")
Back to Journals » Journal of Healthcare Leadership » Volume 16
Predictors of Leadership Competencies Among Nurse Executives in the Kingdom of Saudi Arabia
Authors Alshamlani YA, Alanazi NH, Alhamidi SA , Alanazi RA, Alenezi A , Adalin NM, Alyousef SM, Tumala RB
Received 14 November 2023
Accepted for publication 20 February 2024
Published 29 February 2024 Volume 2024:16 Pages 105—119
DOI https://doi.org/10.2147/JHL.S444890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Russell Taichman
Yousef A Alshamlani,1,* Naif H Alanazi,2,* Sami A Alhamidi,2,* Raeed A Alanazi,2,* Atallah Alenezi,3,* Norisk M Adalin,1,* Seham M Alyousef,2,* Regie B Tumala2,*
1Nursing Department, King Saud University Medical City, Diriyah, Riyadh, Kingdom of Saudi Arabia; 2College of Nursing, King Saud University, Diriyah, Riyadh, Kingdom of Saudi Arabia; 3Nursing Department, College of Applied Medical Sciences, Shaqra University, Shaqra, Kingdom of Saudi Arabia
*These authors contributed equally to this work
Correspondence: Regie B Tumala, College of Nursing, King Saud University, Diriyah, Riyadh, 11421, Kingdom of Saudi Arabia, Tel +966554773976, Email [email protected]
Background: Awareness and development of nurse executives’ leadership competencies has been considered a key strategy for the success of healthcare organizations. However, only a few studies about nurse executives’ leadership competencies are available in the literature, and no study has been conducted about the topic within Saudi Arabian context. The aim of this study was to assess the leadership competencies of nurse executives and the predictors of these competencies.
Methods: This quantitative study used a descriptive, cross-sectional, and correlational design. The study recruited a total convenience sample of 136 nurse executives who voluntarily consented to participate. The respondents self-rated the online survey, “Leadership Competency Assessment Tool: Self-Assessment.” Data collection was conducted between September 2022 and November 2022. Test of correlation and multiple regression analyses were conducted.
Results: The overall mean score of nurse executives’ leadership competencies was 3.38 out of 5.0, which was below the level of having excellent leadership competencies. Four dimensions had mean scores below the level of having excellent leadership competencies, namely, communication and relationship building (3.48), knowledge of the healthcare environment (3.29), leadership (3.45), and business skills (3.15), while nurse executives had excellent leadership competencies only in the professionalism dimension (3.51). Age (p=0.04), highest educational attainment (p=0.01), current role (p< 0.01) and length of experience (p=0.02) as nurse executive, monthly salary (p=0.03), nationality (p=0.04), and having seminars/trainings in leadership and management (p=0.01) were considered predictors of the leadership competencies of nurse executives.
Conclusion: Nurse executives reported a low level of leadership competencies, thus implying necessary actions for improvement. There were personal factors that influenced the level of nurse executives’ leadership competencies. To achieve quality outcomes and maintain a high level of nursing care in hospital organizations, these findings must be considered in planning strategies related to the improvement of the leadership competencies of nurse executives.
Keywords: assessment, leadership competencies, nurse executives, predictors, Saudi Arabia
Introduction
Healthcare organizations have undergone vital developments due to the high demands for less institutionalized patient care, the growing complexity of patients, increasing number of patients with chronic diseases, and the stronger focus on person‐centered care.1 These developments require well-prepared and educated registered nurses who have master’s and doctorate degrees (ie, DNP, DNS, EdD, and PhD) in nursing, working as members in multidisciplinary healthcare teams, and having the required leadership competencies at all levels in their respective healthcare organizations.1,2 Having these leadership competencies constitutes the body of knowledge needed for nurse executives.2–4
In 2005, the American Organization of Nurse Executives (AONE) released the AONE Nurse Executive Competencies (AONE-NEC),5 which has been utilized in academic institutions, healthcare systems, and hospital institutions throughout the United States of America (USA) and other countries across the globe for almost two decades.4,6 The AONE-NEC includes five dimensions: (1) communication and relationship building with eight competencies, (2) knowledge of the healthcare environment with eleven competencies, (3) leadership with five competencies, (4) professionalism with six competencies, and (5) business skills with five competencies.5 The AONE-NEC self-assessment instrument features a 5-point Likert scale using Benner’s Novice to Expert responses, including the following: 1 = novice, 2 = advanced beginner, 3 = competent, 4 = proficient, and 5 = expert.5 In 2019, the AONE changed its name to the American Organization for Nursing Leadership (AONL) and has since positioned itself as an expert organization providing standards for nursing leaders and the management tools they need to excel in their practice and education as nurse executives. In addition, Warshawsky et al7 highlighted the capacity of nurse executives to develop advanced competencies in leadership and management as a key strategy for achieving success in healthcare organizations.
Although most nursing leaders are educationally prepared for their leadership roles, many of them who interact most with patients, families, physicians and nursing staff are less prepared for their leadership roles.8 Moreover, evidence from the literature suggests that registered nurses in leadership and managerial positions, such as those working as nurse specialty managers, nursing directors, and chief nursing officers, are not adequately equipped with the leadership and management competencies required for their roles.9–13 In particular, while there were efforts to identify a set of standard competencies for informatics as a core element of every nurse executive or managers’ set of capabilities, these were not disseminated widely, and gaps in their informatics knowledge and skills were recognized.12,13 At the same time, many authors have reported that nurse leaders are not equipped with the essential informatics competencies,12,13 have low levels of financial literacy,9 lack strategic vision and competencies,11 and are less confident of their leadership roles.10
Previous literature reviews have identified the essential factors and characteristics of nurse executives and argued for the necessity of improving knowledge about their leadership competencies.14–16 In the Kingdom of Saudi Arabia (KSA), a qualitative study was participated by 35 ward staff nurses regarding the nature of leadership styles utilized by the nursing management team in their hospitals.17 One of the suggestions shared by the participants to address ineffectual leadership styles was particularly concerning nurse executives (chief nursing officers) in establishing and maintaining open communication channels.17 This implied that the participants were dissatisfied by the nurse executives’ closed-door policy to discuss their issues directly.17 While various studies have explored the leadership competencies of nurse executives worldwide,6,8–13 to the best of our knowledge, this is the first study to explore about the topic in KSA. The assessment of nurse executives’ leadership competencies in KSA is necessary due to the gaps in the literature that must be resolved. In addition, there is a need for nurse executives to acquire leadership certifications, increase their qualifications or educational levels to a minimum of master’s degree or even any doctorate degree in nursing, and strengthen their leadership competencies.10,12,13 Hence, the vital findings of this study on the leadership competencies of nurse executives and the predictors of these competencies would add to the body of knowledge related to nursing leadership and would benefit nursing leaders in the country and other countries worldwide with similar healthcare system.
Aim of the Study
This study aimed to assess the leadership competencies of nurse executives, and the factors predictive of these competencies.
Methods
Research Design
This quantitative study used a descriptive, cross-sectional, and correlational design that utilized an online survey.
Respondents
This study was conducted using a snowballing technique among a total sample of 136 nurse executives who were employed in government and private hospitals across the KSA. The research respondents were eligible to participate if they were a registered nurse having top-level managerial or leadership positions, such as nurse supervisor, clinical service manager, deputy nursing director, nursing director, chief nursing officer, deputy corporate nursing director, and corporate nursing director. Nurse executives who participated in the pilot test, nurse managers or head nurses, staff nurses, nursing aids and healthcare assistants were excluded from participating in the study. For the sample size of this study, the G*Power version 3.1.9.7 software,18 for the sample size computation was used, and a minimum computed sample size of 107 was considered sufficient to yield a medium size effect of 0.15, at a margin of error of 5%, and confidence level of 95%.
Instrument
This study used the “Competency Assessment Tool: Self-Assessment”, which was designed and published by AONL.4 The tool has two parts, in which the first part is about the personal data of the respondents comprising their age, gender, highest educational attainment, current role as nurse executive, type of hospital, length of experience as nurse executive, length of experience as registered nurse, monthly salary, nationality, and attended certifications/seminars/trainings related to leadership/management.
The second part includes five dimensions with a total of 184 items.4 The first domain is about “communication and relationship building” with a subtotal of 48 items in seven sub-dimensions, namely, effective communication with eight items, relationship management with seven items, influencing behaviors with seven items, diversity with four items, community involvement with five items, medical or staff relationships with nine items, and academic relationships with eight items. The second domain is “knowledge of the healthcare environment” with a subtotal of 55 items in eight sub-dimensions, namely, clinical practice knowledge with seven items, delivery models or work design with five items, health care economics and policy with eight items, governance with eight items, evidence-based practice or outcome measurement and research with seven items, patient safety with six items, performance improvement or metrics with eight items, and risk management with six items.
The third domain is “leadership” with a subtotal of 22 items in five sub-dimensions, namely, foundational thinking skills with seven items, personal journey disciplines with one item, systems thinking with six items, succession planning with five items, and change management with three items. The fourth domain is “professionalism” with a subtotal of 20 items in four sub-dimensions, namely, personal and professional accountability with eight items, career planning with five items, ethics with three items, and advocacy with four items. The fifth domain is “business skills” with a subtotal of 39 items in four sub-dimensions, namely, financial management with seven items, human resource management with 17 items, strategic management with eight items, and information management and technology with seven items.
The tool used a 5-point Likert scale using Benner’s Novice to Expert responses, including the following: 1 = novice, 2 = advanced beginner, 3 = competent, 4 = proficient, and 5 = expert.4 Here, higher mean scores mean that the nurse executives are highly competent (ie, proficient or expert) in their management and leadership practices. In this study, mean score cut-off was 3.50, which meant that any score above 3.50 was considered “excellent” (proficient and expert), while a score below 3.50 was marked as “needs improvement” (novice through competent).19 The reliability of the tool was tested with resulting Cronbach’s alphas ranging from 0.77 to 0.90 in all dimensions and sub-dimensions; the overall Cronbach’s alpha was 0.95.
Data Collection
The researchers recruited the respondents through the membership of nurse executives in the Clinical Nursing Advisory Club (CNAC). The CNAC consists of chief nursing officers or corporate nursing directors in the KSA and is hosted by King Saud University Medical City (KSUMC). The online survey was administered to eligible respondents via an invitation and distributed to the CNAC members. The members were asked to send the survey link to other nurse executives who met the inclusion criteria. This included study information being circulated via the CNAC members through their group communication and via targeted email blasts.
The online survey was prepared using Google Docs, and the respondents were instructed to click on the “Agree” button in the survey indicating that they read and understood the study information and voluntarily agreed to participate in this study. The respondents who opened the online survey and did not continue to participate were asked to click on the “Disagree” button and were instructed to leave the page. Completion of the survey constituted consent, and this was clearly noted within the information sent to the CNAC membership. Only the researchers had access to the respondents’ responses. The pilot study was conducted among 10 nurse executives to test the face validity of the online survey from September 15 to 18, 2022. The face validity evaluated the appearance of the online survey in terms of consistency of style, formatting, readability, and respondents’ understanding of the terminologies used in the instrument. The pilot study respondents evaluated the online survey as clear and easy to complete in an average of 45 minutes. Data collection for the main study started on September 22, 2022, and was completed on November 21, 2022.
Ethical Considerations
The researchers obtained ethical approval from the Institutional Review Board (IRB) at KSUMC (Approval Number: E-22-7135). The conduct of the study was guided by the ethical standards set by the IRB at KSUMC and by the official ethical principles for conducting studies among human subjects published by the Declaration of Helsinki. Privacy and confidentiality were maintained throughout the entire research process. Complete research information, including the purpose of the study, the benefits of the study, the potential risks of participation, the respondents’ rights, and the voluntary nature of the participation were provided to the respondents at the beginning of the online survey. There was no incentive for participation. Prior to the commencement of the study, all the respondents were made aware that if they wanted to withdraw from the study at any point, they could do so without any negative effect.
Furthermore, the respondents’ information and responses were kept confidential to ensure the protection of their privacy and identity. In compliance with the data storage guidelines of the IRB at KSUMC, no identifying information was captured by the survey, and private information and responses were kept confidential to ensure the protection of their privacy and identity. At the end of the study, all recorded data were securely stored, and access was restricted to the researchers only. Upon completion of the study, all data were prepared for collation and archiving consistent with the jurisdictional regulations regarding the retention and disposal of research data, as advised by the IRB at KSUMC. The data were presented and reported collectively with no identifying information, and only codes were used in the analysis.
Data Analysis
Data were collected, tallied, and extracted from the online survey, exported from Google Docs, and transferred to IBM SPSS version 23 (Armonk, New York: IBM Corp.) for analysis. Descriptive statistics, such as frequency count, percentages, mean, and standard deviations were identified for the following study variables, including the personal characteristics and leadership competencies of nurse executives. The chi-square test was used to treat the collected data for the relationship of personal characteristics and leadership competencies of nurse executives. Regression analyses were calculated where the personal characteristics of nurse executives were set in the model as predictor variables of their leadership competencies. Significant findings were inferred if p < 0.05.
Results
Personal Profiles of Nurse Executives
One hundred and fifty nurse executives were invited to answer the online survey, 136 complete responses were received (response rate: 92.7%; Table 1). Majority of the nurse executives belonged to the age group of 41–60 years old (60.29%), were females (51.47%), and had post-graduate degrees (master’s and PhD degrees combined, 56.62%). In terms of occupation, most of them worked as nurse specialty managers (77.94%), while others were employed as deputy/chief nursing officers, deputy/chief nursing directors, or deputy or corporate nursing directors (22.06%). Most nurse executives worked in government hospitals (76.47%), while the remaining ones (23.53%) worked in private hospitals across the country.
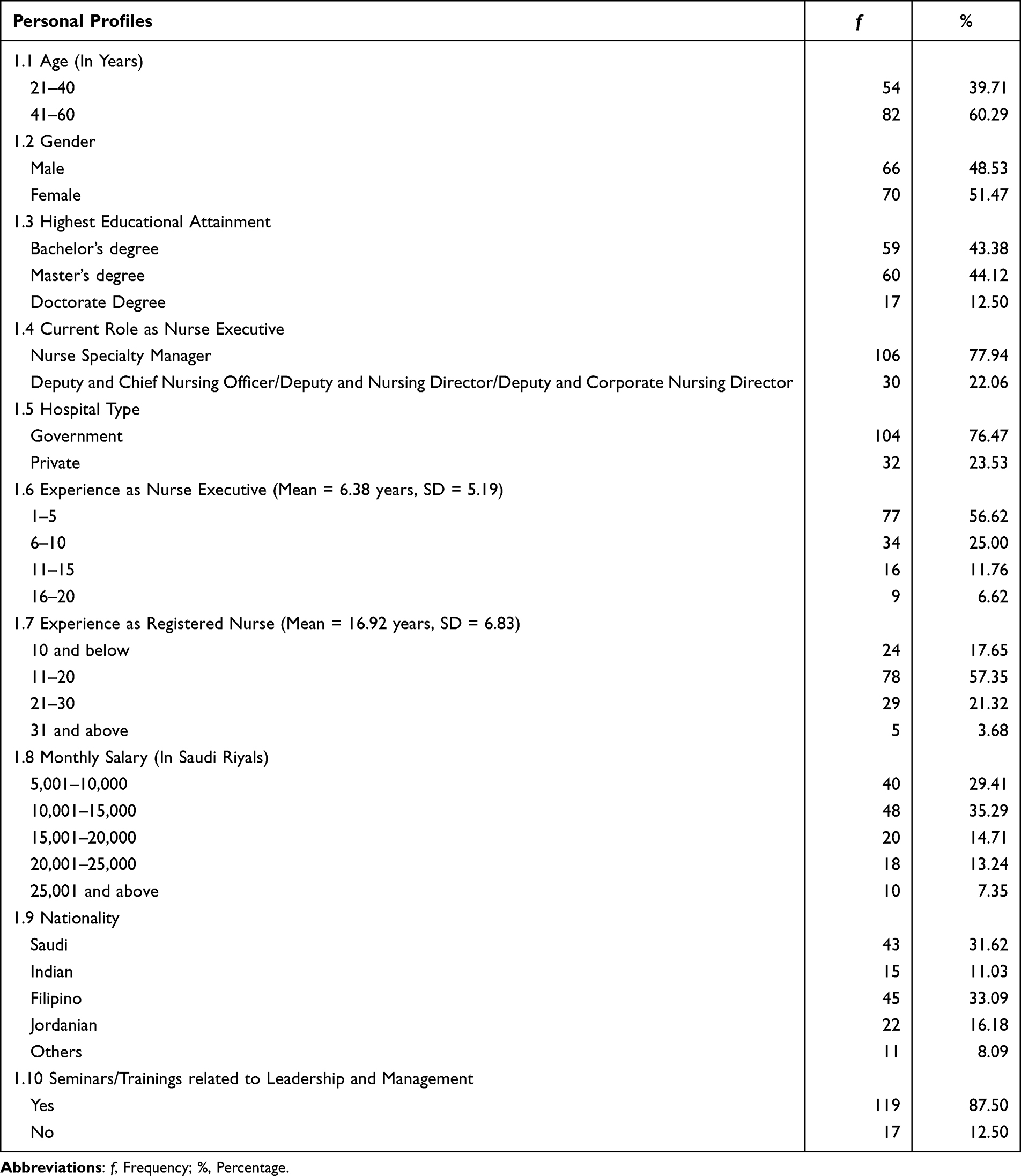 |
Table 1 Personal Profiles of Nurse Executives (n = 136) |
The majority of nurse executives had 1–5 years of experience (56.62%), with the average length of experience at 6.38 years. Meanwhile, for their general experience as registered nurses, the average length was 16.92 years. More than half of the nurse executives worked as registered nurses for 11–20 years, with the highest proportion (35.29%) earning 10,001–15,000 Saudi riyals (2600–4000 US dollars) and the lowest proportion (7.35%) earning 25,001 Saudi riyals (Approximately 6600 US dollars) and above. In terms of nationality, the highest proportion (33.09%) of nurses were Filipinos, followed by Saudis (31.62%), Jordanians (16.18%), Indians (11.03%), and other nationalities (8.09%). Finally, the results showed that most nurse executives (87.50%) had seminars or trainings related to leadership and management, while others (12.50%) did not have any similar trainings.
Leadership Competencies of Nurse Executives
In general, the overall mean score of nurse executives’ leadership competencies (3.38 out of 5.0, SD=1.13) was below the cut-off that indicated not having excellent leadership competencies (See Table 2). Communication and relationship building had an average mean score of 3.48 out of 5.0 (SD=1.04). Its seven sub-dimensions had the following mean scores: effective communication (mean=3.43, SD=1.02), relationship management (Mean=3.66, SD=0.95), influencing behaviors (Mean=3.59, SD=0.98), diversity (Mean=3.66, SD=0.94), community involvement (Mean=3.09, SD=1.12), medical/staff relationships (Mean=3.55, SD=1.08), and academic relationships (Mean=3.35, SD=1.11). The second dimension of the leadership competencies of nurse executives is knowledge of the healthcare environment (Mean=3.29, SD=1.08) with eight sub-dimensions, namely, clinical practice knowledge (Mean=3.58, SD=1.07), delivery models or work design (Mean=3.27, SD=1.09), healthcare economics and policy (Mean=2.91, SD=1.19), governance (Mean=3.03, SD=1.18), evidence-based practice or outcome measurement and research (Mean=3.33, SD=1.14), patient safety (Mean=3.47, SD=1.15), performance improvement or metrics (Mean=3.31, SD=1.13), and risk management (Mean=3.42, SD=1.12).
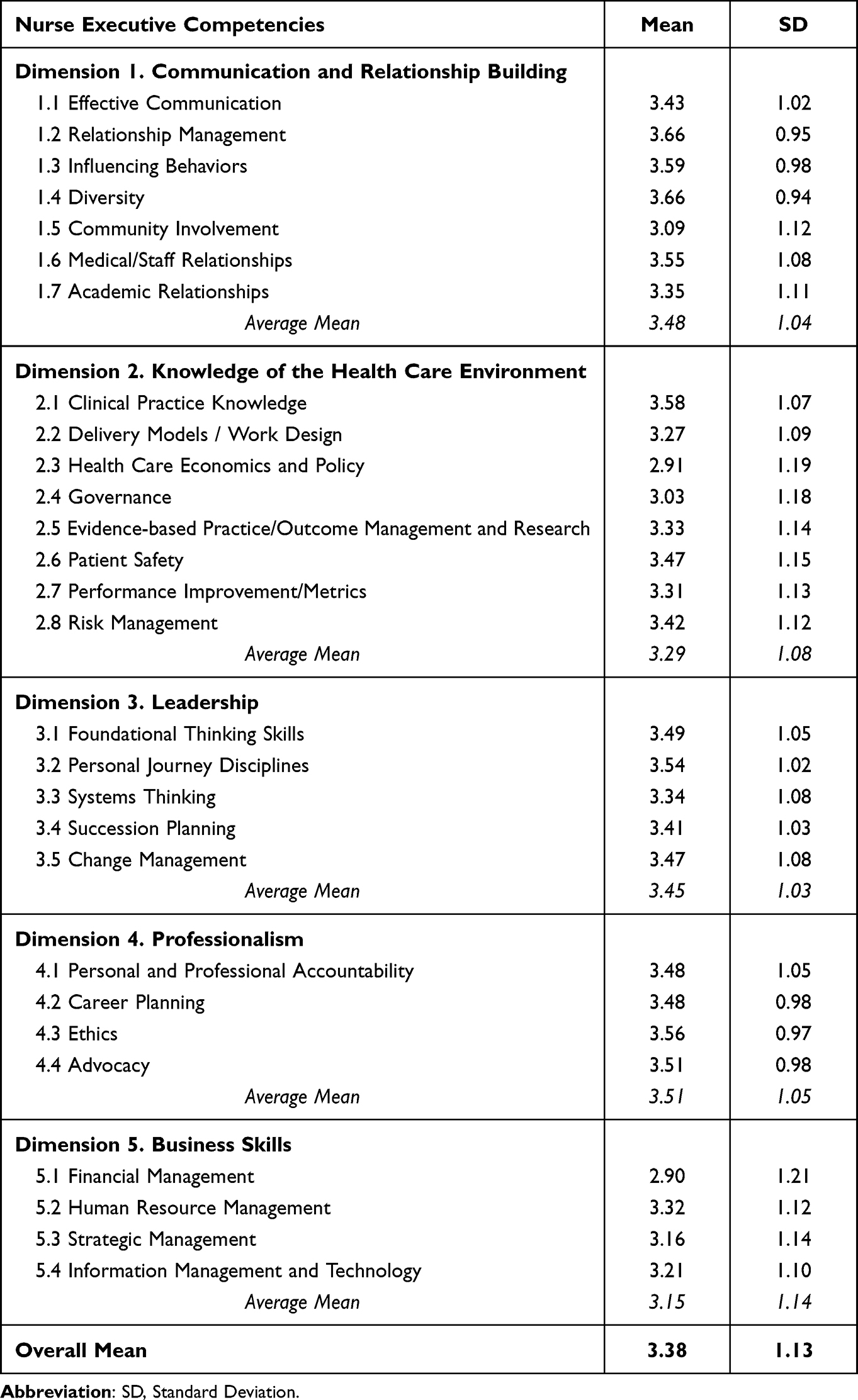 |
Table 2 Leadership Competencies of Nurse Executives (n = 136) |
The third dimension, leadership (Mean=3.45, SD=1.03), had five sub-dimensions, namely foundational thinking skills (Mean=3.49, SD=1.05), personal journey disciplines (Mean=3.54, SD=1.02), systems thinking (Mean=3.34, SD=1.08), succession planning (Mean=3.41, SD=1.03), and change management (Mean=3.47, SD=1.08). The fourth dimension of the leadership competencies of nurse executives is professionalism (Mean=3.51, SD=1.05), the only dimension with mean score above the cut-off of 3.50 that indicated having excellent leadership competencies. This dimension has four sub-dimensions, namely personal and professional accountability (Mean=3.48, SD=1.05), career planning (Mean=3.48, SD=0.98), ethics (Mean=3.56, SD=0.97), and advocacy (Mean=3.51, SD=0.98). The fifth dimension of the leadership competencies of nurse executives is professionalism (Mean=3.15, SD=1.14) with four sub-dimensions, namely financial management (Mean=2.90, SD=1.21), human resource management (Mean=3.32, SD=1.12), strategic management (Mean=3.16, SD=1.14), and information management and technology (Mean=3.21, SD=1.10).
Results of the Test of Correlation between the Personal Profiles and Leadership Competencies of Nurse Executives
This study found significant correlations between the personal profiles and leadership competencies of nurse executives (Refer Table 3). In particular, significant correlations between the communication and relationship building competencies of nurse executives and the following personal profiles were identified: age (X2=31.27, p<0.01), highest educational attainment (X2=19.16, p=0.04), current role as nurse executive (X2=15.98, p=0.02), length of experience as nurse executive (X2=12.61, p=0.01), and attendance in seminars/trainings related to leadership and management (X2=12.82, p=0.01).
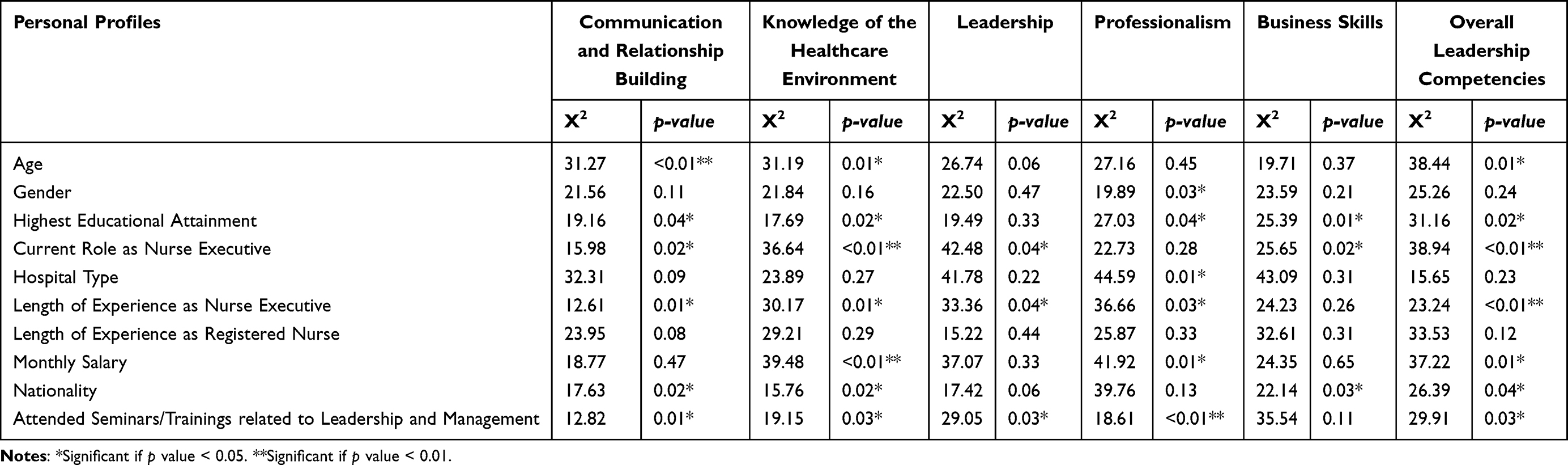 |
Table 3 Test of Correlations Between Personal Profiles and Leadership Competencies |
In addition, age (X2=31.19, p=0.01), highest educational attainment (X2=17.69, p=0.02), current role as nurse executive (X2=36.64, p<0.01), length of experience as nurse executive (X2=30.17, p=0.01), monthly salary (X2=39.48, p<0.01), nationality (X2=15.76, p=0.02), and attendance in seminars/trainings related to leadership and management (X2=19.15, p=0.03) all had significant correlations with knowledge of the healthcare environment competencies of nurse executives. This study also found significant correlations between the leadership competencies of nurse executives and the following personal characteristics: current role as nurse executive (X2=42.48, p=0.04), length of experience as nurse executive (X2=33.36, p=0.04), and attendance in seminars/trainings related to leadership and management (X2=29.05, p=0.03).
Furthermore, the results revealed significant correlations between the professionalism competencies of nurse executives and the following personal characteristics: gender (X2=19.89, p=0.03), highest educational attainment (X2=27.03, p=0.04), hospital type (X2=44.59, p=0.01), length of experience as nurse executive (X2=36.66, p=0.03), monthly salary (X2=41.92, p=0.01), and attendance in seminars/trainings related to leadership and management (X2=18.61, p<0.01). At the same time, highest educational attainment (X2=25.39, p=0.01), current role as nurse executive (X2=25.65, p=0.02), and nationality (X2=22.14, p=0.03) all had significant correlations with the business skills competencies of nurse executives. Finally, the results indicated significant correlations between overall leadership competencies of nurse executives and the following personal characteristics: age (X2=38.44, p=0.01), highest educational attainment (X2=31.16, p=0.02), current role as nurse executive (X2=38.94, p<0.01), length of experience as nurse executive (X2=23.24, p<0.01), monthly salary (X2=37.22, p=0.01), nationality (X2=26.39, p=0.04), and attendance in seminars/trainings related to leadership and management (X2=29.91, p=0.03).
Results of the Multiple Regression Analysis with Personal Profiles as Predictors of the Leadership Competencies of Nurse Executives
In this study, the personal profiles of nurse executives had significant effects or predictions on their leadership competencies based on the results of the multiple regression (See Table 4). In particular, attendance in seminars/trainings related to leadership and management (B =−0.24, p=0.01, CI=−0.03, 0.03) had significant and negative effect on the knowledge of the healthcare environment competencies of nurse executives. Highest educational attainment (B=0.31, p=0.01, CI=−0.09, 0.07), length of experience as nurse executive (B=0.06, p=0.02, CI=−0.15, 0.15), nationality (B=0.12, p=0.03, CI=−0.21, 0.12), and attendance in seminars/trainings related to leadership and management (B=0.13, p=0.01, CI=−0.24, 0.11) all had significant and positive effects on the professionalism competencies of nurse executives. Meanwhile, current role as nurse executive had significant and negative influence on the professionalism competencies of nurse executives (B=−0.10, p=0.04, CI=0.07, 0.09). Length of experience as nurse executive (B=0.18, p=0.01, CI=−0.01, 0.06) had a significant and positive effect on the business skills competencies of nurse executives.
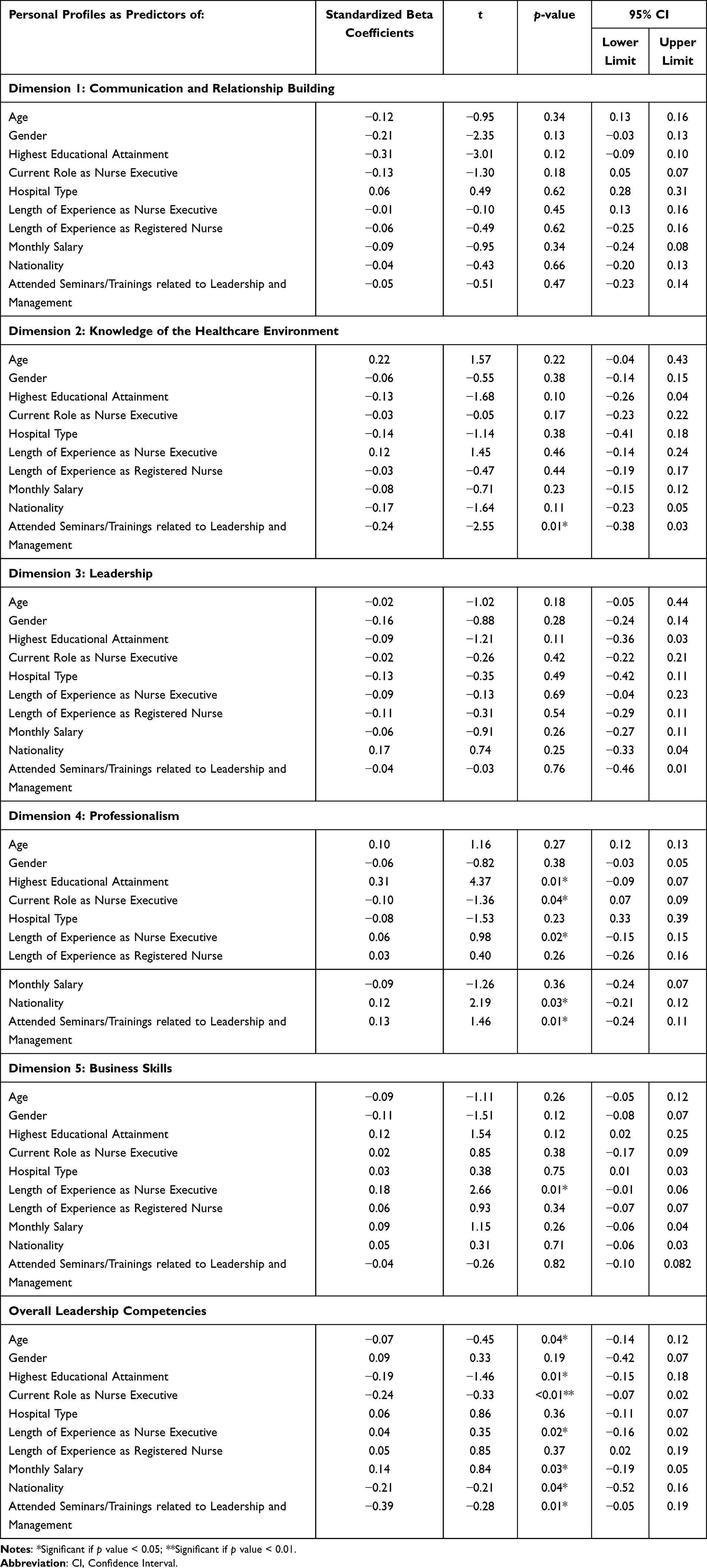 |
Table 4 Multiple Regression with Personal Profiles as Predictors of Leadership Competencies |
In addition, length of experience as nurse executive (B=0.04, p=0.02, CI=−0.16, 0.02) and monthly salary (B=0.14, p=0.03, CI=−0.19, 0.05) both had significant and positive effects on the overall leadership competencies of nurse executives. At the same time, several personal characteristics, namely, age (B=−0.07, p=0.04, CI=−0.14, 0.12), highest educational attainment (B=−0.19, p=0.01, CI=−0.15, 0.18), current role as nurse executive (B=−0.24, p<0.01, CI=−0.07, 0.02), nationality (B=−0.21, p=0.04, CI=−0.52, 0.16), and attendance in seminars/trainings related to leadership and management (B=−0.39, p=0.01, CI=−0.05, 0.19), all had significant and negative effects on the nurse executives’ overall leadership competencies.
Discussion
The overall mean score of the leadership competencies of nurse executives was 3.38 out of 5.0, suggesting that nurse executives needed improvement because the overall mean score was below the cut-off (<3.50). In particular, four out of the five dimensions of leadership competencies, namely, communication and relationship building, knowledge of the healthcare environment, leadership, and business skills, needed improvements because of their mean scores that were below the cut-off. Only the professionalism dimension was above the cut-off, as the respondents generally considered themselves practicing professionalism as nurse executives. The findings could be due to the type of hospital where nurse executives were affiliated as the majority of them worked in government hospitals. In particular, business aspects of healthcare are less expected from those working in government than private hospitals in KSA. This is because healthcare services are provided free to the citizens in all Ministry of Health (MOH) and government hospitals of the country.20,21 Additionally, evidence showed that inequity of care and lack of business ethics in KSA were reported in previous studies.21–24
Nevertheless, nurse executives must develop and improve the necessary competencies, including communication and relationship building, knowledge of the healthcare environment, leadership, and business skills to effectively demonstrate leadership abilities and cultivate credibility and trust in connections established with hospital administrators, medical colleagues, staff members, and the general public.16 The results of this study coincide with previous research that effective leadership necessitates a competency of business skills, encompassing financial acuity, organizational coherence, and effective communication abilities.25,26 Also, the results are contrary to the study in the USA which aimed to gain insights into this subject by examining the perspectives of both emerging and present nurse leaders in Florida.27 The majority (75%) of respondents expressed that nurses are not involved in policy making, lack a cohesive voice, and are not perceived as visible.27 Additionally, it was noted that the presence of 42 major revenue producers served as a hindrance to nursing leadership.27 According to the survey participants, the primary skill requirement for nurse executives is effective communication,27 which is considered important in previous research for several decades.28–30 Moreover, a comprehensive understanding of the healthcare environment is essential for nurse executives to make informed decisions and effectively navigate the complexities of the healthcare industry.3 This includes knowledge of healthcare policies, regulations, quality and safety standards, and emerging trends in healthcare delivery.3 Nurse executives must stay abreast of the changes in the healthcare landscape and understand how these changes impact their organization and the broader healthcare system.3 Leadership is a critical competency for nurse executives, involving the ability to articulate a compelling vision, foster a positive organizational culture, empower and develop staff, and make strategic decisions that drive high quality performance and innovation.31 Nurse executives must also demonstrate emotional intelligence, resilience, and ethical decision-making in their leadership approach.31 In today’s complex healthcare landscape, nurse executives must possess business acumen to effectively manage resources, drive operational efficiency, and contribute to the financial sustainability of their organizations.32 Business skills encompass financial management, strategic planning, data analysis, and an understanding of healthcare economics.32
The results revealed significant correlations between the personal profiles and leadership competencies of nurse executives. The leadership competencies of nurse executives were significantly correlated with certain personal profiles, namely age, highest educational attainment, current role as nurse executive, length of experience as nurse executive, monthly salary, nationality, and attendance in seminars/trainings related to leadership and management. Meanwhile, personal characteristics of nurse executives including age, highest educational attainment, current role, years as nurse executive, monthly salary, nationality, and having seminars/trainings in leadership and management were considered predictors of the leadership competencies of nurse executives. Given the significance of the nurse executives position within a hospital and the necessity for a comprehensive understanding of the evolving healthcare landscape, it is imperative to ensure that nurses receive adequate education and training to effectively assume leadership roles in nursing administration.12,13 According to a qualitative study conducted by Prestia,33 it was determined that possessing a drive and enthusiasm for nurse executive leadership is insufficient on its own. Instead, the attainment of education and competencies is necessary to boost one’s ability to excel in this role.33 By acquiring higher levels of education, nurse executives will enhance their capacity to employ increased levels of innovation in addressing issues that impact the workplace and the provision of nursing care.34 This can be achieved through the utilization of a comprehensive approach that encompasses all aspects of problem-solving that aims to identify sustainable solutions that do not compromise the quality of patient care while also ensuring financial viability for healthcare institutions.34
The importance of training in nursing leadership since the early years of nursing education has been emphasized as essential for future nursing leaders, further underlining the significance of education in developing leadership competencies.35 The need for a consistent framework for nursing leadership education and an evidence base has been highlighted, indicating the importance of structured education in developing leadership competencies among nurse executives.36 The years of experience has been identified as a significant predictor of nurses’ willingness to lead.37 This indicates that as nurse executives gain more experience, they may become more willing to take on leadership roles.37 Seo et al38 highlighted that nursing competence increases with years of experience suggesting that as nurse executives gain more experience, they become more competent. However, Friedman et al39 identified a gap between identity and reputation in nurse executive leadership, suggesting that self-awareness and personal development may also play a crucial role in leadership effectiveness, independent of experience. This indicates that while experience is important, other factors such as self-awareness and personal development should also be considered in assessing leadership competencies.39
The relationship between nationality and nursing executive leadership competency is essential to consider the impact of effective nurse leadership on healthcare outcomes.40 The healthcare system in KSA serves a diverse population with a culturally diverse nursing workforce and the nursing executive leadership competency in this context is crucial to ensure high-quality care and patient safety.41 Feliciano et al42 emphasized the impact of diverse nursing preparations on nursing competencies in KSA, including leadership competencies, suggested that nationality may influence the development of leadership competencies among nurse leaders. As the nursing workforce in KSA is culturally diverse,41 this presents challenges in ensuring that nursing executive leadership is competent in managing a workforce with different nationalities and cultural backgrounds.42 The leadership competencies of nursing executives are crucial in addressing the varied professional competencies of nurses, which may affect the delivery of healthcare services to Saudi public. In addition, the mastery of change management methods is crucial for nurse executives to lead successfully in dynamic healthcare settings.43 This suggests that the ability to navigate change and lead effectively is a critical component of the leadership competencies of nursing executives.43
Moreover, the findings could be attributed to the requirements for being a nurse executive. The American Nurses Credential Center’s Magnet® Recognition Program requires the minimum educational qualification for nurse executives as a master’s degree.44,45 Aside from having the minimum educational qualification, other recommendations are considered including obtaining a doctorate degree in nursing, enrolling in continuing educational activities, and participating in mentorship programs.10,12,13 Mentorship program initiatives address barriers to career advancement, facilitate succession in the organization and increase diversity in nurse executive leadership.46 Harris46 added that diversity among nurse leaders improves self-efficacy of those leaders, ensures equitable care for minority patient populations and improves patient satisfaction.
Strengths and Limitations of the Study
This study has strengths to offer. Notably, to the researcher’s best knowledge, this study is the first to be conducted on this topic in the country. In addition, this study used a standardized assessment tool from AONL.4 Another strength is that the researcher distributed the survey throughout the country through the CNAC, with members practicing and working as nurse executives in their respective hospitals.
However, the current study also has limitations that may serve as basis for improvements in future research related to the leadership competencies of nurse executives. First, there was no participation within some regions in the country. Thus, the study relied solely on the available responses of nurse executives, and this might have reduced the power of the generalizability of this quantitative study to those non-represented regions. Second, the study results were based on the self-assessment of nurse executives, and this might have caused some degree of bias in answering the online surveys. Lastly, nurse executives’ modesty may cause them to self-rate themselves lower than they practice.
Conclusions
The study’s findings revealed that nurse executives reported low levels of leadership competencies, thereby implying that necessary actions for improvement must be initiated. The findings also highlighted the importance of identifying specific areas for the development and improvement of the leadership competencies of nurse executives. In addition, several personal characteristics that significantly influenced the leadership competencies of nurse executives have been identified including age, highest educational attainment, current role and length of experience as nurse executive, monthly salary, nationality, and having seminars/trainings in leadership and management.
Implications and Recommendations for Nursing Education, Practice, and Future Research
To achieve quality outcomes and maintain a high level of nursing care in the hospital organizations of KSA, the study’s findings must be considered in planning for strategies related to the improvement of the leadership competencies of nurse executives. In addition, competent and confident nurse executives are critical in ensuring positive relationships between nurse managers and clinical or staff nurses, this kind of study, which utilized a competency-based leadership assessment, is needed in identifying the development needs of nurse executives, such as in the areas of communication and relationship building, knowledge of the healthcare environment, leadership, and business skills. This competency-based leadership assessment is also vital, because nurse executives can influence and create healthy work environments for staff nurses and help design institutional and healthcare policies for various hospital organizations.
Nurse executives play an important role in building positive communication and harmonious relations, promoting leadership and safety of patient care, effective practice environments for nurses, and the effective and successful performance of organizations and business entities in the healthcare industry. Hence, the findings recognized in this study can be used as valuable references for future educational trainings for hospital and nursing leaders to understand the areas where nurse executives need improvement regarding their leadership competencies, particularly in terms of communication and relationship building, knowledge of the healthcare environment, leadership, and business skills.
For nursing practice, this study also indicates that nurses who want to be promoted to nurse executive positions should work on their leadership competencies relevant to this leadership role’s requirement. Finally, future research can be conducted with consideration to other confounding factors, larger numbers of respondents, and other qualitative approaches to explore why nurse executives tend to have low levels of leadership competencies.
Ethical Statement
This study obtained ethical approval from King Saud University Medical City (Reference Number: E-22-7135).
Disclosure
The authors declare no conflicts of interest related to the publication of this manuscript.
References
1. Heinen M, van Oostveen C, Peters J, Vermeulen H, Huis A. An integrative review of leadership competencies and attributes in advanced nursing practice. J Adv Nurs. 2019;75(11):2378–2392. doi:10.1111/jan.14092
2. González-García A, Pinto-Carral A, Pérez-González S, Marqués-Sánchez P. Nurse managers’ competencies: a scoping review. J Nurs Manag. 2021;29(6):1410–1419. doi:10.1111/jonm.13380
3. González García A, Pinto-Carral A, Pérez González S, Marqués-Sánchez P. A competency model for nurse executives. Int J Nurs Pract. 2022;28(5):e13058. doi:10.1111/ijn.13058
4. American Organization for Nursing Leadership (AONL). AONL Nurse Manager Competencies. Chicago, IL: AONE, AONL; 2022.
5. American Organization of Nurse Executives. Aone nurse executive competencies; 2005. Available from: http://www.nurseleader.com/article/S1541-4612(05)00007-8/abstract.
6. Waxman KT, Roussel L, Herrin-Griffith D, D’Alfonso J. The AONE nurse executive competencies: 12 years later. Nurse Leader. 2017;15(2):120–126. doi:10.1016/j.mnl.2016.11.012
7. Warshawsky NE, Caramanica L, Cramer E. Organizational support for nurse manager role transition and onboarding: strategies for success. J Nurs Administrat. 2020;50(5):254–260. doi:10.1097/NNA.0000000000000880
8. Simpson RL. Chief nurse executives need contemporary informatics competencies. Nurs Econ. 2013;31(6):277–288.
9. Brydges G, Krepper R, Nibert A, Young A, Luquire R. Assessing executive nurse leaders’ financial literacy level: a mixed-methods study. J Nurs Adm. 2019;49(12):596–603. doi:10.1097/NNA.0000000000000822
10. Ecoff L, Stichler JF. Development and psychometric testing of a leadership competency assessment. J Nurs Adm. 2022;52(12):666–671. doi:10.1097/NNA.0000000000001229
11. Sritoomma N, Wongkhomthong J. The components of strategic leadership competencies of chief nurse executives in private hospitals in Thailand. J Nurs Manag. 2021;29(7):2047–2055. doi:10.1111/jonm.13361
12. Strudwick G, Nagle LM, Morgan A, et al. Adapting and validating informatics competencies for senior nurse leaders in the Canadian context: results of a delphi study. Int J Med Inform. 2019;129:211–218. doi:10.1016/j.ijmedinf.2019.06.012
13. Strudwick G, Nagle L, Kassam I, Pahwa M, Sequeira L. Informatics competencies for nurse leaders: a scoping review. J Nurs Adm. 2019;49(6):323–330. doi:10.1097/NNA.0000000000000760
14. Gunawan J, Aungsuroch Y. Managerial competence of first-line nurse managers: a concept analysis. Int J Nurs Pract. 2017;23(1):1–7. doi:10.1111/ijn.12502
15. Gunawan J, Aungsuroch Y, Fisher ML, Marzilli C, Liu Y. Factors related to the clinical competence of registered nurses: systematic review and meta- analysis. J Nurs Scholarsh. 2020;52(6):623–633. doi:10.1111/jnu.12594
16. Meadows MT. New competencies for system chief nurse executives. J Nurs Adm. 2016;46(5):235–237. doi:10.1097/NNA.0000000000000336
17. Saleh U, O’Connor T, Al-Subhi H, Alkattan R, Al-Harbi S, Patton D. The impact of nurse managers’ leadership styles on ward staff. Br J Nurs. 2018;27(4):197–203. doi:10.12968/bjon.2018.27.4.197
18. Kang H. Sample size determination and power analysis using the G*power software. J Educ Eval Health Prof. 2021;18:17. doi:10.3352/jeehp.2021.18.17
19. Stichler JF, Ecoff L. Nurse leadership competency self-assessment study: identifying leadership development needs for a healthcare system. Sigma Repository; 2016. Available from: http://hdl.handle.net/10755/601995.
20. Mufti MHS. Healthcare Development Strategies in the Kingdom of Saudi Arabia. Berlin, Germany: Springer; 2000.
21. Rahman R. The privatization of health care system in Saudi Arabia. Health Serv Insights. 2020;13:1178632920934497. doi:10.1177/1178632920934497
22. Pollock A. NHS Plc: The Privatisation of Our Health Care. London, England: Verso; 2005.
23. Powell M. Who killed the English National Health Service? Int. J Health Policy. 2015;4:267.
24. Almutairi A, Al Shamsi H. Healthcare system accessibility in the face of increasing privatisation in Saudi Arabia: lessons from Australia. Glob J Health Sci. 2018;10(7):111–121. doi:10.5539/gjhs.v10n7p111
25. Haines S. The Business Acumen Handbook: Everything You Need to Know to Succeed in the Corporate World. USA: Jenkins Group Publishing Services; 2019.
26. Dawes N. Senior manager leadership competencies to promote and protect Australian residential aged care quality of care. [Doctoral dissertation, James Cook University]; 2022.
27. Denker AL, Sherman RO, Hutton-Woodland M, Brunell ML, Medina P. Florida nurse leader survey findings: key leadership competencies, barriers to leadership, and succession planning needs. J Nurs Adm. 2015;45(7–8):404–410. doi:10.1097/NNA.0000000000000222
28. Dunham J, Fisher E. Nurse executive profile of excellent nursing leadership. Nurs Adm Q. 1990;15(1):1–8. doi:10.1097/00006216-199001510-00004
29. George V, Farrell M, Brukwitzki G. Performance competencies of the chief nurse executive in an organized delivery system. Nurs Adm Q. 2002;26(3):34–43. doi:10.1097/00006216-200204000-00007
30. Sittler LF, Criswell JR. Using a dyad model for mentoring: the role of the CNO in growing the next generation of executive nurse leaders. Nurse Leader. 2019;17(4):321–324. doi:10.1016/j.mnl.2019.05.008
31. Daradkeh LF, Villar RC, Nashwan AJ. The perception of nursing leaders towards communication and relationship management competencies in using digital platforms during COVID-19 in Qatar: a cross-sectional study. J Nurs Manag. 2022;30(7):2707–2714. doi:10.1111/jonm.13722
32. Foxx M, Garner C. Qualifications of executive nurses for service on hospital boards. J Nurs Adm. 2021;51(12):626–629. doi:10.1097/NNA.0000000000001085
33. Prestia AS. Chief nursing officer sustainment. J Nurs Adm. 2015;45(11):575–581. doi:10.1097/NNA.0000000000000266
34. Ingwell-Spolan C. Perceived work experiences of chief nursing officers. Nurse Leader. 2016;14(2):134–138. doi:10.1016/j.mnl.2015.04.001
35. Aydogdu A. Exploring different aspects of nursing leadership: an integrative review of qualitative studies. Mod Care J. 2023;20(4). doi:10.5812/modernc-130402
36. Miles J, Scott E. A new leadership development model for nursing education. J Prof Nurs. 2019;35(1):5–11. doi:10.1016/j.profnurs.2018.09.009
37. Sabei S, Ross A, Lee C. Factors influencing nurses’ willingness to lead. J Nurs Manag. 2018;27(2):278–285. doi:10.1111/jonm.12698
38. Seo K, Jang T, Kim T. Validity and reliability of the Korean version of the holistic nursing competence scale. Int J Environ Res Public Health. 2022;19(12):7244. doi:10.3390/ijerph19127244
39. Friedman A, Hancock B, Thompson P. Data-based self-awareness as the foundation for effective leadership. J Nurs Administrat. 2021;51(10):478–480. doi:10.1097/nna.0000000000001049
40. Orukwowu U. The impact of effective nurse leadership on quality healthcare outcomes. IPS Interdiscip Journal of Soc Sci. 2022;1(1):1–6. doi:10.54117/iijss.v1i1.1
41. Halabi J, Lepp M, Nilsson J. Assessing self-reported competence among registered nurses working as a culturally diverse work force in public hospitals in the kingdom of Saudi Arabia. J Transcult Nurs. 2020;32(1):69–76. doi:10.1177/1043659620921222
42. Feliciano EE, Feliciano AZ, Maniago JD, et al. Nurses’ competency in Saudi Arabian healthcare context: a cross-sectional correlational study. Nurs Open. 2021;8(5):2773–2783. doi:10.1002/nop2.853
43. Mislan T, Johnson K, Keitel S. Leading the development of a network-wide professional practice model. Nurs Adm Q. 2021;45(4):285–294. doi:10.1097/naq.0000000000000491
44. Magnet ®. The 2023 magnet application manual ®. Silver Spring, MD: American Nurses Credentialing Center; 2023. Available from: https://www.nursingworld.org/nurses-books/2023-magnet-application-manual2/.
45. Lal MM. Introducing the 2023 magnet application manual®. J Nurs Adm. 2021;51(12):593–594. doi:10.1097/NNA.0000000000001090
46. Harris TJ. The reality for minorities exploring nurse executive leadership. J Nurs Adm. 2021;51(6):E18–E19. doi:10.1097/NNA.0000000000001026
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.