimizing treatment duration and assessing the long-term impact of direct-acting antiviral therapy on liver-related outcomes. Collaborative efforts between researchers, healthcare providers, and pharmaceutical companies are essential in driving advancements and addressing unmet needs in the management of pediatric HCV.
Despite the availability of highly effective treatments like SOF/VEL, challenges persist in identifying and diagnosing pediatric patients with chronic hepatitis C. Inadequate screening and low awareness among healthcare providers and parents contribute to delayed diagnosis and treatment initiation. To overcome this challenge, public health campaigns and educational initiatives must be strengthened to increase awareness about HCV in children and adolescents. Routine screening in high-risk populations, such as those with maternal HCV infection or history of blood product transfusion, can facilitate early detection and timely intervention, ultimately reducing the burden of pediatric HCV.
Vertical transmission of HCV remains a concern, and there is an ongoing debate about the use of antiviral therapy during pregnancy to prevent mother-to-child transmission. While some studies have suggested that DAA treatment during pregnancy may reduce the risk of transmission, there are still uncertainties about its safety and potential long-term effects on the infant. Further research is needed to better understand the risks and benefits of maternal treatment, considering factors such as maternal genotype, timing of treatment, and potential implications for the developing fetus.
The availability of highly effective and safe treatment options, including SOF/VEL combination therapy, presents an opportunity for significant progress in combating pediatric HCV. The successful management of pediatric HCV can lead to improved health outcomes, reduced liver-related complications, and overall healthcare cost savings. Therefore, there is a crucial need for policymakers and public health authorities to prioritize screening programs and facilitate access to treatment for all affected children and adolescents. By investing in early detection, comprehensive care, and preventive strategies, public health initiatives can contribute to the goal of eliminating pediatric hepatitis C as a major public health concern.
Conclusion
In conclusion, SOF/VEL is a safe and effective treatment for pediatric HCV based on early clinical trial data. Early treatment with DAAs like SOF/VEL has high SVR rates in children and adolescents. There remain challenges in screening, and implementing effective public health policies, to achieve the elimination of pediatric HCV as a global health burden.
Disclosure
MN reports Consultant Vertex, Research Funding Gilead and AbbVie. The authors report no other conflicts of interest in this work.
References
1. Schmelzer J, Dugan E, Blach S, et al. Global prevalence of hepatitis C virus in children in 2018: a modelling study. Lancet Gastroenterol Hepatol. 2020;5(4):374–392. doi:10.1016/S2468-1253(19)30385-1
2. Indolfi G, Azzari C, Resti M. Perinatal transmission of hepatitis C virus. J Pediatr. 2013;163(6):1549–1552 e1541. doi:10.1016/j.jpeds.2013.06.077
3. Bortolotti F, Verucchi G, Camma C, et al. Long-term course of chronic hepatitis C in children: from viral clearance to end-stage liver disease. Gastroenterology. 2008;134(7):1900–1907. doi:10.1053/j.gastro.2008.02.082
4. Tovo PA, Calitri C, Scolfaro C, Gabiano C, Garazzino S. Vertically acquired hepatitis C virus infection: correlates of transmission and disease progression. World J Gastroenterol. 2016;22(4):1382–1392. doi:10.3748/wjg.v22.i4.1382
5. Yeung LT, To T, King SM, Roberts EA. Spontaneous clearance of childhood hepatitis C virus infection. J Viral Hepat. 2007;14(11):797–805. doi:10.1111/j.1365-2893.2007.00873.x
6. Garcia-Monzon C, Jara P, Fernandez-Bermejo M, et al. Chronic hepatitis C in children: a clinical and immunohistochemical comparative study with adult patients. Hepatology. 1998;28(6):1696–1701. doi:10.1002/hep.510280633
7. Badizadegan K, Jonas MM, Ott MJ, Nelson SP, Perez-Atayde AR. Histopathology of the liver in children with chronic hepatitis C viral infection. Hepatology. 1998;28(5):1416–1423. doi:10.1002/hep.510280534
8. Bortolotti F, Vajro P, Cadrobbi P, et al. Cryptogenic chronic liver disease and hepatitis C virus infection in children. J Hepatol. 1992;15(1–2):73–76. doi:10.1016/0168-8278(92)90014-G
9. Goodman ZD, Makhlouf HR, Liu L, et al. Pathology of chronic hepatitis C in children: liver biopsy findings in the Peds-C Trial. Hepatology. 2008;47(3):836–843. doi:10.1002/hep.22094
10. Gonzalez-Peralta RP, Langham MR, Andres JM, et al. Hepatocellular carcinoma in 2 young adolescents with chronic hepatitis C. J Pediatr Gastroenterol Nutr. 2009;48(5):630–635. doi:10.1097/MPG.0b013e318170af04
11. Strickland DK, Jenkins JJ, Hudson MM. Hepatitis C infection and hepatocellular carcinoma after treatment of childhood cancer. J Pediatr Hematol Oncol. 2001;23(8):527–529. doi:10.1097/00043426-200111000-00012
12. Barshes NR, Udell IW, Lee TC, et al. The natural history of hepatitis C virus in pediatric liver transplant recipients. Liver Transpl. 2006;12(7):1119–1123. doi:10.1002/lt.20793
13. Fernandes ND, Banik S, Abughali N, Sthapit B, Abdullah N, Fragassi P. Hepatitis C virus screening among adolescents attending a drug rehabilitation center. J Pediatric Infect Dis Soc. 2020;9(4):437–441. doi:10.1093/jpids/piz065
14. Indolfi G, Easterbrook P, Dusheiko G, et al. Hepatitis C virus infection in children and adolescents. Lancet Gastroenterol Hepatol. 2019;4(6):477–487. doi:10.1016/S2468-1253(19)30046-9
15. Jara P, Hierro L, de la Vega A, et al. Efficacy and safety of peginterferon-alpha2b and ribavirin combination therapy in children with chronic hepatitis C infection. Pediatr Infect Dis J. 2008;27(2):142–148. doi:10.1097/INF.0b013e318159836c
16. Fahmy DM, Shokeir M, El Zeiny SM, Jonas MM, Abdallah A. Changes in liver stiffness and noninvasive fibrosis scores in Egyptian adolescents successfully treated with ledipasvir-sofosbuvir for chronic hepatitis C virus infection. J Pediatr. 2021;231:110–116. doi:10.1016/j.jpeds.2020.12.031
17. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329–337. doi:10.7326/0003-4819-158-5-201303050-00005
18. Poynard T, McHutchison J, Manns M, et al. Impact of pegylated interferon alfa-2b and ribavirin on liver fibrosis in patients with chronic hepatitis C. Gastroenterology. 2002;122(5):1303–1313. doi:10.1053/gast.2002.33023
19. European Association for the Study of the Liver. Electronic address eee, clinical practice guidelines panel C, representative EGB, Panel m. EASL recommendations on treatment of hepatitis C: final update of the series(☆). J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018
20. Mangia A, Milligan S, Khalili M, et al. Global real-world evidence of sofosbuvir/velpatasvir as simple, effective HCV treatment: analysis of 5552 patients from 12 cohorts. Liver Int. 2020;40(8):1841–1852. doi:10.1111/liv.14537
21. Mangia A, Piazzolla V, Giannelli A, et al.. SVR12 rates higher than 99% after sofosbuvir/velpatasvir combination in HCV infected patients with F0-F1 fibrosis stage: a real world experience. PloS one. 2019;14:5.
22. Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection. New Engl J Med. 2015;373(27):2599–2607. doi:10.1056/NEJMoa1512610
23. Borgia SM, Dearden J, Yoshida EM, et al. Sofosbuvir/velpatasvir for 12 weeks in hepatitis C virus-infected patients with end-stage renal disease undergoing dialysis. J Hepatol. 2019;71(4):660–665. doi:10.1016/j.jhep.2019.05.028
24. Asselah T, Bourgeois S, Pianko S, et al. Sofosbuvir/velpatasvir in patients with hepatitis C virus genotypes 1–6 and compensated cirrhosis or advanced fibrosis. Liver Int. 2018;38(3):443–450. doi:10.1111/liv.13534
25. Pokorska-Spiewak M, Talarek E, Aniszewska M, et al. Efficacy and safety of treatment with sofosbuvir/velpatasvir in patients aged 6–18 years with chronic hepatitis C-Results of the PANDAA-PED study. Liver Int. 2023;43(9):1871–1878. doi:10.1111/liv.15637
26. Gilead Sciences, Inc. Epclusa (sofosbuvir/velpatasvir) prescribing information; 2016. Available from: https://www.gilead.com/~/media/files/pdfs/medicines/liver-disease/epclusa/epclusa_pi.pdf.
27. Sokal E, Schwarz KB, Rosenthal P, et al. Sofosbuvir/velpatasvir results in high sustained viral response rates in paediatric patients 3 to 17 years old with chronic hepatitis C infection. Poster presentation AASLD; 2020.
28. Jonas MM, Romero R, Sokal EM, et al. Safety and efficacy of sofosbuvir/velpatasvir in pediatric patients 6 to <18 years old with chronic hepatitis C infection [abstract 748]. Boston, Massachusetts: The Liver Meeting; 2019.
29. Foster GR, Afdhal N, Roberts SK, et al. Sofosbuvir and Velpatasvir for HCV Genotype 2 and 3 Infection. New Engl J Med. 2015;373(27):2608–2617. doi:10.1056/NEJMoa1512612
30. Jonas MM, Romero R, Rosenthal P, et al. Sofosbuvir–Velpatasvir in Children 3 to 17 Years Old With Hepatitis C Virus Infection. JPGN. 2023;2023:1.
31. American Association for the Study of Liver Diseases and Infectious Diseases Society of America. HCV guidance: recommendations for testing, managing, and treating hepatitis C. Available from: https://www.hcvguidelines.org/unique-populations/children.
32. Indolfi G, Kelly D, Nebbia G, et al. Sofosbuvir-velpatasvir-voxilaprevir in adolescents 12 to 17 years old with HCV infection. Hepatology. 2022;76(2):445–455. doi:10.1002/hep.32393
33. Ruggeri M, Romano F, Basile M, et al. Cost-effectiveness analysis of early treatment of chronic HCV with sofosbuvir/velpatasvir in Italy. Appl Health Econ Health Policy. 2018;16(5):711–722. doi:10.1007/s40258-018-0410-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.