")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Prevalence of Stunting and Its Associated Factors Among Children Residing in Internally Displaced Persons (IDP) Camps in Hargeisa, Somaliland: A Community-Based Cross-Sectional Study
Authors Abdeeq BA, Mohamed AI, Abdi AI, Mohamed J , Tamiru D , Abate KH
Received 13 September 2023
Accepted for publication 30 December 2023
Published 9 January 2024 Volume 2024:15 Pages 17—27
DOI https://doi.org/10.2147/PHMT.S439586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Laurens Holmes, Jr
Barkhad Aden Abdeeq,1 Ahmed Ismail Mohamed,2 Abdiwahab Ismail Abdi,3 Jama Mohamed,4 Dessalegn Tamiru,5 Kalkidan Hassen Abate5
1Department of Child Survival, Save the Children International, Hargeisa, Somaliland; 2Faculty of Nutrition and Food Science, University of Hargeisa, Hargeisa, Somaliland; 3School of Medical Laboratory Science, Edna Aden University, Hargeisa, Somaliland; 4Faculty of Statistics and Data Science, University of Hargeisa, Hargeisa, Somaliland; 5Department of Nutrition and Dietetics, Jimma University, Jimma, Ethiopia
Correspondence: Barkhad Aden Abdeeq, Email [email protected]
Background: Stunting, a consequence of prolonged malnutrition, remains a critical global health issue affecting 165 million children under the age of five, with 10.6 million associated deaths. Its stunting prevalence is particularly pronounced in developing nations, notably Sub-Saharan Africa. Chronic protein-energy malnutrition, identified as a major cause of morbidity and mortality in displaced settings, underscores the urgency of understanding its impact in such contexts.
Objective: This study aimed to assess the prevalence and associated factors of stunting among children aged 12– 59 months and residing in IDP camps in Hargeisa, Somaliland.
Methods: A community-based cross-sectional study was conducted in Hargeisa from May 5 to July 30, 2022, utilizing systematic random sampling, online mobile surveys, and caregiver interviews with anthropometric measurements. The SPSS version 25 was utilized in handled data entry, processing and analysis. Multivariable logistic regression, with p < 0.05 significance, included variables from bivariate analysis (p < 0.2). Stunting assessment utilized WHO AnthroPlus software, categorizing HAZ scores < − 2.0 SD.
Results: The prevalence of stunting among children living in IDP camps was found to be 21.1% [95% CI: 17.0– 24.91%]. Vaccination status (adjusted odds ratio [aOR] = 0.19, 95% CI: 0.09– 0.38), deworming practice (aOR = 6.5, 95% CI: 2.91– 14.52), place of delivery (aOR = 0.14, 95% CI: 0.07– 0.30), measles experience in the last year (aOR = 0.12, 95% CI: 0.04– 0.34), ANC visits (aOR = 0.33, 95% CI: 0.14– 0.81), and maternal insufficient extra food intake (aOR = 2.15, 95% CI: 1.11– 4.15) were significantly associated with stunting.
Conclusion: The observed stunting prevalence in IDP camps (21.1%) was substantial, highlighting the need for targeted interventions. Future efforts should aim to reduce stunting from the current rate to an estimated 5– 10%, emphasizing comprehensive measures such as deworming, maternal nutrition, postnatal care improvement, robust immunization, and promoting healthcare facility deliveries.
Keywords: stunting, IDP, Somaliland
Introduction
Chronic malnutrition among children under the age of five remains a global problem. Approximately 165 million children younger than five years have a height-for-age Z score of −2 or lower, indicating a 35% decline from the estimated 253 million in 2005, the prevalence of stunting has decreased from an estimated 40% in 1990.1 Globally, around two billion people suffer from hidden hunger, and in 2020, an estimated 149 million children under the age of five were stunted, indicating a failure to reach their expected height for their age.2,3
Various factors have been identified as associated with malnutrition, including poor breastfeeding and child feeding practices.4 Lack of access to nutritious food, low levels of parental education and income, inadequate healthcare services, and poor antenatal care are also recognized as key factors contributing to child malnutrition, diseases such as HIV infection can compromise nutritional status.1,4,5 Stunting is most prevalent in Sub-Saharan African countries, particularly in East and Central Africa, particularly, Burundi and Madagascar have the highest prevalence rates of stunting, at 54.6% and 48.4%, respectively. Eastern African countries, including Ethiopia, Kenya, and Uganda, also exhibit high prevalence rates of stunting, ranging from 29.0% to 47.7%.6,7
The predictors of childhood undernutrition are well-researched and could be classified as either proximate or distal, affecting the nutritional status of children at different levels. Proximate factors operate at the individual and child level, which includes age, sex, birth size, birth order, birth interval, and infections. Distal factors include a wider range of conceptual factors within the socio-cultural, economic, environmental, climatic and political context which influence food (in)security, sanitation, access to healthcare services, and education at the household and community levels. Studies have reported that these factors tend to vary spatially depending on geographic location and climatic conditions. Previous studies have reported a relationship between undernutrition and geographical region, clearly acknowledging that a child’s geographic location is an important modifier of known determinants of undernutrition.8–10 Undernutrition is common among underprivileged populations like women, children and adolescents, especially street dwellers. It is the single risk to global public health and by far the greatest contributing factor for child morbidity and mortality. It is a significant public health problem described as the silent murderer. This public health problem can affect any section of the population like children, adolescents, and pregnant women.11,12
In Somaliland, according to the Somaliland Demographic and Health Survey (SLDHS) conducted in 2020, the overall prevalence of stunting among children aged 6–59 months is 21.0%. However, there is limited research on this topic. This study aims to assess the prevalence of stunting among children aged 12–59 months in Somaliland, with a particular focus on families residing in internally displaced persons (IDP) camps within the country. The Somaliland government has developed a policy framework for IDPs, aiming to improve living conditions and provide durable solutions.13,14
Major risk factors contributing to stunting include poor maternal health, lack of access to antenatal care facilities, inadequate feeding and care practices, insufficient infrastructure, and healthcare facilities. Economic wealth and parental education also play vital roles in undernutrition, increasing the likelihood of stunting among primary school students.15,16 Recognizing the broader socio-political context is also essential, as the prevalence of stunting reflects not just nutritional challenges but also the compounding impact of displacement-related factors, emphasizing the critical need for political stability, social support, and comprehensive policy interventions to improve the overall well-being of children in such settings.
Sub-Saharan Africa continues to face significant challenges related to malnutrition. In 2015, the region accounted for over 30% of global underweight children. Despite a global decline in childhood stunting, the African region witnessed an increase from 50.3 million to 58.8 million stunted children in 2018. Notably, Africa’s prevalence of wasting among children under five, at 7.1%, is slightly lower than the global rate of 7.3%. However, the region experiences higher rates of stunting (22.7%) and wasting (9.4%) compared to the global averages. These findings underscore the complex and varied nature of malnutrition in SSA.17,18
Since 2015, the UNHCR (UN Refugee Agency) has estimated that there are 71,753 internally displaced persons (IDPs) in Hargeisa, Somaliland, due to a protracted 20-year civil war.19 However, the nutritional status of children residing in IDP camps has not been adequately monitored. Therefore, this study aims to determine the level of stunting and its determinants among children aged 12–59 months in IDP camps in Hargeisa city.
Materials and Methods
Study Area and Period
The study was conducted in Hargeisa, the capital city of Somaliland, from May 05 to July 30th, 2022, Hargeisa. Somaliland is an unrecognized self-declared sovereign state that is not internationally recognized. It shares borders with Djibouti in the northwest, Ethiopia to the south and west, the Gulf of Aden to the north, and Somalia to the east. Hargeisa, with a population of 1.3 million individuals, has a significant proportion of internally displaced persons (IDPs) camps, accounting for 5.5% of the population. The study focused on eight main districts within Hargeisa, each with its own local administration. The study area is located at latitude 9° 33ʹ 44.4″ N and longitude 44° 10ʹ 37.2″ E, at an altitude of 1334 meters (4377 feet) above sea level. The climate of the region is characterized as semi-arid. The IDP camps, which were included as sub-study areas, are situated in various locations within the city.20
Study Design and Respondents
A community-based cross-sectional study design was employed to assess the nutritional status among children aged 12 to 59 months living in Internally Displaced Persons (IDP) camps in Hargeisa. Children aged 12 to 59 months were the source of the population, including all children within the specified age range residing in the IDP camps, and their parents or caretakers were the respondents. Mothers or caregivers who had hearing difficulties, children with physical deformities, and women or caregivers who had been living in the IDP camps for less than six months were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size for this study was determined using the single population proportion formula based on the following assumptions: a prevalence (P) of 21.0% of children under the age of five being stunted (below −2 standard deviations) from the 2020 Somaliland Demographic and Health Survey (SLDHS).13 A 95% confidence interval (CI) represented by 1.96, and a margin of error of 5%. After adjusting for a 5% contingency and a design effect of 1.5, the final sample size was calculated to be 402 children aged 12 to 59 months residing in Hargeisa IDP camps.
To select the IDP settlements, a proportional listing approach was used. Three IDP settlements were randomly chosen using a simple random sampling method. Within each selected settlement, all households with children aged 12 to 59 months and residing for at least six months were considered as the study population. Systematic random sampling was employed to select households, with an interval (k) of 21. This means that the first household was selected through a lottery method, and subsequent households were chosen at every 21st interval. The three selected IDP settlements were Ayaha, Nasa-hablod, and Cakara.
Data Collection Procedure and Tools
The study data was collected by trained data collectors, through mobile data collection which is Kobo collect. Three enumerators with bachelor’s degrees who received a full day of data collection training. The study focused on two parameters: age and height. Age information was obtained from the caregivers/parents of the children. Anthropometric data, specifically height, was collected by the trained enumerators.
For children aged 12 to 59 months, height was measured without shoes (barefoot) using the UNICEF height board. A stand-height scale calibrated and checked for safety was used to take the measurements. Children aged 24 months and above had their height measured using a vertical height board. The child was positioned in the middle of the board, standing upright, with their head, shoulders, buttocks, knees, and heels touching the board. This protocol ensured accurate measurements were taken.
The collected data was entered into an Excel worksheet and later exported to the WHO AnthroPlus software. The software was used to generate Height-for-Age Z-scores and other anthropometric indicators used to evaluate stunting among the children in the study.
Data Analysis and Quality Assurance
The data was entered and analyzed using the Statistical Package for the Social Sciences (SPSS) software, specifically IBM Version 25.0. Principle component analysis (PCA) was employed to generate wealth status of study participants. Twelve variables related to the ownership of selected household assets, the size and the quantity of durable equipment, materials used for housing construction, home ownership, improved water, and sanitation facilities were considered. Eventually, the generated principal component was divided into three equal quintiles (Poor, Middle, and Rich). To ensure data completeness, a cross-checking process was implemented. The study utilized a structured questionnaire that was adapted from various literature sources.21,22 The questionnaire was initially prepared in English and then translated into the local language which is Somali.
To validate the questionnaire and ensure its effectiveness, a pretest was conducted with 5% of the study participants who shared similar characteristics with the IDP settlements. Descriptive statistics were used to calculate frequencies and percentages for categorical data. Bivariate logistic regression analysis was performed to examine the association between the dependent and independent variables. Variables with a p-value of < 0.2 in the bivariate analysis were considered as candidate variables for the subsequent multivariate logistic regression analysis, which aimed to control for confounding factors.
The multivariate logistic regression analysis was conducted to determine the relationship between the independent variables and the outcome variable. Furthermore, the Hosmer-Lemeshow goodness of fit was used to assess model suitability, with a cut-off point of a p-value <0.05 considered significantly associated with the outcome. Adjusted odds ratios (aOR) were calculated, along with a 95% confidence interval (CI), to measure the strength of the associations.
Ethical Considerations
In conducting this study, ethical approval was secured from the Jimma University Institutional Review Board [IRB] of the College of Health Sciences under the reference number IHIRB/586/2022. Prior to data collection, the participants/caretakers were provided with information about the purpose of the study and their right to refuse participation or withdraw from the interview at any time. Verbal consent, duly accepted and approved by the ethics committee, was obtained from each participant before the interview, ensuring their willingness to participate. The participants assured that the information they provided would be treated confidentially throughout the study. To maintain confidentiality, no identification information, including the names of the participants, was recorded on the questionnaire. Respecting the principles of ethics, the study followed the principles outlined in the Declaration of Helsinki, underscoring our commitment to ethical practices in human research. In addressing the local context, permission was obtained from relevant Somaliland authorities to conduct this study. This underscores our commitment to respecting the autonomy and rights of individuals involved in the study while aligning with ethical committee-approved procedures.
Results
Socio-Demographic Characteristics of Study Respondents
The study included a total of 402 children under the age of five. However, 3.2% of children with a HAZ index that was flagged and were excluded from the study, leaving 389 children for the final analysis. The mean age of the children was 24.6 months with a standard deviation of 11.37. In terms of gender distribution, slightly over half (58.4%) of the respondents were female. All respondents identified themselves as followers of the Muslim religion. Most of the participants (86.1%) were married, and a significant proportion (86.4%) had no formal education. Additionally, the majority (95.9%) of the respondents were Somali regarding their ethnicities (see Table 1).
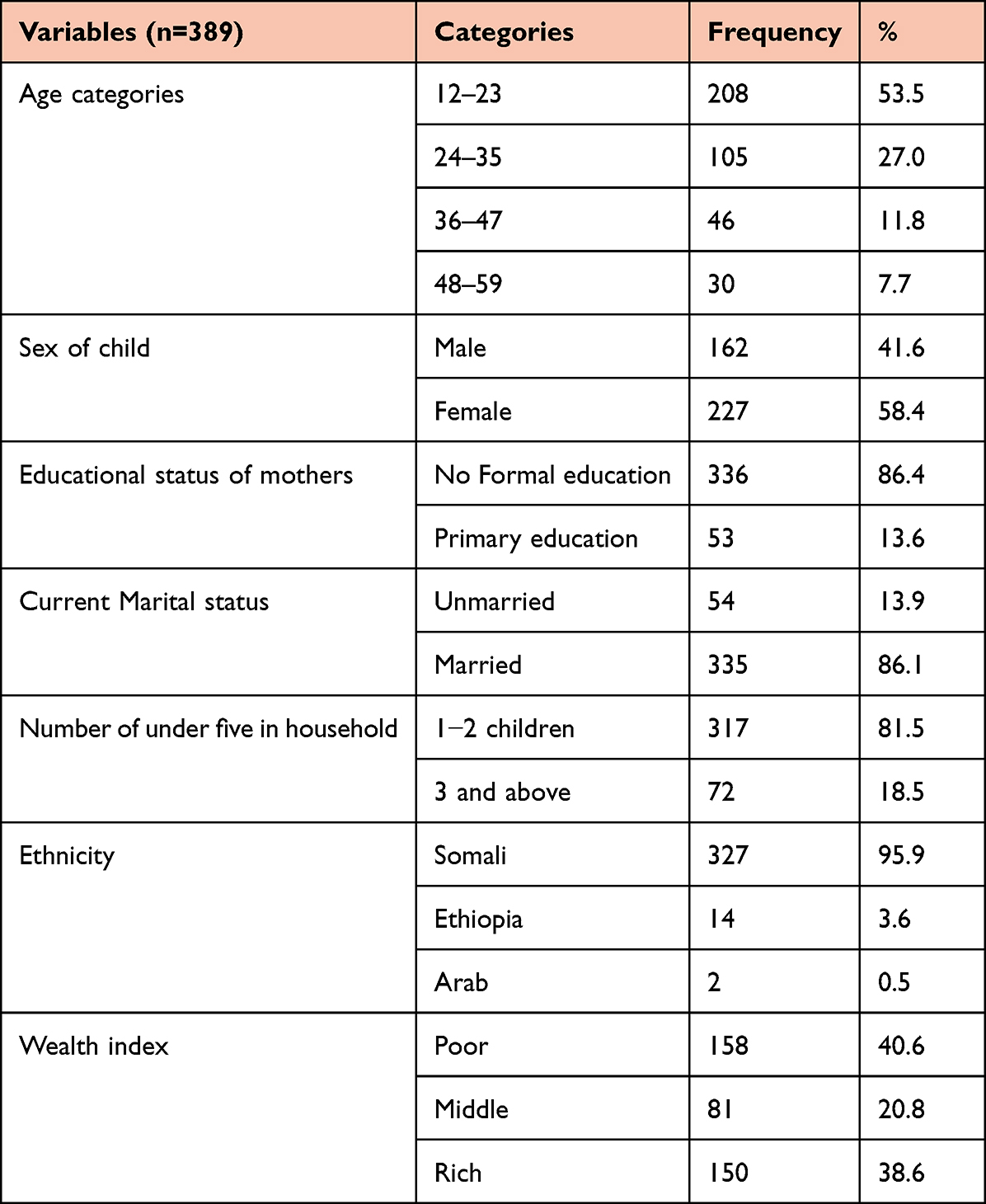 |
Table 1 Socio Demographic Characteristics of the Respondents in an IDP Settings, Hargeisa, Somaliland, 2022 (n=389) |
Prevalence of Stunting
The overall prevalence of stunting among children under five in the IDP setting was 21.1% [95% CI: 17.0–24.9%]. The highest proportion of stunting (57.3%) was observed among females.
Childcaring and Child Characteristics
Out of the study respondents, approximately 170 (43.7%) reported feeding their children three times a day. Regarding vaccination status, 190 (48.8%) of the children were fully vaccinated, while 199 (51.2%) were either partially vaccinated or not vaccinated at all. In terms of delivery method, nearly two-thirds (63.8%) of the study subjects had home deliveries. Additionally, the majority (73.5%) of the children under study were primarily cared for by their mothers. Bottle feeding was reported by almost half (47.6%) of the subjects. Moreover, more than half (57.8%) of the caregivers used deworming tablets for their children. Approximately two-thirds (66.3%) of the mothers in the study sought healthcare for their children when they fell ill. Lastly, one-third of the children experienced measles in the past year (see Table 2).
 |
Table 2 Child Caring and Child Characteristics Among IDP Settings, Hargeisa, Somaliland, 2022 (n=389) |
Maternal Related Characteristics
Among the caregivers under study, nearly two-thirds (65.0%) visited antenatal follow-up during pregnancy fewer than four times. Moreover, more than two-thirds (82.1%) of the mothers had given birth to fewer than six children in their lifetime. The majority of caregivers (76.9%) demonstrated knowledge of family planning, with a significant proportion (67.4%) utilizing natural family planning methods. In terms of hand hygiene practices, out of the study respondents, only 36 (9%) reported using water alone, while more than two-thirds (70.1%) reported using soap occasionally to clean their hands before feeding their children (see Table 3).
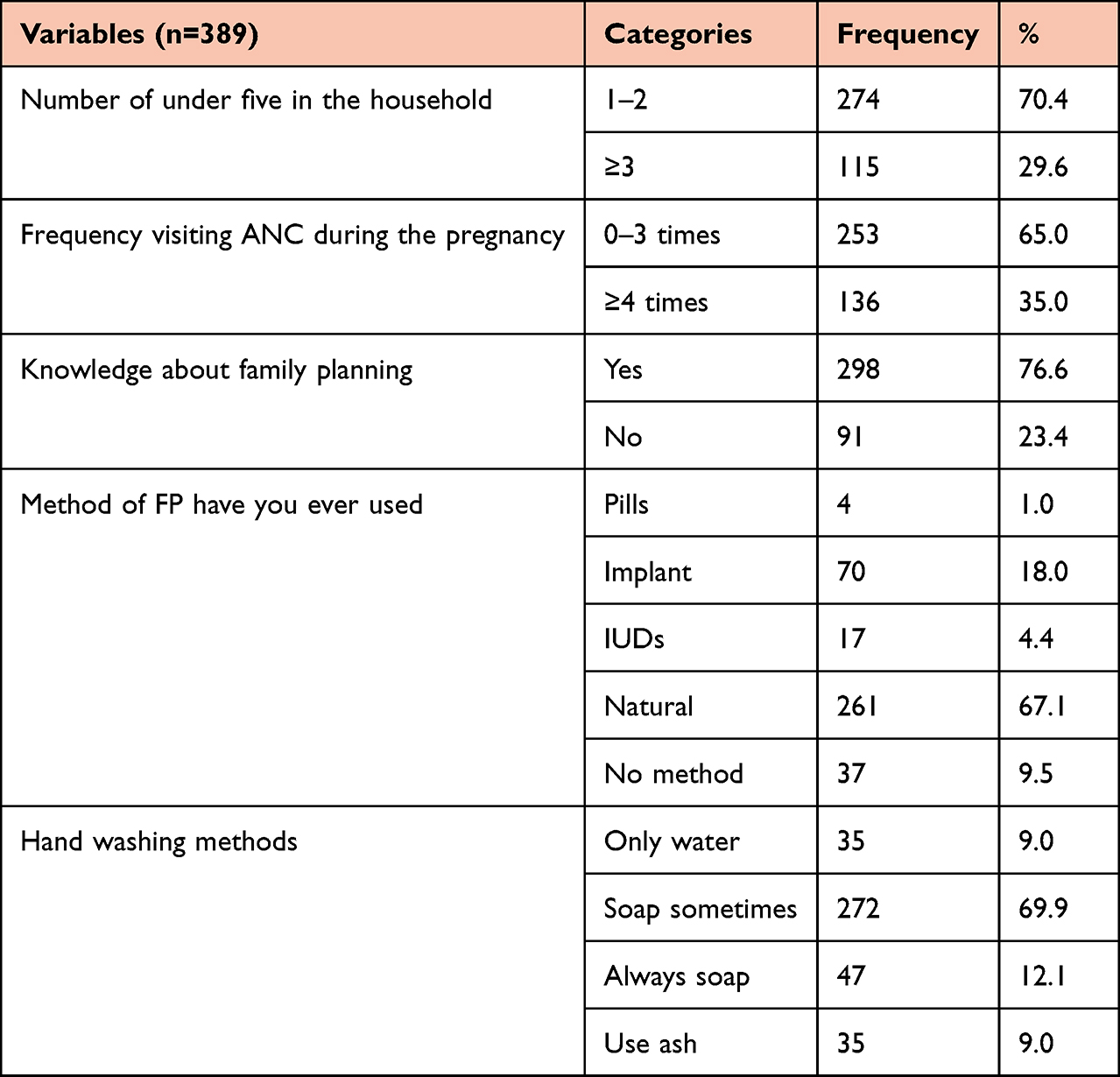 |
Table 3 Maternal Related Characteristics Among IDP Settings, Hargeisa, Somaliland, 2022 (n=389) |
Factors Associated Stunting Among Children in IDP Settings, Hargeisa, Somaliland, 2022 (n=389)
The bivariate and multivariable logistic regression analyses revealed significant associations between various factors and the stunting status of under-five children in an IDP setting (see Table 4). The vaccination status, deworming practice, place of child delivery, child’s experience of measles, and maternal consumption of extra food during lactation were found to be significantly associated with stunting. Children who were fully vaccinated had a significantly lower likelihood of stunting compared to those who were not fully vaccinated (aOR= 0.19, 95% CI: 0.09–0.34, p<0.001), with an 81% reduction in the odds of stunting. Caregivers who did not practice deworming for their children were found to be 6 times more likely to have stunted children compared to their counterparts (aOR= 6.5, 95% CI: 2.9–14.5, p<0.001). Children born in health facilities had a significantly lower likelihood of stunting, with an 86% reduction in odds compared to those born outside health facilities (aOR= 0.14, 95% CI: 0.07–0.3, p<0.001). Similarly, children who did not experience measles in the last year were 88% less likely to be stunted compared to those who did experience measles (aOR= 0.12, 95% CI: 0.04–0.3, p<0.001). Mothers who visited antenatal care services showed a preventive effect towards stunting, with a 67% reduction in odds compared to mothers who did not visit ANC services (aOR= 0.33, 95% CI: 0.14–0.81, p=0.015). Mothers or caregivers who did not consume extra food during lactation were found to have a 2-fold increased likelihood of having stunted children compared to those who consumed extra food during lactation (aOR= 2.15, 95% CI: 1.11–4.15, p=0.02).
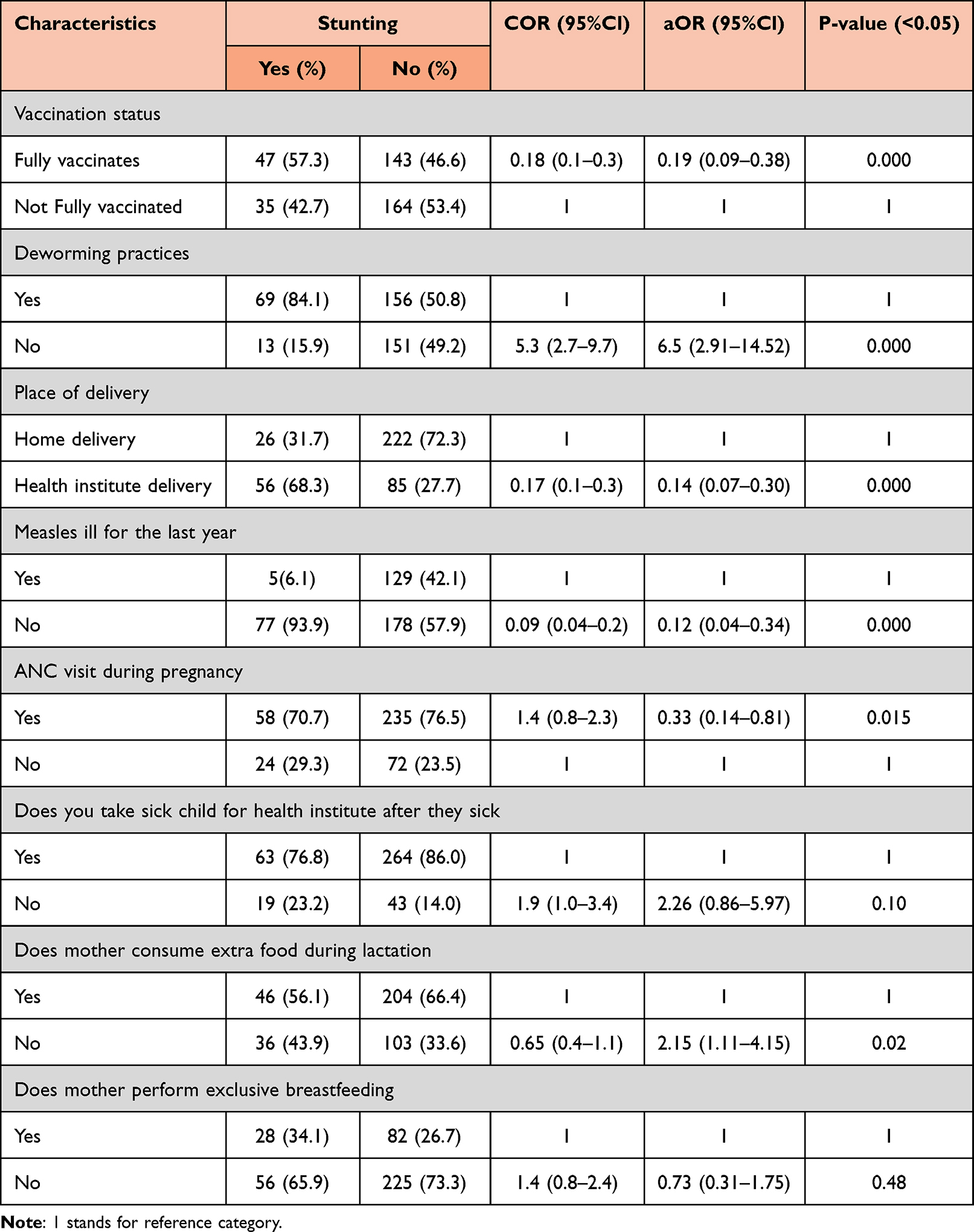 |
Table 4 Factors Associated with Stunting Among Under Five Children in IDP Settings, Hargeisa, Somaliland, 2022 (n=389) |
Discussion
The aim of this study was to determine the prevalence of stunting and its associated factors among under-five children living in IDPs in Hargeisa, Somaliland. The study was specifically conducted in three IDP camps, revealing a stunting prevalence of 21.1% [95% CI: 19.7–28.1%]. This figure indicates a slightly higher prevalence compared to the Somaliland Health and Demographic Survey, which reported a prevalence of 20.0%.13 Other studies conducted in Sub-Saharan Africa and Northwest regions have shown varying prevalence’s of stunting among under-five children. For instance, the prevalence in the Somali regional state of Ethiopia was 33.4%, while in IDP settings in Uganda, it was 52.4%.23,24 Similarly, studies in Pakistan and India reported prevalence rates of 48.2% and 33.8%, respectively.25,26,27 Studies conducted in IDP camps in Myanmar for assessing stunting revealed a prevalence of 59.4%, while in IDP camps in Somalia for measuring the prevalence of stunting was 66.0%.28,29 and the prevalence of stunting among IDP children in Uganda was found to be 52.4%.24,30 The differences in these prevalence rates could be attributed to variations in the study populations. This study assessed children at different stages of under-five age, whereas other studies focused on specific age groups or targeted under-five children in different contexts. Additionally, socioeconomic and cultural differences in dietary habits and care practices among children may also contribute to the variation.
Our findings indicate that mothers who did not consume surplus food during lactation, caregivers whose children were partially or not vaccinated, mothers who delivered outside of health facilities, and children under five who had experienced measles were more likely to have shorter stature. These factors emerged as major determinants of stunting among under-five children in this study. Despite showing no association between family income/wealth status and the child’s stunting, low family income may have an indirect association with the nutritional status of children by influencing the low quality and less diversity of a child’s diet and the low ability to access food.29,31,32 Our study also illustrated that the majority of mothers were illiterate and has no formal education (86.4%), which is consistent with previous studies.29,33 This may be because a mother’s ability of childcare and education level is associated with undernutrition. A mother’s education and approach to information can be essential determining factors in a child’s growth development.34,35 Education might improve mother’s self-rule, thereby increasing her ability to make decisions about her own health.
Studies conducted in various contexts have yielded diverse findings regarding the determinants of stunting among under-five children in IDP camps. Common factors associated with undernutrition and stunting in this demographic include delayed introduction of complementary foods, lack of caregiver knowledge, and food insecurity. For instance, a study in Uganda identified risks such as male children being prone to stunting (aOR = 1.57, 95% CI: 1.15–2.13, p-value=0.004), children aged 3–24 months being at risk of acute malnutrition (aOR = 2.78, 95% CI: 1.26–6.15, p-value=0.012), and de-worming offering protective effects (aOR 0.44, 95% CI: 0.22–0.88, p-value=0.018).24 In northern Ethiopia, being female and the absence of washing facilities and latrines were associated with stunting among under-five children.26 Similarly, in southern Ethiopia, factors such as polygamous marriages of fathers, female sex, fewer meal frequencies, lack of vaccination, poor household wealth status, and severe household food insecurity were significantly associated with stunting among under-five children.28
This study, unique in its focus on IDP children below five years of age, differs from research in other African regions. It identifies factors associated with stunting among IDP children, including vaccination status ((aOR = 0.19, 95% CI: 0.09–0.38), measles experience in the last year (aOR = 0.12, 95% CI: 0.04–0.34) deworming practice (aOR = 6.5, 95% CI: 2.91–14.52), place of delivery (aOR = 0.14, 95% CI: 0.07–0.30), ANC visits (aOR = 0.33, 95% CI: 0.14–0.81), and caregivers/mothers’ consumption of extra foods during lactation (aOR = 2.15, 95% CI: 1.11–4.15). These factors present unique challenges in the IDP context and emphasize the need for tailored interventions to address the specific determinants of stunting in this population.
Limitations of the Study
The limitations of this study encompass several aspects. Firstly, the cross-sectional nature of the study design impedes the ability to establish a temporal relationship between cause and outcome. As a result, causal inferences and the direction of causality cannot be definitively determined.
Furthermore, the study is susceptible to potential recall bias among participants, particularly when answering questions related to events such as fever and diarrhea in the child’s past history. The accuracy of reported information may be influenced by memory limitations or variations in individual recall.
Additionally, the overrepresentation of female children is an outcome of systematic random sampling, wherein caregivers are selected rather than directly controlling the sex of the child. The determination of the child’s sex relies on information provided by caregivers during interviews, and unfortunately, it cannot be controlled due to inherent uncertainty in our study design. This may introduce a gender-related bias that should be considered when interpreting the study findings.
Conclusion
This study underscores a notable prevalence of stunting among under-five children in IDP camps, surpassing the standard range of 10–15%. A significant proportion of the study participants lacked full vaccination, emphasizing the imperative for enhanced adherence to vaccination practices in IDP settings to reduce the risk of stunting. Notably, children born at health facilities exhibited a preventive effect against stunting, suggesting that mothers receiving post-natal sessions, immunization, and health education can potentially mitigate the impact of home delivery. Conversely, the research identified an elevated risk of stunting among children in IDP settlements who did not receive deworming treatment, indicating a high susceptibility to future stunting. Advocating for caregivers to prioritize deworming for children with a history of worm infestations is crucial. Additionally, mothers or caregivers utilizing extra food demonstrated a lower risk of their children experiencing hunger, as revealed in this study.
To translate these findings into actionable measures, it is imperative to promote comprehensive vaccination coverage for children under five in IDP settings. Efforts should focus on sensitizing caregivers about the significance of health facility deliveries to reduce the likelihood of childhood stunting. Encouraging mothers to consume extra food during pregnancy is paramount, given its preventive effect on the risk of stunting. Implementing these recommendations is vital for reducing stunting prevalence and enhancing the overall health of children in IDP camps. Targeted interventions addressing vaccination coverage, deworming practices, delivery location, and maternal nutrition should be prioritized. Ongoing research and collaborative efforts are essential to formulate effective strategies and policies addressing stunting in IDP settings comprehensively.
Abbreviations
ANC, Ante-Natal care; BMI, Body mass index; EPI, Extended Program for Immunization; HAZ= Height for Age Z score; HH, Household; IDP, Internally Displaced Persons; MoH, Ministry of Health; NRR, Non-Response Rate; PNC, post-Natal care; SLDHS, Somaliland Demographic and Health survey; SLSH, Somaliland Shillings (Somaliland Currency); SDG, Sustainable Development Goals; UNICEF, United Nation Child’s Fund; WHO, World Health Organization.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Our gratitude goes to Jimma University College of Health Sciences for permitting us to conduct this research and to all study respondents and data collectors for their time.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
The authors declare that they have no potential competing interests.
References
1. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. doi:10.1016/S0140-6736(13)60937-X
2. Vishwakarma B, David A. Underlying risk determinants of acute and moderate malnutrition in children and its preventive management. Pharm Biosci J. 2021;01–11. doi:10.20510/10.20510/pbj/9/i4/1640
3. World Health Organization. Global action plan for the prevention and control of NCDs 2013–2020; 2013. Available from: https://www.who.int/publications/i/item/9789241506236.
4. S P. Prevalence of underweight and its risk factors among under five children in a rural area of Kancheepuram District in Tamil Nadu, India. IOSR J Dental Med Sci. 2013;3(6):71–74. doi:10.9790/0853-0367174
5. Arinaitwe E, Gasasira A, Verret W, et al. The association between malnutrition and the incidence of malaria among young HIV-infected and -uninfected Ugandan children: a prospective study. Malaria J. 2012;11(1). doi:10.1186/1475-2875-11-90
6. Bloss E. Prevalence and predictors of underweight, stunting, and wasting among children aged 5 and under in Western Kenya. J Trop Pediatr. 2004;50(5):260–270. doi:10.1093/tropej/50.5.260
7. Adebisi YA, Ibrahim K, Lucero-Prisno DE, et al. Prevalence and socio-economic impacts of malnutrition among children in Uganda. Nutri Metabol Insights. 2019;12:117863881988739. doi:10.1177/1178638819887398
8. Stewart CP, Iannotti L, Dewey KG, et al. Contextualising complementary feeding in a broader framework for stunting prevention. Matern Child Nutr. 2013;9(S2):27–45. doi:10.1111/mcn.12088
9. Medhin G, Hanlon C, Dewey M, et al. Prevalence and predictors of undernutrition among infants aged six and twelve months in Butajira, Ethiopia: the P-MaMiE birth cohort. BMC Public Health. 2010;10(1):1–15. doi:10.1186/1471-2458-10-27
10. Kraemer K, Cordaro JB, Fanzo J, et al. Nutrition-Specific and Nutrition-Sensitive Interventions, in Good Nutrition: Perspectives for the 21st Century. Karger Publishers; 2016:276–288.
11. Obeid O. Malnutrition in adolescents and children: the hidden deficiencies. Am Acad Pediatr. 2012;103:516–520.
12. Rathod N, Warbhe P. Assessment of nutritional status of street children in selected wards of an urban area. J Interdiscip Multidiscip Stud. 2014;1(8):136–143.
13. The Government of Somaliland. Somaliland Health and Demographic Survey. UNFPA; 2020. Available from: https://somalia.unfpa.org/sites/default/files/pub-pdf/slhds2020_report_2020.pdf.
14. Somaliland NDRA. Adopting and implementing Somaliland’s draft policy framework. on internal displacement; 2015. Available from: https://www.internal-displacement.org/publications/adopting-and-implementing-somalilands-draft-policy-framework-on-internal-displacement.
15. Headey D, Hoddinott J, Ali D, Tesfaye R, Dereje M. The other Asian enigma: explaining the rapid reduction of undernutrition in Bangladesh. World Dev. 2015;66:749–761. doi:10.1016/j.worlddev.2014.09.022
16. Mushtaq MU, Gull S, Khurshid U, Shahid U, Shad MA, Siddiqui AM. Prevalence and socio-demographic correlates of stunting and thinness among Pakistani primary school children. BMC Public Health. 2011;11(1):1.
17. Obasohan PE, Walters SJ, Jacques R, Khatab K. Risk factors associated with malnutrition among children under-five years in Sub-Saharan African countries: a scoping review. Int J Environ Res Public Health. 2020;17(23):8782. doi:10.3390/ijerph17238782
18. Doctor HV, Nkhana-Salimu S. Trends and determinants of child growth indicators in Malawi and implications for the sustainable development goals. AIMS Public Health. 2017;4(6):590–614.
19. UNHCR. Internal displacement profiling in Hargeisa; 2015. Available from: https://www.jips.org/uploads/2018/10/Profiling-Report-Somalia-Hargeisa-2015.pdf.
20. Hersi L, Tesfay K, Gesesew H, Krahl W, Ereg D, Tesfaye M. Mental distress and associated factors among undergraduate students at the University of Hargeisa, Somaliland: a cross-sectional study. Int J Ment Health Syst. 2017;11(1). doi:10.1186/s13033-017-0146-2
21. Engidaw MT, Gebremariam AD. Prevalence and associated factors of stunting and thinness among adolescent Somalian refugee girls living in eastern Somali refugee camps, Somali regional state, Southeast Ethiopia. Confl Health. 2019;13(1). doi:10.1186/s13031-019-0203-3
22. Geletaw A, Egata G, Weldegebreal F, Kibr G, Semaw M, Valdés-Ramos R. Nutritional status and associated factors among primary school children from pastoral communities, Mieso-Mulu District, Sitti Zone, Somali Regional State, Eastern Ethiopia: institution-based cross-sectional study. Valdés-Ramos R, editor. J Nutr Metab. 2021;2021:1–12. doi:10.1155/2021/6630620
23. Ma’alin A, Birhanu D, Melaku S, Tolossa D, Mohammed Y, Gebremicheal K. Magnitude and factors associated with malnutrition in children 6–59 months of age in Shinille Woreda, Ethiopian Somali regional state: a cross-sectional study. BMC Nutr. 2016;2(1). doi:10.1186/s40795-016-0079-1
24. Habaasa G. An investigation on factors associated with malnutrition among underfive children in Nakaseke and Nakasongola districts, Uganda. BMC Pediatric. 2015;15(1). doi:10.1186/s12887-015-0448-y
25. Khan GN, Turab A, Khan MI, et al. Prevalence and associated factors of malnutrition among children under-five years in Sindh, Pakistan: a cross-sectional study. BMC Nutr. 2016;2(1). doi:10.1186/s40795-016-0112-4
26. Savanur MS, Ghugre PS. Magnitude of undernutrition in children aged 2 to 4 years using CIAF and conventional indices in the slums of Mumbai city. J Health Popul Nutr. 2015;33(1). doi:10.1186/s41043-015-0017-x
27. Abdullah AA, Rifat MA, Hasan MT, Manir MZ, Khan MM, Azad F. Infant and young child feeding (IYCF) practices, household food security and nutritional status of under-five children in Cox’s Bazar, Bangladesh. Curr Res Nutr Food Sci. 2018;6:789–797. doi:10.12944/CRNFSJ.6.3.21
28. Hein AK, Hong SA, Puckpinyo A, Tejativaddhana P. Dietary diversity, social support and stunting among children aged 6–59 months in an internally displaced persons camp in Kayin State, Myanmar. Clin Nutr Res. 2019;8(4):307. doi:10.7762/cnr.2019.8.4.307
29. Sheikh Mohamed Omer A, Mohamud Yusuf A, Yusuf Mahdi A, Abdikarim Daud F. Prevalence and factors associated with malnutrition among children aged 6–59 months in Badbaado Camp in Mogadishu Somalia. Cent Afr J Public Health. 2020;6(3):136. doi:10.11648/j.cajph.20200603.15
30. Wamani H, Tylleskär T, Astrøm AN, Tumwine JK, Peterson S. Mothers’ education but not fathers’ education, household assets or land ownership is the best predictor of child health inequalities in rural Uganda. Int J Equity Health. 2004;3:9. doi:10.1186/1475-9276-3-9
31. Kibr G, Yazew T. Factors associated with stunting among children aged 24–59 months in food secure and insecure households of Kuyu District, Northern Oromia, Ethiopia: a Comparative Cross-Sectional Study. SSRN Electron J. 2021. doi:10.2139/ssrn.3816768
32. Chaparro C, Oot L, Sethuraman K. Overview of the nutrition situation in seven countries in Southeast Asia; 2014. Available from: https://www.fantaproject.org/sites/default/files/download/Southeast-Asia-Nutrition-Overview-Apr2014.pdf.
33. Shine S, Tadesse F, Shiferaw Z, Mideksa L, Seifu W. Prevalence and associated factors of stunting among 6–59 months children in pastoral community of Korahay Zone, Somali Regional State, Ethiopia 2016. J Nutr Disord Ther. 2017;07(01). doi:10.4172/2161-0509.1000208
34. Kinyoki DK, Berkley JA, Moloney GM, Kandala NB, Noor AM. Predictors of the risk of malnutrition among children under the age of 5 years in Somalia. Public Health Nutr. 2015;18(17):3125–3133. doi:10.1017/S1368980015001913
35. Gebru TT, Tesfamichael YA, Bitow MT, et al. Stunting and associated factors among under-five children in Wukro town, Tigray region, Ethiopia: a cross sectional study. BMC Res Notes. 2019;12(1). doi:10.1186/s13104-019-4535-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.